
Abstract
Workplace policies are important because employee rates of alcohol and drug misuse can be associated with work-related risk factors in the United States. To explore the associations, this study analyzed the 2010–2014 National Survey on Drug Use and Health datasets. The overall sample size was 130,726, and the SUD outcome variables included alcohol, marijuana, pain reliever, and illicit drug use disorders. 20% of participants reported no substance use policies in their workplace. Significant associations were identified between all four measured SUD outcome variables, the presence of specific substance use workplace policies, and individual employment sectors. Specifically, comprehensive policies out of six policies were significantly associated with decreased SUDs in nearly every employment sector. The results of this study suggest that workplace substance use policies are important to prevent the development of employee SUDs and comprehensive policies in place can be most effective.
Keywords
Introduction
The prevention of substance misuse has historically been a significant public health policy goal in the United States over the past several decades. Federal grant programs such as Drug Free Communities have created community prevention coalitions that implement environmental prevention strategies in neighborhoods across the U.S., and prevention programming such as the Good Behavior Game or Too Good for Drugs have also been implemented in many schools across the country (Centers for Disease Control and Prevention, 2021; Community Anti-Drug Coalitions of America, 2021). However, one element of prevention that has routinely been overlooked by researchers and prevention specialists in the field is adult prevention, and specifically, the impact of substance use workplace policies (SUWPs). Given that approximately two-thirds of U.S. residents have been employed in the labor force at some point over the past decade (U.S. Bureau of Labor Statistics [BLS], 2022b), workplaces provide largescale opportunities for implementing mental and behavioral health interventions for the adult population. Workplace policies and environments are particuarly important because research suggests that employee rates of alcohol and drug misuse are associated with work-related risk factors. Work stressors, workplace substance availability (i.e., physical access to substances), workplace cultural norms, workplace social norms, and workplace social controls have also been identified as factors that influence employee substance use disorders (SUDs; Chapman et al., 2021; Frone, 2019). As such, the literature base supports the theory that implementing workplace policies that strengthen or mitigate these factors can effectively help to prevent employees from developing SUDs.
In terms of workplace factors affecting SUDs by industry type, workers in goods-producing industries such as construction or mining are at a high-risk for the development of substance misuse issues due in part to the fact that risky and physically demanding work environments have been shown to be associated with heavy alcohol use (Barnes & Zimmerman, 2013; Prins et al., 2019) and nonmedical prescription opioid or illicit opioid use (Ompad et al., 2019; Rosen et al., 2021). Additionally, construction trade and extraction workers have been shown to be more likely to report past-month cocaine and nonmedical prescription opioid use (Ompad et al., 2019). The literature also shows that opioid prescription rates and hydrocodone shipments were positively correlated with the overall employment share in goods-producing industries (Bryson et al., 2022), and evidence suggests that higher prevalence rates of opioid use disorders among these populations can mainly be attributed to workplace injuries (Applebaum et al., 2019; Cooper & Bixler, 2021) and work-related stressors (Cooper & Bixler, 2021). A study regarding Australian construction workers’ illicit drug use also revealed that workplace climate factors such as substance availability, injunctive norms, and descriptive norms, were also associated with employee cannabis and meth/amphetamine use (Chapman et al., 2021). Finally, research suggests that workers’ substance misuse can adversely impact organizational health, reduce workplace safety, and increase organizational costs, making employee substance misuse a significant organizational concern for employers (Burke, 2019; de Oliveira et al., 2020; Goplerud et al., 2017; Sorge et al., 2020).
Workplace Substance Use Rates
According to NSDUH data compiled from 2008-2012, 8.7% of full-time workers aged 18 to 64 engaged in heavy alcohol use (past month), 8.6% engaged in illicit drug use (past month), and 9.5% met the criteria for a SUD (past year). Mining (17.5%), construction (16.5%), accomodations and food service (11.8%), and arts, entertainment, and recreation industries (11.5%) were shown to have the highest prevalence rates for heavy alcohol use, while the accomodations and food service (19.1%), arts, entertainment, and recreation (13.7%), management (12.1%), and information industries (11.7%) had the highest rates of past-month illicit drug use. Workers in the accommodations and food services industry had the highest past-year SUD rates at 16.9%, followed by construction (14.3%), arts, entertainment, and recreation (12.9%), and mining (11.8%). Healthcare and social assistance, public administratoin, and the educational service industries were ranked among the bottom four industries for heavy alcohol use, illicit drug use, and the prevalance of employee SUDs according to the NSDUH (Bush & Lipari, 2015).
Workplace Substance Use Policies
A growing body of international research has begun to examine the impacts of organizational programs and policies on employee substance misuse prevalence rates (Pidd et al., 2016). More specifically, researchers in Australia found that the implementation of SUWPs reduced heavy alcohol use, and that comprehensive substance use policies decreased illicit drug use among Australian employees. Additionally, workplace drug testing has been shown to be effective at preventing marijuana use among construction and trade workers in the U.S. (Ompad et al., 2019), and data from the 2008–2012 NSDUH showed that full-time workers aged 18 to 64 who used illicit drugs (past month) or drank heavily (past month) were less likely to work for an employer with a written SUWP (Bush & Lipari, 2014).
