
Abstract
This study explores substitute addictions – the immediate or gradual replacement of an addiction or set of addictions that have been stopped or reduced by engaging with another addictive behavior – as a central concern in treatment-assisted recovery. Questionnaires were administered to 85 substance use disorder treatment professionals across 20 U.S. states, with qualitative items eliciting their views on why another addiction might replace the substance use disorder being treated; whether and how the facility educates service users about substitute addictions; how substitute addictions may help or hurt service users’ recovery efforts, and assessed general recommendations for addressing substitute addictions. Thematic analysis yielded three themes: (i) substitutes supporting recovery, (ii) substitutes precipitating relapse or worse quality of life, and (iii) treatment of substitute addictions. Given the high rates of post-treatment relapse, we make important strides in addressing treatment professionals’ rarely examined first-hand experiences, to inform service delivery.
“Addiction is a disease with many potential faces, including, but not limited to, alcohol and other drugs” Fenley (2012), p. 71
Substitute addictions—the instantaneous or progressive replacement of an addiction or cluster of addictions that have been stopped, by another addictive behavior (Sussman et al., 2024; Sinclair et al., 2021)—are a central concern in addiction recovery with implications for service user well-being and long-term substance use treatment outcomes. Substitutes may arise at any stage of the recovery journey, commencing, recommencing, or escalating in frequency and/or intensity following resolution of a substance use disorder (SUD) (Sussman et al., 2024; Sinclair, 2022; White & Kurtz, 2006). Substitutes may include substance-to-substance substitution (e.g., crystal methamphetamine being replaced with cannabis), substance-to-behavior substitution (e.g., alcohol being replaced with gambling), behavior-to-substance (e.g., gambling being replaced with alcohol), and behavior-to-behavior substitution (e.g., exercise being replaced with shopping) (Sinclair et al., 2021). Motives for substitution may include conscious instrumental use of time and boredom; enjoyment and upliftment; (re)connection and social acceptance; guilt and emotional regulation, expectancies and experience, and forced abstinence or availability and accessibility (Shapira et al., 2021; Sinclair et al., 2021). Substitutes are also engaged through unconscious or automatic processes, being influenced or triggered by others, or because of treatment-related continuity, meaning the substitute was introduced or engaged in during treatment and endured thereafter (Sinclair et al., 2021). Substitutes potentially function to facilitate recovery (Horvath, 2006), heighten relapse risk, or signal impending relapse (Chiauzzi, 1991; Melemis, 2015; Rasmussen, 2015; Selby, 1993). The evidence suggests that both kinds of outcomes occur. Understanding more about providers’ perceptions regarding differentiating these outcomes as early as possible is one of the aims of this study.
Substitutes are relatively under-researched (e.g., Sussman et al., 2024; Kim et al., 2021; Sinclair et al., 2021), and the clinical insights of substance use treatment professionals are especially underrepresented (see Sinclair et al., 2024). Treatment service users with SUDs often shift to substitute addictions to activate or reactivate the brain reward pathways that the original addiction or set of addictions did (Doweiko, 2018). Treatment professionals work closely with service users and are likely to be the first to observe signs of substitution; substitutes may be negatively consequential to the treatment and overall health of those in recovery. Professionals’ insights are valuable given their education and training, clinical experience, and exposure, and they stand to offer critical insights into the dynamics of substitutes. Given evidence that substitutes are associated with poorer treatment outcomes (Kim et al., 2021), treatment professionals should screen and assess for substitutes to further help the service user develop coping mechanisms, alternative coping plans and skills, and identify high-risk situations and how to manage substitutes. Such assessments can lead to further understanding why they may arise, their likely trajectory, and what current practices are (and the problems with these practices). Simultaneously, research with treatment professionals can point to gaps in treatment provision and training. Considering that people who relapse may receive treatment at the same facility where they were initially treated, it is vital to ensure that treatment is individualized and that the same approach is not mindlessly employed as during their earlier episode (Doweiko, 2018; Fletcher, 2013). While treatment professionals are not gatekeepers of recovery, they do direct treatment and counselling, support skills training, and facilitate access to medication and various other services (Humphreys, 2015). Yet, previous research on substitute addictions has rarely considered their insights.
