
Abstract
Summary
Burnout has become an increasingly prevalent condition, especially affecting professionals in direct contact with clients. Human service workers (HSWs) have quite emotionally taxing jobs supporting vulnerable groups. In developing a close relationship with the communities they work with, it could be possible that community-related variables have an impact on HSWs’ burnout. We aim to analyze the prevalence of burnout in a sample of HSWs from Portugal and the role of community resilience as a predictor of their burnout, as well as explore if their subjective well-being and community attachment could explain the relationship between community resilience and burnout, during the COVID-19 pandemic. Data were collected through an online questionnaire between August 2020 and January 2021 (N = 598).
Findings
Results indicate that HSWs presented medium to low levels of burnout, although 8.9% presented high levels. Those who reported lower levels of burnout perceived higher community resilience and had much higher well-being and community attachment. Findings point to community resilience having a significant direct effect on burnout and also an indirect effect, which was explained by subjective well-being and community attachment.
Applications
Results seem to suggest that this sample's low-medium levels of burnout could be linked to the benefit of experiencing high community attachment and working in communities with high resilience, which consequently impacted their well-being and burnout. This highlights the crucial role of the work context in professionals’ mental health, showing that a broader context needs to be considered in professional mental health promotion programs.
Introduction
Occupational stress and, consequently, burnout have become so increasingly prevalent that the World Health Organization has deemed it a serious health issue (World Health Organization, 2019). Stress occurs when demands overcome an individual's ability to react or adapt to the situation. When those demands are considered a threat and are continuously perceived as surpassing the person's resources, especially in a long-term situation, they can lead to burnout (Gonçalves et al., 2019). Although this construct was originally identified in human service workers (HSWs), research has then tended to focus on other professional groups. The present study centers back on HSWs, recognizing how demanding their professions are, as well as the important role they play in the communities they work in. The role of a HSW is through and for the community, both of which cannot be dissociated, even more so in a period of crisis, such as the COVID-19 pandemic.
The first positive COVID-19 case in Portugal was registered in March 2020, which was followed by mandatory national lockdown rules and the indefinite closure of commercial establishments and educational institutions. The country started reopening in May, gradually resuming some of its routines. In September and October 2020, the number of cases increased again, leading the Government to progressively impose confinement measures once more. In December 2020, a state of emergency was declared and the confinement measures got tighter (e.g., mandatory teleworking when possible). The third wave of the pandemic, the one with the highest death toll, took place in January 2021. By the end of the data collection period (January 2021), over 720 thousand people had been infected in Portugal with the coronavirus and over 12 thousand had died (Direção-Geral da Saúde, 2021).
The COVID-19 pandemic has had an unprecedented impact on health and care systems worldwide, with its effects culminating in the deterioration of the mental health and well-being of frontline response workers (Søvold et al., 2021). Albeit in different roles, HSWs have also been at the forefront of responding to the social crises arising from the current pandemic (Magruder et al., 2022), partly taking the brunt of responsibility for client care and, therefore, substantial pressure (Rothschild et al., 2022). Recent data show that 69.5% of HSWs reported that COVID-19 had at least one form of impact on their lives, with 43.9% of those individuals claiming negative effects on multiple areas of well-being (Magruder et al., 2022).
The experience of burnout in this population is of particular concern, as it tends to lead to worse care delivery to the people who need it and to their dehumanization. To avoid feeling overwhelmed and distressed, these professionals take more self-imposed breaks to escape their patients/clients, which ultimately comes at their expense (Maslach, 1976). A recent study about burnout in mental health professionals (Ensari, 2021), whose caregiving arguably shares many similarities with the work performed by most HSWs, shows that the mental health professionals’ experience of burnout also negatively affected their clients—their empathy and quality of care were reduced, they exhibited more rejecting feelings toward patients, more tardiness, and a decline in active listening. A prior study by Morse and collaborators (2012) showed similar results in the quality of care provided since emotional exhaustion and depersonalization were correlated with negative attitudes (e.g., being emotionally distant).
The United Nations (UN) highlighted the importance of community resilience for recovery amid the COVID-19 pandemic, considering it, alongside social cohesion, as one of the five pillars of economic recovery. It was also suggested that studying this construct could strengthen communities and potentially prevent such negative consequences during a future crisis (Annette, 2021). In this sense, community resilience may play a central role as a protective factor against stress related to disasters and emergency crises (e.g., Gilbar et al., 2022; Kimhi et al., 2017; Kimhi & Shamai, 2004) by increasing preparedness and social stability in these situations (Gilbar et al., 2022). Here, we test the hypothesis that more community resilience is associated with lower burnout levels.
