
Abstract
Swedish drug policy has a strong focus on minor drug violations. This longitudinal study analyses the association between criminality and substance use problems among young people who have received outpatient treatment and risk factors that predict continued problems with criminality. Research on this target group is under development in Sweden, but there are few follow-up studies. The study indicates that about one-quarters of the young people who begin outpatient treatment have been convicted of crimes at 1-year follow-up. Most of them who had been convicted with offences also have ongoing problems with substance use and three-quarters of the young people had been charged with a drug-related offence. More than five risk factors give an elevated risk of continued criminality. Interventions meeting the needs of young people, moving away from the current emphasis on penal law principles, may also contribute to reduced criminality in this target group.
Introduction
Adolescence is a developmental stage often characterised by various kinds of risk-taking, such as experimentation with alcohol, drugs, sexuality and criminal activities. Most people commit minor offences at one time or another in their youth (Bäckman, Estrada, Nilsson, & Shannon, 2014). Half of Swedish pupils in year nine report having committed some kind of crime at some point (National Council for Crime Prevention 2020), while an equal percentage has also been victims of crime. The 15–20-year-old group accounts for one-fifth of all criminal charges, even though this age range constitutes only 8% of the total population (National Board of Health and Welfare 2020). Most commit isolated offences while a small group tends to commit numerous illegal acts. Youth crime in Sweden has generally declined in the past decade, especially among young people aged 15–17 years (National Council for Crime Prevention 2019; Bäckman et al. 2014), but narcotics offences have more than doubled during the same period (National Council for Crime Prevention 2019). Most cannabis-related offences in the Nordic countries are linked to use or possession for personal use (Egnell, Villman, & Obstbaum, 2019). However, the percentage of young people convicted for personal use is higher in Sweden than in the other Nordic countries. Several sanctions for drug-related crime also risk reinforcing social exclusion.
Binge drinking and use of alcohol has declined among Swedish youth in recent decades and is at “continued and historically low levels” (Swedish Council for Information on Alcohol and Other Drugs, 2019, p. 8). The proportion of secondary school pupils who report that they have used drugs (primarily cannabis) in the past 12 months is 13%. A small group of young people use cannabis more regularly, and 3–4% of secondary school pupils reported in 2019 that they had used drugs in the past 30 days or more than 20 times. As with criminality, there has been polarisation between an increasing proportion of young people who do not have alcohol or drug problems and a small group with risky or problematic use, some of whom come into contact with the healthcare system. This study investigates the relationship between continued problems with criminality and drug use among young people who have received outpatient treatment for substance abuse problems and how various risk factors can influence the outcome. The terms drug use and substance use also refer to alcohol, but not tobacco.
The Connection between Criminality and Substance Use
A substantial percentage of youth crime is related to substance use (Egnell et al. 2019; Pedersen & Skardhamar 2010) and there is a well-known and strong correlation between these sets of problems (Chassin 2008; D’Amico, Edelen, Miles, & Morral, 2008; Tripodi & Bender 2011). A large percentage of young people who begin treatment for problematic drug use have committed crimes (Dennis et al. 2004; Kinlock, Battjes, & Gordon, 2004; Mitchell, Kutin, Daley, Best, & Bruun, 2016). Conversely, justice-involved youth often have a substance use disorder (Dembo, Wareham, & Schmeidler, 2007; Hammersley, Marsland, & Reid, 2003).
The connection between criminality and drug use is obvious by virtue of the fact that drug use is illegal in many countries, but the relationship can be complex and manifested in various ways. As well, it is often difficult to determine which of the two problems came first (Bennett & Holloway 2005; Mulvey 2010). The connection may also manifest in different ways in different phases of the course of a substance use problem. Crimes and drugs are rarely related to each other in occasional or experimental drug users, while long-term drug use promotes criminality (Bennett & Holloway 2005; Simpson 2003). The linking between cannabis use and crime mainly constitutes drug-related criminality (Green, Doherty, Stuart, & Ensminger, 2010) and is weaker for offences such as assault and theft (Pedersen & Skardhamar 2010). The connection with non-drug-related crime, however, becomes stronger in relation to more serious cannabis use (Grigorenko, Edwards, & Chapman, 2015) or use of drugs such as amphetamines and opiates (Ford 2005; Kinlock, Battjes, & Gordon, 2004). The connection between drunkenness and violent crime is clearer (Brunelle, Tremblay, Blanchette-Martin, Gendron, & Tessier, 2013). Many young people cease offending when they become adults, but lingering high drug use can delay this development (Mulvey 2010; Sullivan & Hamilton 2007).
The crimes with the highest incidences among drug users are drug offences, shoplifting and theft (Bennett & Holloway 2005). An American study showed that 83% of the included young people had committed offences apart from drug possession or drug use (Dennis et al. 2004). The types of offences were distributed as follows: property crimes (e.g. vandalism, forgery, shoplifting, theft, robbery and auto theft) 55%, crimes against persons (e.g. assault, rape, murder and arson) 45% and drug-related offences (e.g. driving under the influence of alcohol/drugs and manufacturing or dealing drugs) 65%. Boys and young men offend more often than do girls and young women (McAra & McVie 2010). This pattern also applies to young people receiving substance abuse treatment (Hsieh & Hollister 2004; Mitchell et al. 2016).
