
Abstract
Keywords
Introduction
The use of team formulations with staff groups has become an increasingly popular practice within Clinical Psychology in the United Kingdom as a means to engage and work collaboratively with teams (Division of Clinical Psychology [DCP], 2011). The use of idiosyncratic psychological formulations in one-to-one therapeutic work are mainstream practice within the United Kingdom and are guided by the Good Practice Guidelines published by the British Psychological Society (DCP, 2011). Psychologically working with teams (such as facilitating team formulations and providing consultation) is also considered a fundamental role of practitioner psychologists by regulatory bodies (Health and Care Professions Council, 2015). The frequency of team formulations has increased in recent years reflecting the rising prominence of team-based psychological work by clinical psychologists (Johnstone, 2018), the current pressurized U.K. National Health Service (NHS) context in which more is expected with fewer resources (Alderwick et al., 2015) and the growing demand for psychotherapeutically informed approaches to mental health (Department of Health, 2007).
Team formulations can be characterized as the “process of facilitating a group of professionals to construct a shared understanding of a service user’s difficulties” (Johnstone & Dallos, 2013, p. 5) and are often facilitated by a psychologist. These formulations are then often used to explain the development, maintenance of presenting difficulties, and to guide the planning process of future interventions (Geach et al., 2018). A systematic review completed by Geach et al. (2018) found that although no uniform definition was reported across studies a common focus was established as being a forum to share psychological understanding of an individual’s presenting difficulties while guiding interventions. Team formulations have also been found to be helpful in working with complex individuals, particularly when considering the support given to staff (DCP, 2011; Royal College of Psychiatrists, 2017). In addition, team formulation was generally seen to be an umbrella term inclusive of formulation activities which reached multiple people in a short space of time and is reported to be unique to clinical psychology (DCP, 2011; Geach et al., 2018).
Quantitative studies have found that team formulations have improved staff perception of formulation as a useful practice (Geach et al., 2018; Whitton et al., 2016). Throughout the present article and the literature staff usually refers to professional individuals who directly clinically engage service users in therapeutic supportive work. Qualitative studies collecting professional views and opinions of team formulations have uncovered mixed findings. It has also been highlighted that the qualitative findings have potentially been affected by the individual analyzing the data. Research by Summers (2006) highlighted that views on team formulation differed according to the profession of the individual being interviewed; clinical psychologists provided positive and valuing accounts of team formulation and inpatient nursing staff expressed dissatisfaction regarding the meetings with “some people wanting to be right or more powerful” (p. 342). A theme of increased empathy was evident across multiple qualitative studies. Murphy et al. (2013) reported how one individual identified seeing service users more as “people” and less as “patients.”
The DCP (2011) have highlighted a sparsity of evidence related to the influences of team formulations despite noting several benefits and research that has suggested that staff find team formulations useful (Ingham, 2011; Wainwright & Bergin, 2010). Staff views on formulation are important to investigate as they are the primary group using and engaging with team formulations. Although quantitative studies have found potentially positive impacts of team formulation, what the research field is currently lacking is context around “why” team formulations are seemingly having this positive impact.
Aims and Objectives
This review aims to analyze U.K.-based qualitative studies on staff experiences of participating in team formulations using Thomas and Harden’s (2008) method of Thematic Synthesis. The review also aims to provide a thorough quality appraisal of the research which meet inclusion criteria.
The review focused on the following questions: What are mental health staff experiences of participating in service user focused team formulations? What benefits do mental health staff perceive from participating in service user focused team formulations? What is the current quality of qualitative research examining mental health staff experiences of participating in service user focused team formulations?
Method
Systematic Search and Eligibility Criteria
Identification
Nine electronic bibliographic databases covering pertinent topic areas were searched on November 12th, 2019: AMED, British Library ETHOS, CINAHL, Director of Open Access Journals, MEDLINE, PsycINFO, PsycARTICLES, Scopus, and Social Sciences Citation Index. Reference lists of accepted articles were also screened.
Search terms were developed by searching currently published articles and assimilating keywords. Search terms were tested and refined through scoping searches within the selected databases. The search was also limited to studies that took place in the United Kingdom. The search strategy was as follows: (psychological formul* OR case conceptuali* OR case formulat* OR formulat*) AND (staff or nurs* or health care professional or psychiatrist or psychologist) AND (mental health or psychiatric setting). The search criteria applied to titles and abstracts only. A separate hand search was conducted through the online back catalogues of the British Psychological Society’s DCP Clinical Psychology Forum publication. The Clinical Psychology Forum was included as it serves as the main professional forum for issues of relevance to clinical psychologists.
Inclusion criteria required the articles to be primary research with a qualitative component gathering data on staff views and experiences regarding the process of team psychological formulations. Within studies that focused more on case conceptualization, the main focus of the discussions of the group had to be focused on specific service users and not the formulation of the team. Dissertations, doctoral theses, and nonpeer reviewed reports, found through the search strategy, were also included to reduce potential for publication bias. Studies which focused on collecting psychologists’ views and opinions were included as it was felt they would provide a unique insight into the processes of team formulation.
Screening
Figure 1 summarizes the screening process in a PRISMA Flow Diagram. A total of 2,729 titles were screened and considered against the eligibility criteria described above. Following title screening, 89 papers were screened by their abstract and 31 articles were selected for full text screening. A further 35 articles were identified for screening from the Clinical Psychology Forum hand search and of these 22 articles were retained for a full text screening. In total, 53 articles were screened at the full text stage (31 from the title screening and 22 from the Clinical Psychology Forum hand search).