The few pioneer studies have primarily focused on quantitative trends (Sinclair et al., 2021), with little qualitative research on how substitute behaviors and addictions are experienced, understood, or navigated by professionals. Qualitative methods afford in-depth insights into processes and patterns of behavior, accounting for ‘hows’ and ‘whys’ by collecting participants’ attitudes, behaviors, and experiences (Tenny et al., 2022). To fill this gap, qualitative survey responses examined how substance use treatment professionals understand, address, and perceive the impact of substitutes in the context of recovery. By centering the voices of treatment professionals, we contribute to a deeper, practice-informed understanding of how substitutes intersect with recovery, to support more responsive, substitute addiction-aware approaches to substance use treatment.
Methods
Data Collection
The survey was administered between June 2023 and August 2024. Recruitment began with cold calls and emails to the administrative offices of the facilities on the Newsweek (weekly news) magazine list. We were then referred to treatment professionals who could report on their respective treatment and referral systems. Additional facilities were recruited via snowball sampling to increase the sample size. Anonymous structured interviews, conducted via Zoom (n = 53), in person (n = 20), or telephonically (n = 12), lasted approximately 30 minutes. As an incentive, participants received a $50 gift card.
Participants
A total of N = 85 SUD treatment professionals participated in the study. The analytic sample included N = 47 participants recruited from Newsweek magazine's rankings of 'America's Best Addiction Treatment Centers 2021' (Newsweek, 2021) and 2023 (Newsweek, 2023) lists (per STATISTA methodology [Statista, 2021] based on accreditation, service quality and reputation), as well as a convenience sample of N = 38 respondents recruited using snowball sampling to increase representativeness and add a non-STATISTA sample. In all, 68 unique treatment facilities across 20 U.S. states were represented. Two interviews were drawn from nine participating facilities (13.2%), while three were recruited from four centers (5.9%).
Survey Instrument
The questionnaire included socio-demographic questions, questions on SUDs, behavioral addictions, and substitute addictions. Sociodemographic variables included the respondent’s position at the facility and length of employment; age; gender; ethnicity; languages spoken other than English; highest level of education, licenses or credentials held, and whether respondents had lived experience of substance use and behavioral addiction. The instrument explored the occurrence of behavioral addictions at the facility (including gambling; electronic/social media including TV, phone, internet; online or offline gaming; exercise; shopping online or offline; sex; love; work or study; tanning/cosmetic modification; hoarding or others), whether treatment is offered for behavioral addictions (which kinds or why they are not), and recommendations for treating behavioral addictions. The section on substitute addictions queried whether the treatment professionals had observed the occurrence of substitutes (yes/no) at their facility (either during or after service users leave the facility). They were also asked to specify which substitutes were most common (open-ended). Thereafter, they were asked to provide reasons why another addiction might replace the primary addiction being treated; whether and how the facility educates service users about substitute addictions; how substitutes may help or hurt service users’ recovery efforts; and recommendations for addressing substitutes (open-ended).
Data Analysis
The research team members have psychology and public health backgrounds, and this diversity in perspectives shaped data interpretation. The analysis process commenced with repeated reading of the text to achieve data familiarization. The following questions were coded and included in the analysis: ‘In your opinion, why might another addiction replace the primary addiction being treated?’; ‘Does your facility educate service users/clientele about substitute addictions’ (with examples provided)?; ‘In what ways might substitute addictions help or hurt service users’/clientele’s recovery efforts?’ and ‘If you could make any recommendations for addressing substitute addictions, what would they be (either substance or behavior substitutes)?’
Codes were not imposed a priori, but rather developed inductively. Regular coding meetings enabled reflections on assumptions, biases, and first-hand insights from data collection, all of which informed coding and theme development. After developing and refining a codebook, and to minimize bias, the data were coded by multiple members of the research team. A team of three researchers coded the data independently and identified patterns in the direct quotes. We identified all the data relevant to the patterns and organized recurring elements into sub-themes. We integrated sub-themes into overarching themes, forming theme statements and constructing a storyline. Through dialogue and negotiation, disagreements informed the refinement of codes and themes (Aronson, 1995). All discrepancies in coding were resolved through discussion among all researchers until full consensus was reached (100% agreement).
Findings
Participant Characteristics
The study sample (n = 85) consisted of 52 females (61.2%) with a mean age of 46.3 years (SD = 1.4 years). Most respondents (n = 59, 69.4%) were non-Hispanic White and had a master’s degree as their highest level of education (n = 40, 47.1%). The mean length of employment for treatment professionals was 8.0 years (SD = 7.8). More than half of the respondents (n = 45, 52.9%) had a personal history of SUD, while 27 (31.8%) reported a history of behavioral addiction.