Drug use and crime are factors that limit individuals' ability to participate in society and may lead to social exclusion (EMCDDA 2003; March, Oviedo-Joekes, & Romero, 2006; Millar 2007). The concept of social exclusion includes various dimensions such as education, economy, housing, social relations, norms and values, but also societal interventions and legal sanctions that in themselves can be stigmatising. It is dynamic and cumulative, that is, deficiencies in one area can negatively affect other life domains and the exclusion process is increased by accumulating several problems (Kronauer 1998).
Risk Factors Linked to Crime and Drugs
Criminality and drug abuse share common risk factors (Fleming, Catalano, Haggerty, & Abbott, 2010; Hawkins 2006; Mulvey 2010). Longitudinal studies that follow young people from an early age to adulthood have identified several risk factors related to the community, family, school and peers as well as to the individuals, factors that in turn increase the probability of future criminality and substance use problems. Although the risk factors for criminality and drug use are similar for both genders, the genders may be affected by these risk factors in different ways (Herrera & Boxer 2019; Bright et al. 2017). Both criminality and drug use are higher in communities and neighbourhoods characterised by poverty, segregation and social exclusion (Casswell, Pledger, & Hooper, 2003; Stone, Becker, Huber, & Catalano, 2012). Young people from socioeconomically disadvantaged areas are also arrested by the police and charged with crimes to a much greater extent (McAra & McVie 2012; National Council for Crime Prevention 2018).
School failure is a particularly influential risk factor for the development of criminality and of alcohol and drug abuse, while a strong connection to school and good academic outcomes are related to reduced risk of these problems in young adulthood (Bäckman et al. 2014; Fleming et al. 2010; Gauffin, Vinnerljung, Fridell, Hesse, & Hjern, 2013, Gauffin, Vinnerljung, & Hjern, 2015; Merline, Jager, & Schulenberg, 2008). There is also strong evidence that a childhood rife with family conflict, criminality and/or substance abuse problems in parents or siblings often leads to criminality and drug use among young people (Cheng & Lo 2011; Stone et al. 2012). Young people with a history of physical or sexual abuse are also at higher risk of developing problems with both criminality and drugs (Brunelle et al. 2014; Nooner et al. 2012). Involvement with peers who have been convicted of offences and often use illegal drugs is one of the most significant factors for both problems (Aston, 2015; Hoeben, Meldrum, Walker, & Young, 2016). Non-participation in structured recreational activities with prosocial peers seem to increase the risk of later drug use (Stone et al. 2012). Individual factors such as poor self-control, thrill-seeking and externalising behaviours pose a risk for later criminality and drug abuse (Cleveland, Feinberg, Bontempo, & Greenberg, 2008; Mulvey 2010). It is common for young people who have problems in one area to have difficulties in other areas as well. When several risk factors co-exist, a cumulative negative effect may arise (Spooner 1999). As in the case of drug use, an accumulation of various risk factors leads to increased risk of offending (Hawkins 1995, 2006; Hussong, Curran, Moffitt, Caspi, & Carrig 2004).
There is a lack of Swedish research into what characterises young people with alcohol and drug use problems who are convicted of crimes and into the outcomes of various treatment interventions in the target group (National Board of Health and Welfare, 2018). These risky behaviours have often been regarded as two separate problems that are studied in isolation (Carney & Myers 2012). Increasing knowledge and understanding of the relationship between the two problems and of their predictive factors is highly significant to the development and improvement of preventive interventions and treatment.
Aim
This article presents the results of a longitudinal/prospective study of criminality among young people with substance use problems who undergo outpatient treatment. The aim is to analyse indications of continued problems with criminality and drug use, and how various risk factors predict outcomes 1 year after initiated treatment contact at outpatient clinics. The analysis includes whether individual risk factors or combinations of these affect the outcome for the target group in question.
Methods
This study was carried out within the framework of the research project Treatment Research on Adolescents at the Maria clinics (TRAM). The central aim is to study young peoples’ change trajectories with regard to alcohol and drug use, mental health and social situation, and how specific risk and protective factors affect outcomes for various groups after outpatient treatment. The study has been ethically approved (Ref. no. 2015/160-31). The project combines data from structured interviews with young people at intake and data from various registers at follow-up 1 year after baseline. Similar strategies have been successfully used in several Swedish studies to follow-up children and adolescents placed in various forms of institutional care or sentenced to custodial care or imprisonment (e.g. Franzén et al. 2008; Gauffin et al. 2013; 2015; Shannon 2011; Vinnerljung & Sallnäs 2008).
Participants
Initial data collection was carried out at Maria clinics in 12 cities: Stockholm, Gothenburg, Malmö, Linköping, Helsingborg, Norrköping, Eskilstuna, Södertälje, Kristianstad, Solna, Hässleholm and Sundbyberg. These clinics are specialised outpatient units for substance-using adolescents and are operated in cooperation with social services and the healthcare system. All clinics offer various forms of individualised and/or manual-based treatment of alcohol and drug use problems. The average treatment length is 4–6 months.
All young people aged 15 years and above who initiated contact with the Maria clinics in 2016 were invited to participate in the study; 932 individuals were informed and asked about participation in the study by the therapist in question and 469 chose to participate. No register data were available for 12 individuals due to incomplete civic registration numbers or migration out of Sweden, and two individuals died during the follow-up period. Thus, a total of 455 young people participated in the follow-up study reported here.