Summing up, this study analyzes the prevalence of burnout among HSWs in Portugal during the pandemic (2020–2021) and aims to understand how it is influenced by the resilience of the community they work with/in. This study will further explore if HSWs’ subjective well-being (SWB) and community attachment could be a two-process way to explain the relationship between community resilience and burnout.
Burnout among HSWs
Burnout can be conceptualized as the result of chronic workplace stress that has not been effectively managed (World Health Organization, 2019) and it traditionally includes three dimensions: exhaustion (i.e., individual strain dimension); depersonalization and cynicism (i.e., interpersonal context dimension); and reduced personal accomplishment or inefficacy (i.e., self-evaluation dimension; Maslach et al., 2001).
The consequences of burnout occur at the individual, family, and organizational levels (Maslach et al., 2001) and at different dimensions. More specifically, it is possible to divide burnout outcomes into affective (e.g., irritability), cognitive (e.g., difficulty in concentrating), physical (e.g., headaches, insomnia), behavioral (e.g., excessive procrastination), and motivational (e.g., resistance in going to work). These negative effects invariably translate into some form of job withdrawal, such as absenteeism, intention to leave the job, and actual turnover. Even when employees remain on the job, burnout leads them to be late more often, to be less productive and less invested in their work, as well as to lower job satisfaction and a reduced commitment to the organization (Maslach et al., 2001; Queirós et al., 2014).
These outcomes render clear why burnout has been widely explored across occupations. Although the vast majority of burnout studies tend to focus on healthcare professionals (i.e., physicians and nurses), there is evidence to suggest that it is relevant to study other professional groups who work in direct contact with communities (Lizano, 2015).
Human service workers provide a variety of services aimed at improving their clients’ lives, as they tend to work with groups struggling with hardship (e.g., homeless people), and assist communities to function as effectively as possible (Moffat, 2011). These professionals intervene in a broad number of settings, from housing and shelter organizations to nursing homes, and can work in various fields depending on the type of organization they are a part of, their roles within the organization, and the population they are serving (Moffat, 2011).
A systematic review (Lizano, 2015) showed that HSWs are at great risk of stress and burnout due to the emotionally taxing nature of their work with vulnerable or distressed clients, when compared to other occupations (demonstrating one of the worst experiences of physical health, psychological well-being, and job satisfaction in the workplace). It remains fundamental for these workers to show compassion and empathy to build a connection with their clients, which implies a significant daily emotional commitment, a process that can cause emotional exhaustion and depersonalization (Lizano, 2015). Beyond that, HSWs are exposed to their clients’ experienced trauma, which can negatively impact their health and well-being, especially as it often results in compassion fatigue (i.e., experienced stress resulting from exposure to a traumatized individual rather than from exposure to the trauma itself (Cocker & Joss, 2016).
In accordance, a study with child protection workers and in-home caregivers showed high levels of emotional exhaustion and depersonalization (19.4% and 22.7%, respectively) and 43.6% of the sample showed low levels of personal accomplishment. At the same time, 20.4% were at risk or already developing symptoms of burnout (Jenaro et al., 2007). With similar results, in a study developed with social workers, 33.2% presented emotional exhaustion, 22.1% depersonalization, and 54.2% low personal accomplishment (Gómez-García et al., 2020). High levels of burnout have also been found in midwives and social care workers (Borritz et al., 2006), nursing home caregivers (Kandelman et al., 2018), and frontline workers in homeless services (Waegemakers Schiff & Lane, 2019).
Community resilience, well-being, and community attachment
Community resilience refers to a community's ability to transform its environment after the occurrence of a negative event (e.g., natural disasters) through deliberate, collective action toward recovery. This process requires them to utilize local assets and work together to effectively deal with new-found adversity and to learn from that experience (Pfefferbaum et al., 2011). Community resilience emerges from the communities’ ability to deal with uncertainty and to organize their resources to better navigate complex crises (Sherrieb et al., 2012). In particular, this work's conceptual framing of community resilience follows the Communities Advancing Resilience Toolkit (CART; Pfefferbaum et al., 2016) which focuses on five domains to describe and promote community resilience: connection and caring, community resources, transformative potential, disaster management, and information and communication. Communities with higher levels of competence in these domains are expected to mitigate the unfavorable effects of disasters and adversities more effectively (Pfefferbaum et al., 2013). Community resilience has been widely explained and predicted using these dimensions, including in communities with different cultural backgrounds (e.g., de Deuge et al., 2020; Fenxia, 2022; Kim et al., 2023; Kinanthi et al., 2020; Pfefferbaum et al., 2016; Tavares et al., 2023). Therefore, CART's dimensions appear to be fundamental to explaining community resilience worldwide, as they encompass local and cultural aspects that appear to be translated into the relative importance that the communities assign to these five dimensions (Raich et al., 2017; Yang et al., 2020).