Study Purpose and Hypotheses
Despite evidence suggesting that workplace environments can serve as a critical access point for implementing public health interventions to reduce substance misuse and the development of SUDs in the adult population (Shaw et al., 2020), research shows that SUWPs have historically been undervalued and underutilized in the U.S. (Rosen et al., 2021). While recent studies have been able to identify relationships between SUWPs and trends in employee substance use patterns (Cooper & Bixler, 2021), a lack of knowledge still exists regarding the relationship between SUWPs and employee substance trends. The current study seeks to bridge that gap by exploring the effects of workplace policies on the development of employee SUDs. In this context, the study identifies WSUP implementation rates and employee SUD rates and explores associations between categories of WSUP, types of employment, and employee SUD rates. In relation to the study, the following hypotheses were explored: 1) U.S. workers in goods-producing industries will have higher prevalence rates for past-year substance use disorders than those working in service-providing industries; 2) implementation of any substance use workplace policies will be associated with decreased rates of past-year substance use disorders; and 3) the subcategories of the substance use workplace policies will be differentially associated with past-year substance use disorders.
Methods
Sampling and Participants
To examine the research questions regarding how different types of SUWPs influence employee SUD rates in various workplace settings, this study analyzed datasets from the 2010–2014 NSDUH which is a nationally representative, cross-sectional survey conducted annually for the purpose of estimating rates of drug use and mental illness among non-institutionalized U.S. residents aged 12 or older (Center for Behavioral Health Statistics and Quality [CBHSQ], 2018). The NSDUH’s sampling design is based on multistage area probability sampling and uses a 4-stage stratification process based on geographic/demographic variables including state of residence, sampling region, area segment, and type of dwelling (CBHSQ, 2018).
Participants in the NSDUH surveys were interviewed by Computer-Assisted Personal Interviewing and Audio Computer-Assisted Self-Interviewing techniques, and the weighted interview response rates ranged from 71.2% to 74.6%. For the purposes of this study, participants included in the analysis sample were defined as individuals who were 18 years or older and employed full time or part time in the labor force at the time of the survey. The final sample size utilized in the analyses was 130,726 individuals.
Measures
Employee Substance Use Disorders
A past-year SUD for alcohol, marijuana, pain relievers, or an illicit drug use disorder were selected as outcome measures for the study and were identified in the sample based on assessment criteria specified in the Diagnostic and Statistical Manual of Mental Disorders (DSM), fourth edition (American Psychiatric Association, 2000). An illicit drug use disorder was defined as “any kind of illicit drug dependence/abuse other than marijuana dependence/abuse” (Choi et al., 2016). Responses for each SUD category were dichotomously coded as 0 = no/unknown and 1 = yes.
Substance Use Workplace Policies
NSDUH participants were asked five questions designed to identify if their workplace had drug and alcohol policies in place at the time of the survey (CBHSQ, 2018). These questions included: (1) “At your workplace, is there a written policy about employee use of alcohol or drugs?“, (2) “At your workplace, have you ever been given any educational information regarding the use of alcohol or drugs?“, (3) “Through your workplace, is there access to any type of employee assistance program or other type of counseling program for employees who have alcohol or drug-related problems?“, (4) “Does your workplace ever test its employees for alcohol use?“, and (5) “Does your workplace ever test its employees for drug use?”
Each survey response was originally coded dichotomously (1 = yes, 2 = no), however, after aggregating the responses, the data was recoded into six dichotomous umbrella policy categories (0 = no policy, 1 = any policy) based on previous research conducted by Pidd et al. (2016). The six umbrella categories consisted of none (no policies in place), use (a written policy on alcohol/drug use only), use plus testing (a written policy on alcohol/drug use and/or alcohol/drug testing), assistance (provision of educational information and/or assistance regarding alcohol/drugs only), use plus assistance (a written policy on alcohol/drug use plus information/assistance), and comprehensive (a written policy on alcohol/drug use plus alcohol/drug testing plus information/assistance).
Workplace Categories
Workplace categories were defined and stratified according to the occupation categories listed in the 2003 Census codes (CBHSQ, 2018). Additionally, the categories were dichotomized into goods-producing industries (agriculture, forestry, fishing, & hunting; Mining; Construction; manufacturing, nondurable goods; manufacturing, durable goods) and service-providing industries (transportation & utilities; information & communications; wholesale trade, durable goods; wholesale trade, nondurable goods; retail trade; finance, insurance, real estate, rental, & leasing; professional and scientific services, management, administrative services, & waste management; education, health & social services; arts, entertainment, and recreation, & accommodation and food services; public administration; other services) based on all the categories listed in the North American Industry Classification System (NAICS) code (BLS, 2022a; Cartwright et al., 2011). This method of employment stratification was selected based on its use in previous NSDUH analyses (Bush & Lipari, 2015).
