
Abstract
Although prior research has advanced our understanding of the drivers of organ donation attitudes and intentions, little is known about how to increase actual registrations within explicit consent systems. Some empirical evidence suggests that costly, labor-intensive educational programs and mass-media campaigns might increase registrations; however, they are neither scalable nor economical solutions. To address these limitations, the authors conducted a field experiment (N = 3,330) in Ontario, Canada, testing the effectiveness of behaviorally informed promotion interventions as well as process improvements. They find that intercepting customers with materials targeting information and altruistic motives at the right time, along with streamlining customer service, significantly increased registrations. Specifically, the best-performing intervention, prompting perspective taking through reciprocal altruism (“If you needed a transplant would you have one?”), significantly increased new registration rates from 4.1% in the control condition to 7.4%. The authors followed up with seven posttests (total N = 3,376) to find support for their theoretical predictions and to explore the mechanisms through which the interventions may have operated. This article provides evidence for low-cost, scalable marketing solutions that increase organ donor registrations in a prompted choice context and has important implications for public policy and societal welfare.
Current statistics on organ donation point to an ever-increasing demand yet inadequate supply of available donors. For example, in Canada, more than 4,400 people are waiting to receive lifesaving organ transplants (Canadian Blood Services 2019). Similarly, in the United States, there are over 113,000 individuals currently on the transplant waiting list, and 22 people die each day waiting (Donate Life America 2020). Concerningly, the gap between those needing transplants and those receiving them continues to widen (Donate Life America 2020). One way to address the growing demand for transplantable organs is to increase the number of individuals who register as donors (Christmas et al. 2008). To illustrate, in the United States, the “conversion” rate for registered donors who have died and are medically suitable for organ donation is nearly 100% (Thaler and Sunstein 2020).
Low registration rates are especially prevalent in countries with explicit consent registration policies—that is, individuals must opt in to become organ donors—compared with countries with presumed consent policies—where individuals are organ donors by default but can opt out (Johnson and Goldstein 2003). Although changing the default appears to be a promising intervention (Steffel, Williams, and Tannenbaum 2019), the impact on actual donations has been mixed due to, among other things, uncertainties about a deceased person’s donation preferences (Domínguez and Rojas 2013; Noyes et al. 2019). Furthermore, changing registration policies involves implementation challenges and ethical considerations surrounding informed consent (Ferguson, Murray, and O’Carroll 2019). To date, most jurisdictions have maintained their existing policies (Saab et al. 2018), thus prompting the following question: What can be done within explicit consent systems to improve organ donor registration rates?
Prior research has identified factors predicting organ donation attitudes and intentions, such as having adequate information about organ donation as well as altruistic motives (for reviews, see Falomir-Pichastor, Berent, and Pereira [2013] and Radecki and Jaccard [1997]). However, attitudes and intentions do not consistently translate into actual registrations (Radecki and Jaccard 1999). In Canada, where we conducted our study, even though the vast majority of Canadians (90%) are in favor of organ donation, and 81% say they themselves would be willing to register (Ipsos 2006), only 23% have actually registered their decision to become an organ donor (Canadian Blood Services 2019).
Furthermore, the limited work focusing on registrations has largely tested elaborate and costly interventions outside of organ donor registration systems (e.g., testing workplace education programs and mass-media campaigns; for reviews, see Feeley and Moon [2009] and Golding and Cropley [2017]). Finally, in a recent article on living organ donation, Bradford and Boyd (2020) emphasized that promotional messages, despite being the primary focus of most charitable giving research (e.g., Fajardo, Townsend, and Bolander 2018; Leipnitz et al. 2018; Liu and Aaker 2008; Reed, Aquino, and Levy 2007; Winterich, Mittal, and Aquino 2013), are only one aspect of the marketing mix that can be employed to solicit donations. Through a qualitative study, they outlined how the entire marketing mix—product, price, promotion, place, process, and people—may be employed to reduce experiences of sacrifice in the complex and cumbersome process to encourage living organ donations.
Our article contributes to the limited empirical evidence for low-cost and scalable marketing solutions to increase actual in-person organ donor registrations in current explicit consent systems. In addition, this research contributes to our understanding of how to employ multiple elements of the marketing mix to help achieve the objectives of nonprofit organizations (Bradford and Boyd 2020). Specifically, our field experiment demonstrates how intercepting customers with promotional materials at the right time (an information brochure and perspective-taking prompts), along with other process improvements (streamlined customer service that includes additional time to review the promotional materials and a simplified form), can increase new organ donor registrations. By leveraging behavioral science to design our marketing interventions, we contribute to the understanding of how to reduce the intention–action gap in the context of organ donation, improve public policy, and enhance societal welfare.
Theoretical Foundations
Organ Donation Systems
Organ donation systems typically take one of two forms: explicit consent and presumed consent. In explicit consent systems, individuals have to enroll in the organ donor registry (i.e., opt in). The specific process can vary, but it usually occurs when people obtain or renew identification (e.g., driver’s license) at a local government office such as the Department of Motor Vehicles. Although many countries have recently made online registries available, to date the majority of registrations still take place offline (Donate Life America 2018). For example, in Ontario, where our research was conducted, 85% of registrations in 2016 occurred in person at ServiceOntario centers (i.e., Department of Motor Vehicles equivalent; Trillium Gift of Life Network 2017).
Within explicit consent systems, one technique used to “nudge those who are willing donors into becoming registered donors” is mandating or “prompting” choice (Thaler and Sunstein 2020, p. 125). In prompted choice contexts, customer service agents ask individuals whether they would like to register their consent to be a donor. Prompting forces individuals to decide, instead of waiting for them to actively volunteer their consent unsolicited, which can help overcome procrastination, inertia, and limited attention (Thaler and Sunstein 2020). However, even when prompting is implemented, many jurisdictions continue to have low organ donor registration rates (Donate Life America 2018; Kessler and Roth 2014). For example, at the time of our field experiment, only 24% of the 12 million eligible Ontarians were registered, despite using prompted choice (Trillium Gift of Life Network 2014).
