
Abstract
Summary
Social workers have been members of community mental health teams (CMHTs) for many years. However, a combination of factors has resulted in their removal from CMHTs in some areas in recent years. This study presents findings from a 2018 national survey of CMHT team managers (44% response rate), to ascertain the current position of the social worker within CMHTs in England. Analyses focussed on membership, roles and tasks, and change within the previous 12 months. Descriptive statistics were used to analyse the quantitative data and content analysis to interpret free text comments.
Findings
Social workers were found to undertake a variety of generic roles and tasks but were reported to do so proportionally less often than nurses. A large minority were involved in non-traditional social work tasks such as monitoring medication. In one-fifth of teams, managers thought they had too few social workers. Free text comments suggested that managers valued social workers for their social perspective and expressed concern regarding their removal or the curtailment of their role, perceiving this as having a negative effect on overall CMHT service delivery.
Applications
The findings provide evidence of some instability in the position of social workers within CMHTs in relation to both their membership and their involvement in traditional and non-traditional roles and tasks. Free text comments suggest that if a biopsychosocial model of mental health support, now recognised as essential to long-term wellbeing, is to be achieved, a social work presence in CMHTs is required.
Introduction
There is growing recognition internationally of the social determinants of mental health and of how social inequalities leave those with the least social and economic agency at most risk of mental disorders (World Health Organisation, 2014). A comprehensive mental health service is consequently required to provide support that goes beyond medical treatment to consider the whole person in their environment, an approach that is sometimes referred to as the biopsychosocial model. Social workers play an important part in this process. Within multidisciplinary teams they have been reported to support their non-social work colleagues to ensure the delivery of support that places the service user and their social and familial networks at the heart of practice, providing non-judgemental, strengths-based input that promotes self-determination and long-term recovery (Abendstern et al., 2014, 2020; Allen, 2014; All-Party Parliamentary Group on Social Work, 2016). Evidence from service users and carers suggests that they value social workers for their ability to see them ‘in the round’, to work in partnership with them, and to provide clear communication (Allen, 2014; Kam, 2019; Vicary & Bailey, 2018; Wilberforce et al., 2019). Service users have reported that social workers, when compared with their health colleagues, deliver more person-centred support (Boland et al., 2019). Despite such endorsement, the social work membership of community mental health teams (CMHTs), the cornerstone of mental health services in England, appears under threat (Association of Directors of Adult Social Care Services (ADASS), 2018; Lilo, 2017; McNicoll, 2016).
This article provides new empirical evidence from a national survey of CMHT managers. Its aims are to consider the position of social work within CMHT practice today. Is it secure or shifting, integral or peripheral? And what difference might this make to the quality of support offered by CMHTs? These aims are approached through an investigation of:
The extent of social worker membership of, and the variety of roles and tasks undertaken by them within CMHTs in England, comparing them with other CMHT members, and The views of team managers regarding social work membership (amount), roles and tasks, and the impact of reported changes to these.
The article begins by providing some background on the development of CMHTs and the social work role within them, as part of an integrated health and social care workforce, in order to place the current findings in context.
Background
Adult mental health services have been primarily located within community-based provision across the UK, Western Europe, and elsewhere for many years following a de-institutionalisation process. In England, this dates back to the 1959 Mental Health Act which declared the community as the most appropriate setting to support people with mental ill health, although large scale hospital closures were only evident from the 1980s (Gilburt et al., 2014). From this time, community services for people with severe and enduring mental ill health have been largely provided by CMHTs (Rapaport, 2005) with variation in focus over time reflecting shifts in policy and practice developments about the optimal way of providing support (Department of Health (DH), 1999; Royal College of Psychiatrists, 2018). Two key CMHT features have persisted. First, a responsibility for the delivery of specialised community-based support for specific groups of people. This encompasses assessment and diagnosis, coordination, including within the framework of the Care Programme Approach (CPA), a form of case management introduced to improve care in the community for people with severe mental ill health (DH, 1990, 1995), and provision of a range of therapies, advice and support regarding health and wider social issues. Second, multidisciplinary membership, including medical, health, allied health and social care, and social work staff (Carpenter et al., 2003). Membership has expanded over time with the introduction of new roles following policy reforms (DH, 2007) leading to increases in the employment of clinical psychologists, mental health nurses and psychiatrists and to the introduction of support workers, a wide ranging staff group without professional registration and including peer support workers (Wilberforce et al., 2017).
