
Abstract
Canada continues to be in the midst of an ongoing unregulated drug poisoning crisis, with over 40,000 opioid-related deaths since 2016. To develop a better understanding of the context of drug use, we interviewed safer supply program participants in Ottawa, Canada. Data collection included semi-structured interviews which were analyzed thematically. Overall, 2 major themes arose, which included 1) the historical and ongoing effects of trauma, and 2) a cycle of drug use that overwhelmed them. From this, a framework was created which depicts the context of substance use. Our research reinforced the importance of considering the historical and ongoing effects of trauma on the lives of people who use drugs when developing harm reduction and substance use programs. Further, participants found safer supply programs to be useful in disrupting a cycle of drug use they felt trapped in and allowed them a sense of autonomy regarding their drug use.
Introduction
Canada continues to be in the midst of an unregulated drug poisoning crisis, with over 40,000 opioid toxicity deaths having occurred since 2016 (Special Advisory Committee on the Epidemic of Opioid Overdoses, 2023). In 2023, this was the equivalent of 22 opioid toxicity deaths each day. This drug poisoning crisis has been predominantly driven by the contamination of unregulated drugs with unexpected, and often dangerous, substances. This largely began in 2016, when fentanyl was increasingly found in unregulated heroin supplies (Mayer et al., 2018). Given the potency of fentanyl, this inevitably resulted in increased opioid-related morbidity and mortality, including increased overdose rates, increased rates of hospitalization, and an increasing number of opioid-related deaths (Special Advisory Committee on the Epidemic of Opioid Overdoses, 2023). Currently, fentanyl continues to be a source of harm among people who use drugs (PWUD) – for example, in 2022, 81% of opioid toxicity deaths involved fentanyl (Special Advisory Committee on the Epidemic of Opioid Overdoses, 2023). Recent drug-checking results in Toronto show that unregulated fentanyl is commonly contaminated with other substances, such as fentanyl analogues, benzodiazepines, and tranquillizers (Centre on Drug Policy Evaluation, 2023). The ongoing stigma and marginalization of PWUD compounds and exacerbates the harms associated with the toxic unregulated drug supply. Research with PWUD has demonstrated that they frequently report negative experiences (such as stigma) within the healthcare system which can result in delays to accessing care (Chan Carusone et al., 2019; Motavalli et al., 2021). Further, PWUD continue to be criminalized and punished for their unregulated drug use as a result of inequitable drug policies (Tyndall & Dodd, 2020).
Many harm reduction measures have been implemented nationwide to address the ongoing harms related to the drug poisoning crisis, such as supervised consumption sites, distribution of sterile drug use equipment, and take-home naloxone programs (Government of Canada, 2021; Moustaqim-Barrette et al., 2019). To more directly address and replace the contaminated unregulated drug supply, safer supply pilot programs have been established in a few communities across Canada (Government of Canada, 2020; Health Canada, 2022). Safer supply is a harm reduction measure aimed to “decrease harms related to the toxic drug supply (e.g., risk of overdose, criminalized behaviour, trauma/mental health concerns, etc.) by providing PWUD with pharmaceutical grade prescription medication (often opioids and stimulants)” (Haines et al., 2022, p. 4). Evidence also suggests that safer supply programs do help achieve these outcomes. A recent safer supply program evaluation completed in Ottawa, Canada found that over 70% of participants reported a decrease in their unregulated fentanyl use since starting the program (Haines et al., 2022). Further, 81% of participants who reported experiencing a recent drug overdose during their intake assessment subsequently reported no overdoses at their most recent safer supply check-in (Haines et al., 2022). Participants also reported feeling a sense of community, connectedness, and safety when engaging with their safer supply program (Haines & O’Byrne, 2023a).
Understanding the needs of PWUD has been essential to the development of impactful substance-use-focused programs and harm reduction services. The context of drug use – why someone may use drugs – is central to the development and utility of harm reduction programs for PWUD. This makes it an important topic to consider in the context of addressing the ongoing drug poisoning crisis. To develop a better understanding of the context of drug use, we interviewed 30 PWUD participating in a safer supply program. These interviews were conducted as part of a larger safer supply research evaluation occurring in Ottawa, Canada (Haines & O’Byrne, 2023a). Each of the participants spoke about the broader context of their substance use and emphasized the importance of this context being considered by their care teams when engaging in harm reduction programs.
Methods
Design
We completed a qualitative study with current safer supply participants in Ottawa, Ontario. Semi-structured interviews were used to allow for the exploration of the impacts of safer supply programs from the perspective of participants through rich descriptions of processes, phenomena, concepts, and experiences.
