
Abstract
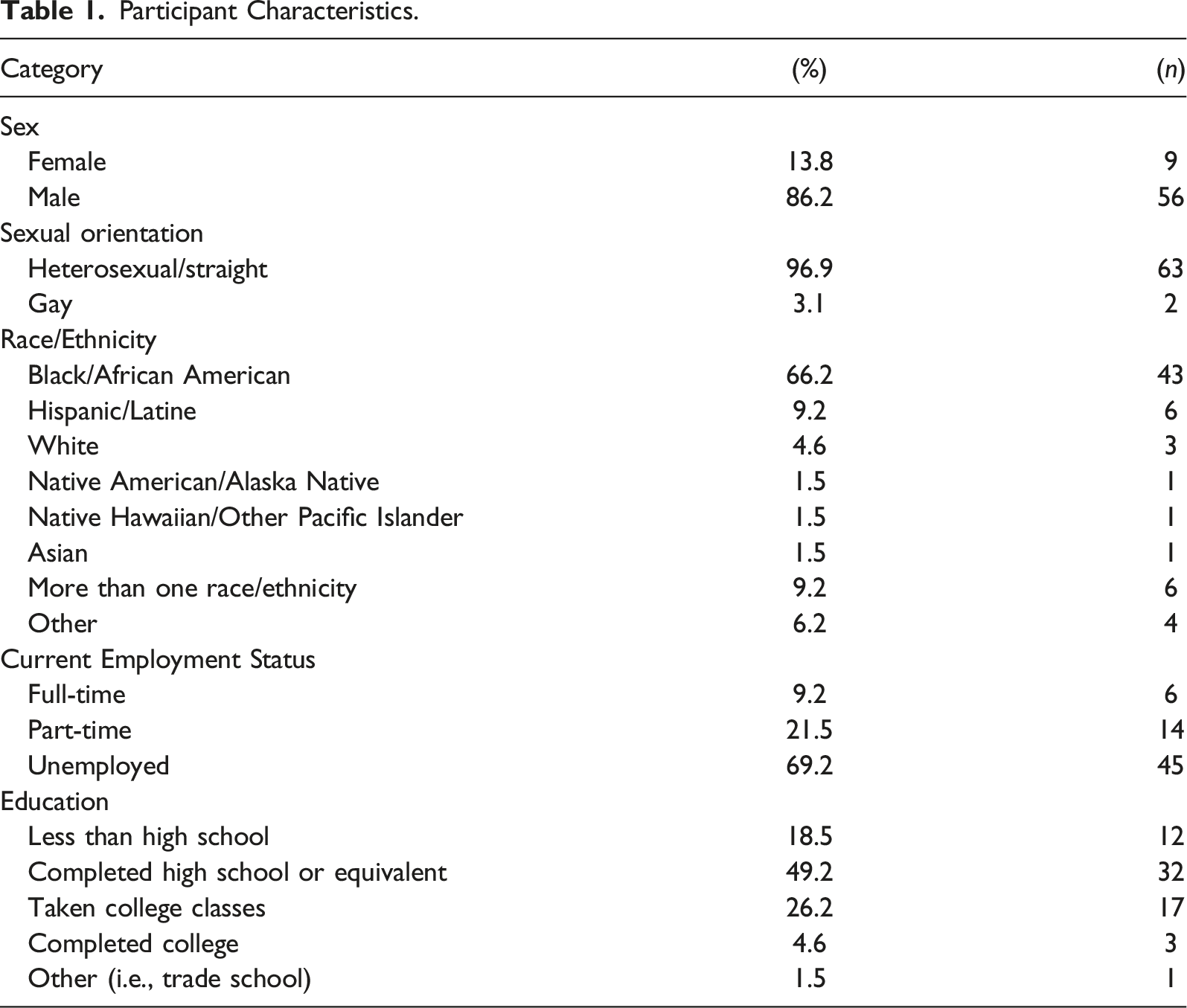
Synthetic cannabinoids (SCs) are low-cost substances that have been associated with adverse health outcomes and an increase in emergency department visits over recent years, particularly among people experiencing homelessness. This mixed methods study explored the connection between homelessness, SC use, and readiness to quit in order to inform the development of harm reduction strategies. Individuals (18+) residing in homeless encampments in Houston, TX with experiences of SC use were eligible to participate. Participants (N = 65) completed an interviewer-administered survey about their SC use. Most participants were Black/African American (65.7%), male (82.9%), and most (75.4%) reported using SCs to avoid positive drug tests. Many wanted to quit using SCs (69.2%) and already employed harm reduction strategies while using SCs. Organizations supporting individuals experiencing homelessness who use SCs should focus on reducing barriers to stopping SC use and increasing the availability of housing and supportive services.
