
Abstract
The sheep is a popular animal model for human biomechanical research involving invasive surgery on the hind limb. These painful procedures can only be ethically justified with the application of adequate analgesia protocols. Regional anaesthesia as an adjunct to general anaesthesia may markedly improve well-being of these experimental animals during the postoperative period due to a higher analgesic efficacy when compared with systemic drugs, and may therefore reduce stress and consequently the severity of such studies. As a first step 14 sheep cadavers were used to establish a new technique for the peripheral blockade of the sciatic and the femoral nerves under sonographic guidance and to evaluate the success rate by determination of the colorization of both nerves after an injection of 0.5 mL of a 0.1% methylene blue solution. First, both nerves were visualized sonographically. Then, methylene blue solution was injected and subsequently the length of colorization was measured by gross anatomical dissection of the target nerves. Twenty-four sciatic nerves were identified sonographically in 12 out of 13 cadavers. In one animal, the nerve could not be ascertained unequivocally and, consequently, nerve colorization failed. Twenty femoral nerves were located by ultrasound in 10 out of 13 cadavers. In three cadavers, signs of autolysis impeded the scan. This study provides a detailed anatomical description of the localization of the sciatic and the femoral nerves and presents an effective and safe yet simple and rapid technique for performing peripheral nerve blocks with a high success rate.
The sheep is a valuable animal model for biomechanical and translational research due to its relatively inexpensive husbandry and easy handling.1–4 Analogies between various ovine and human joints as well as a high comparability of the ovine bone morphology with the human skeleton enable not only studies concerning the replacement of joints and ligaments but also the treatment of chondral and osteochondral defects.5,6 Many of the surgical procedures are highly invasive and painful thus requiring adequate perioperative pain management to ensure postoperative well-being.7–11
The use of locoregional anaesthesia techniques allows the depth of anaesthesia to be reduced during surgery and decreases the need for systemic analgesic drugs during and after surgery due to their long-lasting analgesic efficacy.7,12 In humans, application of such techniques often allows the induction of general anaesthesia to be circumvented. Furthermore, the risk of adverse effects such as vomiting and nausea is minimized during the postoperative phase while pain is reduced and patients can be released from the hospital earlier.13–15 In most animals, the need for unconsciousness during orthopaedic surgery remains unavoidable due to a lack of compliance.
A large variety of regional anaesthesia techniques has been described in dogs and cats.16–18 In small ruminants, only a few methods have been evaluated so far, spinal administration of analgesic drugs being the technique of choice for surgery on the hind limb.19–21 However, bilateral motor blockade can cause severe stress during recovery.20,22,23 The intra-articular administration of analgesic drugs leads to effective analgesia during and after surgery involving the stifle joints,24,25 though cytotoxic effects of local anaesthetics on articular chondrocytes have recently been demonstrated in vitro. 26
The sciatic and the femoral nerves are the main nerves of the hind limb. A peripheral blockade of these nerves allows surgery of the knee and the tibia to be performed and, therefore, is a popular technique in human and small animal medicine.27,28
The innervation of the hip joint is species-specific. In the dog, this joint is innervated by the sciatic and the femoral nerves, the latter apparently containing both motor and sensory fibres, and the glutaeus cranialis nerve with a pure motor function. 29 In humans and horses, the obturator nerve, which is also considered to be purely motor, is involved as well.30,31 No species-specific information has been published for ruminants so far.
Until now, the neuraxial administration of analgesic drugs has been the only technique allowing effective anaesthesia of the hip joint in sheep, 21 as a very proximal blockade of the sciatic nerve is needed to block sensory afferents from this area. In humans and dogs, the paravertebral or parasacral administration of local anaesthetics to the sciatic nerve leads to an adequate level of perioperative analgesia in the hip joint.32,33 This approach reduces the potential for cardiovascular side-effects such as hypotension and bradycardia and reduces the risk for postoperative complications compared with epidural anaesthesia. 34 As a consequence, postoperative well-being may be improved in animals and humans.7,33,35
Several anatomical landmarks can be used for the perineural administration of local anaesthetics to the sciatic and the femoral nerves. Notwithstanding, the success rate of these blocks could be even further increased with smaller volumes of injected local anaesthetics when using a nerve stimulator.17,33 Lately, the technique has been further developed and perineural injections can now be performed under sonographic guidance. Various ultrasound-guided locoregional anaesthesia techniques have been established in human and small animal medicine.36–40 To the authors’ knowledge, however, the blockade of the sciatic and the femoral nerves under ultrasound guidance has not previously been described in sheep.
