
Abstract
There is no existing qualitative synthesis of the music therapy literature on parents’ perspectives on their children’s music therapy. This study seeks to fill this gap, motivated by the first author’s experiences as a clinician/researcher. A systematic search of health databases, hand searches of key journals and searches of doctoral theses were undertaken to identify relevant studies. Thirteen studies which met inclusion criteria, including a total of 102 participants, were identified. Relevant data were extracted from these studies for comparison and analysis, with quality of studies assessed using the CASP appraisal tool. Findings were analysed following procedures of thematic synthesis. Six descriptive themes were grouped into three analytic themes: Parents perceived positive impacts of music therapy on their children; parents experienced music therapy as a nurturing environment for themselves and their children; and some parents experienced challenges to their engagement with music therapy. Most studies (12/13) explored parents’ perceptions of music therapy where they were included in sessions. The findings identify positive perceptions of family-centred models of music therapy for children and parents. Parents’ perceptions of children were altered positively through experiencing them in new ways in music therapy. Parents also perceived positive outcomes for their children. These findings identify an emphasis in the qualitative literature on parents’ perceptions on research into music therapy which includes parents in sessions. Only one study explored perceptions of a model where parents were not present during their child’s sessions. More research is needed into parents’ perceptions of music therapy where parents are not present during sessions. Further intervention studies into family-centred models of music therapy with children are also recommended.
Introduction
Music therapy with children and young people incorporates various models of practice in a wide variety of clinical settings, including work with autism, learning disability, social and behavioural difficulties, and trauma (Cobbett, 2009; Kim et al., 2009; Robarts, 2014; Sutton, 2002; Wigram and De Backer, 1999). Parental roles in relation to their children’s music therapy can range from direct active participation to minimal involvement, covering a spectrum between these two possibilities. Much of the case study literature describes children seen individually by a music therapist, with a focus on the therapeutic relationship between the therapist and the child (Brown, 2013; Levinge, 2015; Mahns, 2002; Nordoff and Robbins, 2007). Parents might have a supportive role, where they function as facilitators, enabling and encouraging the child to attend music therapy, and exchanging information with the therapist as needed (Fearn and O’Connor, 2003). In some settings, parents may have less involvement, particularly where music therapy takes place in schools (Tomlinson et al., 2011).
In recent years, there has been an increasing tendency towards practice which includes the parent directly in the work (Cassidy and Stegemann, 2016; Edwards, 2011; Flower and Oldfield, 2008; Jacobsen and Thompson, 2016). Some approaches specifically describe themselves as ‘family-centred’, suggesting an intention to encourage active parental participation, or interaction between parent and child (Jacobsen and Thompson, 2016; Oldfield, 2016; Pasiali, 2013). Alternatively, the parent might be involved more actively, either as part of dyadic work between the parent and child (Gilboa and Roginsky, 2010), or within a group, in which musical interaction between parents and children is a key aspect of music therapy (Abad and Williams, 2006; Nicholson et al., 2010). In other cases, a parent may be present in the therapy room as an observer or facilitator, and some children may require a flexible approach, where family members are present during some, but not all sessions (Mitchell, 2017).
Despite the variety of models of work described in the literature regarding parental involvement in music therapy, there is no review to date of the qualitative literature on parent’s/carer’s perspectives on music therapy. Cassidy and Stegemann (2016) conducted a systematic review of direct parental involvement in music therapy, finding a variety of positive outcomes in the identified studies, but did not explore parents’ perceptions, including only a brief summary of the qualitative literature. This was the only available review of the music therapy research literature on parents identified by the authors. The current study will address this gap by synthesising the qualitative literature on how music therapy is perceived and experienced by the parents themselves.
Reflexivity
This study was conducted in partial fulfilment of a master’s degree in clinical research (MRes). The emphasis of the clinical research training, which broadly aligns with the paradigm of evidence-based practice, incorporating qualitative and quantitative methodology as appropriate, and determined by the research question, informs the approach to this study. The first author’s perspective, as a music therapy clinician/researcher within a National Health Service music therapy service in the United Kingdom, working with children and young people, has also informed the stance towards this study. The topic was chosen alongside a separate primary clinical research project exploring a similar research question (Annesley, 2020). The first author acknowledges the impact of this personal perspective on the process of study selection and data analysis. Inevitably, clinical background and theoretical models derived from training and practice have influenced the first author’s stance towards the data.
Aims of the study
The current study seeks to identify and synthesise qualitative research evidence on parents’ and carers’ perspectives on their child receiving music therapy, including exploring how parents perceive their own relationship to their children’s music therapy.
The study seeks to answer the research question, ‘What are parents’ perspectives on their children’s music therapy?’
Methods
The study follows procedures of thematic synthesis (Thomas and Harden, 2008) and seeks to gain a deeper understanding of the range of parents’ perspectives by synthesising the available literature. This involved a systematic approach to literature search and data extraction, followed by coding of text and the extrapolation of themes.