Social workers have been members of CMHTs from the outset and regarded as core members since the 1990s (Onyett, 2003), despite being employed by Local Authority (LA) Social Services Departments (HMSO, 1968), unlike their health and medical colleagues. This remains the case today with many social workers working in CMHTs seconded from their LA to an NHS trust. Integrating health and social care has been a policy goal of all UK governments for more than 20 years (Cameron et al., 2014; Heenan & Birrell, 2017) with integrated health and social care CMHTs regarded as the best way of delivering comprehensive mental health services, particularly to people with complex needs, despite limited evidence of effectiveness (Brown et al., 2003; Cameron et al., 2014; Carpenter et al., 2004). Social work membership has been viewed as a key marker of progress in this area (Wilberforce et al., 2011). Evidence suggests that the social work membership of CMHTs has been rising with an average of 3.4 per team in 2007 compared with 1.9 in 1994, although social workers remain a much smaller percentage of these teams compared with mental health nurses (Evans et al., 2012; Onyett & Heppleston, 1994).
Despite being a longstanding policy and practice objective (DH, 1998, 1999), achieving integration has been demonstrated to be challenging. One recent report described just 39% of mental health services in England as fully integrated, based on six criteria, including having NHS and social care staff work as part of a co-located multidisciplinary team, an attribute found in 70% of services (ADASS, 2018). Previous research suggests that integration needs to be undertaken at a range of levels from organisational to cultural, to become embedded, with structural mergers having the capacity to improve some aspects of the experience of support, but being insufficient to produce integrated working (Cameron et al., 2014; Onyett, 2003; Pearson & Watson, 2018; Reilly et al., 2007). Measures aimed at overcoming organisational and professional barriers have included the introduction of ‘Section 75 Agreements’ (NHS Act, 2006) that enabled the pooling of health and social care budgets and integration of management structures and functions to enhance service delivery. More recently the Care Act (2014) in England placed a duty on LAs to promote integration of health and social care whilst 2016 saw the introduction of sustainability and transformation partnerships, some of which have developed into Integrated Care Systems, place-based partnerships with control over local funding and services (The Kings Fund, 2018).
Some evidence suggests that where integrated practice emerged from organisational merger, it relied on individual ‘boundary spanners’ (Williams, 2002) who were committed to new ways of working (Hannigan & Allen, 2011; Pearson & Watson, 2018) and who had successfully navigated professional and cultural divides (Cameron et al., 2014). Boundary spanning requires professionals to take on so-called generic roles and tasks alongside those that are considered specific to their profession and others that might have traditionally been regarded as the domain of another professional group. Neither boundary spanning nor generic working have, however, been universally welcomed to date with the erosion of boundaries between professional groups, referred to by Brown et al. as ‘creeping genericism’ (2000, p. 426) leading at times to role entrenchment (Vicary & Bailey, 2018). Those arguing against generic practice cite the loss or underuse of specialist knowledge and skills to the detriment of the service user. This is a particular concern for social workers, whose role has often been difficult to articulate (Morriss, 2017) and who have described experiencing a ‘clash between their unique social work contribution and their role as generic care co-ordinators’ (Bailey & Liyanage, 2012, p. 1113).
The role of social work within mental health has been outlined recently by the DH (2016). This document describes key areas of practice as including: the promotion of recovery and social inclusion; provision of professional leadership and skill in complex, risky and ambiguous situations; support for individuals and communities around resilience and active citizenship; leadership of the Approved Mental Health Professional (AMHP) workforce; and the promotion of a personalised social care ethos and discharging statutory duties (Allen, 2014). In addition, social workers are obliged by law to put service user wellbeing at the heart of their practice (Care Act, 2014), adding a statutory imperative to practice rooted in values of social justice, and the social model of mental health (Tew, 2014). Qualitative research into the CMHT social work role has emphasised their use of value-based approaches such as relational practice and positive risk taking, in achieving long-term recovery, advocating for the centrality of service users rights and wishes, and providing guidance to colleagues in relation to social issues (Abendstern et al., 2020). Research has also referenced social workers’ involvement in work requiring statutory intervention, where there are high levels of social deprivation and complex family relationships (Abendstern et al., 2020; Evans et al., 2012) as well as social workers’ ability to coordinate care and engage with communities (Vicary & Bailey, 2018, p. 78). Together, these practice goals and research evidence demonstrate a distinctive role for social workers within multidisciplinary CMHTs at the core of which is the recognition of inequality due to social deprivation and the need to provide support that takes these issues into account.