While presented as distinct, the identified themes are deeply interwoven, reflecting the complex nature of substitute addictions (see Figure 1). Thematic Category 1 explores how substitution may support recovery. It includes (a) making recovery more manageable and (b) substitutes as harm reduction/healthier behaviors. Category 2 focuses on substitution in relation to relapse and worse quality of life, including: (a) relapse; (b) poor long-term outcomes; (c) underlying issues unaddressed; (d) new addictions/inhibits skills building; (e) a temporary solution; (f) lack of coping/maladaptive coping; (g) positive reinforcement, and (h) negative reinforcement. Category 3 examines treatment for substitute addictions, comprised of (a) current treatment responses, which include recovery groups/group therapy; individual therapy; guest speakers/psychoeducational lectures; print curriculum, and videos. Category 3 also addressed (b) respondents’ recommendations, namely a need for treatment/education/training, the importance of spirituality/religion/12-step groups, and the need for research. Summary of themes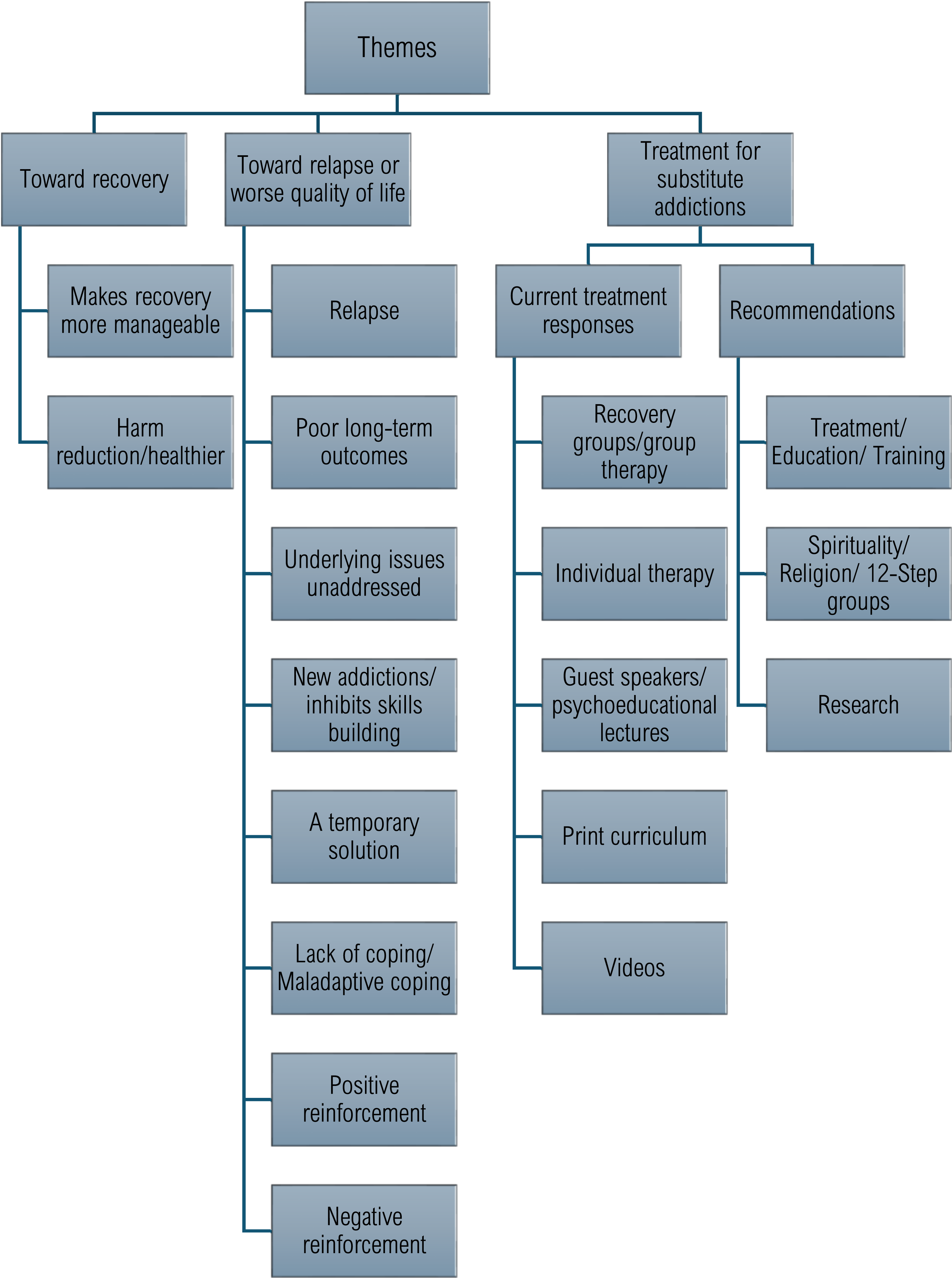
Toward Recovery
“Better for someone to play video games for hours instead of drinking alcohol for hours; behavioral addiction may be better than substance addiction, but not effective long term.” “Most of the time, to change the way they feel and what is perceived to be safer than what they were initially being treated for. If someone comes in with fentanyl addiction and they don't want to go back to another substance, they will turn to sex or love ... or work, which is seen as ‘safer’ and a lot of times they lack the education on the consequences or where that can take them.” “Help: would definitely be if it’s not a bad addiction like gambling, and if it's pro recovery that doesn't kill or hurt you. No one will OD knitting a sweater, but the downside is what if it's something that requires purchase and it’s not available or attainable?” “It really doesn’t matter what substance they use. I subscribe to harm reduction, although our facility is abstinence-based. If you use a substance for another substance, it mostly causes problems down the line. Harm reduction is not something I would recommend, but if a client comes to treatment and doesn't want to stop but just cut down, I think they should be allowed to try it rather than risking the severing of the relationship because of abstinence only.” “I think it depends on what they are subbing. Long term, if they are addicted to food, they become unhealthy and unhappy. Shopping can cause financial distress. If they can get help simultaneously with the primary, it might not be problematic.” “It depends on the person. Something that could be harmful to one person, like the gym, could be supportive to others, people will use the gym or healthy eating due to their body dysmorphia, and it becomes a compulsion, but sometimes it could help their life out, and others to destroy themselves.” “It might hurt - they can relapse, might help - could keep the person sober for a while, but it is not 'good'.” “It may serve a harm reduction aspect, but