Selection criteria/participants, intervention and context
The focus of the study was on parents or carers of children receiving music therapy. (For brevity, ‘parents’ will generally be used to refer to all primary caregivers in the studies, as they formed the majority of participants.) These criteria were chosen to reflect the priorities of the research questions, with the focus on parents’ perspectives on any interventions described as ‘music therapy’. The study was not confined to a specific context, diagnosis or reason for referral (see Table 1). Both individual therapy and group music therapy were included. Music therapy exclusively with neo-nates and infants under 2 was excluded from the study, although studies including work with both children under 2 and older children were included. It was the perception of the first author that work exclusively with under-2s typically has a strong focus on parent–infant bonding, with an emphasis on the role of the parent in this process (Shoemark, 2017; Shoemark and Dearn, 2008). It was the aim of this study to focus on work where the child, rather than the parent–child dyad, has been referred to music therapy (as emphasised in the research question).
PICo table.

PICo: participants, intervention and context.
Only studies specifically seeking primary caregivers’ views on music therapy were included. Synthesis of qualitative data has been critiqued regarding potential difficulties of combining data from studies which adopt conflicting paradigms, for example, positivist versus constructivist (Greenhalgh et al., 2005). To achieve homogeneity, selection criteria were chosen to focus on studies using similar methods of data collection and where the data were analysed and presented in ways that enabled comparison across studies. Studies were included which involved interviews or focus groups with parents or carers, where the data were analysed qualitatively. The intervention had to be described specifically as ‘music therapy’ in the abstract and delivered by a qualified Music Therapist or trainee under qualified supervision, where service users were children and young people aged 0–18 (for a full list of inclusion and exclusion criteria, see Supplemental Appendix 1).
Search strategy and selection method
The databases PsycINFO, CINAHL, MEDLINE, AMED, EMBASE and PubMed were searched in February 2018 using the NICE HDAS platform (https://hdas.nice.org.uk/). No date limits were imposed on searches. Search strategies were intended to identify studies with a focus on music therapy as a specific health intervention, employing a qualitative methodology using interviews or focus groups. Medical and health databases were used because of the role of music therapy primarily as a health intervention and the need to identify studies compatible with the paradigm of evidence-based medicine. For PsycINFO, the following search terms were used (MeSH terms in capitals): ((‘MUSIC THERAPY’/OR (music* AND therap*).ab) AND (‘FAMILY MEMBERS’/OR PARENTS/OR (parent* OR carer* OR famil*).ab)) AND (INTERVIEWS/ OR (interview* OR ‘focus group’ OR ‘focus groups’).ab). Similar search terms were used for the other databases (see Supplemental Appendix 2 for full search strategy). Articles were screened by the first author by abstract to ascertain whether they fell within the criteria. A co-reviewer screened 25% of the articles to check for consistency. Any discrepancies were discussed by the two reviewers and resolved. Academic supervisors were consulted for studies where there was ambiguity regarding inclusion criteria which was not resolved by the two reviewers.
Google Scholar was used to conduct a search of the British Journal of Music Therapy, the Journal of Music Therapy and the Nordic Journal of Music Therapy in March 2018 using the search terms ‘parents’ and ‘interviews’. Eleven articles were identified and screened by abstract by the first author. EThOS was searched using the term ‘music therapy’, to identify PhD theses relevant to the study. Sixty-eight theses were identified, and abstracts were screened for relevance by the first author.
Following the identification of studies meeting the criteria for inclusion, full texts of all studies were obtained. Any studies found upon closer examination not to meet criteria were then excluded. Reference searches and citation chaining were then used to identify additional relevant studies.
Data extraction
A data extraction form was devised to compare equivalent data from each study (see Supplemental Appendix 3). Key elements of each study were listed (e.g. reference, sponsoring institution, type of intervention, sample size, research questions). The purpose was to compare characteristics of studies to ascertain key similarities and differences. Specific areas of clinical and research relevance were patient group, type of intervention, sample size and method, and research questions for each study. For findings/results, all the text in the ‘findings’ or ‘results’ section of each article was pasted into the form. Where tables were used in the study, these were only included where they contained findings that were not in the body of the text. Findings/results were then imported into NVivo11 software for comparison and analysis across studies.
Quality assessment
The quality of studies was assessed using the CASP Qualitative Checklist (Critical Appraisal Skills Programme, 2018) (see Supplemental Appendix 4 for the full CASP appraisal of all the studies). While the CASP Checklist does not produce a score for each study, observation of the data in the table indicates that studies were broadly of good quality; 11/13 studies were strong on clarity of aims, appropriate methodology and design; 5/13 were ambiguous with regard to recruitment strategy, and some (5/13) did not show clear evidence of consideration of the relationship between researcher and participants.
The role of quality assessment in qualitative synthesis is debated, since there are no broadly accepted methods for exclusion on the basis of quality (Dixon-Woods et al., 2004; Thomas and Harden, 2008). Furthermore, it has been noted that poor quality of reporting does not necessarily indicate poor data (Boland et al., 2017). This study follows the model of Thomas and Harden (2008) by including quality appraisal to provide context, and including all identified studies in the synthesis.