The direct visualization of the needle and of the target nerve as well as of the surrounding anatomical structures such as blood vessels, bone, muscles, tendons and fat tissue allows an exact positioning of the needle tip close to the targeted nerve. Due to real-time visualization of the spreading of the local anaesthetic, the drug volume used can be minimized. A precise localization of the target nerve leads to a faster onset of blockade, a longer duration of effect and therefore a better quality of nerve blockade. 41
As a first step in the process of establishing a new technique, it is useful to inject dye into cadavers in order to assess the success rate by staining the target nerves.36,37,42
The aim of this study was to establish the technique of perineural injection of methylene blue close to the sciatic and femoral nerves under ultrasound guidance in sheep cadavers and to evaluate the distribution of a minimal amount of methylene blue solution at the desired locations. We hypothesized that it would be possible to visualize the sciatic and the femoral nerves by ultrasound in adult sheep cadavers and that the injection of a small volume of methylene blue would lead to a distinct colorization of the target nerves.
Materials and methods
Animals
Fourteen cadavers of adult farm-bred female Swiss Alpine sheep with a mean weight of 72 (56–83) kg were used in this study. The animals were euthanized at the end of an experimental cardiovascular trial.
Both hind limbs, the pelvis and the lumbar spine were abscised in toto before freezing for 2–8 weeks. The cadavers were thawed for 36 h at room temperature before starting the experiment.
Pilot study
In one sheep, the anatomy of the sciatic and the femoral nerves was assessed and compared with the structures previously identified by ultrasound (linear array probe, 6–13 MHz; MTurbo®, Sonosite, Seattle, WA, USA).
Procedures