Recruitment and Sampling
Participants were recruited through posters displayed at each of the safer supply sites as well as snowball sampling. Participants were selected on a first-come, first-served basis. The researchers went in person to safer supply programs to conduct interviews. Inclusion criteria for the research project included any PWUD who is currently participating in a safer supply program in Ottawa, Canada, and who is capable of consenting to participation in the research study. Currently, there are three separate safer supply programs in Ottawa which serve nearly 500 participants through safer opioid and stimulant programs. Each of these programs offers a unique model of care, including a community health centre, a supervised consumption site within a shelter, and a substance use clinic. Detailed descriptions of these programs are available in a separate manuscript (Haines & O’Byrne, 2023b).
Data Collection
Data collection occurred through audio-recorded, semi-structured interviews with participants. Interviews probes were available for referral by the interviewer to guide the conversation. However, the interviews will be highly flexible and guided by the thoughts and experiences of the participants. Probes have been screened by several individuals to confirm they are open-ended, clear, and use appropriate and sensitive language. Interviews were audio-recorded and transcribed to ensure the quotes were accurate. Surveys were also completed with participants to collect socio-demographic data and substance use information – the results from these surveys can be found elsewhere (Haines & O’Byrne, 2023a). The research team provided an overview of the research objectives and questions to all potential participants prior to starting. Two consent forms were also signed by each participant and the researcher: one form was kept for the research team, and one form was given to the participant to keep. Participants were given US$100 compensation for their time.
Data Analysis
All interviews were thematically analyzed as per Smith, Flowers, and Larkins (Smith et al., 2009): 1. The audio-recorded semi-structured interviews were transcribed verbatim, including both interviewer and participant text. 2. Two authors individually read through the transcripts multiple times and listened back to audio recordings as needed to help nuance interpretations. 3. Initial noting was completed individually by each author, with notes and comments assigned to individual sections of data while maintaining contextual information. 4. Notes and comments were clustered together to form larger codes within individualized interactions with participants. 5. Codes were bunched together to create concrete themes and theoretical underpinnings which aimed to reveal the essence of the participant experience.
Decisions made throughout the analysis process were well documented to maintain a clear audit trail. Quotes and text segments that lend themselves particularly well to the themes that arose were flagged for future use in the writing of thick descriptions. The research team used nVivo 1.7.1. To complete data analysis. As the research team was analyzing the interview data, several key themes and concepts describing the “cycle of substance use” were found consistently throughout participant data. As the research codes were bunched together to create themes (step 5), a clear framework began to emerge from the participant descriptions of their substance use.
Ethics and Funding
This study was approved by the Research Ethics Board at BLINDED (H-03-22–7890). All participants provided written informed consent prior to enrollment in the study. Funding for this research was provided by Health Canada’s Substance Use and Addictions Program.
Results
Survey
As previously mentioned, participants were invited to complete surveys in addition to semi-structured interviews. Detailed results of these surveys are available in a separate manuscript (Haines & O’Byrne, 2023a). Overall, 30 participants engaged in this research project. The median age of participants was 42 years old, and participants reported they had been part of a safer supply program for a median of 20.5 months. Most (57%) participants self-reported their gender as men, and the remaining 43% of participants self-reported as women. This includes both cis and trans individuals. Given the small number of individuals who were trans within these programs, gender was grouped this way to protect participant privacy and confidentiality. Just over half of the participants were white (53%) and 9 were Indigenous (30%). Participants reported starting to use drugs at the age of 13 on average. The most commonly used drug across the lifespan reported by participants was cocaine (100%), followed by fentanyl, other opioids, and crack cocaine (97%).
Interviews: Context of Substance Use
The importance of understanding the broader context of substance use was highlighted by all participants. This context included reflecting on their own personal history of initiating and continuing drug use as well as the broader structural violence that has impacted their mental health and well-being. Overall, participants emphasized 1) the historical and ongoing effects of trauma in their life, and 2) a cycle of drug use that overwhelmed them. From this, a framework was created which depicts the context of substance use as described by the research participants.
Theme 1: Impacts of Trauma, Marginalization, and Substance Use
Participants described trauma as encapsulating their lives, and many spoke about trauma as a central factor in starting to use drugs. One participant described using opioids to manage painful memories of a traumatic childhood: Because [opioids] helped me not think about a lot of the trauma that I went through – and I went through a lot of trauma. I was on the streets when I was 15. Runaway from children's aid. Being physically, sexually, mentally abused by my foster family… the reason I use [opioids] is to forget and not to think about that (P25).
