
Abstract
Globally little is known regarding substance use service providers’ perceptions of substitute behaviours and this significant gap could hinder service provision and recovery outcomes. Semi-structured focus group discussions (including 22 service providers across five sites) were conducted in residential treatment facilities in the Western Cape, South Africa. Service providers recognised substances (e.g. cigarettes and caffeine) and behaviours (e.g. gambling, eating, love, sex, shopping, exercise, and gaming) as potential substitutes. Identified substitute motives included managing cravings; self-medication; filling the experiential void of the primary substance, and time-spending. Concurrent behaviours and addictions were believed to be a key mechanism underlying substitution however, service providers did not uniformly screen for co-occurring behavioural addictions. Substitute behaviours were primarily considered a pathway to relapse and service providers emphasised prevention, detection and family education. To suitably intervene, screening for co-occurring behaviours should be an integral part of the assessment of those presenting for substance use treatment.
Background
Studies published over the past several decades indicate that a substantial number of individuals with substance use disorders (SUDs) develop substitute behaviours during recovery: behaviours and/or substances that replace the functions of the terminated SUD (Sussman, 2017). Emerging literature identifies various underlying motives, mechanisms, presentations, and outcomes of substitute behaviours. Substitute motives include curiosity and experimentation, outcome expectancies, time-spending, being influenced/triggered by others and availability, accessibility, and prior experience with (potential) substitutes (Chiauzzi, 1991; Shapira et al., 2021; Sinclair et al., 2021b; Sussman et al., 2011; Sussman & Black, 2008; Sussman & Sussman, 2011). In terms of the process by which a substitute behaviour may occur (mechanisms), they may develop from a previously co-occurring addictive behaviour, may precede a primary substance and re-emerge after its termination, or, may constitute ‘novel’ behaviours arising during recovery (Chiauzzi, 1991; Sinclair et al., 2021a; White & Kurtz, 2006). Substitute behaviours occur on a spectrum of duration (e.g. time-limited and short-term, or long-term), severity (i.e. impact on functioning), and relapse risk (i.e. role in relapse, developing new addictive behaviours, or both) (Selby, 1993; Sinclair et al., 2021a). Studies on substance-to-substance substitution demonstrate that while cigarette smoking has been used to adjust to life in recovery (Murphy & Hoffman, 1993), newly initiated smoking often increases (Friend & Pagano, 2004) and has been linked to substance use relapse (Weinberger et al., 2017). Similarly, post-treatment alcohol use has been linked to relapse and alcohol becoming the primary addictive behaviour (Staiger et al., 2013). Those that highlight the risks of substituting emphasise that the use of another mood-altering substance may diminish the resolve to abstain from the SUD, or lead one to downplay the associated harms and losses making it reasonable to use again (Selby, 1993). While the subject of much less research, work on substance-to-behaviour substitution provides evidence of pornography substituting for alcohol to become the primary problem, displaying addiction-like characteristics, while alcohol abstinence endures (Sinclair et al., 2020). Similarly, cannabis has been replaced with pornography, web-series viewing and gaming (Tadpatrikar & Sharma, 2018) and while initially used to prevent relapse, pornography use grew to the strength of an addiction. Substitute behaviours are distinct from substitute addictions. Genuine addictions, including those for which diagnostic criteria are lacking (Sussman & Sinclair, 2023), are characterised by withdrawal symptoms, tolerance, (cognitive-behavioural) salience, relapse, modification of mood states, and conflict (Griffiths, 2005).
Substitution has also been conceptualised in terms of harm reduction. Substitute behaviours may be an intermediate step towards (abstinence-based) recovery, ease early recovery, or represent recovery without abstinence (see Horvath, 2006; McKeganey et al., 2004; Neale et al., 2011; Sussman & Black, 2008). However, the nature of and motives for the substitute are important for conceiving of its risk for greater or comparable harm (Horvath, 2006; White & Kurtz, 2006). Even healthy, recovery-supportive substitutes could be associated with relapse (Sinclair, 2022). Furthermore, “any substance or behavior that is reinforcing, used to cope, or provides robust and desired changes in experience has the potential to become an addiction” (Freimuth et al., 2008, p. 151).
Recovery capital, a conceptual framework that describes the sum of resources that an individual can access to initiate and maintain recovery, encompasses personal (e.g. safe and recovery-conducive shelter; interpersonal skills), social (e.g. relationships that support recovery efforts) and community (e.g. a full continuum of addiction treatment resources) assets, may be present at treatment entry or be obtained or accessed during treatment (Parlier-Ahmad et al., 2021; White & Cloud, 2008). “Though people who already have recovery capital may either recover on their own or with formal help, those who have lost, or who never really had, adequate recovery capital will first have to acquire some amount of internal and external resources before being able to take up the challenge of recovery in a fully effective and sustained way” (Davidson et al., 2010, p. 2). Recovery capital can be accrued or depleted continually and is dynamic, tending to fluctuate with circumstances and conditions (Best & Hennessy, 2022). Lower levels of recovery capital have been linked to relapse (White & Cloud, 2008) while moderate levels are positively associated with substitute behaviours post-treatment (Sinclair et al., 2021b). Recovery support is a catch-all term for a diverse continuum of services that seek to build recovery capital, including recovery support groups, aid with education and employment, childcare, and housing-related support (Davidson et al., 2021). Recovery support relates to recovery-oriented systems of care, “the idea is that persons with substance use disorders often have multiple problems and can receive help from diverse types of peer and professional resources in the community” (Polcin et al., 2023, p. 8).
Despite the known high risk of relapse immediately post-treatment and the association between substitution and poorer treatment outcomes, many questions remain unanswered concerning the dynamics of substitute behaviours (Kim et al., 2021; Shapira et al., 2021; Sinclair et al., 2021a). Views on the outcomes of substitute behaviours differ: some hold that substitute behaviours heighten relapse risk or signal impending relapse (Chiauzzi, 1991; Melemis, 2015; Rasmussen, 2015; Selby, 1993), while others contend that substitutes potentially facilitate recovery (Horvath, 2006). Little is known about treatment professionals’ views on substitute behaviours and how to address these during treatment. Given that service providers are afforded considerable discretion and treatment-related knowledge and experiences accumulate in recovery trajectories, knowledge of their conceptions, theories and responses to substitute behaviours enables insight into current strategies and clinical realities. Simultaneously, engagement with service providers will elucidate areas that are essential for workforce development efforts and relevant and responsive treatment. Given the limited resources in low- and middle-income countries and the increased relapse risk among persons who substitute, it is important to address this topic among treatment professionals. A recent study in South Africa demonstrated that almost one-third of service users developed substitute behaviours during the initial months after residential treatment (Sinclair et al., 2021b). The purpose of this study is to explore substance use service providers’ perceptions of substitute behaviours during and after residential treatment in the Western Cape, South Africa. To our knowledge, this is the first study to explore service provider perceptions of substitute behaviours in South Africa and low- and middle-income SUD treatment settings.