Thematic synthesis
The focus in this study was on first- and second-order constructs (Schutz, 1973, cited in Toye et al., 2013), as this addresses the research question, ‘What are parents’ perspectives on their child’s music therapy?’ First order constructs are defined as the participants’ own words, whereas second-order constructs are the researchers’ interpretations, including codes and themes derived from the participants’ words (Toye et al., 2013). Toye et al. (2013) also acknowledge that the selection of participants’ words is determined by the authors. Since ‘discussion’ sections normally compare findings to those of other studies, bringing in the view of other authors, these constitute third-order constructs, which are less relevant to the focus of this research question. For the purposes of this review, text was extracted from ‘findings’ or ‘results’ sections of all studies.
Analysis was conducted following methods of thematic synthesis as described by Thomas and Harden (2008). Thematic synthesis is not a method that has been widely used in music therapy qualitative literature reviews, but is a recognised method in the broader health literature (Barnett-Page and Thomas, 2009; Boland et al., 2017). It was deemed to be an appropriately concise and pragmatic approach within the limited scope of this project. Thematic synthesis draws on the techniques of thematic analysis (Braun and Clarke, 2006), used in primary research, and applies these to the synthesis of qualitative literature. The method seeks to address ‘questions relating to intervention need, appropriateness and acceptability – as well as those relating to effectiveness – without compromising on key principles developed in systematic reviews’ (Barnett-Page and Thomas, 2009: 6). The emphasis in this study is on intervention appropriateness and effectiveness, as perceived by parents of children receiving music therapy. Thomas and Harden emphasise the importance of ‘translation’ across studies (p. 3). The generation of analytic categories is described as an inferential process which enables the synthesis to ‘go beyond’ the content of the original studies in order to answer the research questions posed at the outset (Thomas and Harden, 2008: 3). This is the process by which shared concepts are identified, partly through the process of coding and devising themes. Text from the ‘results’ or ‘findings’ sections from the articles was imported into NVivo 11. Data were coded line by line and codes were compared across studies. Initially this produced a very large number of codes across all of the studies. Codes were then merged within studies and across studies where appropriate to produce a final list of 44 codes. These codes were then grouped into six descriptive themes. Descriptive themes were grouped into three analytic themes, producing a hierarchy of codes and themes which informed the findings.
Findings
Included studies