During the COVID-19 pandemic, HSWs had to reorganize and streamline the way they worked to protect and support their communities and ensure the continuity of services. Considering the undoubtedly close synergy between the communities they serve and HSWs, it could be expected that a community's level of resilience has an impact on the professionals working locally, even more so during a pandemic.
Community resilience is an ongoing process that starts before the crisis and can buffer its impact on the community and all its members (Annette, 2021), with HSWs being seen as part of the community in which they are so heavily involved. Consequently, these professionals often become the backbone of the community they work in, having a privileged central position and a wide network of contacts (with individuals and services), both before and during pandemics, and taking part in the common goal of reconstructing the previous functional dynamics.
The pandemic highlighted not only the importance of the HSWs’ role in the community but also of their well-being. Much like the general population, many HSWs had their work–life balance and social connections compromised, which are important well-being dimensions (Organisation for Economic Co-operation and Development [OECD], 2021). For that reason, the great challenges that this period brought and the work they had to develop at the communities’ frontlines put pressure on several dimensions: physical, psychological, and financial, in addition to occupational (Magruder et al., 2022).
At the same time, recent research is calling attention to the importance of studying how people identify with and attach to places, clearly distinguishing the place and the communities that live in them (Lima et al., 2022). Well-being is frequently considered in burnout research (e.g., Janosy & Anderson, 2021), but not community or place attachment, that is, the affective bonds established with the community. When it comes to HSWs, whose work is so closely linked to the community setting, community attachment should have a fundamental role. Despite the strain on social ties and decreased social interactions, due to isolation and social distancing measures created during the pandemic (Ma, 2021), the level of community attachment that existed before the pandemic emerged is expected to impact the level of burnout of HSWs during the crisis and in the recovery phase.
The present study
In addition to providing care, already overloaded HSWs have a vital role in delivering support and monitoring their communities’ needs (Pfefferbaum & North, 2020), which in turn can contribute to their previously reported high levels of burnout, especially during a stressful situation like the COVID-19 pandemic. However, to our knowledge, there are currently no studies (both national and internationally) exploring burnout in this population during this period. Additionally, the literature often mentions the importance of looking at context variables and not exclusively at individual characteristics because “employees do not just distress or burnout because of flaws in character, behavior, perception, or productivity. Rather, the context in which people labor may be responsible for much of the problem in employee health and burnout” (Peterson & Wilson, 2002, p. 16). To rectify these gaps, the aims of this study are to (1) analyze the prevalence of burnout in a sample of Portuguese HSWs during the COVID-19 pandemic; (2) analyze the role of community resilience as a predictor of their burnout; and (3) explore if HSWs’ SWB and community attachment could explain the relationship between community resilience and burnout. We expect that higher levels of community resilience will lead to higher HSWs’ well-being and higher attachment toward the community they serve, which will in turn serve as a buffer for their burnout.
Method
Data collection and participants
Participants were recruited in collaboration with the European Anti-Poverty Network, which shared a link to the online questionnaire with their partners. The researchers also disseminated it within their professional networks. Before responding, participants had to give their informed consent digitally, which included information about the study, its objectives, and how data would be handled anonymously and confidentially. Respondents were also informed that their participation was voluntary and that they could withdraw from the study at any moment (data and/or participation) if they so wished. Data were collected between August 2020 and January 2021, amid the COVID-19 pandemic.
Five hundred and ninety-eight Portuguese respondents were recruited to participate in this study. Participants were mostly female (91.2%) and married (64%), and their ages ranged from 22 to 70 years old (M = 41.45; SD = 9.22). Their areas of training were Social Work (40.8%), Psychology (22.3%), Sociocultural Animation (3.6%), Social Policy (3.1%), Sociology (8.6%), Law (0.3%), or other (21.4%). Regarding their educational level, 56.1% had completed a bachelor's degree or an equivalent degree and 42.7% had a postgraduate course (i.e., master's or a PhD degree). This percentage is consistent with Portuguese legislation, according to which a master's degree is mandatory for some professions (e.g., psychologists), while for others it is optional. Participants had, on average, 14.26 years of experience working in human services (SD = 8.82).