Methods
As part of a broader multiple methods study on the nature and dynamics of substitute addictions (Sinclair, 2022), this study employed an exploratory, qualitative design to report on service providers’ perceptions based on five focus group discussions. A qualitative methodological framework is well-suited to meet the aims of the study, given the in-depth, insiders’ understanding of the phenomena it affords (Gelo et al., 2008). The focus groups were guided by a semi-structured schedule focused on understandings of substitute addiction, experiences of delivering treatment concerning substitute addictions, and recommendations for clinical practice.
The Study Setting
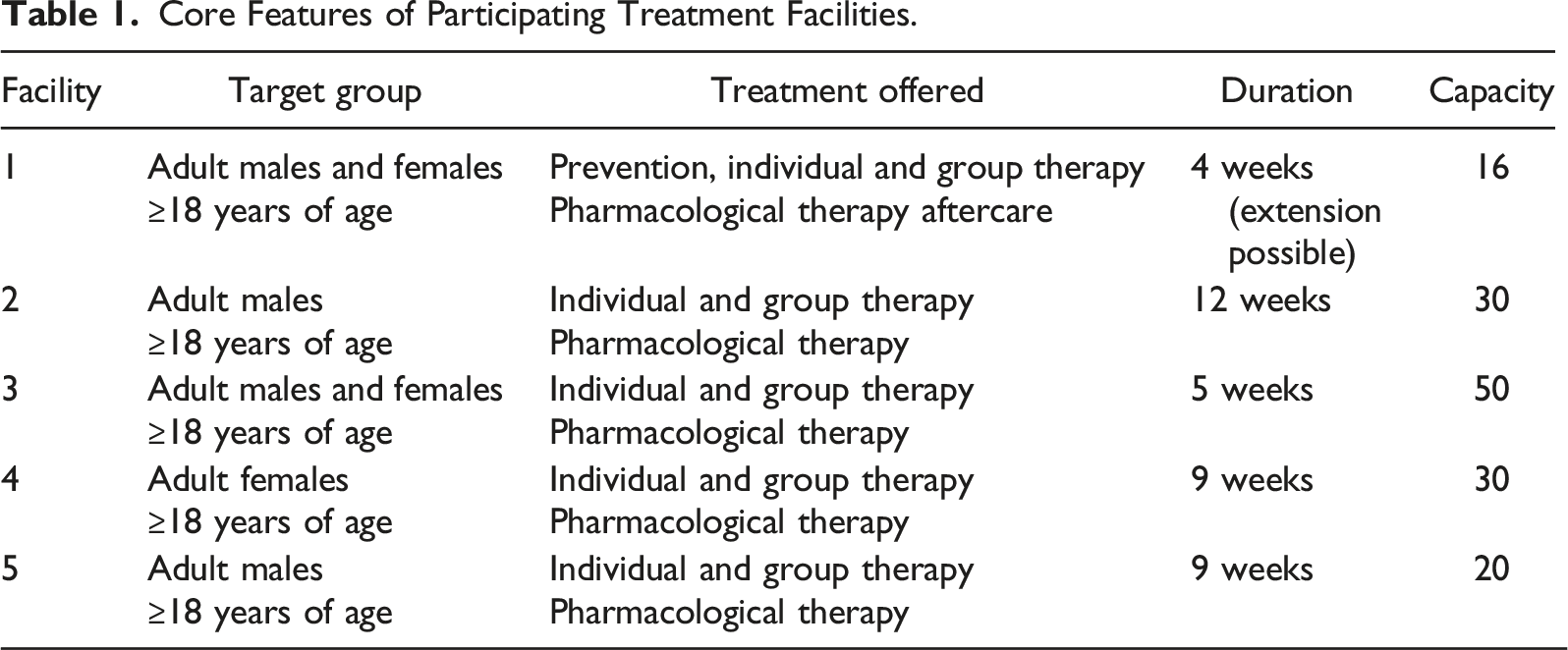
The study was completed in the Western Cape, one of the nine provinces of South Africa. With an estimated 7 005 741 inhabitants in 2020, 11% of South Africa’s population, the Western Cape constitutes the third-largest province by population (Statistics South Africa, 2020). In the first half of 2021, 2433 (22% of all admissions across 27 outpatient and residential treatment centres) persons were admitted to substance use treatment in the region. The most commonly reported primary substances at treatment entry were crystal methamphetamine (known locally as tik; 40%), cannabis (34%), alcohol (18%), and heroin (17%) (SACENDU, 2022). Two systems of care exist for addressing SUDs: treatment services in the for-profit private sector and those fully or partially funded by the government. The latter category seeks to provide a more accessible, affordable service offering to the broader South African public and those without health insurance (Myers et al., 2008; Myers & Parry, 2005). Access to these non-private residential treatment necessitates referrals, which are primarily made by social services. Notwithstanding that social service offices are centrally located and render wide-ranging, essential social welfare services including early intervention and referral services for SUDs, for free, this referral requirement has been found to be a barrier to treatment (Burnhams et al., 2012; Isobell et al., 2015). These facilities’ treatment policies reflect a disease-model orientation. The National Drug Master Plan (2019–2024; Department of Social Development, 2019), which governs service provision throughout the country, has identified the need to increase harm reduction services within substance use treatment, as these are presently lacking (Department of Social Development, 2019; Scheibe et al., 2017). Yet, although prevention, post-treatment aftercare and reintegration services facilitate recovery and support the gains of treatment, they remain limited in South Africa (Isobell et al., 2018). Treatment services are delivered by multidisciplinary teams, comprising social workers, occupational therapists, (psychiatric) nurses, recovery assistants, and psychologists.
Participants and Sampling
Core Features of Participating Treatment Facilities.