With the rise of behavioral science and nudging in policy, one solution that has received attention is changing legislation from explicit consent to presumed consent, where individuals are considered organ donors by default but can opt out (Ferguson, Murray, and O’Carroll 2019). Recent evidence finds that donation rates are approximately 30% higher, on average, in countries with presumed consent systems (Steffel, Williams, and Tannenbaum 2019), though default policies were argued to be only one factor among many that determined donation rates (e.g., systems for obtaining family consent, transplant infrastructure, religious beliefs). In fact, some countries even observed a decrease in donations when moving to presumed consent (Arshad, Anderson, and Sharif 2019; Domínguez and Rojas 2013). To date, very few countries have chosen to change their default policy to presumed consent (e.g., Singapore, the United Kingdom, Argentina, the Netherlands; Saab et al. 2018), as doing so can present several challenges. These include (1) a significant investment of time and money (Noyes et al. 2019), (2) ethical concerns relating to informed consent and individual autonomy (MacKay 2015; MacKay and Robinson 2016), and (3) ambiguity for the surviving family about the deceased’s wishes (Beshears et al. 2008). Together, these factors lead Thaler and Sunstein (2020, p. 121) to conclude, We favor the policy of prompted choice because there is no evidence that a viable alternative system would save more lives (and hence is superior in terms of the interests of Patients), and because we think that it does the best job of respecting the rights and interests of Potential Donors and Families. At the same time, we favor more nudges, and better choice architecture, to improve the prompting.
Current Research on Organ Donation Behavior
To date, research focused on actual organ donor registrations remains rare. Golding and Cropley (2017) recently conducted a narrative review of all empirical research measuring actual registrations. Although they identified 24 studies, the authors concluded that many suffered from methodological weakness including selection bias, confounds, and self-reported dependent variables. As a result, the authors could not conduct a meta-analysis or provide clear prescriptions for how to improve registrations. In fact, only eight studies were found to be methodologically robust, and even among these, the majority were conducted outside the current registration systems and tested interventions that were relatively complex, costly, and labor intensive. For example, interventions tested included town halls with expert panels (Alvaro, Siegel, and Jones 2011), mass-media campaigns (Sanner, Hedman, and Tufveson 1995), and workplace lunch-and-learn programs with presentations by transplant recipients and donor family members (Quinn et al. 2006). Though some interventions proved promising (e.g., educational programs), they were neither scalable nor economical ways to improve registration rates within existing explicit consent systems.
One notable exception is recent work by Sallis, Harper, and Sanders (2018), who conducted a field experiment testing the effects of adding persuasive messaging (e.g., using reciprocal altruism or social norms) to an online prompt to join the national organ donor registry in the United Kingdom. The authors found that their reciprocal altruism message (“If you needed an organ transplant would you have one? If so please help others.”) performed best and increased individuals’ sign-ups from 2.3% in the control condition to 3.1%. This study was the first to illustrate the potential for low-cost, scalable interventions, in general, and persuasive messages, specifically, to improve actual organ donor registrations. However, it was unable to distinguish between new and existing donors. In addition, it was conducted outside of the typical organ donor registration system. For example, it was conducted online at a time when most transactions were done in person (U.K. Cabinet Office 2013), after drivers completed their government transactions. Given both the novelty and practical importance of these findings, there are several opportunities to extend this research that are worth pursuing. For instance, what might this effect look like for in-person transactions and on only new registrations? Would these findings replicate when applied within the more typical explicit consent registration system?
Following an early release of these findings (Behavioral Insights Team 2013), O’Carroll et al. (2017) wanted to test the effectiveness of reciprocal altruism persuasive messages on registration intentions in both online and in-person contexts. The authors found that reciprocal altruism primes significantly increased intentions to register online but had no such effect in person. Moreover, no significant effects were found on proxies for donation behavior (i.e., whether participants accessed optional information on organ donation), regardless of mode of delivery. Although this study did not measure actual registrations, it provides some support for the use of reciprocal altruism messages in the organ donation context, while also calling into question whether such messages would be effective for in-person registrations.
Taken together, although prior research on organ donation suggests that targeting altruistic motives and information may be promising, we know little about how to encourage actual, new, in-person organ donor registrations, especially in a low-cost and easy-to-scale manner. We designed our field experiment to explore these opportunities.
Promotional Materials to Increase Actual Organ Donor Registrations
Promotional materials are commonly used by for-profit and nonprofit organizations to inform, persuade, and motivate actions. For example, nonprofit organizations can employ promotional tools when individuals are in the deliberation stage of a donation to help them proceed to the actual decision stage (Bradford and Boyd 2020). We built on prior research to develop and test promotional materials to increase new organ donor registrations by providing information (with an information brochure) and enhancing altruistic motives (with perspective-taking prompts). We supported our interventions with improvements to streamline the registration process (i.e., additional time to review the promotional materials, intercepting customers at the time of decision, and a simplified form).
Information
Most theories of human judgment and decision making argue that individuals make decisions on the basis of declarative knowledge—facts and information—that comes to mind at the time of decision making (for reviews, see Higgins [1996], Wyer [2008], and Wyer and Srull [1989]). The information can be obtained from external sources (such as an information brochure) or retrieved internally from long-term memory. Information can also increase procedural knowledge—the knowledge of how to perform a specific task (Sadler 1989). Studies have shown that providing information targeting each of these types of knowledge encourages action (e.g., Peterson and Pitz 1988; Robitaille, House, and Mazar 2020; Swann and Gill 1997; Tsai, Klayman, and Hastie 2008). In the context of organ donation, declarative information has been shown to be effective at enhancing attitudes, especially when framed positively (e.g., “one individual organ donor can donate organs [e.g., heart, lungs, kidneys, liver] to eight other people”; Reinhart et al. 2007). Messages providing procedural information about how to become a donor were particularly effective at enhancing attitudes when individuals were unaware of these details (McIntyre 1990). Building on the aforementioned research, we predict that providing individuals with promotional material (i.e., an information brochure containing declarative and procedural information), specifically at the point when they are deciding, will make that information salient to them and increase new organ donor registrations.
Altruistic Motives
Altruistic motives arise from empathy toward others and have been found to drive prosocial behavior across multiple domains (Batson 1987; Batson, Early, and Salvarani 1997; Batson and Shaw 1991; Tusche et al. 2016;). Research finds that one effective way to evoke altruistic motives is through perspective taking, considering a situation from a different point of view (Underwood and Moore 1982). In the context of organ donation specifically, perspective taking correlates with positive attitudes and willingness to register (Cohen and Hoffner 2013; Milaniak, Wilczek-Rużyczka, and Przybyłowski 2018), though we do not yet know if perspective taking can be employed to reliably increase actual registrations. Moreover, perspective-taking manipulations have been tested almost exclusively in the lab until recently, and therefore, it is unclear how their effects would translate to field settings (cf. Ku, Wang, and Galinsky 2015; Sallis, Harper, and Sanders 2018).