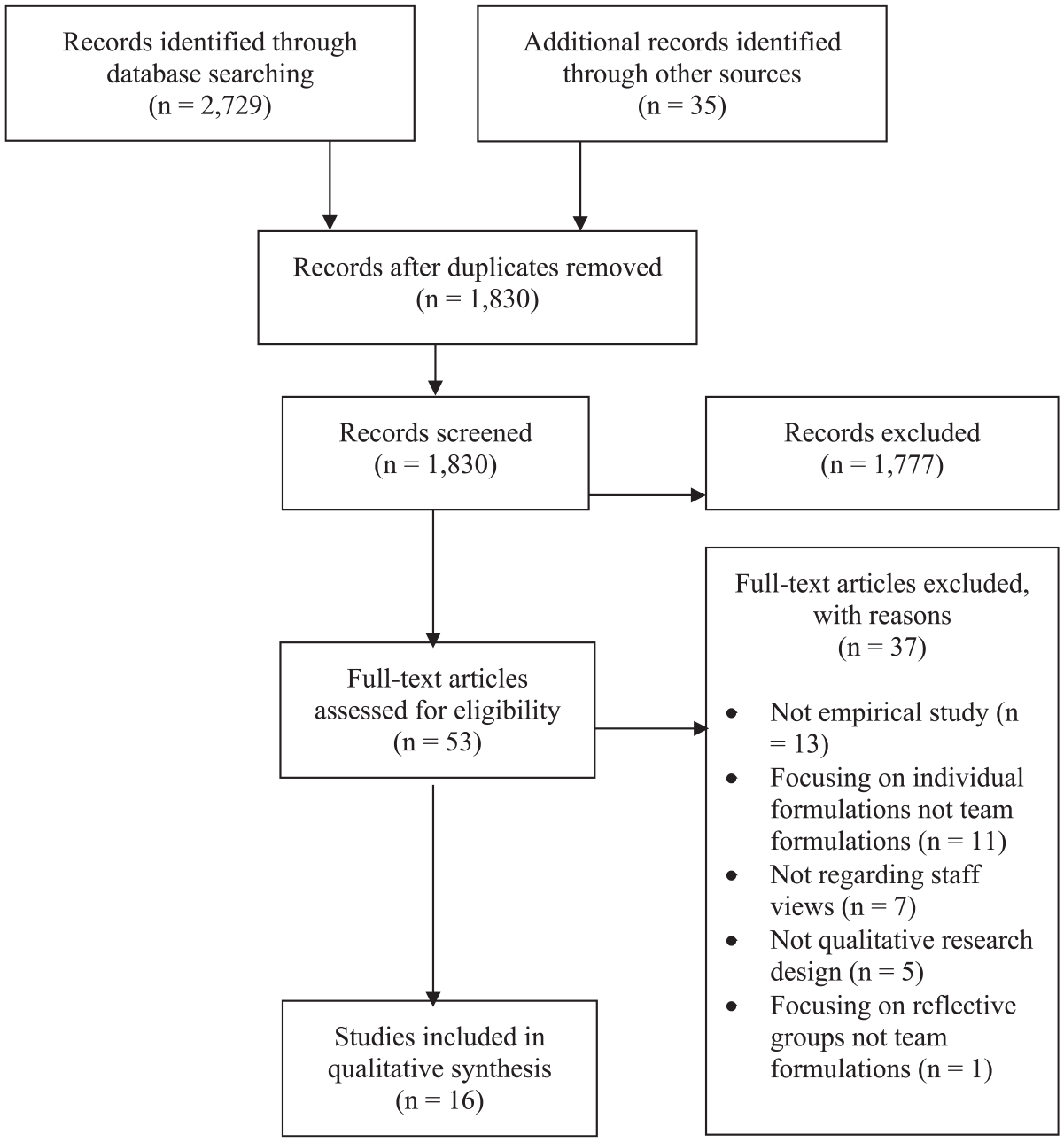
PRISMA flow diagram.
Eligibility
The full text of 53 articles were sought for review, of these 13 were excluded due to not being empirical papers. A further five were excluded as they did not contain a formal qualitative analytic component. A final 19 studies were excluded due to their focus being on either formulations by individuals, reflective groups or not encompassing staff views into their study.
Data Quality Assessment
The Critical Appraisal Skills Programme (CASP; 2017) checklist for qualitative research was employed. The CASP checklist covers three broad issues, across 10 questions, for appraising qualitative research; are the results of the study valid, what are the results, and will the results help locally. The CASP checklist was used as a framework to not discredit studies that, although may have scored lowly on some items, make a valuable contribution to the field (Sandelowski & Barroso, 2002). Each item on the CASP scale was rated as either “yes,” “partial,” “no” or “unclear,” and was graphically represented using an adapted Cochrane traffic light scheme (Voss & Rehfuess, 2012). Two random articles of the 16 (representing 10% of the articles included) were double rated by a second investigator to ensure accuracy of appraisal. Uncertainties were resolved during discussion and a third investigator was available if necessary. All studies were retained for synthesis, no matter their rating, due to the inherent difficulties in accurately assessing qualitative studies (Dixon-Woods et al., 2004), particularly when considering publication pressures and structures (Walsh & Downe, 2006). The quality of the studies will be considered in the analysis.
Procedure of Thematic Synthesis
Thomas and Harden’s (2008) Thematic Synthesis method was used to combine the findings. A Thematic Synthesis approach is deemed appropriate when bringing together a large set of qualitative studies (Tong et al., 2012; van Leeuwen et al., 2019). The identification of important and recurring themes between studies is the main aim of Thematic Synthesis, while not negating the importance of subjectivity in the nature of participants experience (Barnett-Page & Thomas, 2009; Centre for Reviews and Dissemination, 2008).
Data were extracted from the studies through transfer of the results sections of the papers into QSR’s (2018) NVivo v12 software. The results sections were then reviewed and data that was not explicitly related to staff views was excluded.