Non-Participation
A non-response analysis shows that the study group (455 individuals) had somewhat more serious substance use problems than did the group (477 individuals) opting not to participate in the study. The study group consisted of 29% girls and 23%, while the percentage of girls in the non-response group was 22%. The proportion of young people with a foreign background is 23% in the study group and 34% in the non-response group. The median age was 17 years in both groups. In the study group, 68% of the young people were from an outpatient unit in a large city (Stockholm, Gothenburg and Malmö), and in terms of initiators of care contact, 50% state their own/the network. For the non-participation group, the corresponding data are 66% and 45%. The proportion of young people convicted of crimes was slightly higher in the study group (33%) than the non-participation group (28%). Regarding primary drug, both groups reported a similar pattern: percentages reported in the study group were 76% for cannabis, 14% alcohol and 10% other drugs, while the figures in the non-response group were 79% for cannabis, 13% alcohol and 8% other drugs (i.e. opiates, amphetamine and cocaine). There were significant differences in other variables related to drug use, and the study group generally had more serious substance use problems than did the non-response group in terms of higher frequency of substance use (51% vs. 41%), greater extent of mixed substance use (38% vs. 26%) and a larger proportion with previous treatment for substance use problems (31% vs. 20%). This result differs from earlier follow-up studies in which, in contrast, groups that opted not to participate often had more serious problems (Meyers, Webb, Frantz, & Randall, 2003).
Measures and Outcomes
When the treatment process began, initial data collection began via intake interviews. UngDOK is a semi-structured interview method developed specifically for young people with various forms of alcohol and drug problems. The primary purpose of the interview is to identify problems, needs and the current situation to enable relevant assessment, and the planning and delivery of treatment. The interview contains a total of 75 questions covering the following 10 life domains: housing and financial support, occupation, treatment history, criminality, childhood, exposure to violence, family and relationships, physical health, mental health, as well as alcohol and drug use. Each domain ends with some open-ended questions. The interview also covers administrative data, sociodemographic data, information concerning ongoing treatment contacts and some concluding open-ended questions. The UngDOK interview method has satisfactory reliability and validity (Dahlberg et al. 2017).
The outcome measures were based on experience gained in earlier studies and provided a multifaceted and reliable picture of the young peoples’ progress (see, e.g. Vinnerljung & Sallnäs 2008). Data indicating continued problems with criminality refer to offences processed in 2017 and were found in the processed offences register kept by the Swedish National Council for Crime Prevention. Individual offences have been categorised based on information taken from the register. The outcome used as an indicator of continued substance use problems was one of the following: a new contact with a Maria clinic, other substance use treatment in outpatient care, substance use treatment in inpatient care, medication for substance use disorder, compulsory substance treatment or drug-related criminality. Data were taken from several national registers: National Board of Health and Welfare’s Patient Register, National Board of Health and Welfare’s Pharmaceutical Register, National Board of Health and Welfare’s Compulsory Care Register and the processed offences register kept by the Swedish National Council for Crime Prevention.
Analysis
The first analyses covered descriptive data and bivariate associations between risk factors and the indication of continued problems with criminality. Next, logistic regressions were used to describe the predictive value of the risk factors. This was done with and without controlling for gender, age, prior drug use frequency (of the primary drug) and place of residence. In addition, separate analyses were conducted to investigate the impact of the cumulative risk load. We examined risk factors that might discriminate between individuals engaging in drug-related criminality and individuals committing other types of crimes. When treating the 10 risk factors as a composite index, the internal consistency was .60. In addition to more traditional statistical analyses, we also conducted a configural frequency analysis (von Eye et al. 1996), which seeks specific patterns or configurations that occur more frequently than expected by chance (“types”) or less frequently than expected by chance (“antitypes”). To reduce the risk of spurious significances due to multiple tests, the p-level was adjusted with Bonferroni correction.
Results
Criminality and drug use at intake and 1-year follow-up. Data stated as percentages. Gender differences tested with chi2 test (ns = not significant).