This participant described extensive mental health concerns as a result of their trauma and relied on opioids as an essential coping mechanism. They stated, “I’ve been in and out of psych ward my whole life because of that. And I haven’t been in a psych ward for probably 15 years now. And that’s probably as long as I’ve been doing opioids” (P25). Although they were repeatedly admitted to mental health institutions, self-medication through opioids was reported as helping them manage their complex trauma.
Other participants described relying on opioids to manage their emotions as well, with one participant noting, “I started using fentanyl to stop feeling” (P8); another echoed this sentiment: “the main reason why people use drugs is to hide, to block out everything bad that you have done or has been done to you” (P20). Traumatic and painful events as well as escalating mental health concerns often preceded escalating substance use: I had just lost my kids to my baby dad because of my relapse due to my switch from Methadone to Suboxone not working. I was very depressed and started using fentanyl because of the withdrawals, but then started using [fentanyl] heavily because of my depression (P23).
Understanding and processing trauma was a complex topic, though essential, with a participant stating, “to get to the heart of the issue, you have to get to the heart of the reason why you’re using drugs” (P20). This required a safe space, trusted individuals, and a mutual understanding of trauma and substance use, which were often difficult to find and access.
Participants expressed a desire for society and people who are not part of their community to “educate themselves on drug use and why people use… there’s so many layers underneath the reason why” (P22). Misunderstandings about substance use being related to willpower and ongoing victim blaming of PWUD were sources of frustration, and tied into conversations regarding stigma and marginalization: Everybody uses for a reason, whether it's you lost your job or you had an operation that didn’t go well, or something bad happened to you like rape, or kids getting thrown out of their parents' house. Nobody's doing this because they want to. They're doing this because shit happened to them… Nobody chooses to be in this position (P20).
The pervasive experience of stigma and marginalization was ubiquitous in our interviews. Participants described feeling rejected by the general population as a result of their drug use, often reflected in both covert (“they seem to look at you because you’re an addict and they just judge you” [P26]) and overt (“they have a tendency to veer away from you” [P20]) moments of ostracization.
I walk down the street and I’ll see some guy overdosing on the sidewalk and people are standing around taking pictures of him laughing, and I’m sitting there trying to save his life… [but], It’s life, right? P13).
These experiences resulted in avoidance of interactions with those outside of their community and “hiding basically from everybody” (P17). Many participants reflected on health care being a particularly inaccessible system to navigate and engage in: When you have been a drug user in the past, your injuries or things that you've gone through in your life, whether it be mental or physical, many people don't want to listen to you if they know that you've used illicit drugs in the past. They think that you're just out there seeking drugs just for a good time or for no reason (P18).
One participant reported an experience of being hassled at a pharmacy when they went to pick up medication they were prescribed. The pharmacist questioned their prescription and humiliated them: “they can be real dicks… [I wanted to say] just please, can you dispense it and let me be with my day” (P21). Participants expressed feeling misunderstood and disrespected in their daily lives. They were stripped of their individuality and viewed as a homogenous group of people who were often primarily categorized as “just another junkie. No, it’s somebody’s child, sister, brother, mother, uncle, whatever. It’s somebody’s somebody” (P9). Experiences of dehumanization were summarized succinctly by a participant commenting on the war on drugs: “It’s not on drugs. Drugs is an inanimate object. It’s a war on people” (P21).
Feelings of guilt and shame were pervasive within the interviews. Many participants reported participating in criminalized behaviours to be able to purchase unregulated opioids before safer supply, often describing this as a demeaning activity: “it’s embarrassing but I had to do it…. I needed the drugs (P3). In other words, the participants reported engaging in criminalized behaviours to survive, with several participants feeling as though they had no choice: “I didn’t like [participating in crime], but I had to do what I had to do” (P2). Participants described intense feelings of remorse: I hated that feeling, but that was just how I was good at making my money. Stealing and all that, I've done it. I don't like doing that kind of stuff. I'd rather do something where I feel like I work to get my money more or less than steal my money (P8).
Additionally, participants described an overall sense of hopelessness tied to their drug use and often struggled to conceptualize the future. Prior to safer supply, many participants reported that they “just didn’t care” (P19) about the future, describing themselves as “at the end of [their] line” (P30) and “having nowhere to go… want[ing] to give up” (P1). Two participants described feeling abandoned and repeatedly let down: “I slipped through the cracks” (P2) and “I’m falling through the cracks and they don’t know which crack I fell in and they don’t care” (P7). Participants felt extremely limited in their ability to make decisions for themselves when using unregulated fentanyl and felt out of control: “I really didn’t even care [about dying] because I didn’t think there was a way out” (P18). One participant described feeling extremely despondent about their fentanyl use: Because it's pointless, [unregulated fentanyl] is just a ticking clock for everybody that's on it. It's just a matter of whose clock has more time on it than the next person's… the end result is death (P13).