Method
The article reports the results of a national survey, conducted as part of a larger mixed-methods research project. The larger study was designed to explore the contribution of the social work role in CMHTs for working age adults and older people (Challis et al., 2014). It examined the responsibilities, roles and tasks of social workers in CMHTs through a national survey (reported on here) as well as focus groups with team members (Abendstern et al., 2020); the characteristics of people supported by social workers in CMHTs via a caseload audit; and aspects of CMHT social work practice most valued by service users through face-to-face interviews using a Best-Worst Scaling tool (Wilberforce et al., 2019). Finally, service user and staff experiences were captured via postal surveys. The research team included three qualified social workers (MA, DC, JH).
Locating teams
To execute a national survey of CMHTs, a complete list of teams had first to be compiled. This involved developing a definition of a CMHT for the study, locating and confirming team names, and contacting the teams themselves. The definition of a CMHT used for this study is a team comprising three or more professions, offering medium to long-term support to either adults of working age or all adults, with a wide range of severe and enduring mental health problems.
A list of mental health trusts (n = 54) was obtained from the NHS website: https://www.nhs.uk/servicedirectories/pages/nhstrustlisting.aspx. Individual trust websites were then searched and a list of CMHTs operating within them extracted. Research and Development teams for each trust were contacted to request confirmation or amendment of these lists in conjunction with our inclusion criteria. In some areas, Clinical Research Networks supporting several trusts were approached. Efforts to contact two trusts failed and two others withdrew due to restructuring or understaffing, reducing our sample to 50. A final list of 421 CMHTs was identified.
Data collection
The questionnaire was derived from a previous study (Wilberforce et al., 2011) and elicited information about team structures and processes, emphasising social work membership and role. It consisted largely of closed questions with defined response options. One question, for example, asked the respondent to describe the sufficiency (amount) of the social work contribution to their team as either very poor, poor, adequate, good, or very good. A small number of questions requested free text responses, including two open-ended questions soliciting further information about the nature of any major change that teams had undergone in the previous 12 months and a request for general comments at the end of the questionnaire.
Paper questionnaires were initially sent out to all teams with information sheets about the study and a link to an online completion option. Teams were contacted between March and September 2018. An initial response rate of 18% was increased to 44% through reminder emails.
Data analysis
Data were analysed using SPSS (Version 23) statistical software. A 10% validity check was undertaken of all data entry with a 1% error found. Missing data on key variables (Bannon, 2015), ranging from 10% to 15%, were randomly distributed. Responses to free text questions were post-coded using coding frames prepared from responses, creating new categorical variables. This included, for example, ‘other’ categories relating to types of staff not listed within the questionnaire. Descriptive statistics (frequency distributions, means and standard deviations) were used to explore these data.
Responses to the two open-ended questions were systematically categorised using content analysis (Bowling, 2002). Although the context of what is said can be as important as the number of times a word or phrase is used, the nature of the current data (a large quantity of short statements) indicated that the number of times particular issues were raised was also essential to report as one measure of importance given to them. Text was categorised into discrete ‘content areas’ and then grouped into higher level ‘dimensions’. In a small number of cases, where individual comments related to more than one content area, they were split, to ensure that all issues were included. This task was iterative and undertaken by two researchers working together (MA and RP).
Results
A total of 188 team managers returned a questionnaire (44% response rate), spanning the 50 participating Trusts and covering all nine English regions. The spread of responses ranged from 80% in three regions to under 30% in three others. Most (59%) completed paper copies. Quantitative results are reported below in relation to membership and role. The findings from the open-ended questions follows, providing evidence of change experienced by the teams over the previous year and managers’ views regarding this.
