
Abstract
Germ-cell tumors are the most common malignant neoplasms of the testis. Seminomatous and non-seminomatous tumors must be differentiated because the treatment and the prognosis are different. In light microscopic examination, seminoma may sometimes be difficult to distinguish from the solid pattern of embryonal carcinoma (EC). Although studies have shown that CD30 was a good marker of embryonal carcinoma and that c-kit was regularly expressed in seminoma, none has described the value of CD30 and CD117 (c-kit) in combination for the differential diagnosis between EC and seminoma. We selected 25 pure seminomas, seven pure ECs, and seven mixed germ-cell tumors composed of seminoma and EC from our archives and studied their immunoreactivity for CD30 and CD117. We observed that 27/35 seminomas were CD117+/CD30-; none of the seminoma was CD117-/CD30+. Conversely, 11/14 ECs were CD30+/CD117- and none was CD30-/CD117+. Our findings suggest that CD117 and CD30 immunohistochemistry used in combination represents a valuable tool for distinguishing seminoma from EC.
GERM-CELL TUMORS are the most common malignant neoplasms of the testis. Seminoma constitutes 35–50% of all germ-cell tumors (Ulbright et al. 1999). Usually, seminomatous cells are easily recognized with routine stains. However, when the fixation is not adequate, seminoma may be confused with the solid pattern of embryonal carcinoma (EC) (Ulbright et al. 1999). The distinction between seminoma and EC is very important because the treatment differs. Seminoma confined to the testis is treated by orchiectomy and radiation therapy to pelvic lymph nodes. After orchiectomy, EC requires a retroperitoneal lymph node dissection or chemotherapy (Parkinson et al. 2001). Immunohistochemistry (IHC) has been proposed as an aid to diagnosis. Initially, cytokeratin expression was reported as rare and weak in seminoma and frequent and diffuse in EC. However, several studies have demonstrated that cytokeratins are expressed in many seminomas (30–40% of cases) (Fogel et al. 1990; Denk et al. 1987; Cheville et al. 2000). CD30 is a member of the tumor necrosis factor (TNF) superfamily and is expressed on the surface cells of EC but very rarely in seminomas (Hittmair et al. 1996; Pallesen and Hamilton-Dutoit 1988; Pera et al. 1998).
Proto-oncogene c-kit encodes a surface membrane tyrosine kinase receptor that is required in normal spermatogenesis. C-kit is regularly expressed in seminoma but rarely in non-seminomatous germ-cell tumors. KIT signal transduction appears to be an important pathway for carcinogenesis of seminoma (Izquierdo et al. 1995). In this study we investigated the combined value of CD30 and CD117 (c-kit) to differentiate EC from seminoma.
Formalin-fixed, paraffin-embedded tissue from 25 pure seminomas, seven pure ECs, and seven mixed germ-cell tumors composed of EC and seminoma were selected from the files of the Department of Pathology, Lille University hospitals. All slides and pathological reports were reviewed for diagnosis. Immunohistochemistry (IHC) was conducted on 4-μm-thick paraffin sections using an automated immunostainer (ES; Ventana Medical Systems, Strasbourg, France). After deparaffinization, IHC was performed using a three-step undirected process based on the streptavidin-biotin complex. The primary antibodies used were CD30 (1:40, BerH2; Dako, Glostrup, Denmark), CD117 (1:50, Dako). Pressure cooker pretreatment in citrate buffer (pH 6.0) was performed for 1 min 30 sec. Endogenous peroxidase activity was suppressed by first incubating the specimen in 3% hydrogen peroxide. Slides were counterstained with hematoxylin. Positive and negative controls were added to each automated immuno-histochemistry run. Negative controls consisted of slides run without the primary antibody. Mast cells were used as internal positive control for CD117 and an anaplastic large-cell lymphoma as positive control for CD30.