Sociodemographic Associations
Demographic information analyzed in the study included sex (male, female), race/ethnicity (White, non-White), marital status (married, not married), age (18–34 years, 35–49 years, 50 years and older), educational attainment (less than high school, high school graduation, some college, college graduation), annual income (less than $20,000, $20,000–$49,999, $50,000–$74,999, $75,000 or higher), urbanicity (urban, rural), and perceived health status (poor/fair, good).
Data Analysis
STATA 17.1 (StataCorp, 2017) was utilized to conduct all analyses. Due to the complexity of the NSDUH’s survey design, the analyses were conducted in three steps. First, descriptive and bivariate analyses were utilized to describe and compare the prevalence rates of SUWPs and the rate of employee SUDs based on workplace categories. Second, multiple logistic regression analyses were utilized to explore for associations between SUWPs and SUDs. Finally, multiple logistic regressions were employed again to identify the effects of SUWPs on employee SUDs with regard to their employment sector.
Results
Descriptive Statistics
Demographic Characteristics of People who Employed, From National Survey on Drug Use and Health 2010–2014 (Unweighted n = 130,726).
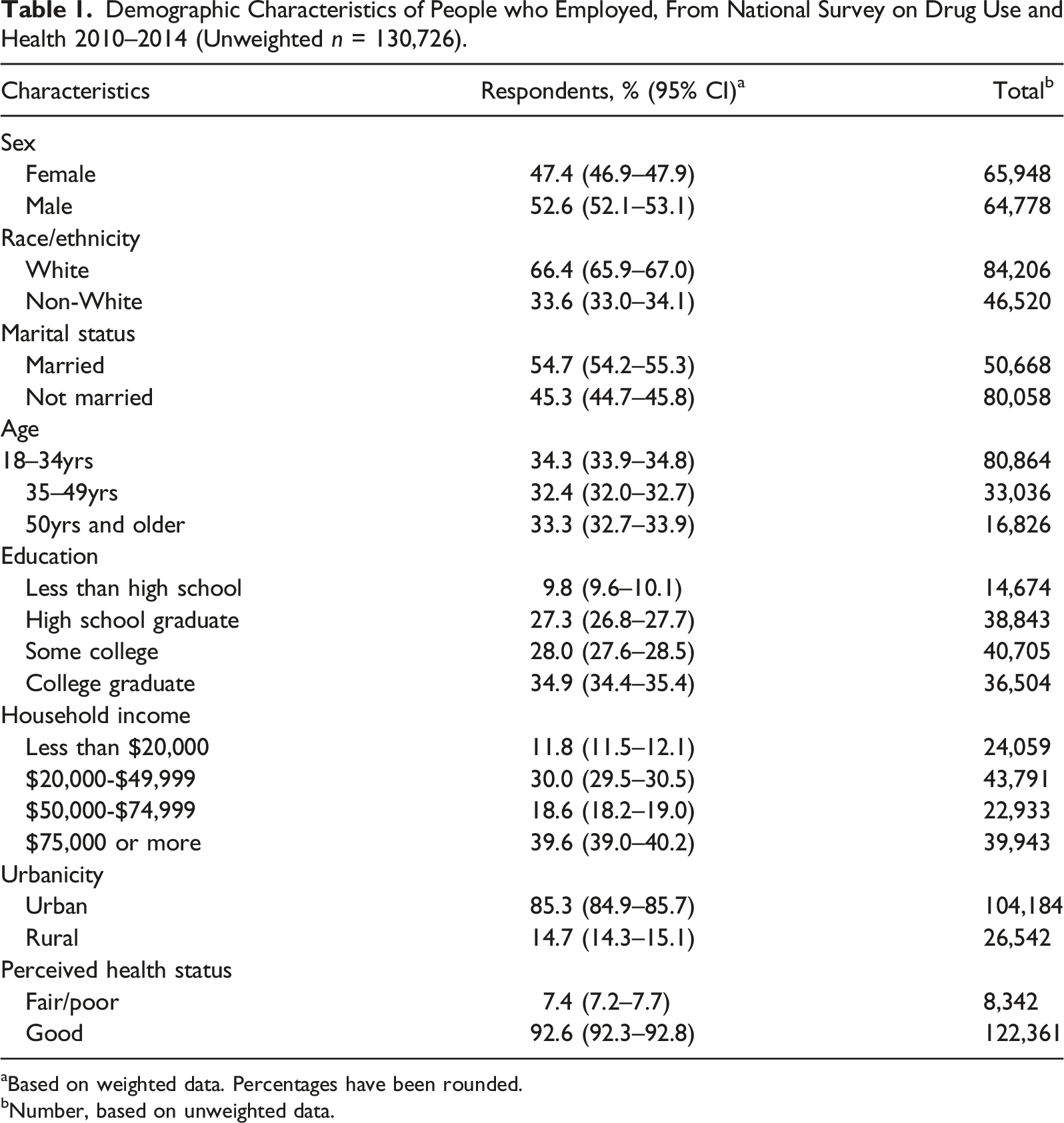
aBased on weighted data. Percentages have been rounded.
bNumber, based on unweighted data.