Related to these experiences of hopelessness, participants described feelings of powerlessness in their life before safer supply. Extended blackout periods when using unregulated fentanyl were not uncommon: “When on the fentanyl you don’t really remember anything, right? Everything’s a blur. You try to think back on your days and you can’t remember nothing” (P8). When participants were prompted to reflect on their life just before safer supply, many reported they “don’t remember much” (P18) and expressed frustration when “nobody can tell you what happened” (P17). One participant described life as “chaotic, definitely chaotic… From one day to the next that you don’t even know what’s going on” (P24).
Given the unpredictable nature of consuming unregulated substances, all participants recounted the pain of constantly losing loved ones to overdose deaths, and the complex, disenfranchised grief associated with this. Participants disclosed, “A lot of my friends have dropped so far” (P26), “I’ve seen a lot of friends go” (P13), and “Today they’re no longer with us… they’re dead” (P16). Participants also describe the experience of cumulative grief, as the volume of people dying in their lives was astounding. One participant noted, “298 people, that’s a lot of people to lose… you don’t even realize until you have a memorial about them” (P20). Another participant stated, “I also think about how many friends I’ve lost in the last couple years, and 25 is a high number to lose in a year and a half” (P30).
Further overlaying this intense barrage of grief were stories of participants also experiencing trauma related to witnessing and responding to the overdoses of their friends and peers in the community: “I’ve seen my friends go down on it and die” (P7). The strain of responding to an emergency was immense, with one participant noting “I just had such bad PTSD from bringing people back” (P23), and another stating “To actually watch somebody drop, turn gray, turn cold, turn blue, scares the shit out of me” (P7). Participants voiced their hopes for change, stating “When you see that many friends die, someone’s got to start doing something about it” (P8), and another noting, “How many other parents have to outlive their children?” (P23).
Overall, the experience of trauma was raised as a central point of discussion by all participants. Participants discussed using opioids to manage traumatic memories and experiences, as well as ongoing mental health symptoms. They also disclosed repeated instances of marginalization and stigma due to their status as a PWUD, which included negative experiences within the healthcare system. Feelings of guilt, shame, and hopelessness were commonly reported by participants and were often linked to specific events such as participation in criminalized behaviours and disenfranchised grief.
Theme 2: Cycle of Drug Use
Through all the interviews, most participants very clearly outlined what they described to be “a cycle of drug use” (P12). Participants evoked an image of a cyclical process they became stuck in because of their unregulated fentanyl use: “Because you’re always doing the same thing over and over… It’s not the kind of drug that you could just say, ‘Hey, okay, I’m not going to do it today.’ Doesn’t work like that” (P8). One participant described a day in their life before safer supply: Well, you get up. If you had money, you were going searching for the drugs. You get the drugs, you do them. As soon as you're done doing them, you're looking for money again for your next hit. And it's a cycle, the entire day (P17).
This cycle forced participants to constantly prioritize their unregulated fentanyl use: “My single purpose, 24 hours a day, was to get money for drugs” (P10), “My sole purpose in life was just to stay unsick or to get high” (P14). Even important meetings and events needed to be pushed to the side to ensure cravings and withdrawal symptoms were kept at bay: “Every day was ruined, and we were missing out on appointments and important things we had to do because we were chasing the drug” (P9).
Indeed, participants articulated feeling trapped and ultimately unable to care for themselves: “If you’re sick or if you’re chasing your next high, then there’s no time for you to get better” (P20). This process compounded feelings of anxiety and uncertainty, which further reinforced the cycle of use: “it amplified the sickness, the worry, the anxiety about where am I going to get my fix? Where am I going to get my drugs? How am I going to get this money? What am I going to have to do to get this money?” (P10). Participants felt beat down and restrained, with one participant stating, “it tears your soul apart” (P17).
A clear driver of the cycle of use was the need to stave off opioid cravings and withdrawals each day. With regards to experiencing withdrawals (dope sickness), one participant noted: “I would rather been dead than be sick… it’s just brutal. It’s nothing that I would want my worst enemy to go through” (P25). Another stated, “opioid withdrawal is the worst thing you could possibly go through” (P20). Understanding the feeling of being dope sick is often difficult for people who do not use opioids to understand – one participant attempted to describe it: It’s like dying very, very slowly…. It feels like icy hands going all over me all the time. You can't sit still, you can't sleep, but you want to sleep because if you're sleeping, you can't feel it. So, the few hours that you do sleep, if somebody wakes you up, you get really pissed off… it's like your skin wants to crawl off” (P27).