We sought to test the effectiveness of enhancing altruistic motives on organ donor registrations in the field with three differing perspective-taking prompts: imagine other (IO), imagine self (IS), and reciprocal altruism (RA). The imagine other prompt asks individuals to consider how others would feel in a situation, enhancing one’s pure altruistic motives to help (Batson, Early, and Salvarani 1997). Alternatively, asking individuals to imagine oneself in the situation—imagine self—can increase both one’s altruistic as well as self-interested motives (Cialdini et al. 1987), which some have suggested may be even more effective for encouraging prosocial behavior (Batson and Shaw 1991; e.g., Andreoni 1989; Gershon, Cryder, and John 2020). Perspective-taking prompts can also encourage prosocial behaviors by making additional psychological concepts salient (e.g., reciprocity). For example, recent research has found that the reciprocal altruism prompt “If you needed an organ transplant would you have one? If so please help others” significantly increased online organ donor registrations (Sallis, Harper, and Sanders 2018). Such a statement evokes both self-interest and reciprocity by pointing out that that if individuals are willing to accept an organ, they should also donate (Landry 2006; Stijnen and Dijker 2011; Trivers 1971). Given that prior research has found that benefits to the self as well as benefits to others can drive prosocial behaviors (Batson, Early, and Salvarani 1997; Böckler, Tusche, and Singer 2016), we predicted that prompting these three types of perspective taking (imagine other, imagine self, and reciprocal altruism), would increase actual organ donor registration rates.
Field Experiment Methods
Participants
Our field experiment was conducted over a 2.5-week period (March–April 2014) in one preselected ServiceOntario location in Ontario, Canada—an explicit consent jurisdiction with prompted choice. To maximize the generalizability of our findings, we carefully considered the choice of location for the experiment. The specific location chosen has a sizable population (one of the largest and busiest centers in the province) that is demographically representative of Ontario’s total population on several preselected characteristics including age, income, education, and religion. 1
In 2014, when our experiment was conducted, all Ontarians were required to visit ServiceOntario centers in person for almost any public service including driver’s license, health card, and photo identification transactions, thus reducing sampling bias concerns. 2 Each individual who visited this service center was a participant in our experiment (N = 3,330), and all participants visiting on a given day were exposed to the same experimental condition or phase. Because the timing of the phases and conditions was defined before the start of the experiment, neither the center, nor individual service agents, nor the researchers had control over which individuals received each condition. On average, 214 individuals visited the center each day. New donor registrations were measured using the service center’s computer system. For each individual, we observed the type of transaction(s) they completed, the service agent they saw, and whether they registered during that visit as a new organ donor (yes/no). No identifying information about the participants and service agents was shared with the researchers to maintain privacy and protection of all parties involved.
Standard Organ Donation Registration Process and Materials
The standard in-person registration process in Ontario is similar to that of many prompted choice jurisdictions. Upon arrival at ServiceOntario, individuals are given a number at the reception desk and wait until their number is called. Once called on, individuals perform the transaction(s) they came for at a service agent’s counter, and during these transactions they are prompted to register. That is, they are asked by the service agent if they would like to register their consent as an organ donor today. Only if they affirm, they are then given the center’s standard organ donor registration form to complete on the spot (Figure W1–1 in the Web Appendix).
The standard organ donor registration form is a black-and-white full-page document consisting of three sections (for a visual of the standard form, see Figure 1). The left-hand column primarily presents legal and procedural information about organ donation (e.g., “You have the right to decide whether or not to consent to the donation of your organs and tissue”). Although this information is meant to inform consumers, it is handed to consumers only after they agree to register and thus comes too late in the process. On the right-hand column of the document, the top portion serves to collect personal information from the individual (e.g., name, address, date of birth). It is important to note that for in-person registrations, that information is redundant as customers just completed another transaction in which they provided that information (e.g., renewing a driver’s license) and therefore unnecessarily lengthens the process. Finally, on the bottom right-hand side, individuals are asked to indicate their consent and sign the form.

Registration form layouts.
Experimental Conditions
We created five experimental conditions for our field experiment: A control condition that involved two process changes (time and simplification) and four promotion intervention conditions (information brochure and three perspective-taking prompts). The process changes made in the control condition were also present in all of the experimental conditions, enabling us to test for improvements specifically resulting from our promotion interventions. For an overview of the persuasive materials tested, see Table 1; for the forms and brochure, see Web Appendix W1.
Overview of Promotional Materials.

Control
Our control condition included two process changes designed to streamline customer service and support our interventions tested in the experimental conditions. First, individuals were handed the organ donor registration form with their waiting number when they arrived at the reception desk to allow adequate time to read, process, and consider the materials (vs. during their transaction[s] at the agent’s counter). An additional benefit of handing the form out in advance is that it reduces the variation in registrations that may be caused by the individual service agents 3 and ensures that every customer is handed a registration form.
Second, to increase the salience of our interventions, we created a simplified version of the organ donor registration form 4 (for a comparison of the forms, see Figure 1; for the simplified form, see Figure W1–2 in the Web Appendix). In addition, behavioral research consistently finds that reducing the effort required to perform an action, or even just simplifying content (i.e., reducing “sludge”; Sunstein 2020; Thaler 2018), can increase the number of people taking action (Behavioural Insights Team 2014; Sunstein 2013). In creating our simplified version, we first removed all material from the standard form that was not required, legally or practically, for in-person transactions. As a result, the simplified form retained only the consent questions and a place to sign the form, focusing individuals on the decision at hand. In addition, we added a colored banner on top to add visual appeal, which, importantly, provides a location to highlight the perspective-taking prompts in three of the experimental conditions. Finally, we printed this smaller form on a half sheet of cardstock paper because the thicker, sturdy paper would enable individuals the option to complete the form without counter space (e.g., while waiting).
In all experimental conditions, participants received this simplified form upon arrival at the reception desk. These two process changes—extra time and simplified form—ensured that we could better capture the effect of our key behavioral interventions. Stated differently, without this streamlined customer service, our interventions might not be able to improve registration rates, because they may be overlooked and/or would come too late (i.e., after responding to the prompt to register). The control condition serves as a clean, conservative benchmark that enables us to quantify the effect of our interventions.
Information
Behavioral researchers have argued that policy interventions are more likely to be successful if you consider their timing and prompt people when they are most likely to be receptive (Behavioural Insights Team 2014). In our information condition (info), we aimed to intercept customers and provide information at the right point in time. Although this condition presents promotional material, it is primarily a test of improving process; Ontario’s standard organ donation brochure (see Figure W1–3 in the Web Appendix) includes detailed declarative (e.g., “1 organ donor can save 8 lives”) and procedural information (e.g., “Registering is easy. Ask at the counter or do it online.”) presented in a visually appealing and easy-to-process way (i.e., cleanly organized and relatively large font). This brochure is always readily available to take from self-serve brochure stands in the waiting area of ServiceOntario centers. It is also mailed to individuals with their driver’s license renewal notice. However, in this condition, we tested the impact of handing out the brochure along with the simplified form to all customers when they arrived at the reception desk. By providing this information while individuals were waiting and deciding, we predicted that this would increase their likelihood of reading the brochure; the salience of the information during decision making (Wyer 2008); and, in turn, registrations.
