
Abstract
Social constructivists have significantly advanced our understanding of how digital technologies give rise to different forms of organizing between organizations but less is known about similar dynamics within the organizations. Therefore, we investigated the implementation of telehealth within an academic health center during the COVID-19 pandemic. We developed a grounded model of the integration of work with technology based on 54 interviews with 27 healthcare professionals. The model comprises two moments. During the moment of enactment, four connected themes—material affordances, material constraints, embodiment, and relationality—emerged. In the subsequent moment of variation, two themes—stabilization and closure—determined the bifurcation into technology-adjacent and technology-distant organizing. Technology-adjacent organizing involves a telemedicine team continuing to treat patients with serious mental illness admitted to remote state hospitals. Technology-distant organizing entails the redeployment of telehealth in the focal psychiatric hospital for future disasters. The model contributes to scholarship at the intersection of institutional theory and information studies.
Introduction
Digital transformations that continue to reshape the nature of work and forms of organizing cannot be fully understood without considering organizational contexts (Barley & Orlikowski, 2023; Orlikowski & Barley, 2001). Social constructivists contend that people respond to new technologies, as well as to each another, through their actions. Their empirical work has demonstrated how and why identical technologies yield divergent outcomes across multiple organizations (Leonardi & Barley, 2008). This logic underpins our shift to a lower level of analysis, examining how and why identical technology produces different outcomes within a single organization.
Orlikowski and Scott (2021) recently advocated for a “strong sociomateriality” approach to identify and account for spatially and temporally displaced digital relations and dynamics. Telehealth, which entails the use of telecommunications for delivering health services remotely, exemplifies these spatial and temporal displacements. Although sociomateriality and social constructivism both fall under voluntarism—which posits that humans have agency and the ability to shape their environments to achieve their goals—sociomaterialists have critiqued constructivist studies of technology implementation (Leonardi & Barley, 2010). The sociomaterial perspective asserts that “materiality is integral to organizing, positing that the social and the material are constitutively entangled in everyday life” (Orlikowski, 2007, p. 1437). Given the complexity of technology implementation in professional settings, we propose a walk back from strong sociomateriality, or even sociomateriality, toward social constructivism.
Artifacts, namely hardware or software with material properties, can strengthen the core production system of organizations when they are implemented, but they can also introduce unique risks and complications to users. This duality may be observed in psychiatric hospitals, considered as total institutions (Goffman, 1961) or high-reliability organizations (Perrow, 1984). Multiple digital technologies coexist with practitioners in these healthcare organizations, particularly as technologies that augment practitioners’ work are layered onto assistive ones (Shen et al., 2024). Thus, the sociomaterial fabric is already constitutively disentangled during technology implementation. We suspect it could be further untangled during disasters like the COVID-19 pandemic, when practitioners are prompted to reinterpret and renegotiate the use of technologies.
The purpose of this article is to assess how and why an identical technology could trigger different dynamics and outcomes within an organization. In this study, we consider the user (healthcare provider) and the artifact (telehealth) as they work to accomplish a task (treatment of patients with serious mental illness [SMI]) within an organization (academic health center) embedded in an institutional environment (Texas, United States), all while responding to an external event (the COVID-19 pandemic). We interviewed healthcare providers to gauge their perceptions of and clinical practices with telehealth. We find that this shaped two distinct forms of organizing: technology-adjacent organizing and technology-distant organizing. Technology-adjacent organizing involves a telemedicine team continuing to use telehealth as part of a hybrid model, combining it with in-person visits to treat patients admitted to state hospitals in rural areas. Technology-distant organizing entails repurposing telehealth for deployment in future disaster scenarios. The heterogeneous forms of organizing, or organizing forms, that emerge from technology adoption have implications for institutionalized ways of working.
Theoretical Background
Management scholarship, from scientific management discourses (Taylor, 1911) to contemporary discourses on the future of work (Malhotra, 2021) and the future of organizing work (Beane & Leonardi, 2022), has explored how the outcomes of technology implementation within organizations are socially constructed. Management literature on this topic is vast yet dispersed, and organizational theory stands to evolve alongside technology (Grodal et al., 2023). In this section, we establish the effects of digitalization on both work and organizing.
Technology and Work
Practitioners use an array of digital technologies to perform their work. These entities—humans and technology—merit separate yet interrelated considerations. First, a new technology does not always replace older ones. Telehealth represents the culmination of key inventions from each industrial revolution: mechanization from the first; telecommunications, such as the telegraph and telephone, capitalizing on electricity in the second; computers and the internet from the third; and digitalization in Industry 4.0. It therefore exhibits “interpretive flexibility”—that is, the capacity of a technology to sustain heterogeneous opinions among practitioners (Pinch & Bijker, 1984). Implementing telehealth as a new technology does not necessarily mark a complete departure from previous ways of working.
Second, multiple technologies coexist in professional settings. Murray et al. (2021) examined the joint capacity of humans and technology to exercise intentionality over two work tasks: protocol development and action selection. The main forms of conjoined agency are assistive (i.e., technology does not develop protocols or select action), augmentative (i.e., technology develops protocols but does not select actions), and autonomous (i.e., technology makes decisions and executes actions) technologies. Telehealth closely resembles assistive technology, serving as an adjunct to the healthcare providers. It can transform the practitioner's work in terms of workspace and time, work relationships, work content, and task allocation (Alfes et al., 2022).
Finally, practitioners mediate the diffusion of technological innovations. The extent of a given technology's impact on organizations is moderated by human agency (Orlikowski, 1992), particularly as the reception of new digital technologies may differ across professions in large organizations like hospitals (Abbott, 1989; Ferlie et al., 2005). Reflecting on the ethical dilemmas psychiatrists face when using electroconvulsive therapy to alter patients’ minds for societal integration, Simon (1969) wrote: “Developments in technology give professionals the power to produce larger and broader effects at the same time that they become more clearly aware of the remote consequences of their prescriptions” (p. 150). This awareness is echoed by a practitioner in discussing telemedicine: You don't start with a technology that you’re set on using and expect people to change their workflow. You don't buy expensive hardware and then make everyone on your team learn to use it. You start with empathy for the people you're serving—and build your solution from there. (Kerr, 2016)
Technology and Organizing
Organizational knowledge can be gained by examining practices and relationships, not just individuals and their actions, a point Nicolini (2006) emphasized based on his seminal three-year research project on telemedicine in Northern Italy. However, organizational theorists continue to struggle to explain the new forms for organizing introduced by technological advancements. A form of organizing is broadly defined as a specific set of solutions to four universal problems that any organization must address in order to exist: information flows, reward distribution, task allocation, and task division (Puranam et al., 2014). The novelty of an organizing form comes from its enhanced effectiveness in addressing these four universal problems compared to existing forms. The challenge lies in analytically characterizing the epistemological and ontological nature of such sociomaterial practices (Leonardi & Barley, 2008).