In all, 320 articles were identified from the database search. Of these, 126 duplicates were identified and deleted using the online tool Rayyan (Ouzzani et al., 2016). The remaining articles were screened by title and abstract, according to the inclusion and exclusion criteria. Ten studies from this database search were included. The hand search of the British Journal of Music Therapy, the Nordic Journal of Music Therapy and the Journal of Music Therapy identified one additional study, and the EThOS search identified two PhD theses which met the inclusion criteria. Upon closer reading of full texts, three studies were found not to fall within inclusion criteria. One was a quantitative intervention study (Thompson et al., 2014), another was a study of perceptions of a performance following music therapy (Fairchild et al., 2016) and the third was a mixed-methods study from which qualitative data were not extractable (Pasiali, 2012). A further three studies were identified through reference searches and citation chaining, producing a total of 13 studies including a total of 102 participants (see Figure 1).
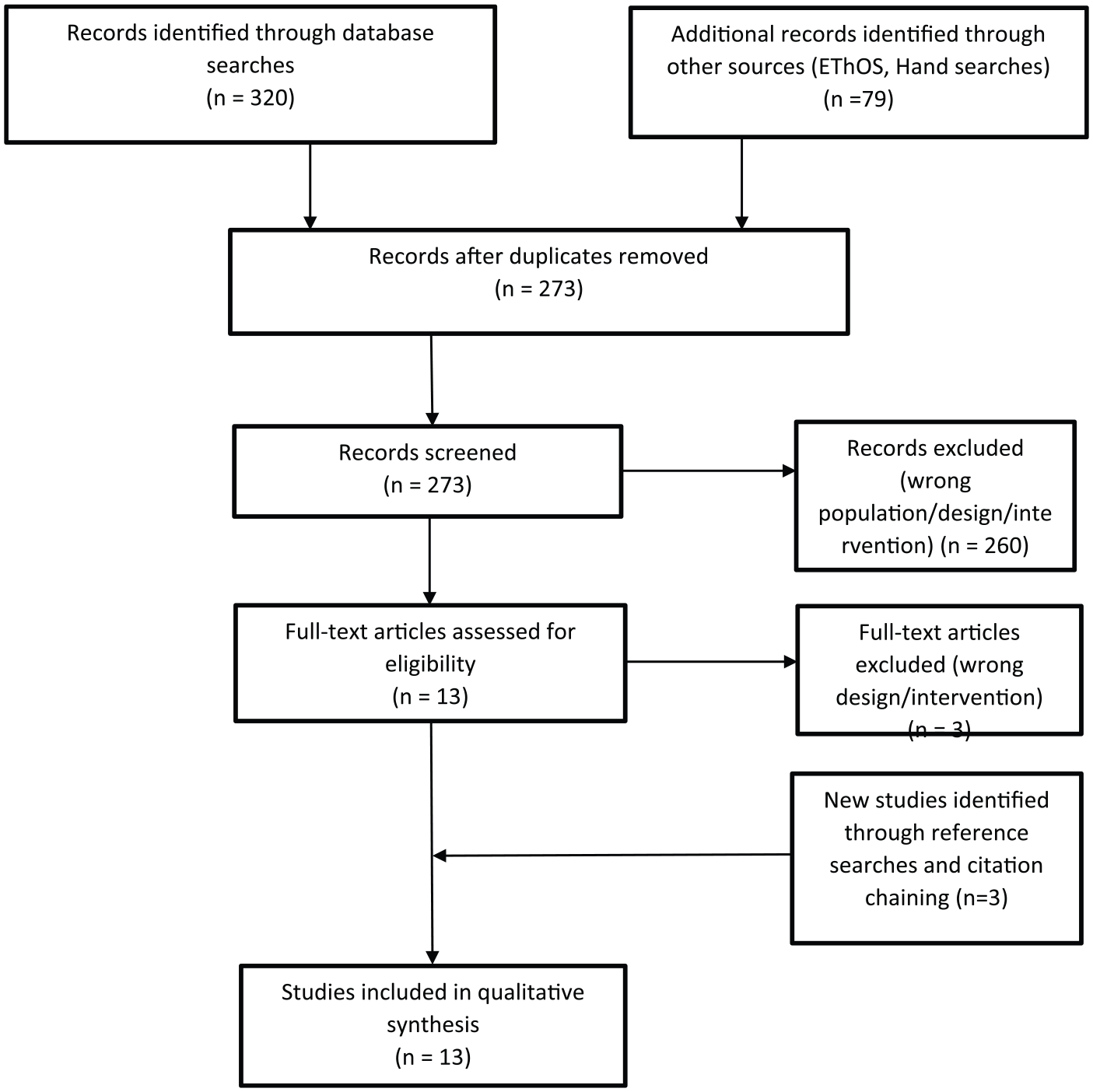
PRISMA flow diagram of progress through the systematic review.
In 12 of the 13 eligible studies, authors describe sampling children with specific needs: 2 in palliative care settings (Lindenfelser et al., 2008, 2012), 5 with autistic spectrum disorders (Allgood, 2005; Oldfield, 2003; Schwartzberg and Silverman, 2017; Thompson, 2017; Thompson and McFerran, 2015) and 5 with other disabilities or ‘special educational needs’ (Archer, 2004; Chiang, 2008; Flower, 2014; Gutierrez-Jimenéz and Franco, 2018; Kaenampornpan, 2015). One did not specify referral reasons, as the study took place in a context where children were seen for a variety of reasons (Procter, 2005). All studies falling within criteria employed interviews as the method for qualitative data collection.
Authors describe parents not being present during sessions in one study only (Procter, 2005). In the remaining 12 studies, 10 describe active parental involvement in sessions, while 1 study describes parents as ‘observing’ sessions (Chiang, 2008), and 1 does not specify the level of active involvement (Gutierrez-Jimenéz and Franco, 2018) (see Table 2).
Summary of studies included in thematic synthesis.
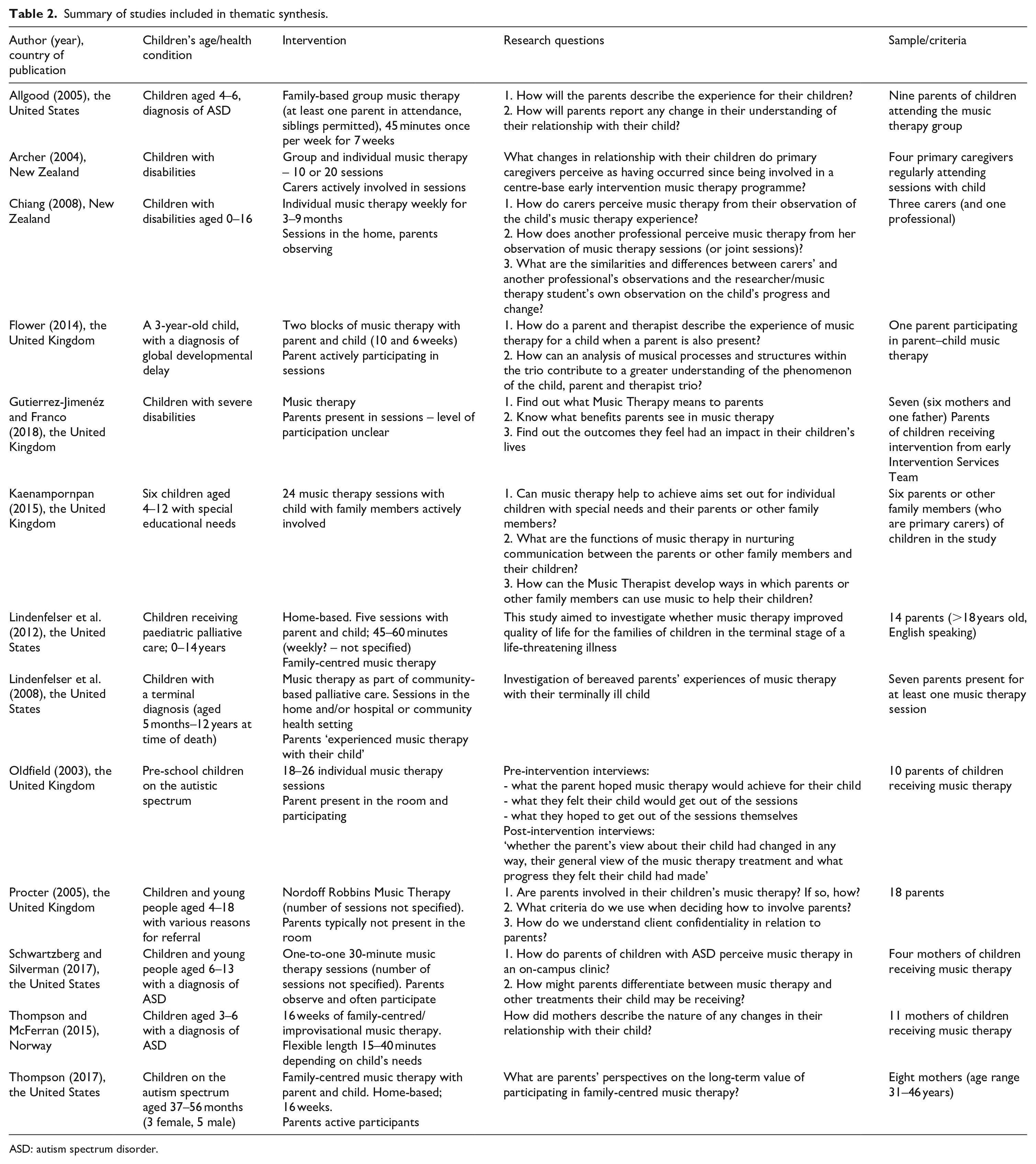
ASD: autism spectrum disorder.
Synthesis of findings
The thematic synthesis indicated that participants perceived that music therapy led to beneficial changes in relationships with their children and met their children’s needs in ways that had a positive impact across physical, emotional and developmental spheres. However, some parents also described difficulties with their engagement with music therapy. In one study, specific issues were explored in relation to the issue of confidentiality (Procter, 2005). The three analytic themes identified through the thematic synthesis are as follows:
Parents perceived positive impacts of music therapy on their children
Parents experienced music therapy as a nurturing environment for themselves and their children
Some parents described difficulties with engaging with music therapy
The analytic themes (italics) and descriptive themes (in single quotes) will now be explored (see Supplemental Appendix 5 for the full list of analytic themes, descriptive themes and codes).
Parents perceived positive impacts of music therapy on their children
Positive impacts of music therapy were perceived across several domains. These included impacts on emotional parameters such as mood or confidence, as well as, in some cases, specific physical benefits. Some of these areas of perceived improvement were specific to patient group, whereas others were more generally applicable across studies.