Data Collection
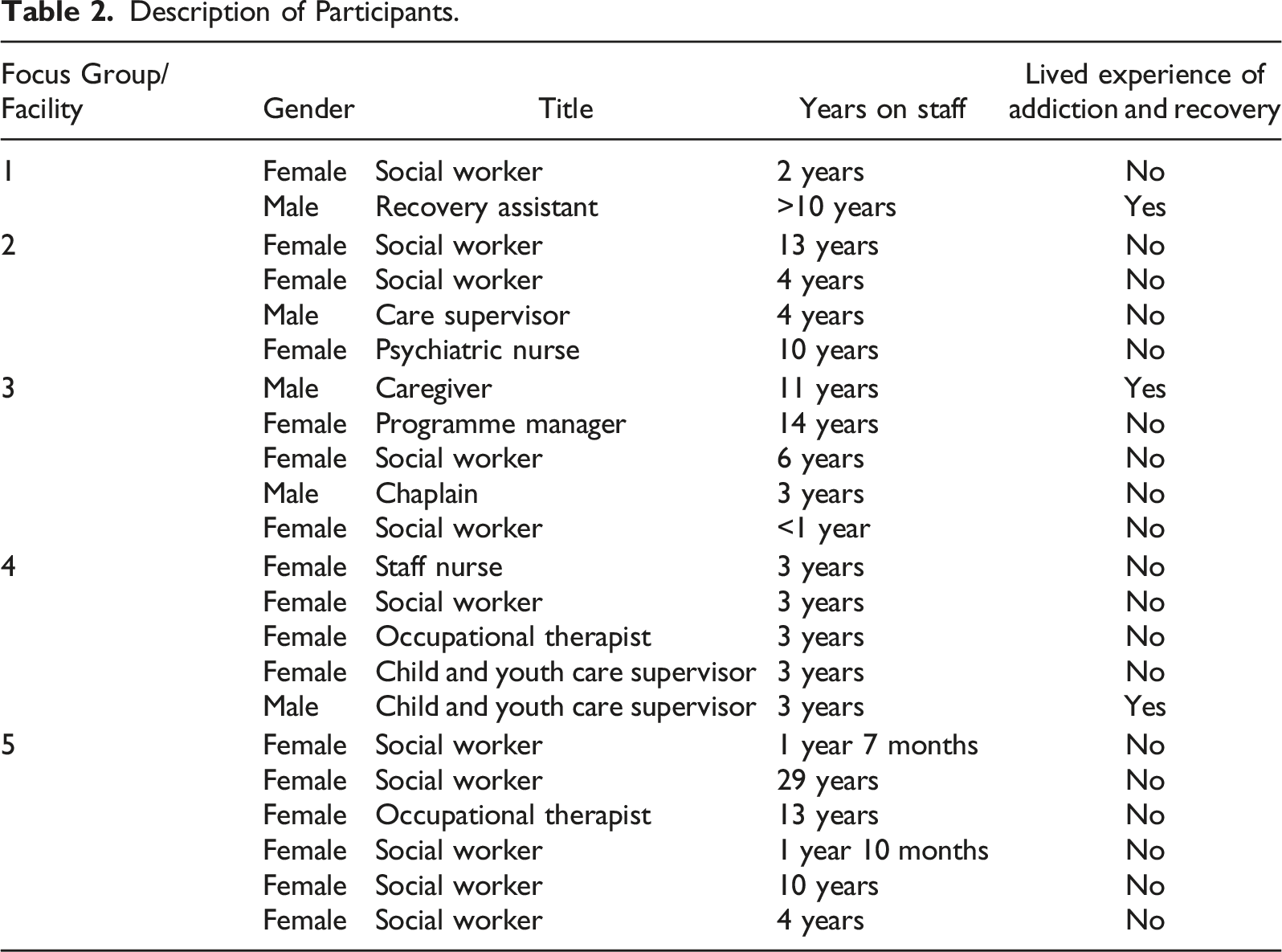
Description of Participants.
Data Analysis
Data were analysed using thematic analysis (Braun & Clarke, 2006). The first stage of the analysis entailed the third and first authors transcribing the audio recordings of focus group discussions verbatim. To further become acquainted with the data, both authors read the transcripts to derive a global understanding of the texts. Thereafter, the transcripts were re-read and, with the research question in mind, first-level codes were assigned independently. Through discussion, the coders re-examined each coded transcript to identify patterns in participants’ experiences. Through an iterative process, themes and sub-themes were formulated. This dual-coder analysis simultaneously refined the themes derived and enhanced study validity. Finally, the themes were framed by the extant research literature.
Results
The focus group findings demonstrate that the concept of substitute addictions was known to all service providers. Participants shared various definitions of substitute addictions, outlined a range of underlying motives and mechanisms and discussed substitution in relation to recovery, and relapse. Therapeutic responses emphasised prevention and detection, and the importance of including the family Figure 1. Themes and sub-themes.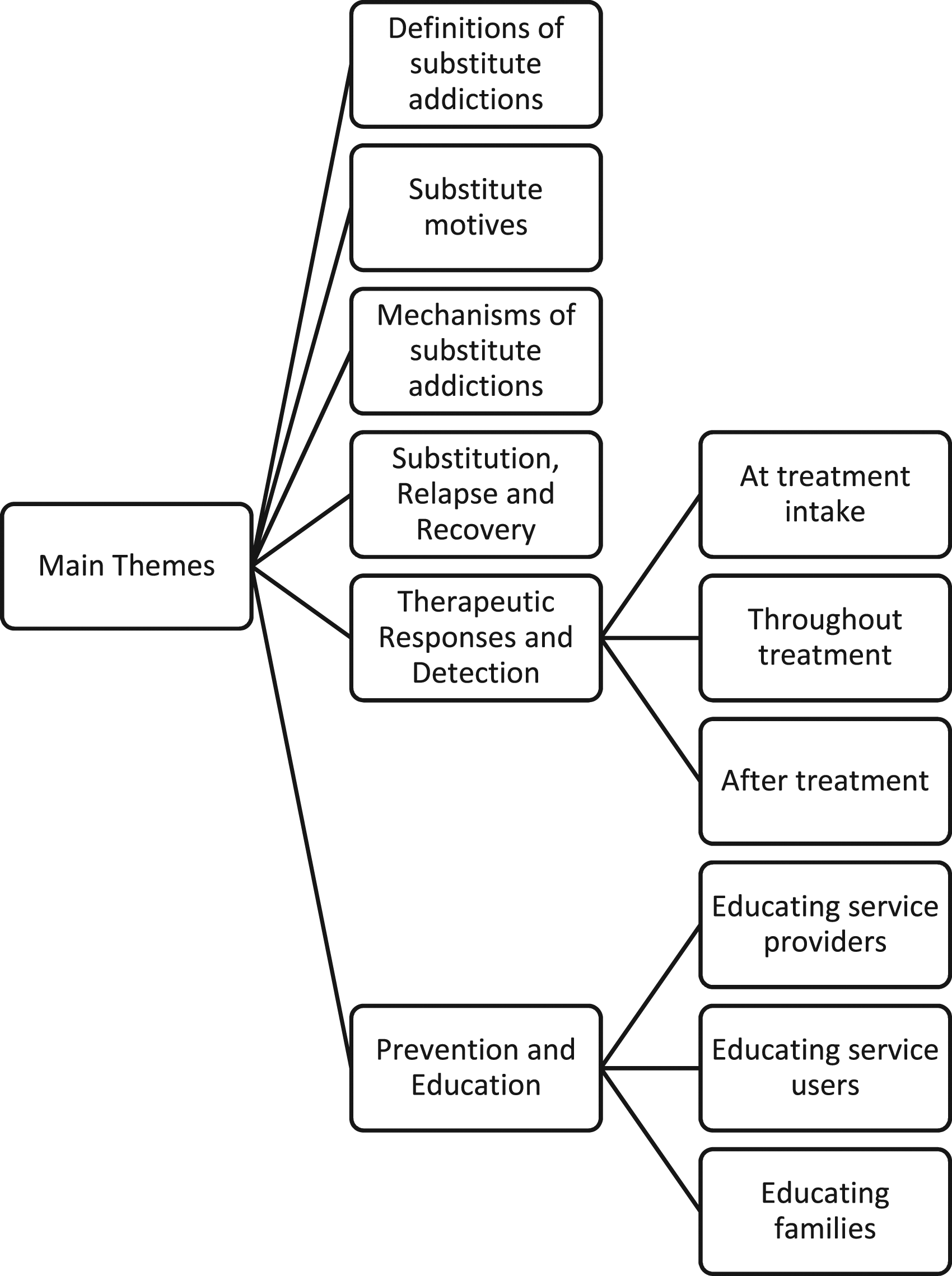
Definitions of Substitute Addictions
All service providers, three of whom had a personal history of addiction and recovery, were familiar with the concept of substitute addictions, and recognized substances (e.g. cigarettes and caffeine) and behaviours (e.g. gambling, eating, love, sex, shopping, exercise, and gaming) as potential substitutes. Others stated that persons with SUDs substituted to pursue the same or similar appetitive effects provided by the primary addiction; to satiate a craving; to alter a feeling state; or due to the perception that the replacement behaviour is less harmful. Substitutes may immediately or gradually replace the primary addictive behaviour.
