
Abstract
Knowledge transfer in global mental health services has long been depicted from Western perspectives. This article destabilizes this discourse through a conceptual model that integrates the top-down approach (macro postcolonial context, meso transnational knowledge transfer and micro mental health programmes) and the bottom-up approach (the roles of transcreation in reconfiguring micro mental health intervention, meso mental health services integration and macro policy advocacy and reform). This article raises social workers’ awareness of ongoing development of mental health services from a decolonizing perspective, and guides social work research and practice to continue the decolonization of global mental health services.
Keywords
Introduction
Knowledge transfer (KT) is understood as a complicated process in which various participants such as researchers, users and other stakeholders interact and exchange to facilitate the application of knowledge from research information to different practice (Ayuso-Mateos et al., 2019; Racine and Petrucka, 2011). This concept can be broad, as various synonyms including knowledge translation and knowledge implementation have been interchangeably used to describe it (Siron et al., 2015). This concept has further been used in the global context, particularly to examine how knowledge produced in the West is transferred to developing countries (Siron et al., 2015). Although this concept shows how knowledge can be mobilized dynamically across different contexts, it is essentially depicted from the Western perspective and vindicates the dominant position of Western countries (Kanu, 2005). The inequality between Western countries as hegemonic knowledge producers and developing countries as passive knowledge recipients is thus created, a situation that exacerbates the on-going colonization in KT (Kanu, 2005). This situation also happens in social work. Social work in the Global South still relies on knowledge imported from the West, due to its Western origin and ‘universal’ standards developed by the West (Noyoo and Kleibl, 2019). Nevertheless, the contemporary postcolonial era that highlights decolonization has profoundly affected KT and enlightened researchers and practitioners from both the Global North and South to critically evaluate this linear transitive process (Bunk, 2019; Racine and Petrucka, 2011). For instance, Smith (2019) suggested that epistemic decoloniality, a movement that promotes indigenous knowledge production, can be applied to guide the development of social work education in the Global South. Briskman (2019) depicted that social workers working in Australia’s offshore detention centres have been challenging the knowledge of human rights twisted by the dominant Australian nation-state. As these detention centres are not within Australia’s territory, the powerful Australian nation-state can continue colonialism and conduct state violence to asylum seekers who are often racialized. The nation-state justifies its violation of human rights (e.g. abuse) with the excuse of protecting national security, yet social workers have realized the wrongdoing and called for systemic reforms to truly protect these vulnerable asylum seekers.
Despite that the decolonizing discussion in KT is emerging, surprisingly, relevant discussion in mental health services is still limited. Previous research still explicitly justifies how Western knowledge of mental health services should be transferred to other countries to ‘help’ them establish mental health services (Ayuso-Mateos et al., 2019). This ‘mainstream’ discourse seems to be humanitarian, yet the fundamental colonized premise that underscores Western domination is downplayed (Kanu, 2005). Mental health services are also different from other healthcare services. For instance, while healthcare services accentuate more positivist and instrumental knowledge such as medicine that can be relatively easily adopted by developing countries, mental health services may emphasize more hermeneutic and contextual knowledge (Cooper, 2016). These services need to be placed within clients’ social contexts and assess their social relations to ascertain how social and individual factors may result in mental health issues (Yip, 2006). In addition, each nation-state may view mental health services and individuals’ access to such services differently due to their unique legislative and sociocultural contexts (Wondie and Abawa, 2019). For example, the illustration of different understandings of human rights across countries in defining mental health services and deciding who can access these services may cause inconsistencies when knowledge of mental health services is being transferred globally (Antić, 2022). Another fact that is often overlooked is that both producing countries and receiving countries in KT are not monolithic. Western countries are often treated as a homogeneous group, yet there are also different demands and conflicts about knowledge production and transfer within the Western context (Tsang and Yan, 2001). Each developing country positioned as the recipient is also faced with different situations in the process of KT, as some countries may need to develop their own practice models of mental health services due to the inadequacies of Western knowledge (Yip, 2006). In addition, KT can be a multidirectional process in which the knowledge of mental health services created by developing countries can also be recognized and contribute to global KT (Breuer et al., 2019). Therefore, KT in global mental health services should be seen as an interactive, dynamic and equitable process in which recipient countries defined by the colonizing KT concept can also be recognized as playing a role in knowledge production and exchange (Mills, 2014). In addition, relevant discussion in social work about the roles of social workers in participating in the decolonization of KT in global mental health services is scarce.
