
Abstract
The apparent intensity of hyaluronan (HA) staining in tissue sections can vary as a function of fixation techniques. We examined the histochemical distribution of HA in normal human skin using an HA-specific binding peptide derived from bovine nasal cartilage. The HA, particularly in the dermis, was best preserved in sections fixed in 10% acid-formalin with 70% ethanol. In contrast, sections fixed in the routine 10% neutral-buffered formalin had a much weaker intensity of HA staining. Furthermore, acid-formalin/ethanol-fixed sections retained much of their apparent HA after incubation with saline, in contrast to the neutral formalin-fixed sections, in which most of the stainable HA was lost. Such marked differences in staining intensity were not observed in slides stained with Alcian blue, a procedure pressumed to stain HA as well as other glycosaminoglycans. Staining using the HA binding peptide was entirely absent when sections were first preincubated in hyaluronidase, whereas similar Alcian blue-stained sections retained most of their staining intensity. Caution should be exercised in evaluating the distribution of HA in tissues using the HA binding peptide, particularly when different fixation techniques among several laboratories are being compared. In addition, the ability to evaluate the HA content of tissues using Alcian blue staining should be reconsidered. The sulfated glycosaminolglycans of the “ground substance” appear to be the predominant substrates for Alcian blue.
Recently, a technique for the histolocalization of HA (Ripellino et al. 1985) that utilizes a highly specific HA binding peptide (HABP) has become widely used. This peptide, derived from aggrecan, the chondroitin sulfate-rich proteoglycan of cartilage, is isolated from tryptic digests of bovine cartilage by HA immunoaffinity chromatography and then biotinylated (Tengblad 1979). Such preparations also contain cartilage link protein, a small protein that enhances the aggrecan–HA interaction. However, even this HABP procedure may seriously underestimate the HA content of tissues fixed in a routine manner.
The distribution of HA in human skin has been described using the HABP technique (Tammi et al. 1988; Meyer and Stern 1994). Dermal HA staining was not conspicuous in these studies, although the dermis is a major reservoir of HA (Reed et al. 1988). Studies by Wells et al. (1990) demonstrated enhanced HA levels in the dermis utilizing the same HABP staining procedure, except that the tissue had been fixed in neutral paraformaledehyde containing 1% cetylpyridinium chloride (CPC). Although CPC improves the preservation of HA in samples, total HA cannot be accounted for. A drawback to the CPC fixation procedure is the frequent appearance of precipitates. In this study we demonstrated that tissues fixed in solutions of acid–formalin with alcohol have markedly enhanced patterns of HA staining. The HA appears to become permanently bound to tissues after such fixation. Subsequent incubations in aqueous solutions did not decrease the apparent tissue content of HA. Therefore, the mode of fixation can modulate the apparent distribution and content of HA in tissues.
Materials and Methods
Tissue Samples
The sample of human skin, obtained from a routine autopsy in the Department of Pathology, University of California, San Francisco, was taken from the scalp of a 35-year-old white man. The specimen was divided in two and one sample was fixed in 10% formalin in 70% ethanol and 5% glacial acetic acid (acid-formalin/EtOH), all v/v. The precise formulation of this solution is as follows. For each 100 ml of fixative, 10 ml of stock 37–40% formaldehyde, 70 ml of 100% ethanol, 5 ml of glacial acetic acid, and 15 ml of water were utilized. The other sample was fixed in 10% neutral-buffered formalin, using 0.1 M PBS, pH 7.35, as described (Hellstroem et al. 1990). Both skin samples were embedded in paraffin using routine procedures, sliced at 5-μm thickness, and mounted on glass slides coated with polylysine.