overall, addiction is addiction.” “Obviously, if they’re doing heroin and now they're just drinking a lot of coffee with sugar, it's less dangerous than heroin, but they could develop other conditions, such as diabetes, that would become more dangerous long term.” “If you can develop a healthy substitute addiction, it could be a godsend and life-saving for many people. Like if someone quits meth for the gym I think that's life-saving.” “It's socially acceptable, a person doesn't understand the reward pathway (dopamine) in the brain.”
“Well, from a harm reduction stance, some substitutes are less harmful, so that would be a way as they move towards health to a middle ground.” “It helps if they can find something positive to bond with. Just because the substance or behavior is removed doesn't mean that the addiction goes away, and it's about having and finding a balance.” “Mixed research on this, I see it as if they can relieve some of the pain, they are less likely to relapse, but it depends on the person. It can help them tolerate the discomfort of early recovery long enough for them to get through.” “Gets me thinking about dealing with one demon at a time. We all have addiction in one form or another, like I have my coffee here; we all struggle. The goal is to meet people where they are at and increase their sobriety, in which the individual is wanting to quit, and we encourage that person.” “It fills the void, feels good, if it encourages life balance.” “It can help if mindful about it and the direction is good.” “As long as they are not involved deeply and for a long time, they keep busy (e.g., with work or exercise as a new habit).”
In some instances, the substitute was also considered healthier than the original addiction. In the short term, a behavioral addiction may be preferable to an SUD. As such, substitution for harm reduction could move someone closer to their recovery goal. In addition, it could relieve some of the pain of the primary addiction and thus prevent relapse. Notably, certain substitutes were seen as detrimental (e.g., fentanyl), whereas others were seen as less harmful and supportive of recovery (e.g., work). In this context, certain substitutes may be regarded as the lesser evil. However, for the substitute to serve a harm reduction function, it needed to be used in moderation and not as a replacement for the primary addiction. While the substitute may halt an addiction with an abundance of negative consequences, it can also incur consequences if not managed properly. For example, one provider expressed willingness to support harm reduction for the sake of the service user, rather than losing them to an abstinence-only rule. Moreover, the impact of the substitute was also said to depend on the nature of the substitute, and in the long term, it could pose its own problems. Nevertheless, if help could be sought alongside the primary addictive behavior, the consequences could be handled. Ultimately, the effect of the substitute was said to be dependent on the person and the substitute. While “addiction is addiction,” the potential life-saving effects of substitution were also recognized.