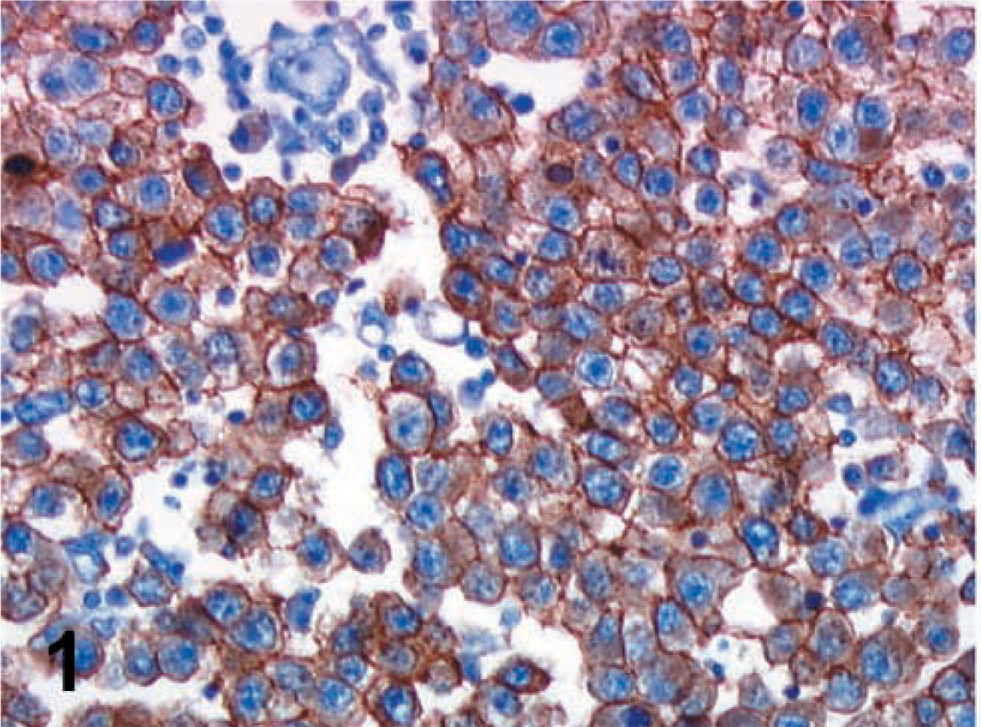
Strong immunostaining for CD117, showing a membranous pattern in a seminoma. Original magnification × 400.
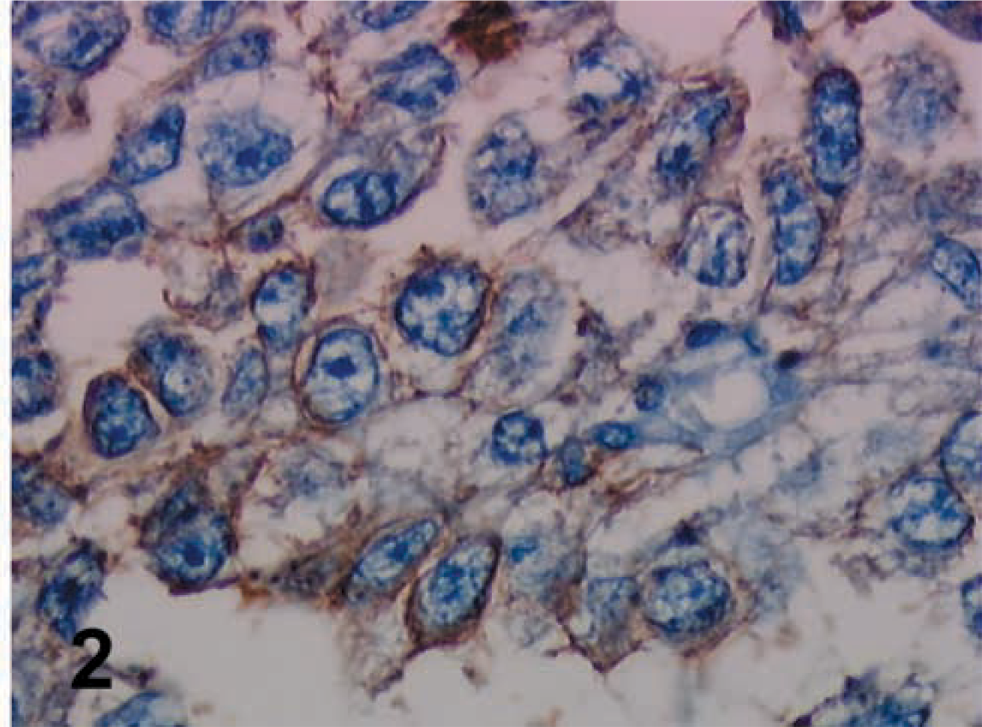
Embryonal carcinoma. CD30 showing diffuse membranous positivity. Original magnification × 400.
Immunostaining was evaluated by two pathologists (XL, DA) by determining the percentage of positively staining cells as follows: 0, no staining; +, 1–10% of staining cells; ++, 11–50% of staining cells; +++, >50% of staining cells.
Of the seminomatous tumors, 23/25 pure seminomas were stained with antibody to CD117. The staining was often intense and diffuse with a membranous pattern (Figure 1). Six of seven seminomatous components in mixed germ-cell tumors were also stained with CD117. CD30 was positive in one pure seminoma; the staining was moderate and focal (less than 10% of tumor cells). Few seminomatous cells were also CD30-positive in one mixed germ cell tumor. A total of 27 seminomas were CD117+/CD30-, three seminomas were CD117-/CD30-, two seminomas were CD117+/CD30+, and none was CD117-/CD30+.