Histochemical Staining for HA
The HA-specific HABP was prepared as described (Tengblad 1979; Meyer and Stern 1994). The histolocalization of HA was determined using the biotinylated HABP according to a modified technique described previously (Meyer and Stern 1994). Briefly, sections were subjected to deparaffinization followed by rehydration. They were divided into four treatment sets. One set of sections was stained for HA using the HABP. A second set, a control, was stained with HABP that had been preincubated overnight at 4C in a solution containing 0.3 mg/ml HA (ICN; Irvine, CA). The third set, an additional control, was pretreated with 50 U/ml Streptomyces hyaluronidase (Calbiochem; San Diego, CA) at 37C for 24 hr. The fouth set was preincubated with PBS at 37C for 24 hr before staining for HA. Normal goat serum (Vector; Burlingame, CA) at 3% concentration was used as a blocking solution. For final color development, avidin-conjugated alkaline phosphatase and its corresponding substrate (Vector) were utilized. All slides were counterstained with Nuclear Fast Red and mounted with Permount. Microphotographs were taken using an Olympus Vanox AHBT3 microscope (Olympus; Woodbury, NY) with an integrated Olympus C-35AB-Y camara.
Alcian Blue Staining
The Alcian blue staining was performed in pH 2.5 buffers using a method as described (Luna 1960). Briefly, slides were deparaffinized, rehydrated, and incubated in 3% acetic acid solution for 3 min. The slides were then incubated with 2% Alcian blue, pH 2.5, at 37C for 24 hr. The slides were washed, followed by counterstaining with Nuclear Fast Red solution, and mounted with Permount. Similar to the procedures described above for HABP staining, a control set of slides was preincubated with PBS at 37C for 24 hr before staining with Alcian blue.
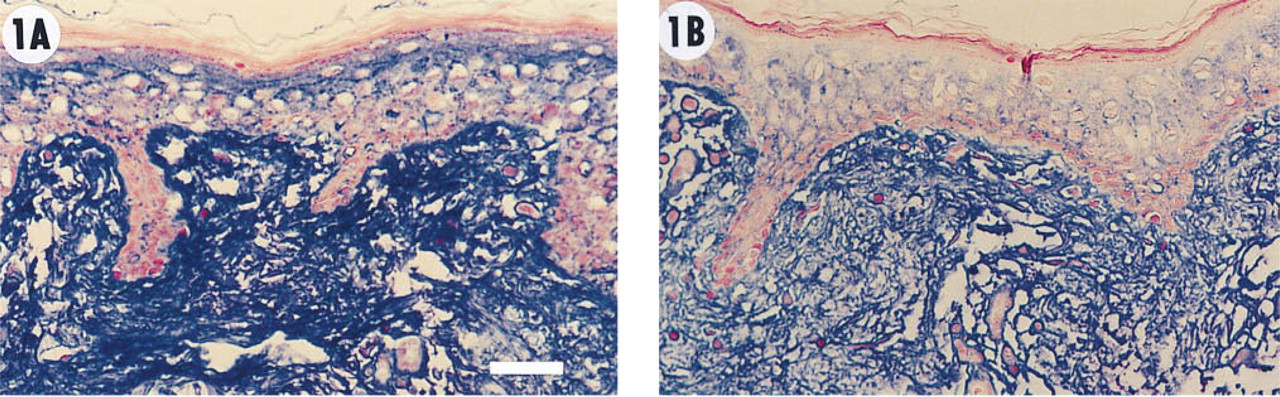
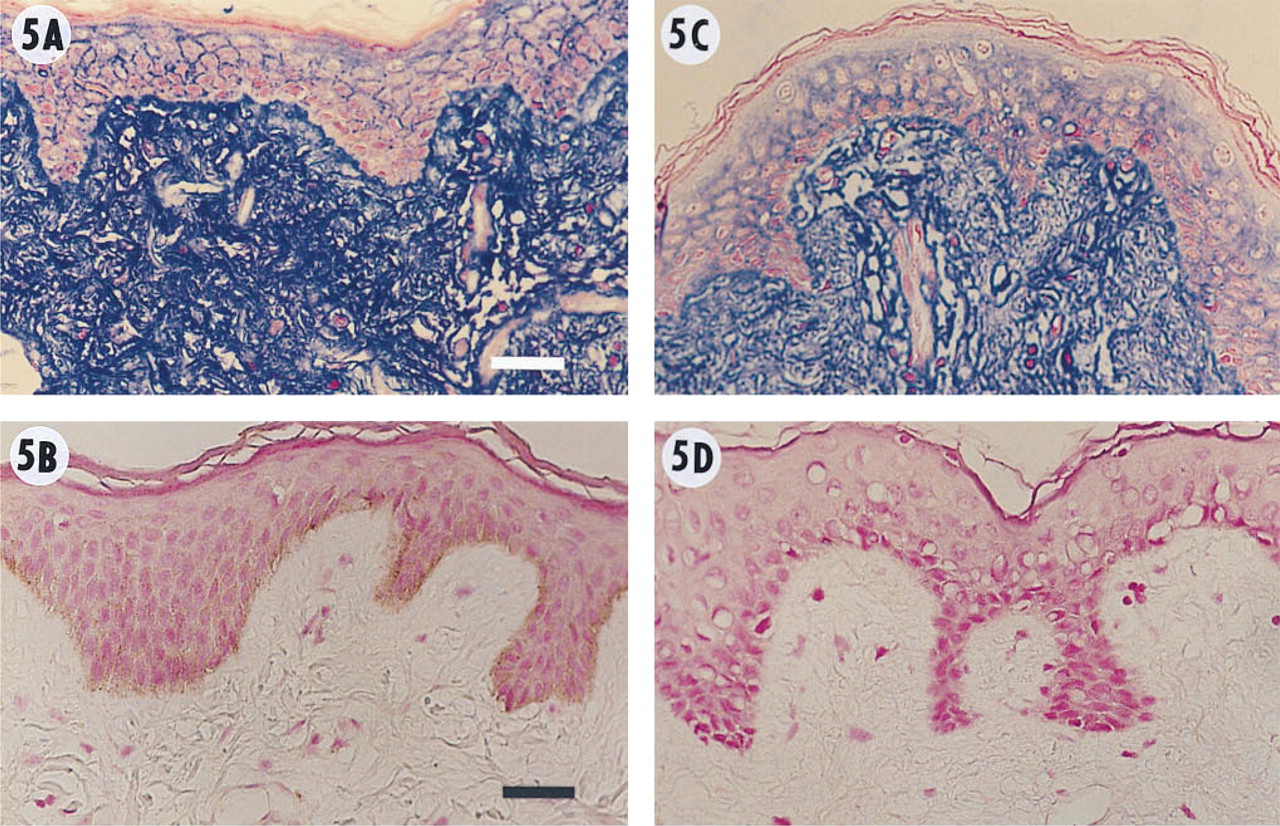