Introduction
Within the past decade, the rise of designer drugs like synthetic cannabinoids (SCs) has brought this substance use problem to the forefront as a public health priority (Weinstein, Rosca, Fattore, & London, 2017). SCs (commonly known as K2, Spice, and ‘kush’ in some regions) are manmade chemicals that consumers use as an alternative to marijuana (Centers for Disease Control and Prevention [CDC], 2018; Yeruva, Mekala, Sidhu, & Lippman, 2019). Many SCs are legal, easily accessible, and low cost in the U.S. (Drug Enforcement Administration (DEA), 2017). They are sprayed onto products such as incense and are marketed as “a legal high” (Bush & Woodwell, 2014; Yeruva et al., 2019), difficult to regulate because manufacturers of SC make products with different ingredients to get around U.S. state laws banning specific SC ingredients (CDC, 2021). SC products are commonly sold as “Spice” brand products, herbal blends, and incense (Vandrey, Dunn, Fry, & Girling, 2012). They look like and are marketed as potpourri and sold under names such as Spice Diamond, Black Mamba, ChillX, and Pandora’s Box (DEA, 2017; Gunderson, Haughey, Ait-Daoud, Joshi, & Hart, 2012; Müller, Kornhuber, & Sperling, 2016; Zarifi & Vyas, 2017). An increase in calls to national poison control centers [to report incidents of SC toxicity and adverse effects] in 2009 intensified concerns of SC use in the U.S. (Gunderson, 2013).
The effects of SCs can be felt within 10 min and can last between two to 6 hours (Weaver, Hopper, & Gunderson, 2015). Symptoms of SC intoxication include severe agitation, anxiety, nausea, vomiting, tachycardia (racing heartbeat), myocardial infarctions, elevated blood pressure, seizures, hallucinations, paranoia, non-responsiveness, and suicidal and homicidal thoughts (Babi, Robinson, & Maciel, 2017; Bush & Woodwell, 2014). Acute cardiac-related morbidities, particularly tachycardia, are among the most common effects experienced by SC users seeking emergency department (ED) care (Alipour, Patel, Shabbir, & Gabrielson, 2019). Other clinical symptoms include delusions, panic attacks, and psychosis (Gunderson, Haughey, Ait-Daoud, Joshi, & Hart, 2014; Müller et al., 2016). Psychosis, delirium, and agitation are among the most reported psychiatric signs of SC toxicity (Alipour et al., 2019). The potential for more serious complications, such as acute renal and respiratory failure have also been reported, even in otherwise healthy patients (Gunderson et al., 2014; Zarifi & Vyas, 2017). Calls to the poison control center in the state of Illinois identified 155 cases of individuals experiencing serious complications following use of contaminated SCs (Alipour et al., 2019; Moritz et al., 2018; Yeruva et al., 2019). Of these cases, 4 individuals died from major bleeding, 147 individuals were hospitalized, and 8 individuals required care in the ED (Alipour et al., 2019).
Recent studies document a notable increase in SC use among older individuals and individuals experiencing homelessness (Joseph, Manseau, Lalane, Rajparia, & Lewis, 2017; Maxwell, 2018). A study in an emergency psychiatric setting concluded that homelessness (sheltered and unsheltered) was the characteristic most correlated with SC use (Joseph et al., 2017). People experiencing homelessness reported use of SCs as a source of relief against difficult physical living conditions, to be able to sleep in vulnerable outdoor environments and public spaces, to keep warm, forget their problems, and to pass the time (Gray, Ralphs, & Williams, 2020). Individuals experiencing homelessness report replacing other drugs of choice, including heroin and crack cocaine, with SCs (Gray et al., 2020). SCs have been described as more addictive than other substances (e.g., crack cocaine and heroin), and individuals experiencing homelessness have reported continued use to avoid withdrawal symptoms (Gray et al., 2020).