In light of these issues, this article aims to reconceptualize KT in mental health services in the contemporary postcolonial era through a conceptual model that articulates the micro (interventions), meso (integration) and macro (policy advocacy) aspects of mental health services. By introducing the concept of transcreation, this article explores the possibility of decolonizing global KT in mental health services at these three integrated levels. The potential roles of social workers in transcreation are also discussed in an integrative manner to bridge the gap in the social work discipline. This article provides a starting point for social work researchers and practitioners to continue elaborating on their roles in decolonizing mental health services in future empirical and theoretical explorations.
Postcolonial discussion and global KT
Postcolonialism can refer to a bundle of theoretical discussions about how marginalized groups such as Indigenous populations and racialized immigrants in former colonies and colonized spaces fought against oppression (Hodgson, 2011; Loomba, 2015), as well as how previous colonies of Western countries strived to be independent politically, economically and culturally (Young, 2016). These theoretical discussions derive from the global context in which independence and anti-colonialism movements worldwide have shattered the colonial order (Loomba, 2015). However, colonial remnants still exist and profoundly shape the global order, which is interpreted by some scholars as on-going colonization (McEwan, 2008; Young, 2016). Hence, two distinct features of postcolonialism emerge from this discussion. The first one is the enduring colonial remnants. For instance, there is a viewpoint that the inspiration of independence of developing countries has gradually dimmed, as these countries have been incorporated into a new order that still prioritizes Western power (Hodgson, 2011). The second feature is the continuous resistance to on-going colonization and exploration of decolonization. For example, Abrahamsen (2007) indicated that developing countries should be alert to the implicit colonial order embedded in the contemporary world, and participate in global communications flexibly through their unique strengths to advocate decolonization. The postcolonial discussion shows a hybrid between colonialization and decolonization and accentuates the need to constantly reflect on decolonization (Loomba, 2015).
This postcolonial discussion in the global context also affects how knowledge should be produced, transferred and utilized between the former colonizers and the colonized. For instance, McEwan (2008) suggested that in postcolonialism, knowledge is a ‘situated’ (p. 35) concept that is determined by the context and creators’ positions in this context. Specifically, Western countries monopolize and universalize this concept drawing on their inordinate power. McEwan (2008) further indicated that the contextual changes in different parts (e.g. socialist revolution in China) of the world across time should not be overlooked, as they create different knowledge and break the monopoly of Western countries.
However, relevant postcolonial discussion, particularly regarding KT in mental health services, is still rare. Breuer et al. (2019) put forward a new model of global mental health services that emphasizes the mutual partnership between Western developed countries and developing countries, as well as the leading roles of developing countries in different stages of mental health services. Nevertheless, the premise of this partnership is still based on the ‘superiority’ of Western countries (the United Kingdom in this case). Particularly, the leadership of developing countries is largely overlooked at the early stage of model design, and this model is only funded and evaluated by the United Kingdom. Their leadership is also limited to the adaptation of different knowledge from the Western context, and the roles of indigenized knowledge from each developing country, particularly in the global KT, remains unarticulated in this model.
Hence, there is an emerging awareness among mental health professionals including social workers from developing countries, aiming to find a process of KT that is best for them. However, this discussion is still nascent, and needs to be explored based on a decolonized conceptualization of inter-country relations in knowledge production. The following section focuses on this point and discusses the concept of transnational KT.
Transnational KT from a postcolonial perspective
Following the above discussion of the macro postcolonial context and its influences on KT, how inter-country relations should be reconsidered is important in reforming the KT concept in a reciprocal and equitable manner, especially when different strengths of each country in knowledge production, utilization and transfer should be recognized.