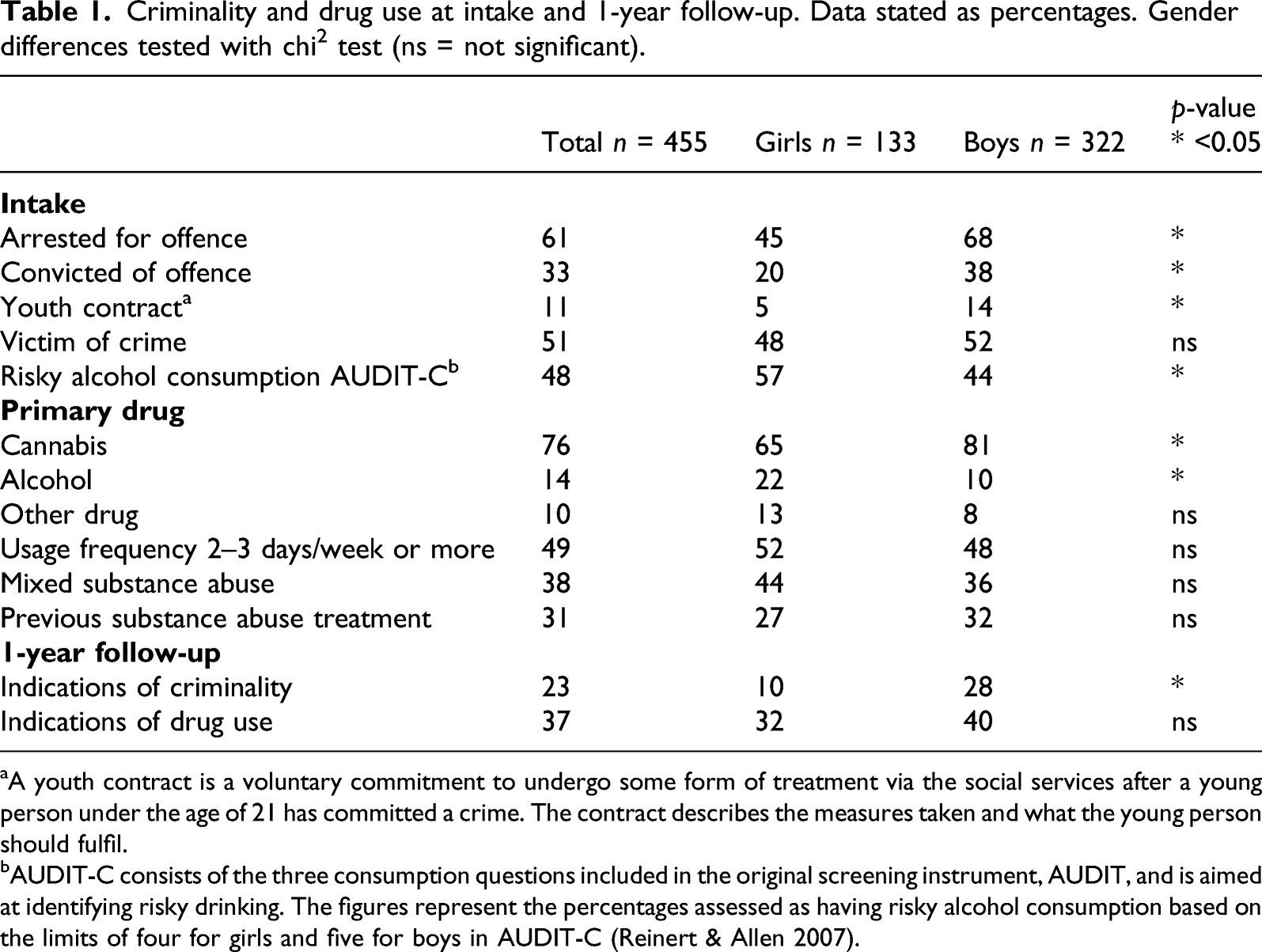
aA youth contract is a voluntary commitment to undergo some form of treatment via the social services after a young person under the age of 21 has committed a crime. The contract describes the measures taken and what the young person should fulfil.
bAUDIT-C consists of the three consumption questions included in the original screening instrument, AUDIT, and is aimed at identifying risky drinking. The figures represent the percentages assessed as having risky alcohol consumption based on the limits of four for girls and five for boys in AUDIT-C (Reinert & Allen 2007).