People experiencing homelessness may experience more adverse outcomes following SC use, including theft and robbery (Ellsworth, 2019). The use of SCs among individuals experiencing homelessness also leads to loss of consciousness and the need for emergency medical care (Gray et al., 2020). An outbreak investigation of adverse outcomes of SCs determined that people experiencing homelessness were involved in 39.5% of SC ED visits, and this proportion was likely underestimated (Springer et al., 2016).
Individuals experiencing homelessness engaged in SC use are uniquely positioned to provide information about SC use and supportive strategies relevant to their circumstances. This includes harm reduction strategies for individuals who wish to continue to engage in SC use as well as recommendations for services needed to support individuals who wish to stop using SCs. To the best of our knowledge, there are no studies documenting harm reduction, treatment-seeking, and stages of change for SC use among individuals experiencing homelessness. The latter, a concept of the Transtheoretical Model (TTM), posits that individuals move through the change process in five stages: precontemplation, contemplation, preparation, action, and maintenance (Ramo, Thrul, Vogel, Delucchi, & Prochaska, 2020). The TTM is a useful framework oftentimes used in understanding risk behaviors and for the development of related interventions (Ramo et al., 2020).
In a previous study examining the process of quitting substance use with individuals receiving treatment for substance use disorder (SUD), participants’ lives in the contemplation stage [prior to treatment] were characterized by chaos, near-death experiences, and homelessness (Gressler et al., 2019). Another study with individuals receiving inpatient treatment for SUD described participant awareness of the harms associated with substance use early on, but this awareness did not always lead to treatment-seeking (Årstad, Nesvåg, Njå, & Biong, 2018). Furthermore, a previous study with young adults engaged in substance use report that barriers to treatment include waitlists and cost (Noyes et al., 2022). Another study noted that adults aged 50 years and older and non-white adults were more likely to lack access to substance use treatment, highlighting that less than 30% adults receive treatment for opioid use disorder (OUD) (Saini, Johnson, & Qato, 2022). Another recent study concluded that people who use illicit opioids and have children face unique challenges in accessing substance use treatment programs. Specifically, women engaged in illicit opioid use and who live with children are more likely to avoid accessing substance use treatment programs for fear of involvement with child welfare agencies and are less likely to be trained to use Naloxone (Scheidell, Hoff, Khan, Bennett, & Elliott, 2022). The purpose of the present study is to describe the harm reduction strategies utilized by individuals experiencing homelessness as well as their efforts to cut down and quit using SCs.
Methods
Recruitment and Sample
This study was initiated and supported by a Houston community-based organization serving individuals experiencing homelessness, guided by the principles of Community Action Research. Data collectors visited two homeless encampments with outreach workers employed at the partnering community organization, who were familiar to the encampment residents, in order to ensure the comfort and trust of participants. The two homeless encampments where data collection took place were identified by the homeless service outreach team as areas with frequent SC use.
Utilizing a purposive sampling strategy, recruitment and data collection focused on English-speaking individuals over the age of 18 (N=70) who were at one of the two selected homeless encampment sites at the time of the study and had present or past experiences with SC use. Individuals at the two homeless encampment sites were approached and prescreened for eligibility. Participants received $5 for their participation in the study.
Data Collection
Cross-sectional surveys with closed and open-ended questions were conducted over several weeks during October of 2018. The data collectors visited the encampments a total of eight times and conducted anonymous interviewer-administered surveys lasting approximately 30 min. The instrument used in this study was a modified version of a survey used in a study with young adults (Gunderson et al., 2014). With permission from the authors, the survey instrument was chosen because it was one of a few published survey instruments administered to individuals engaged in SC use at the time of the present study. The adaptations made were minor language changes (e.g., options added to multiple choice questions) to make the instrument culturally relevant for individuals experiencing homelessness. One of the unique benefits of the community-academic partnership is the opportunity to gain insight on the language that was most culturally appropriate for individuals experiencing homelessness and engaged in SC use. For example, the use of the term ‘kush’ for SCs, since that reflects the language that was used in the local community/population. Additionally, instead of comparing SC use to marijuana, we asked participants of our study to compare it to their drug of choice. The 43-item survey contained open-ended and close-ended questions including demographics, self-protective strategies, and suggestions for support programs and initiatives. Open-ended items were structured, short answer questions. In order to best capture the responses to the open-ended items, participants were asked if they would be comfortable having the conversations recorded using password-protected encrypted tablets and saved under pseudonyms selected by participants.