The Thematic Synthesis took a three-step approach. Initially, each line was coded individually according to its context and meaning. These codes were then grouped together to form higher order codes and developed into descriptive themes through looking at similarities and differences between the codes. These themes were named taking into consideration the meaning of the groups of codes. Finally, an inductive thematic analysis was carried out to create analytic themes using the descriptive themes to answer the review question. To ensure context and rigor was maintained throughout the synthesis, detailed records were maintained through the use of NVivo software. These detailed electronic records enabled researchers to clearly see the process by which themes were developed and how the themes were represented across the papers (Soilemezi & Linceviciute, 2018; Thomas & Harden, 2008). To ensure clarity, the steps described above were closely followed and the focus remained on the review questions and context of the research (Soilemezi & Linceviciute, 2018).
Results
Quality Appraisal
From the quality appraisal, nine of the studies were rated highly, four rated moderately, and three rated poorly. Table 1 outlines the study authors, title, data analysis approach, and quality appraisal. In total, across the studies approximately 178 staff participants were included, while a further 89 case consultation reports of team formulation meetings were analyzed from Walton (2011). This number excludes any participants from Beardmore (2016) as this study did not include the total number of participants or any means of estimation. The professions included in these studies were: mental health nurses, psychologists, occupational therapists, recovery workers, support workers, social workers, team leaders, specialist registrars, residential staff members, and an activities coordinator. Studies rarely signposted where the meetings themselves took place, but there was an eclectic mix of both community and inpatient settings.
Summary of Quality Appraisal for Studies.
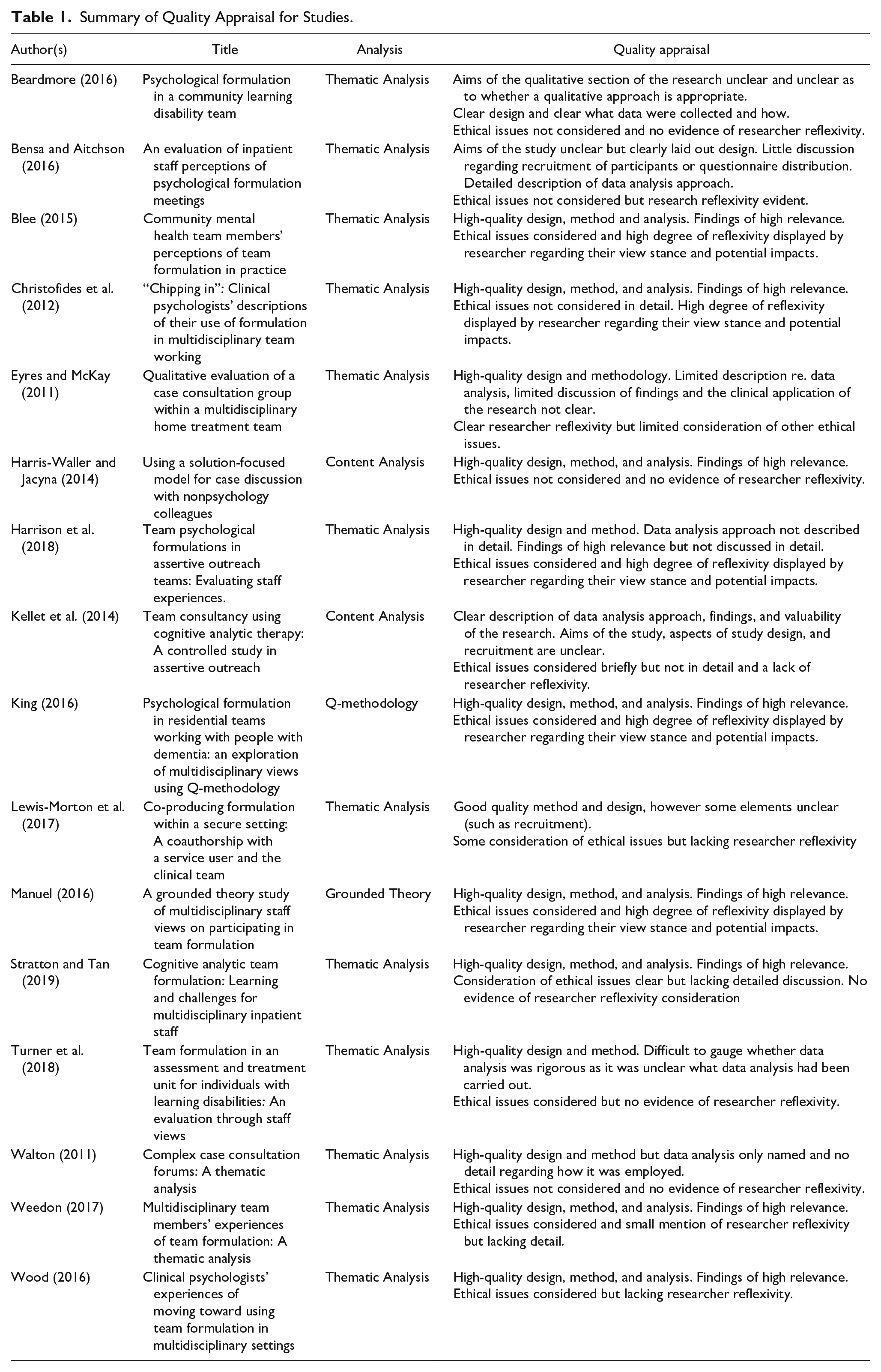
The criteria most frequently not met was evidence of consideration of the relationship between the researcher and the participants. At times it was unclear who conducted the data collection or the researcher’s epistemological stance was referenced but without clarity as to how this may have affected the findings. Within three studies it was clear that the researchers were actively known to the participants and the impact of this was not considered. In comparison with other ethical limitations, the absence of researcher reflexivity feels particularly important in research of this kind as the collection of staff views has the potential to be selective in terms of how open and honest participants feel they can be. Studies were typically good at communicating the value and contribution of their research to clinical practice and the research field.