Team size and membership
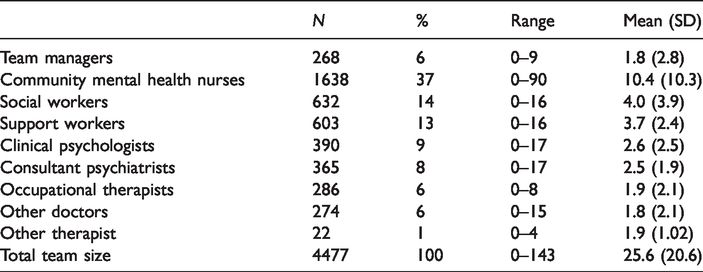
All teams included a team manager, nurses and one or more consultant psychiatrist. Just over 80% of teams included social workers with 87% reporting occupational therapist (OT) membership. As shown in Table 1, mean team size was 25.6. Almost all staff, regardless of profession, were classed as core team members. The largest single group were nurses (37%, mean = 10.4) with social workers (14%, mean = 4) comprising the second largest group. Support workers, albeit incorporating a range of job titles, had only a slightly lower mean than social workers, whilst psychologists had a higher mean membership than OTs.
CMHT membership by profession.
Over half of respondents described the sufficiency (amount) of the social work contribution to their team as being either ‘good’ or ‘very good’. Just over one-fifth (22%) described it as ‘poor’ or ‘very poor’ with the same amount describing it as ‘adequate’. Just over half (55%) also reported gaining one or more social workers over the previous 12 months with just under half (47%) reporting social work losses. Those team managers’ reporting poor or very poor sufficiency of the social work contribution to their team also tended to report social work losses in the last 12 months (and to comment negatively on this issue when describing change). Sufficiency ratings were also positively related to the number of social workers reported to be core team members with those reporting good or very good sufficiency having a higher number of social workers in their teams than those reporting sufficiency as adequate, poor or very poor.
Team roles and tasks
Analysis of data on team roles and tasks (Table 2) revealed a high level of generic practice across professions with nurses, OTs and social workers undertaking a range of roles in the majority of teams. These included acting as care coordinator or enhanced CPA coordinator, and undertaking ‘duty’ work. These professional groups also undertook tasks such as conducting initial assessments, in over 60% of teams. The percentage of nurses undertaking these roles and tasks was substantially higher (between 88% and 97%) than for social workers (or any other team member) who were reported to undertake the same roles and tasks by fewer than 70% of respondents.
Roles and tasks within CMHTs by profession.
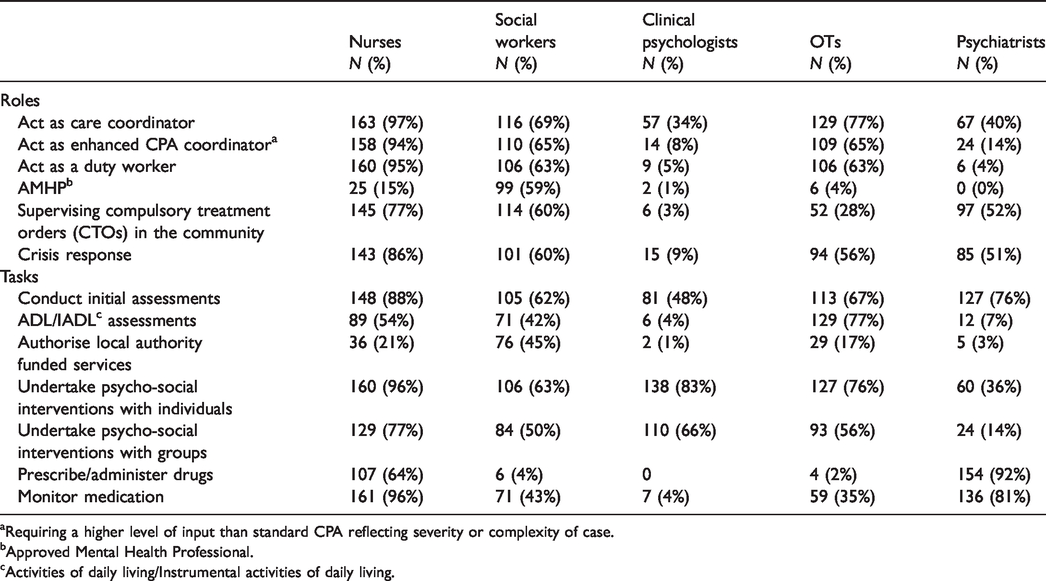
Requiring a higher level of input than standard CPA reflecting severity or complexity of case.