We adopted a transnational lens to view inter-country relations in the postcolonial era and reconstruct KT among countries based on this lens. Transnationalism is a broad concept; it can be understood as a process in which communications among countries sustained by different participants such as non-governmental organizations, multinational corporations and individuals have been reconfigured, due to the increasing global immigration and migration, economic and cultural interactions (Vertovec, 2009). In parallel with postcolonialism that illustrates the mix of colonial remnants and decolonizing resistances, transnationalism shows how colonization and decolonization continue to be entangled and are manifested through different aspects such as economy, politics and culture across countries (Miyoshi, 1993). However, this concept also contains an emerging decolonized dimension that accentuates the unique role of each country in global communications, as well as dynamic interactions among countries across the boundaries (Briggs et al., 2008). A transnational perspective cognizant of the power imbalance resulting from colonial history is thus adopted to inform our reflection on the influences of postcolonialism, in which colonization and decolonization co-exist, on the reconstruction of power relations among countries and the consequent global KT. Moreover, this discussion shows a dynamic approach to understand various positions of different countries in international relations and the consequent influences on global KT in this postcolonial era. Specifically, the concept of transnational KT has been put forward to illustrate the influences of transnationalism on KT (Duan et al., 2006, 2010). It can be seen as a process of dynamic knowledge flow and interactions across countries (Duan et al., 2006); it breaks the linear KT that was formed in the colonial era and shows the emanative nature of KT (Antić, 2022). Despite the remaining colonial influences on this concept as mentioned earlier, a decolonizing perspective to understand this concept is emerging (Chen, 1996), and affects how knowledge of mental health services transfers globally.
China can be an example that illustrates this concept of transnational KT. In the last two decades, China is emerging as a knowledge producer with increasing global impact, as its investment in research and development (R&D) and number of patent applications have increased dramatically (World Intellectual Property Organization, 2019). However, in the field of social sciences and humanities, particularly in mental health, China still faces long-standing challenges and is eager to acquire knowledge from other countries (Liu et al., 2011). At the same time, its indigenized knowledge of mental health and related services programmes is steadily growing (Zhu et al., 2020). For example, as the first country in the world to deal with the COVID-19 outbreak, research on mental health services during the pandemic in China has already surged (Zhao et al., 2022). In this case, China has not only become a knowledge producer in mental health services, but can also make its knowledge available to other countries. This example of China reveals the practical and complex situation of each country in global KT, and challenges us to think about how transnational KT can be adopted to complement a more current understanding. In the section that follows, knowledge transcreation is introduced as a potential pathway towards a more decolonized approach to KT.
Moving beyond KT to knowledge transcreation
The concept of transcreation first emerged in the field of translation studies. Specifically, scholar and translator Purushottam Lal used this term to describe his process of adapting ancient Sanskrit texts to suit the local contexts of modern language (Pedersen, 2014). In their systematic review of the literature on transcreation, Diaz-Millon and Olvera-Lobo (2023) documented the adaptation of this concept in other fields. For example, transcreation has emerged in the field of health education as a strategy to simultaneously translate interventions both across different languages and across different cultural contexts (Corvin et al., 2017; Nápoles and Stewart, 2018; Simmons et al., 2011). In their research on the implementation of chronic disease self-management programmes in Latina/o/x communities, Corvin et al. (2017) noted transcreation as a key outcome of moving evidence into practice through community-based research.
This conceptual progression from KT to knowledge transcreation has significant implications for our understanding of how research evidence in mental health services travels and changes over the course of its journey from researcher(s) to stakeholders around the world. Most notably, it has the potential to disrupt the epistemological dominance of Western KT strategies as part of the larger colonial system of knowledge production, and through which knowledge producers outside of the West are rendered absent. It does so by reframing the dynamics of KT in two ways. First, the evolution of transcreation through translation studies makes visible the linguistic realities and processes entangled in KT, and in turn opens a critical discussion around how the colonial dominance of the English language shapes, and ultimately limits, the way knowledge travels and transforms through time and space. Second, knowledge transcreation illuminates the non-linear and ever-changing nature of knowledge that extends the time of production long past phases of dissemination. Knowledge consumers in this view are repositioned as co-producers who continue the journey of production as they adapt and reshape knowledge in ways that integrate ‘local’ and/or indigenous ways of knowing. This notion is particularly relevant at times when research evidence is resurrected from the abstract and brought to life in the world of everyday practice.