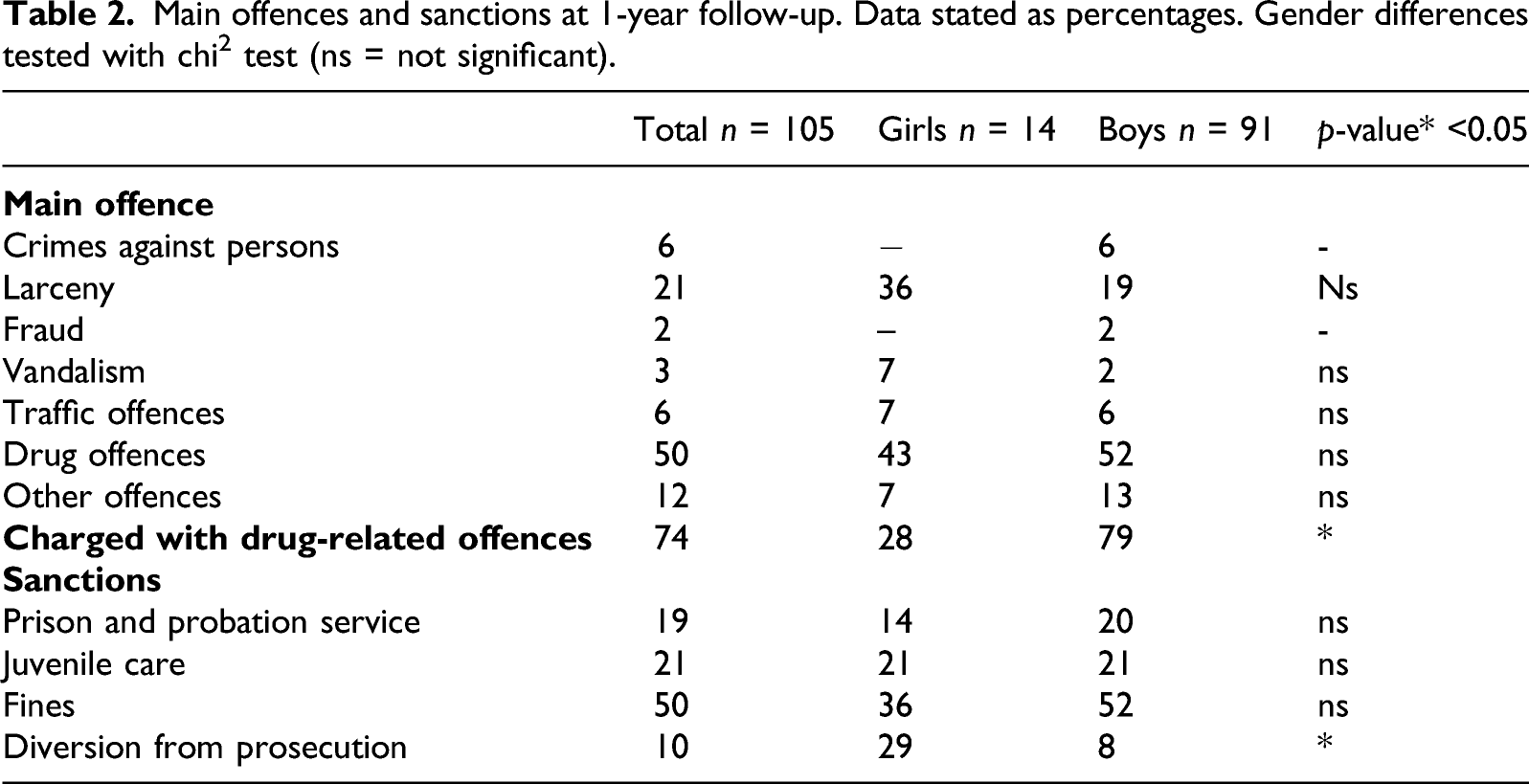
Main offences and sanctions at 1-year follow-up. Data stated as percentages. Gender differences tested with chi2 test (ns = not significant).
Odds ratios and confidence intervals for the association between juvenile risk factors and continued criminality at the 1-year follow-up (N = 455).
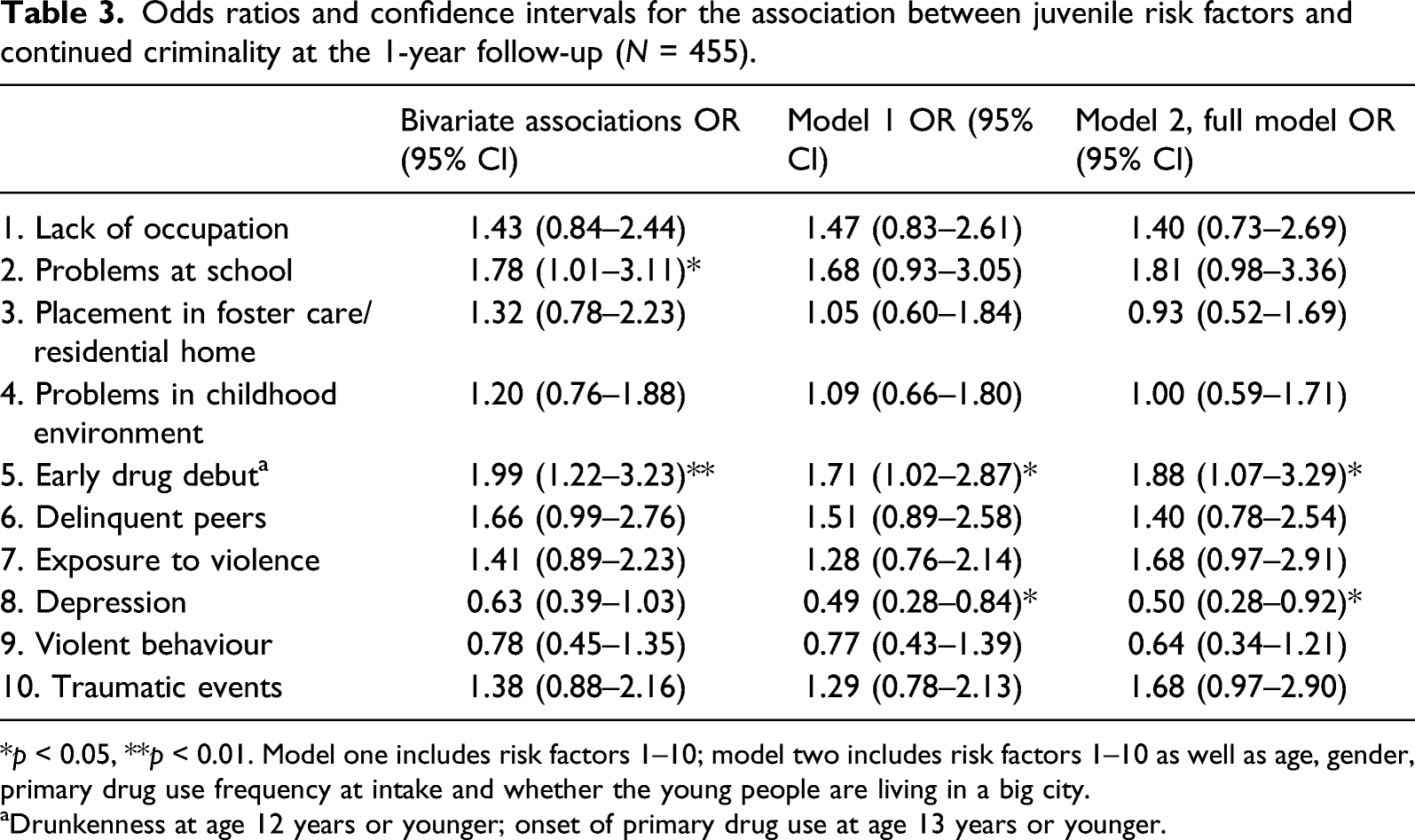
*p < 0.05, **p < 0.01. Model one includes risk factors 1–10; model two includes risk factors 1–10 as well as age, gender, primary drug use frequency at intake and whether the young people are living in a big city.