Approved Mental Health Professional.
Activities of daily living/Instrumental activities of daily living.
Roles and tasks traditionally associated with particular professions were still largely undertaken by them. For example, in 92% of teams psychiatrists prescribed or administered medication compared to nurses who did this in 64%, and social workers and OTs in 4% and 2% of teams, respectively. Social workers were the largest group to have the task of authorising services funded by LAs and were AMHPs, additionally qualified professionals undertaking a range of statutory roles, in 59% of teams compared with nurses and OTs in 15% and 4% of teams, respectively. Finally, nurses monitored medication in almost all teams compared with social workers who undertook this task in just over two-fifths and OTs in just over one-third of teams. Social workers were found to conduct psychosocial interventions with individuals in fewer teams than psychologists, nurses and OTs and to be routinely involved in the supervision of Compulsory Treatment Orders less often than nurses although more frequently than other professional groups. Comparing nurses and social workers overall, nurses were reported to be more frequently involved in almost all the roles and tasks listed, than were social workers, with the exceptions of undertaking the AMHP role and the task of authorising LA-funded services.
Experience of change
Topic focus of free text comments.
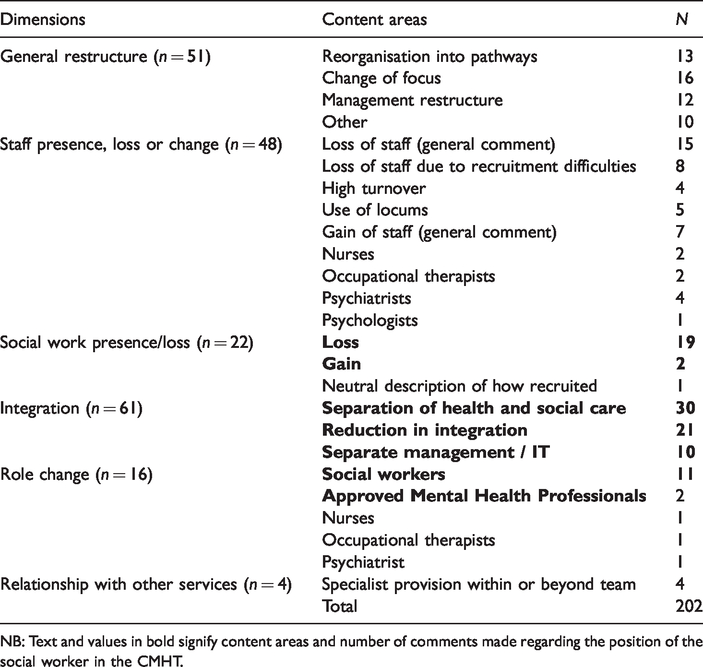
NB: Text and values in bold signify content areas and number of comments made regarding the position of the social worker in the CMHT.
Approximately half the comments to the question about change in the last 12 months were general statements relating to a change in team focus and/or management structures. The remainder related more specifically to integration with the separation of health and social care and particularly the extent of the social work contribution, being the most numerous. Most comments at the end of the questionnaire also focused on issues of integration and concerns about the loss of social workers to their teams. A small number referenced how their team related to a range of specialist services in their locality, expanding on the previous question in the survey which asked about this issue. The text below focuses on topics relating to the position of the social worker within the CMHT which accounted for 46% of comments overall.
The changing position of the social worker in the CMHT
Changes relating to the position of the social worker in the CMHT were described in terms of causes, substance and impact. The former consisted of the ending of Section 75 agreements and additional LA duties such as statutory assessments, delegated to social workers, following the introduction of the Care Act (2014). Substance included the removal of social workers from CMHTs in some trusts and a curtailment to the work they did within the teams, in particular a move away from generic roles and tasks (e.g. care coordination or CPA) in others. Impact was described in terms of a reduction of integrated approaches resulting in more limited communication and collaboration; loss of experience and knowledge; increased workloads and types of tasks and roles taken on by other CMHT staff; and the larger negative impact on staff and service user experience and service delivery. Commentary noted, for example, the ‘detrimental effect on the care we provide across localities’ due to the loss of social workers (17.1) and to the ‘unnecessarily fractured care provision’ (12.2) it resulted in. Another manager commented that ‘since social workers were removed from joint working the care/support to service users I feel has been negatively impacted' (17.5).