Perspective-taking prompts
The other three experimental conditions targeted altruistic motives using perspective-taking prompts. Participants were handed the simplified registration form with one prompt printed in the colored box at the top of the form (Table 1). First, our reciprocal altruism prompt, “If you needed a transplant, would you have one?” (adapted from Sallis, Harper, and Sanders [2018]), leveraged self-interest, empathy, and reciprocity. Our second prompt, imagine self, leveraged self-interest and empathy by stressing that without enough registered donors, they (the reader) or their loved ones might not have a transplant available if needed. Finally, our third prompt, imagine other, leveraged empathy by highlighting that without enough registered donors, others might not have a transplant available if needed. We conducted a pretest to confirm that each prompt induced the correct perspective taking as intended (see Web Appendix W2).
Timeline of Field Experiment
Our experimental conditions were each run consecutively for three business days. In addition, we added two phases, each pre- and postexperiment, in which we (1) measured registrations with the standard registration process (standard process phases) and (2) included time for acclimating service agents to the procedural changes caused by the experiment and informing them registrations would be tracked, a jurisdictional requirement (acclimation phases; for more details, see Web Appendix W3). During the acclimation phases, visitors were given our new simplified form but otherwise the service center followed the standard registration process. That is, the registration form was handed to individuals during their transactions at the service agent’s counter only if they agreed to the registration prompt. Therefore, in total, data collection spanned an eight-week period beginning on February 24, 2014. For an overview, see Table 2.
Timeline of Field Experiment.

Notes: The chosen location operates six days a week, Monday through Saturday. Due to required messaging sent to service agents informing them it was “the last week” of the organ pilot, A2 was run for one business week (six days) instead of three days. Also, although the standard process phases were planned for two weeks each, one day during SP2 landed on a holiday and the service center was closed. Therefore, we have data for only 11 instead of 12 days.
Results
To analyze the impact of the field experiment on new organ donor registrations, we start by presenting model-free evidence. Here, we adopt a-two-part approach. First, to test the effectiveness of our behavioral interventions, we compare the registration rates of each experimental condition with that in our control condition. Second, to explore the impact of our field experiment process changes (additional time and simplified form) relative to the standard registration process, as well as the impact of acclimating service agents to the experiment, we compare the registration rates in the pre- and postexperimental phases with that in the control. We then present logistic regressions that control for time-varying factors, such as the day of the week and the available agents. Next, we present a set of validity checks and robustness checks that test our hypotheses using alternative modeling specifications. Finally, we present a summary of seven follow-up posttests to provide support for our theoretical predictions and to explore the potential mechanisms through which our interventions may have operated. 5
Model-Free Evidence
Behavioral interventions versus control
The gray-shaded bars in Figure 2 illustrate how registrations were affected by our interventions (see also Table W1–1 in the Web Appendix). A joint F-test confirmed that there were statistically significant differences between the conditions (F = 5.285, p < .001). New organ donor registrations were highest in the reciprocal altruism condition (7.4%; 95% confidence interval [CI] = ±2.08%). In fact, reciprocal altruism was the only condition that significantly increased donor registrations (Δ = 3.30%, p = .012, Cohen’s h = .143) relative to our control condition (4.10%; 95% CI = ±1.51%). That said, registration rates in the reciprocal altruism condition were not significantly greater than any of our other interventions at the 5% level (info: Δ = 1.51%, p = .279; IS: Δ = 2.36%, p = .076; IO: Δ = 2.40%, p = .070).

New organ donor registration rates, raw means.
Pre- and postexperiment phases versus control
We found that the registration rate in our control condition was not significantly different from that in any of the pre- and postexperimental phases (all ps
Logit Model
Behavioral interventions versus control
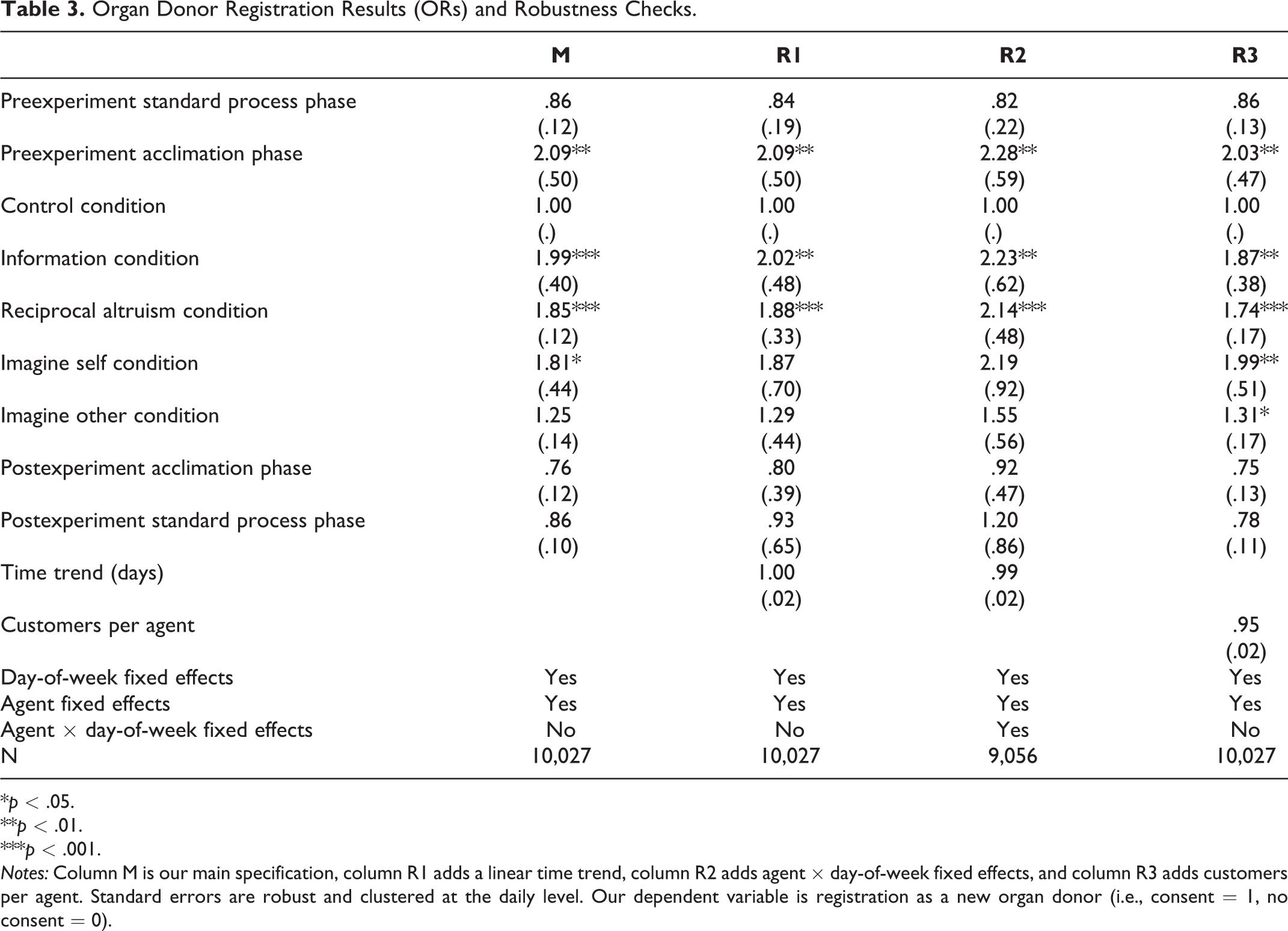
Because each experimental condition was run for three consecutive days, we account for potential differences across days when treatments were applied. To do so, we ran a fixed-effects logistic regression using all individuals who engaged in a transaction during our entire eight-week data collection period (i.e., during the experimental and pre- and postexperimental phases; N = 10,043). In this analysis, we controlled for day of week fixed effects and agent serving each individual (“agent”) fixed effects. 6 Our experimental control condition served as the baseline. To be conservative, we use robust standard errors and have clustered all standard errors at the daily level as this was the unit where treatments were assigned (Abadie et al. 2017). The dependent variable was whether an individual registered as a new organ donor (see Table 3). Results are presented in terms of odds ratios (ORs), that is, the odds that an individual registered as a new organ donor given a particular treatment (e.g., information condition) compared with the odds of the individual registering in the control condition.
