
Abstract
Forty-six advanced-stage human breast carcinoma specimens were evaluated by immunohistochemistry for PKCα expression and compared with 25 samples of normal adjacent breast tissue. For normal tissue, the median staining of ductal epithelia was of moderate intensity. No staining was observed for 67% of tumor specimens, and only 4% showed intensities greater than the median observed in normal tissue. Faint to moderate PKCα staining was observed in the stroma, inflammatory cells, and fibroblasts of tumors but was absent in normal tissue. These findings demonstrate that downregulation of PKCα protein occurs in epithelial cells of advanced breast tumors (p<0.001).
Keywords
P
Because of a lack of suitable antibodies for immunohistochemistry (IHC), early efforts to elucidate the role of a PKC isoform in human tumors were limited to assay of whole tumor extracts either by PKC catalytic activity or isoform abundance by Western blotting (O'Brian et al. 1989). This approach does not recognize the complex organization of a tissue that includes several cell types: epithelia, stroma, fibroblasts, inflammatory cells, smooth muscle cells, endothelium, and nerve cells (Masso-Welch et al. 2000). Recently, isoform-specific antibodies that perform well in paraffin-embedded material have greatly improved detection and analysis of the expression and localization of a single PKC isoform in different cell types of the intact tissue. In this regard, decreased expression of the novel isoform PKCη was observed in invasive breast tumors (Masso-Welch et al. 2001). In view of the complexity of breast tissue, the use of immunochemical methods that preserve the heterogeneous organization of cells in breast specimens can yield detailed and coherent results that clarify the clinical significance of PKC isoforms in breast cancer progression. Here we present an IHC method by which advanced-stage human breast carcinomas and normal breast tissue can be successfully compared for PKCα expression.
The specimens used for this study were collected under an IRB approved protocol (IMP024) such that the specimen could not be linked to the human subject and was considered exempt from 21 CFR parts 50 and 56, requiring no Subject Informed Consent.
A titration analysis was conducted with the PKCα antibody (clone H-7, mouse IgG1) (Santa Cruz Biotechnology; Santa Cruz, CA) to determine the minimal concentration of antibody that generated the maximal specific staining intensity while not causing significant background staining with the murine IgG1 isotype-matched control antibody (Sigma-Aldrich; St Louis, MO). In pilot experiments with kidney as the positive control tissue and serial dilutions of PKCα antibody (1.25–20 μg/ml), a concentration of 5 μg/ml was judged to be optimal because it produced strong staining in the distal tubule, whereas the same concentration of murine isotype-matched negative control antibody produced no significant background staining. Western blotting analysis (not shown) demonstrated that the PKCα antibody showed no crossreactivity with recombinant proteins standards corresponding to other PKC isoforms (βI, βII, γ, δ, ∊, η, theta;, and ≃) (Pan-Vera; Madison, WI).
IHC studies with formalin-fixed, paraffin-embedded breast tumor specimens were performed using the Envision+ Kit (DAKO; Carpinteria, CA). Unless otherwise indicated, all reagents were provided in this kit. Specimens were sectioned at 5 μm and applied to positively charged glass slides, where they were depar-affinized with xylene, rehydrated through a series of graded alcohols, and then rinsed with PBS. For epitope retrieval, slides were placed in sodium citrate buffer, pH 6.0 in a 95–99C water bath for 40 min, cooled at room temperature (RT) for 20 min, and then washed three times for 5 min in PBS. (Relative to other methods, the heat-induced method gave the best combination of morphological preservation and staining intensity with normal human kidney distal tubules.) Endogenous peroxidase activity was blocked with a 5-min incubation in hydrogen peroxide solution, followed by three 5-min PBS washes. Specimens were incubated with PKCα antibody (5 μg/ml), or the species- and isotype-matched negative control antibody (Sigma-Aldrich) (5 μg/ml) in DAKO primary antibody diluent for 30 min at RT. The slides were washed three times in PBS and incubated with a polymer conjugated to horseradish peroxidase for 30 min at RT. After three additional PBS washes, the peroxidase reaction was visualized by incubation for 5 min with 3,3′-diaminobenzidine tetrahydrochloride solution. Tissue sections were thoroughly washed with tapwater, counterstained with Mayer's hematoxylin solution (American Master∗Tech Scientific; Lodi, CA) dipped in 0.25% acid alcohol, blued in 0.2% ammonia, dehydrated through graded alcohols, cleared in xylene, and coverslipped.