After ‘sternal’ positioning of the cadavers, the skin and subcutaneous fat tissue were gently removed as these had become hard and dry due to the freezing process. The sacrum and the tuber coxae were palpated and used as anatomical landmarks. A linear array probe (6–13 MHz; MTurbo®, Sonosite,) was positioned on the tuber coxae at an angle of approximately 70° to the long axis of the cadaver and moved in a caudal direction until the sciatic nerve could be visualized where it left the foramen ischiadicum majus. A needle specifically designed for injections under ultrasound guidance (22 G × 80 mm; SonoTAP cannula®, Pajunk, Geisingen, Germany) was positioned in-plane in a lateromedial direction until the needle tip could be detected in close proximity to the nerve (Figure 1). Methylene blue solution (0.5 mL; 0.1%) was then injected under sonographic control. Due to the small volume, the space being occupied by the injected fluid was not visible.
Ultrasonographic image of the left sciatic nerve (a) near the greater sciatic foramen. Needle (b) with its reflector mark and the ilium (c).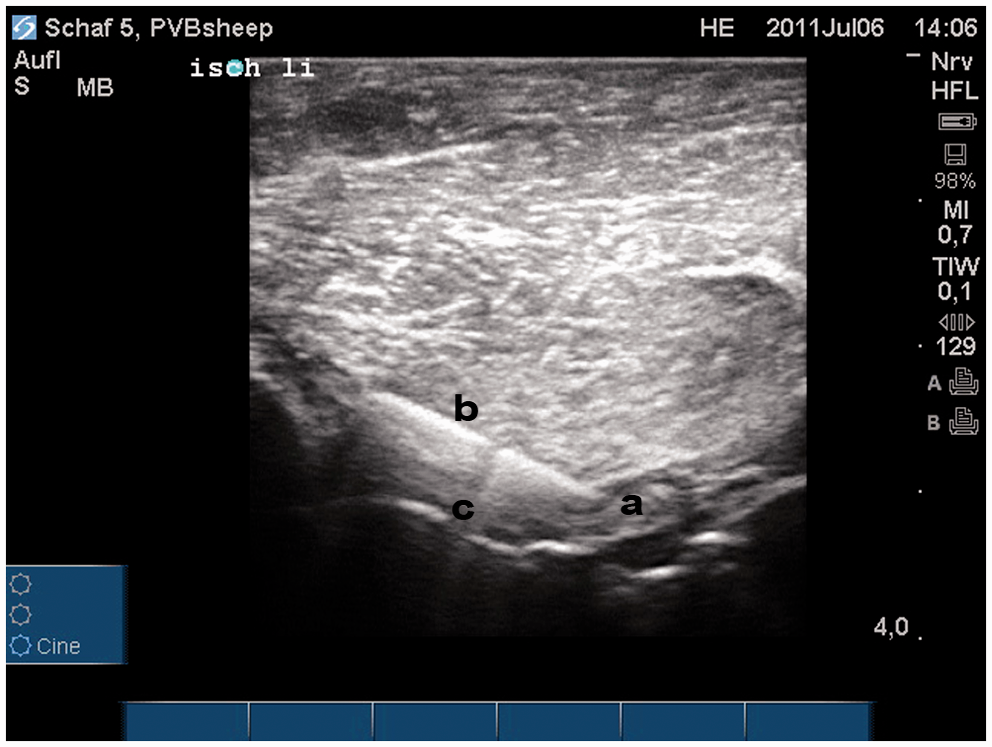
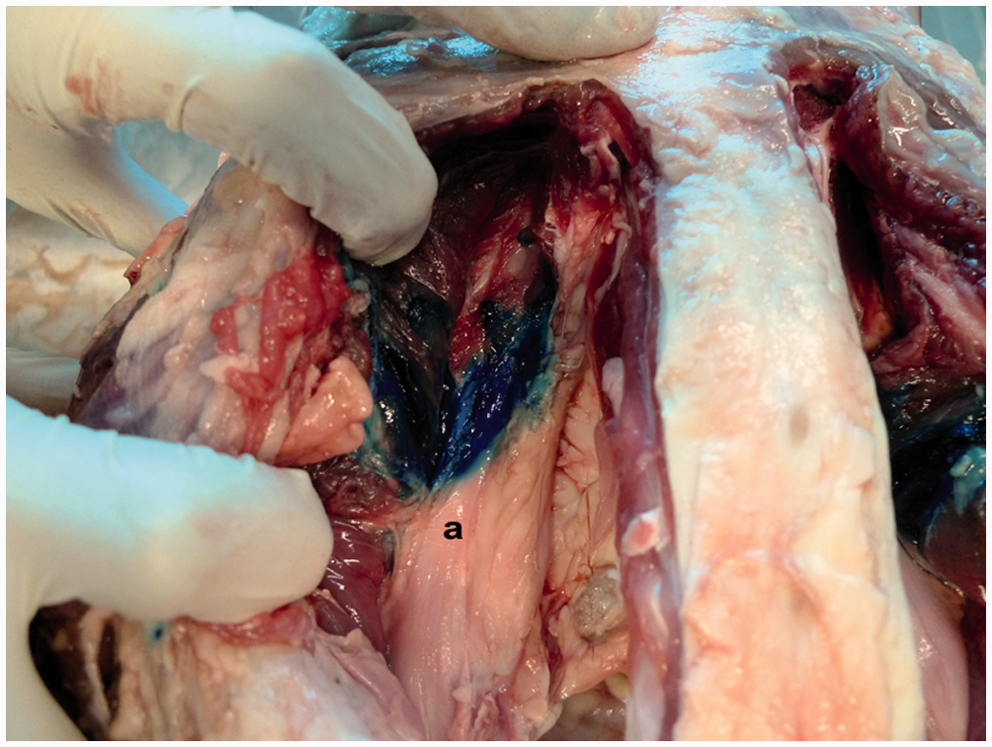
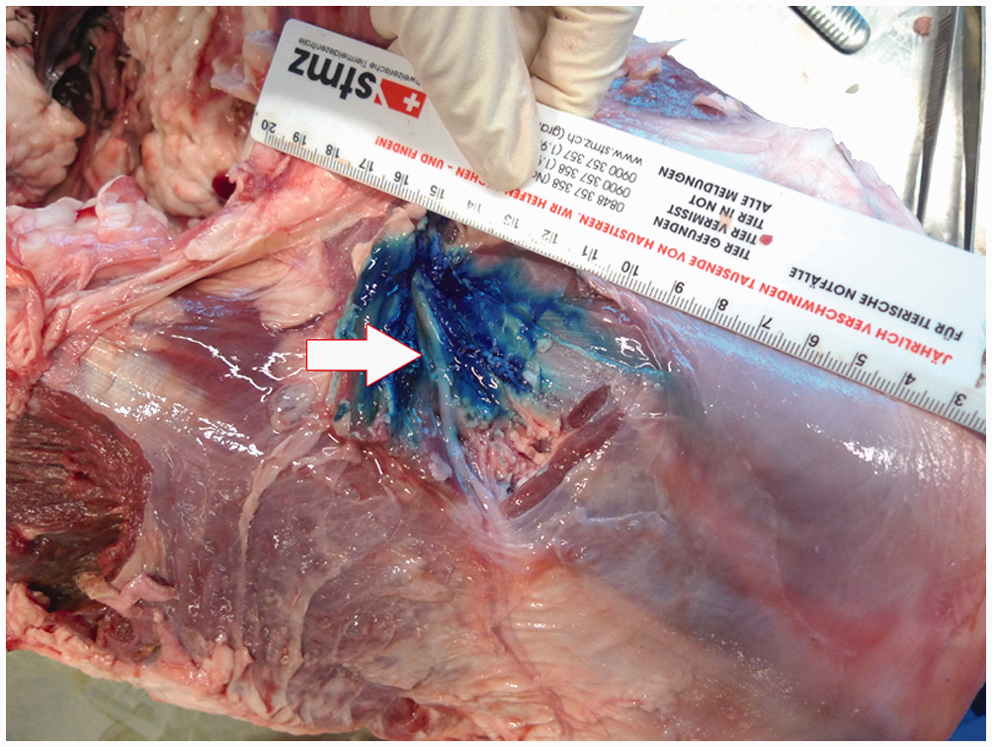
In a second step, the cadaver was positioned in supine position. The sartorius muscle at the midpoint of the medial aspect of the thigh was used as an anatomical landmark. The probe was positioned perpendicular to the long axis of the thigh upon the sartorius muscle and was moved in a proximal and caudal direction until the femoral artery, the vein and the nerve could be visualized under the fascia of the sartorius muscle as proximally as possible. The needle was positioned in-plane until the tip of the needle reached the targeted structures (Figure 2). Directly after injection of the methylene blue, the quality of colorization of the target nerves was quantified by measuring of the length of colorization after dissection of both nerves. A photo of the coloured tissue with a scale was taken to allow for later evaluations (Figures 3 and, 4).
Ultrasonographic image of the right femoral nerve, the femoral artery and the femoral vein (d). The needle tip can be seen underneath the fascia of the sartorius muscle near the femoral nerve, the femoral artery and the femoral vein. The sartorius muscle with its triangular appearance (a), the femur (b) and the needle (c). Left