Workplace Substance Use Policy Prevalence
Workplace Substance Use Policy Prevalence (%) by Industry Group (Unweighted n = 130,726).
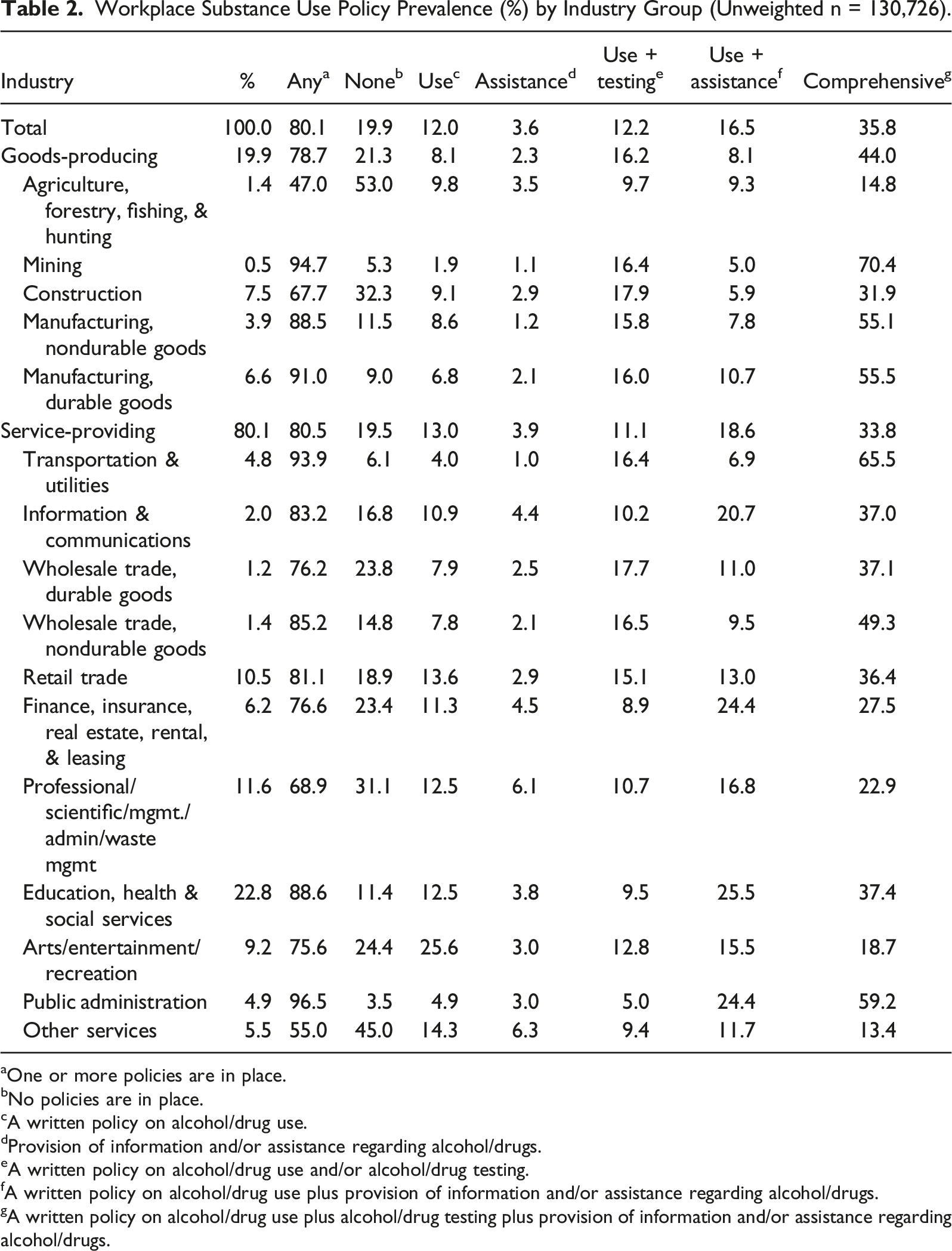
aOne or more policies are in place.
bNo policies are in place.
cA written policy on alcohol/drug use.
Provision of information and/or assistance regarding alcohol/drugs.
A written policy on alcohol/drug use and/or alcohol/drug testing.
A written policy on alcohol/drug use plus provision of information and/or assistance regarding alcohol/drugs.
A written policy on alcohol/drug use plus alcohol/drug testing plus provision of information and/or assistance regarding alcohol/drugs.
Employee Substance Use Disorder Prevalence
Employee Substance Use Disorder Prevalence (%) by Industry Group (Unweighted n = 130,726).