IHC of PKCα expression in normal adjacent breast tissue (
Interpretation of stained slides was performed by microscopic examination by a board-certified pathologist. The staining intensity of each specimen was judged relative to the intensity of a control slide containing an adjacent section stained with an irrelevant negative control antibody that is matched by species and isotype to the specimen. Staining of the section labeled with the negative reagent control was considered background. A score of zero indicated no staining relative to background, 1+ = weak staining, 2+ = moderate staining, and 3+ = strong staining. According to standard pathology practice, staining intensity was reported at the highest level of intensity observed in all tissue elements, except the distinctive tissue element for which an expanded scoring scheme was reported.
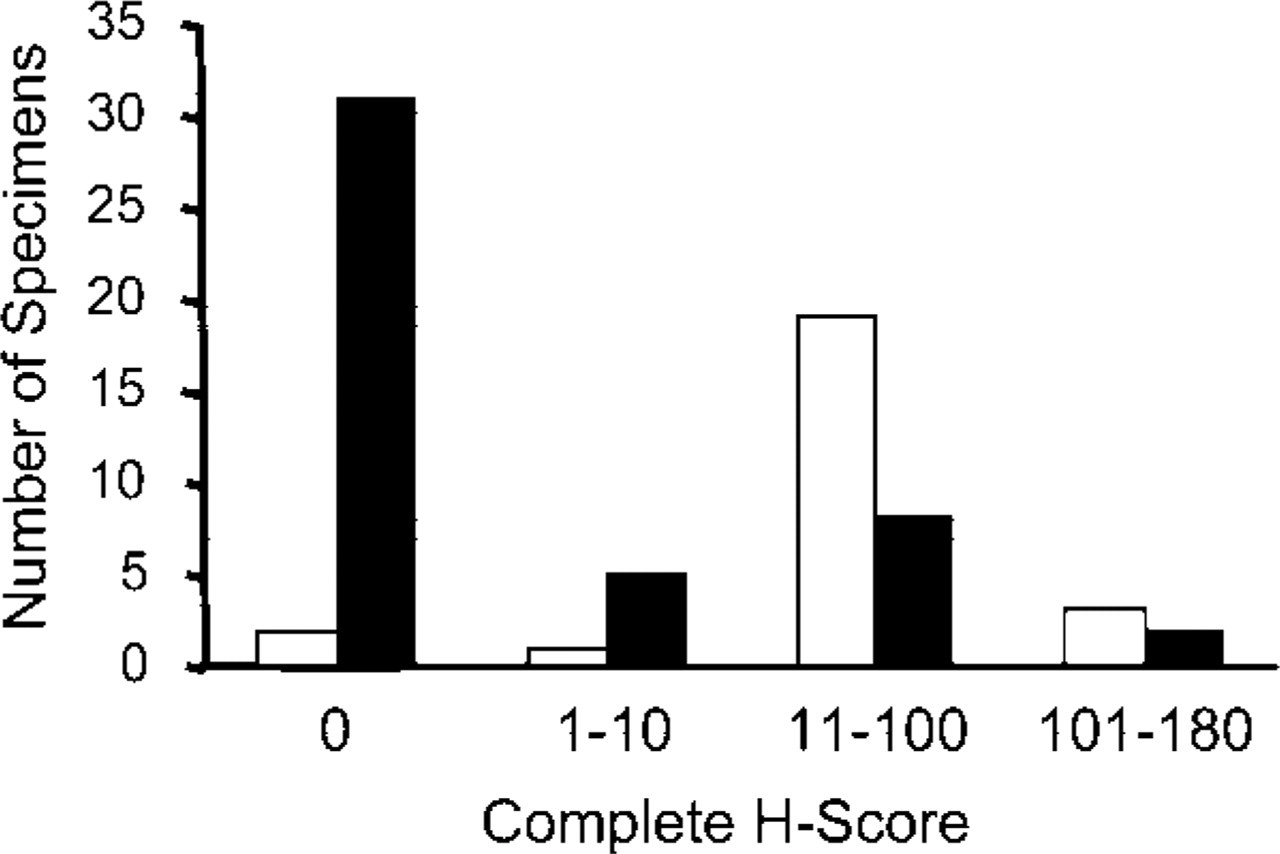
Compiled expression levels of PKCα in normal human breast and tumor specimens. The complete H-scores from Figure 1 that correspond to immunochemically detected PKCα in normal breast tissue samples (white bars) are compared with the complete H-scores obtained with invasive human carcinomas (black bars).