Organ Donor Registration Results (ORs) and Robustness Checks.
*p < .05.
**p < .01.
***p < .001.
Notes: Column M is our main specification, column R1 adds a linear time trend, column R2 adds agent × day-of-week fixed effects, and column R3 adds customers per agent. Standard errors are robust and clustered at the daily level. Our dependent variable is registration as a new organ donor (i.e., consent = 1, no consent = 0).
The results of this analysis appear in column 1 of Table 3 (overall model: χ2 (d.f. = 39) = 1,978.19, p < .001). As with our model-free results, we found that being exposed to the reciprocal altruism prompt significantly increased the odds of registering compared with the control condition (OR = 1.84, p < .001). After controlling for day of week and agent effects, we found two additional conditions to be significant. Compared with the control, the odds of registering were also significantly higher in the information condition (OR = 1.99, p < .001) and imagine self condition (OR = 1.81, p = .015). Follow-up pairwise Wald comparison tests under our main specification (i.e., agent and day-of-week fixed effects) show that these three interventions did not significantly differ from one another in their effectiveness (all ps > .699; for details, see Table W1–2 in the Web Appendix, columns “Info” and “RA”).
Pre- and postexperiment phases versus control
Although we did not observe a significant difference in the model-free results, after adding agent and day of week fixed effects, we find that registrations were significantly higher in the preexperiment acclimation phase (OR = 2.09, p = .002) compared with control. All other comparisons with our control condition remained nonsignificant.
During the preexperiment acclimation phase, attention was being drawn to organ donor registrations, service agents were exposed to our new form for the first time, and service agents were informed that organ donor registration rates were being tracked during this pilot period. Critically, for the interpretation of our subsequent experimental conditions, registration rates declined immediately afterward. Nevertheless, to test whether these specific process changes impacted registration rates, the following section presents a validity check that decomposes the different elements of our interventions. Moreover, we subsequently test additional controls to account for changes in agent’s behavior with a series of robustness checks.
Validity Check: Decomposing the Elements of our Interventions
Given the constraints of our government partners, we were limited in the number of experimental conditions we could run. As a result, we were unable to counterbalance and test each element of our interventions individually. It was for this reason that we created an experimental control condition: to serve as a clean benchmark against which we compared our interventions. However, a result of this approach is that compared with the center’s standard process, each of our interventions comprised a combination of multiple changes. For example, unlike the standard process, those in the information condition received additional time, a simplified form, and an information brochure (see Table 2). Our analysis formally separates the following seven elements: (1) the standard process, (2) the simplified form with agents aware of tracking, (3) additional time, (4) information brochure, (5) reciprocal altruism prompt, (6) imagine self prompt, and (7) imagine other prompt. We calculated the effect of each these elements using a fixed-effects logit model predicting the odds of registering (see Table 4).
Analysis of Organ Donor Registrations (Odds Ratios): Validity Check Decomposing the Elements of the Interventions.

*p < .05.
**p < .01.
***p < .001.
Notes: Our dependent variable is registration as organ donor (i.e., consent = 1, no consent = 0). SP = preexperiment standard process phase, RA = reciprocal altruism condition, IS = imagine self condition, IO = imagine other condition.
This analysis illustrates that the process changes initiated during the preexperiment acclimation phase (i.e., using the simplified form and making service agents aware of the fact that we were tracking registration rates) by themselves did not significantly increase an individual’s odds of registering in comparison to the standard process, nor did handing the materials out in advance to provide more time. However, as predicted, and in line with our previous results, we find that adding a reciprocal altruism prompt did significantly increase individuals’ odds of registering (OR = 1.870, p < .001). Similarly, providing an information brochure significantly increased individuals’ odds of registering (OR = 1.697, p = .012). Finally, the results presented in Table 4 show that changing from the reciprocal altruism prompt to the imagine self prompt had no significant impact on the odds of registering (OR = .833, p = .479), nor did changing from the imagine self to the imagine other prompt (OR = .814, p = .456).
Robustness Checks
In this subsection, we perform a series of robustness checks to confirm that our results are robust to alternative sets of controls, in particular a time trend, agent–day of week interactions, and the number of customers per agent (for the inclusion of type of transaction controls such as health card or driver’s license, see Web Appendix Table W1–4; for the use of different “baseline” conditions, see Web Appendix Table W1–5).