Measures
Burnout
The Oldenburg Burnout Inventory (Demerouti & Nachreiner, 1998; adapted to Portuguese by Sinval et al., 2019) is a questionnaire developed to assess burnout. The questionnaire includes 16 items, grouped into two subscales: exhaustion (e.g., “during my work, I often feel emotionally drained”) and disengagement (e.g., “lately, I tend to think less at work and do my job almost mechanically”). Response items were scored on a 5-point Likert-type scale, ranging from 1—Strongly Disagree to 5—Strongly Agree, with higher scores indicating a higher level of burnout, when accounting for the reverse-coded items. In this study, the scale showed good internal consistency values (α = .85 and α = .84 for the exhaustion and disengagement subscales, respectively).
Community resilience
The CART Assessment Survey is a theory-based evidence-informed questionnaire developed to assess community resilience. The extended version used in this study (Pfefferbaum et al., 2016) includes the 28 core community resilience items, grouped into five dimensions: connection and caring (e.g., “people in my community help each other”), resources (e.g., “people in my community know where to go to get things done”), transformative potential (e.g., “my community has priorities and sets goals for the future”), disaster management (e.g., “my community can provide emergency services during a disaster or community crisis”), and information and communication (e.g., “my community keeps people informed about issues that are important to them”), as well as three new items created for the COVID-19 pandemic (e.g., “my community tries to prevent public health crises”). Response items were scored on a 5-point Likert-like scale, ranging from 1—Strongly Disagree to 5—Strongly Agree. Higher scores indicate a higher level of community resilience. The CART was adapted and translated to Portuguese by Tavares and colleagues (2023). This version of the scale showed adequate to high internal consistency (ranging from α = .78 to α = .94), and the final model's fit was very good (NFI was higher than .90, CFI scores were higher than .95, and the RSMEA value was below .06).
Subjective well-being
Based on well-being indicators from the European Social Survey (e.g., Lima & Novo, 2006), two items were used to measure SWB, one of them relating to life satisfaction (“All things considered, these days, how satisfied are you with your life as a whole?”) and the other to happiness (“All things considered, how happy would you say you are?”). Response items were scored on a 10-point Likert-like scale, ranging between 1 (Extremely dissatisfied/Extremely unhappy) and 10 (Extremely satisfied/Extremely happy), respectively. High scores indicate a generally high level of SWB.
Community attachment
A measure of community attachment was created based on the concept of place attachment, which describes the emotional bond between a person and a place where they feel comfortable (Hernández et al., 2007). For the purpose of this study, this measure was adapted to assess how attached HSWs are to the communities they work in. Three items were used to measure attachment: “I enjoy working in this community,” “I feel connected to this community,” and “I would regret having to work in another community,” subsequently being aggregated in a composite measure with good internal consistency (α = .80). The response items varied between 1 (Not at all) and 5 (Really a lot), with higher scores indicating higher community attachment.
Sociodemographic and professional characteristics
To characterize the sample, participants were asked to answer questions regarding their sociodemographic characteristics (e.g., age, marital status, completed education). There were also questions aimed at understanding the participants’ professional context, such as current employment situation, working hours, work format, number of years spent working in human services, job role, target population, and average number of cases, among others. To assess if there had been changes in their professional lives due to COVID-19, a few questions addressed this situation specifically (e.g., “Was there a change in your vacation plan because of the pandemic?,” “Did you have to perform any work activities at home during the period of the state of emergency?”).
Results
Prevalence of burnout
Mean burnout results were significantly below the medium point of the scale (3.5), M = 2.78, SD = .60, t(582) = −30.43, p < .001, Cohen's d = −0.126. These results indicate average medium/low levels of burnout.
Nine percent of the sample of HSWs scored above 3.5 (8.9%, n = 55), indicating higher levels of burnout. In this subsample, most HSWs were women (90.4%), had a college degree (58%), were in a romantic relationship (63.5%), had children (60%), and had a mean age of 40.8 years old (SD = 7.95). Independent samples t-tests between the group of professionals with lower burnout (<3.5) and higher burnout (>3.5), equal variances between groups not assumed, did not illustrate any differences in these variables. Regarding the services they worked in, 28.8% worked with children and youth, 1.9% with mental health, 17.3% with addiction, 51.9% with the elderly, 15.4% with homeless people, 3.8% with HIV/AIDS, 15.4% with people with disabilities, and 30.8% in other social services. Independent samples t-tests (equal variances between groups not assumed) did not illustrate differences between these variables in the sample of individuals with low and high burnout. There was only one exception: individuals working in other social services had lower burnout levels (t(62.96) = 42.49, p = .043, Cohen's d = 0.284), but the effect size was small.