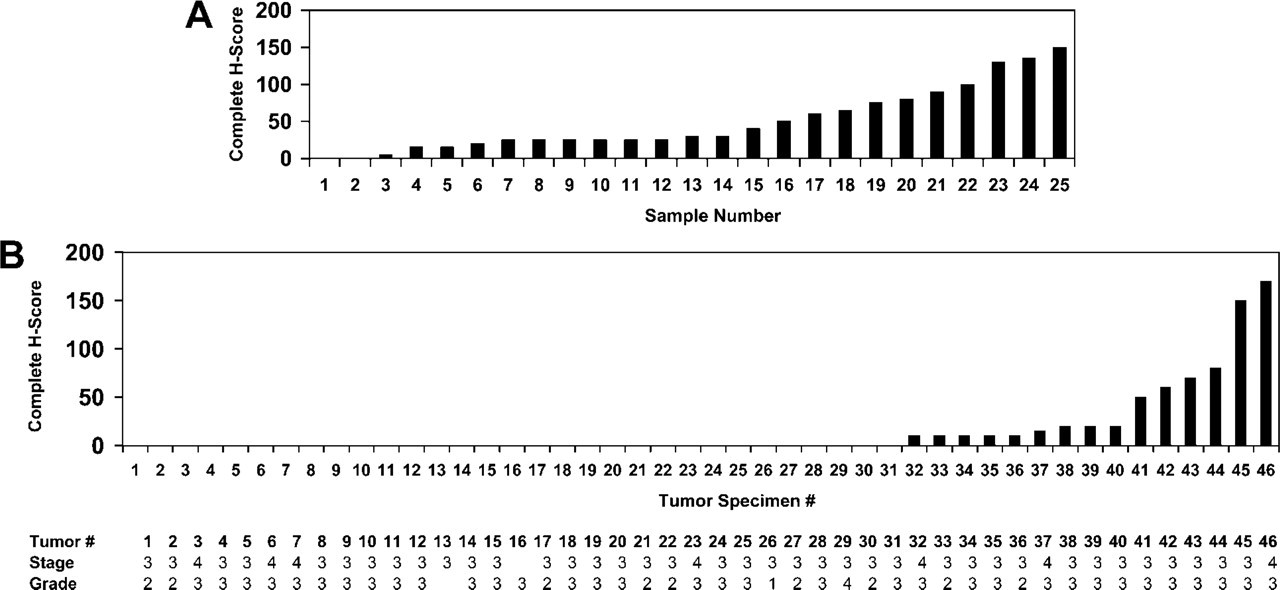
For comparison of staining among tissues, the results were quantified by calculation of a complete H-score that considers both staining intensity and the percentage of cells stained at a specific range of intensities. A complete H-score was calculated by summing the products of the percentage cells stained at a given staining intensity (0–100) and the staining intensity (0–3). For example: a specimen with 10% of cells staining 3 +, 30% of cells staining 2 +, 20% of cells staining 1 +, and 40% of cells unstained would have a complete H-score of (3 × 10) + (2 × 30) + (1 × 20) = 110. Statistical analysis of the complete H-scores obtained for the normal tissue and tumor sample populations was carried out by using the two-tailed Student's t-test with unpaired data of equal variance.
Forty-six advanced-stage human breast carcinoma specimens and 25 histologically normal samples of normal adjacent human breast tissue from anonymous female donors were analyzed. The cancer specimens were either stage III or IV, signifying that the underlying disease had advanced into the lymph nodes and/or distal tissues, and were mostly either grade 2 or 3 (moderately or poorly differentiated, respectively). Only one tumor (#29) was grade 4 (undifferentiated).
