
Abstract
Engagement in “chemsex” among men who have sex with men is associated with higher rates of STIs and HIV seroconversion as well as an increased mental health burden. MSM were recruited for an anonymous online survey. The survey included questions of substance use, consumption motives, sexual risk behavior, HIV serostatus, and psychological characteristics. A latent class analysis was used to identify subgroups based on the consumed substances. 597 MSM answered the questionnaire. The latent class analysis revealed four different clusters. Most men described the use of amyl nitrite and cannabis (n = 370). One cluster consumed mainly MDMA, cocaine, and amphetamine (n = 106) and another cluster used mainly chemsex-related drugs (n = 43). A fourth cluster reported a range of consumed substances (n = 78). This cluster reported higher rates of suicide attempts, STIs, and risk behaviors. Substances typically related to chemsex were consumed in a sexualized context to a relevant extent.
Introduction
Substance use among men who have sex with men (MSM) is higher than in comparable non-MSM samples (Hunter et al., 2014). Substances like 3, 4-Methylendioxy-N-methylamphetamine (MDMA) and cocaine are commonly used in gay party scenes and are sometimes, among other substances, referred to as “club drugs” (Drumright et al., 2006). Another phenomenon of increasing importance among MSM is “chemsex,” the planned sexual intercourse with changing partners under the influence of so called “chems” (Giorgetti et al., 2017). The term “chems” usually refers to a range of synthetic drugs like mephedrone, methamphetamine, γ-hydroxybutyric acid (GHB) or γ-butyrolactone (GBL), and ketamine (Giorgetti et al., 2017; Schmidt et al., 2016). High prevalence of chemsex has been reported for certain metropoles with well-established gay communities (Schmidt et al., 2016).
Main reported motives for chemsex are not only enhanced sexual performance and increased sexual pleasure but also the feeling of belonging and destigmatization (Deimel et al., 2016). Methamphetamine as a psychostimulant especially intensifies sensitivity, can maximize sexual pleasure, and enhances the feeling of intimacy. It might, therefore, help to establish relationships and facilitates sexual intercourse with more partners over a longer period of time (Graf et al., 2018). On the other hand, prolonged intercourse, disinhibition, and decreased sensation of pain are often associated with sexual practices like unprotected anal intercourse with partners of unknown HIV serostatus or fisting, which increases the risk of STI transmission or injuries (Deimel et al., 2016; Dirks et al., 2017; González-Baeza et al., 2018; Schecke et al., 2019; Sewell et al., 2017). Previous studies have also shown the association between methamphetamine consumption and HIV seroconversion in sexually active men, especially with concurrent use of cocaine, amyl nitrite, alcohol, or erectile dysfunction medications (Plankey et al., 2007; Shoptaw et al., 2012). While on the one hand cross-sectional studies reveal associations between the sexualized consumption of certain substances and poorer health outcomes, on the other hand there is an emerging controversy regarding the lack of causal explanations and pathologizing of chemsex engagement (Bryant et al., 2018).
Studies using statistical approaches to identify different clusters found three to six subgroups of MSM with substance use, including individuals engaging in chemsex (Achterbergh et al., 2020b; Card et al., 2018; Lim et al., 2015; Melendez-Torres et al., 2018). Most analyses distinguished a cluster of men with no or negligible drug consumption against several clusters of men using “chems” in terms of chemsex or polyvalent substance users (Achterbergh et al., 2020a; Achterbergh et al. 2020b; Card et al., 2018). Comparisons of these subgroups confirmed associations of polyvalent use with various risk behaviors. Polyvalent users had the highest tendency to risky sexual practices and the highest prevalence of sexually transmitted infections (STIs) including HIV (Achterbergh et al., 2020b; Melendez -Torres et al., 2018; Schecke et al., 2019). Users of this subgroup and men engaged in chemsex were more likely to have unprotected anal intercourse, with a higher number of partners, and were more likely to take pre- or post-exposure prophylaxis (Achterbergh et al., 2020a; Achterbergh et al., 2020b; Card et al., 2018; Lim et al., 2015; Melendez -Torres et al., 2018; Wong et al., 2020).
Among healthcare providers, awareness for MSM engaged in chemsex is rising, but further understanding of their potential psychological and social problems might improve the quality of treatment and advice particularly in more general counseling and medical centers. Recent findings link engagement in chemsex to higher self-reported anxiety and depressive symptoms (Bohn et al., 2020; Pufall et al., 2018). Especially the consumption of methamphetamine in sexual settings has been associated with depressive symptoms, anxiety, and symptoms of PTSD (Schecke et al., 2019). This is of importance in the face of studies finding MSM disproportionally affected by psychiatric disorders and symptoms like panic attacks or depression (Cochran & Mays, 2000; Cochran et al., 2003; Sandfort et al., 2001). However, this susceptibility might at least in parts be caused by further factors, like minority stress (Meyer, 2003). Further, psychosocial problems are associated with an increased risk for HIV infection (Mustanski et al., 2007), which might be important for prevention and the development of harm reduction strategies (Cochran & Mays, 2000). Other authors propose that HIV prevention and therapy in MSM might be more effective if it also addresses psychiatric symptoms and psychosocial issues (Safren et al., 2011). Nevertheless, these aspects need to be discussed in a wider framework since recent research revealed that even screening for mental disorders in combination with health-related advice does not have an impact on help-seeking and risk-taking behavior in MSM with psychiatric symptoms (Achterbergh et al., 2021).
The objective of this study was to gain a better understanding of the characteristics of MSM with substance consumption in general and in a sexual context to inform preventive strategies for potentially existing subgroups. For this, we analyzed the substance use and potentially relevant co-variables among a broad population of MSM. The hypothesis was that different subgroups with regard to their consumption patterns exist, including at least one group using substances in a sexual context, and that these subgroups would also differ with regard to mental health burden, sexual risk behaviors, and the prevalence of STIs.