pelvis, dorsal view. The sheep cadaver was positioned in sternal recumbency. The left sciatic nerve (a) and the surrounding tissue have been stained with methylene blue. Right pelvic limb, medial view. The cadaver was positioned in supine position. The left femoral nerve and the surrounding tissue have been stained with methylene blue.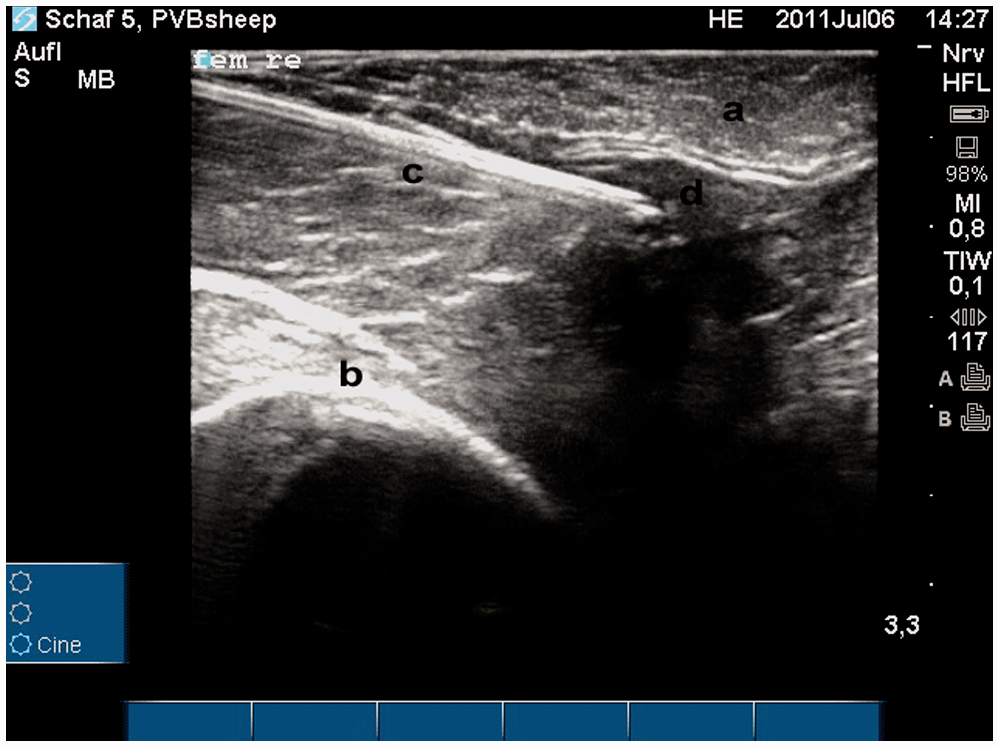
Results
Pilot study
The sciatic nerve was identified sonographically in the foramen ischiadicum majus of the pilot animal (Figure 1). Therefore the tuber coxae and the tuber ischiadicum served as the most important anatomical landmarks. When a line was drawn from the tuber coxae to the tuber ischiadicum, the injection site could be located in the middle of this line.
The sartorius muscle with its triangular appearance and its fascia as the limit between the muscle, nerve and vessels were identified as the most important anatomical landmark for the femoral nerve (Figure 2). The nerve was located underneath the fascia but superficial to the femoral artery and vein.
Main study
We were able to identify 24 sciatic nerves in 12 out of 13 sheep cadavers using ultrasound. They appeared as oval, hypoechoic structures with hyperechoic rims (Figure 1). The cadavers were dissected after injection of methylene blue: 10 sciatic nerves could be stained perineurally using methylene blue over a mean length of 4 cm, eight sciatic nerves were stained either perineurally or along the nerve itself over a mean length of 3 cm (Figure 3), and six sciatic nerves were stained over a mean length of 4 cm.
Twenty femoral nerves were identified in 10 out of 13 sheep cadavers underneath the fascia of the sartorius muscle (Figure 2): in six femoral nerves adequate scanning and perineural injections were not possible due to signs of autolysis, in six femoral nerves, dye was found perineurally over a mean length of 3 cm and in 14 femoral nerves, the mean length of staining was 4 cm (Figure 4).
Again, slight neural staining was expected while every effort was made to avoid intraneural injections.
Discussion