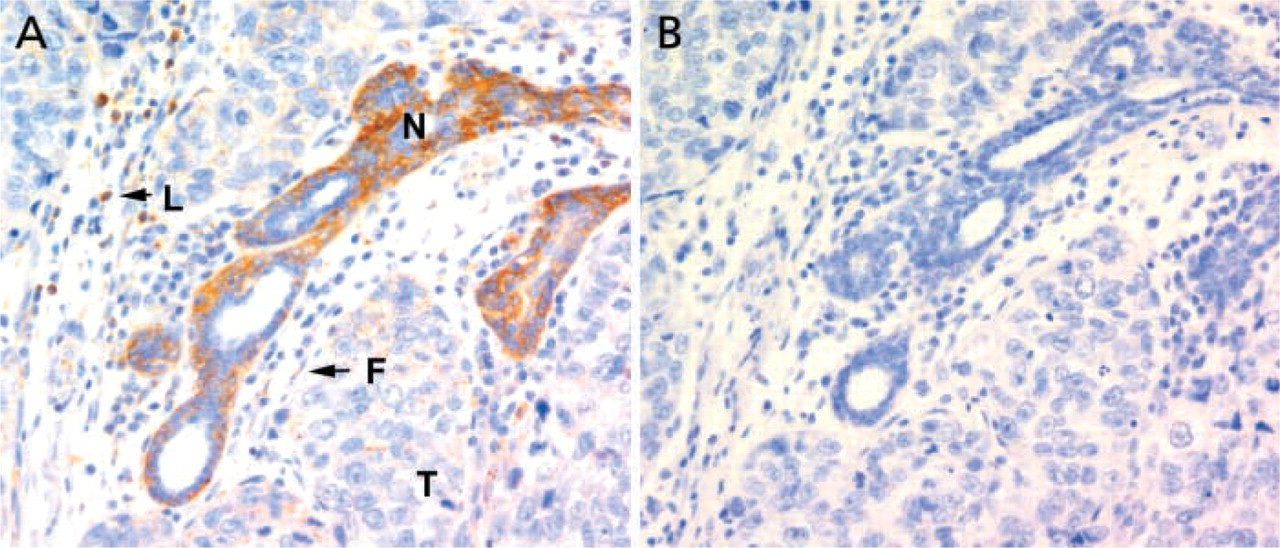
Histology of PKCα expression in tumor specimens. PKCα immunohistochemistry (
Summary of PKCα staining intensity in normal breast tissue and tumors a
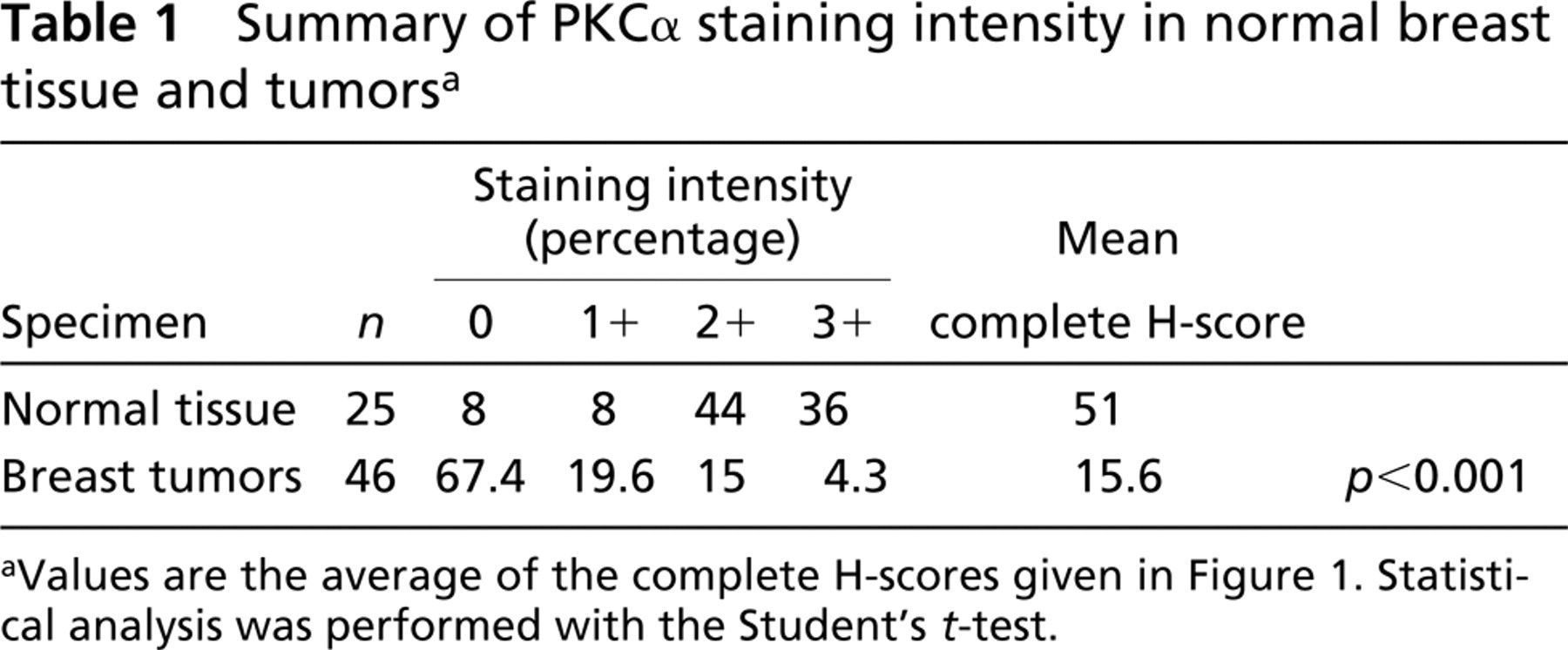
aValues are the average of the complete H-scores given in Figure 1. Statistical analysis was performed with the Student's t-test.
The staining intensities of human breast tumors and normal breast tissue specimens are presented in Figure 1. Of the normal breast specimens, 92% exhibited detectable PKCα in epithelial cells, where the median staining intensity was 2 +. Calculation of the complete H-score for each sample yielded values in the range of 10–100 for 44% of normal tissue samples (Figures 1A and 2) and produced an average complete H-score of 51 (Table 1). These results were in sharp contrast to the values obtained for human breast tumors (Figure 1B), of which 67.4% gave an epithelial cell staining intensity of zero (Figures 1B and 2), thereby yielding a much lower average complete H-score of 15.6 (p<0.001). Of this population of tumor specimens, only 4% (tumors 45 and 46) exhibited PKCα staining intensities of 3+ of the ductal epithelia, whereas 36% of normal breast specimens displayed 3+ staining.
In a sample representing this differential staining, Figure 3A shows epithelial staining of normal adjacent breast tissue (identified by the dark brown staining) that was apparent in almost half of the tumor specimens. Comparison of staining patterns