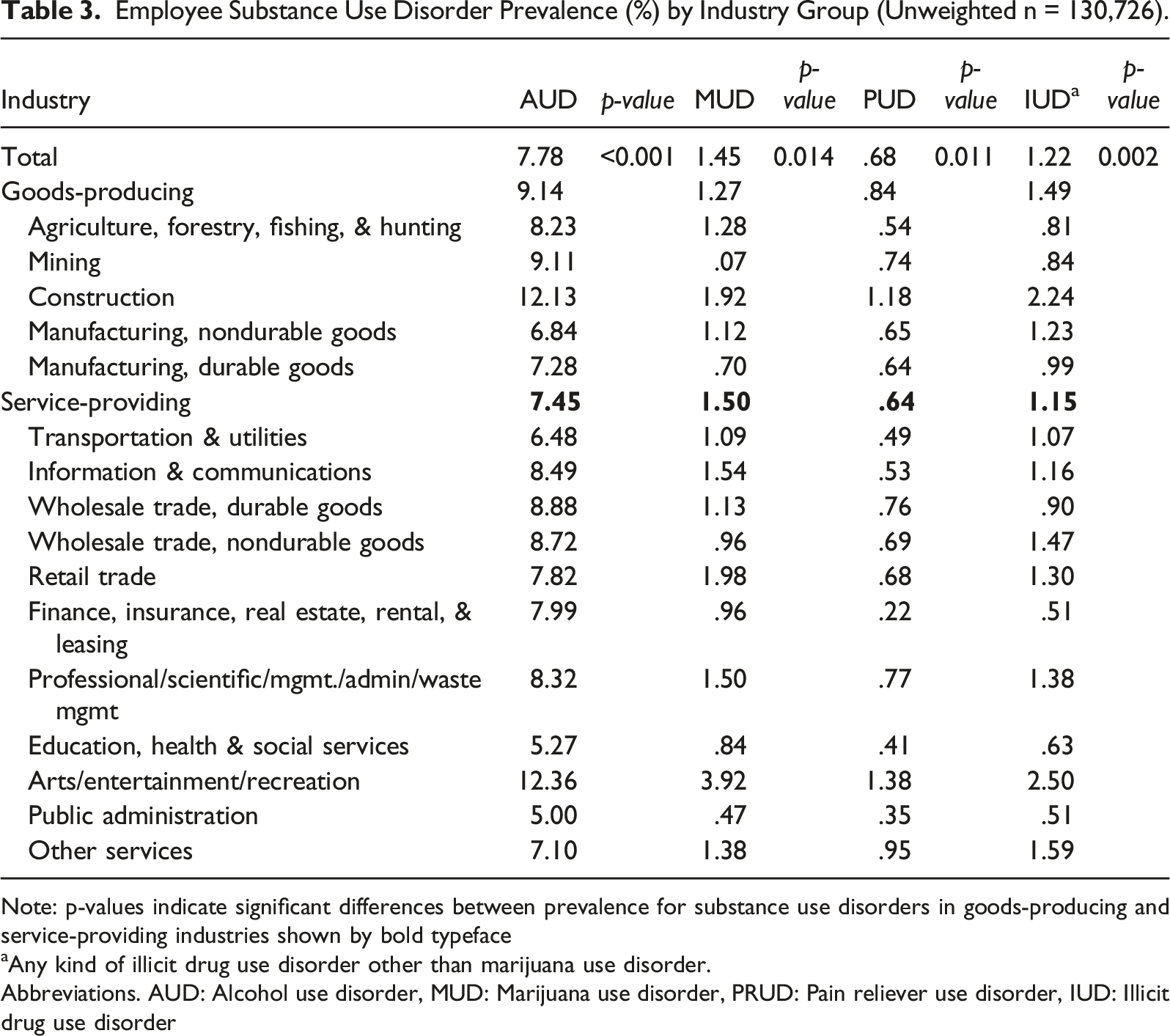
Note: p-values indicate significant differences between prevalence for substance use disorders in goods-producing and service-providing industries shown by bold typeface
Any kind of illicit drug use disorder other than marijuana use disorder.
Abbreviations. AUD: Alcohol use disorder, MUD: Marijuana use disorder, PRUD: Pain reliever use disorder, IUD: Illicit drug use disorder
Associations Between Workplace Substance Use Policies and Employee Substance Use Disorders
Associations Between Any workplace Policy and Substance Use Disorders (Unweighted n = 130,673).