Technological breakthroughs can punctuate entire industries down to the inner workings of an organization. Waves of digitalization generate tensions across industries, leading organizations and key stakeholders to question whether modifications to industry rules, norms, and values are necessary (Seidel & Berente, 2013). Orlikowski and Scott (2021) focused on a particular causal pathway leading to “institutional displacement” based on examples from the book publishing and hospitality industries. Institutional apparatuses, defined as “established industry-wide structuring mechanisms (e.g., rules, standards, protocols, norms, values, and measures) that coordinate and regulate the performance of activities, flows, and relations across an industry or sector” (Orlikowski & Scott, 2021, p. 7), are displaced when they no longer correspond to—and thus generate existential tensions with—new digitalized phenomena. However, they do not elaborate on an equally plausible pathway in which tensions are addressed, resulting in “institutional reinforcement.” We have reason to believe both causal pathways operate within organizations of the healthcare industry. In healthcare, autonomous technologies remain rare in practice, while augmentative technologies, such as the use of artificial intelligence in prior authorization, are often layered onto assistive ones like telehealth (Shen et al., 2024). These technologies, individually or in combination, can enhance or alter the competencies of individuals within a profession (Beane, 2019) and firms within an industry (Tushman & Anderson, 1986).
Emerging technologies are driving a diversification of organizing forms. The coconstitution of technology and organizing can be better understood from a relational perspective (Bailey et al., 2022) or through Faraj and Pachidi's (2021) “regime of organizing,” defined as “sociomaterial arrangements of practices, rules, norms, framings, and material infrastructures that provide distinct affordances for organizing and shape decision making, control, and coordination in organizing” (p. 8). This concept closely resembles Orlikowski and Scott's concept of digital undertow, as discussed in the last paragraph. It also leaves open multifarious organizing regimes within an organization while acknowledging institutional apparatuses within the industry.
Constructivists who study technology implementation hold that organizational change emerges from an ongoing stream of social action in which people respond to a technology's constraints and affordances, as well as to each other (Leonardi & Barley, 2008). They have asked how and why identical technologies can trigger different dynamics and outcomes between organizations and have demonstrated how new computer-based technologies are implemented in established organizational contexts (Barley, 1986; Leonardi & Barley, 2010). A gap in theorizing was evident, with only 2.8% of the research published in four leading journals focused on the relationship between technological function and organizational form across contexts (Zammuto et al., 2007). In this study, we instead ask how and why an identical technology could trigger different dynamics and outcomes within an organization. A gap in contemporary theorizing underscores our examination of how a technological advancement shapes organizing forms within a context. Through interviews with healthcare providers, we examine the material and social dimensions of organizing work with telehealth in a psychiatric hospital during the COVID-19 pandemic. The resulting model contributes to the literature at the intersection of institutional theory and information systems, exploring how changes in technology, forms of organizing, and future of work are linked within institutional contexts (Barley & Orlikowski, 2023; Currie, 2009; Jarvis et al., 2022; Mignerat & Rivard, 2009; Orlikowski & Barley, 2001).
Methods
Case
The University of Texas Health Science Center at Houston (UTHealth Houston) was theoretically sampled as an extreme case (Eisenhardt, 1989; Yin, 2003). UTHealth Houston is an academic health center with a mission focused on education, research, clinical care, and public health. It includes seven schools, including the McGovern Medical School, and the UTHealth Houston Harris County Psychiatric Center (HCPC), a teaching hospital. All HCPC staff are employed by UTHealth Houston, and its psychiatrists and psychologists are also on the McGovern Medical School faculty.
Telehealth services were provided separately by two entities within UTHealth Houston: on-site at HCPC and remotely by a telemedicine team to the North Texas State Hospital. HCPC is a 274-bed, free-standing psychiatric hospital located in Houston, Texas. It is the largest provider of inpatient psychiatric services in the city, with approximately 8,000 admissions of adults, adolescents, and children annually. During the first wave of the COVID-19 pandemic, HCPC providers used Zoom for telehealth between March 23, 2020 and May 15, 2020. In Harris County during this period, the first Declaration of Local Disaster for Public Health Emergency was issued on March 11, 2020, the Stay Home, Work Safe Order was enacted on March 24, 2020, and the Order Use of Face Coverings was issued on April 22, 2020 (Harris County Commissioners Court Agenda, n.d.). These orders were subsequently extended seven times and amended four times each.
The telemedicine team is employed by the McGovern Medical School's Louis A. Faillace, MD, Department of Psychiatry and Behavioral Sciences. Even before the pandemic, the telemedicine team had a contract with the Texas Health and Human Services Commission to provide adult psychiatric services—primarily competency restoration—to patients of state hospitals operated by the Texas Health and Human Service Commission through telehealth. This contract also required team members to visit the hospital monthly.
Context
Five contextual factors deserve highlight. Along with state hospitals in Texas, HCPC provides treatment to people with SMI, defined as “a mental, behavioral, or emotional disorder resulting in serious functional impairment, which substantially interferes with or limits one or more major life activities” (NIMH, 2022). The prevalence of SMI among adults aged 18 and older in Texas between 2019 and 2020 was estimated at 4.8% or about 1,020,000 people (SAMHSA, 2022). HCPC and state hospitals are often the last resort for those with SMI who are unable to receive treatment within their communities or who pose danger to themselves or to others. Figure 1 shows the locations of HCPC and the 10 state hospitals in relation to mental health professional shortage areas and the prevalence of SMI in Texas's adult population.