Bivariate correlations between burnout levels in the entire sample and sociodemographic variables showed, once again, that sex, schooling, marital status, and having children were not related to burnout. However, older age was strongly related to having lower levels of burnout (r = −.84, p = .044). We further explored burnout levels in the occupational areas of HSWs. Most participants worked in elderly services, other social services (suggesting a lack of specialization), and children and youth services (see Table 1). Working with children and youth services was the only social response that was meaningfully related to burnout. Those working in this area had lower levels of burnout. The other significant correlation, which was also negative, related to “other social services.” Interestingly, no positive correlations were found.
Correlations between burnout and social responses.
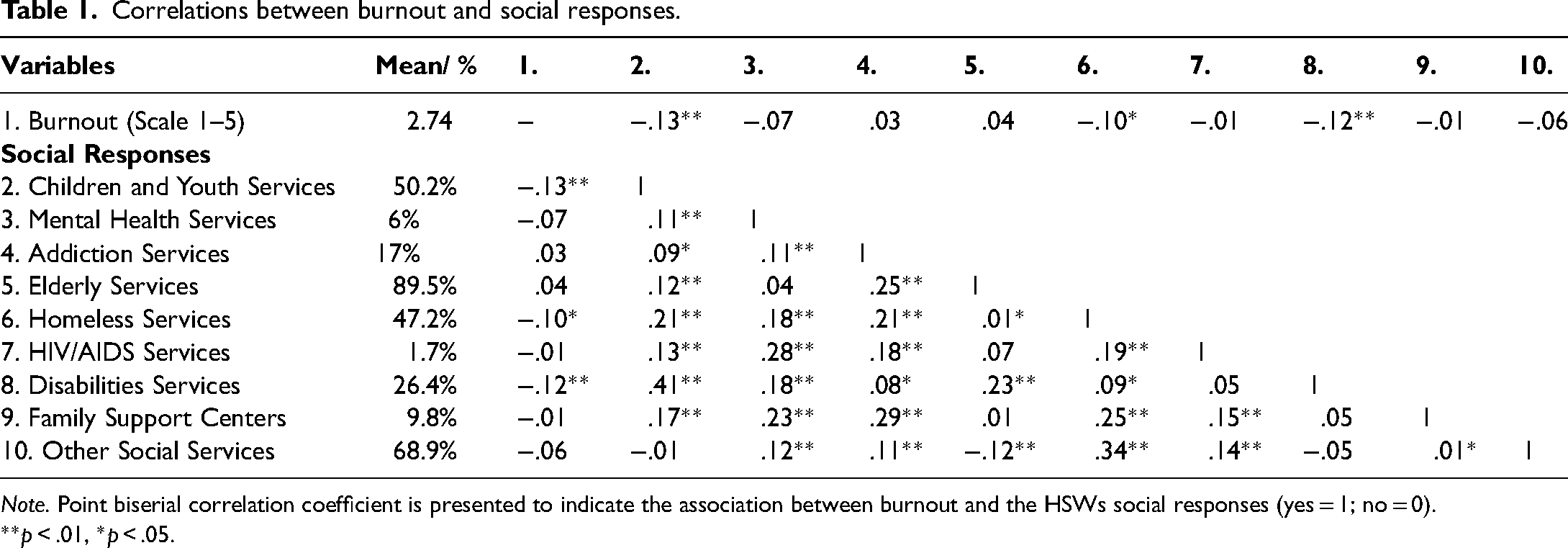
Note. Point biserial correlation coefficient is presented to indicate the association between burnout and the HSWs social responses (yes = 1; no = 0).
**p < .01, *p < .05.
When asked to compare their work situation and conditions before and after the pandemic, most participants reported changes in their workplace and schedule (61.1%). A substantial segment of people started working remotely, at least partially (46.8%), and suffered changes in their vacations, such as a reduction of vacation days or rescheduling (41%). Bivariate correlations between having or not experienced these changes and burnout levels showed that vacation changes were associated with higher burnout levels (r = .08, p = .047).