aDrunkenness at age 12 years or younger; onset of primary drug use at age 13 years or younger.
Cumulative risk load and the risk of continued criminality at the 1-year follow-up (N = 455).
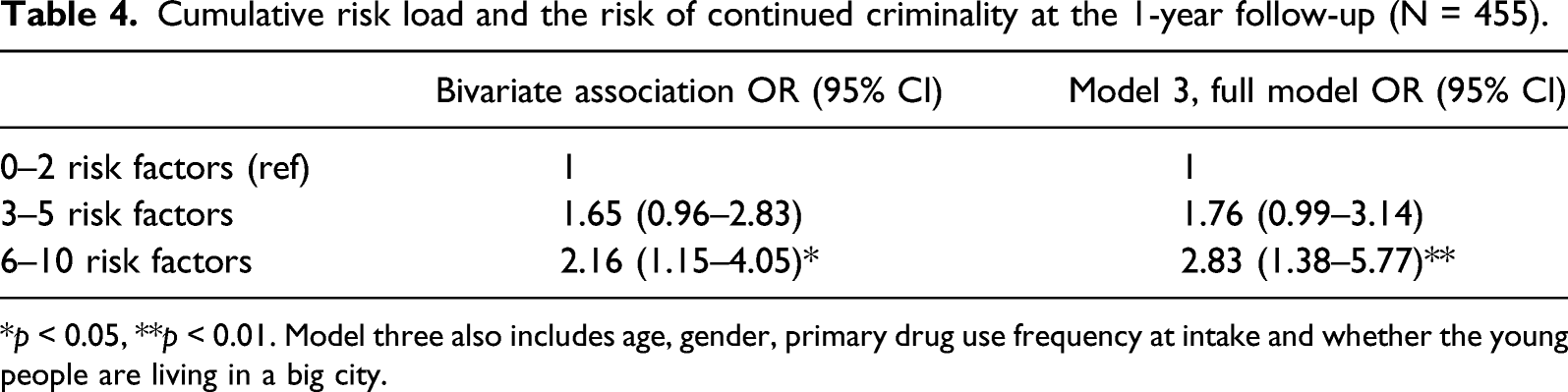
*p < 0.05, **p < 0.01. Model three also includes age, gender, primary drug use frequency at intake and whether the young people are living in a big city.
Patterns of gender, early drug debut, depression and criminality.
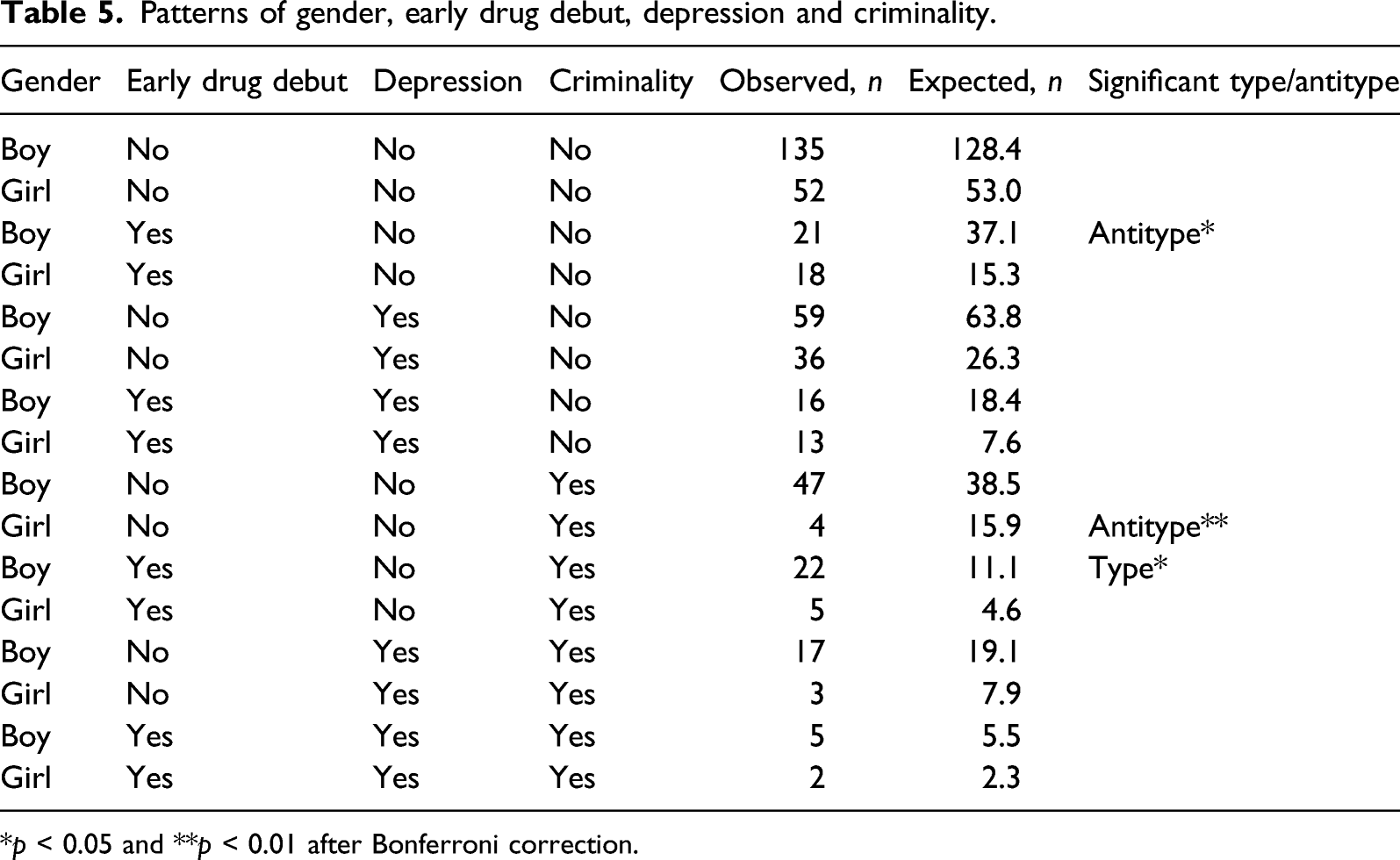
*p < 0.05 and **p < 0.01 after Bonferroni correction.
Discussion
The results show that six out of 10 of the young people who began outpatient treatment for substance use problems at a Maria clinic had been arrested by the police and that one-third had previous criminal convictions. These results are consistent with those of several earlier studies showing that a large percentage of young people who begin treatment for alcohol and drug use problems have criminal records (Dennis et al. 2004; Mitchell et al. 2016).
At 1-year follow-up, just under one-quarter of young people had been charged with offences committed during the relevant period, while 37% had displayed continued problems with drug use. There is, however, considerable overlap, as most (84%) of the young people who had been convicted of crimes showed indications of continued problems with alcohol or drugs. Drug offences of various kinds appear frequently among the charges, and three-quarters of those charged had been convicted of such an offence at some time during the period, sometimes on multiple occasions. Drug offences were also the most frequent main offence. These results are not particularly surprising, considering that all drug use in Sweden is criminalised. Sweden has by far the highest number of drug offences per capita in the Nordic countries, and nine out of 10 of these offences refer to the consumption or possession of drugs (Egnell et al. 2019).
Just over three-quarters of the young people had not been convicted of offending. This result should be interpreted with some caution, as the relevant registers do not pick up the young people who have ‘gone under the radar’ and may be continuing to offend and use drugs without any involvement with the justice or healthcare systems. The problems of criminality and substance use are two sides of the same coin. As a result, the treatment interventions aimed at young people could affect a reduction of both drug use and criminality. Another possible hypothesis is that the study group is heterogeneous, and for many young people, drug use and criminality represent facets of an experimental and transitory period in their lives (von Sydow et al. 2001). Many young people stop offending and using drugs in the transition to adulthood as a consequence of a natural process of maturation in which age and social factors such as education, occupation, having a driving licence and a home of their own and other adult commitments become more significant (Mulvey 2010).