Materials and Methods
Recruitment
An anonymous online survey was carried out from August 5, 2016 to January 3, 2017. The survey was developed in cooperation with institutions in the field of sexual health in Germany, including a large network in the field of HIV prevention and psychosocial counseling for MSM. Central supporting institutions were the German AIDS Service Organization (DAH) and regional AIDS Services in Berlin, Cologne, and Munich as well as initiatives that promote safer use information in nightlife and festival settings, including Leipzig-based Project Drug Scouts.
To reach a broad range of MSM, the survey was promoted online by the supporting institutions, on regional and national websites directed at the gay community members, in online magazines, and through social networks such as Facebook. It appeared on websites of online magazine for fashion or travel as well as in social media groups that address MSM health, culture, and HIV-related topics.
According to the responsible Ethical Review Board (Chamber of Physicians, Federal State of Hamburg), no ethical concerns arose.
Online Questionnaire
The questionnaire covered age and basic demographics as nominal or ordinal values, for example, sex, size of city, employment, and relationship status.
We included homo- or bisexual men as well as heterosexual men with same-sex intercourse. Drug experience of any kind was an inclusion criterion. We excluded participants of female or other sex or with missing statement on sexual orientation.
We asked for the consumption of alcohol and illicit substances, including chemsex-related drugs such as ketamine, methamphetamine, GHB/GBL, and mephedrone in a ordinal scaled response options (“never”/“within the previous 30 days”/“within the previous 12 months”; Giorgetti et al., 2017; Schmidt et al., 2016). Reasons for consumption of the respective substance were collected nominally scaled (“rather in a sexualized context”/“rather other contexts”/“both”).
Self-reported psychiatric symptoms, HIV, and other STIs were reported dichotomously (“yes”/“no”), with the number of partners as a free text. Depending on their self-reported HIV serostatus, participants were asked more specific dichotomous questions, for instance concerning the use of antiretroviral medication, pre-exposure prophylaxis, and sexual risk-taking behaviors (“yes”/“no”).