Even though this concept of transcreation has the potential to significantly shift our understanding of the flow of knowledge from research to practice, knowledge transcreation has not yet entered contemporary KT debates in the fields of mental health services and social work. Transcreation is consistent with the lenses of social justice and human rights in the definition of social work, as this profession and discipline promote equity and liberation for those who are oppressed (International Federation of Social Workers, 2014), a decolonizing perspective that challenges hegemonic Western knowledge systems that shape KT in social work. The Lancet Commission also integrated global equity in mental health into its sustainable development goals as a way of continuously promoting social justice and human rights in the world, especially for developing countries in the Global South (Patel et al., 2018). These contexts thus create a positive space for transcreation to be applied to the re-design of global KT in mental health services. Nápoles and Stewart (2018) encouraged us to view their introduction to transcreation as an opportunity to reflect on the inequality of the ‘mutual’ partnership between developed countries and developing countries covered in previous literature of mental health services (Breuer et al., 2019), and think about how global KT in mental health services should be reconceptualized.
Transnational KT in mental health services
Building upon the concept of transcreation, this section reconceptualizes transnational KT in mental health services through the levels of micro intervention, meso service integration as well as macro policy advocacy and reform, an integrative framework that is often overlooked by social work researchers and practitioners in mental health (Zhao et al., 2022).
The micro level of mental health interventions
Despite indigenized knowledge of mental health interventions in various contexts (e.g. groups, communities) has been developed from different cultures (Hickling, 2020), the transcreation concept from the study by Nápoles and Stewart (2018) can be adopted to promote the proactive role of each country, particularly developing countries, in producing mental health knowledge, facilitating equitable global collaboration and eventually establishing decolonized transnational KT in mental health services. First, mental health services need to be fundamentally reviewed by social workers and other mental health professionals through collaborations with stakeholders and service users such as individuals, groups and organizations. Some possible starting points are how mental health services can be better defined and implemented (e.g. the design of mental health services and access to these services) in their own legislative and sociocultural contexts, and how these services are perceived by those clients and can be continuously adjusted to benefit them. For example, the contexts such as community settings and mental health needs should be carefully assessed within the collaboration (Wondie and Abawa, 2019; Zhao et al., 2023), in order to enable mental health services to be better rooted and grown in their contexts. Social workers, with rich practice experience and close interactions with their contexts, are expected to ascertain the limitations of mental health interventions in their contexts and contemplate how these interventions can be better improved (Bogo, 2018). This step is particularly important for developing countries, as it helps them start to view mental health services from their own perspectives and find their unique strengths (e.g. cultural uniqueness in mental health) that should be paid attention to when developing mental health services (Hughes et al., 2020; Rathod et al., 2017; Wondie and Abawa, 2019). This step can become the foundation for reciprocal collaborations as well as transcreation of knowledge of mental health services across countries. Second, social workers, other professionals and stakeholders from different countries can form a partnership that respects the leadership of local experts in establishing and developing mental health services in their own contexts (Kumar, 2019; Kumar and Bahar, 2019). For instance, social workers in each country should be empowered to critically evaluate their indigenous knowledge of mental health interventions, and work with partners from other countries on transferred knowledge to co-create new knowledge for local mental health services (Kumar, 2019). Third, theoretical and empirical evidence emerging from the above step should also be carefully examined within the partnership (Nápoles and Stewart, 2018). How the scientific evidence can be used properly is a transcreation process whereby both indigenous and transferred knowledge of mental health services are merged, evaluated and utilized based on the discretion of local experts with the support from the partnership. Fourth, feedback from services recipients such as individuals, organizations and communities should also be collected and further taken into the improvements of mental health services. This process is continuous, which requires the engagement with recipients throughout the interventions (Nápoles and Stewart, 2018; Zhao and Bhuyan, 2023). Specifically, service recipients should be able to assist local experts to better ascertain their mental health needs based on intervention implementation, and help them adjust the transcreation process to reflect characteristics of various service recipients (Nguyen et al., 2020). A dynamic circle involving local social workers, other mental health professionals, experts from other countries and service recipients can be formed to constantly boost mental health interventions. Fifth, knowledge produced in this transcreation needs to be actively promoted through this inter-country partnership in different formats such as international conferences. This step facilitates global communications in mental health services, enlightens other countries to critically form partnerships, co-creates new knowledge of mental health, and decolonizes global KT constantly (Kumar and Bahar, 2019).