Three of the four studies taken from the British Psychological Society’s DCP Clinical Psychology Forum were rated poorly. However, this publication also has the lowest word count limits potentially meaning relevant quality indicators could not be sufficiently described within this limit. The quality of all papers was considered during the development of themes in the Thematic Synthesis.
Thematic Synthesis
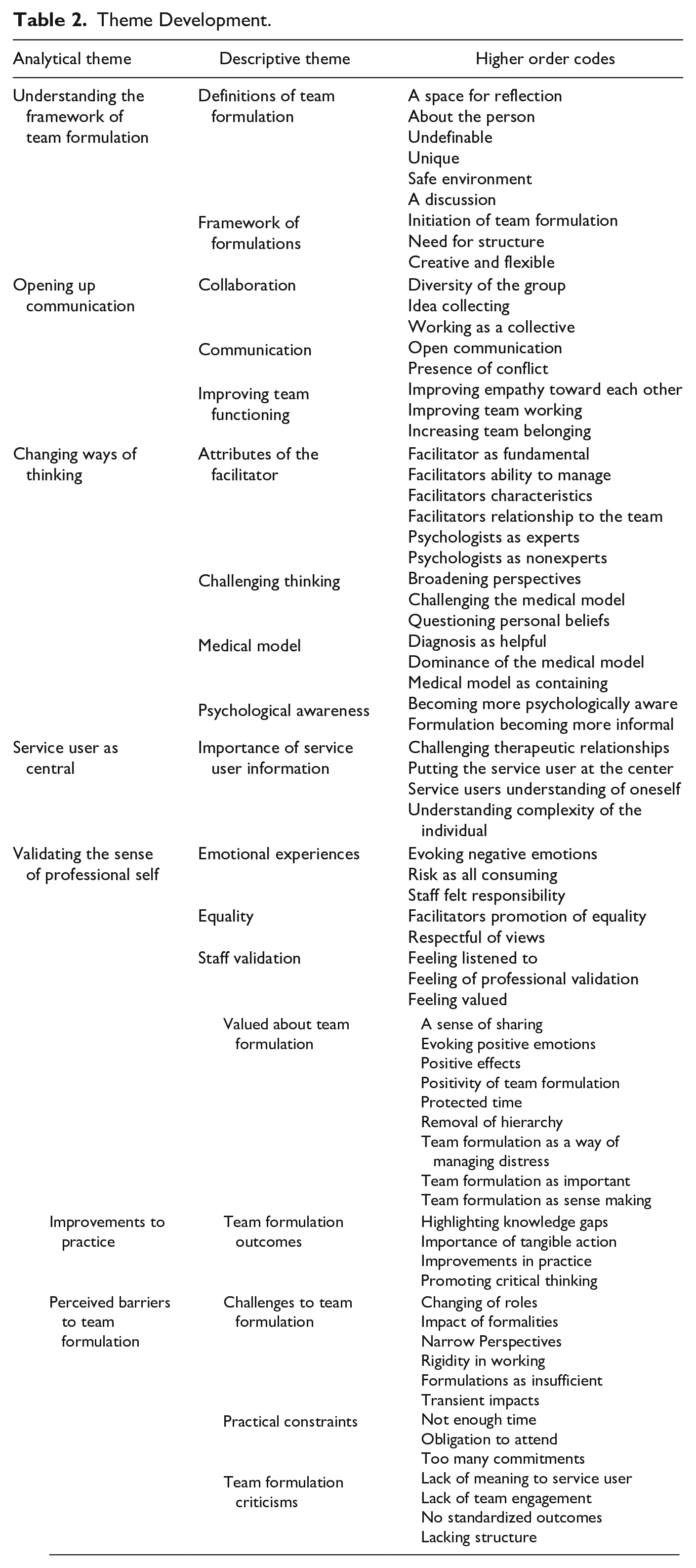
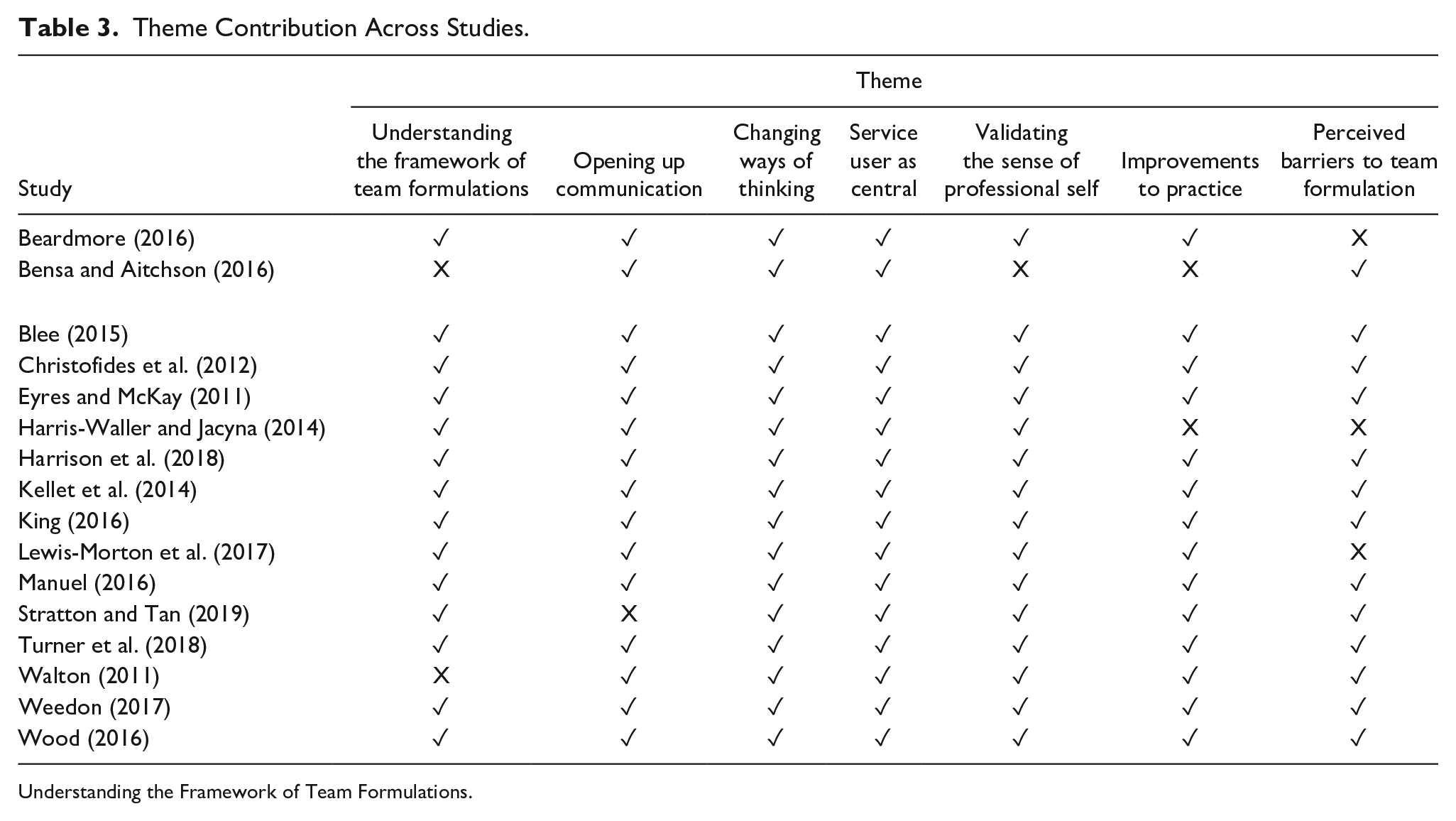
Seven analytical themes were identified in the data: (a) understanding the framework of team formulations, (b) opening up communication, (c) changing ways of thinking, (d) service user as central, (e) validating the sense of professional self, (f) improvements to practice, and (g) perceived barriers to team formulation. See Table 2 for outline of all the themes and how they developed from the data. Ten papers contributed to all seven themes; Table 3 provides the details for which papers contributed to each individual theme.
Theme Development.
Theme Contribution Across Studies.
Understanding the Framework of Team Formulations.
Definitions of team formulation
Staff members defined and described the framework of team formulations in multiple ways seeming to struggle to find a common understanding. Most participants seemed clear that a team formulation was different to other meetings (this theme was relevant to 12 of the papers analyzed), with many participants describing the formulations as a “space to think” (Christofides et al., 2012, p. 429) or an “informal discussion” (Manuel, 2016, p. 82). However, some participants descriptions of the process were ambiguous, describing team formulation as an “experience” (Manuel, 2016, p. 91), and as being “distinctly separate from other multi-professional meetings” (Manuel, 2016, p. 86).
Framework of formulations
Participants were also ambiguous when describing the structure of the formulation meeting themselves. Participants cited a space in which to reflect on cases as a main function of a team formulation, while others felt the purpose of team formulation was to promote an environment of safety in which “staff felt safe to float ideas” (Manuel, 2016, p. 77). Participants communicated about an environment in which formulations are viewed as enabling a “sense of safety” (Weedon, 2017, p. 172). Within Kellet et al.’s (2014) study many of the staff felt that it had “provided a time to reflect on practice and so helped the team to share experiences” (p. 694).