Time trend
We incorporated a linear time trend in column R1 of Table 3 to address a potential confound related to history and ensure our results were not being driven by seasonality or a change in agents’ behavior due to the experiment (Shadish, Cook, and Campbell 2002). Our results are robust to the inclusion of a time trend, and if anything, increased the estimated effect of the information and reciprocal altruism interventions. The estimated effect of imagine self also increased, but the effect was not significant due to a higher standard error.
Agent-day of week interaction
In column R2 of Table 3, we incorporated agent–day of week fixed effects to account for the possibility that certain agents may perform better on certain days of the week. Again, our results are robust to the addition of this control.
Customers per agent
Another potential confound is how busy the center was. Customers may have been more likely to register on days with longer wait times, as they would have more time to attend to the materials. Conversely, agents may be more likely to promote organ donation transactions when wait times are short. To account for this, we controlled for the ratio of the number of customers to the number of agents working on a given day in column R3 of Table 3. Our results remain robust to the addition of this control.
Follow-Up Laboratory and Crowdsourcing Platform Posttests
To provide support for our hypotheses and test possible alternative mechanisms, we conducted seven online posttests (five preregistered) with 3,376 North American participants. 7 The purpose of these experiments was to explore the process through which our interventions may have been operating. In all of the posttests, participants were randomly presented the actual materials of one of our experimental conditions (between-participants design), they were asked a series of questions aimed at measuring their reactions toward these stimuli, and our experimental control condition served as the point of comparison. To increase confidence in significant findings, we sought to replicate them across posttests. Next, we discuss the main results from our posttests (for an overview of measures and findings see Appendix W4).
Posttest 1: risk perceptions (N = 502, Amazon Mechanical Turk [MTurk] workers)
Posttest 1 examined whether our interventions may have affected perceptions of risk. It is possible that our materials focused participants on specific aspects of risk, such as the risk of not having a transplant available if needed, leading to self-interested motivations to act (Cialdini et al. 1987). Conversely, our interventions may have shifted participants’ focus away from the risks and onto the benefits of registering (Tversky and Kahneman 1981). We assessed the perceived risk of five factors: (1) needing a transplant in the future, (2) being able to get a transplant if needed, (3) encountering an organ donation shortage, (4) the medical system treating organ donors fairly, and (5) the medical system allocating organ donations efficiently. We found no evidence that our interventions significantly changed risk perceptions compared with control (all ps
Posttest 2: reciprocal altruism prompt mechanism (overall N = 767)
In posttest 2a (N = 403, MTurkers) and 2b (N = 364, Ontario students), we examined an important assumption of our reciprocal altruism prompt: that individuals envision themselves in a position where they are accepting help, which then increases their likelihood of reciprocating (see Trivers [1971]). Specifically, we hypothesized that the presence versus absence of the prompt “If you needed a transplant, would you have one?” would significantly increase registration intentions, both when participants were explicitly asked to answer the prompt or—as in our field experiment—when they were simply presented the prompt. However, individuals’ registration intentions—that is, their hypothetical registration likelihood (seven-point scale), consent decision (indicating “I would consent to help save lives by becoming an organ and tissue donor”), and exclusions decision (indicating “I would wish to donate any needed organs and tissue”)—were not significantly different from the control at the 5% level (all ps ≥ .091). In hindsight, these null effects are likely the result of the aforementioned organ donation intention–action gap that many countries, including Canada, observe. In support of this, we found extremely high registration likelihood ratings and consent rates even without the reciprocal altruism prompt (posttest 2a: Mcontrol = 5.55 and Mcontrol = 99.0%, respectively; posttest 2b: Mcontrol = 5.57 and Mcontrol = 96.6%, respectively). Finally, as a manipulation check, we explored whether people envisioned themselves accepting a transplant, if they needed one. Indeed, when forced to respond to the reciprocal altruism prompt, almost all participants answered with “yes” (posttest 2a: 92 of 99, posttest 2b: 87 of 88).
Posttests 3–7 (N = 2,107, MTurkers)
Posttests 3–7 aimed to examine a combination of (1) perceptions of the materials (e.g., educational, thought-provoking, focused on self vs. others); (2) the thoughts and feelings evoked from our interventions, including positive and negative emotions, feelings of sympathy, comfort registering; and (3) the extent to which our interventions affected participants’ general views on organ donation (i.e., the importance and norms of registering). Finally, we conducted an internal meta-analysis (McShane and Böckenholt 2017) focusing on each of the measures assessed in at least two posttests. Next, we present the reliable insights from this meta-analysis.
First, in terms of perceptions of our promotional materials, we found that indeed the brochure was viewed as significantly more educational (β = .84, 95% CI = ±.36; p < .001). In addition, it was seen as more emotionally positive (β = .67, 95% CI = ±.23; p < .001) and less emotionally negative (β = −.37, 95% CI ± .27; p = .008). These results are in line with our hypothesis that the information condition (brochure) would make additional information salient.
Second, in terms of thoughts and feelings, we found that our perspective-taking prompts evoked significantly stronger feelings of sympathy (in fact, all of our interventions, including the information condition, did so; βinfo = .63, 95% CI = ±.37; βRA = .52, 95% CI = ±.37; βIS = .60, 95% CI = ±.37; βIO = .76, 95% CI = ±.37; all ps ≤ .006). In addition, all but the reciprocal altruism intervention (p = .17) were viewed to be significantly more focused on others (βinfo = .44, 95% CI = ±.27; βIS = .53, 95% CI = ±.27; βIO = .55, 95% CI = ±.27; all ps ≤ .003; no difference for focus on self: all ps ≥ .10). These results support that our perspective-taking prompts in the field experiment likely evoked stronger altruistic motives.
In terms of alternative mechanisms, it is possible that our interventions may have stimulated new considerations (Wyer 2008), impacting registrations in our field experiment. For example, in our posttest meta-analysis we found that all of our interventions, except the imagine self prompt (p = .113), were rated as significantly more thought-provoking (βinfo = .45, 95% CI = ±.30; βRA = .34, 95% CI = ±.30; βIO = .43, 95% CI = ±.30; all ps ≤ .027). It is also possible that providing information caused individuals to feel more knowledgeable (Hart 1965), feel greater comfort with the decision to register (Parker, Lehmann, and Xie 2016), and feel more prepared to register (Tsai, Klayman, and Hastie 2008), positively affecting registration rates. However, in our meta-analysis, we found no evidence that our interventions influenced feeling knowledgeable (all ps ≥ .407), comfort registering (all ps ≥ .260), or preparedness (all ps ≥ .518). Finally, our interventions could have changed general perceptions of how important it is to donate (Batson 1987) or how much it is the right thing to do (norms; Fisher and Ackerman 1998), in turn increasing registrations in our field experiment. However, we found no evidence for such effects in our meta-analysis (all ps ≥ .300; for other nonsignificant measures that were explored, including feelings and perceptions of ethicality, see Table W4–3 in the Web Appendix).