Service providers indicated that substitute behaviours functionally replace the original addiction and are used for an expected outcome. […] giving me the outlet of feeling something other than what I am feeling at the moment […]. Replacing the initial addiction with something that also creates that endorphins in your brain or that thrill-seeking behaviour. […] any experience that would trigger the emotion that you could possibly crave, or that you need, and then becomes a craving.
Service providers outlined possible presentations of substitute behaviours. In one presentation the ‘primary’ addiction in a set of addictive behaviours may be terminated due to treatment while a ‘secondary’ escalates, becoming an addiction or a more severe addiction. Substitutes may be substances within the same drug class or different activities; may be employed deliberately to replace an inaccessible addictive behaviour, or is perceived to be less harmful, or may also be used to fill the experiential void of the terminated behaviour. Use of the replacement substance may initially be legitimate, as in the case of a prescription for pain management, but over time may become problematic. Insight concerning the substitute may develop at a later stage. […] they stop drinking but now they exercise to the extreme. Or […] somebody who was on heroin substitutes it with maybe painkillers […] it might be they were an alcoholic and then they are in an accident […] the doctor prescribes […] Tramadol and then after a while […] they’re misusing the script […] my mind used to be occupied by this one thing. So, to keep my mind occupied while that’s gone I could fill with something else. […] It may be, people feel that it is safer, better or less harmful. If I don’t have the one I will find something else. To give me […] more or less the same effect.
Substitute Motives
According to service providers, substitutes may be used to mask feelings in the same way that the primary addictive behaviour did. Or, to foster recovery, someone may experiment with different activities to fill the experiential void left by the primary addiction. There may not always be an awareness that the replacement could potentially become problematic. The same thing with your addiction: you’re masking your feelings and emotions […] trying to fill this gap […] when we take it away, that life is so empty […] now you’re looking for things to be clean and sober to be in recovery, but at the same time you don’t know what you’re adding could potentially also […] become your new thing.
Whereas a primary substance may provide preferred acute effects, a secondary substance may simply be part of the repertoire to achieve intoxication when desired. The legal status of a substance and acceptance by the family may also reinforce use. The primary drug is the one they will always return to and they would do anything to procure […]. With the secondary drug, it is more about ‘I just want to use something’ […]. Sometimes, when people leave an illegal drug they might substitute with something that’s legal because their family also still uses alcohol […] quite a few patients, they would leave tik […] and the wife allows the husband still to drink alcohol.
According to service providers, substitutes may be motivated by guilt and trying to compensate for role impairment during active addiction. Some service users may initiate smoking during early recovery. Or, ‘healthy’ and ‘productive’ behaviours such as work or exercise may become a central focus, to the neglect of recovery support activities. Should these ‘positive’ behaviours become unmanageable, a substance such as caffeine may be used for its effects, to cope. This ‘unbalanced’ life was likened to life in active addiction. Interviewee 5: People would push it to the extreme, so much so […] that they would start neglecting their aftercare […] either going to the gym or hiking […] or […] working an extra shift […] because they see it as productive or as healthy – they don’t see it as a substitute […] or they would start smoking cigarettes. […]. Because it’s legal […] they rationalise it […]. Interviewee 2: ‘[…] in the past I didn’t pay my maintenance (child support)’ […] ‘now I have to work overtime' […] Interviewee 4: […] it starts to take its toll, they start picking up things […] to try and cope. […] working extra-long shifts then […] lots of caffeine.
Food may also be used to manage cravings for the terminated primary substance. Substitution with food was said to be particularly challenging to address as it is necessary for survival, and active addiction was characterised by food deprivation. Cravings […] that’s why they eat […] especially because you need food to survive […] it’s such a dangerous substitute. Because when is enough ever? […] you never ate because you were using meth and […] now […] your appetite is coming back. So, do you stop them? Or do you let them catch up?
The preferred substitute may be found through experimentation until the desired effect is achieved or, by replacing a previously used substance when it no longer provides the desired appetitive effect. It might not necessarily be the more acceptable one. Because I could be starting out with cannabis and eventually end up with tik. We often see that. […] ‘I’ve tried it, it just doesn’t do it anymore. I add Mandrax. I don’t like it at all. Let me try something else’.
As service users may not derive enough pleasure from prosocial activities, they may seek out other activities. Service users may also be prompted to start a new relationship in treatment. […] You can’t just address the substance […] dependency is all about the dopamine […]. So they still don’t find enough pleasure with family time, or, constructive free-time activities. They still seek other things. Love […] or, what they think love is: relationships […] they fall in love so quickly and one asks them ‘how long have you known each other?’ ‘A day’. ‘And you love this person?’ ‘Yes!’ Obviously, an addiction has a lot to do with dopamine and […] anything that they think lets them feel a bit better […] we see love (as a substitute) a lot, first. Because they can experience love here.
Religion, except for when service users became ‘obsessive’, was one of the only ‘positive’ substitutes identified. Engagement in religious activities may be used to occupy any unstructured time. Sometimes patients that get very religious. One or two may be obsessive. Some others […] it might be something to fill up their days and their free time and their Sundays. To go to church, they want to go and do motivational work in their communities and - which is then positive […]
Substitutes may also be used to replace the self-medication function of the primary substance. Sometimes our patients self-medicate when they actually need Ritalin® or Concerta® then they use tik. […] makes them calm down their brains. […] self-medication that causes them to use due to an illness like ADHD.