Relations between community resilience, well-being, and community attachment
Independent samples t-tests between the group of HSWs with lower burnout (<3.5) and higher burnout (>3.5), equal variances between groups not assumed, illustrated that those with lower scores of burnout perceived higher community resilience, t(58.44) = 4.00, p < .001, Cohen's d = .663, had much higher well-being, t(55.19) = 5.62, p < .001, Cohen's d = 1.168, and had much higher community attachment, t(60.18) = 7.15, p < .001, Cohen's d = 1.092.
Furthermore, the relationship between burnout, community resilience, SWB, and community attachment of the entire sample is presented in Table 2. As expected, burnout is negatively correlated with all variables, this being particularly true about community attachment and SWB. Since the results confirmed the expected associations between community resilience and burnout, as well as between these variables and SWB and community attachment, we proceeded to explore a parallel mediation model, testing if well-being and community attachment could both have an indirect effect on the relationship between community resilience and burnout. To test for mediation and conditional processes, we used the PROCESS macro for SPSS version 4.1 (Hayes, 2018), which is based on ordinary least square regression and path analysis. The number of bootstrap samples for percentile bootstrap confidence intervals was 5000.
Correlations between burnout, community resilience, subjective well-being, and community attachment.
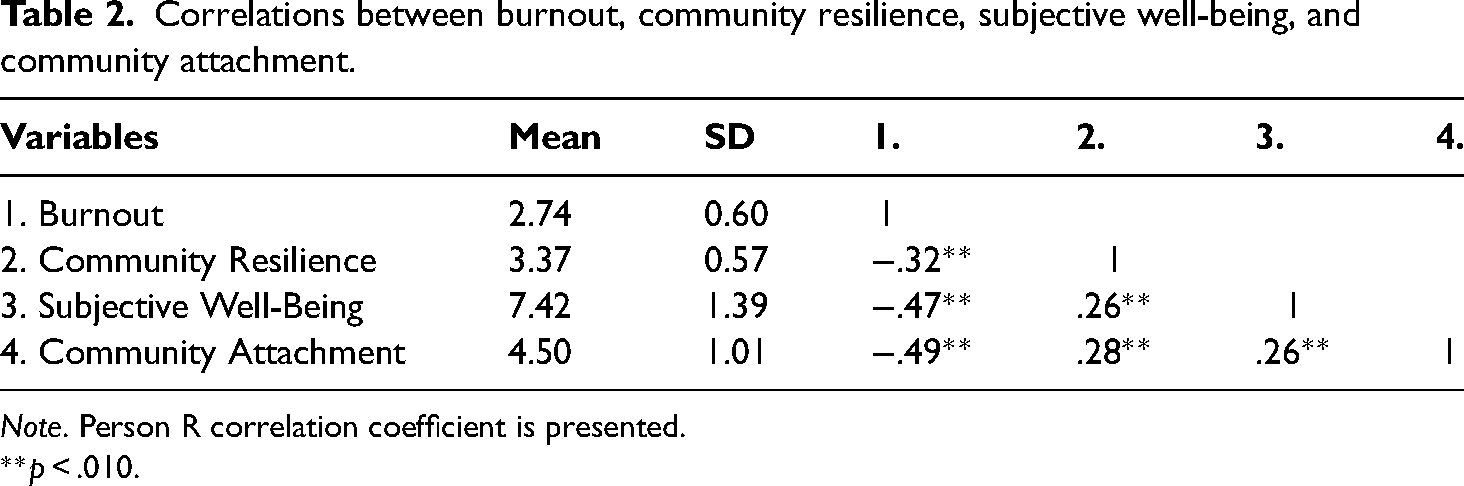
Note. Person R correlation coefficient is presented.
**p < .010.
The conceptual model and coefficients are presented in Figure 1. Community resilience was a negative predictor of burnout (b = −.34, p < .001) and a positive predictor of both SWB (b = .62, p < .001) and community attachment (b = .49, p < .001). SWB and community attachment were further negative predictors of burnout (b = −.15, p < .001; b = −.22, p < .001, respectively). The total indirect effect of the mediators was −.20, 95% CI [−.26, −.14]. Both specific indirect effects were significant. The indirect effect of community resilience on burnout via SWB was −.09, 95% CI [−.13, −.06], and the indirect effect of community resilience on burnout via community attachment was −10, 95% CI [−.15, −.07]. To summarize, community resilience had a significant direct effect on burnout and also an indirect effect, which was explained by SWB and community attachment.