As mentioned in Theme 1, prior to safer supply, many participants disclosed engaging in criminalized behaviour out of necessity: “crime was a portion of my life in order just to survive” (P14), “I was doing crime. Drug dealing to get money, to feed my habit” (P25). Participation in criminalized behaviours was a common driver of the cycle of drug use participants felt trapped within. One participant noted that fentanyl was a catalyst into criminal activity: “I now have a criminal record where I never had one before” (P20), whereas another found themselves “getting arrested every week, or every two weeks, or every three weeks, by the same person” (P11). Repeated engagement with the legal system was common, with one participant noting they were arrested “eight times in eight months” (P1) and another explaining “I had like 14 charges within the first year… All because of my fentanyl abuse” (P11). Time spent in jail accumulated, for some more than others: “I’m 56 years old, and I have 25 years done” (P19).
Another commonly reported consequence of the cycle of unregulated drug use was repeated overdose events. Given the state of the toxic unregulated drug supply, participants struggled with the unknown of what they were consuming: “through all my many overdoses, I always thought the next one could be it” (P13). One participant described overdosing “up to probably 80 times” (P18), while another stated “I would usually be overdosing at least a few times a week or at least a couple times a month” (P12). One client reported that they “only had overdoses when I tried to” (P6). Suicidal ideations and attempts before safer supply were cited by several participants: “I wanted to die” (P21 and P26), “I kind of almost wish for overdose before to escape it all” (P14). The desire to die tied back into the feelings of hopelessness and powerlessness many participants described: “I didn’t care… I knew, if this was the last one, well, so be it. Didn’t matter. Because you know what? Then I wouldn’t have all these problems anymore” (P17).
Participants described using unregulated fentanyl as “Russian Roulette” (P7) and regarded the unregulated drug supply as extremely inconsistent: “some [unregulated fentanyl] doesn’t even get you unsick… or you could just get totally ripped off and buy something that’s not even fentanyl” (P14). Some participants reported having to guess how much unregulated fentanyl they should use at a time, stating “you can’t just stick with the same average amount… that could be like 10 times stronger than what you were doing the day before” (P13). One participant recounted intense fear and helplessness when using unregulated fentanyl: “I just take the chance every time I push the needle” (P1).
Of importance, many participants reported that the key to disrupting their cycle of drug use was safer supply. Many participants felt as though the consistency of safer supply allowed them to “finally get to a point where we could think of other things than just doing drugs” (P1). Developing a structured routine that did not only revolve around unregulated drugs was helpful for many participants, and repetition of this routine helped immensely: “It’s easier to do learned behaviour multiple times” (P6). Safer supply lessened the sense of anxiety that often accompanied drug cravings and withdrawals, as there was “comfort in knowing that it’s only going to be a little bit longer before I can get better [manage withdrawal symptoms]” (P10). Further, participants were able to re-engage in meaningful activities: “I love swimming… I love writing, I love sitting outside reading books, I love walks, I love going out for outside meals – just normal stuff” (P28).