Toward Relapse or Worse Quality of Life
Respondents expressed that the potential harms associated with substitute addictions include the risk for relapse, poor long-term outcomes, unaddressed underlying issues, the onset of new addictions, inhibited skills building, substitution as a temporary solution, and lack of coping/maladaptive coping.
“Substitute addictions could lead to a relapse back into substance use if not carefully monitored.”
“It hurts recovery by not addressing the underlying cause. They may relapse once the substitute addiction is unavailable.”
“It's a new problem that can lead to relapse.”
“I think it hurts recovery, but 12-step helps. People feel guilty and shameful when this happens, and it can lead to relapse.”
“It can delay dealing with the real issues and set them up for a multi-layer relapse triggered by the substitute addiction.”
“I think that’s the challenge with other addictions, it’s hard to argue the good side of heroin addiction, but if it does give them some reward and often leads back to their drug of choice or the drug they originally got wrapped up with.”
“Hurting enables them to hide from their feelings. You've got to start working on yourself, got to change your thinking, and hiding from your thinking won't get you anywhere, and you will relapse.”
“Behavioral addiction may be better than substance addiction, but not effective long-term.”
“Long-term avoidance of pain and not dealing with trauma leads to poor outcomes by not addressing the issue over time.”
“It hurts the client in the long run since we're trying to form new healthy coping skills, but they're still getting the reward system in the brain activated, making kicking their original addiction worse.”
“Addiction is addiction. Even if it feels healthier, like exercise, it could become obsessive and cause one to neglect other parts of life.”
“Clients sometimes go back to old peers who are a negative influence; e.g., ones they did drugs with in the past.”
“The substitute behavior is harmful as well, so it could interfere with their lives and prevent them from moving forward. Risky and dangerous behaviors as a result are a concern.”
“If we’re talking about addiction, it can't help them. It will hurt them because it keeps them in that cycle and continues to make the person feel trapped.”
“It can hurt recovery if they don't remain aware of the impact and the potential to impact functioning. I can’t teach people to not eat, but balance and exercise, it’s good for you, but when it tips, that's when it hurts their recovery.”
“A relationship for youth may seem like a good substitute, but it could become a trigger if it ends.”
“They hurt recovery by not addressing the core issue, but as part of their journey, they need to ‘figure it out.’ Sometimes they are in denial about new addictions, which complicates their path to recovery.”
“It would primarily hurt in the sense that if they are just overusing a behavior, it would be just another distraction from their underlying issues or the real reason why they overuse substances or engage in a behavior.”
“Any addiction can be dangerous, so it's not something that is helpful in my opinion ... they are potentially hiding something else and trying to compensate for that ... It’s just switching patterns or behaviors that are not addressing what's really happening in their life.”
“Substitute addictions can cause legal problems, health issues, or relational problems. They may still be avoiding feelings and true healing.”
“Could be a form of harm reduction, may be problematic, and the things they are substituting may be used too, which may be harmful since the underlying cause may not be resolved because of that perpetuating of the issues.”
“If someone has addiction cross-tolerance (e.g., replacing coke with alcohol), they would need to seek treatment for the new addiction.”
“Replacing an addiction with hiking or running is great, but not if it becomes an addiction as a result.”
“It can hurt a client because they become preoccupied/obsessed, affect finances, they go through withdrawal, they need help with the substitute addiction.”
“I think if they have a substitute type of addiction, they fail to, or they don’t take care of themselves in order to heal from the initial addiction. It starts consuming their time throughout the day, their spiritual life, their relationships.”
“It hurts because it is the same obsession after use. There is no healing or differentiating the substance and treatment.”
“Behavioral addiction is similar to substance addiction, and it hurts them by taking the focus away from building skills to help them beat substance use, and causes them to not focus on the parts of themselves getting better. Overall, it's harmful.”
“I think substitute addictions like exercise are good for recovery, but when it becomes interfering, it's a problem, so moderation is the key. Any time you have an urge to run but when you run, run 30 minutes a day. As long as there's moderation and doesn't replace the primary addiction, that's the goal.”
“It can help in the way that it stops one addiction that creates a lot of consequences, but now they are addicted to food and overeating, which is unhealthy, or staying in unhealthy relationships.”
“Better for someone to play video games for hours instead of drinking alcohol for hours; behavioral addiction may be better than substance addiction, but not effective long term.”