Human skin stained for HA with HABP as described in Materials and Methods. The localization of HA was shown after color (blue) development using avidin-conjugated alkaline phosphatase and its corresponding substrate. The slides were then counterstained with Nuclear Fast Red to visualize skin structures. (
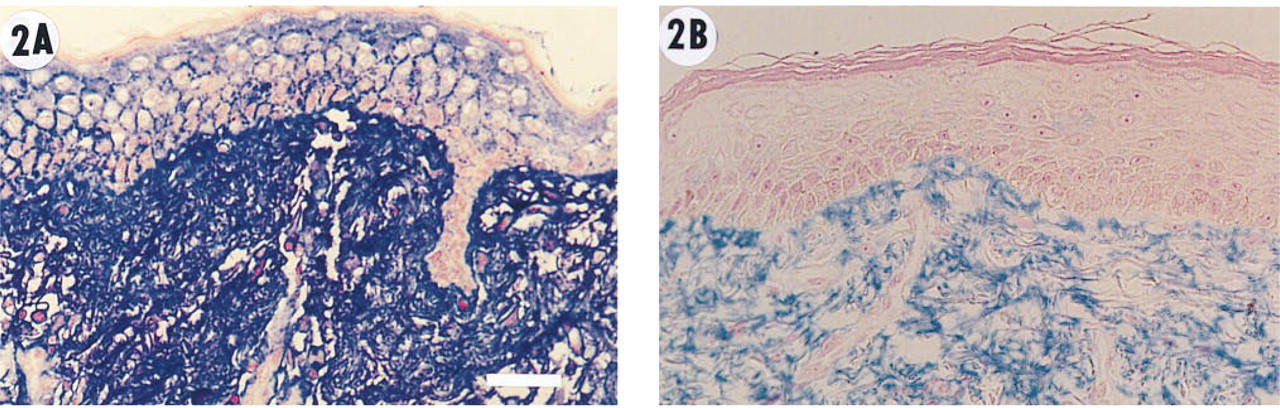
Human skin stained for HA with HABP after preincubation with PBS at 37C for 24 hr before staining for HA with HABP as described in Materials and Methods section and in Figure 1. (
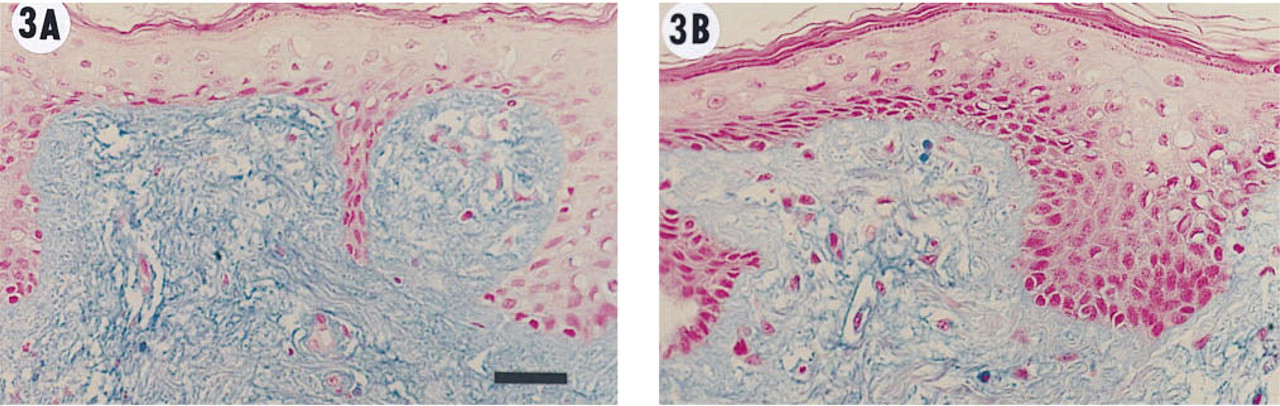
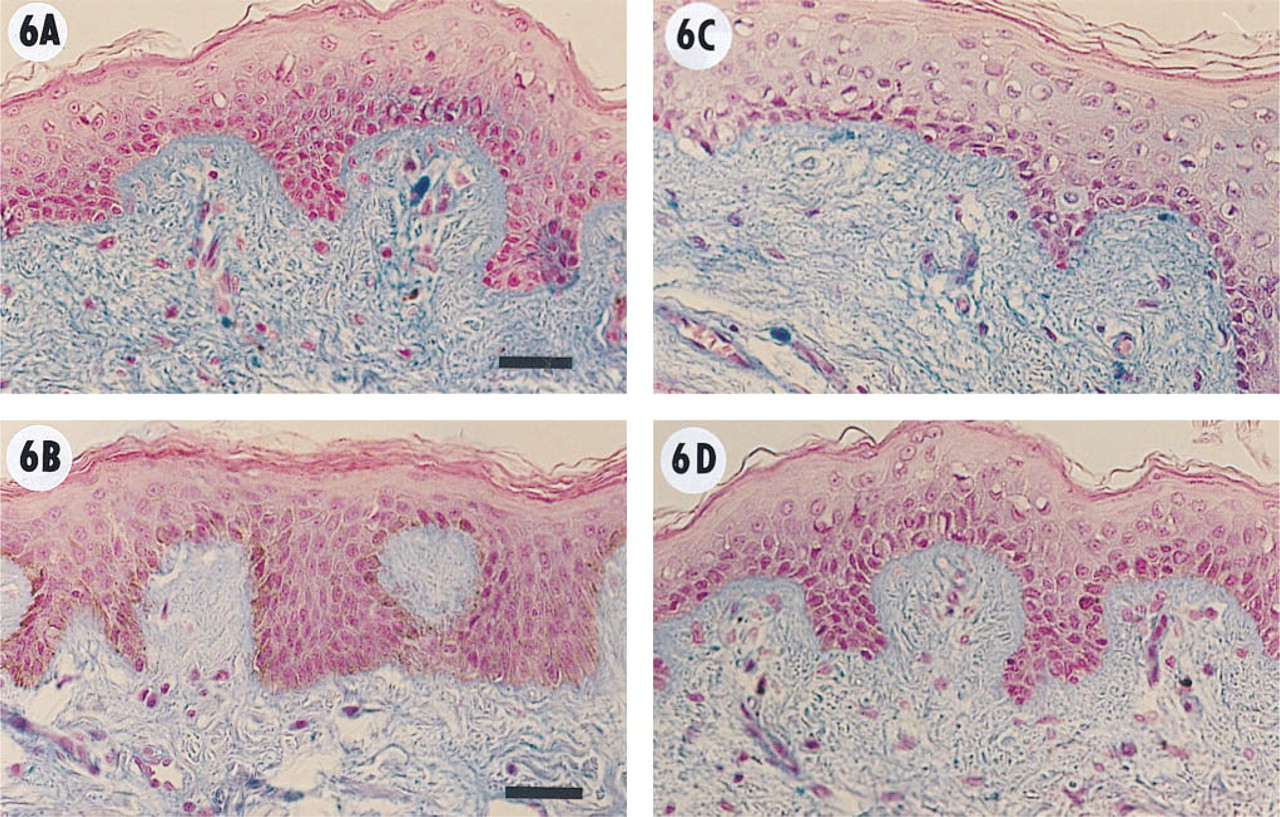
Histochemical staining of GAGs in human skin using Alcian blue staining at pH 2.5 as described in Materials and Methods. The slides were then counterstained with Nuclear Fast Red solution. (
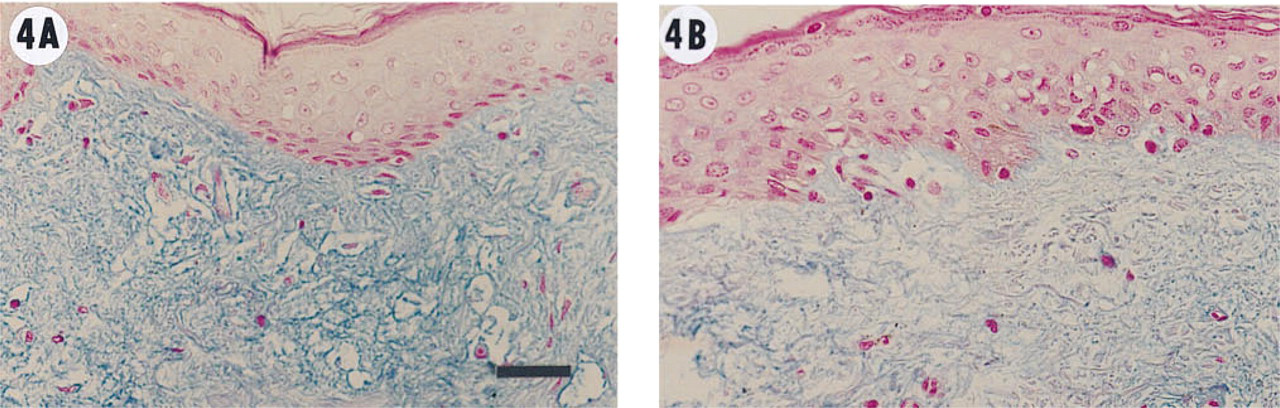
Histochemical staining of GAGs in human skin using Alcian blue after preincubation with PBS at 37C for 24 hr before staining with Alcian blue as described in Materials and Methods and in the legend to Figure 3. (
Results
In this study, HA staining in skin was found predominantly in the dermis, rather than in the epidermis, particularly in the papillary dermis (Figure 1). The most intense staining was observed in sections fixed with acid-formalin/ethanol (Figure 1A) compared to sections fixed with conventional neutral-buffered formalin (Figure 1B). Of particular interest is that small scattered foci of staining in the epidermal layer were comparable to the intensity of staining found in the dermis using acid-formalin/ethanol (Figure 1A). Such foci in the epidermal layer stained less intensely in conventionally fixed samples (Figure 1B). The staining for HA was blocked by preincubation of the HABP with HA. In addition, preincubation of the HABP with other GAGs such as chondroitin sulfate, dermatan sulfate, and keratan sulfate at the same concentration did not decrease the intensity of subsequent HA staining (data not shown). These results demonstrated that the HABP staining reaction was highly specific for HA and did not react with other tissue GAGs.