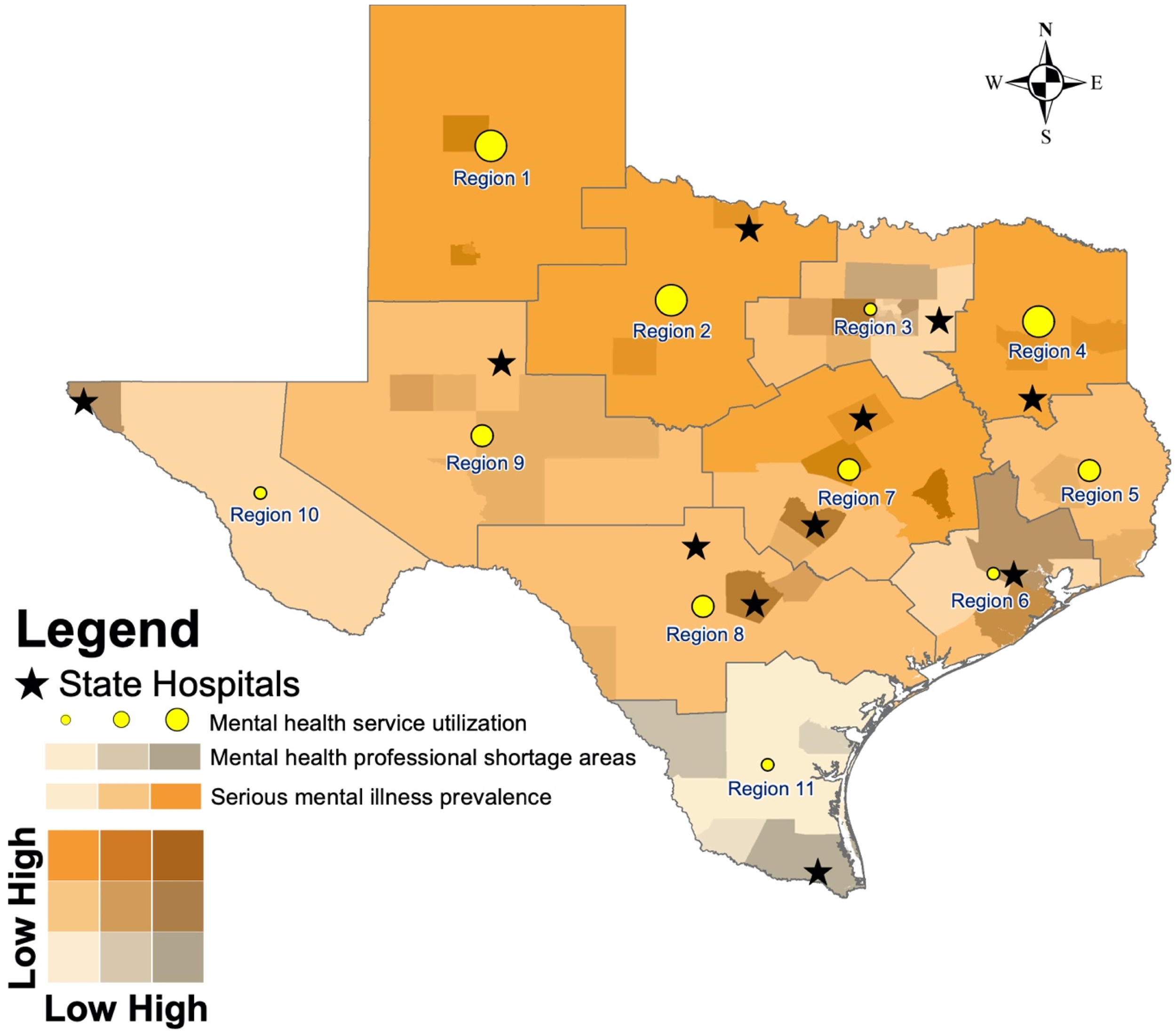
Need, demand, and supply of mental health care in Texas.
Houston is an area of recurring risk for natural disasters. The city has experienced seven federally declared disasters since 2015, including the coronavirus pandemic (Understanding Houston, n.d.). A leading disaster preparation strategy for hospitals during weather events like Hurricane Harvey—a Category 4 hurricane that struck Texas and Louisiana in 2017, causing $125 billion in damages (Blake & Zelinsky, 2018)—is the “ride-out” provision. The strategy ensures continuous operation during a critical event (Texas Hospital Association, n.d.; UTHealth Houston, n.d.). Ride-out teams, composed of medical professionals, support staff, and sometimes administrative and facility maintenance personnel, stay on the hospital site for extended periods of time to care for patients. However, the stress of working consecutive days poses a concern for ride-out team members (McRaven, 2017). Telehealth became a ubiquitous alternative strategy during the COVID-19 pandemic.
Telehealth became a prominent mode of healthcare delivery during the COVID-19 pandemic in the United States as in other countries (Gunja et al., 2023). Emergency orders and legislation temporarily amended laws, reimbursement policies, and licensure regulations (Hogg Foundation for Mental Health, 2023; Weigel et al., 2020). While some of these amendments were extended beyond the COVID-19 pandemic or made permanent at the state and federal level, others were not (Center for Connected Health Policy, n.d.-a; Center for Connected Health Policy, n.d.-b). The pandemic nonetheless led to a precipitous increase in telehealth visits for patients with SMI compared to those without (Miu et al., 2023). Behavioral health specialists had the highest utilization of telehealth for patient visits compared to other specialists during the pandemic (Samson et al. 2021). However, telehealth adoption varied significantly by physician and practice characteristics across the country (Yu et al., 2024). Providers feel ambivalent about telehealth (Doran & Lawson, 2021). They have voiced concerns about its integration into routine clinical practice (Schoebel et al., 2021; Torous & Wykes, 2020).
Even before the COVID-19 pandemic, mental healthcare needs were often unmet in rural areas across the United States. This issue persists partly because of a chronic workforce shortage, with mental health professionals concentrated in urban areas. Approximately 97% of counties in Texas are designated as mental health professional shortage areas (Texas DSHS, 2004). The nine mental health facilities and one residential treatment facility for adolescents, collectively referred to as state hospitals and overseen by the Texas Health and Human Services Commission, face persistent staffing shortages (Simpson, 2023). Rural residents often travel long distances to access services (Lam et al., 2018). Telehealth holds promise in bridging the rural–urban divide in access to care (Stamm, 2003).
Healthcare providers nationwide still face workplace violence. In the United States, 73% of all nonfatal workplace injuries and illnesses resulting in days away from work occurred within the healthcare industry (BLS, 2018). Violence from patients toward providers is most common in psychiatric and substance use hospitals (BLS, 2018). Hospital-acquired infections attributed to COVID-19 placed an additional burden on providers (Weiner-Lastinger et al., 2022). Telehealth has the potential to mitigate the dangers of the profession.
Study Design and Participants
All interviewees were employees of UTHealth Houston. We purposefully sampled study participants from three social groups. The first group comprised the clinical and administrative staff of HCPC. The second group included medical residents who were training at HCPC during the study period. The third group consisted of members of the telemedicine team who served state hospitals.
One of the principal investigators introduced this qualitative study at the HCPC monthly staff meeting in August 2020 and again at the telepsychiatry team meeting in September 2020. Following these announcements, we sent 62 recruitment emails to individuals registered on these two groups’ distribution lists. Separate emails were sent to medical residents. We also relied on snowball sampling, specifically through word-of-mouth referrals. Of 35 prospective participants who were sent up to three invitation emails, 27 matriculated into the study. The characteristics of the sample are shown in Table 1.
Demographic Characteristics of Interviewees.
Note: We reported age, year during which interviewee obtained a medical license, and number of years employed at UTHealth as median (range). There are missing values for the year during which two interviewees obtained their medical licenses. UTHealth Houston : The University of Texas Health Science Center at Houston.
Participants in our study provided informed consent via Qualtrics (Qualtrics, Provo, CT) and indicated their preferred modality (WebEx or telephone) and recording option (yes or no) within the same survey. Each participant received a $150 Amazon gift card upon completion of the baseline interview and an additional $50 Amazon gift card upon completing the follow-up interview one month later. The UTHealth Houston Committee for the Protection of Human Subjects approved our research protocol (HSC-MS-20-1093) in October 2020.