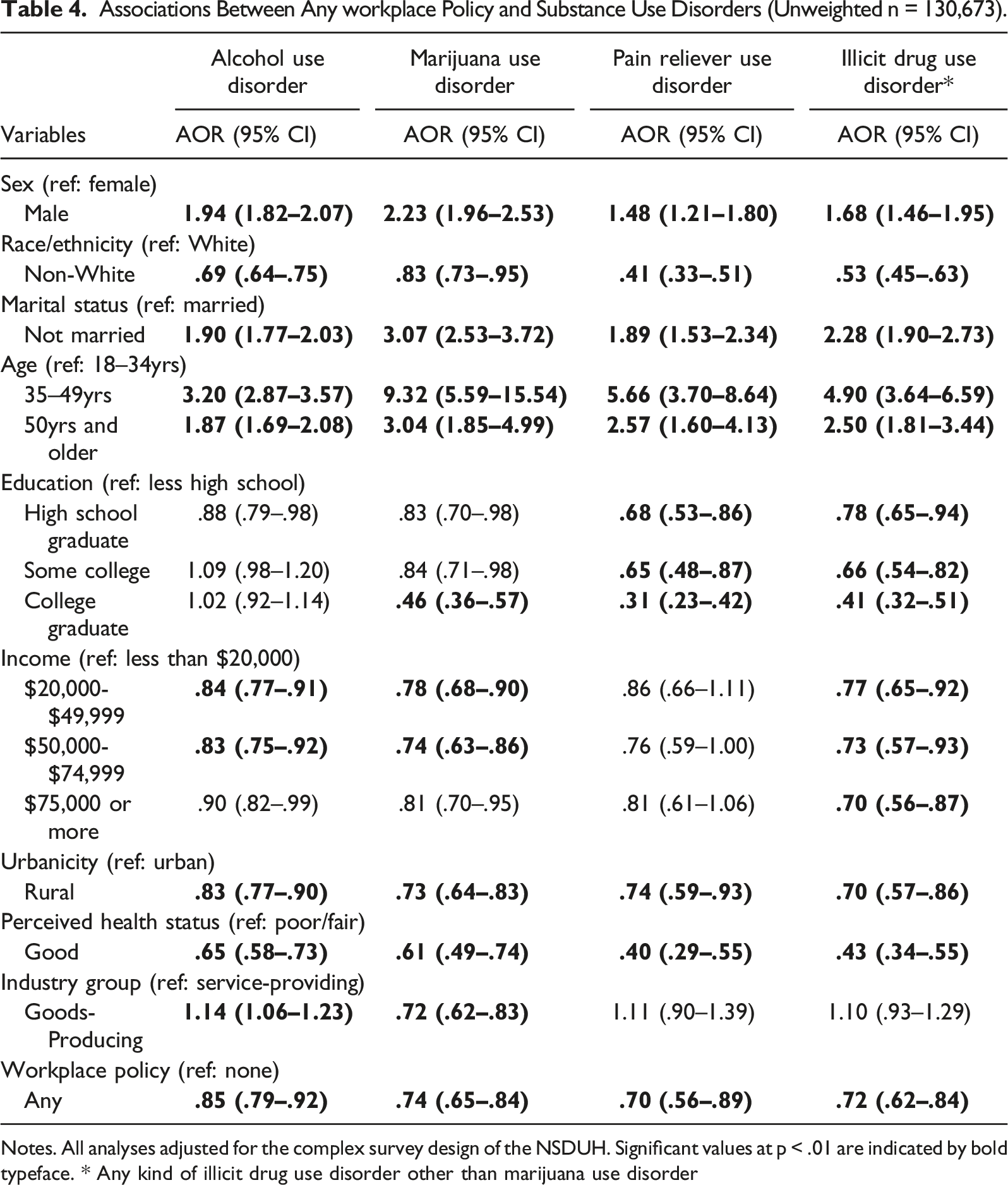
Notes. All analyses adjusted for the complex survey design of the NSDUH. Significant values at p < .01 are indicated by bold typeface. * Any kind of illicit drug use disorder other than marijuana use disorder
Associations Between Substance Use Policy Type and Substance Use Disorders by Workplace Category
Associations Between workplace Policies and Substance Use Disorders by Industry Group (Goods-Producing [Unweighted n = 23,797] vs. Service-Providing [Unweighted n = 106,876]).