The meso level of mental health services integration
Building upon the discussion of the micro mental health interventions, the integration of mental health services needs to be discussed to boost mental health systems in the long run (World Health Organization, 2013). The integration of mental health services is comprehensive and can refer to different dimensions. For instance, Zhao et al. (2022) discussed how mental health services on governmental and organizational levels should be integrated to better serve people with mental health needs amid the COVID-19 outbreak in Wuhan. The transcreation concept provides a unique lens to further facilitate the integration of mental health services in the global context. First, based on their reflections upon legislative and sociocultural contexts, social workers and other professionals need to scrutinize mental health interventions on different levels and ascertain strengths and drawbacks of these interventions, and an integrative system that effectively connects these services can be further established (Zhao et al., 2022). These steps are also transcreation processes whereby expertise from different partnership members can contribute to identification of strengths and drawbacks of mental health interventions and establishment of the integrative system, through the discussion, exchange and co-creation of knowledge from their different backgrounds. Local social workers can implement these ideas based on their discretion of fair presentation and inclusion of varied voices in the partnership as well as their familiarity with the local contexts. Second, this integration of mental health services on different levels should also be constantly tested through service recipients’ engagement. For example, while reflecting on their experience of utilizing mental health services, individual clients as well as organizations that seek mental health services to support vulnerable groups might have suggestions on how these services should be integrated so that those who need such services can be better helped in the future. Their feedback can be incorporated by partnership members and inform the changes of implementation of mental health interventions in an integrative manner (Bullock et al., 2010). Third, knowledge regarding the integration of mental health services co-created in this process can contribute to the global mental health services and be critically evaluated and recreated by other countries and their partnerships. Hence, the above-mentioned steps can be dynamically recirculated in other countries, to continuously decolonize the global KT in service integration.
The macro level of policy advocacy and reform
Policy advocacy and reform are also needed to maintain and improve the vigour of mental health services (Funk et al., 2006). They have been found to keep healthcare services sustainable and boost equity in service accessibility and utilization, especially for marginalized groups (Funk et al., 2006). Building upon the previous two levels, partnership members particularly local social workers can obtain comprehensive understandings of mental health services in their contexts and contemplate the role of mental health policies in better supporting these services. With their frontline experience of delivering mental health services, integrating these services, as well as interacting with different service users, social workers can have a tangible feeling of the limitations of the extant policies. Therefore, local social workers and experts from different countries can work together in the partnership to examine mental health policies in the local context, bring in their own knowledge, consider service recipients’ engagement and feedback and co-create new knowledge of mental health policy with the leadership of local experts. This transcreation process of improving policies on mental health services shows how social work in mental health can be contextualized and follow the principle of human rights to address service users’ concerns on different levels, a perspective that can guide social work education, research and practice to continue the decolonizing path (Schmid et al., 2022).
In addition, policy advocacy should also be a sustainable procedure that reflects the reality of community setting as well as the needs of service recipients, particularly vulnerable populations and organizations that help these populations (Abdulmalik et al., 2014). This procedure also requires the reciprocal partnership between empowered researchers and service recipients in transferring knowledge between practice and research (Lawrence et al., 2019). KT on the level of policy advocacy and reform needs to be expanded to the global context, as experiences of this partnership can be critically adopted by other countries and their transnational partnerships, and become the pillar of the development of mental health policies in each country (Wang and Liu, 2018).
Building upon the above analyses, the transcreation of mental health services on the levels of intervention, integration and advocacy can form an integrated system and promote transnational KT in a comprehensive manner. These procedures are also dynamic processes that illustrate the human agency of social workers (Bogo, 2018), as knowledge co-created by different countries can always be adjusted based on their continuous explorations.