Participants were not remunerated. The participation was anonymous and voluntary. The data security and privacy concept developed for this study did not allow to count or analyze datasets that were not completed and authorized by the participant by clicking a “send” button. Unsent datasets were, therefore, not imported from the survey tool and were deleted after the final data import. Participants were informed about this approach before entering the survey. We additionally conducted plausibility checks, and checked for technical failures, that is, double submissions.
Statistical Analyses
Overall Use of Substances.
An iterative modeling process was applied to produce models with two to five classes. Based on two-fit indices (bootstrap likelihood ratio, BRLT (Nylund et al., 2007); Bayesian information criterion, BIC (Morgan, 2015), the best fitting model was selected (Tein & Cham, 2013). The level of significance was set to p < 0.05. BLRT test revealed significant differences between the classes 2 and 3 and between three and four. The best fitting model was chosen using the lowest BIC (for BICs of all classes, see Supplementary Material). Allocation of participants to the groups was based on the LCA. Participants were allocated to the group for which they showed the highest class-membership probabilities. Using entropy as an additional indicator for correct class assignments, the chosen classes showed a value of 0.88, which can be considered high entropy (Clark and Muthén, 2009).
Results
Characteristics of Respondents
A total of 969 participants completed the survey. Average time to complete the survey was 12. 5 minutes. Individuals who did not report experience with substance use or were not MSM were excluded. Data could be obtained from N = 597 MSM from all federal states in Germany. Mean age was 38.2 years (SD = 11; range = 16–81). Participants predominantly stated to be employed (76.7%), and about half of them lived in a city with more than one million inhabitants (58.1%). Most men self-identified as homosexual (95%, n = 540) and about a quarter of them reported to be living in either an open (28.5%) or in a monogamous relationship (25.8%).