“Harm reduction stance is more healthy in the short term, but long-term avoidance of pain and not dealing with trauma leads to poor outcomes by not addressing the issue over time.”
“Well, I think it can be a diversion. If there's too much emphasis on substance use termination than on coping skills development, then it won't be a sustainable, healthy pattern, but maybe it could be in the short term. Exercise is more healthy and sustainable than meth and could be used as a replacement ... if energies are focused on working to figure out their issues, moderation on the behavior, and coping skills, it could be more useful for them.”
“It helps temporarily since it's used as a coping skill to manage discomfort, trauma, or mental health issues that come up.”
“When you take away their substance of choice and they don't have coping skills set up, they will still be working to get their needs met and feel good. They were struggling before to get their needs met and used substances, but without coping skills, they will still substitute substances for another way to feel good.”
“It boils down to when people get in early recovery, they have a hard time dealing with their emotions again; it's the hardest part of recovery. You don't feel like a human, and they don't have a grip on how to handle themselves. Once they get sober, they redirect their emotions into something else since their coping method is gone—how do I deal with these things? So they get into a relationship or (use) something else to help them cope.”
“Understanding the root cause is important … clients do it to escape emotional pain, resulting in patterns of more unhealthy behaviors.”
“… unresolved mental health issues, they get something to address their anxiety or depression.”
“The quick answer would be the lack of coping skills, self-soothing ... and the need for self-soothing for post-acute withdrawal (chemicals that are off in the brain due to heavy substance use)--those physiological issues. There may also be some kind of underlying mental health issues that the client might not know how to manage yet, and they turn to something else.”
“They are struggling with underlying trauma and may not have the coping skills or support to be able to manage those things positively, so they use what they have to relieve the stressor- feelings, thoughts, etc.”
“The chemicals in the brain during post-acute withdrawal crave dopamine and serotonin that can be gained from foods like sugar, carbs, snacks, and junk food. They are looking for that hit of endorphins that they can get from foods, maybe not as intense but just to get the hit, and no one likes to go running.”
“Well, I think that because they have been homeless, they are depleted by the time they come in, and so food becomes the substitute for fixing their feelings, and they'll use food to make them feel good.”
“… to deal with withdrawal symptoms, pain, to recoup feelings, to get a high.”
“The need to get an adrenaline rush or looking for something to get excited about, like the habit of smoking meth (or) smoking something else (that) can get that desired effect. Looking for excitement or trying to get less bored, and also the physical need to engage in that behavior, both in the sense of physical addiction and impulse to act on that behavior.”
“When you take an addiction away, it's a big part of your life, like it leaves a hole, and they try to fill that hole with something else, like another addiction.”
“Addiction is an attempt to fill a void and form meaningful connections, and when you take away their coping mechanism, regardless of how destructive it is, they will try the next thing to get that fulfilment and fill that void.”
Taken as a whole, the themes suggest that substitute addictions should be monitored, as they can trigger relapse due to unavailability, guilt, shame, avoidance of underlying issues, and continued engagement in addictive behaviors. Substitutes may inhibit understanding of addictive patterns, enabling avoidance, emotional suppression, and reliance on compensation, ultimately hindering true healing. They can become new addictions and/or limit the development of healthier coping mechanisms, and may also require formal treatment. Current mental health difficulties and past trauma, in the absence of adaptive coping skills, may drive substitution. Participant statements suggest the conscious, instrumental use of substitutes.
Treatment Approaches for Substitute Addictions
Recovery groups/group therapy. Respondents described sessions where service users discuss and learn about substitute behaviors/addictions in a group setting, guided by a therapist or peers. Individual therapy. One-on-one counselling sessions were also used to educate service users about managing substitute addictions. Guest speakers/psychoeducational lectures. Facilities also drew on external experts/guest speakers/formal presentations to provide information or education about substitute addictions. Print curriculum. Certain respondents incorporated structured educational material designed to teach service users about substitute behaviors; this could be a formal curriculum or other print materials. Videos. Video resources or multimedia content were also used to educate service users on substitute addictions.
Recommendations for Attending to Substitute Addictions
In response to the question about their recommendations for addressing substitute addictions, treatment professionals (n = 82) highlighted components of treatment approaches, alongside education and training, spirituality, religion, and 12-step group affiliation, as well as research.
“Education around coping skills and that substitute addiction is a possibility and a reality that can be very helpful. I am a big proponent for education on what addictions can look like and how they can change throughout someone's life, and find out how they can moderate that behavior and self-monitor, so they can have self-awareness and put healthy boundaries and set healthy goals for themselves, by themselves.”