Context of Substance Use Framework
From these interviews with safer supply participants, an overall framework depicting the context of substance use from their perspective was created (see Figure 1). As PWUD move across the lifespan (line through the centre of the framework), participants described their substance use as a cycle which they felt often controlled the decisions they made day to day. It frequently forced them into participating in certain activities (e.g., criminalized behaviours such as selling unregulated drugs, survival sex work, etc.) to manage their substance use, particularly to address ongoing drug cravings and withdrawal symptoms. Context of substance use framework.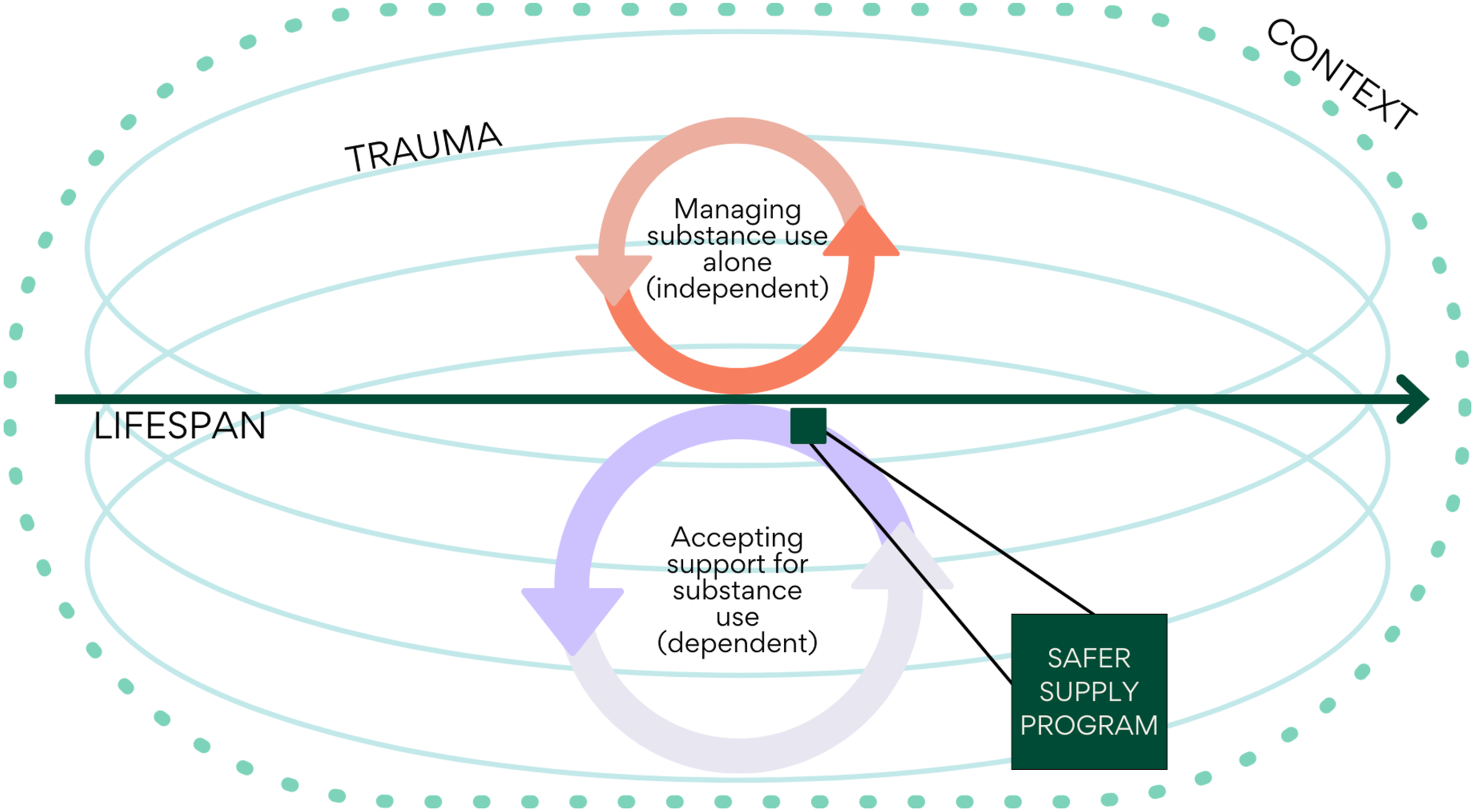
The top orange arrows represent how the participants described managing their substance use alone. This cycle was often described as comprising the following components: 1. The participant experiences drug cravings and withdrawal symptoms. 2. They must access a poisoned unregulated drug supply due to having no access to a regulated supply of drugs. 3. The participant must acquire money to purchase unregulated drugs to manage their ongoing drug cravings and withdrawal symptoms. 4. Given the acuity of the cravings and withdrawal, participants feel forced to participate in criminalized behaviours to acquire money as quickly as possible. 5. Once the money is secured, participants must find a reputable drug dealer; if one is not available, they may have to purchase drugs from someone they do not know or rely on others to acquire drugs for them. 6. Once the drugs are purchased, the participant must find drug equipment and a safe space to use their drugs. 7. Repeat.
The top orange cycle is smaller to represent the participant’s descriptions of managing their substance use independently before safer supply. Participants clearly described a rapid and chaotic cycle of using unregulated drugs in interviews. Participants described this cycle as controlling their lives and ultimately reported feeling trapped within this cycle (making money, acquiring drugs, using drugs, repeat). This is supported by participants having described high levels of chaos surrounding their drug use when they were unable to access appropriate and safe support systems. Conversely, the bottom purple cycle represents participants who are accessing support for their substance use – in this instance, as interviews were completed within safer supply programs, the support system was safer supply, represented by the green square in the purple cycle. The purple cycle is larger as participants described how accessing support (rather than managing their substance use independently in the context of an unregulated toxic drug supply) assisted them in slowing down the cycle of drug use they felt caught within. Participants described in their interviews how the intervention of safer supply helped to lessen the chaos they were experiencing and assisted them in regaining control over their life. It is important to note that the intervention (green square) does not only represent safer supply. This framework can be applied to any form of support (e.g., rehabilitating, treatment, detox, peer support, etc.) that individual PWUD feel is impactful for them.