Positionality Statement
Our research team consists of six members: a healthcare management researcher (“Principal Investigator 1”), a psychiatrist who is also part of the HCPC top management team (“Principal Investigator 2”), two research coordinators, a Master of Public Health student, and a PhD student. To address power dynamics during recruitment, only Principal Investigator 1 coordinated with the two research coordinators on participant recruitment. We acknowledge that these positionalities influenced data collection, so Principal Investigator 2 conducted interviews exclusively with members of the telepsychiatry team. Four other team members—Principal Investigator 1, the research coordinators, and the Master of Public Health student—conducted interviews with HCPC staff, telepsychiatry team members, and medical residents. We also acknowledge that these positionalities influenced data analysis, so we invited the PhD student to code the interview transcripts and help interpret the findings.
Data Collection
We conducted semistructured interviews from November 2020 to August 2021. More specifically, we interviewed each interviewee twice during this period: at baseline with an average duration of 45 min and at follow-up averaging 20 min. There was no loss to follow-up. Our data collection modes include audio and video for 20 participants, audio only for five participants, and no recording for two participants. We continued the interviews until we reached theoretical saturation, the point at which successive interviews ceased to generate new concepts (Patton, 2002).
Principal Investigator 1 worked with a human-centered design consultant to develop two interview guides—one for the baseline interview and another for the follow-up. The baseline interview guide was divided into four sections, each exploring a different aspect of telehealth: (1) practice philosophy, where we inquired about interviewees’ priorities in patient care; (2) prototypical patient visit journey mapping, a heuristic we used to contrast in-person and virtual visits; (3) future of telemental health, where we asked interviewees to free-list factors influencing telehealth utilization in clinical settings, categorized into technical, clinical, administrative, and regulatory domains; and (4) job satisfaction graph, which prompted interviewees to chart the positive and negative valences of their job satisfaction in 2020 and explain the graph's fluctuations.
The follow-up interview guide was shorter, containing two sections: (1) practice philosophy revisited, to assess any changes in care priorities and (2) Eisenhower matrix, which asked interviewee to assign factors they had listed in the third section of the baseline interview into a 2 × 2 urgent/important matrix. We followed these two interview guides, using open-ended questions and probes to elicit details about interviewees’ experiences with telehealth. We used Google Jamboard for the visual components of the interviews.
Two members of the research team conducted each interview: Interviewer 1 acted as the primary interviewer, while Interviewer 2 acted as the facilitator. This setup allowed Interviewer 1 to conduct the interview, while Interviewer 2 managed Jamboard and took notes. Throughout the interview, Interviewer 2 asked clarifying questions as needed. After the interview, Interviewer 1 filled an impression sheet, which Interviewer 2 reviewed for accuracy. We used these impression sheets to assist in subsequent analyses of the transcripts. In total, we recorded 54 interviews—two with each of the 27 interviewees who gave their consent—and transcribed the recordings using Reduct.Video (Reduct.Video, San Francisco, California).
Data Analysis
We used naturalistic inquiry methods (Lincoln & Guba, 1985) and the constant comparison method (Glaser & Strauss, 1967) to iteratively collect and analyze qualitative data. These methods guided us in sampling strategy and content foci of data collection efforts. They also provided the basis for delineating themes and aggregating dimensions (Gioia et al., 2013) relative to key events (Isabella, 1990).
We began the analysis with open coding to identify first-order concepts within the data set, grouping them into categories. More specifically, we assigned “in vivo” (Strauss & Corbin, 1990) or “first-order” (van Maanen, 1979) codes to the language used by the informant or simple descriptive phrases when no in vivo codes were available. Next, we applied axial coding to develop second-order themes by clustering related categories. We further collapsed themes into overarching dimensions that formed our model. This was a recursive analytic process in which we moved between the emerging theoretical patterns and the data until there are no new alternative conceptual frameworks (Locke, 2000; Miles & Huberman, 1994). We used Dedoose (version 9.0.17) to manage interview transcripts and facilitate data analysis.
We took three measures to ensure the trustworthiness of our data. First, two research team members independently performed line-by-line coding of each interview transcript. The pair then met to discuss discrepancies and reach consensus. As mentioned in the positionality statement, we also invited an additional team member during the data analysis phase to provide a new perspective and discern emerging patterns. This approach yielded high intercoder reliability (Gwet's AC1 of 0.93). Second, we engaged informants in “member checks” to gather their feedback on our interpretive scheme (Lincoln & Guba, 1985). Finally, we adhered to qualitative research reporting standards by using the Consolidated Criteria for Reporting Qualitative checklist, which is available upon request from the corresponding author.
Findings
In this section, we first discuss of four core, connected themes—material affordances, material constraints, embodiment, and relationality—that contribute to the emergence of organizing forms at UTHealth Houston. These themes form the basis of organizing clinical care with telehealth. Additionally, we identify two distinct themes—stabilization and closure—that each play a pivotal role in shaping specific organizing forms. Stabilization drove the development of technology-adjacent organizing for the telemedicine team, while closure steered HCPC toward technology-distant organizing. We provide an overview of these findings, guided by the data structure illustrated in Figure 2, with additional supporting evidence provided in Table 2.