This study also shows that girls are arrested for and convicted of offences to a significantly lesser extent than are boys, both when treatment is initiated and at 1-year follow-up. A corresponding gender difference also applies to continued alcohol and drug use, although this difference is not significant. Significant gender differences as regards criminality in youth with substance use problems have also been reported in several earlier studies (Grella & Joshi 2003; Shane et al. 2006).
The incidence and ranking of main offences is largely aligned with the results of other studies (Bennett & Holloway 2005; Green et al. 2010; National Council for Crime Prevention 2019). Narcotics offences are followed first by larceny, then by crimes against persons and traffic offences. Overall, it was only a small group of young people in this study who committed serious crimes, compared with the results of studies from, for example, the USA (Dennis et al. 2004). Of the group that had been charged and convicted, half were sentenced to fines, one-fifth to probation or imprisonment and one-fifth to juvenile care, while diversion from prosecution was the sanction in one-tenth of cases. Contacts with the police, the correctional service or with institutions such as special youth homes and prisons can also create an institutional exclusion (Kronauer 1998). Girls were sanctioned with diversion from prosecution to a significantly greater extent than were boys. Studies have shown that young people who are warned or charged but have no further contact with the justice system have better outcomes than do those upon whom penal sanctions are imposed (McAra & McVie 2010). Imposing a high fine for a minor drug offence can have huge adverse consequences for a young person, for example, in the form of debt when they are often already in a socially disadvantaged situation as well as by inclusion in the register of persons charged with an offence. An increasing number of employers in Sweden are demanding extracts from the criminal record, which in turn can lead to increased stigmatisation and reduced opportunities to get a job in the future. It provides another ground for an exclusion from the labour market and in the long run also an economic exclusion. Instead, diversion from prosecution attached to a ‘youth contract’ may be a more effective sanction (Lindquist-Grantz et al. 2021). A small percentage is offered this alternative, but it is reasonable to assume that more young people with substance use problems could be offered this intervention.