Summary of Findings
The results of our field experiment support our prediction that marketing interventions grounded in behavioral science, targeting information and altruistic motives, would significantly increase new organ donor registrations in a prompted choice context. While our interventions did not significantly differ in effectiveness from one another in the majority our analyses, 8 our reciprocal altruism intervention (“If you needed a transplant, would you have one? If so, please help save lives and register today”) was the best performing. It led to the highest registration rates and was the only condition to significantly increase registrations compared with our control condition consistently across all analyses, including our model-free results. After including relevant controls (e.g., day-of-week and agent fixed effects), we found that our information and imagine self interventions also significantly increased registrations compared with control.
Our posttests provide some initial evidence for the mechanisms driving our interventions. As we predicted, all of our perspective-taking prompts induced greater feelings of sympathy compared with control (Batson et al. 1997), and our information condition was rated as more educational. Moreover, all of our perspective-taking prompts, except reciprocal altruism, were perceived to focus more on others. The posttests also suggested some additional mechanisms through which our interventions may have been operating. For example, our brochure was found to be more emotionally positive and less emotionally negative than the control. Previous research has shown that declarative information is especially effective at increasing organ donation attitudes when framed positively (Reinhart et al. 2007), which may have contributed to its success. The brochure also increased feelings of sympathy and focus on others, suggesting that it may have targeted altruistic motives as well (Batson 1987). All our interventions, aside from imagine self, were viewed to be more thought provoking than our control, suggesting that they may have changed what individuals were considering when deciding (Wyer 2008). Other mechanisms tested (e.g., risk perceptions, comfort registering, importance of donating, norms) were not supported. Although our posttests exposed participants to the actual materials used in our field experiment, it is critical to note that they were conducted outside the in-person, actual organ donor registration context (e.g., online MTurk and online university student samples) limiting our ability to draw conclusions about what occurred in our field experiment. Furthermore, previous research has shown that organ donation attitudes and intentions often do not translate into actual behavior (Morgan, Miller, and Arasaratnam 2002). For these reasons, it is important to exercise caution when drawing conclusions from these posttests.
General Discussion
This field experiment contributes to the literature by testing marketing interventions to increase new organ donor registrations within the prevalent explicit consent systems. Prior organ donation research has primarily focused on factors that influence intentions and attitudes (Ferguson, Murray, and O’Carroll 2019); however, the shortage of registered donors appears to be primarily a problem of inaction (Siegel et al. 2010). To date, a small number of studies have documented some positive impact on actual registrations from elaborate education programs and mass-media campaigns (Golding and Cropley 2017), yet they provide little insight into how to increase new registrations within explicit consent systems in an economical and scalable way. This research contributes to the limited empirical evidence for low-cost and scalable marketing solutions, targeting knowledge and altruistic motives, to overcome the intention–action gap and improve registrations within the current systems. Specifically, we find that in our best-performing condition, prompting perspective taking through reciprocal altruism (“If you needed a transplant, would you have one? If so, please help save lives and register today”) significantly increased registration rates from 4.1% in the control condition to 7.4%, an 80% increase.
Our work also contributes to our understanding of how to employ multiple elements of the marketing mix to help achieve the objectives of nonprofit organizations. Research on charitable giving has primarily focused on promotional strategies to solicit donations of time, money, and blood (e.g., Lacetera, Macis, and Slonim 2013; Sargeant and Woodliffe 2007). Recently however, Bradford and Boyd (2020) qualitatively examined how the entire marketing mix could be employed, more broadly, to encourage living organ donations. We expand on this research by empirically testing interventions to support the more common request to register as a deceased organ donor. We demonstrate that intercepting customers with promotional materials at the right time, along with streamlined customer service—additional time and a simplified form—significantly increased new organ donor registrations. Importantly for practitioners, this streamlined organ donation process ensured that every customer was exposed to the materials and had ample time to consider them and complete the form. It also reduced the burden on the individual service agents to prompt registrations and reduced agent-caused variation in registrations. We obtained preliminary evidence, based on a small postexperiment survey, suggesting that our process changes may have reduced the time it took for individuals to register. 9 Processing transactions faster would save ServiceOntario time and money and could also lead to happier customers, as they would have shorter wait times. Moreover, other research has found that giving individuals something to read while waiting can make the time go by faster and increase satisfaction (Katz, Larson, and Larson 1991). Therefore, these simple changes (i.e., reducing “sludge”; Thaler 2018) may help increase not only organ donor registrations but also the efficiency of the registration process as well as customer satisfaction.
This work also expands our understanding of how altruistic motives can be leveraged to increase prosocial behavior. While prior research has largely tested perspective taking in the lab (Ku, Wang, and Galinsky 2015), we demonstrate its effectiveness in the field. In addition, we replicate and extend the generalizability of using reciprocal altruism to improve organ donation behavior (Sallis, Harper, and Sanders 2018) by demonstrating its effectiveness at encouraging new and in-person registrations within the typical registration system and in a different national culture. We predicted that the reciprocal altruism prompt would be especially effective due to its combined focus on benefits for self and others (Landry 2006). While it did perform best, it is important to reiterate that our three perspective-taking prompts (reciprocal altruism, imagine self, and imagine other) did not significantly differ in effectiveness from each other across the majority of our analyses. The fact that all of our prompts improved registrations, albeit to varying degrees and not consistently significantly different from control, suggests that each of these different forms of perspective taking might be viable solutions for motivating organ donor registrations, though it would be important to test variations of their conceptualization in the field.
Our results highlight the importance of carefully considering the process and timing of delivering promotional materials. For example, the fact that our information condition was successful (after controlling for day of the week and agent) is noteworthy because the brochure that we provided was the standard one that was both readily available in self-serve stands at ServiceOntario centers (throughout the experiment) and was mailed with all drivers’ license renewal notices along with a standard registration form. Therefore, it is important for managers to intercept customers at the right point in time.
For practitioners, our results highlight the critical importance of testing interventions in the field and measuring their realized impact. For one, individuals in our pretest (Web Appendix W2) did not accurately predict the relative effectiveness of our interventions. Moreover, it would have been reasonable to predict that merely providing individuals with a simplified form along with additional time to decide would increase donor registrations (i.e., our control condition; Behavioural Insights Team 2014), but our results revealed otherwise. Finally, in a recent meta-analysis, DellaVigna and Linos (2020) suggested that nudge interventions tested in academic research tend to have a significantly larger effect than those tested “at scale” by government “nudge units.” While our field experiment is similar to that of academic research in terms of sample size and effect size, many other features of our experiment suggest it is similar to research of nudge units: we tested elements of simplification, had relatively representative sampling, and our findings were released to the general public by our government partners, irrespective of the results. Together, these observations highlight the importance for researchers and policy makers to consider issues such as statistical power, selection effects, and characteristics of the interventions when planning at-scale implementations of interventions from academic research.