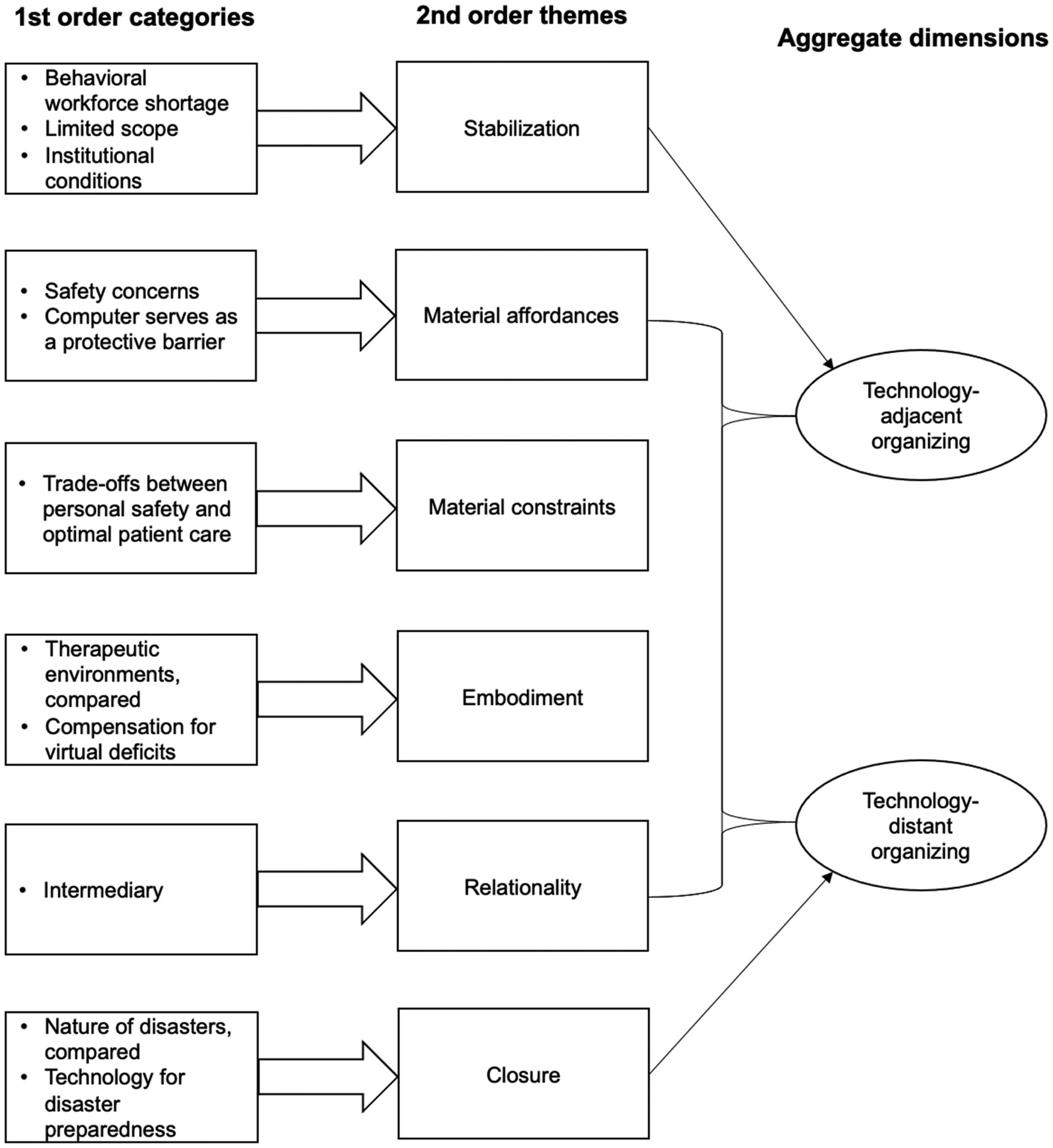
Data structure.
Representative Quotes Underlying Second-Order Themes.

Note: HCPC: Harris County Psychiatric Center.
Material Affordances
Healthcare providers (“providers”) we interviewed expressed concerns about risks stemming from facing attacks from patients and contracting the coronavirus, as reflected in 21 excerpts from 14 study participants (“participants”). Even as physicians, participants worried about their own health and the possibility of contaminating others—patients, children, and other family members. These concerns compounded the baseline risk of physical violence inherent in treating people with SMI, which existed even before the pandemic. The “unpredictability” of patient behavior (HCPC 4, TelemedTeam 18, and Resident 22) and the risk of COVID-19 transmission influenced providers’ interaction with patients. One provider (Resident 20) admitted to rushing during face-to-face interactions with patients during the pandemic and observed other providers doing the same. Falling ill, whether due to physical aggression or biological contamination, carried serious consequences for both providers and their patients.
Telehealth allowed providers to see patients from home, mitigating the risk of illness. As a result, …we're [provider and patient] both safe [with telehealth], I'm safe because if they [patients] become aggressive, they're not going to attack me. But then in the same way, they kind of feel like they can express themselves without going to attack me. And some people actually become more open with the video. I'm not sure if it's because, mostly with expressing anger I would say, because it's not straight to my face, there's a video barrier there too. (HCPC 1)
Provider safety is afforded by digital technology, with the screen acting as a protective barrier that filtered out potential triggers for the patient.
Material Constraints
Providers reflected on a trade-off between personal safety that telehealth affords and the need to provide optimal patient care. This trade-off is partly due to the nature of patients with SMI. Providers used the following terms to describe patient symptoms or diagnoses: psychosis, psychotic, delusions, hallucinations, schizophrenia, psychotic episode, manic, mania, perceptions of reality, paranoia, paranoid, angry, aggressive, aggression, agitation, impaired, and intact. One provider recounted a patient who “asked me what I was doing in the screen. I think he had so severe impaired reality testing that he thought that I somehow got into that screen” (HCPC 11). Providers considered telehealth more suitable for patients in outpatient settings because these patients tend to have higher functioning than those admitted to inpatient settings (24 excerpts among 13 participants).
The use of telehealth makes it difficult for providers to remotely care for—and control—inpatients. One provider explained: When the patients get frustrated, it was very difficult for me to verbally redirect them by telemedicine, because they're supposed to sit there and talking to a screen. When they go and leave the room, you cannot just even verbally redirect and make them come back again. (HCPC 11)
The separation between provider and patient is a constraint that is “inherent to telemedicine in general, you can't actively go and de-escalate a patient in the middle of a crisis,” another provider added (TelemedTeam 14).
Embodiment
The therapeutic environment differs significantly between in person and online settings. In HCPC, patients were often not seen in consultation rooms when they are agitated or aggressive or when social distancing was necessary during the pandemic. Instead, it became more common for providers to see patients in their own rooms or in common areas rather than in designated consultation spaces. One provider (HCPC 2) sees the upside of the virtual setting, noting that it contains therapeutic elements that the provider can use to customize therapy. However, patients are often distracted by stimuli in their homes during virtual sessions. For this reason, one provider bluntly stated: “I just don't think that is a substitute for genuine in-person therapy, with a skilled therapist” (Resident 27).
Providers realized that the tactile quality of in-person interactions was missing when using telehealth to see patients. What they could glean within the camera frame, such as subtle affect and verbal cues, was often not nuanced enough. Furthermore, providers were unable to observe subtle body language outside of the frame, such as patients bouncing their legs or tapping their feet. Signs and symptoms were less apparent when patients were seen over a screen.
Providers were not only frustrated by such material constraints but felt they could not do their jobs as effectively online as in person. Therefore, they “have to work at it [relationship with patient] a great deal” (TelemedTeam 12). More specifically, they had to compensate for the lack of tactile quality, as one provider (Resident 21) explained: “I'm sort of somebody that would pat somebody's hand or be sitting where they wanted to sit. And so I had to work a little bit harder to make that connection.” That “personal touch” (HCPC 6) is important for building rapport and trust (38 excerpts among 16 participants). Furthermore, providers often had to overcompensate for patients who “weren’t matching the effort I was putting in” (Resident 27). Until technology improves, “it's kind of incumbent upon us [providers] to approximate as much as possible the in-person visit to the best of the extent to kind of bridge that gap” (Resident 21).