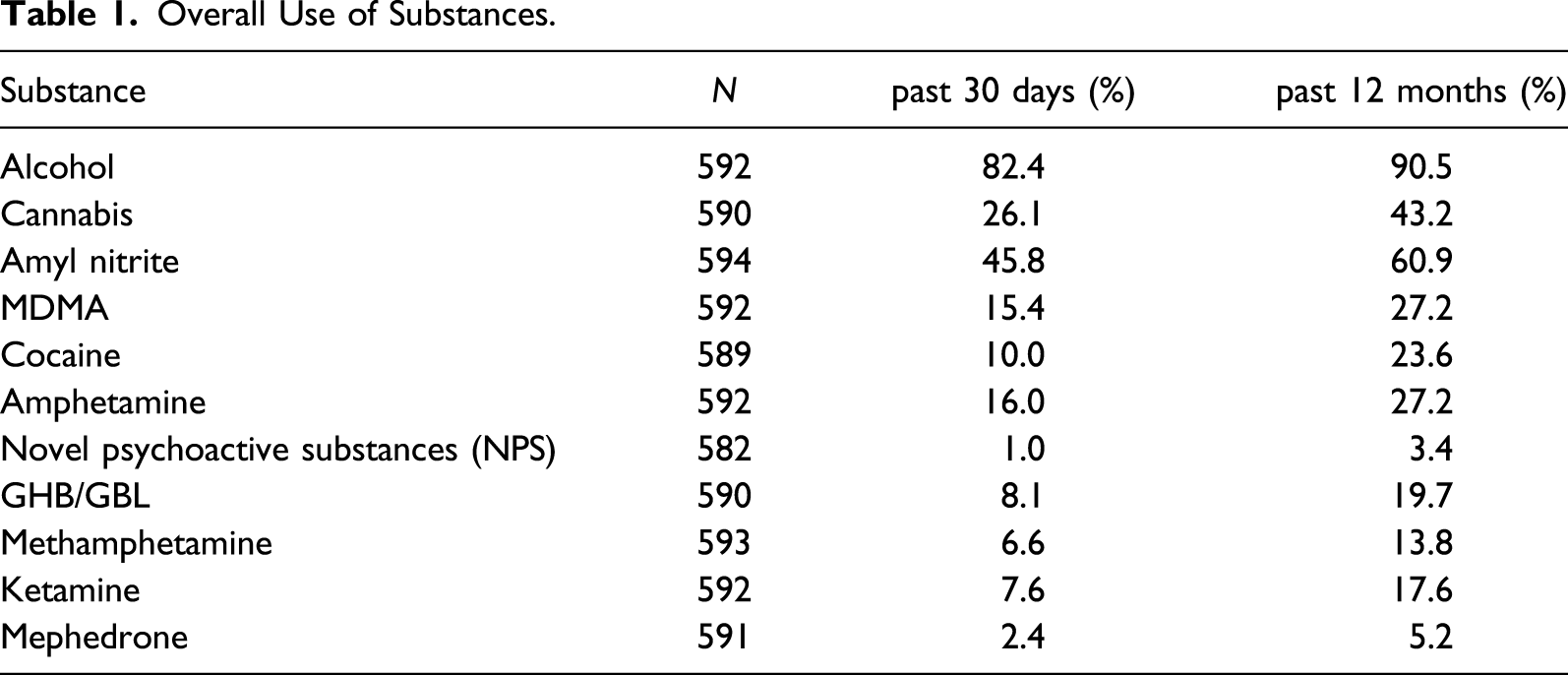
Overall Use of Substances
Alcohol was the most commonly used substance with a 12-month prevalence of 90.5%, followed by amyl nitrite (“poppers”; 60.9%) and cannabis (43.2%; see Table 1). The first consumed illicit substance was cannabis for 58.1% of the participants. Substances associated with chemsex in the literature, like methamphetamine, GHB/GBL, or ketamine, were used by a small but relevant proportion of participants (13.8%, 19.7%, and 17.6% 12-month prevalence, respectively).
Results of the Latent Class Analyses (LCA)
Statistical characteristics of each 2- to 5-class solution are shown in Table 1. BLRT test revealed significant differences between the classes 2 and 4 (Table 1), which indicates that each of these four models fits significantly better than the one before. Best fitting model was chosen using the lowest BIC. BIC was 4553.8 points for the 4-class solution. According to the entropy value of 0.88, the 4-cluster model showed the highest classification accuracy.
In our 4-cluster model, the first cluster (“poppers only”, n = 370) consisted of men consuming hardly any substances besides poppers and cannabis. Men in the second cluster (“club-druggers”, n = 106) showed a high prevalence of MDMA, cocaine, amphetamine, amyl nitrite, and cannabis use, but low rates of ketamine and GHB/GBL consumption and virtually no consumption of methamphetamine or mephedrone. Men in cluster 3 (“chems-users”; n = 43) reported the use of chemsex-related drugs such as methamphetamine, GHB/GBL, and ketamine. A fourth cluster was labeled “polyvalent users” (n = 78) due to the wide range of reported substances. (Figure 1) Use of substances across the clusters (%).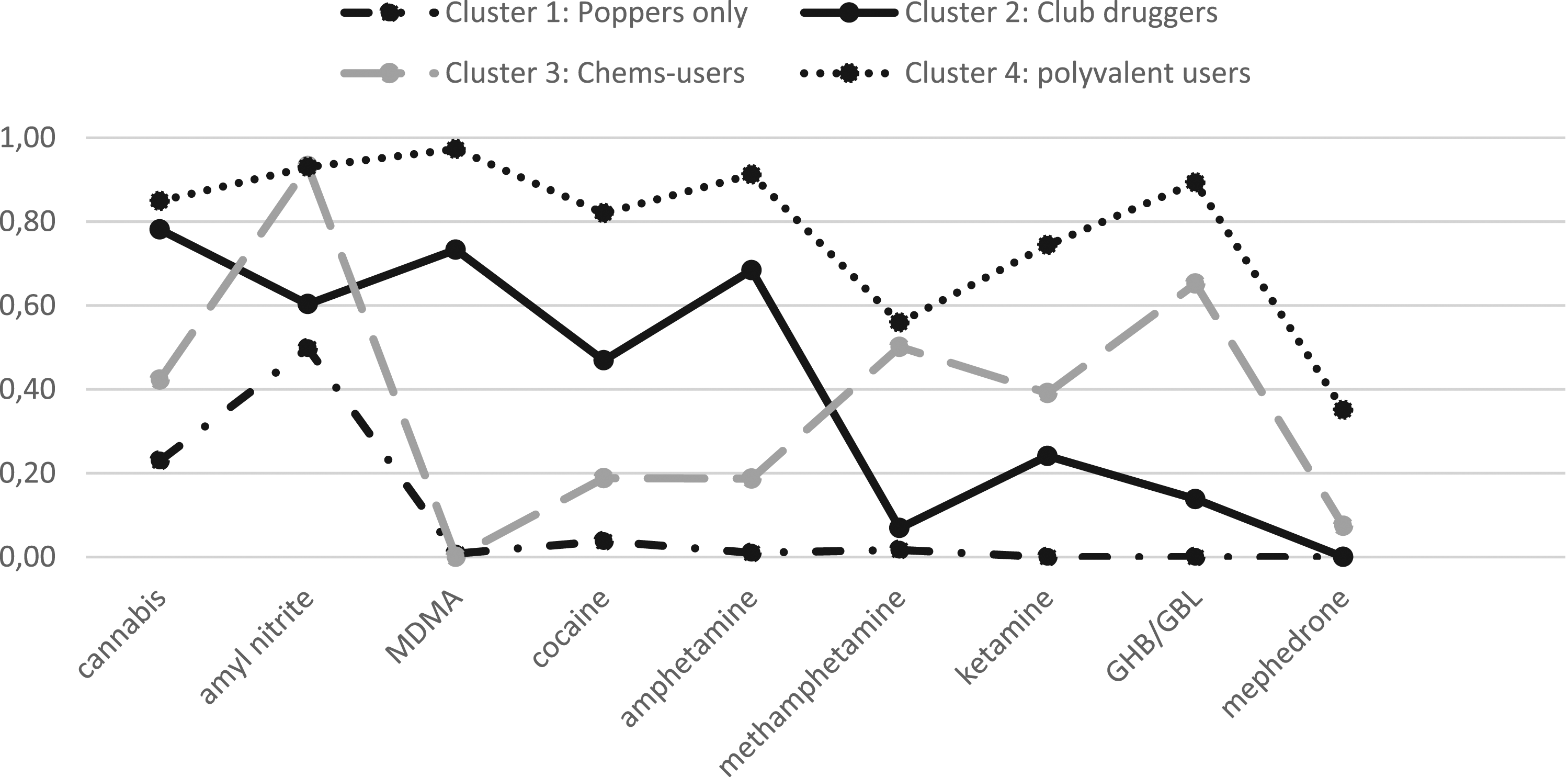
Characteristics of Clusters - Sociodemographics
Descriptive Statistics for the Different Clusters.
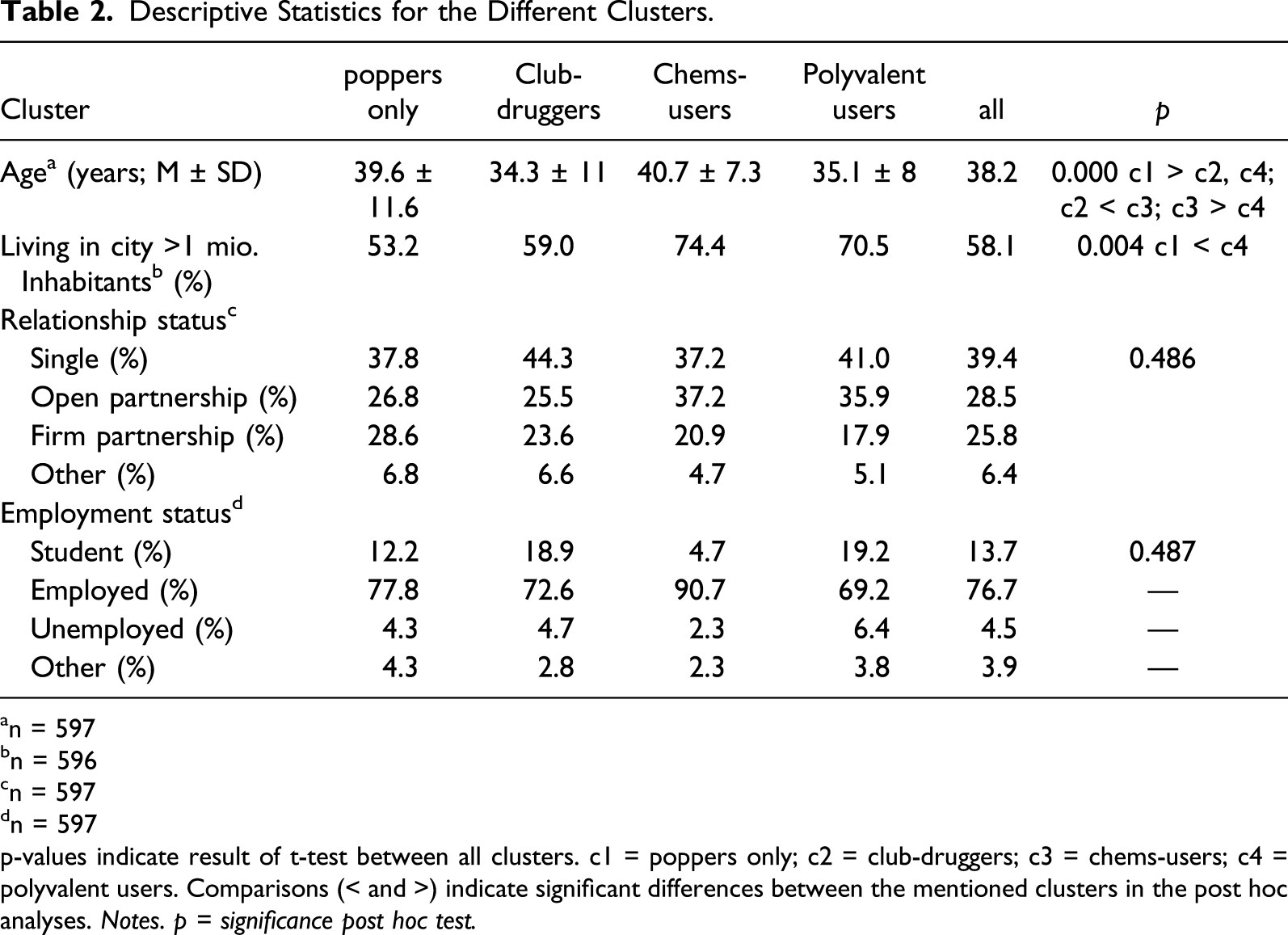
an = 597
bn = 596
cn = 597
dn = 597
p-values indicate result of t-test between all clusters. c1 = poppers only; c2 = club-druggers; c3 = chems-users; c4 = polyvalent users. Comparisons (< and >) indicate significant differences between the mentioned clusters in the post hoc analyses. Notes. p = significance post hoc test.