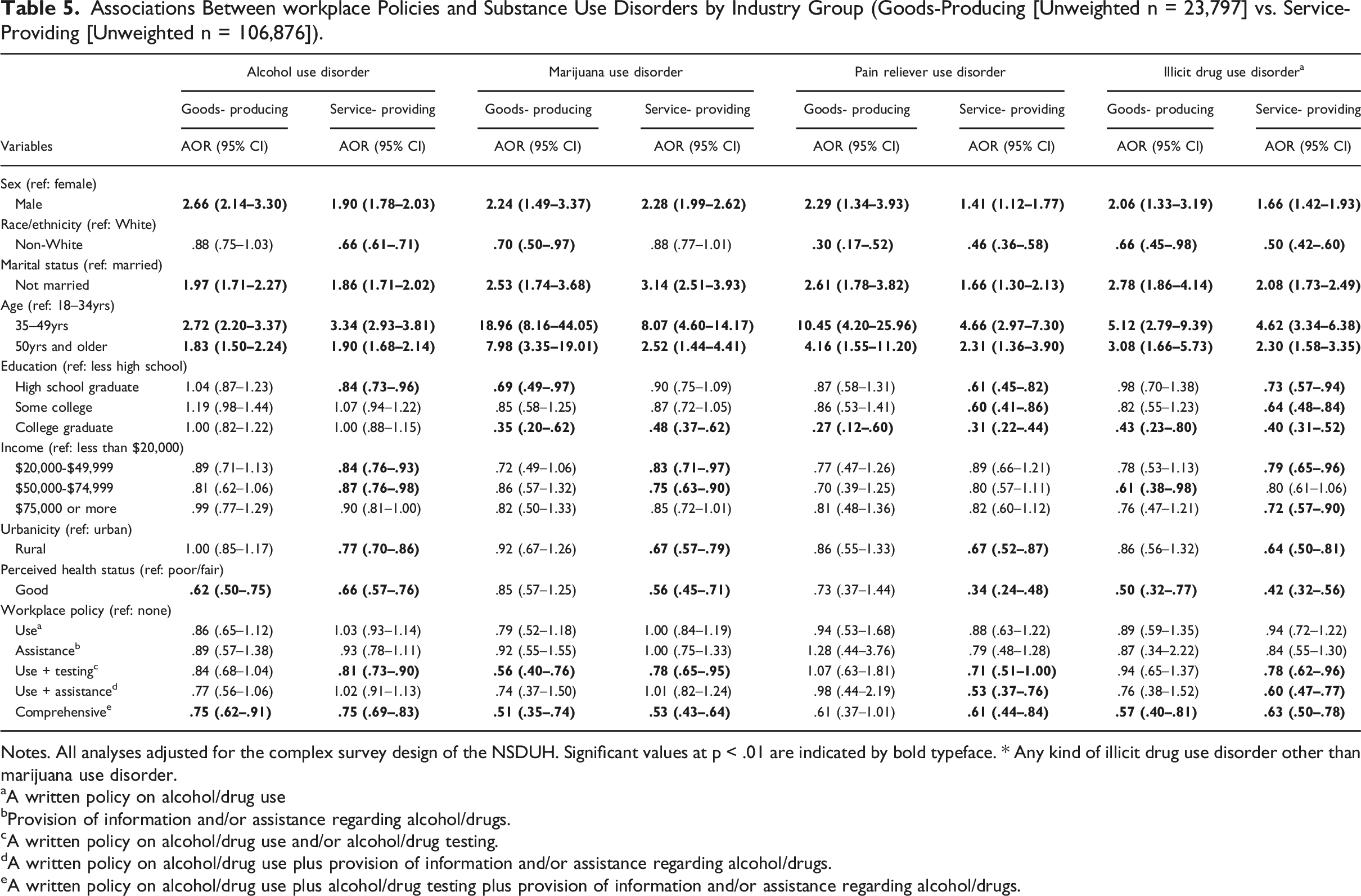
Notes. All analyses adjusted for the complex survey design of the NSDUH. Significant values at p < .01 are indicated by bold typeface. * Any kind of illicit drug use disorder other than marijuana use disorder.
aA written policy on alcohol/drug use
bProvision of information and/or assistance regarding alcohol/drugs.
cA written policy on alcohol/drug use and/or alcohol/drug testing.
dA written policy on alcohol/drug use plus provision of information and/or assistance regarding alcohol/drugs.
eA written policy on alcohol/drug use plus alcohol/drug testing plus provision of information and/or assistance regarding alcohol/drugs.
In regard to the six SUWP categories, no significant associations were found between use or assistance policies and any of the measured SUD categories. Implementation of use plus testing policies in service-providing industries were associated with decreased odds for developing all four types of SUDs, while use plus testing policies in goods-producing industries were associated with decreased odds of developing MUD only (AOR = .56, 95% CI = .40–.76). Implementation of use plus assistance policies in service-providing industries were also associated with decreased rates of PRUD (AOR = .53, 95% CI = .37–.76) and IUD (AOR = .60, 95% CI = .47–.77). However, there was no significant association between use plus assistance policies and any SUD category in the goods-producing sector. Finally, and most importantly, respondents working in any employment sector with comprehensive policies in place were less likely to have any type of SUD, with the exception of PRUD for respondents who worked in goods-producing industries.
Discussion
The results of this study produced several significant findings in relation to SUWPs, employee SUD rates, and industry SUD rates in the United States. According to the study’s findings, around 20% of respondents identified that their workplace did not have any type of SUWP. More specifically, over half of respondents who worked in the agriculture, forestry, fishing, and hunting sectors reported not having a SUWP, whereas only 3% of workers in the public administration sector identified that their workplace did not have a SUWP. In regard to employee SUD rates, workers in construction showed higher prevalence rates for all types of SUDs within the goods-producing sector, while notably, workers in the arts, entertainment, and recreation sector reported the highest prevalence rates for all types of SUDs among all industry sectors. Given the consistency of these results with previous studies that showed high prevalence rates of binge drinking (30.3–30.6%) and past-year SUDs (12.9–16.9%), further research is warranted to identify specific work-related SUD risk factors in the arts, entertainment and recreation, and accommodation and food service sector (Bush & Lipari, 2015; Shockey & Esser, 2020).