‘Emotional benefits of music therapy’
Parents described children feeling calmer and more relaxed because of music therapy. This feeling of calmness was identified primarily during the sessions themselves, with music perceived to have a soothing effect on children who were in distress from an illness (Lindenfelser et al., 2012). Some children were also described as becoming more socially open and outgoing.
Music activities increased Justin’s awareness of self and others which helped him engage in social play. (Chiang, 2008: 42)
Linked to this, parents also saw improved potential in their children’s openness to contact with others.
She actually was interested in how I was feeling or reacting to her while she was playing an instrument. She wanted me to watch her or she tried really hard to join in. (Thompson and McFerran, 2015: 14)
Other perceived positive emotional impacts were improved confidence and a perception that children were feeling positive about sessions and enjoying their time in music therapy, both widely shared views across the studies.
‘Social communication benefits of music therapy’
Parents perceived music therapy as having positive developmental outcomes for their child in several areas. They saw benefits for the child’s capacity for concentration and their communication skills.
Mothers identified that their child developed vocabulary and gestures, and could see sustained improvements in social engagement through better eye contact. (Thompson, 2017: 444)
‘Physical benefits of music therapy’
Physical benefits included an impact on motor skills, including the ability to hold objects. While this was particularly relevant for children with disabilities, it was perceived by participants across various studies as a beneficial outcome. The use of musical structures was reported to have a positive impact on some children’s ability to respect boundaries within the sessions, for example, waiting and taking turns. Music therapy was also perceived to develop the child’s independence.
Parents experienced music therapy as a nurturing environment for family relationships
Music therapy provided opportunities for parents to experience themselves and their children in new ways, supported by the therapist, in the therapeutic environment. Music was often described as having a strong motivating influence on the child, enabling them to engage with the sessions, and parents spoke about their children being enthusiastic about attending sessions.
‘Changing family relationships’
Parents described how music therapy changed their perception of their child in positive ways. For some parents, music therapy brought out a different side of their child’s personality. This was, for example, about seeing their child ‘actually having some fun’ (Thompson, 2017: 445). These new experiences altered the quality of the parents’ relationship with their child. Parents changed the way they interacted with children, becoming more playful. Music therapy ‘encouraged them to engage with their children more’ (Kaenampornpan, 2015: 160). Parents linked these changes to feeling closer to their child which led to positive changes in the overall quality of their relationship. These changes in relationship were specific to session formats where parents were included in music therapy sessions (12/13 studies).