Mechanisms of Substitute Addictions
Participants identified various mechanisms (interplay among addictions over time) by which substitute addictions may arise in service users presenting to treatment. One mechanism underlying substitution may be that service users have co-existing behaviours of which one is identified as a primary addiction to be addressed in treatment. The concurrent behaviour, which may have complemented the primary addiction, then stands to grow to the strength of an addiction. Now that you stop using drugs, when you go back to gambling now they highlight that as a warning sign […]. It was fine all the time because that’s not really the addiction […] it does become because now it escalates […]. You just left your drugs and sex has now become the primary thing […]. It was always there, it was a secondary. […] Drug use and the sex maybe went hand in hand.
However, if a service user did not regard their concurrent behaviour as problematic, it may not be disclosed until a later stage. Service users may also minimize a coexisting addiction and when the full extent of it is known, it may emerge as more severe than the identified primary substance. I have two patients currently that both only mentioned to me their gambling use […] like session number five or so. […] They don’t think it’s a problem, at all. […] One patient, […] has had so much debt […] and other problems […] worse than his alcohol use […]. I first told him ‘but you stop that use as well’ and I spoke, explained why - he came back the next week and said: ‘so I stopped my gambling but I’m going to gamble on Friday […]. ‘Yes, in the past I’ve had debt but I don’t have a problem’.
Service providers contended that service users’ belief that they did not have to abstain from mood-altering substances that were unproblematic previously, may be another mechanism by which substitutes arose. In still other cases, the substitute may arise from multiple addictions that alternate such that one comes to the fore periodically. That’s very common […] they don’t understand the fact that they have to abstain from everything, they think that ‘okay I’m just here for this one drug and that’s the one that has caused the most problems in my life’. […] Sometimes they have more than one addiction […] so they chop and change.
Alternatively, the family may unwittingly facilitate a substitute addiction by providing access to licit substances. We had a role model client. […] I […] asked the mother how he was doing. He was ‘doing quite fine, staying indoors the whole day’ […] didn’t have a job. […] ‘in his bedroom playing the Xbox all the time’. […] He’s coming to ask for painkillers and then he goes back to his bedroom […] he was doing drugs indoors. All the time.
Another presentation entails the initiation of a behavioural addiction after abstinence from a primary substance. For some, these behaviours may also have been engaged previously. The reward derived from the activity may drive continued use, and ultimately, addiction. I come to rehab and then I stop using tik, but I start gambling […] a different activity entirely. […] They might have done gambling in their lifetime. […] It was a rewarding activity. […] It’s something that I’ve been doing casually and continue using and doing […]. The process of addiction takes place. […] I don’t think people purposefully look for a substitution.
Substitution, Relapse and Recovery
As the behavioural addiction may be resumed post-treatment, it represented potential substitute addictions. Participants concluded that life in recovery should not encompass (potentially addictive) behaviours that cause dysfunction. Interviewer: If someone has substituted their addiction, are they in recovery? […] That depends on the addiction or the substitution […] how harmful is the behaviour? […] Your behaviour and attitude is the same […]. You’ll start doing the same things.
Service providers grappled with the question of whether a service user admitted to an residential substance use treatment facility was in recovery if they did not disclose a concurrent behavioural addiction. Interviewee 3: When I leave the facility and I’m no longer using the substance but I’m continuing with my gambling addiction… am I in recovery? […] ‘I am addicted to tik, but I’m also addicted to gambling’. What if I do identify both of them as an addiction? […] Interviewee 2: You’re 50% in recovery.
Being triggered, overwhelmed by cravings or, perceiving that the substitute behaviour is not sufficient to meet the desired need may precipitate relapse. And eventually when you have too much other triggers […] the substitute is not enough, then you relapse. Impaired judgment, or your cravings are just too much […].
Substitute behaviours were believed to be detrimental to recovery and to precipitate relapse by masking feelings, and emotions, leading to a false sense of coping. Family members heightened relapse risk by permitting the use of certain substitutes. Their endorsement of certain substitutes may be a result of their substance use or limited insight into addictive behaviours. It does take away one’s focus from the recovery process […]. That thing actually puts you back 10 steps. […] you’re gonna be focused on one area […] too much. This thing becomes and consumes you. […] Because you’re masking your feelings and emotions and it will always be your go-to then. […] you’re not really coping. So, families will also just glance over the substitutes. Or they will even provide. […] ‘Methamphetamine is my drug of choice, but the people at home are still smoking marijuana’ […] so then they will substitute it. So, if the family isn’t educated […] relapse has a much higher chance.
It was argued that substituting indicated that someone had not acquired the necessary skills and knowledge to stimulate the reward centre in more adaptive ways. Furthermore, participants perceived that persons who substituted were not in recovery, as the substitute functionally replaced the terminated substance. Substituting was seen as a sign of impending relapse and as a mechanism for relapse to the primary substance. When substitution hindered engagement with recovery support, such as checking in with specific people (e.g. a support group sponsor) or became the default response over coping skills acquired or developed in treatment it was regarded as a relapse risk. Over a period of time, it does impact your recovery because it will become your go-to thing and you’re not using your tools anymore. […] So, you’re not […] coping. […] I’m not checking in with anybody, because now I already had an outlet. It is a risk […]. You are not really recovered from the drug addiction. […] If you substitute you go back to the original drug. If you leave one substance for the other one, in the end, the other one becomes your crutch. […] if it’s like alcohol, you get drunk and you just relapse into your primary substance. […] it’s a very negative prognosis because if you really want to recover you shouldn’t substitute anything […]. I’m in recovery with the substance but I’m still gambling. […] whether I consciously see it as an addiction or not […] it’s gonna cause problems in different facets of my life. […] It means that I haven’t gained the necessary skills, the knowledge […] to stimulate my reward system without […] a negative impact. […] the chances that I will relapse into my other addiction is greater. […] You cannot be in recovery if you’re still engaging with something that causes dysfunction […].
One participant, with a personal history of recovery, appeared to endorse a harm reduction stance, stating that certain behaviours may continue in recovery, provided it is within socially acceptable parameters. However, colleagues outright dismissed his views. Interviewee 2: Substituting is not recovery […] Interviewee 3: […] you are relapsing and you were never in recovery […] Interviewee 5: […] if there is behavioural change, to socially acceptable norms and […] standards. Then you can say that ‘I am in recovery’ […]. Because now you are (in recovery), with the exception of socially acceptable drinking and cigarettes, pardon those. Interviewee 2: Don’t fool yourself. Interviewee 5: […] For me, 26 years of recovery […] I had to substitute a lot of things. […] So, I’m speaking from my own perspective as a recovering addict.