Limitations and Opportunities for Future Research
Although this experiment provides us with low-cost, scalable marketing solutions to increase actual organ donor registrations, we were unable to test the mechanisms driving our interventions and did not have the opportunity to replicate the study over a longer period or at a larger scale. For example, to maintain customers’ privacy, we could not survey the individuals who came to the center or collect any personal information about them, and therefore, it was not feasible to administer manipulation checks or process measures. While our posttests provided some initial process evidence, they can only be considered as indicative, at most, because they were conducted outside the in-person registration context (e.g., online student samples, MTurk workers), and measured feelings, thoughts, and intentions, which do not always map onto behavior (Radecki and Jaccard 1999). Future research should systematically examine the underlying mechanisms driving interventions within field settings to facilitate generalizations.
In addition, due to timing and design constraints we were unable to counterbalance each component of our interventions with a fully-crossed and randomized design. Although we estimated the unique impact of the elements of our interventions, future research could experimentally manipulate each to explore whether they had additive or interactive effects. For example, it may be worthwhile to formally test how information and perspective-taking work in combination with one another, as they may be more effective together than either condition alone.
Finally, another area for future research would be to examine the role that customer service agents play in encouraging organ donor registrations. First, our data revealed significant effects of agents on registrations. Second, registrations in the preexperiment acclimation phase (a hybrid between the center’s standard process and our subsequently introduced experimental process) were significantly higher than the preexperiment standard process phase and, after including day-of-week and agent fixed effects, also higher than our experimental control condition. In the preexperiment acclimation phase, service agents encountered our new simplified form for the first time and received formal communication from their manager drawing attention to the organ donation task and making them aware that registrations would be tracked. These factors may have led to excitement or changes in agents’ behavior that in turn led to increased registrations. In all of our experimental conditions, we took care to limit any variation in registrations caused by the service agents by handing the form out in advance (i.e., when individuals arrived at the registration desk). However, these findings suggest that maximizing agent effectiveness could be another interesting avenue for future research aiming to increase organ donation rates.
Conclusion and Policy Recommendations
With thousands currently on the transplant waiting list, the need for organ donors is urgent, and as the population ages, the demand is only predicted to increase further. One way to address the ever-growing demand is to increase the number of individuals registered as donors within the prevalent explicit consent systems, in which low registration rates are especially common. In our field experiment we were able to increase new in-person registrations in a prompted choice context using easy-to-scale, low-cost 10 promotion interventions supported by process improvements. We were able to do so without imposing on individuals’ freedom, raising ethical concerns (i.e., changing defaults), or passing new legislation. To illustrate the potential impact of our findings, if we were to assume that everything held constant over time and we introduced our best-performing intervention (reciprocal altruism) throughout Ontario, we could expect roughly 225,000 additional new registrations annually. While quantifying the effect of increased registrations on the ultimate goal—lives saved or enhanced—is challenging (see, e.g., DeRoos et al. 2019), research has shown that those who register their consent are significantly more likely to actually donate than those who have not (Christmas et al. 2008). Specifically, the majority of registered individuals in Ontario who become eligible to donate are ultimately converted to donors (Toews and Caulfield 2016), and Ontario’s Trillium Gift of Life Network (2020) advertises that one single donor may save up to eight lives and enhance as many as 75 more lives.
Compared with the center’s standard registration process, all of our interventions significantly increased organ donor registration rates (see Table W1–1 and W1–2 in the Web Appendix). We recommended Ontario implement our reciprocal altruism intervention and track its performance for three reasons: (1) this intervention was successful in increasing registrations in both the United Kingdom (Sallis, Harper, and Sanders 2018) and our field study, (2) it significantly increased registrations compared with the control across all our analyses, and (3) it avoids the costs associated with printing additional brochures. In 2016, the Ontario government adopted our recommendation partially by introducing a somewhat simpler organ donor registration form with the reciprocal altruism prompt province-wide (compare Figure W1–7 with Figure W1–4 in the Web Appendix). For policy makers who want to use our insights to improve organ donor registrations in a similar context, we recommend implementing as many of the design elements of our marketing materials as possible (e.g., colored banner on cardstock), along with implementing the supporting process changes (e.g., simplified form, intercepting customers at the right time, providing time to attend to the materials). Together, we believe this research not only informs our understanding of how marketing can be leveraged to improve nonprofits' goals but also offers insights that could benefit society by increasing organ donor registrations.
Supplemental Material
Supplemental Material, sj-pdf-1-jmx-10.1177_0022242921990070 - Increasing Organ Donor Registrations with Behavioral Interventions: A Field Experiment
Supplemental Material, sj-pdf-1-jmx-10.1177_0022242921990070 for Increasing Organ Donor Registrations with Behavioral Interventions: A Field Experiment by Nicole Robitaille, Nina Mazar, Claire I. Tsai, Avery M. Haviv and Elizabeth Hardy in Journal of Marketing
Footnotes
Acknowledgments
The authors thank the Ontario Ministry of Health and Long Term Care, Trillium Gift of Life Network, ServiceOntario, and Ontario Treasury Board Secretariat’s Behavioural Insights Unit for the collaboration; the Behavioural Economics in Action at Rotman (BEAR) center (in particular, Dilip Soman and Min Zhao) for support; their research assistants Donella Plastik, Aybike Mutluoglu, and Joel Mohr; and Mathieu Marcoux and Avi Goldfarb for data analysis advice.
Author Contributions
Conceived experiments: NR NM CT EH. Designed experiments: NR NM CT EH. Directed experiments: NR NM CT EH. Data analysis: NR NM CT AH. Interpreted the results: NR NM CT AH. Wrote the first draft: NR. Edited the manuscript: NR NM CT AH.
Associate Editor
Robert Meyer
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: At the time of the field experiment, Nicole Robitaille was employed as behavioral scientist at the Behavioural Insights Unit (BIU), Government of Ontario, and Elizabeth Hardy was the BIU’s manager. Nina Mazar and Claire Tsai were uncompensated academic advisors with the BIU.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a DI McLeod Grant from the Smith School of Business, Queen’s University awarded to NR, a TD Bank Group Research Fund awarded to BEAR at the Rotman School of Management, University of Toronto, that NM codirected at the time of the research, and a SSHRC Insight Grant awarded to CT.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.