Several of the open-ended items in the survey, including participant readiness to stop using SCs, were developed using the constructs under the TTM (Prochaska & Velicer, 1997). The constructs under the TTM were measured using the Readiness Ruler (RR), which asks participants to rate their readiness to cut down or quit using a substance on a scale from 1-10 (Hesse, 2006). The TTM is regularly used in research to describe the gradual process of quitting addictive behaviors, and the stages of behavior change include precontemplation, contemplation, preparation, action, maintenance, and termination of the behavior (Bartholomew Eldredge et al., 2016).
Data Analysis
The audio-recorded, pseudonymized conversations with participants were transcribed by graduate students, and a selection of relevant quotes from participant responses to the open-ended questions are embedded in the results of this article. All transcripts were read thoroughly by the team of graduate students and verified by Author ACV, who compared the transcripts to both the audio recordings and the quantitative data to ensure that all of the data collected for each participant matched. The open-ended items in the transcripts were then analyzed further, with the goal of identifying dominant categories and topics in the data. Dominant categories and topics in the open-ended data were then compared to participant responses in the close-ended data to ensure thematic alignment and consistency. An analysis of the dominant categories and the comparison of these to the close-ended survey data provided a more holistic understanding of participant experiences. Quotes from the open-ended data were selected in order to provide additional context and depth to the quantitative data. Data from close-ended, quantitative survey items were analyzed using IBM SPSS Statistics (version 27) (IBM SPSS statistics for Windows. 2017, 2021). The quantitative data includes descriptive statistics, particularly measures of frequency (e.g., percentages and counts).
Institutional Approval
Approval for this study was granted by the University of Texas Health Science Center at Houston (UTHealth) Institutional Review Board (IRB). All participants provided verbal informed consent to participate in the study.
Results
Participant Characteristics
Participant Characteristics.
Reasons for SC Use
The majority of the participants were current SC users at the time of data collection (n = 50, 76.9%), and more than half reported using SC “everyday” (n = 42, 64.6%). Most participants were aware that SCs are harmful for human consumption (n = 55, 84.6%) but used SCs to avoid a positive drug test (n = 49, 75.4%), to sleep (n = 46, 70.8%), and because they are easy to find (n = 45, 69.2%). Study participants also mentioned that using SCs curbed irritability (n = 38, 58.5%) and were more affordable than their other drugs of choice (n = 38, 58.5%). Half of study participants were also drawn to SCs because the high from SCs is stronger than the high with their drugs of choice (n = 33, 50.8%). Over half of study participants stated that marijuana was their drug of choice (n = 20, 58.8%). More than half of participants stated that they would not use SCs if marijuana were legal (n = 40, 61.5%).
Readiness to Stop SC Use
Most participants indicated that they would like to stop using SCs (n = 45, 69.2%), and another 15.3% of participants (n = 10) had already stopped using SCs at the time of the study. The remaining participants (n = 10, 15.3%) did not wish to stop using SCs. On a scale from 0 to 10, 40% of participants (n = 26) rated stopping SCs use as “very important” (score of 10) while a smaller percent (n = 16, 24.6%) of participants reported feeling “very confident” (score of 10) in their ability to stop using SCs.
Most of the participants were in precontemplation or determination, with only 9 participants in the action stage. There were no significant differences in the reported stages of change of the participants by demographic or SC use characteristics (p>.05).
More than half of participants reported previous attempts to stop using SCs (n = 38, 58.4%), with 10 participants describing multiple past quit attempts (15.3%). Reasons for stopping SC use included health concerns, fear of death and other adverse health consequences, legal consequences such as arrest, and financial motivations. One participant who was on parole at the time of the study shared that they, “eventually want to start using weed again when off parole.” Other participants experienced legal consequences and criminal justice involvement, and avoiding these experiences was motivation to stop using SCs. As one participant put it, their main motivation to stop using is, “legal consequences. I’ve gotten arrested before.”
Several others shared witnessing SC users becoming ill or dying, and one participant shared, “I saw a lot of people, my friends, die smoking this stuff. Someone just died the other day, a white guy. He was laying on the sidewalk, everybody thought he was asleep. He was smoking kush [SCs] the night before.” The financial burden of purchasing SCs was also a motivation for some participants. One participant shared that, “It’s too expensive to keep buying kush [SCs].”