Characteristics of Clusters – Substance Use in a Sexual Context
Substance-Consumption in the Sexual Context.
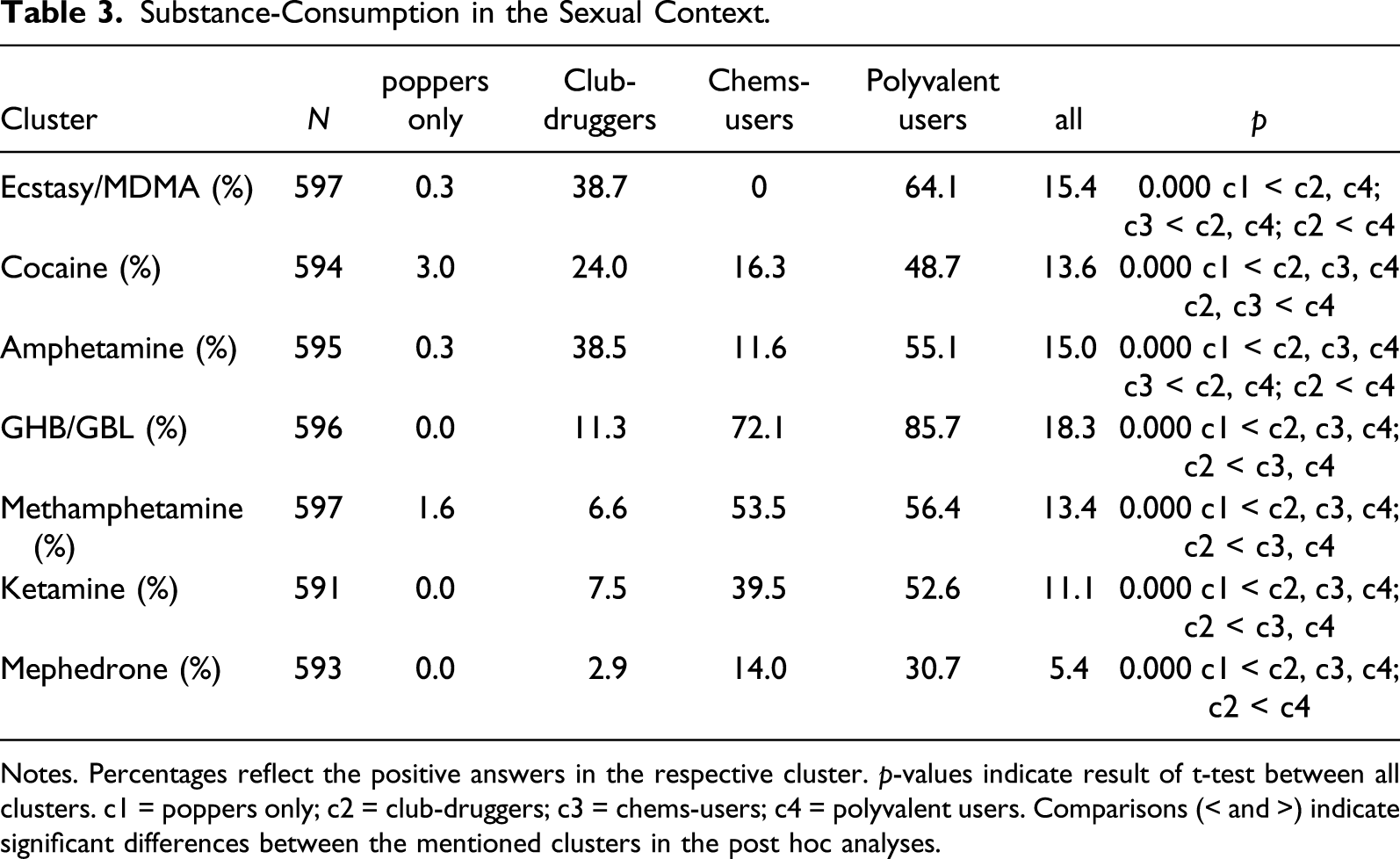
Notes. Percentages reflect the positive answers in the respective cluster. p-values indicate result of t-test between all clusters. c1 = poppers only; c2 = club-druggers; c3 = chems-users; c4 = polyvalent users. Comparisons (< and >) indicate significant differences between the mentioned clusters in the post hoc analyses.
Characteristics of Clusters – Psychiatric Symptoms and Problems
Psychiatric Symptoms.