Relationality
An intermediary, such as a nurse, a medical student, or a physician assistant, would need to be present in HCPC or state hospitals' telehealth consultation room with the patient. This intermediary would relay information about the patient's entire body that the provider would otherwise miss during a telehealth checkup, addressing the disembodiment that occurs during telehealth visits. For example, providers would require assistance from an intermediary during examinations for cogwheeling, a specific type of muscle rigidity associated with Parkinson's disease.
However, providers expressed discomfort with this stratification of labor. One felt it defeated the purpose of telehealth, which is to minimize the risk of physical aggression or biological contamination—key material affordances for providers: I didn't feel comfortable asking my student to go and do that because, the whole reason essentially we're doing telehealth is because we didn't think it was safe to do face-to-face visits. But then meanwhile, I'm asking someone to still go and interact with the patient while I'm at home. So I didn't feel comfortable doing that but on the adult side, I would serve as the person to go and do all of those steps with a patient, so someone could see them from home. Does that make sense? So I wouldn't ask somebody to do that for me, but I would fill in if somebody wanted to work from home. (TelemedTeam 8)
Another provider (HCPC 10) concurred, stating that this staffing arrangement would essentially put the intermediary in harm's way.
Resident 23 summarized the overall dynamic: … how well virtual visits work depend a lot on the technology. First of all, you need good training, and second of all, you need good software. And also, you need good support. And if all those come together, then virtual visits go a lot more smoothly. I think it's actually quite clinic dependent. It can work well or it can be very messy, and that affects patient care and the provider experience and the feeling of satisfaction and burnout.”
The four themes we abstracted—material affordances and constraints, embodiment, and relationality—form the basis of how inpatient mental healthcare is organized with telehealth at UTHealth Houston. We now turn to two themes—stabilization and closure—that distinguish specific technology-related organizing forms.
Stabilization
Even before the pandemic, the McGovern Medical School Psychiatry and Behavioral Sciences Department's telemedicine team (“team”) had a contract with the Texas Health and Human Services Commission to provide care to patients of state hospitals through telehealth. This contract also required team members to visit state hospitals monthly. The contract addressed staffing shortages at state hospitals. For instance, a state hospital in need of a full-time psychiatrist could be served remotely by two part-time psychiatrists. With this arrangement, team members could “supplement the boots on the ground” (Resident 12). These in-person visits were halted when the pandemic began due to provider safety concerns but resumed once team members were vaccinated when the situation stabilized.
For team members, their scope of work encompassed both clinical and non-clinical services. As one explained: The essence of the contract was that we make the monthly trip in order to make face-to-face with our team [at the state hospital], meet with the medical director, attend any trainings of sort … Also, it's not that we can't see our patients via telemed[icine] 100% of the time, but what is taken away is the one-on-one connection with the team members, any administrative responsibilities on site, any court testifying as well. (TelemedTeam 14)
Team members used technology to deliver clinical services, namely diagnosis, treatment, and follow-up care. In spite of the four aforementioned themes, to them, telehealth is more than just telemedicine, as their work also includes nonclinical services such as provider training, administrative meetings, and legal testimony.
Institutional flexibilities were introduced early during the COVID-19 public health emergency in 2000 to expand telehealth service coverage in Texas and nationwide. The measures included requiring insurance plans to offer payment parity for virtual and audio-only services with in-person services; removing restrictions on patient access locations to allow visits from home instead of designated sites in rural areas; authorizing providers to deliver telehealth services across state lines without licensure penalties; relaxing Health Insurance Portability and Accountability Act patient privacy regulations; and providing financial and infrastructural support for broadband expansion to improve internet access in rural and low-income areas. The team providers we interviewed were hopeful that these flexibilities, along with technological advancements, would persist to not only support their work in the future but also continue to fill workforce gaps across in the state.
Closure
Providers drew direct comparisons between the COVID-19 pandemic and Hurricane Harvey, highlighting key differences in the nature of the two disasters. COVID-19 operated on a larger scale (HCPC 9), while Hurricane Harvey was described as “acute” (TelemedTeam 11, Resident 21, and Resident 26). Interestingly, two providers remarked on the “visibility” of these disasters: Hurricane Harvey is more visual, isn't it? I mean, there is rain; I mean there are homes flooding, and people can actually see it happening, but with a virus, it's invisible. I mean, even though it's dangerous or more dangerous than a hurricane because there are 300,000 people dead now in America. (HCPC 10)
Another provider (TelemedTeam 12) noted the “move towards the telemedicine approach and the whole concept of it being an invisible illness, whereas the catastrophe by Harvey was very much visible.”
Providers also pointed out the temporality of these events. Hurricane Harvey had a ‘time-limited” (Resident 23) impact, meaning providers dealt with its aftermath. COVID-19, in contrast, had a “prolonged traumatic course” (Resident 27), asking providers to deal with its protracted effects. Telehealth became a part of the organizational response to a critical event that lacked a physical manifestation but had profound and widespread consequences.
Each disaster reshaped providers’ understanding of the self in relation to the collective. Hurricane Harvey disproportionately impacted specific populations, while the pandemic isolated individuals regardless across all demographics. These events also differed in their penetration of HCPC: Harvey had a lot of external pressures that the hospital couldn't solve…I think the difference is, is COVID, one person could have COVID, it could affect the whole unit. One person being affected by Hurricane Harvey had no effect on anybody else. (HCPC 8)
During Hurricane Harvey, it was incumbent on patients to reach HCPC because the ride-out provision was activated, and providers stayed there for an extended period to deliver care.
HCPC eventually discontinued the using of telehealth as the pandemic reached closure. Study participants perceived telehealth as a viable “option” (HCPC 9 and TelemedTeam 19), “alternative” (TelemedTeam 15), or “backup” (Resident 22) to support disaster preparedness, provided there is electricity at HCPC during or after the next disaster. The social arrangement—namely, relationality and embodiment—has already been tested, as noted by the president of the medical staff (TelemedTeam 11). The technological configuration, despite its material affordances and constraints, is also in place for telehealth to be deployed on site at HCPC or at a nearby evacuation shelter, as elaborated upon by a provider knowledgeable about information technology: The other goal of the [telehealth] project was assuming there is another natural disaster, with UT Southwestern, UT San Antonio, and UT Houston already connected and working together as a team, let's say another “Harvey” is about to happen. You could gather up a whole bunch of computers with cameras and you could go drop off all those laptops at [the] NRG [Stadium]. And now you can set up make-shift clinics. (TelemedTeam 19)
Technology and work can be reconfigured in the event of another disaster, as the “structure is already in place and you don’t have to go create this new structure and this new workflow for doing things.” (HCPC 9)
Discussion
Model
Our findings are integrated into a model, Figure 3, that illustrates organizing work with technology within an organization. Disasters present moments that prompt individuals and social groups to engage in sensemaking around the use of technologies in changing ways of working. The onset of the COVID-19 pandemic catalyzed the widespread implementation of telehealth, acting as a “trigger” (Berente & Seidel, 2022) or providing an “occasion” (Barley, 1986) for novel structuring as this digital technology was enacted in medical practice. Reading from left to right in the figure, professional groups (i.e., HCPC staff, the telemedicine team, and medical residents) scrutinized the form and function of telehealth upon the widespread implementation of this technological artifact at UTHealth Houston. Four connected themes—material affordances, material constraints, embodiment, and relationality—emerged during this moment of enactment, with their connections discussed in the Findings section. Professional groups assigned meaning to telehealth, shaping the artifact's use in practice. In the next moment, these professionals reevaluated whether and how to continue using telehealth to treat patients with SMI. The two themes that emerged during this moment of variation—stabilization and closure—determined the bifurcation into technology-adjacent organizing and technology-distant organizing, respectively.