“Need more education on the topic; we need to correct misperceptions; prevention through education.”
“They would have to be part of the treatment plan more. It has to happen very early on during assessment or diagnosis, otherwise we won't catch it, and it probably won't come up until later in treatment, and that's problematic.”
“Offering the education and the aftercare, like offering resources to support groups to continue therapy outside of the facility.”
“In general, we need to recognize the need for using the stages of change approach. They may not be ready to deal with them (substitute addiction); when it comes to behavioral addiction, they haven't seen it as a problem yet, and humans don't address things they don't see as a problem. We provide psychoeducation on how the behavioral addiction could derail their recovery and get them stuck in the same behavioral patterns with a different area of focus.”
“More education on it for the clients and the counsellors.”
Treatment professionals’ insights underscore the shared responsibility between service users and themselves in managing substitute addictions.
“Not to negate spirituality, ultimately it is a higher power that can do for us what we can't do for our own self. That's my testimony. Offering onsite spirituality services is very critical for ultimate health and healing from pain and trauma, and gives us the strength to live and have a prescriptive life. From a Christian living [perspective], it's a way with biblical advice that offers us freedom, purpose, and peace.”
“Put your faith in God. Give up idols.”
“Number #1 is to stay sober. Then, when it comes up, you address it (if you're honest; have to be honest). 12-step helps to address substitute addictions.”
“The gospel is the power of God and the salvation for anyone who believes. Something that is mastering us, other than the Creator, is not good, and once your heart is changed, you start to bear fruit and have self-control. We don't want them to cut everything all at once. We see genuine life change happens—like a smoker we had ... he didn't want to continue after 40 years, and that was amazing—that it occurred through the gospel.”
“Also, the self-help groups and referring them to continue with those self-help groups like GA (Gamblers Anonymous) and AA (Alcoholics Anonymous) – long-term programs. That worked for me, but you have to have external support systems.”
The ongoing support provided by 12-Step groups and the accountability it fostered were foregrounded as an asset for recovery. Spirituality was regarded as critical for managing pain and trauma, and submission to a higher power aided ‘self-control’.
“More research, due to split views on it, on how it impacts long-term recovery, and seeing it through a harm reduction lens- does it work? Most things out there right now are anecdotal.” “PET scans are needed to be seen by clients to see and understand what's going on in their brain, why they're using substances, and how they can address it. The lack of advancement, more notably accessibility and affordability of medical advancements, is limited and needs to improve.”
Rather than relying on anecdotal evidence, research could elucidate the trajectory of substitution on recovery, the outcomes of using substitution for harm reduction, and clarify the brain-level changes during ‘active addiction’ and recovery.
Discussion
This qualitative analysis makes significant contributions to the limited literature examining how SUD treatment providers understand and address substitute addictions. Respondents highlighted diverse motives for substituting. Some motives suggest that substitution is transient once the necessary tasks of treatment or recovery have been completed, such as developing adaptive coping skills and attending to the mental health and trauma of service users. Various current treatment practices aim to educate service users, consistent with treatment professionals’ recommendations for how substitution should be dealt with. The focus on group and individual treatment processes is also consistent with the need to address underlying drivers of addictions and to build the skills necessary for sustained recovery. Substitutes exhibit dual effects, as they may ease recovery, reducing harm and temporarily solving problems, or they may derail abstinence-based recovery through relapse, new addictive behaviors, and the failure to address underlying issues and build the skills needed for enduring recovery. The importance of treatment and ongoing recovery support highlights the need for equipped professionals and engaged service users. There is a call for more research to strengthen the evidence base.
Professionals’ emphasis on spirituality, religion, and 12-step groups is congruent with the literature, as substitute addictions have long been discussed by members of self-help groups such as Alcoholics Anonymous (Sussman & Black, 2008). While it has also been argued that 12-step groups themselves may be substitute addictions (Galaif & Sussman, 1995; Lile, 2003), attendees emphasize that fellow members are inclined to raise concerns about (potential) substitutes, often prompting self-reflection and action (Sinclair et al., 2023).