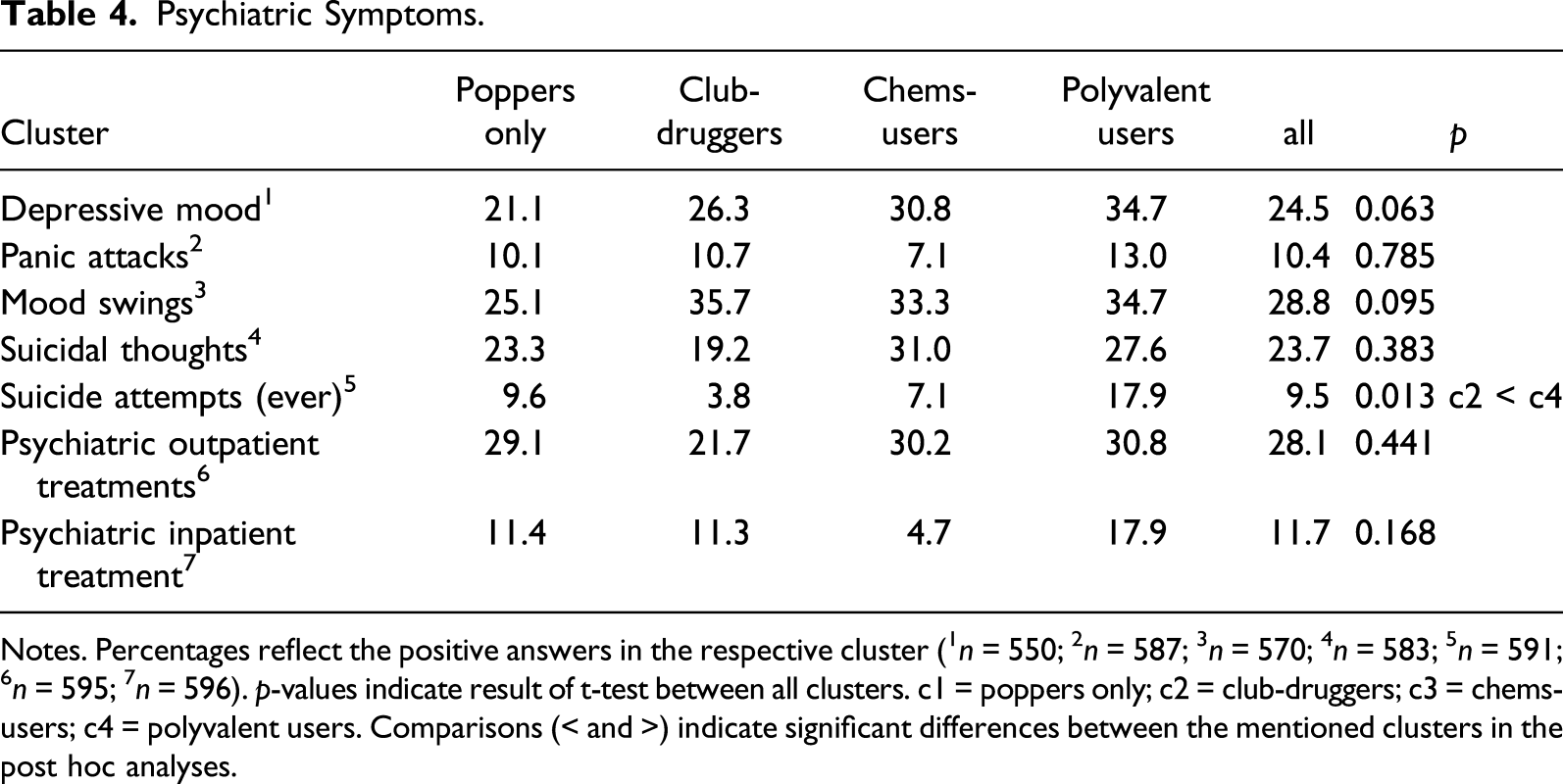
Notes. Percentages reflect the positive answers in the respective cluster (1n = 550; 2n = 587; 3n = 570; 4n = 583; 5n = 591; 6n = 595; 7n = 596). p-values indicate result of t-test between all clusters. c1 = poppers only; c2 = club-druggers; c3 = chems-users; c4 = polyvalent users. Comparisons (< and >) indicate significant differences between the mentioned clusters in the post hoc analyses.
Characteristics of Clusters – Infectious Diseases and RISK-TAKING Behavior
Infectious Diseases, Risk-Taking Behavior and HIV-Medication.
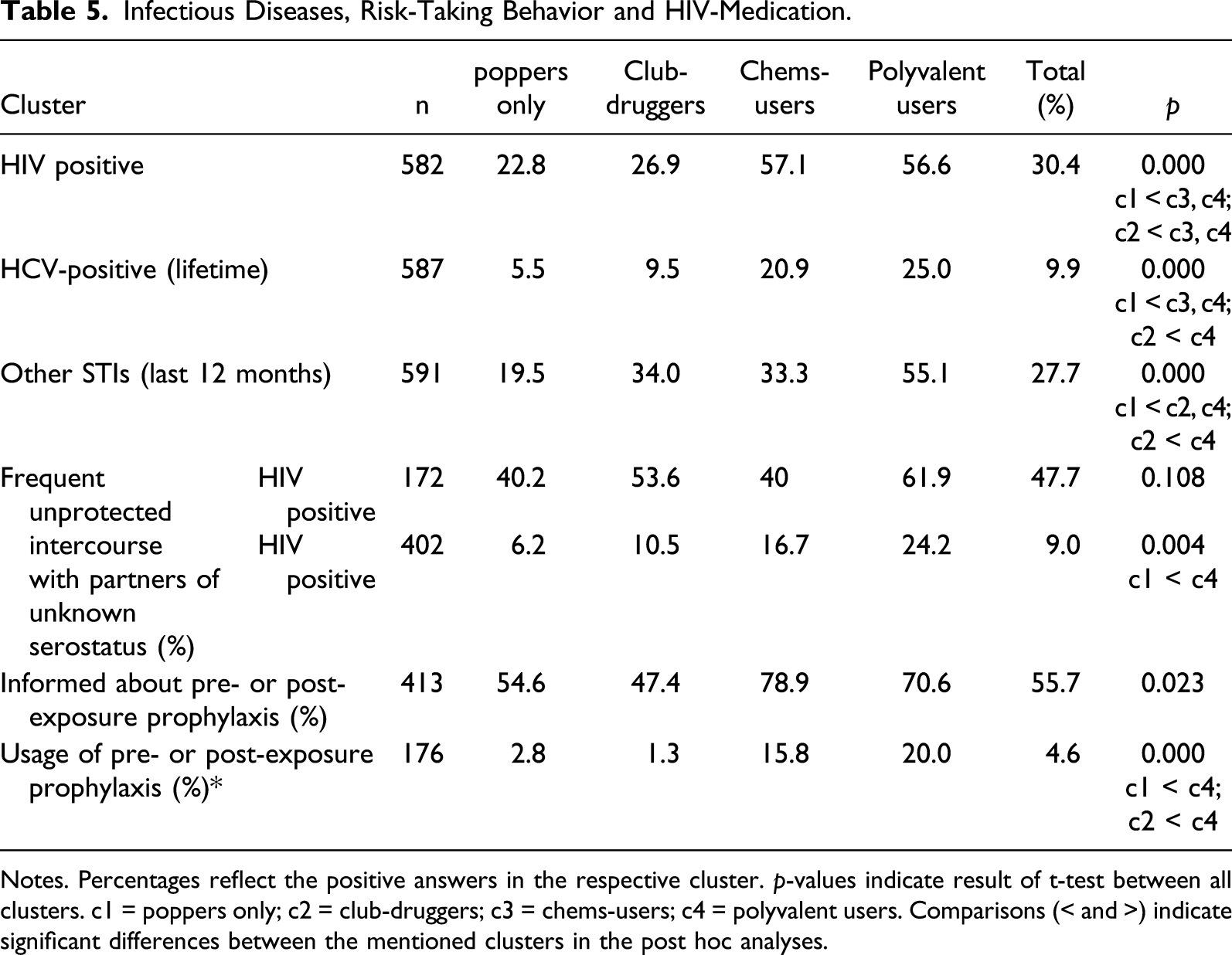
Notes. Percentages reflect the positive answers in the respective cluster. p-values indicate result of t-test between all clusters. c1 = poppers only; c2 = club-druggers; c3 = chems-users; c4 = polyvalent users. Comparisons (< and >) indicate significant differences between the mentioned clusters in the post hoc analyses.
Across the whole population, the number of sex partners during the preceding 12 months ranged from none to 500 with a mean of 23.8 (SD ± 49.5; n = 594; see Table 5). The median number of sex partners within the preceding 12 months was significantly higher in the polyvalent cluster 4 (median = 30 partners), and the chemsex cluster (median = 20 partners) than in the “poppers only” and “club-druggers” clusters 1 and 2 (p < 0.001). HIV-negative participants in the polyvalent cluster four were more likely to have sexual intercourse with a partner of unknown serostatus on a regular basis (24.2%) and showed higher usage of pre- or post-exposure prophylaxis (20%; n = 7) than cluster 1 and 2.
While at least half of the men across all clusters had sought information about pre- and post-exposure prophylaxis at some point, only men of cluster 3 and four had also used it to a larger extent (see Table 5).
Almost all men being tested HIV positive stated to be under current antiretroviral medication with 100% in the chems-cluster and no significant differences between the clusters (see Table 5).
Discussion
In this study, we recruited a large sample of MSM with substance use to gain a better understanding of their substance use, psychosocial, and health-related characteristics, including sexual risk behaviors. The median age of our population was comparable to samples in previous studies suggesting that our findings might be comparable to the existing literature (Achterbergh et al., 2020a; Lim et al., 2015). We also managed to reach both participants from cities with over a million inhabitants (58.1%) and from smaller cities or communities (41.9%).
Using latent class analysis, we found four clusters based on the participants’ patterns of drug consumption. This number lies in the range of comparable studies that reported from three to six subgroups of MSM with substance use (Achterbergh et al., 2020a; Achterbergh et al., 2020b; Lim et al., 2015). The majority of men were categorized in cluster 1 (“poppers only”) with negligible use of substances other than amyl nitrite and low rates of STIs. Cluster 2 (“club-druggers”) consisted of rather young men consuming MDMA, cocaine, amphetamine, cannabis, and