Personal health concerns were also mentioned as motivations for stopping. One participant shared, “I’m a diabetic and it’s messing with my health. Breathing problems, stomach problems, not eating right.” Another stated, “I’m pregnant, 7 months.... I have been smoking kush [SCs] and crack during my pregnancy.” Other participants shared that their desire to stop using SCs was motivated by previous bad experiences with the drug. One participant said, “It makes you sick and if you don’t get more you get sick.” Another shared that, “I thought I was going to die.” Another study participant shared that they wish to stop because they, “want to hurt people during it.” For one participant, the motivation to stop using was, “not knowing where I was at” after using SCs.
In an additional open-ended item about previous negative experiences with SCs, participants commonly shared experiences about hospitalizations and ED visits, being victims of robberies, and previous experiences with being violent toward themselves and others. Less common were experiences with vehicular accidents, vision problems, and being victims of rape/sexual assault.
Challenges Stopping SC Use
Participants shared previously unsuccessful attempts to stop using SCs. Some participants quit using while incarcerated. One participant shared that they only stopped because they were incarcerated, “2014-2016, I didn’t smoke because I was in jail…” Another participant shared that they were also forced to quit using SCs while incarcerated, “the only time I ever really tried [quitting] was when I went to jail…Didn’t really feel different [referring to withdrawal symptoms].” Other participants shared that their attempts to stop using SCs were thwarted by difficulties with stress and mental health challenges. As one participant shared, “I went 6 months without it and started using it again because I lost a family member.” Another participant stated, … I feel like kush [SCs] is the only thing that can take care of my depression. When I smoke, when I get high, that—that is the only time I feel like I’m not depressed. Other than that, I am always thinking about my loved one. And then I just recently lost another relative. Like last two months.
Other stressors also caused relapse among participants. One participant shared, “I tried to stop using kush [SCs], but I got very angry and sick and had to smoke…” Another stated, “…it was fine but something happened and I got upset.” Another participant stated, “I tried, but didn’t succeed…from stress and dealing with other people and a close death in family that made me unbalanced.”
One of the most common deterrents to participants’ attempts to stop using SCs was the addictive nature of SCs. Participants describe SCs as an addictive substance to which they have built dependence. One participant shared, “I tried for about 2 months. I tried leaving and going to hang out in other places and do other things. But I came right back, it’s like a magnet.” Another individual stated, “I did good for two months, and then I ended up relapsing. I only smoked one time and that is all it took.” Another individual described their experience as, “…not well. I tried to stop and it only lasted a few hours. Made me nauseous and I needed it.” One participant shared, I did not use for about 3 days, and I had no withdrawal or nothing. I went downtown and then I smoked some. I ended up waking up… in the middle of the street. It is worse the longer you go without using because not everyone gets withdrawal. But when you use after a few days without it, you fall out.
Other participants shared experiences with withdrawal symptoms while trying to stop using SCs. One participant shared, “I started to have withdrawal like a heroin addict--- sweating, throwing up, peeing on myself, defecating on myself. I had to take pills to build my system back up [vitamins].” Another stated, “the first time I tried to stop, I went through some withdrawal… pain in stomach, made me sleepy or irritable…” Additionally, other participants shared, “I ended coming right back in and getting some more. It does cause a lot of anxiety when you don’t have it” and “…it was hard. I went through withdrawals with sweating. I didn’t feel good for a couple of days…” Another participant stated, “…the first time took a week and bad with nausea, could not sleep waking up with hot sweats…”.
Safety and Harm Reduction Strategies
During the interviewer-administered survey, participants were asked to share some of the ways that they keep themselves safe while using SCs. The most common responses focused on staying with friends or trusted acquaintances (n = 15, 23%). One participant explained that they, “Hang out around people who have the same trip that you do. Make sure you around people that won’t mess with you. You don’t want to be around people who let you run into the street.” Another shared, “I don’t usually be around a lot of people, and if I am, it has to be someone I am very, very familiar with. I also roll my own blunts because you never know what people put in pre-rolled blunts.” Another participant stated that they prefer to be, “Sitting around positive people. I don’t like crowds of people. When you are in a crowd of people, something will start. People will steal your stuff.”