Parents’ perceptions of their child’s capacities to achieve certain goals were raised in the music therapy environment. One parent, for example, described that ‘music therapy assisted Eric [their child] to do what was originally thought to be impossible to achieve’ (Chiang, 2008: 24), while another described their child as ‘a lot more adaptable than I gave him credit for’ (Allgood, 2005: 97). Music therapy was perceived to provide an environment where children who struggled in their daily lives were able to thrive in unexpected ways. Parents were sometimes surprised by their child’s ability to follow instructions or to understand the structure of the music therapy session. The mutual enjoyment provided by music therapy was perceived to stimulate children to greater connectivity and interaction. This was also described as extending beyond the sessions themselves. The activities used in the session reportedly gave most parents a model for using music at home with their child.
‘Meeting child and family’s needs’
Parents felt that music therapy provided opportunities to focus on the child. Music therapy was experienced as a safe environment where children would not be judged detrimentally. Across most studies, parents valued sessions as a space where children had opportunities for expression, particularly for finding alternatives to verbal expression. This was particularly the case for children with a diagnosis of autistic spectrum disorder.
She is learning a variety of avenues that she can utilize to express herself better. Expression, it takes so much work for her brain, to organize her thoughts and feelings into the words she knows you and I will understand. (Schwartzberg and Silverman, 2017: 103)
Music therapy was felt to facilitate connection between parents and children, but also between parents and therapists. In one instance, the music therapy session also enabled connections between families, where they were working together in a group (Allgood, 2005). The relationship between the parent and the therapist was perceived as providing mutual support. A co-operative approach was seen to be beneficial, where the therapist was open to suggestions and flexible in their own responses. Parents also valued time spent in discussions with the therapist outside the session, whether in one-to-one meetings or over the phone. Parents acknowledged the importance of their trust in the therapist, both as a professional with expertise and as a person with knowledge of their child’s difficulties and needs. The therapist’s perceived expertise was important not only in relation to clinical knowledge and training but also in relation to the therapist’s ability to create a relaxed supportive atmosphere in the music therapy session.
Some parents described difficulties with engaging with music therapy
This analytic theme explores more challenging experiences described by some parents. This includes difficulties with engagement for the child as well as feelings of disconnection experienced by the parent. Several studies did not report any difficulties with engagement and it is the smallest theme in terms of its representation within the studies. However, this theme is important in that in brings out experiences which were more difficult, and which in some cases contradict some of the other findings. The importance of anomalous or surprising findings has been identified as an important feature of qualitative enquiry, in that it can challenge established theory, as part of an ongoing interaction between theory and data (Tavory and Timmermans, 2014).
‘Disempowerment of parents’
Parents in one study (Procter, 2005) experienced feelings of disempowerment. This was linked to not being present during the child’s sessions, and highlights a perception of a power imbalance, with the therapist perceived to have more power than the parent.
Some parents gave moving accounts of their feelings of disempowerment resulting from what they experienced as a lack of awareness of what was going on in their child’s music therapy. They were reluctant to demand more information as they feared that this would be received as disrespect or lack of trust or perhaps jeopardise what was in their child’s best interest. (Procter, 2005: 51)
Participants in this study were also sceptical about the benefits of confidentiality in respect of their own child’s sessions, despite being able to see the value of it in principle. They understood that the therapeutic space was ‘private’ but found this experience of exclusion difficult.
‘Ambivalence about music therapy’
This theme was more widely applicable across studies. Music therapy induced feelings of emotional vulnerability for some parents, who were unclear about their role in sessions or lacked confidence in their own musical abilities, which they perceived as a barrier to using music at home.
There is much difference. I am not a musician. I just play around randomly. But with the music therapist, she sang, made a song in different tempo. The music is better. (Kaenampornpan, 2015: 184)
Some parents said they would have preferred longer sessions or for the period of music therapy to have lasted for longer.
In the post-treatment interview Mi’s mother was openly angry that Mi’s sessions had stopped. She felt that Mi was just starting to show signs of progress in the last few sessions. (Oldfield, 2003: 183)
A small number of parents said that their child did not engage well with music therapy, or that it had taken their child a long time to engage.
Participant 2’s mother stated that she felt that her son struggled with auditory processing issues, did not like the room, and did not feel comfortable in the group. (Allgood, 2005: 97)
Many also described the difficulties their child faced prior to therapy, and that the family were going through a difficult process of adjustment, for example, after a diagnosis.