amyl nitrite, but no methamphetamine. These “club drugs” were to a relevant percentage used in the context of sexual intercourse. Our findings thus indicate that sex-related consumption was not limited to drugs usually discussed in the context of chemsex (methamphetamine, GHB/GBL, ketamine, and mephedrone), but also included other substances (e.g., cocaine or MDMA). This idea corresponds with findings from a recent study including a network correlation that revealed high associations between the consumption of the “chems” ketamine and GHB/GBL and the “club drug” MDMA (Achterbergh et al., 2020a). Cluster 3 (“chems-users”) consisted of men with a high prevalence of chemsex-related drugs (methamphetamine, ketamine, GHB, and mephedrone). This cluster also reported the highest rate of employment, suggesting a rather high level of functioning. In contrast, cluster 4 (“polyvalent users”) reported a high prevalence of chemsex drugs. This cluster also reported more risk behavior, including more polyvalent consumption patterns with a wide range of used substances, which has repeatedly been associated with increased risk for HIV seroconversion and other STIs (Plankey et al., 2007; Shoptaw et al., 2012). In line with this, the prevalence of HIV, HCV, and “other STIs” was higher in this cluster as compared to the other clusters. Interestingly, the strongest association between substance use and sexual motives was found in the cluster with polyvalent use, not in the cluster that mainly used the “chems” ketamine, GHB/GBL, methamphetamine, and mephedrone (cluster 2). This suggests that focusing only on these substances as chemsex-related might not be justified in MSM samples. The number of sexual partners was significantly higher in cluster three or four than in the other clusters (Achterbergh et al., 2020a). Men in these clusters were more likely to live in an open relationship than the other two clusters. Since no data about the viral load were collected, the isolated number of sex partners or the frequent serodiscordant intercourse of the HIV-positive subgroup might not be a risk factor for HIV transmission per se. But among the HIV-negative men in the polyvalent cluster, the significantly higher number of sexual partners could pose a risk of HIV transmission in combination with other factors such as unprotected intercourse and unknown serostatus of the partner (Kingsley et al., 1987). Men of both, cluster 3 and cluster 4, predominantly lived in big cities. This is in line with previous findings that described the phenomenon of chemsex as predominantly existing in urban regions but in different forms and among different subgroups of users in rural areas, too (Schmidt et al., 2016). The majority of men across all clusters stated to be informed about antiretroviral pre- and post-exposure prophylaxis. Knowledge about HIV prevention seemed to be comparable among all clusters, but their utilization of pre- or post-exposure prophylaxis differed. Further research should therefore address the use of preventive medication in this context and potential opportunities to improve healthcare approaches related to these practices.