To confirm further that the HA in skin fixed in acid–formalin/ethanol was better preserved than in neutral-buffered formalin, one set of slides was incubated with PBS overnight before the staining reaction. As shown in Figure 2, approximately 80–90% of HA was retained in slides fixed in acid–formalin/ethanol (Figure 2A) compared to sections fixed in neutral-buffered formalin. Notably, the staining of the epidermis was almost unchanged. However, much of the stainable HA in the dermis had leeched out of the sample fixed with neutral formalin during the overnight incubation in PBS (Figure 2B). Therefore, tissue fixed in acid–formalin/ethanol retained HA far better than that fixed in neutral-buffered formalin.
An artifact became evident in the course of these studies. In the acid–formalin/ethanol-fixed sections (Figure 1A), HA staining was most prominent in the upper spinous and granular layers of the epidermis. In the conventional formalin-fixed section, however (Figure 1B), the converse was true. The basal and spinous layers of the epithelium had the most pronounced HA staining, with little staining observed in the outer granular layers. A plausible interpretation of this apparent inversion artifact may be the following. The HA moieties of the outer spinous and granular layers are more loosely associated, whereas the HA of the basal and inferior portions of the spinous layer are more firmly tethered to tissue structures. The aqueous formalin solution is able to dissolve and elute out the HA of the outer epidermal layers, whereas the HA associated with inferior layers of the epidermis are less soluble and thus more resistant to being leeched out.
Alcian blue, a classical histochemical cationic dye, is reputed to stain HA as well as other acidic GAGs. Staining of both HA and the sulfated GAGs is assumed to occur at pH 2.5, whereas preferential staining of the sulfated GAGs occurs at pH 0.5 to 1.0. When sections were stained with Alcian blue at pH 2.5, slightly more intense staining occurred in sections fixed with the acid–formalin/ethanol (Figure 3A) compared to sections fixed in the standard neutral-buffered formalin (Figure 3B). Preincubation with PBS did not cause an appreciable decrease in the intensity of staining in sections using either fixative (Figures 4A and 4B). This suggests that Alcian blue actually stains predominantly the sulfated GAGs and does not stain HA appreciably in the presence of the tissue-fixed sulfated GAGs.
Histochemical staining of human skin for HA using the HABP as described in Figure 1. (
Histochemical staining of human skin with Alcian blue as described in Figure 3. (
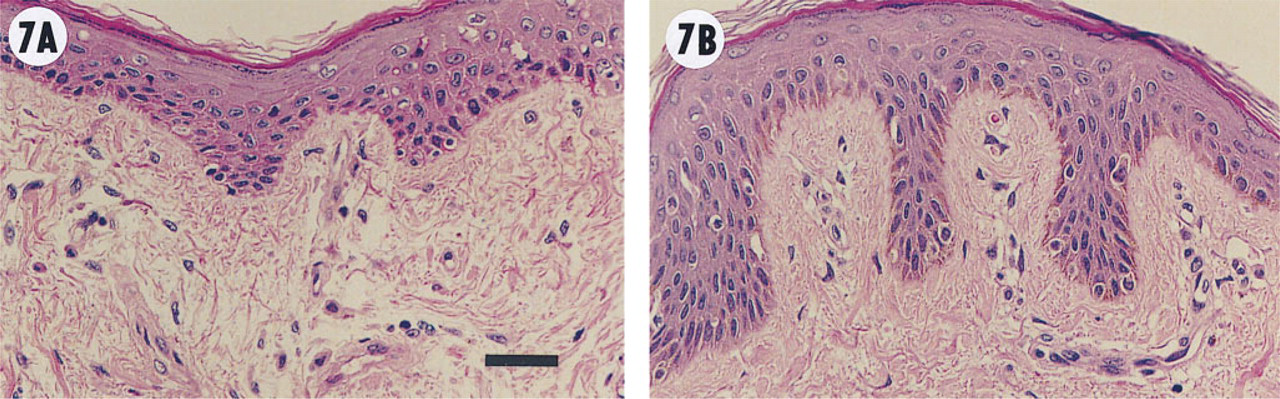
Histochemical staining of human skin using conventional hematoxylin and eosin. (
This phenomenon was investigated further. Sections were preincubated with Streptomyces hyaluronidase and the staining was then compared. In both acid–formalin/alcohol- and formalin-fixed sections (Figures 5A and 5C), all staining disappeared after hyaluronidase predigestion (Figures 5B and 5D). However, with Alcian blue staining (Figures 6A and 6C), only a slight decrease in staining intensity was observed after hyaluronidase predigestion (Figures 6B and 6D).