Discussion
This review synthesises themes from qualitative research studies exploring parents’ perceptions of their children’s music therapy. The thematic synthesis highlighted three key areas. These were parents’ perceptions of outcomes of music therapy for their children, parents’ experiences of the therapeutic environment and perceived barriers to engagement. The findings indicate that parents perceived music therapy as beneficial for their children and for family relationships. In most studies, music therapy was perceived to provide a nurturing and facilitative environment for both parents and children. Most studies focused on music therapy where parents were directly involved in sessions. Positive perspectives on these experiences align with the wider literature, which identifies benefits of family-centred work and parent–child dyad work (Horvat and O’Neill, 2008; Jacobsen and Thompson, 2016; Oldfield, 2016). One study described isolated occasions where the parent was not present (Kaenampornpan, 2015), while Procter (2005) explored a model where parents are typically not present during sessions, identifying specific barriers to parental engagement with music therapy which were not described in the other studies. These findings identify, in the qualitative literature on parents’ perceptions, a strong prevalence of research into music therapy which includes parents in sessions.
Music therapy was perceived to have the potential to relax children, inducing a calmer mood, while it also provided motivation to engage. Positive impacts were perceived by participants both during and following music therapy. Parents saw music therapy as improving areas such as social communication, concentration, flexibility of responses, confidence and independence.
Descriptions by parents of the therapeutic environment, and of how their experiences in music therapy led to changes in perspectives on their children, might be understood within a social or ecological frame, where human relationships, rather than perceived clinical outcomes, might be a focus of the work. Music was perceived to facilitate the re-examining and deepening of relationships within families or wider social groups. This perception is supported by Ansdell (2016), who describes music therapy as helping people ‘find or re-find connection, companionship and community’ (p. 143). Primadei (2014) describes the music therapy setting as ‘a space with a less medicalized context, where a child can experience her therapeutic process in an artistic, creative way’ (p. 198). Baron (2016) describes how ‘I see my role as a pediatric music therapist to connect with a family and enhance family relationships where possible’ (p. 59). This also shows similarities with parent work in Child and Adolescent Mental Health Services (CAMHS), where fostering the parent’s empathy for their child may be an important aspect of the work (Holmes, 2018).
The perception of music contributing to an environment which facilitates connection links to the concept of ‘communicative musicality’ (Malloch, 1999; Malloch and Trevarthen, 2009). Links between parent–infant attunement and musical processes of interpersonal connection in music therapy have also been made by Pavlicevic (1997), who relates her theory of dynamic form in clinical improvisation to Stern’s (1985) concept of affect attunement. Some parents described a change in the quality of their relationship with their child which is brought about through music, including one example of a child who would let the parent sing to him following music therapy (Oldfield, 2003). They also emphasise the importance of shared enjoyment, which resonates with Ansdell’s (2002) emphasis on communitas as a function of music therapy and which forms part of the rationale for the Community Music Therapy (CoMT) movement. In CoMT approaches, there are attempts to look beyond the focus on treating an individual and towards seeing people as part of a wider supportive community, where music can create links between people to foster well-being (Aigen, 2018; Ansdell and Pavlicevic, 2004).
Parents’ understanding that music therapy had positive outcomes is supported by some intervention studies, including studies which demonstrate positive impacts on the parent–child relationship (Colegrove et al., 2018; Jacobsen et al., 2014; Thompson et al., 2014). The perception of the impact of music therapy on areas of functioning for children and young people such as mood, independence and confidence, as described by parents, has some limited evidence in intervention studies (Porter et al., 2017). In case study and theoretical literature, music therapy with children is often framed as supporting confidence and developing a stronger sense of self through play (Flower and Oldfield, 2008; Halliday, 2017; Levinge, 2015). The narrative of intervention and outcomes also links to reasons for referral. All of the studies describe the music therapy referrals as stemming from the needs of the children, either because of a diagnosis, disability, illness or emotional/behavioural difficulties.
Parents described barriers to engagement with their child’s music therapy in Procter’s (2005) study. There was a focus in this study on difficulties with client–therapist confidentiality and feelings of disempowerment associated with this. There are clear structural reasons why this would not be an issue for parents who are in the room during sessions, since confidentiality is not a relevant issue where parents are witnesses to the child’s therapy. However, other studies also show parents who lacked confidence to carry the work forward at home, highlighting a perception of a gap in musical expertise between the therapist and parent (Archer, 2004; Kaenampornpan, 2015). Jacobsen and Thompson (2016) explore the various roles that music therapists might adopt in relation to families, identifying a risk that any lack of clarity might be experienced as ‘confusing and chaotic’ (p. 324). Therapists might be ‘an equal within the family system or an expert outside of the family system’ (Jacobsen and Thompson, 2016: 324). They identify the importance of having a clear rationale for either stance (Jacobsen and Thompson, 2016). The varying roles of parents when they are present in the music therapy room has been critiqued by Horvat and O’Neill (2008), who identify a need for flexibility on the part of the therapist. They recognise that parental involvement might be necessary for different reasons, including the need to provide additional support for the child, or to adopt a stance where ‘difficulties in the child–parent relationship become the main focus of the therapy’ (Horvat and O’Neill, 2008: 98).