Opening up Communication
Collaboration
Staff highlighted the importance of a whole team presence in contributing and generating ideas within formulation meetings. The diversity of the group appeared to be a significant factor in the success of a team formulation and the widening of the discussion. The theme of diversity and perspective sharing was widely present across the included papers, being in a total of eight of the studies. One member of staff highlighted the usefulness of having a wide variety of professionals “who actually know the person” citing that this results in “good discussions when you feel like everyone is contributing” (Harrison et al., 2018, p. 78).
Communication
Staff members also referenced an improved communication between themselves but also of knowledge sharing between individuals. Staff commented on how the groups have widened their understanding of other professions: “helped me to realize that each profession brings their own expertise to the table” (Beardmore, 2016, p. 31). Several other professionals also commented on how team formulations had led them to understand the importance of learning from others, staff likening it to seeing “different angles,” “different strands” of service users (Weedon, 2017, p. 169), and the “widening instead of sort of narrowing in your discipline” (Weedon, 2017, p. 169).
Improving team functioning
The sense of working as a collective also appeared to improve team working in general. There was a sense across the research that participation in team formulations seemed to increase professionals’ empathy toward each other, as well as increasing their sense of belonging. Participants cited having a developed understanding of “what’s going off with each other” (Kellet et al., 2014, p. 695) and being able to share the emotional impact of the work as important outcomes. Staff generally felt that there was an improvement in team cohesion reducing a sense of isolation. One member of staff felt that it had helped to humanize other professionals in the team more: “we look at each other more I think, whereas before people just had their caseload and someone was just a name on the list” (Kellet et al., 2014, p. 695).