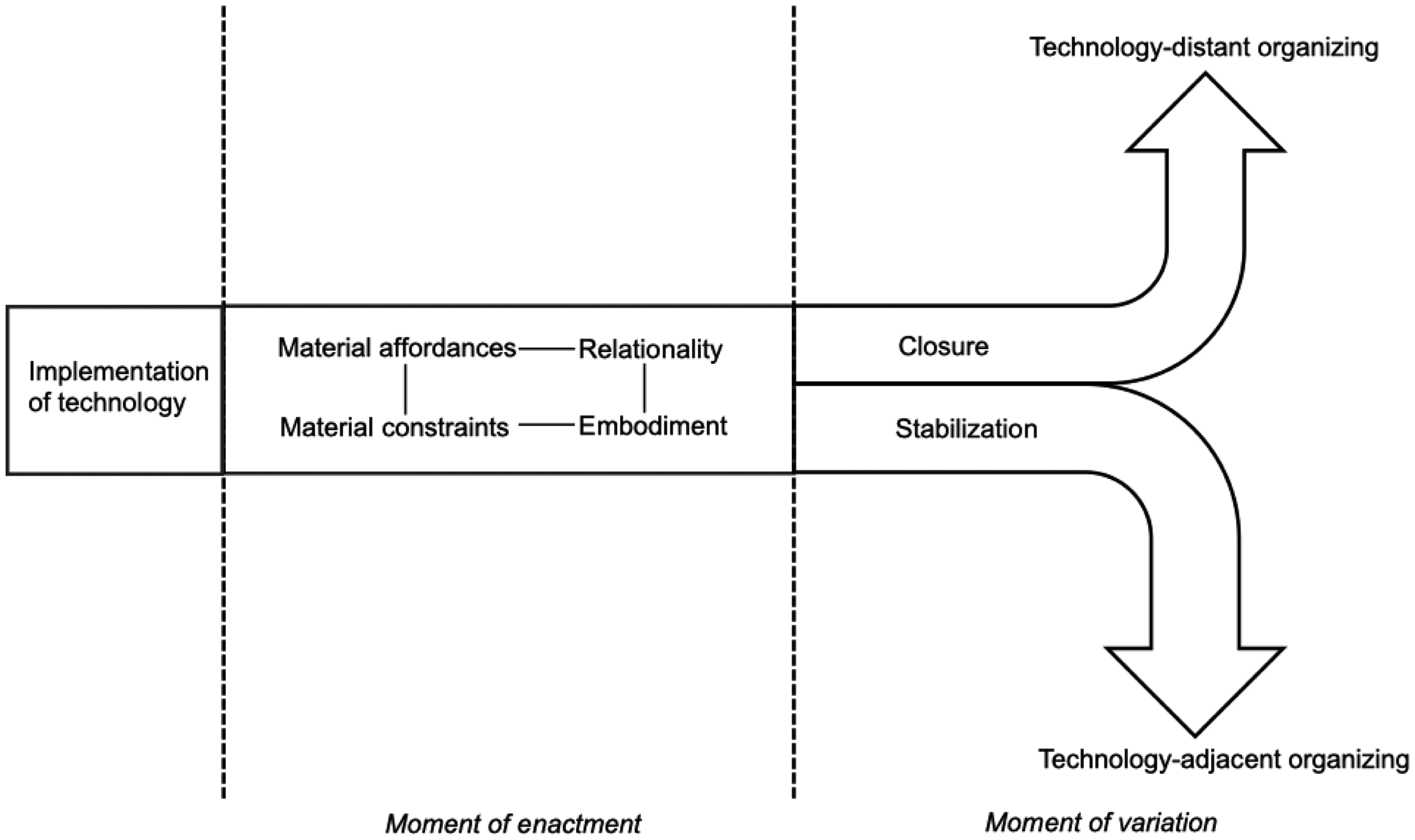
Model of organizing work with technology.
Both the HCPC and telemedicine team had to reconcile the material affordances and constraints associated with practicing medicine via telehealth, thus contributing to the two forms of organizing. Individual healthcare providers and professional groups realized that telehealth could protect them from being attacked by patients or exposed to the coronavirus. These material affordances emerged from their engagement with the focal technology (Faik et al., 2020; Faraj & Azad, 2012). On the flip side, the features of telehealth, designed in this case by the meeting platform Zoom, neither simulated the therapeutic environment nor fully embodied the presence of both provider and patient. These features altered dyadic interactions between provider and patient, fostering limited “distanciated intimacy” between the two, even with real-time afferences and efference in liminal space (Rauch & Ansari, 2022). Telehealth's material constraints hindered the efficacy of treatment, particularly when providers could neither control nor care for their patients remotely.
Some providers rejected the introduction of intermediaries to support the implementation of telehealth, a reordering of social relations of production (Blau et al., 1976; Kallinikos & Hasselbladh, 2009), citing concerns that the intermediaries themselves could fall ill. This relationality deepened the boundary between providers who saw patients from home (e.g., psychiatrists and psychologists) and those who were with patients on-site at HCPC or a state hospital (e.g., nurses, medical students and physician assistants). This dynamic resembled the one Barrett et al.'s (2012) observed among pharmacists, technicians, and assistants working with robotics in a hospital pharmacy. Providers interpreted and perceived this particular digital technology in light of their personal (e.g., work from home), professional (e.g., “first, do no harm”), and organizational (e.g., treat patients so they can be returned to the community) goals (Leonardi, 2011; Markus & Silver, 2008). Together, these four themes provide the foundation for the subsequent bifurcation of technology-related organizing.
Our model highlights an organization's differential responses to the institutional environment through its implementation of digital technology, specifically addressing the health workforce shortage and the occurrence of natural disasters. To address the former, technology-adjacent organizing involves a telemedicine team continuing to use telehealth as part of a hybrid model, combining virtual patient appointments with in-person visits to state hospitals. As one telemedicine team provider said, “By having this virtual health network, you're able to connect [medical] schools to work together for [state hospital] patient access across the state” (TelemedTeam 19). This digitally enabled form of organizing strengthens the interorganizational relations that govern the state-wide behavioral healthcare system. Existing cognitive, normative, and regulative forces from the institutional field continue to fortify this organizing form (Alaimo, 2022; Hinings et al., 2018; Scott, 2013).