In an effort to further improve analgesia, we evaluated the sciatic and femoral nerve block under ultrasound guidance with encouraging results. With this study we were able to demonstrate the feasibility to block the sciatic and the femoral nerves in sheep with a high success rate. Ultrasound guidance was very useful in detecting and staining the sciatic and the femoral nerves perineurally. The results of this study promise effective blockade of the sciatic and femoral nerves under ultrasound guidance for orthopaedic surgery in sheep.
Anatomy
The sciatic nerve leaves the spine from the segments L6 to S2 of the plexus lumbosacralis and exits the pelvis through the foramen ischiadicum majus. It courses between the gluteus medius and profundus muscles before bending distally between the trochanter major of the femur and the tuber ischiadicum.43,44 The nerve progresses on to the caudal side of the thigh. In the middle of the thigh it splits into the tibial and peroneus communis nerves which run caudally to the fossa poplitea. 45
After leaving the pelvic cavity, the nerve crosses the gemelli muscles between the trochanter major of the femur cranially and the tuber ischiadicum caudally. Along this way, the sciatic nerve sends motor branches to the gluteus profundus muscle, the gemelli muscles and the quadratus femoris muscle. The sciatic nerve is the most important sensory nerve of the hip joint as it dispatches nerve branches to the hip joint capsule. 45 The nerve passes distally to the plantar side of the thigh, deep to the biceps femoris muscle. 43 In the middle of the thigh, the sciatic nerve splits into the tibial and peroneus communis nerves. 45
The desensitization of the hip joint requires a very proximal block of the sciatic nerve in order to block its branches to the hip joint, too.32,33 Between the acetabulum and the sacrum, the sciatic nerve could be visualized sonographically as a hypoechoic structure of an oval shape with a hyperechoic rim. Due to the very deep position of the sciatic nerve and the limited depth of penetration of the ultrasound waves, the sciatic nerve can only be visualized near the foramen ischiadicum majus in sheep by using a linear high frequency transducer.