Finally, we examined for possible artifacts introduced with acid–formalin/alcohol fixation using conventional H&E staining. As shown in Figure 7A, the collagenous fibers of the dermis appear contracted, leaving spaces between fibers, compared to the dermal collagen in the formalin-fixed section (Figure 7B). However, structural preservation and cellular detail otherwise appear comparable between the two methods of fixation.
Discussion
Our results demonstrate that fixation modulates the apparent distribution of HA in human skin. It appears that the acid–formalin/ethanol preserves HA in skin far better than the neutral formalin in PBS and may generally be the fixative of choice for the evaluation of HA in tissues. Formalin crosslinks amino groups of proteins to form methylene bridges. Hyaluronan does not contain such free amino groups but does have – NHCH3 moieties. We have observed that acid–formalin/ethanol solidifies a 1% HA solution, generating a semisolid gel (unpublished observation). This phenomenon was not observed with either 70% ethanol or 5% acetic acid alone or with the neutral-buffered formalin. Furthermore, the semisolid gel remained insoluble during overnight incubation in PBS. Although it is unlikely that formalin crosslinks HA, in the presence of 70% ethanol and 5% acetic acid the formalin appears to modify the structure of HA so that it binds to tissue components in a noncovalent manner. This aggregation or binding is relatively water-insoluble. Staskus and Johnson (1988) describe formation of a double-stranded structure for HA at low pH in the presence of ethanol. Their observations may explain in part the changes in structure of HA that promote tissue binding.
Most other GAGs in the ECM are covalently bound to structural proteins to form proteoglycans. In contrast, HA is generally not covalently bound to protein, although exceptions have been described (Yoneda et al. 1990; Chen et al. 1996). Because of its huge molecular mass, HA is gel-forming and is present in both free and tissue-bound forms (Laurent et al. 1981; Laurent and Fraser 1986; Yoneda et al. 1990). Instead of covalent protein links, HA is decorated with a myriad of binding proteins, termed hyaladherins (Toole 1990; Knudson and Knudson 1993). Such physical and biochemical differences between HA and other GAGs may explain the observations made in the present study. Formalin causes crosslinking of proteins during fixation. Other GAGs are fixed as a result of their covalent binding to proteoglycan core proteins. However, the free form of HA apparently diffuses slowly into the fixation solution during the process. Formalin in the presence of ethanol and acid is able to hinder this diffusion.
Hyluronan and its receptors are taking on increasing importance in biology (Laurent and Fraser 1992), being involved in such basic processes as carcinogenesis (Pauli and Knudson 1988), embryogenesis (Toole 1991), and wound healing and inflammation (Weigel et al. 1986). A wide range of histochemical staining patterns for HA can be obtained as a result of various fixation techniques, making it difficult to compare results reported by different laboratories. A standardized fixation method for studying the distribution of HA in human tissues is recommended. The acid-formalin/ethanol fixative appears to be the method of choice. Moreover, the classic histochemical assumption that it is possible to estimate HA content of tissues by contrasting Alcian blue staining intensity at pH 2.5 with that at pH 0.5 or 1.0 should be reevaluated.
Footnotes
Acknowledgements
Supported by Hyal Pharmaceutical Corp., Ontario, Canada, and by a DHHS grant from the US National Institutes of Health (GM46765).