In addition to the findings regarding SUWP implementation rates and SUD prevalence rates, this study also identified several sociodemographic factors that place employees at greater risk for developing a SUD. In regard to the sociodemographic variables, positive associations were identified between sex (male respondents), marital status (not married respondents), age (35–50 years and older respondents), and a past-year SUD. AUD was also found to be positively associated with the goods-producing sector, a result that is in line with previously conducted studies (e.g., Barnes & Brown, 2013; Pidd et al., 2016). One result that was identified that was unexpected was that workers in the service-providing sector were found to be more likely to have MUD than those in the goods-producing sector. This finding runs counter to previous studies that have suggested that employees in the goods-producing sector have a higher prevalence rate for marijuana use (Graber et al., 2016; Ompad et al., 2019).
In regard to categories of SUWPs and their effectiveness in different employment sectors, the results of the study showed that a single policy (e.g., a written policy only, assistance only) was not an effective prevention measure for any of the SUD categories. However, use plus assistance policies decreased rates of PRUD and IUD, and the implementation of use plus testing policies were shown to be effective at decreasing all types of SUDs in the service-providing sector. This finding is consistent with research conducted by Ompad et al. (2019), which identified that random drug testing in the workplace is associated with decreased rates of marijuana use among construction, trade, and extraction workers. Finally, comprehensive policies, which were the most prevalent type of implemented policy reported in the study, were shown to decrease rates of nearly all SUDs in all employment categories with the exception of PRUD in the goods-producing sector. Workers in industry sectors where comprehensive policies were implemented at a lower rate (e.g., construction, arts/entertainment/recreation) also reported relatively higher rates of SUDs than those working in other employment sectors.
Despite the overall effectiveness of SUWPs at preventing the development of various employee SUDs, they were not shown to have a significant association with PRUD for respondents working in the goods-producing sector. Of the five goods-producing industries, construction was shown to have the highest prevalence rate for PRUD. These results suggest the need for additional prevention efforts that target opioid use for employees in male-dominated industries. In regard to this need, workplace training programs on opioid use awareness have been shown to effectively increase training knowledge of opioid risk factors and prevention resources (Persaud et al., 2021, 2022). However, future work is still needed to examine the effects of trained instructors’ education on substance use prevention among employees.
Comprehensive workplace policies that involve recovery-friendly workplace initiatives have also been shown to reduce employee opioid use (Cooper & Bixler, 2021; Imboden et al., 2021; Osborne et al., 2021; Rosen et al., 2021). Recent research suggests that workplace cultures that reduce stigma for workers with mental health or SUD issues can serve as effective prevention measures (Roche et al., 2015; Rosen et al., 2021; Seaton et al., 2019). Conversely, masculine workplace cultures in male-dominated industries tend to limit workers’ disclosure about injury and vulnerabilities (Seaton et al., 2019) and elevate their perception of workplace drug availability (Chapman et al., 2021; Roche et al., 2015). Punitive SUWPs can also create stigmatizing work cultures that produce a fear being marginalized by co-workers, leaders, and employers, which, in turn, can hinder employee access to substance use treatment (Rosen et al., 2021). Thus, future research needs to further identify the effectiveness of recovery-friendly and stigma-reducing workplace initiatives in male-dominated industries.
Limitations
There are several limitations associated with this study. First, the NSDUH data was collected using self-reported surveys which contain inherrent bias concerns and the potential for under or over reporting on survey items. Second, the survey was cross-sectional and therefore can not identify the longitudinal effects of SUWPs on SUD prevalence rates. Additionally, this study did not address the effects of geographic factors, education-level, or industry size characteristics on differences in SUD prevalence rates by industry. Thus, the prevention effect of SUWPs could be affected by possible confounding factors, and in particular, geographic regions. Considering the geographic variations in SUD prevalence rates (Aliprantis et al., 2019; Veldhuizen et al., 2007) and the size of industry sectors (Henderson, 2015), future research is needed to identify the impact of these variables on SUWPs and SUDs. Finally, because the employment sectors were grouped into larger categories in the analytical process, inferences about individual professions cannot be made based on the findings of the study.
Conclusions
The results of this study identified that U.S. workers in goods-producing industries had higher prevalence rates for AUD and IUD, while those working in service-providing industries had higher prevalence rates for MUD. Additionally, this study identified that the arts, entertainment, and recreation sector had the highest prevalence rates for all types of SUDs among all industry sectors. Finally, this study identified that comprehensive SUWPs significantly reduced the presence of all four types of SUDs regardless of employment sector with the exception of PRUD in the goods-producing sector. Based on these findings, it is suggested that (a) employers in goods-producing industries emphasize AUD and IUD policies while employers in the service-providing industry emphasize MUD policies, (b) employers in the arts, entertainment, and recreation sector ensure that they strategically market and enforce SUWPs with current and new employees, and (c) employers ensure that they have a comprehensive SUWP in place to prevent and/or reduce the risk of employees developing an SUD and to promote a healthy work environment. It is also suggested that researchers expand on this line of inquiry to account for potential industry differences related to geographic area, education-level, industry size, and their impacts on SUD rates.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.