Finally, surrounding these different components of the framework are the past and current experiences of trauma that permeate the lives of PWUD, as well as the context of substance use and how that impacted the participants. Firstly, the four blue ovals labelled as trauma represent the past and current experiences of trauma which participants described as impacting their substance use. In fact, some participants noted that they began to use drugs to manage traumatic memories and experiences – many of them found substances to be a helpful coping mechanism. Secondly, the green dashed line surrounding the framework represents how participants spoke about the overarching societal context of their drug use, and how the ongoing stigma, criminalization, and marginalization of being a person who uses drugs informed the vast majority of their experiences with people outside of the community of PWUD.
Discussion
In this paper, we reported on the results of semi-structured interviews with 30 safer supply program participants. Overall, two themes arose from these interviews, including the impacts of trauma, marginalization, and substance use, as well as the cycle of drug use. Participants highlighted how the historical and current context of their substance use impacted their lives, and conversely, how their substance use was impacted by the context of their life experiences, such as previous trauma. From this, a framework depicting the context of drug use as described by participants was created, as seen in Figure 1. Overall, our results raise a number of important points of discussion.
First, our results reinforced the importance of understanding the context of drug use among PWUD when developing harm reduction programs, such as safer supply in this instance. When considering any harm reduction based service, it is essential to note that the creation of harm reduction programs has consistently been led by PWUD and is often associated with civil disobedience (Boyd et al., 2009). For example, one of the first supervised consumption sites in Canada was Back Alley, opened in 1996 by PWUD in Vancouver, Canada as a response to a growing number of overdose deaths in the city. The PWUD working at Back Alley successfully reversed many drug overdoses – with no drug fatalities – before they were shut down by law enforcement approximately a year after they opened (Boyd et al., 2009). Similar PWUD-led origin stories can be found with regard to other harm reduction programs, such as safer supply and sterile drug equipment distribution. This is an important finding as it reinforces the need to include PWUD in the design, implementation, and evaluation of any substance use-focused program to ensure it is useful and impactful for the community. The risk of developing programs without the involvement of PWUD includes funding and program development that further marginalized PWUD, or even worse, harms them. For example, a study was done with racialized (Black, Indigenous, or people of colour) PWUD to better understand their perspectives regarding harm reduction service access. Overall, a central result of this research was that whiteness in harm reduction programs pose a barrier for racialized PWUD. Further, the individuals interviewed provided clear changes they sought to see in harm reduction programs to better serve the community (Godkhindi et al., 2022).
Second, many current understandings of drug use rely on describing unregulated drug use as either a health concern or as a criminalized behaviour. In the former, healthcare providers often rely on classifying substance use based on resources such as the Diagnostic and Statistical Manual of Mental Disorders (DSM), now in its fifth edition (American Psychiatric Association, 2013). The DSM-5 is influenced by a biomedical, postpositivist understanding of psychological health wherein individual symptoms are pathologized. Should the client’s reported symptoms sufficiently align with the DSM criteria for a substance use disorder, a diagnosis may be explored. While the DSM undoubtedly has utility in many circumstances, critics have described it as “a grab bag of contextless symptoms, divorced from the complexities of people’s lives and the social structures that give rise to them” (Burstow, 2003, p. 1296). In the latter, the label of criminal is applied to PWUD through the reinforcement of problematic and dangerous drug policies and legislation. Overall, labelling PWUD as both a criminal who is actively breaking the law and a patient who is unwell creates immense ostracization and forces navigation of an impossibly unpredictable landscape (Krausz & Jang, 2018). Both understandings of drug use fail to acknowledge and incorporate the overarching context of drug use.