Some did not regard substitution as a form of harm reduction as each potentially addictive behaviour had its harms and risks and would progress. Substitution is not harm reduction because substitution […] is replacing one addiction with another. […] crystal methamphetamine brought its own set of harm, of risk […] gambling […] its own set of risk and harm. […] I’m now no more aggressive […] but I’m selling all my stuff and my house […]. My whole salary goes to casinos […]. Addiction is a progression […] it’s gonna get worse, the longer I stay with that substitute.
While ‘one or two’ service users sought to reduce their alcohol consumption, service providers found that use soon escalated. Though aware of the related literature, harm reduction was not taught within the programme. What we teach them […] is not to drink at all, but I know there is lots of evidence on harm reduction for people that’s maybe at an Ambivalence stage of totally quitting. […] We have one or two that try to just drink less but then in a while we hear oh they’re back up there again.
Another participant recounted how in a postgraduate addiction care training programme case study she considered cigarettes to be a form of harm reduction for the earlier SUD. One of the case studies concerned with Christmas […] and the person’s patient had stopped using cigarettes. As a result of the stress etc., he started smoking again. […] And it was terrible for this therapist. And deep within myself I thought: ‘it’s ok’. […] ‘at least it’s not the drugs'. It is still not a coping mechanism. […] ‘Take your cigarettes, it’s fine’. So, harm reduction.
While participants in one group shared that substance-based substitutes could lead to relapse to the index substance or another substance becoming a primary SUD, in another group a provider with lived experience expressed that “socially acceptable” alcohol and cigarette consumption were considered within the parameters of recovery and not as inevitably negative for recovery. I once had a patient who used tik and on his own - easily - stopped using because […] - there were consequences; his wife threatened him etc. And then he started using alcohol to the point where it became his primary substance. […] he had developed the insight that it was his behaviour and that […] ‘it doesn’t matter what (substance), I become dependent’. […] if there is behavioural change, to socially acceptable norms and […] standards. Then you can say that ‘I am in recovery’ […]. Because now you are (in recovery), with the exception of socially acceptable drinking and cigarettes, pardon those.
Therapeutic Responses and Detection
Service providers outlined their therapeutic responses to substitute addictions. Detection of substitutes occurred at various points during and after treatment. Some service providers screened for the presence of multiple, co-occurring addictions during the initial intake assessment interview as these represented potential substitute behaviours. During treatment, staff members monitor and engage in dialogue with service users to detect any potentially worrisome behaviours and substitute behaviours. When clinical staff are off-duty, non-clinical staff observe and interact with service users, later providing feedback to service providers or encouraging the service user to make disclosures.
At Treatment Intake
During the intake assessment, service providers gathered detailed information on the addiction career of service users, sometimes aided by diagnostic instruments. However, service providers did not uniformly screen for co-occurring behavioural addictions during intake and some service users withheld or did not think to disclose potentially relevant information. Our assessment tool that we’re using now […] only asks about substances […]. So, asking the questions: ‘Are there anything else that you are using excessively?’ […] ‘Are there any other activities that you are doing that you find problematic in your life?’ Or maybe the question wasn’t asked earlier. I’m thinking now if our admission form asks that question about gambling or other things now; so maybe that is something that we need to look at.
Nevertheless, (potential) substitutes could be detected throughout the programme, potentially altering the treatment course. Other behaviours may only manifest post-treatment, necessitating psycho-education and enabling facilities providing aftercare to continue intervening.
Throughout Treatment
Substitute addictions could be detected during treatment sessions, through dialogue and observations or, during the routine operation of the treatment facility. These interactions may reveal potential substitutes that the service users may be unaware of. Consequently, effective collaboration between clinical and support staff necessitates sufficient knowledge of substitute addictions on the part of support staff, and competent reporting skills. I’m the social worker […] I only get certain amounts of information: clients who behave very well. But then you have the Recovery Assistants, who are just observing them at night, when they’re talking […] relaxed […] we allow for that interaction because we get so much information […]. When we meet in the morning […] we get to address it. Patterns change and the behaviour changes […]. We need to observe. All the time. The people who work with them for 24 hours need to be dedicated, […] trained, […] considered as important in […] observing and reporting, and they need to know how to do it in a manner that is sensible, that you can use that information. […] They won’t tell you, because they don’t realise it’s a problem. […] you’ll see; you know them.
After Treatment
Service providers expressed that substitute behaviours may be detected post-treatment, such as in an aftercare programme. A very difficult thing to deal with […]. It’s just constant maintenance […]. People need to make you aware of these things […] and some sort of therapeutic help as you go along. […] While we’re dealing with the primary we’re able to see, when we analyse your lifestyle […]. But often not and it only then manifests then in aftercare or after treatment. […] and only after a month or two because clients are on a pink cloud.
Prevention and Education
Service providers discussed the necessity of educating service providers, service users, their families and the community to prevent substitute addictions and to potentially influence its course.
Educating Service Providers
The first step to preventing substitute addictions was said to be for service providers to be aware and informed. We’re just happy that they’re running outside or that they are eating. So sometimes we don’t pick up that there is a red flag. […] If service providers are also just aware of the dangers of substitute addictions, that can be something that is focused on. If I don’t understand dependency I won’t be able to treat you appropriately and I think the same with family.
This was particularly important given that substitutes may be engaged or acquired in treatment: Sitting in front of the TV […]. The smoke breaks. The smoke breaks. Because that’s something that we still allow, although we’re not supposed to. […] that becomes an obsession, fixation. ‘I must’. Something actually very similar to the use of the substance.
Educating Service Users
Service providers believed that educating service users was central to preventing substitute addictions. Two facilities (FGD 1 and FGD 5) had dedicated lectures while others discussed substitution during assessment and treatment (FGD 2, FGD 3 and FGD 4).
One lecture discussed substitution within relapse prevention and included former service users receiving aftercare. Week five, we focus on relapse prevention […]. Warning signs, high-risk situations, triggers, reservations […] and substitution. […] The clients are aware of substituting […]. They are also aware of their reservations […]. Justifications. […] we have aftercare clients sitting with inpatient clients and those things get thrown back and forth. I’ll give a topic, and they also speak about it. And then the inpatient clients will ask the aftercare clients: ‘how do you actually deal with this thing?'
Another psycho-educational lecture focused on leading substitute behaviours. We highlight the 10 most common cross addictions. I always start with alcohol because alcohol is legal […] nicotine dependence […] food addiction […]. Then I bring it back to drugs. Some people smoke drugs because they don’t want to get fat […] video games […] sex addiction, shopping addiction, pills […] cell phone addiction. […] browsing the internet, you keep watching videos […].