Discussion
A model (see Figure 1) that aims to reconceptualize global KT in mental health services in the postcolonial era was put forward to integrate the above-mentioned discussions on three levels. An upside-down pyramid was first presented to show how postcolonialism shapes international relations between previous colonies and colonizers, and how these influences are further narrowed down to transnational KT. The field of mental health services is then focused to demonstrate both the meso influences of transnational KT and the macro influences of postcolonialism. The needs for countries, especially developing countries, to access and utilize more decolonized knowledge of mental health services from transnational KT are thus emerging. Particularly, the transcreation concept was adopted from micro healthcare services and expanded as a new lens to accelerate the decolonization of KT in mental health services. This process requires social workers and other partners to re-establish reciprocal relations and engage with stakeholders and service recipients based on their human agency. A regular pyramid was connected to this transcreation concept and presented to show how transcreation can be illustrated through the implementation of mental health interventions, integration and policy advocacy and reform, and how these three levels in mental health services can form a joint force to shift transnational KT from previous Western domination to more equitable collaborations across countries. These attempts of transcreation knowledge of mental health services across countries can be valuable experiences of KT, transferred to other countries and consolidate the empowerment of local social workers to continuously decolonize mental health services in inter-country collaborations. This conceptual model is also consistent with the perspective on reflexive development put forward by Lutz (2019) in this postcolonial era, as this developmental pattern emphasizes timely adjustments in each country’s social work, following the rapid global changes.
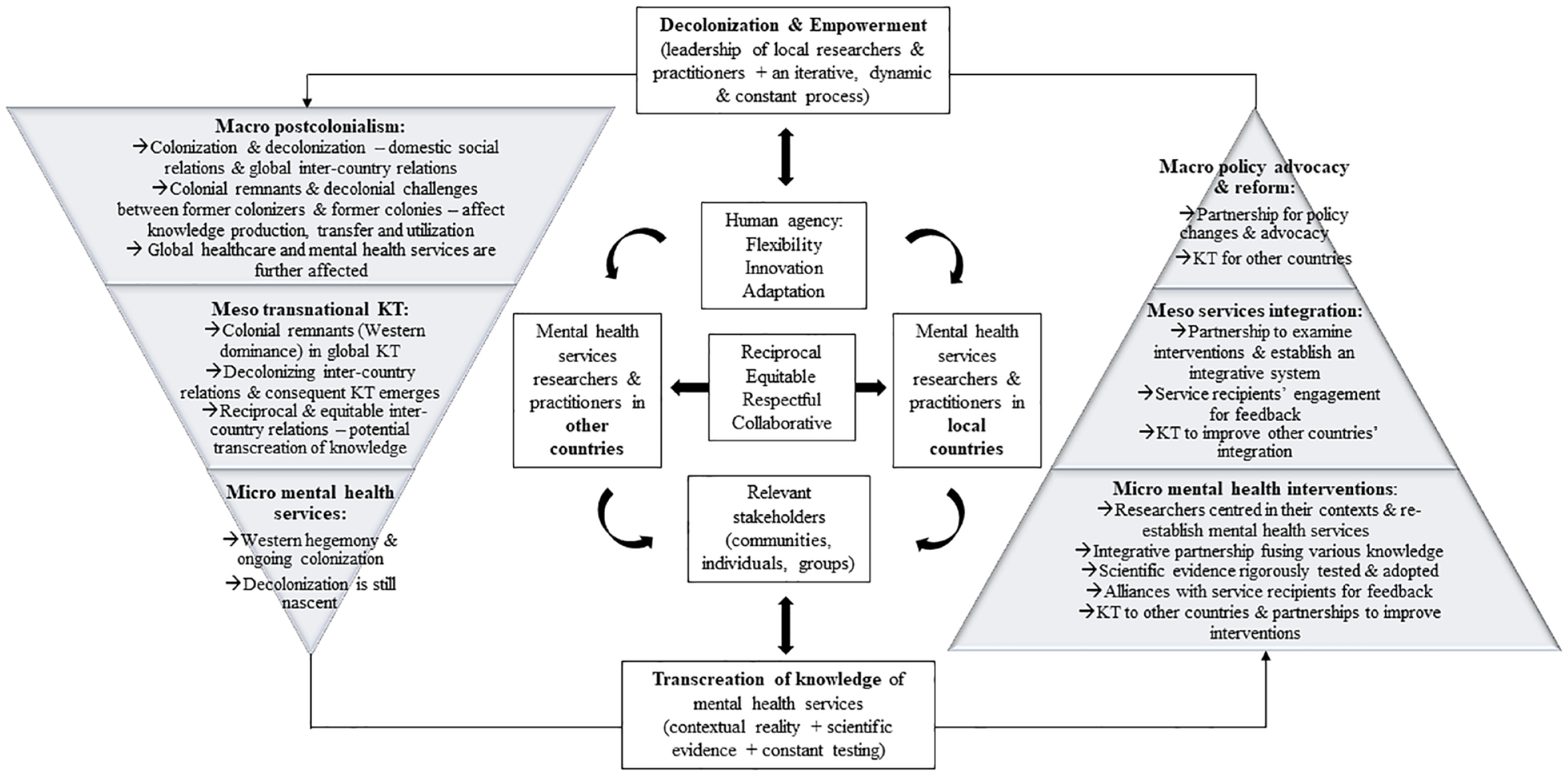
A model to reconceptualize transnational knowledge transfer in mental health services.