It seems clear from Procter’s (2005) study that problems arose with engagement where parents felt themselves to be disconnected from the process. What Procter (2005) did not explore with parents was whether there might be any specific advantages in this way of working. Procter’s consultation with music therapy experts, part of the same study, did explore this issue. Experts expressed ‘a perception that older children can benefit from space to “grow” without a parent present’ (Procter, 2005: 53). The implications of this alternative perspective will be explored below in the recommendations for further research. It would seem to point to a therapeutic potential not explored in any of the studies identified in this synthesis. While the findings of this review point to music therapists actively seeking to involve parents more closely in their children’s music therapy where possible, the potential for music therapy to facilitate the child’s independence, and for this to be seen as a positive development by parents, is notably absent from the discourse.
Implications for practice
The synthesis of data across studies may have legitimate implications for wider practice (Thomas and Harden, 2008). The review demonstrates some commonly held perceptions among parents and carers regarding the benefits of music therapy which includes them in the sessions. There are indications that music therapy can provide opportunities for shared positive experiences which may have beneficial impacts on parent–child relationships. Where parents are not present in the room during sessions, it may be helpful for practitioners to consider processes of communication with parents, although this conclusion is drawn from findings of just one study (Procter, 2005). The perception of some parents that their lack of musical expertise was a barrier to using music outside the session suggests that solutions to this might be beneficially incorporated into models of practice.
Limitations of the study
It is important to acknowledge that the studies identified in this review present a variety of parental roles in relation to the music therapy clinical setting. Parents’ perceptions of their child’s music therapy are inevitably influenced by their own roles, and by their relationship with their child, with the child’s Music Therapist, and with the clinical focus of the work. Studies included in this review work across a variety of client groups, within a range of ages (0–18) and with various reasons for referral. It could be argued that to compare studies where children are being treated for different reasons is problematic. This may be particularly important when examining clinical impact. For example, some studies identify impacts of music therapy on language development for children with learning disabilities, whereas other studies have a stronger focus on children for whom language development is not identified as a reason for referral. Similarly, the two studies on palliative care described the value of music therapy in providing memories of times with children who subsequently died (Lindenfelser et al., 2008, 2012) which was not a feature of any of the other studies.
Literature searches were systematic, but because of the subjectivity in defining terms, it could be that alternative strategies would have produced more results. The economic and time constraints of the study imposed certain limitations, including the restriction to English language publications and the process of coding being undertaken by a single researcher. While ‘bias’ is a debated concept in relation to qualitative research (Galdas, 2017), the process of coding and identifying themes is inherently subjective, and it is acknowledged that the findings of the synthesis are a product of the personal reflections and considerations of the first author alone.
Recommendations for research
Parents’ perceptions of positive outcomes point to a need for further intervention studies. Studies of the impact of music therapy on children’s social confidence, anxiety, concentration and motor skills may be of value. Further studies on the impact of family-centred and dyadic approaches to music therapy on family relationships, and on the family’s use of music beyond music therapy intervention are also needed, as these were all positive benefits identified by participants.
The strong prevalence of qualitative studies of parents’ perspectives on music therapy where they are present during sessions, combined with the anomalous findings from Procter’s (2005) study, indicate a need for further studies of parents’ perspectives on their child’s music therapy where they are not present during sessions. This model of working, where parents are not in the therapy room during sessions, is better represented in the case study literature than in qualitative research. Since this is common practice in music therapy, in part due to the prevalence of sessions taking place in school contexts (Tomlinson et al., 2011), this remains a relatively unexplored but important area of enquiry. It may be that parents’ views have been unduly ignored by music therapist researchers, except where they have direct involvement in the work, and if so, this indicates a need for this to be redressed.
Conclusion
This thematic synthesis of the qualitative literature demonstrates positive perceptions of children’s music therapy by parents across a range of studies. This has implications for music therapy practice with children and young people, indicating, in particular, the potential of parental inclusion in sessions, which is perceived by parents to have positive outcomes across several domains. These include perceptions of specific outcomes for the child, as well as broader positive impacts on social and family relationships. A prevalence in the literature of music therapy which includes parents in sessions has been identified. This has implications for research, since there is a gap in the research literature on parents’ perceptions of music therapy, where they are not included in sessions with their children. Parents’ roles and level of involvement would appear to be worthy of consideration by music therapists. The variety of approaches identified here would seem to indicate benefits of a flexible approach to practice across cohorts and depending on individual need. In some cases, parents may find clear benefits to being present during sessions. Conversely, benefits of a therapist–child dyadic approach require further exploration with regard to communication with parents, and specific advantages for children receiving music therapy.
Supplemental Material
BJMT_Submission_Appendices – Supplemental material for Parents’ perspectives on their children’s music therapy: A synthesis of qualitative literature
Supplemental material, BJMT_Submission_Appendices for Parents’ perspectives on their children’s music therapy: A synthesis of qualitative literature by Luke Annesley, Eamonn McKeown and Katherine Curtis-Tyler in British Journal of Music Therapy
Footnotes
Acknowledgements
The author(s) would like to acknowledge Oxleas Music Therapy Service, Sarah Hadley, Anthony Davis, Holly Wilkinson, Gemma Knight and all of the participants who took part in this study. This study was completed in partial fulfilment of the Clinical Research MRes at City, University of London.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Funding for the MRes was provided by the HEE/NIHR Integrated Clinical Academic Programme.
Supplemental material
Supplemental material for this article is available online.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.