Educating Families
Each focus group emphasised that service users’ families should be involved in treatment to avoid (unknowingly) facilitating harmful substitution or leaving the behaviour of the service user unaddressed. Once families understand the possible trajectory of substituting – that it may promote but also detract from recovery efforts – they could intervene early and/or prevent it. It’s very important to include them. […] Families almost dump the person in a centre and […] they don’t expect that they need to change anything. […] we work with the patient; they heal. But they go back to the same environment. […] So, they will then just be also […] too happy that the person is eating or […] is not the same as […] before. Illegal, yes, to something legal, and then sometimes the family even supports them. Because in the family’s eyes there’s not really something wrong with a few glasses of wine – (compared) to the tik they were using.
Discussion
This study explored the viewpoints of service providers from five residential SUD treatment facilities concerning substitute behaviours and addictions using focus group discussions. The key findings to emerge from the study were that service providers defined substitute addictions as (licit or illicit) substance or behavioural replacements for a terminated primary SUD. Substitutes were believed to emerge gradually or immediately upon abstinence from the primary substance to (un)consciously fill the void. According to service providers, key motives for substitution were functional replacement: to manage cravings; mask feelings and emotions; achieve intoxication, and time-spending. Substitution may also be intentional during periods of forced abstinence or, arise from an initially legitimate use of a licit substance for treatment with awareness only developing later. Social acceptance, legality and/or familial endorsement may influence the nature of the ‘selected’ substitute. The focus group discussions reveal that substitutes may also be engaged after a period of experimentation until the desired appetitive effect was achieved, and, to self-medicate. Substitution may be motivated by deriving insufficient pleasure in the reward centre from prosocial activities (e.g. helping others, exercising, attending recovery support meetings) or, coping with an unmanageable lifestyle. The leading mechanism identified by service providers through which substitute behaviours were thought to arise was co-existing behaviours. That is, service users may present to treatment with a set of addictive behaviours of which they typically identified a primary addiction to be addressed. The secondary, concurrent behaviour that may not be disclosed, may escalate and grow to the strength of an addiction. When the addictive behaviour led to dysfunction the individual was believed to no longer be in recovery. The ‘secondary’- concurrent behaviour - which may have complemented, been masked by the primary addiction, or emerged periodically, may not be addressed or disclosed during treatment (Irons & Schneider, 1994; Sinclair et al., 2021a). Furthermore, service users may minimize the co-existing behaviour (which may be more problematic than the behaviour that is the focus of treatment). The factors that aid in the termination of a primary substance may also differ for another substance or co-occurring addictive behaviour (Downey et al., 2000; White & Kurtz, 2006).
Substitution was most commonly discussed in the context of relapse risk, which service providers sought to mitigate. Therapeutic responses centred on detecting and preventing substitute addictions. While a key challenge remains the lack of a universal definition, it is notable that all service providers aligned with a recent, comprehensive definition of substitute addictions constructed from a scoping review of the literature that defined substitution as “the immediate or gradual functional replacement of an addiction or set of addictions that have been terminated” (Sinclair et al., 2021b, p. 692). Given the array of terms for substitution and lack of standardized terminology, it is also noteworthy that service providers preferred the term “cross addiction”, arguably the most widely used and known term (Sinclair et al., 2022). However, it has been cautioned that addiction should not be applied too loosely and that the substitute should display characteristics of addiction (Sinclair et al., 2021b), such as incurring negative consequences, loss of control, preoccupation and achieving an appetitive effect (Sussman, 2017; Sussman & Sussman, 2011). Recent empirical work on substitution has thus made an important distinction between substitute behaviours and substitute addictions. Conceptualised on a continuum, behaviours have the potential to progress to addictive levels over time, and addictions vary in severity (Sinclair et al., 2021a). Though service providers did discuss the progressive nature of addictive disorders, they did not distinguish substitute behaviours from addictions. Relatedly, conversations concerning substitution centred on relapse risk, and not on harm reduction.
Service providers’ perceptions of the motives for substitution are in keeping with extant literature that substitutes are used for specific outcome expectancies such as managing cravings; achieving intoxication; time-spending; experimentation; due to social acceptance and legality, and, to self-medicate (Chiauzzi, 1991; Sinclair et al., 2021a, 2021b; Sussman & Black, 2008; Sussman & Sussman, 2011). While substitution has been attributed to being influenced/triggered by others (Sinclair et al., 2021a), the role of familial endorsement identified by service providers is an important nuance. ‘Enabling’ behaviours of significant others is known to help precipitate relapse (Chiauzzi, 1991).
Participants’ awareness that service users may present to treatment with an identified primary addiction that they focus upon amidst co-occurring behaviours, aligns with the finding of increased use of/greater engagement in behaviour in the ‘untreated’ addiction in a set of addictions (Sinclair et al., 2021b; White & Kurtz, 2006). Yet, screening for multiple addictions at intake was not a uniform practice. This is in line with a South African study (Keen et al., 2015) on multiple addictions in which 54% and 24% of 123 residential service users in treatment for SUDs respectively, presented with addictions to gambling or sex, and coexisting gambling and sex addictions. However, none of the three participating facilities routinely assessed for the presence of multiple addictions or incorporated its management into the treatment programme (Keen et al., 2015). Multiple addictions may also precipitate reciprocal relapse, wherein a compulsive behaviour triggers relapse to a substance and vice versa (Schneider, 1991). Service providers have been cautioned to recognise that service users may become trapped in a reciprocal relapse pattern upon terminating an addictive behaviour and substituting it with another addictive behaviour (Irons & Schneider, 1994).
The relationship between co-occurring behaviours which may complement, be masked by the primary addiction, or may emerge periodically, relates to Carnes et al.’s (2005) concept of Addiction Interaction Disorder, in which co-existing addictions interact, support and join in 11 distinct patterns. Interactions compound the harms of every addiction and the addiction ‘package’ is more problematic than each on its own (Carnes et al., 2005). Of the 11 meta-patterns of addiction interaction, Carnes and colleagues’ concepts of alternating addiction cycles (the dominant addiction shifts in a patterned, cyclical way), fusion (addictions that are tied together) and masking (using one addiction to conceal another) relate directly to substitute addiction (Sussman, 2017).
A comprehensive assessment of relapse potential is best conducted collaboratively with the service user, wherein the service provider draws upon formal assessment instruments and clinical judgements; the service user, in turn, provides subjective and experiential information (Chiauzzi, 1991). Chiauzzi (1991) offers an empirically-informed relapse risk assessment framework, as an aid to uncovering undisclosed information or information considered unimportant by the service users; a key challenge also identified by participants. The assessment covers the following areas: (1) historical factors (i.e. family, relapse, treatment, self-help, and substitute addictions); (2) biological risk factors (including health, reactivity to cravings and cues, and sensation-seeking); (3) psychological factors (e.g. psychopathology, expectancy, coping strategies); and (4) social factors (environmental and relational dynamics). In doing so, a more transdiagnostic treatment approach can be adopted in which the underlying mechanisms common to both substances and behaviours may be incorporated and targeted (Kim & Hodgins, 2018). Furthermore, as expressed by service providers, the nature of and motive for the substitute are important to consider when assessing its risk for leading to similar or greater harm, relapse and/or the development of another addiction (Horvath, 2006; White & Kurtz, 2006).