This reconceptualization of transnational KT in mental health services has several strengths. First, this conceptual piece helped us form a comprehensive perspective to understand transnational KT in mental health services influenced by postcolonialism and consequent inter-country relations. Building upon this direction, an inclusive perspective was adopted to reframe inter-country relations in transnational KT as more equitable, rather than justify previous colonized relations that featured the superiority of Western countries (Kumar and Bahar, 2019). We further attempted to reconceptualize KT in mental health services across countries through the lens of transcreation, a process that identifies the subjectivity of each country, particularly developing countries, in implementing mental health services in their own contexts, with a reciprocal partnership formed with social workers, other professionals from different countries and relevant stakeholders (Fricchione et al., 2012). This transcreation process is essentially emanative and includes KT both between developing countries and from developing countries to developed countries. It also continues to challenge the colonized KT in mental health services in an iterative manner and bridges the research gap as similar discussion is extremely rare in the literature. Finally, this reconceptualization illustrated the empowerment of local social workers, and emphasized continuous decolonization featured by respectful partnerships. Hence, a vision of how the decolonizing process can be carried out in the long term, according to this discussion of the contemporary context, can guide future social work research and practice in global mental health services. In addition, this conceptual piece also integrated three levels of mental health services, an important insight that is still missing in the field of mental health services (Hughes et al., 2020). Therefore, we believe that this article provides a new lens of decolonizing mental health services in the postcolonial time and can be a good conceptual start for future explorations of global KT in mental health services.
However, several limitations also exist in this model. First, as this conceptual model only discussed transnational KT in mental health services in a global context, its effects on specific countries and their mental health services are thus out of the scope of this article. Future studies can focus on specific countries, explore how global KT, especially the transcreation process, can better serve different countries, as well as reflect decolonization in mental health services. Second, future studies need to explore different roles of social workers and other mental health professionals vis-a-vis those of other community stakeholders and service users, and the effects of their collaborations in the implementation of mental health services. For example, roles of social workers in the partnership (e.g. collaborating with different professions) and their engagement with the implementation of mental health services on different levels (e.g. coordinating mental health interventions, service integration, policy advocacy) can be further developed based on future empirical studies, which in turn guide the continuous development of this conceptual transcreation model. Third, as mental health services are a comprehensive topic with many potentials, social workers across the world need to continue delving into this field, explore all different and subtle dimensions of mental health services and contemplate how transnational KT in these dimensions can be decolonized to ensure equity for marginalized developing countries.
Conclusion
In this postcolonial era where decolonization has gradually been in the spotlight on the international stage, more critical perspectives are emerging to examine global KT. We see this concept being embedded into the contemporary context in which colonization and decolonization are hybrid, with the increasing challenges and resistance to colonization and being illustrated through the implementation of mental health services in the global context. The concept of transcreation provides new insights into how transnational KT in global mental health services can continue decolonizing, so that each country can benefit. Through the conceptual model, it is seen that decolonization of transnational KT in mental health services through the lens of transcreation is a dynamic process that requires constant reflection and innovation from social workers. It is also a long-drawn out process that demands collaborations and commitments across the world, especially when transcreation is still nascent.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.