Changing Ways of Thinking
Attributes of the facilitator
Staff also attributed success of the team formulation to the role of the facilitator. Staff described the role of the facilitator being important to create an appropriate environment for the meetings as well as being assumed to have specialist knowledge. A large number of staff also felt that the facilitator needed to be a psychologist, due to the assumed attributes of their profession such as being nonjudgmental and “experts” (King, 2016, p. 79). One participant was quoted as saying it “makes me feel more comfortable knowing that a psychologist is in charge of it” (Manuel, 2016, p. 74).
Staff members views on the directedness of the facilitator did vary. Staff members’ views on the role of the facilitator were divergent with some believing the facilitator to be there to “teach clear-cut strategies” (Eyres & McKay, 2011, p. 28), while others believed the facilitator should have a more indirect role.
Challenging thinking
As a result of team formulations, professionals often cited a change in their usual way of thinking about service users. Staff views were that they had a broader understanding of service users and their difficulties as a result of team formulations. Some members of staff attributed a shift in their thinking to an “understanding of the service user better” (Blee, 2015, p. 104) or having a broader understanding of the service users’ difficulties (Christofides et al., 2012).
Medical model
Team formulations were highlighted as being a direct challenge to the typical medical model of some mental health teams, within three of the included papers. One member of staff in particular highlighted the difference between formulations and the “very definite” medical model as potentially being the “fly in the ointment” of the use of team formulations (Manuel, 2016, p. 88).
On the other hand, within Weedon’s (2017) research, a small minority of participants, did discuss the ability for diagnosis and formulations to go “alongside each other” (p. 166). Describing diagnosis as being important for “medication” and formulations being “one step deeper” (p. 166)
Psychological awareness
Team formulations also appeared to increase psychological awareness amongst staff with individuals actively advocating for more psychologically informed approaches. At times professionals described an increase in their psychological awareness, with one member of staff describing it as “like everyone’s a psychologist in the team now” (Eyres & McKay, 2011, p. 28).
Service User as Central
Importance of service user information
Team formulations were seen as a way of providing focused attention on individual service users and staff commented that it enabled them to retain focus on what is best for the service user. Staff highlighted this as being particularly unique to team formulations as they often lacked the space to dedicate isolated time to an individual service user. Developing an understanding of the complexity of an individual and providing consideration of an individual’s past history were deemed important within a team formulation meeting. Five of the studies focused on staff preference to discuss service users in team formulations whom the team were struggling to forge strong therapeutic relationships.
Staff commented that “gaining a greater understanding of a client’s background” (Bensa & Aitchson, 2016, p. 36) often helped consider possible past traumatic events or childhood events rather than overlooking them in favor of information supporting the diagnosis (Manuel, 2016). One staff member commented on the importance of “remembering as well where they come from, what are their triggers . . . how much they have suffered” (Stratton & Tan, 2019, p. 91).
One professional believed that through developing a deeper understanding of a service user they could establish a stronger relationship: “one step deeper, which is what’s needed to be able to get to know people a little bit better and develop that relationship with them” (Weedon, 2017, p. 166). Discussions appeared to often center on helping the staff member feel less “stuck” (Blee, 2015, p. 102) and developing ways in which to connect to the service user.
Validating the Sense of Professional Self
Emotional experiences
In 12 of the studies, negative emotions were frequently referred to by staff in association with team formulations, particularly when related to risk or risk management. Individuals across the papers referenced feeling that the process was “intensive” (Wood, 2016, p. 24) and “frustrating” (Eyres & McKay, 2011, p. 28). Some staff believed that other professionals lacked the confidence to openly voice their opinions during team formulations: “I think a lot of people probably hold back and that could possibly . . . lessen the effectiveness I suppose” (Stratton & Tan, 2019, p. 91). However, some staff felt that formulations had been positive in stopping staff feeling “governed by the seriousness and nature of the risks and behaviors” (Lewis-Morton et al., 2017, p. 233).
Equality
Staff referenced feeling equal to other professionals in the team within team formulations, regardless of their specific role. Across nine of the studies participants expressed positive feelings of being professionally validated during the team formulation meetings and staff empowerment was recorded by participants across four of the studies. The importance of feeling equal in the meetings despite their role in the team also came across: “the equalness of everybody in that’s in the situation regardless of your role or whatever. You go in there as equals, that sense of equalness” (Manuel, 2016, p. 79).
However, for some participants, this was a negative experience of team formulations and led to them feeling “frustrated” when individuals were voicing opinions as if in a “talk shop” without the aim to make direct changes to a service users care (Weedon, 2017, p. 171).
Staff validation
Team formulations appeared to help validate staff professionalism, in addition to aiding staff to feel listened to. Some of the participants believed that previous unsuccessful attempts at working with service users had led to professionals feeling “disenfranchised” resulting in the need for staff to be “empowered” to take part in the revised interventions (King, 2016, p. 76). One participant stated, “it’s given people more confidence that what they’re doing is right” (Manuel, 2016, p. 98).
Improvements to Practice
Team formulation outcomes
The importance of team formulations generating tangible outcomes was referenced across 13 of the studies. Some of the perceived outcomes from team formulations were care plans, improvements in clinical practice and a written formulation report.
In one study, team formulations were intrinsically linked to the production of individual service user care plans. Within Blee (2015), all 12 participant transcripts reported care plans to be integral to a team formulation by providing a clear direction for the therapeutic work and aiding staff to feel less stuck. In other studies, team formulation was utilized as a method to “provide more accurate care plans” (Beardmore, 2016, p. 31) or “collectively decid[ing] a way forward” (Eyres & McKay, 2011, p. 27). Team formulations appeared to be viewed more positively when associated with clear cut goals and outcomes: “it has made visits more purposeful as I am achieving quite a few objectives” (Kellet et al., 2014, p. 694).