Others described the positive impact of the integrated practices – that had been lost when social workers were removed – which had produced: ‘Supportive working relationships with social work colleagues with enhanced and more informed level of care able to be offered from shared resources being within team’ (21.2). Social work team members were described as having ‘benefited service users and provided support for all professional disciplines’ (17.3). Another respondent commented on the range of interventions undertaken by social workers, stating that these were ‘often the most effective intervention for service users who are unable to tolerate therapy or group work’ (19.4). In contrast to these concerns about the negative impact of the loss of social work input into CMHT practice, were others who suggested that the social work role itself had been diluted as a result of integration with a focus on ‘social workers facilitate[ing] care packages’, linking this with poor social work recruitment and retention (4.1).
Overall, managers’ remarks indicated that social workers were valued by them both as an extra pair of hands when undertaking generic work (e.g. ‘additional social workers can offer a lot of generic working … now required’ (27.4)) and for their specialist contribution, including ‘skilled risk assessments, assessments of mental capacity [and] focussed social work interventions’ (19.4) which enabled CMHTs to offer more comprehensive and holistic support. Their loss to the team meant a loss of easy and informal access to their ‘specialist skills and knowledge within mental health’ (37.2) and of a collaborative approach that benefited all. One manager, commenting on imminent change in their team, noted that:
In the coming weeks the role of the social workers will change within the CMHT … we will no longer offer a holistic care coordination approach but instead a fragmented health/social work divided approach with the social work staff offering ‘Care Act’ work with mental health populations only … This is due to a focus on finances over client need (13.2).
Another manager’s comment stressed the importance of full integration between health and social care within CMHT practice and that these sectors and their staff needed ‘to work together to promote seamless care for our patients’ (4.3).
Discussion
These findings provide new evidence about the numbers and contribution of social workers within CMHTs as well as recent and imminent changes regarding these features at the time of data collection in 2018. The implications of the findings are considered below in relation to the aims of the article: to consider the position of social work in CMHTs in England, whether stable or in flux, peripheral or central, and the implications thereof.
Team membership
Findings from this study are in line with a trend towards larger teams over the last 25 years (Boardman & Parsonage, 2005; Huxley et al., 2011; Onyett & Heppleston, 1994). Previous surveys of CMHTs for working age adults and for older people both reported smaller mean team size than the current study (Huxley et al., 2011; Wilberforce et al., 2013). A comparison of the current findings on social work team membership with those from a previous study suggest a slight upward shift in mean numbers per team alongside social workers representing a smaller percentage of the whole: 14% compared with 19% in 2007 (Huxley et al., 2011). The same study reported that nurses made up 33% of team membership in 2007, compared with 36% in the current study. These comparisons suggest that CMHTs have grown due to increasing numbers of non-social work staff, particularly mental health nurses. Other evidence supports this. A recent social care workforce study (NHS Digital, 2019) reported that social workers and occupational therapists, part of the same ‘professional job group’, employed by LA social services departments, from where, as noted earlier, social workers in CMHTs are often seconded, had increased in size by only 700 between 2011 and 2018. In contrast, between 2014 and 2019 the Care Quality Commission (2019) reported an increase of 15% in mental health nursing numbers from a larger baseline. This discrepancy between social worker and nurse numbers in CMHTs found in earlier studies has continued despite guidance issued at the start of the century that indicated the need for a ratio of three social workers to every four nurses (DH, 2001). Looking to the future, this gap seems likely to continue with NHS England (2019) recently committing to recruit an additional 1540 nurses and just 360 social workers to adult community mental health services over the next five years.
Compared with earlier research findings, the mean number of psychologists per team was higher in this study (e.g. Huxley et al., 2011). The impact of the growth of other staff groups, including psychologists, on social workers is unclear. Whilst psychologists may share certain values and approaches there are also important differences between them and social workers. These include the social worker’s statutory knowledge and function and their more informal relational approach (Folgheraiter, 2007), something that, as noted by one respondent above, was more suitable for some service users with chaotic lives, compared with the formal counselling provided by psychologists.