obtained with a species and isotype-matched control antibody run at the same concentration (Figure 3B) indicated that the signal was not due to nonspecific interactions. Other cell types in tumors that acquired faint to moderate staining activity or showed increased staining intensities relative to normal tissue, included inflammatory cells (leukocytes), fibroblasts, smooth muscle cells, nerve cells, and the stroma. For both tumor and normal tissues, there was zero staining of the vascular endothelium.
The very low frequency of PKCα protein observed in breast tumors is similar to the decrease in PKCα with increasing histopathological grade that was recently reported for ovarian carcinomas (Weichert et al. 2003). An attractive hypothesis suggested by our results is that during or preceding late-stage breast disease, PKCα is subjected to complete proteolysis. Evidence of PKC downregulation was previously noted in primary cultures of explanted advanced mammary carcinomas (Regenass et al. 1989), in which 6/7 carcinomas exhibited decreased Ca2+-dependent PKC activity compared with the nonmetastatic MCF-7 cell line. Thus, ex vivo cultures or established cell lines that exhibit absence of PKCα may offer a proper intracellular setting for studies aimed at late-stage breast disease. Further analysis of PKCα expression at earlier stages will define the interval during which PKCα protein is subject to downregulation.
Footnotes
Acknowledgements
Supported in part by a grant from NIH (CA 91341).