Staff also generally spoke about team formulations improving their clinical practice overall. For example, one participant explains, “it has influenced my practice, not only for my clients but for the other clients in the team that I didn’t even know about” (Kellet et al., 2014, p. 695). Some participants believed that participating in team formulations had developed their compassion toward others or created a “consistent approach” (Turner et al., 2018). Professionals believed that some of this change in practice came from adopting a more critical stance to their work: “when she asks you something about your work so far you are thinking, ‘well am I missing something? Is this very subjective? How objective am I being here?’ And that all helps” (Manuel, 2016, p. 75).
Perceived Barriers to Team Formulations
Throughout this review staff highlighted several barriers to the utilization of team formulations.
Challenges to team formulation
Across 13 of the studies, staff cited challenges to the process of the team formulation, such as other staff’s views and opinions or difficulties with the hierarchy through the meeting. Staff felt that teams were at times “set in their ways” (Christofides et al., 2012, p. 431) or that certain staff held quite “fixed beliefs” (Wood, 2016, p. 28). The fixed viewpoint of some members of staff left others unwilling to contribute for fears that they were the minority viewpoint.
Practical constraints
Across six of the studies, time was referenced as a significant barrier to professionals attending team formulation meetings. Other potential barriers to team formulations appeared to be more related to staff personal views and opinions. Staff members discussed how it was difficult to ensure “protect[ed] time” (Bensa & Aitchson, 2016, p. 36) which resulted in the “timing of meetings” (Turner et al., 2018, p. 280) being unhelpful and staff feeling that there was “too much to discuss” (Turner et al., 2018, p. 281). Some staff cited the barrier to ensuring there was protected time for meetings as being trying to “negotiate” (Wood, 2016, p. 24) a time when the whole team was available with many seeing it as a major “drawback” (Harrison et al., 2018, p. 79).
Staff also referenced the competing demands of working in mental health services leaving them with little time or space to participate in team formulations: “some of the people that really need to go to case formulation . . . who are working with the women face to face don’t often get the opportunity” (Stratton & Tan, 2019, p. 91). These practical constraints are important to note, however, on some occasions these will be team and context specific.
Team formulation criticisms
Staff also levelled criticisms at the idea of team formulations in general. Many staff cited team formulations as potentially “vague” or “wishy-washy” (Christofides et al., 2012, p. 430) leaving staff feeling that the meetings were pointless or lacked action-orientated outcomes.
Discussion
The review found that nine of the studies rated highly, four rated moderately, and three rated poorly on quality appraisal. Sandelowski and Barroso’s (2002) approach was utilized to include papers of a poor quality, when corroborated with other studies as they still make a valuable contribution to the field. Therefore the three papers that were considered to be poor in quality (Bensa & Aitchson, 2016; Eyres & McKay, 2011; Walton, 2011) were still included in the development of themes. The criteria that was least frequently met was the inclusion of researcher reflexivity. Reflexivity was particularly important in the current review due to the presence of inherent “power” dynamics and hierarchy in community mental health teams requiring the researcher to reflect on how they may be contributing or affecting these dynamics (Currie et al., 2012; Singh, 2000).
The variety of types of papers that have been included in the current review should also be considered. Nine of the included studies were taken from grey literature and five of these were doctoral theses. Grey literature constitutes unpublished pieces of work which are produced by academia, government, business, or industry but are not controlled by commercial publishers (Bellefontaine & Lee, 2013). Although themes were balanced across all of the included papers, the length of the doctoral theses in comparison to a generic published study may have resulted in certain themes containing a larger collection of data than other themes. The other four studies were taken from DCP publications and were therefore shorter in length than other publications. Grey literature is an important contribution to systematic reviews and helps provide balanced viewpoints without publication bias (Paez, 2017). However, the reasons why the vast majority of the studies included in the current review are located within grey literature should be considered. Six of the seven published papers were evaluations of service developments related to team formulations whereas the five doctoral theses related to the collection of general staff views and opinions. It may be that grey literature reflects the gap between science and practice that has previously been highlighted in clinical psychology (Grol & Grimshaw, 2003). Direct service evaluations of tangible projects are potentially seen as more directly practical and replicable within individuals own services (and therefore more publishable) as opposed to overall staff viewpoints which may be viewed as nebulous.
The present review demonstrated how participating in formulations could potentially aid staff to humanize, develop their compassion toward service users, and place the service user at the center. Previous research, such as that by Murphy et al. (2013), has also found that formulation helps individuals to see service users as “people” and less as “patients.” The idea of seeing an individual as a whole and as a person rather than just their difficulties has its roots in person-centered care (Naldemirci et al., 2018). Research has begun to highlight the importance of and the positive impact that this can have to individuals with mental health difficulties (Lindström et al., 2019; Staniszewska et al., 2019).
In addition to the positive impacts on service users, the review found that staff felt listened to and that formulation provided a time for reflection and being heard, findings echoed in previous studies (Undakat et al., 2015). A previous review completed by Geach et al. (2018) highlighted the need for further research into the positives of team formulation as only weak evidence existed for the perceived benefits of team formulations. The current review adds additional insight into the potential beneficial effects team formulation may have on staff and adds additional richness to previous quantitative findings that have found team formulation to increase staff perceptions of formulations as a useful practice (Geach et al., 2018; Whitton et al., 2016). Qualitative studies, such as McMullan et al. (2019), have also found that providing staff with protected time and space in which to reflect help reduce feelings of burnout and helplessness. Additional research has also found that teaching and widening staff repertoires of intervention and working techniques has also helped reduce staff burnout (Ewers et al., 2002; Posner et al., 2017) findings that are corroborated by the current study. Ensuring staff have a protected time and space in which to reflect is pertinent for future practice.