The results indicate that only a few of the 10 risk factors studied predict continued problems with criminality. Early drug use debut seems to be significantly related to continued criminality and is a well-known risk factor in the negative progression towards a problematic future life situation (Anthony & Petronis, 1995; King & Chassin 2007). This result also indicates that many of the studied young people had lived in an at-risk environment in which both drugs and criminality were prevalent (Rhodes et al. 2003). That depression in boys could be a protective factor against continued criminality is evident in this study and likely means that a reported history of depression may indicate a lesser extent of externalised behaviour.
Another important result is that it is the accumulation of risk factors that is linked to a negative outcome. If an adolescent has more than five risk factors, there is consequently a significantly elevated risk of continued problems with criminality. This cumulative effect is highly consistent with the conclusions of earlier studies of the relevant target group (Anderberg & Dahlberg 2018; Hawkins et al. 1992; Ostaszewski & Zimmerman 2006). There may be both methodological and actual causes behind the fact that multiple risk indicators are more predictive of continued problems with criminality than isolated risk factors. One can expect higher reliability in data where there are many indicators of problem load, but it is also reasonable to expect that change and abstinence may be achievable even if there are problems in individual life domains, while it may be insurmountable if the problems span multiple life domains. The cumulative problem weight can also be a challenge for the outpatient clinics that meet the target group in question.
The exploratory configural frequency analysis provides some guidance related to the risk factors and combinations of risk factors that could increase or decrease the risk for continued problems with criminality. The analysis shows that the combination of three factors occurred as typical for displaying criminality: being a boy, having an early debut and having no depression. This result is also consistent with results from other analyses performed.
Limitations
There is likely some under-reporting of the extent of criminality in connection with intake at the Maria clinics since charges, diversion from prosecution and fines are not specifically recorded at that time. At follow-up, some young people may have continued to offend without having been arrested or charged. At the same time, the non-response analysis shows that the study sample generally had more serious psychosocial problems than did the non-participant group. Another limitation of the study is that the results are not immediately generalisable to young people with substance use problems engaged in other types of treatment, such as compulsory care or inpatient treatment. However, a strength of the study is that the included young people represent several outpatient clinics in various Swedish cities, which contributes to reasonably high generalisability concerning criminality among young people involved in this form of care. Combining information from structured interviews at baseline and national registers at follow-up yielded reliable data and could be an innovative method for dealing with the problem of non-response, which is common in traditional follow-up studies (Garner et al. 2007).
Implications
The significance of the cumulative effect illustrates the importance of taking an initial history of criminality in connection with the treatment of drug use problems. Particular attention should be paid to young people with more serious problems, including coordinated interventions to support more positive development, if possible. Five risk factors seem to constitute a key threshold, although isolated risk factors can still be very important to consider in the treatment context regarding some individuals. Young people with co-existing problems with drug use and criminality should be provided integrated or parallel treatment for a more optimal outcome (Stein et al. 2013; Tripodi & Bender 2011). As criminality and drug use are so closely linked, interventions that focus on one of these problems in a high-risk population may also contribute to reducing the other problem (cf. D’Amico et al. 2008; Dembo et al. 2007). Early and justifiable interventions have also been shown to have good effects on both criminality and drug use (Carney & Myers 2012).
Swedish youth policy needs to be based to a greater extent on a holistic perspective and on interventions meeting the needs of young people, moving away from the current emphasis on penal law principles. Courts also need to more fully live up to the principles of the UN Convention on the Rights of the Child, based on the best interests of children and youth. Young people should be kept out of the legal system to the greatest possible extent, as there is risk that early prosecution of young people in the risk zone will stigmatise them and create a self-fulfilling prophecy (McAra & McVie 2010). It should be reasonable for a larger percentage of young people, including those over the age of 18 years, to be covered by some form of penal warning attached to a ‘youth contract’. This would allow more young people to be offered adequate interventions that can prevent social exclusion and counteract continued problems with both criminality and drugs.
Overall, research shows that there is support for a preventive youth justice policy such as early interventions, prevention of school failure, mediation, diversion from prosecution and avoidance of detention (Scottish Government 2015). The school system should offer children and young people the educational and social support they need to succeed in school and thus avoid social exclusion in the longer term (Bäckman et al. 2014; Christle et al. 2005; Hammersley et al. 2003). These policy changes would be important in Sweden as an alternative to a development towards a more populist and repressive legal system where children and young people are treated in the same way as adults.
Outpatient care is the most common form of care for young people with alcohol and drug problems in Sweden and elsewhere in the world, so more knowledge of and continued research into this particular form of care is necessary.
Conclusion
This is the first Swedish study in which young people with substance use problems in outpatient care have been studied to any great extent. This study indicates that about one-quarters of the young people who begin outpatient treatment at Maria clinics have been convicted of crimes at 1-year follow-up. Most of them who had been convicted with offences also have ongoing problems with drug use and three-quarters of the young people had been charged with a drug-related offence. High fines for minor drug offences and registrations in the criminal record can also have negative consequences for a young person and contribute to social exclusion.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This was financial supported by Systembolaget alcohol research council and Folkhälsomyndigheten.