For surgery in the area of the stifle joint and more distal structures, an additional blockade of the femoral nerve is required.7,39
The femoral nerve originates from the segments L4 to L6 of the plexus lumbalis and reaches the lacuna musculorum in conjunction with the iliopsoas muscle. Distally to these structures, it splits off the saphenous nerve as the main sensory nerve for the stifle joint and exits the abdominal cavity through the lacuna musculorum which is delimited by the ligamentum inguinale and the fascia iliaca. It then enters the quadriceps femoris muscle where it gives off branches innervating the quadriceps femoris muscle.44,45 Close to its origin, the saphenous nerve sends motor branches to the sartorius, pectineus and gracilis muscles and courses in the femoral triangle embedded between the vastus medialis muscle and the sartorius muscle in compound with the femoral artery and vein under the fascia of the sartorius muscle near the caudal margin of the femur between its proximal and middle third.7,38,39,43,44
In this trial, the femoral nerve could not be differentiated from blood vessels due to the lack of blood flow in the cadavers. Consequently, the triad of femoral artery and vein and the saphenous nerve could not be resolved visually from each other.
The femoral nerve can be blocked at the paravertebral level (lumbosacral block). With this approach, the local anaesthetic needs to be injected to the roots of the femoral nerve at three or four injection sites.18,33 At the mid-femoral level, the saphenous nerve can be blocked with one single injection.7,38,39
The peripheral blockade of the sciatic and saphenous nerves allows effective desensitization of the tissue at the hind limbs, especially at the stifle joint and the tibia.7,39 The decisive factor is the localization of the nerve. Anatomical landmarks to block the sciatic and the saphenous nerves under ultrasound guidance or by use of a neurostimulator have been evaluated. In most trials, the sciatic nerve was blocked at the ‘mid-femur’ before the peroneus communis nerve and the tibial nerve diverge near the stifle joint.37,40 The femoral nerve was blocked at the medial aspect of the thigh, distally to the pectineus muscle but cranially to the femoral artery and ventrally to the fascia iliaca. 40
Rasmussen et al. 46 successfully blocked the common peroneal and the tibial nerves at the caudal thigh in the groove between the biceps femoris and semimembranosus/semitendinosus muscle at the midpoint between the patella and the greater trochanter. The saphenous nerve was blocked at the medial aspect of the thigh at the midpoint between the pectineus muscle and the medial epicondyle of the femorotibial joint between the sartorius and gracilis muscles.
With the use of a nerve stimulator, the sciatic nerve can be blocked between the trochanter major and the tuber ischiadicum.7,39,42,47 The femoral nerve can be blocked at the medial thigh cranially to the femoral artery and caudally to the fascia of the rectus femoris muscle 47 and medially to the sartorius muscle. 39
In this trial, we chose a very proximal approach to the sciatic nerve in order to block the nerve before branches for the hip joint are given off: parasacrally in the foramen ischiadicum majus where the nerve crosses the ilium. The saphenous nerve was blocked between the proximal and middle thirds of the femur, underneath the sartorius muscle and superficial to the femoral vessels. The sciatic and the femoral nerves are the main nerves of the hind limb and, thus, have to be blocked for hip or stifle joint surgery to ensure adequate perioperative analgesia. Surprisingly enough, no additional analgesic effect could be detected after blocking these nerves in an experimental study in sheep undergoing a surgical procedure at the stifle joint. 48 The systemic administration of a large variety of analgesic drugs besides the block to the animals might explain this result.