In opposition to these labels, this research highlights the use of unregulated substances as an important coping mechanism and response to trauma. Participants challenged the ways in which drug use is typically portrayed and sought to highlight both the benefits and consequences of drug use. For example, while participants did disclose feelings of shame and hopelessness they associated with their drug use, they also described the utility of drug use in managing previous and ongoing traumatic experiences. For many, drug use was a means to survive. Indeed, there is a well-established collection of research which describes the association between unregulated substance use and previous trauma, particularly with regard to childhood trauma and abuse (Carliner et al., 2016; Halpern et al., 2018). Participants in our study delved into this further and spoke about the use of substances such as opioids to relieve uncomfortable mental health symptoms (e.g., depression, anxiety) which were often related to previous experiences and memories of trauma. The importance of being able to use unregulated drugs to manage mental health concerns was further underscored by participant disclosures of negative experiences within the healthcare system when attempting to access care. This commonly resulted in a lack of trust in healthcare providers as well as avoidance of healthcare services altogether. This creates a dangerous chain of events: PWUD are commonly categorized as a marginalized group who should be prioritized for healthcare services; PWUD are treated poorly when they attempt to access healthcare services; PWUD do not feel safe accessing healthcare and do not access these services regularly. Ongoing stigma and marginalization are common occurrences recounted by PWUD when discussing accessing the healthcare system (Biancarelli et al., 2019; Muncan et al., 2020; van Boekel et al., 2013), demanding re-evaluation of how healthcare services, programs, and pathways can be adapted to meet the needs of PWUD. This research emphasizes the need for healthcare service providers, politicians, policymakers, researchers, and others involved with PWUD to consider both the benefits and consequences of substance use through a trauma-informed, strengths-based approach.
Third, the finding of feeling controlled by an ongoing cycle of drug use was emphasized by nearly all our participants. This cycle consumed their lives and often resulted in feelings of powerlessness and a loss of autonomy. This finding aligns with previous harm reduction research which spoke with women who use drugs. This study found that women described the process of injection drug use as a “cycle of obtaining capital to purchase [drugs] and, ultimately, fulfilling their cravings” (Kitson & O’Byrne, 2021, p. 139). Our research explores this further and found that safer supply was a tool which allowed participants to interrupt and slow down the cycle of drug use. Participants discussed having more space to re-prioritize certain aspects of their lives, as well as engage in future and goal-oriented thinking once they were engaged in a safer supply program. As previously mentioned, the phenomena of support interrupting and slowing down the cycle of drug use is not unique to safer supply programs. Instead, it is important to consider that any support or service (e.g., Opioid Agonist Treatment, Narcotics Anonymous, rehabilitation, detox, etc.) that PWUD find effective and useful to manage their personal substance use would apply. This reinforces the importance of providing a spectrum of services to PWUD, including harm reduction based programs such as safer supply. Other services should include low-barrier access to supervised consumption sites (including drug inhalation sites), substance use treatment, rehabilitation, detox services, housing workers, counselling services, take-home sterile drug use equipment and naloxone programs, peer support, and primary care.
Limitations and Future Directions
This research project allowed for the voices of PWUD to be at the forefront of describing their experiences within safer supply programs. However, it is important to note a few limitations and describe our recommendations for the future directions of safer supply research. This research only spoke with PWUD who were currently engaged in a safer supply program. This meant that participants who may not have been retained on program were not eligible to participant. More research is needed to speak with participants who were not maintained on safer supply to understand their experiences and barriers to care. This research did not include a control group, meaning that objective program impacts could not be studied. Given the research objectives of understanding subjective participant experiences, a control group was not needed at this time. Ongoing safer supply research would benefit from large longitudinal studies involving participants in safer supply programs examining several important quantitative and qualitative outcomes. These could include outcomes such as adherence or retention in the program, all-cause and substance use-specific mortality, engagement in criminalized behaviours, changes to unregulated drug use, and other quality of life indicators. More research is needed to better understand safer supply programs which are based on a non-medical model of care, such as compassion and buyers’ clubs. Additionally, research focusing on safer stimulant programs in particular is needed given the growing harms related to unregulated stimulant use.
Conclusion
The toxic unregulated drug supply continues to be a predominant driver of the drug poisoning crisis which has resulted in over 40,000 deaths in Canada. To address this crisis, it is essential to consider the needs of PWUD, including the context of drug use. To better understand this, we completed interviews with 30 safer supply program participants. These interviews revealed the impact of the historical and ongoing effects of trauma on the lives of PWUD, as well as the complex cycle of drug use as depicted by research participants. Overall, participants described a cycle of drug use before safer supply (when they were limited to accessing drugs through the unregulated toxic drug supply) that was chaotic and all-consuming. Once participants joined a safer supply program, they felt as though this allowed them to regain a degree of autonomy and freedom in their lives. A framework was created to better depict the context and underlying factors driving this cycle of drug use. Further, our findings highlighted the need for taking into consideration the context of substance use when developing programs for PWUD, which includes the potential pitfalls of criminalizing or medicalizing substance use. Instead, participants emphasized the importance of situating their substance use in the context of trauma, marginalization, and stigma. Ultimately, many participants found participating in a safer supply program useful to disrupt the cycle of drug use they felt trapped in and regain decision-making power with regards to their substance use.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Health Canada’s Substance Use and Addictions Programs (grant # 2021-HQ-000059).