Overall, the quantitative data demonstrated similar rates of flux in relation to teams gaining and losing social workers, in line with NHS Digital (2019) data. However, these figures started from a position of insufficient social worker contribution in a fifth of teams. Finally, the turnover of staff, as noted in other studies, may have resulted in a loss of expertise as long-serving staff move on and are replaced by newly qualified personnel who are cheaper to employ (Hanley et al., 2017).
Social work contribution to CMHTs
As noted in the introduction, how social workers and others CMHT members are utilised: as either generic practitioners carrying out roles and tasks that are also undertaken by others, or as specialists focussing on areas that require their particular expertise, has long been debated (e.g. Brown et al., 2000; Hannigan & Allen, 2011; Peck & Norman, 1999). Central to these debates are issues of effective multidisciplinary team working and how to optimise professional specialisms within integrated practice. Some research suggests that social workers have faced particular challenges in relation to these issues, being minority members of health-dominated CMHTs (Morriss, 2017), whilst other research indicates similar issues for occupational therapists (Reeves & Mann, 2004) and psychologists (Holmes, 2001; Onyett et al., 1997).
Qualitative evidence of the social work role within CMHTs for older people (Abendstern et al., 2014; Challis et al., 2014) showed social workers combining generic and specialist functions. The former included undertaking initial assessments and care coordination, arranging care packages, conducting financial assessments, whilst the latter involved the provision of expert knowledge of mental health legislation and safeguarding issues. The quantitative results within the current study indicate that social workers in these teams undertook a similar mix of tasks, suggesting continuity of role content over time and between settings. However, the free text and quantitative data also suggest that this might be changing. Whilst the quantitative data showed social workers undertaking a range of generic roles and tasks they were found to do so proportionally less often than nurses, for example, in relation to acting as a care coordinator, undertaking ‘duty’ work, and conducting initial assessments. At the same time, the free text data reported a curtailment of the social work role away from generic practice within some teams alongside their removal altogether in other CMHTs. As respondents’ free text comments suggest, it is possible that the pressure of ‘creeping genericism’ (Brown et al., 2000) has come up against a new obstacle, that of legislative change brought in by the 2014 Care Act, that has resulted in additional statutory duties for social workers such as Care Act Assessments, limiting the time they have to undertake the range of roles and tasks expected of a generic CMHT workforce.
Some functions traditionally associated with social workers were found by this study to be still largely undertaken by them. This included undertaking the AMHP role, although the percentage of social workers reported to be doing this (59%) was much smaller than that reported by ADASS (2018). The latter found that only five per cent of the workforce came from professions other than social work despite the role having been open to other professions since 2007 (Mental Health Act, 2007). Given the very small proportion of teams indicating that this role was undertaken by other team members in the current sample, it may signify that the ‘shortfall’ is being undertaken by social workers outside CMHTs. Again, the ADASS (2018) report would support this with a range of models of AMHP practice noted to be in existence with only 36% operating an approach where most AMHPs are based in CMHTs.
Another finding from the study is that social workers were also engaged in tasks not typically associated with their profession, such as monitoring medication, in a substantial minority of teams. Given the social model of mental health at the heart of social work practice, rather than seeing this as a misuse of their specialist skills, it could be argued that the social workers’ involvement in this work is vital to support a shift in mental health treatment ‘to a system of biopsychosocio-cultural care where medications are prescribed with attention to the broader social and environmental context’ of the service user (Hughes et al., 2017: 424) as well as their wellbeing and wishes. In North America this recognition has led to an increased acknowledgement of the ‘importance of including neurobiology and pharmacology on their curricula’ (Lee & Fleischer, 2014: 475).
As described above, social workers bring a specific set of skills and values to mental health practice that often result in a different perspective on treatment and support to their health and medical colleagues. This has been reported elsewhere, for example, in relation to judgements about case complexity (Cestari et al., 2006), operating least restrictive approaches (Pinfold et al., 2002; Steinert et al., 2005), and placing the person at the heart of practice (Penhale & Young, 2015). Findings from other elements of the larger study provide additional evidence to support this with social workers described as leaders of the social model, required to ensure that CMHT support was holistic, person-centred, and promoted long-term recovery (Abendstern et al., 2020). The free text data within the current study suggested that where social workers had been removed or had left teams, it had had a negative impact on other staff and service users alike, resulting in a less collaborative, coordinated and holistic service. Byrne and Onyett (2010) argue for integrating models that place the service user at the centre and focus on achieving long-term recovery. Social workers have a key role to play in CMHTs in leading and supporting the whole team in such a joint a mission. These findings chime with the recent English policy and practice context, including an independent review of the Mental Health Act (Department of Health and Social Care, 2018), which advocated that mental health social workers play a growing leadership role in psychiatric care.