McNamee et al. 49 evaluated the additional obturator nerve block to the sciatic femoral nerve block in humans undergoing total knee replacement. This study showed an improvement in postoperative analgesia by adding the obturator nerve block. In domestic species, the following spinal nerves provide skin sensation at the stifle joint: the iliohypogastric, ilioinguinal, genitofemoral and cutaneous femoral nerves. 45
To the authors’ knowledge, the additional obturator nerve block has not previously been described in sheep. However, the obturator nerve is described as a pure motor nerve with the exception of the stifle joint in horses. 45 Thus, an obturator nerve block is unlikely to improve overall hind limb analgesia.
Learning curve
After a very short period of adjustments, the anatomical landmarks were easily identified. The sciatic and femoral nerve blocks were feasible and rapidly performed. A person lacking previous ultrasound experience quickly learned how to use the ultrasound technique and to improve accuracy and speed in performing the nerve blocks under ultrasound guidance. The possibility of controlling each injection in necropsy further accelerated the learning process.
A steep learning curve of the needle placement under ultrasound guidance has previously been shown for breast cyst aspiration.50,51
Limitations of the study
In two cadavers, the sciatic and the femoral nerves could not be identified because of the limited quality of the cadaveric tissue. Before scanning the cadaver, the skin and the subcutaneous fat tissue of the frozen cadaver had to be removed as they became firm and dry due to the freezing process, thus generating severe artefacts impeding the sonographic view on the underlying structures. When the sciatic nerve was evaluated sonographically in an anaesthetized sheep being involved in another experimental trial, the sciatic nerve could easily be identified.
Use of ultrasound
The necessity of an expensive ultrasound machine might limit the application of such a technique in experimental settings. For this trial, a linear array probe (6–13 MHz) was used to allow the best possible visibility of the sciatic and femoral nerves, but due to the very profound position of the sciatic nerve and the embedding in the muscles, the quality of the ultrasound image was reduced. 41 The use of probes with lower frequency would have led to an increased depth of visualization but also to a loss of detail visibility.
The in-plane technique used in the present study offers significant advantages over the out-of-plane technique as the tip of the needle and the shaft can be visualized while advancing in direct proximity to the target nerve.
The femoral nerve is lying relatively superficial. Anyway, the identification was difficult due to the lack of blood flow through the femoral vessels and the impossibility of differentiating the neural structures from the vessels.
The success rate of peripheral nerve blocks can be significantly increased with the use of ultrasound guidance as compared with the application of a nerve stimulator.39,41,52 Intraneural injections of local anaesthetics can lead to nerve damage and should be avoided. 52 Therefore, complete neural staining was not expected with the minute volumes used.
The use of needles designed for injections under ultrasound guidance with reflector marks allows an even more precise localization of the needle tip. Consequently, with the combination of modern sonographic accessories and the in-plane technique, a successful perineural injection of analgesic drugs can be provided.
As intended in this trial, the small volumes of methylene blue usually stained the perineural tissue instead of the nerve itself. Therefore, intraneural injection of methylene blue could be excluded.
The experiment described here was a pure cadaveric study. Therefore, the analgesic efficacy of the sciatic and femoral nerve blocks could not be evaluated. However, the proof of the principle that both nerve blocks in dogs, humans and goats can desensitize the stifle joint has been established before.7,39,53 To the authors’ knowledge, the effectiveness of a single parasacral sciatic block for hip surgery has not been demonstrated previously, either in humans or in animals.
As a next step it will be necessary to test the described regional anaesthesia techniques in animals undergoing orthopaedic surgery. Even though the duration of effects of local anaesthetics is longer in sheep than in humans, a perineural catheter will be helpful in prolonging the postoperative analgesia for several days.
Conclusions
With this study we provide an exhaustive anatomical description of the localization of the sciatic and femoral nerves by using ultrasound imaging in sheep. The evaluated technique can be performed simply and rapidly and produces precise and clear images of the nerves. In vivo studies will be necessary to assess the efficacy of this technique in providing satisfactory perioperative sensory analgesia and motor blockade.
Footnotes
Declaration of conflicting interests
None of the authors of this paper has a financial or personal relationship with other people or organizations that could inappropriately influence or bias the content of the paper.
Funding
The project was partly funded by the 3R Foundation.