For other participants (n = 15, 23%) staying safe meant isolating themselves from crowds and unfamiliar people in order to avoid being victims of robbery and violence. Avoiding robbery was a common concern, as shared by one participant, “I try to be by myself because they are going to steal whatever I got if I go to sleep.” As one participant shared, “One, I leave this area. Two, I stay alone by myself. Three, I look at my surroundings for any suspicious persons eyeballing or lurking. Just stuff that could get me in trouble or get me hurt.” Another participant explained, “When I do smoke kush [SCs], I go somewhere where I know I will be safe if I dose off or be around someone who can look after me.” One participant shared that he avoids using SC around specific individuals, such as the police, pregnant women, and children. The participant stated, “I stay away from other people. I stay in a safe environment with people who I know are not going to trip and hurt me. A place where there is no pregnant women or children. Or police.”
To avoid robbery and theft, participants carefully curated the environment where they smoked SCs. Participants stated that they avoided passing out and secured their personal belongings. One participant said they, “put stuff in pockets, secure belongings”. Another stated, “I just put my stuff on my backpack and sleep on my backpack.” Another common way that people kept themselves safe while using SC was to prioritize hydration. Participants shared that they keep fluids like water and milk nearby. One participant said that they, “…sit back chill and relax. Have some water nearby.” Another shared, “I keep a lot of fluids around: Gatorade, water, bananas, cantaloupes, apples. Stuff that is not so hard on your body. You gotta keep fluids in your body. That kush [SCs] will dry you up, and you will be dead around here.” Other strategies that participants utilized in order to stay safe included exercising, eating, sitting down, rolling their own blunts (avoiding pre-rolled blunts), and pacing themselves (not putting as much kush [SCs] into a blunt or joint).
Community Support Initiatives
Participants of this study were asked about things that local programs and organizations can do to support people using SCs and to help people who wish to do so stop using SCs. Several participants suggested community outreach. As one participant stated, “Come out and ask them. Outreach workers need to earn trust and spend time with people, they need to be non-judgmental. Don’t tell people what to do, motivate them…. keep trying….” Other participants suggested jobs, job training, housing, education, and access to medical care. One participant explained, “Help people get into programs that will help them reconstruct their lives. Help people rehabilitate. Help with the stress of living out here.” Another stated, “getting into housing, wouldn’t have to worry about stress as much.” Yet another shared the need for “jobs, housing, providing a way to get out of homelessness.”
Several participants mentioned that there are no rehabilitation and detox programs for SCs and suggested that it is necessary to, “…have a 12-step program for kush [SCs], like for alcohol.” Another participant shared, “people have to make the decision but maybe help with withdrawals like throwing up,” suggesting that support with withdrawals may be helpful for individuals trying to stop using SCs. Another participant stated that it would be helpful to, “try to have some kind of a rehab for that stuff. If they want to stop...if they do not want to stop, let them do what they want to do. To each their own.”
To address the lack of information around SCs, several participants suggested that education and awareness building would also be helpful for individuals who use SCs. As one participant stated, “…teach about the effect of kush [SCs] and what in can do and what harmful effect it can do.” Another individual stated that it would be helpful, “If people were more knowledgeable about what is it, how to treat it, and how to diagnose it. But they don’t know, so you can’t get any help.” One participant suggested, “…research, flyers showing people what smoking leads to.” Another recommended, “education classes to make people more aware of long-term use…”
Providing safe spaces, social support, and opportunity for recreation were also mentioned several times by participants. One individual stated, “Give us a safe haven; a place to get away from it.” Another suggested, “get them away from it off the streets filling time with other things.” Participants listed “having something to do” and “not so much exposure and proximity to it” as ways to support individuals who are using and/or wish to stop using SCs.
The legalization of marijuana and participant preference of marijuana over SCs came up throughout the conduct of this study. Several participants shared that the legalization of marijuana will help them stop using SCs. One participant explained, “push the legalization of marijuana. Marijuana relaxes you, helps you think better.” Another participant shared a few ways that could help individuals experiencing homelessness who are using SC including, “Getting involved in a lot of activities. Helping others. Legalizing cannabis. Nonprofit organizations come together to help the community to help people get off kush [SCs]….”
Discussion
Most of the participants of the present study indicated that they wanted to stop using SCs, but with low perceived confidence in their ability to quit. Challenges in past quit attempts were reported, including serious withdrawal symptoms such as “hot sweats,” nausea, trouble sleeping, vomiting, stomach pain, sleepiness, and irritability. Study participants reported SCs as being more addictive and affordable than their drugs of choice, such as crack cocaine and heroin (Gray et al., 2020).