Against previous studies, we did not find higher rates of depressive mood or anxiety symptoms in MSM engaged in chemsex, and no differences between the clusters existed in the portion of men that had received psychiatric treatment (Bohn et al., 2020; Cochran et al., 2003; Pufall et al., 2018). However, suicide attempts were significantly more often reported in the polyvalent cluster. In previous studies, stigmatization, self-stigmatization, and minority stress have been discussed as factors associated with sexualized substance use (Chard et al., 2018; Meyer, 2003; Pollard et al., 2018). The higher rate of suicide attempts in our polyvalent cluster might therefore be an indicator for elevated susceptibility for these stressors (Chard et al., 2018; Pollard et al., 2018; Semple et al., 2011). The concept of chemsex as a coping strategy in certain susceptible subgroups has been discussed previously, but robust data to proof this association is still missing (Pollard et al., 2018). At the same time, some authors criticize the biased scientific consideration of chemsex exclusively as a problematic kind of self-medication (Pienaar et al., 2018).
Considering chemsex exclusively in the context of sexual activity and enhanced sexual performance might also fall to short. Further efforts should be made to inform more specific prevention strategies as well as for medical and psychiatric healthcare providers. This is emphasized by study findings associating for instance anxiety symptoms in MSM with methamphetamine consumption with homelessness, adverse childhood experiences, and more risky sexual practices (Semple et al., 2011). With the increasing scientific interest in chemsex, it becomes important to avoid overgeneralization of chemsex as an “MSM-topic” as well as pathologization of any kind of sexualized substance use, and a priori assuming that MSM are a vulnerable population (Pienaar et al., 2018). The aspects of pleasure in chemsex are seldom interest of research and the majority of MSM does not consume psychoactive substances on a regular basis. Nevertheless, besides this large group of MSM with negligible substance consumption, several studies show that certain smaller subgroups exist that might need further support.
The different clusters we and other authors found underline the complexity of this phenomenon. Although there is a distinct association between for instance the consumption of methamphetamine and sexual risk-taking in literature, most of the existing studies do not established causality. Cross-sectional and quantitative instruments might not be the ideal approach to understand the complex relationships between consumption patterns, substance dosage, setting of consumption, inner psychic factors, and potential health harms (Bryant et al., 2020). Both considering chemsex exclusively in the context of problematic substance use and STI transmission or solely in the context of enhanced sexual pleasure might fall short.
Strengths of this study are the large sample size and the advanced recruitment strategy; a number of limitations also have to be considered. By promoting the survey not only on websites for nightlife and drug aid but also on social media like Facebook, we tried to prevent a recruitment bias. Nevertheless, we assume drug-experienced men to be more interested in a drug-related survey. We further assume that the recruited sample were men with an active internet use (i.e., social networks, forums, and dating apps). This should be considered when interpreting and reflecting the results. The online recruitment strategy may have led to a recruitment bias by not addressing men without internet access (e.g., homeless men). The high rate of HIV and HCV in our sample points out to a rather sexually active sample.
Our sample can, therefore, not be considered to be representative for MSM with drug use. Moreover, all data were self-reported, a limitation our study shares with comparable studies in the field. This might lead also to under-reporting the consumption of illicit drugs, but the anonymous nature of the online survey highly likely minimized this bias. Finally, it could be considered a limitation that we did not include alcohol use in our analyses. Previous studies reported that subgroups of MSM with harmful use of alcohol exist, as their main substance or in combination with illicit drugs (Lim et al., 2015; Melendez-Torres et al., 2018). Since our focus was on drug use, however, we decided to include only these substances in the analysis.
Subgroups of MSM engaged in chemsex seem to differ in their characteristics. Knowing the characteristic traits of the different clusters may help to further develop a chemsex-specialized aid system. The specific role of chemsex as a coping strategy should be addressed in further studies. Consumption in the sexual context is not limited to substances commonly associated with chemsex (methamphetamine, GHB/GBL, ketamine, and mephedrone), but might also include further substances like cocaine or MDMA.
Supplemental Material
sj-pdf-1-jod-10.1177_00220426211040564 – Supplemental Material for Substance Use and Chemsex in MSM - A Latent Class Analysis
Supplemental Material, sj-pdf-1-jod-10.1177_00220426211040564 for Substance Use and Chemsex in MSM - A Latent Class Analysis by Anne Deborah Scholz-Hehn, Sascha Milin, Bernd Schulte, Jens Reimer, Sven Buth and Ingo Schäfer in Journal of Drug Issues
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
He is editor or member of the editorial / advisory board of the journals European Addiction Research, Substance Abuse, Heroin Addiction and Related Clinical Problems, and Suchttherapie. Professor Reimer is member of the board of the German Addiction Foundation, and the scientific board of the German Main Institution on Addiction Issues. He has published widely in the areas of addiction and health care research.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.