Service providers’ contention that vigilance is necessary for recovery is consistent with leaders in the recovery arena that highlight the high risk of relapse, as well as substitute addictions in early recovery (Sussman & Black, 2008; Vanderplasschen & Best, 2021). Substitute behaviours may be an antecedent to relapse by lowering inhibitions and/or detracting from engagement with recovery support. For example, excessive work as a substitute may occupy time that is no longer devoted to substance use and yet may inhibit aftercare compliance, and lead to boredom and fatigue (Chiauzzi, 1991). Service providers asserted that substitution was a sign that someone was not coping or was not using their coping skills. The substitute behaviour may also exact a toll and lead the person to other (maladaptive) coping mechanisms. Recovery capital is closely allied to the availability of alternative, adaptive, appropriate and effective coping skills within the service user’s repertoire that can be applied to high-risk situations (Sinclair et al., 2021a; White & Cloud, 2008). Coping skills, referring here to behavioural or cognitive strategies (Menon & Kandasamy, 2018) may be taught during individual and group sessions where the latter allows for practising new skills, receiving feedback, and modelling others’ behaviour (Moos, 2007). Programmes with the same treatment philosophy may differ concerning the specific treatment interventions used, and the frequency and duration of sessions allocated to developing coping skills. Factors that hamper recovery are conceptualized as recovery barriers (Best & Hennessy, 2022). Thus, there is a need to differentiate substitutes that lead to negative consequences from substitutes that reduce harm and may support recovery efforts. While the complexity and challenges inherent in treating persons with SUDs are not to be diminished (Sharma, 2012), it is equally important for service providers to be critical of their clinical practice. Some facilities appeared to allow smoke breaks while recognising nicotine as a leading substitute in their psycho-educational lectures. Cigarette smoking is associated with an increased risk of relapse to SUDs (Weinberger et al., 2017), as well as the leading preventable lifestyle cause of premature death (Sussman, 2017). Finally, service providers should also recognise that substitution can be a time-limited activity. In this study, temporary substitution was not described as a tool that could potentially be leveraged in early recovery (depending on the nature of the substitute behaviour), but rather as something engaged short-term until desired appetitive effects were derived.
Taken together, our findings underscore the importance of service providers' overt and implicit conceptions of recovery. These beliefs impact the treatment aspirations and recovery goals (e.g. abstinence only) they are willing to support and see as valid. How recovery is framed also has implications for how substitute behaviours and addictions are understood and the belief that they can be leveraged in recovery while remaining vigilant. Service providers with lived experience may play a critical role in scaling up the limited harm reduction services in South Africa.
Clinical Implications
Given that co-existing behaviours were the leading mechanism through which substitute behaviours appeared we recommend that screening for concurrent behaviours and multiple addictions becomes a routine practice. Once the set of behaviours and addictions is established, an assessment should be performed to define their nature, dynamics and interactions. When exploring substitutes, service providers should also be mindful of the relative harm caused (Sussman, 2017), and do a case-by-case risk analysis to determine the service user’s awareness of their “potential danger” (Chiauzzi, 1991, p. 67). However, service providers should also remain aware that substitute behaviours are not only potential threats to recovery that lead to or foreshadow relapse; substitute behaviours may foster recovery (Horvath, 2006). That is, service providers must distinguish between negatively consequential, harmful substitutes and harm reduction, recovery-supportive substitutes. While conceptually understood by all, providers with lived experience appeared less bound to an abstinence-only recovery orientation and more open to harm reduction substitutes. It is plausible that they better understood its potential uses. Substitutes can be used instrumentally, and temporarily to “reduce the process of change to one of smaller, more manageable, steps” (Horvath, 2006, p. 1). The use of “a good substitute” enables one to alleviate cravings for the original addictive behaviour while reducing harm, and with time, cravings will dissipate (Horvath, 2006, p. 2). Recovery status has been found to influence treatment approach: service providers in recovery have been found to adopt a wider range of treatment techniques and goals than their professionally-trained counterparts (Stöffelmayr et al., 1999). The dynamics observed in FGD 3 also appear to support Stöffelmayr and colleagues’ finding (1998) that service providers in recovery believe that other staff wield more power over administrative and clinical decisions. Within the broader framework of harm reduction, we also found substitution between illegal and legal substances of relevance for understanding and preventing relapse. Legality is a known motive for substitution as people with SUDs may want to reduce legal problems. However, in a study of treatment attendees in Israel, legality was the least frequently reported motive for substituting (Shapira et al., 2021).
While some service providers screened for multiple, co-occurring addictions, it did not emerge that screening for substitute behaviours or behavioural addictions existed as a routine practice. Many psychometric assessment tools are being developed for specific behavioural addictions based on the ‘components model of addiction’, even in the absence of diagnostic criteria. Sussman and colleagues’ (2011) Addiction Matrix Self-report measure, a listing of 29 substances and behaviours may form part of screening and assessment at intake (see Sinclair et al., 2021a). Furthermore, measures such as the Strengths and Barriers Recovery Scale (Best et al., 2020) could enable service providers to compare recovery strengths and deficits during active addiction and in recovery, to inform treatment planning.
Limitations
The findings from this study should be considered in light of its limitations. Our sample represents a limited number of service providers from one South African province and residential facilities with an abstinence-based philosophy. Therefore, the views expressed may be unique to such settings and programme philosophies. Furthermore, while only three participants identified as being in recovery, interactions with them suggest that their lived experiences were not equally valued. For example, whereas in FGD 1 lived experience was considered vital for programme delivery (e.g. monitoring service user progress, and educating them about relapse), in FGD 3 the social worker with lived experience appeared to be harshly challenged about their perceptions. These power dynamics limited a deeper exploration of alternative recovery models. In addition to exploring substitute addictions with service providers in other contexts, a high priority for future research is to recruit diverse service provider participants that represent varied practitioner types, lived experiences, treatment philosophies and settings. Additional research is also necessary to elucidate co-existing behaviours and substitution.
Conclusions
This study has demonstrated the importance and value of understanding how service providers conceive of substitution and its etiologic mechanisms and draw on these views to inform their decision-making and practice. Given the relatively limited literature base on substitute behaviours, these findings represent a critical first step toward implementing good practices and optimizing recovery outcomes.
Footnotes
Acknowledgements
The authors wish to thank Joan Sarah Isobell for her editorial support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ghent University’s Special Research Fund (BOF) for Candidates from Developing Countries, and the National Research Foundation South Africa (grants 107586 and 121068).
Author Biographies
![]()
![]()
![]()
![]()
![]()