While our findings do not directly mention recovery capital (“the sum of resources that an individual can draw on to support their recovery pathway”, Cano et al., 2017, p. 11), they allude to it throughout. Recovery capital exists at the personal, social, and community ecological levels (Best & Laudet, 2010). Professionals can support service users in developing positive resources and systematically remove or limit recovery barriers (Best & Hennessy, 2022). While recovery capital is generally depleted by the time formal treatment is sought (White, 2002), it can be accumulated and varies depending on circumstances (Best & Hennessy, 2022). The maladaptive or deficient coping skills highlighted by participants have been conceptualized as a recovery barrier or negative recovery capital, potentially hindering recovery (Patton et al., 2022). Alternative coping strategies should be jointly developed (Freimuth et al., 2008), and professionals’ treatment plans should include ongoing assessments of recovery capital and flexible individualized plans to foster its development (Vanderplasschen et al., 2025; Sussman et al., 2024). While respondents’ recommendations for treatment are largely in line with another recent study with treatment professionals in South Africa, and both recognize recovery support groups, aftercare, and connections to community resources (Sinclair et al., 2024), the current study does not emphasize family. Spouses, children, parents, and other family members – representing ‘concerned and affected others’ (Orford et al., 2005) – may unwittingly reinforce the use of specific substitutes which they accept, approve of, or even provide. This limited insight stands to heighten relapse risk and can also be addressed through psycho-education (Sinclair et al., 2024). While cultural differences between the two study contexts may explain this finding, addiction is considered a ‘family disease’ (Roth, 2010).
Findings from this study also imply that treatment professionals distinguish between substitute behaviors versus substitute addictions. Their assertions consistently highlight that substitutes can be temporary and that there is a risk of them growing into the strength of the terminated addiction. These insights are consistent with earlier research demonstrating that the duration may be short- or long-term, and that behaviors may progress to addictive levels of varying severity (Sinclair et al., 2021; White & Kurtz, 2006). Substituting may be “an effective, time-limited strategy for managing early recovery (requiring professional understanding, if not tolerance) … [but may become] a mutation of the existing problem (requiring prevention, early intervention, or focused treatment)” (White & Kurtz, 2006, p. 5). While a case-by-case risk analysis should determine the “potential danger” of the substitute (Chiauzzi, 1991, p. 67), it is evident that respondents more readily accepted certain substitutes than others (e.g., gaming over alcohol, or exercise over crystal methamphetamine). In this implicit hierarchy, the perceived danger of various addictive behaviors may lead providers to downplay some substitutions while problematizing others. As these differences likely reflect beliefs, culture, and stigma, rather than lived experience, they may be negatively consequential for recovery efforts (Blomqvist, 2009).
While the importance of further educating treatment professionals was recognized, respondents also addressed the need for more research on substitution. Relative to other areas of interest in the field, substitute addictions are under-researched (Sussman et al., 2024; Sinclair, 2022). In our experience, inconsistent terminology, the absence of a universal definition, and challenges in publishing work that straddles the lines between SUDs and behavioral addictions, and abstinence-based recovery and harm reduction (see Sinclair et al., 2021; Kim et al., 2021; Sussman et al., 2024) pose their own challenges.
Limitations
Our findings should be considered in light of the following limitations. A notable proportion of the treatment professionals recruited into this study are employed at facilities listed on ‘America’s Best Addiction Treatment Centers’. It is worth considering that providers may be hesitant to criticize practices at their facility, leading to a social desirability bias. Our findings would likely also have been enhanced by interviewing both professionals and service users from the same facilities regarding their insights into substitute addictions, treatment, and recovery. That notwithstanding, our work offers rich insights from experienced professionals and enhances the depth of current research. To augment treatment and recovery support services, we echo our respondents’ calls for further long-term research into substitute addictions and add that more qualitative research, particularly with treatment professionals, is necessary to capture contextual nuances and tailor interventions and education needed to advance the field.
Conclusion
The present study identified several factors regarding why substitute addictions may arise, their potential outcomes for recovery, how treatment professionals are currently addressing them, and recommendations on how these behaviors should be treated. Given the globally limited availability of treatment-assisted recovery services and high rates of post-treatment relapse, this study makes important strides in addressing the paucity of research on treatment professionals’ firsthand experiences and can inform and improve service delivery.
Footnotes
Ethical Considerations
The University of Southern California Institutional Review Board (IRB) approved the study.
Consent to Participate
Each prospective participant was provided with an information sheet, informed about the purpose of the research, and verbally consented prior to participation.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the National Center for Advancing Translational Science (NCATS) of the National Institutes of Health under award number UL1TR001855. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request. Restrictions apply to the availability of these data due to privacy and consent limitations.