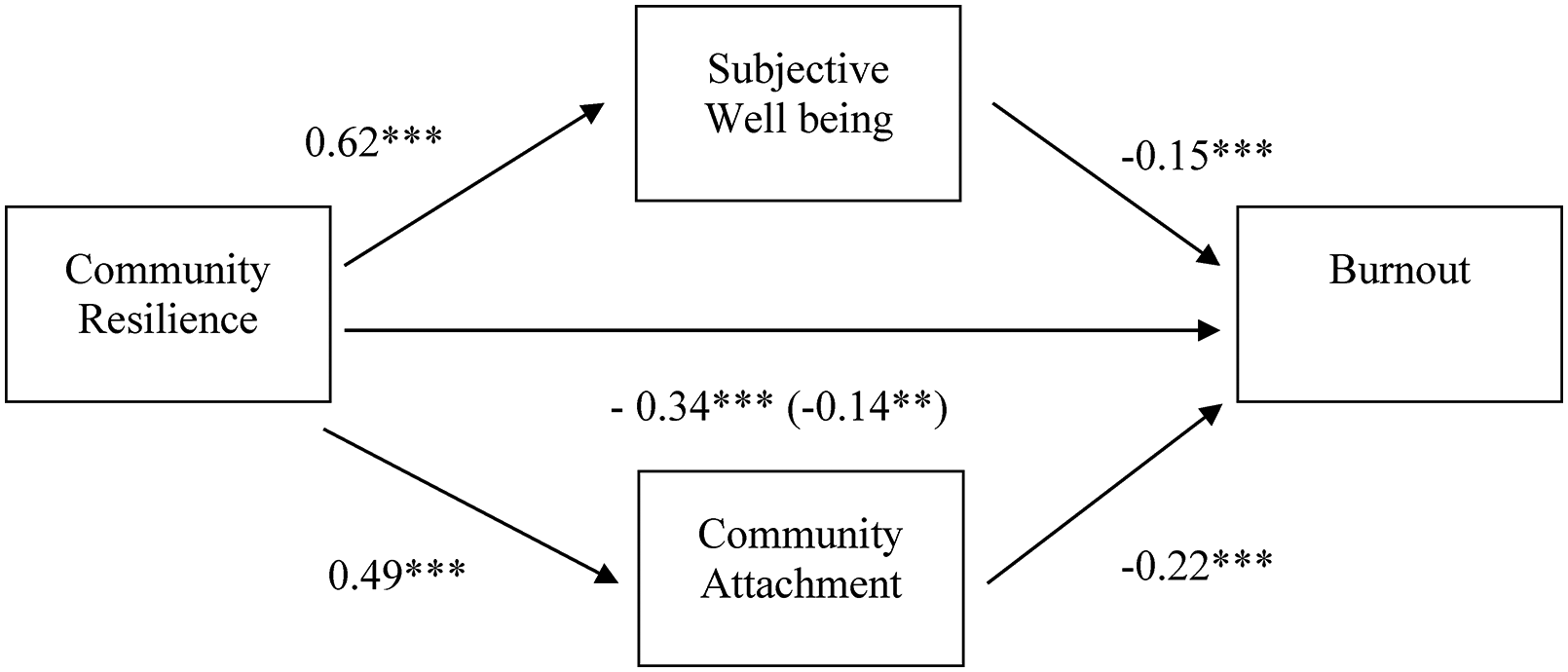
Parallel mediation model showing the relation between perceived community resilience and burnout as mediated by subjective well-being and community attachment. Regression coefficients are unstandardized and the one in brackets expresses the inclusion of the mediators. **p < .010, ***p < .001.
Discussion
The present study analyzes the prevalence of burnout among a varied sample of Portuguese HSWs during the COVID-19 pandemic, including social workers, psychologists, sociologists, social educators, and others. Additionally, it further analyzed the role of community resilience as a predictor of burnout and looked at whether the HSWs’ SWB and community attachment could explain the relationship between community resilience and burnout.