Changes seen in participants’ thinking is also reflective of the DCP’s assertion that team formulations are an effective way of achieving cultural change and promoting psychosocial perspectives (DCP, 2011; Kennedy et al., 2003; Onyett, 2007). Team formulations should be utilized as a method of achieving cultural change and promoting person-centered care.
Perceived barriers to team formulation, especially time, were also highlighted within the present review. Considering the current pressurized context of the NHS and the culture of expecting more with fewer resources (Alderwick et al., 2015), it is important that team formulations are as efficient and impactful as possible. Mental health nurses have cited large workloads, as a result of excessive administrative duties, as a principle concern in the perception of their roles (Dallender & Nolan, 2002). Within this review staff cited the difficulties of team formulation as being negotiating the time together and competing demands. In future practice, these difficulties should be considered and more creative solutions, such as remote technology assisted meetings, need to be employed.
Limitations
Although the quality appraisal was considered in a clear and thorough way, some researcher influence still remains. The researcher considered their standpoint and enlisted another appraiser to appraise two of the include pieces of research to ensure a continuity of practice and allow for a space of reflection on the appraisal process.
Furthermore, a Thematic Synthesis can be influenced by the reviewer and their own opinions, and this is something that should be considered (Noyes et al., 2018). Thematic Synthesis allows the participants experiences to be at the forefront of the research, however the reviewer’s own experiences and opinions may have influenced what themes were found or discussed. The single primary researcher’s background is as a clinical psychologist and has previously participated in team formulations as both facilitator and participant. The researcher has had both negative and positive experiences and empathized with the more practical challenges facing participants in the current review. The structured process of Thomas and Harden’s (2008) Thematic Synthesis approach allowed the reviewer to refer back to a framework and enabled multiple reiterations of coding to take place to give the researcher time to reflect on any potential impact they may have had. The addition of a reflective log would have also been beneficial to allow for a subjective space within which the reviewer may have reflected on the process.
Through the exclusion of papers outside of the United Kingdom, important data related to staff experiences of team formulations may have been missed. The rationale of excluding studies outside of the United Kingdom was rooted in the notion that within the United Kingdom there were frameworks and a certain consistency put in place by professional bodies toward what was deemed to be a team formulation. The primary researcher is also U.K.-based and therefore it was hoped that through completion of the study the results of the present review could influence U.K.-based procedures for team formulations. However, it may be that studies from outside of the United Kingdom utilize a similar formulation framework and has therefore resulted in important data not being considered in the current review.
In addition, including data from psychologist participants is also a limitation to the current study. Although the aim of including psychologists was to allow more of an insight into the process and limitations of formulation, there are obvious limitations. In comparison with other members of the mental health team, psychologists may provide an alternative viewpoint of team formulations, usually from the role of facilitator rather than participator. The inclusion of data from the facilitator’s perspective means that some themes may not have been representative of those participating in the formulation.
Implications for Practice
This review demonstrates that staff place a strong importance on the process of team formulations, the impact on their clinical work and their professional values. Mental health teams should ensure that staff participating in team formulations feel that they are equally valued as well as feeling safe to contribute without being marginalized by more dominant members. It is clear that the benefit of team formulations is also felt on a personal level by staff, reflecting in the “Staff Validation” descriptive theme, and these benefits are an important consideration for the well-being of the team.
Staff highlighted the barriers to engaging in team formulation, including the lack of time and juggling multiple commitments, while highlighting the need for team formulations to be a safe and protected space. Future practice should ensure that team formulations are valued from a managerial level ensuring that staff members have a dedicated time to participate. Team formulations should either be scheduled for appropriate times to ensure that all staff, including those working on the front line, are included, or use more creative strategies utilizing technology assisted meetings. Overall, the current review demonstrates the potential benefits of team formulation in mental health settings, highlighting the impact of an increased use of psychotherapeutically informed approaches and working psychologically in the modern NHS.
Conclusions and Future Research Recommendations
The current review highlights the importance of team formulation in general practice for both enhancing staff understanding of service users and improving professional confidence and validation. The review also highlights the barriers to team formulation, namely time and staff juggling multiple commitments. The articles reviewed lacked researcher reflexivity, potentially resulting in overlooking the more negative facets of team formulations and this should be taken into account when considering the results of this review. Future research should consider the researcher’s impact on the data collection and engagement with participants, ensuring that staff feel they can be as open and honest as they need to be. Although not the focus of this review, it should be acknowledged that other perspectives, namely those of service users, are missing and should be considered when contextualizing the findings.
All of the research included in the current review took place within the United Kingdom, so future reviews may benefit from examining those studies that took place outside of the United Kingdom and consider different methods and forms of team formulations. Half of the research included in this review was taken from grey literature, which is an interesting point to note, and researchers should consider why more published data does not relate to experiences of team formulations.
The current review focuses on staff members’ views and opinions on team formulation; however, more research is needed to help define what a team formulation is and how it is often used. Once team formulations have been clearly defined and frame worked as a concept then the field would benefit from further research focusing on the effectiveness of these team formulation approaches in practice. An improvement in the evidence base of team formulations is important if it is a practice that is being frequently employed in clinically focused work. In addition to this, future research focused on staff views should make a clearer distinction between facilitator and participant viewpoints to facilitate clearer and more neutral feedback.
The present thematic synthesis also highlights the need for future research into team formulations, and indeed formulations themselves, to be published in peer-reviewed journals rather than remaining in the grey literature. The publication of team formulation focused research in peer-reviewed journals would increase awareness of research into this field by increasing the accessibility of the research while also subjecting the research to more stringent reviewing procedures.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.