Technology-distant organizing entails redeploying telehealth in the event of future natural disasters. Providers drew on their experience from organizing work during previous disasters, particularly the ride-out provision enacted during Hurricane Harvey. Ultimately, HCPC reverted to fully treating patients in person because telehealth's features rendered the quality of care suboptimal. This form of “arms-length” organizing resonates with the conclusion of a prior case in which telehealth was used to maintain the operations of an intensive care unit during a winter storm that struck Baltimore in 2009: “… there is a major opportunity to develop a substantial disaster preparedness model based upon these active, existing programs” (Reynolds et al., 2011, p. 749). It also accounts for both providers’ individual psychological resilience in the workplace and high-reliability organizations’ capacity to maintain operations in high-risk contexts (Bisbey et al., 2021; Williams et al., 2017).
Contributions
Our model makes three contributions and concomitant directions for future research to generalize beyond the UTHealth Houston case. The primary contribution is showing how and why a technology triggered different organizing forms within an organization. Forms of organizing depend on social and material “imbrication” (Leonardi, 2011), “entanglement” (Barad, 2003; Orlikowski, 2007), “coconstitution” (Faraj & Pachidi, 2021), or “assemblages” (Pollock & Williams, 2008) in the workplace. But technology and work were not treated with equal importance in our case. What both of our case's organizing forms have in common is the integration of work with technology rather than technology with work. Work takes precedent over technology in healthcare compared to other industries because patient care is a relatively fixed means of production. Where the two organizing forms differ is in providers’ continued use of telehealth. For technology-adjacent organizing, providers of the telemedicine team accepted online practices in spite of material constraints and sustained them alongside offline practices due to staffing shortages in state hospitals. For technology-distant organizing, online practices are acceptable to HCPC providers only under disaster conditions. Telehealth use at HCPC was discontinued until the next disaster because it could not be fully implemented with sociomaterial practices in situ and disrupted clinical encounters and therapeutic relationships. Providers’ shared experiences with presence, proximity, and participation—the hallmarks of hybrid online and offline practices—remain more salient for technology-adjacent organizing than for technology-distant organizing (Whyte et al., 2023).
The second contribution of our model is highlighting the consequences of implementing a highly rigid digital technology. New technologies, often originating from different source fields, are imported into organizations that are institutionally pluralistic (Berente & Seidel, 2022; Nielsen et al., 2014). UTHealth Houston broadly implemented telehealth in response to the COVID-19 pandemic. The healthcare providers we interviewed expressed limited tolerance for the fixed audio-visual functionalities of telehealth in their enacted practices. This is tied to telehealth's appropriation by stakeholders broader than health professionals, as observed in Israel, who are each guided by different institutional logics (Oborn et al., 2021). Nonetheless, we call attention to the differential agency of professionals in configuring organizing forms—sets of practice roles, values, beliefs, and scripts—within an organization whenever a new digital technology is introduced. Organizations already carry out digital transformation projects under normal operational circumstances, at times bringing the points of design and use together (Yoo et al., 2012). Crises create additional opportunities for experimentation and improvisation with digital technologies, as other scholars have noted during the COVID-19 pandemic (Gkeredakis et al., 2021; Orlikowski & Scott, 2021), facilitating more effective resolution of patient conditions.
The third contribution of our model is considering how each organizing form is shaped by the local context. When we set out to observe telehealth at UTHealth Houston, we were reminded by Nicolini (2006) that technologies are anchored not only to legacy systems already in place but also to broader organizational, legal, and economic conditions. We therefore investigated how organizing telehealth and practicing medicine within the organization align with the institutional environment. The COVID-19 pandemic disrupted usual practices at HCPC. Technology-distant organizing denotes the means to rapidly shift clinical practice from being held in a physical place to a digitally configured space during the pandemic and for future crises. Whereas the COVID-19 pandemic interrupted the established practices of the telemedicine team; it temporarily suspended in-person visits complementing the virtual treatment of patients admitted to state hospitals. Such local sociomaterial enactments need to be supported by macrolevel policies. The resumed use (technology-adjacent organizing) and discontinued use (technology-distant organizing) of telehealth depend on the users, telehealth as an intervention, and the context of telehealth's use (Giddens, 1984; Parker & Grote, 2022; Patel et al., 2023; Reinhardt et al., 2021).
There are many possible uses of digital technology and, consequently, multiple trajectories within an organization. Despite its global reach, digital technology is locally adapted and implemented in specific contexts. Furthermore, technology implementation does not disrupt every unit of an organization equally. Under normal circumstances, individuals and social groups receive new technologies in different ways, partly because they can undermine a set of professional identities while reinforcing others (Jarvis et al., 2022). Crises and disasters put routine practices to the test, destabilizing the organization while creating favorable conditions for new work and technology “configurations” (Orlikowski & Scott, 202) or “entanglements” (Porter, 2013) to emerge. The distant future of work has been imagined with, for example, digital “safe zones” within which disrupted organizational practices could resume during a crisis or disaster (Dries et al., 2024; Gkeredakis et al., 2021). The use of technology to respond to COVID-19 has many localized variations, as exemplified by studies on the continued use of telehealth in Indonesia (Wijaya et al., 2023), Singapore (Li et al., 2023), and Taiwan (Chen et al., 2022). Future studies conducted in different cultural contexts could further explore whether the divergent organizing forms resulting from idiosyncratic, situated enactments of technologies challenges, or reinforces prevailing professional and institutional orders. Institutionalists have suggested that these forms of organizing can engender societal changes from the bottom-up (Hinings et al., 2018; Zilber & Goodman, 2021). Local deviations in the enactment of technology can generate newly legitimate organizing forms, potentially generating broader changes when society is in flux during a crisis.
Footnotes
Acknowledgements
We are very grateful, first and foremost, to our interviewees who generously shared their time and insights with us. This article would not have been possible without the contributions of Ana Cristina Ruiz, Sarah Hernandez, Joanna Luo, Nnenna Mba-Oduwusi, Patenne Mathews, and Umair Hemani. We thank the audience of the 2022 Organization Theory in Health Care Association Conference for their feedback and the audience and two anonymous reviewers of the Society for Studies in Organizing Healthcare for their thoughtful suggestions on an early version of this article. We benefitted greatly from informal conversations with Zach Hyman, Brian Ackerman, and Jennifer Wang, whose professional perspectives enriched this article. Finally, we are grateful to Tracey Adams and the two anonymous reviewers for their invaluable and constructive feedback, which greatly shaped this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was made possible by a grant from The University of Texas Health Science Center at Houston (UTHealth Houston) Center for Clinical and Translational Sciences (CCTS) COVID-19 Pilot Project Awards Program. The content is solely the responsibility of the authors and does not necessarily represent the official views of the UTHealth Houston CCTS.