Despite the increased workload and personal risk (both mental and physical) for HSWs during the pandemic, many of them working on the frontlines (Magruder et al., 2022), our data shows low to moderate levels of burnout. This can be the result of compensation strategies used by professionals to buffer the impact of burnout symptoms on their performance, namely at the exhaustion level (Demerouti et al., 2014). It can also be explained by self-care activities acting as a well-being promoting factor in times of mounting stress, thus facilitating the way helpers connect with their users’ needs, while also fulfilling their own, which, in turn, will help reduce stress and prevent burnout (Hricová, 2019). Having said that, we did find that having their vacations changed during the emergency period was related to higher HSWs’ burnout levels, which could indicate that vacations matter when it comes to reducing burnout. Systematic reviews among physicians have indeed evidenced that having time off is a protective factor for well-being (McGrade et al., 2020) and good practice for reducing burnout (Kruse et al., 2022).
In terms of the sociodemographic variables, only age was related to burnout, with older individuals showing lower levels of burnout. Although the literature on this topic seems to be inconclusive, there is some evidence that older people develop more and better stress management strategies to deal with their work experiences (e.g., Tepperman & Curtis, 1995). If so, providing HSWs with training courses on stress-related coping strategies developed by older professionals with experience would be beneficial and effective.
The results also show that the HSW's level of burnout was, as expected, negatively associated with community resilience, as well as with SWB and community attachment. Not only could we identify a direct effect of community resilience on the HSW's burnout but also an indirect effect through SWB and community attachment. We propose that community resilience may act as an additional resource that supports these workers, helping them to reduce stress (Bakker & Demerouti, 2007). This appears to be quite relevant when considering that community resilience can be strengthened in many ways, thus improving the HSWs' and the communities’ well-being in case of collective crises. Namely, the existence of social capital (Niu et al., 2022), community engagement (Pfefferbaum et al., 2016), or even the development of coproduction strategies in the community to include the voice of the people as part of the process (Davis et al., 2021). It is well known that cultural dimensions can inform specific paths for community resilience, as they influence how people perceive, respond to, and define any crisis or risks (Nuryanti et al., 2022). For that reason, respecting community heritage and celebrating its specificities, by promoting the people's participation, can be utilized as a prevention strategy and be an important way to safeguard the resilience process as posted by the UN Agenda 2030 (Fabbricatti et al., 2020).
This is, as far as we know, the first Portuguese study to consider HSWs during the pandemic and, in particular, their levels of burnout. Another contribution is the fact that we explored the interaction between burnout and community-related variables. As previously suggested, community factors cannot be disregarded. This became particularly clear since the pandemic, which highlighted the interconnectedness that exists at the individual, family, and community levels. Human service workers had to find new ways of intervening and making their professional networks function—creating or strengthening ties between different social, health, and/or education services while following lockdown and social distancing rules. The well-being, burnout, and community engagement of these professionals, as well as the level of community resilience within the setting they work in, are key factors in the mental health and work outcomes of HSWs. Looking at these factors, as was done in this study, allowed for a deeper understanding of the HSW's complex reality and needs.
Limitations of the study
As is always the case, further work is required to complement our findings. Data provided by the HSWs’ organizations and the community members they work with could provide invaluable information, leading to a more detailed and comprehensive understanding of a complex framework. Consequently, this would result in a more robust analysis, integrating the individual, organizational, and community levels, and exploring the relationship between these dimensions, in an ecological, systemic, and holistic approach. Considering cultural dimensions in the future could also help deepen our understanding of the impact that Portuguese cultural specificities have in the collective response to adversity, when compared with other cultures/countries. Collecting longitudinal data would also allow for a better understanding of how burnout occurs and develops in this population, bringing at the same time insight into how these professionals adapt in the pandemic recovery period. Finally, future studies could include interviews with these professionals to explore individual differences, needs, and coping strategies, which could then inform burnout reduction and well-being promoting interventions.
Footnotes
Ethical Approval
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Informed consent to participate in this study was provided by the participants.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Portuguese national funds through FCT (Fundação para a Ciência e a Tecnologia) under the grants UIDP/00713/2021 and UIDB/05380/2020. FCT had no involvement in the study design, in the collection, analysis, and interpretation of data, in the writing of the paper nor in the decision to submit the paper for publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Authors Contribution
All authors contributed to the study's conception and design. Material preparation and data collection were performed by SG, CR, SL, and LT. Analysis was performed by SL and JH. The first draft of the manuscript was written by JH, SL, and CR and all authors contributed to writing and revising later versions of the manuscript. All authors read and approved the final manuscript.
Acknowledgements
The authors would like to kindly thank Sarah Stephenson and Matthew Breedlove for their assistance with grammar for this manuscript.
Consent to Participate
The respondents were informed beforehand and participated voluntarily in the study.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Code Availability
The code used will be shared on reasonable request to the corresponding author.