Of the embryonal carcinomas, 6/7 pure ECs were positive for CD30 and 6/7 ECs in mixed germ-cell tumors were positive for CD30 (Figure 2). The staining was membranous and diffuse in the great majority, but in four cases the staining was weak and focal. All tumors except one were negative with CD117.
A total of 11 ECs were CD30+/CD117-, two were CD30-/CD117-, one case was CD30+/CD117+, and none was CD30-/CD117+.
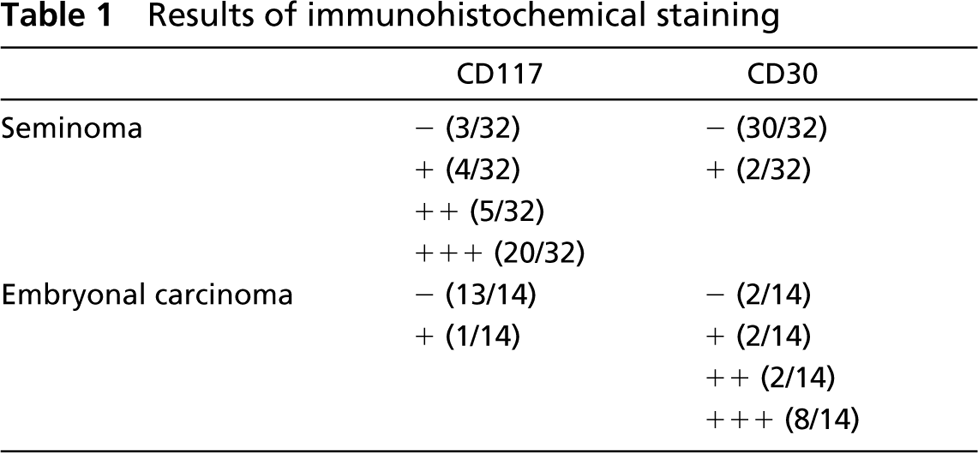
The results of immunohistochemical staining are summarized in Table 1.
Differentiation between seminoma and EC is very important in consideration of the therapeutic approach. Light microscopic examination remains the gold standard for the diagnosis, but in some cases the differential diagnosis between seminoma and the solid pattern of EC may be difficult (Ulbright et al. 1999; Parkinson et al. 2001). Therefore, immunohistochemistry may be helpful. Cytokeratin is generally more expressed in EC than in seminoma. However, in a recent large series studying cytokeratin expression in seminomas, 30–40% of these tumors reacted with various antikeratin antibodies (Cheville et al. 2000). The staining was often focal (less than 10% of cells stained), mainly with CK7. In another study, 19/26 seminomas expressed cytokeratins, and constantly CK8 and CK18 (Fogel et al. 1990). In EC, cytokeratins are often diffusely expressed but rare tumors may be entirely negative (Cheville et al. 2000).
Results of immunohistochemical staining
In 1988, a study about CD30 expression in non-hematopietic tissues showed that CD30 was expressed by EC and not by seminomas (Pallesen and Hamilton-Dutoit 1988). Further studies confirmed that CD30 was a valuable marker of EC (Ferreiro 1994). But, again, rare ECs may be negative and seminomas may be focally positive with CD30 (Hittmair et al. 1996; Pera et al. 1998). This expression of CD30 in seminoma appeared to be always limited to rare foci of tumor cells, which presented the characteristic features of seminomatous cells. In one tumor, the seminomatous cells were stained both with cytokeratin and CD30 (Hittmair et al. 1996).
In searching in the literature for a positive marker of seminoma, we find that c-kit (CD117) was regularly expressed in seminomatous cells (Izquierdo et al. 1995; Bokemeyer et al. 1996; Kraggerud et al. 1999). Izquierdo et al. (1995) reported a diffuse membranous positivity of c-kit in 28/28 seminomas. In 32% of nonseminomatous germ cell tumors of the series, a focal cytoplasmic staining in occasional cells was observed without membranous reactivity. Kraggerud et al. (1999) showed that all classical seminomas tested in their work were c-kit-positive (22/22) but that some spermatocytic seminomas (7/17) were also stained. Our study is the first to investigate the combined value of immunohistochemical detection of CD30 and c-kit. We demonstrated that no ECs showed a phenotype of CD30-/CD117+ and that no seminoma had a phenotype of CD30+/CD117-. We observed that a phenotype of CD30-/CD117+ was very suggestive of seminoma and that a phenotype of CD30+/CD117- was very evocative of EC.
In conclusion, we suggest that CD30 and CD117, used in combination, are helpful for the differential diagnosis between EC and seminoma.