Implications
Overall, the findings point to some flux in the position of social work within CMHTs. There was a perceived curtailment of their contribution to the team, to some extent supported by quantitative evidence that social workers undertook a range of generic roles proportionally less often than nurses. At the same time, involvement in non-traditional tasks such as medication monitoring was also noted. Curtailment of the social work role in some teams and its loss altogether in others was met with concern from team managers. Respondents spoke positively of the social work contribution and of how social workers were leaders in the social model with the skills to support their colleagues to understand this perspective and to work collaboratively to deliver holistic support. This suggests that the loss of social work to CMHTs may be a step backwards in relation to integration and towards more silo working that has been found to be detrimental to effective practice in a range of sectors (Willcock, 2016). Role curtailment might also impact on recruitment and retention, with social workers’ job satisfaction diminishing where their role is restricted to facilitating care packages and undertaking statutory obligations. The finding that social workers were involved in medication monitoring in a substantial minority of teams points to the need for training in this task to become a core part of mental health social work education (Bentley et al. 2005; Hughes & Cohen, 2010) and to the need for clarification of the social work role in this context. Finally, the findings do not tell us how many social workers are enough. However, their continued minority status places them in a position of some vulnerability to policy and practice change despite evidence suggesting that they play an important role in sustaining and developing a biopsychosocial model of care and strengthening the voice of service users.
Strengths and limitations
First, the study achieved a respectable response rate (Bowling, 2002) although lower than in previous studies of a similar nature undertaken by this research group. This is in line with other research findings (Cook et al., 2009) and perhaps reflects the pressure that managers are under in the present climate of austerity and service restructuring alongside increasing demands from research itself. Second, it is possible that the language used to describe roles and tasks within the questionnaire was inadvertently linguistically biased towards health care practice resulting in an under-representation of social workers’ roles. The free text data adds weight to this view with comments emphasising roles that are not reflected in the tasks list, suggesting that the results should be treated with caution. On the other hand, these data also point to certain roles, such as care coordination, being undertaken less frequently by social workers, a finding in line with the quantitative evidence. Finally, there is a possibility that the phrase used in one question in this survey about the sufficiency of the social work contribution to the team, could have been misinterpreted. This is a recognised shortcoming of structured questionnaires which rely on the assumption that question wording will be understood uniformly by all respondents (Bowling, 2002). Our expectation was that this would be understood to mean the adequacy, or not, of social work numbers. However, some managers might have understood the question in terms of the adequacy or level of social work practice.
Conclusion
The study provides evidence of instability in social work membership and role within CMHTs in England and of managers’ concerns about the loss of social workers and the curtailment of the role of those remaining in CMHTs. Managers’ views, alongside quantitative evidence of roles undertaken by social workers in CMHTs, support statements from within and beyond the profession (e.g. Allen, 2014; Department of Health, ADASS, PSW Network, 2017) that social work is integral to the provision of a modern integrated mental health service that recognises the importance of the biopsychosocial model to service user wellbeing and long-term recovery. Decisions to remove social workers from CMHTs are likely to undermine important aspects of this work.
Footnotes
Authors’ contributions
MA led the work, contributed to data collection, supported analysis and drafted the manuscript. MA, MW, JB, JH, RP and DC all contributed to the survey development. SB and JB undertook data collection activity. MW and SB supported data analysis. JH and DC provided oversight to the general conduct of the study. CR oversaw the final stages of the study. All authors contributed to the final manuscript.
Ethics
Ethical approval was granted by the NHS Health Research Authority, North of Scotland (2) Research Ethics Committee: grant number: 17/NS/0127.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was funded by the NIHR School for Social Care Research.
Acknowledgements
The views expressed are those of the authors and not necessarily those of the NIHR SSCR, the National Institute for Health Research or the Department of Health and Social Care.