Participants of this study highlighted how easily accessible and affordable SCs are, as well as their notable intensity and quick high. These characteristics have been previously outlined as reasons why SCs may appeal to individuals experiencing homelessness (DEA, 2017). Study participants believed that SCs were harmful for human consumption, but used them regularly in lieu of marijuana (CDC, 2018; Gunderson et al., 2012). Because SCs do not appear on drug tests like marijuana and other drugs of choice, participants of this study use SCs in order to avoid a positive drug test for parole or probation (Bush & Woodwell, 2014). As reported in other studies with individuals engaged in SC use, marijuana was the primary drug of choice for most of the participants of the present study (Gunderson et al., 2012).
Individuals who unsuccessfully tried to stop using SCs stated that their mental health, stress, living conditions, and the quality of the high from SCs were challenges to quitting. Another study with individuals quitting substance use indicated that participants’ lives were chaotic, they faced homelessness and near-death experiences, which aligns with the experiences of the participants of the present study (Gressler et al., 2019). One participant stated that they were unable to stop due to, “My living arrangements. It just had a lot to do with me being outside.” It has been previously reported that, for people experiencing homelessness, SCs provide a relief against difficult living conditions (Gray et al., 2020). In alignment with a previous study with individuals quitting substance use, the participants of the present study were aware of the harms of SC use, had experienced adverse consequences after SC use, and believed SCs to be harmful for human health. However, such awareness does not always motivate participants to seek treatment (Årstad et al., 2018). When asked why they were unable to stop, another participant stated, “I don’t know; I still just wanted that high. Still looking for that high. That superhigh. Marijuana you are on cloud 9, you hit kush [SCs] and you are in the orbit.” In addition to dependence and withdrawal, the low cost of SCs, the intense high, and the ubiquitous nature of SCs drew individuals back in.
The findings provide insights into potential harm reduction strategies that are contextually relevant to the SC users experiencing homelessness in Houston, Texas. Protective strategies cited by participants included staying hydrated, limiting how much SC goes into a blunt, and rolling their own blunts. There does not seem to be a consensus about whether using alone or with others is safer, but individuals who use with others mentioned using around trusted individuals, with people who can keep an eye on each other, and around individuals who experience the high similarly. Community interventions to reduce harms associated with SCs should consider distributing food, water, and information about the symptoms and complications of SC use as well as harm reduction strategies. At the time of the present study, there were no SC-specific services in Houston, Texas. There are general recovery services for individuals engaged in substance use in the area, though stigma and the criminalization of substance use may lead to hesitancy in accessing these services.
Limitations
This study has several important limitations. The point-in-time nature of the cross-sectional data collected does not lend itself to establishing causal relationships or identifying longitudinal trends due to the setting of study and the demographics of both Houston and homeless encampments. Self-reported data are also subject to several types of biases, including social desirability bias and recall bias. Additionally, reliance on a small sample and subset of the population limits its generalizability. Further, while semi-structured interviews could have provided a richer understanding of participant SC use as well as the circumstances that facilitate or hinder harm reduction and attempts to cut down and/or quit SC use, such methodology was not possible due to time and resource constraints. Despite these limitations, this study makes an important contribution to the exploration of an understudied and poorly understood substance. The dearth of research and public health programming on SC use among homeless and unstably housed adults paired with the rise in adverse outcomes makes the cross-sectional design’s cost-effectiveness and simplicity worthwhile in the process of determining time-sensitive interventions to address the growing community need.
Conclusion
Individuals experiencing homelessness use SC as an affordable alternative to marijuana, and to cope with their living conditions and circumstances. Organizations looking to support individuals experiencing homelessness who use SCs should consider focusing on addressing mental illness and chronic stress. Housing strategies were also recommended by participants, particularly initiatives that enable participants to move from homeless encampments and gain more stability. Future research observing longitudinal trends in SC use are needed to understand people’s experiences while in detox and predictors of use. More research is needed about a range of topics, including policing related to SC and emergency responses to SC intoxication. Future studies should also consider utilizing in-depth qualitative interviews and ethnographic methods in order to understand the experiences of individuals engaged in SC use.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the SEARCH Homeless Services and Robert Wood Johnson Foundation.