
Abstract
Background:
The impact of trauma on immigrants’ mental health is well-documented, but less is known about how pre- and post-migration trauma affects mental health within the context of family relationships.
Aims:
The objective of the study is to examine the role of family dynamics in shaping the association between trauma exposure and psychological distress among Latino immigrants in the U.S.
Methods:
This study is based on a sample of Latino immigrants (N = 1,569) from the National Latino and Asian American Study (NLAAS; 2002–2003). Moderation and mediation analyses were performed to test the associations between trauma exposure, family relationships, and psychological distress.
Results:
Both pre-migration trauma and post-migration trauma were significantly associated with greater levels of psychological distress. While family cohesion was not directly linked to distress, it moderated the impact of trauma exposure, with high family cohesion reducing distress from both pre-and post-migration trauma. Family conflict was not only directly associated with increased levels of distress but also mediated 35% of the relationship between post-migration trauma and distress (indirect effect = 0.458, p < .05, 95% CI [0.104, 0.812]). Furthermore, conflictual family relationships exacerbated the detrimental mental health impacts of both pre- and post-migration trauma.
Conclusion:
The mediating and moderating role of family relationships in the adverse mental health impacts of trauma exposure among Latino immigrants underscores the need for culturally tailored, family-centered interventions that enhance family bonds and manage conflicts to mitigate trauma-related psychological distress in this vulnerable population.
Introduction
Latinos represent one of the largest and fastest-growing immigrant groups in the U.S. (Moslimani & Lopez, 2023), bringing diverse cultural and sociopolitical backgrounds shaped by complex migration histories. Many face significant mental health challenges linked to traumatic experiences (Peña-Sullivan, 2020). Nationally representative data show that about half of the Latino immigrants endure trauma before arriving in the U.S. (Li, 2016; Sangalang et al., 2019), ranging from political violence and natural disasters to forced migration, with profound psychological and emotional impacts influencing acculturation (L. R. Fortuna et al., 2008; Li, 2016; Montgomery et al., 2014; Ornelas & Perreira, 2011; Perreira & Ornelas, 2013; Sangalang et al., 2019). Though the prevalence of post-migration trauma is relatively lower than that of pre-migration trauma, immigrants are not exempt from exposure to trauma during and after migration. Cleary et al. (2018) found that 59% of Latino immigrant youths reporting trauma experienced it in their home country, 20% during migration, and 18% after arriving in the U.S. Such exposures across the migration trajectory are strongly linked to PTSD, anxiety, and depression (Barton et al., 2021; Peña et al., 2017; Potochnick & Perreira, 2010).
Contemporary migration flows from Central and South America continue to be driven by displacement, political instability, violence, and poverty (Bueno & Müller, 2025; Noe-Bustamante et al., 2020). Simultaneously, restrictive immigration policies—including heightened enforcement, family separations, and deterrence-oriented border programs—exacerbate systemic stressors for immigrant families. Recent shifts, such as changes to humanitarian-parole pathways and proposals like the “One Big Beautiful Bill” in 2025, have been flagged as threats to immigrant health, family stability, and psychological well-being (L. Fortuna et al., 2025; Hill et al., 2023). Evidence syntheses confirm that hostile post-migration environments are associated with heightened anxiety, depression, and trauma symptoms among asylum seekers and other migrants (L. Fortuna et al., 2025; Navarro Flores et al., 2023). Situating the present study in this sociopolitical climate calls for a closer examination of how pre- and post-migration trauma intersect with family dynamics to shape mental health among Latino immigrants.
Immigrant health research increasingly emphasizes the role of structural forces in shaping psychological well-being. In the current U.S. climate, immigration policy functions not only as a legal regulation but also as a source of chronic stressors that fuel instability and fear for immigrant families (L. Fortuna et al., 2025). Yet while the mental health consequences of trauma are well documented, less is known about how the timing of trauma—pre-and post-migration—interacts with family processes to influence distress. Post-migration trauma, in particular, is often conflated with acculturative stressors such as language barriers, discrimination, or financial strain, potentially obscuring its distinct effects (Barton et al., 2021; Hynie, 2018; Ornelas & Perreira, 2011).
One possible mechanism by which traumatic exposure affects mental health in Latino immigrants is by depleting crucial social resources, particularly within family relationships. While families are often seen as sources of resilience and support during times of stress, severe stressors such as trauma can place considerable strain on family bonds. Studies have shown that trauma impacts not only individuals but also family dynamics, affecting parenting, cohesion, and children’s development (Anakwenze & Rasmussen, 2021; Bryant et al., 2018; Perreira & Ornelas, 2013; Solheim et al., 2016). Latino families, with their cultural emphasis on familismo—family cohesion and support—face unique challenges and sources of resilience when confronting trauma (Priest & Denton, 2012; Priest & Woods, 2015).
In this study, pre-migration trauma refers to exposures before immigration, and post-migration trauma refers to events during migration or after settlement (e.g. political violence, detention, disasters, serious accidents). Using the National Latino and Asian American Study (NLAAS), which records the timing of trauma, we are able to distinguish between these exposures. Integrating perspectives from the biobehavioral family model and the stress process theory, this study examines the interrelationships between trauma exposure, family functioning (cohesion and conflict), and the mental health of Latino immigrants. Using a representative U.S.-based sample of Latino immigrants, it addresses two questions: (1) How are pre- and post-migration trauma linked to psychological distress? (2) How do family dynamics moderate or mediate the mental health impacts of trauma exposure? By examining these dynamics, this research provides insights into the resilience and vulnerabilities in Latino families, informing tailored support and intervention strategies.
Social and Interpersonal Mechanisms in Trauma and Mental Health
Social support is a key protective factor against mental health challenges, offering emotional comfort and coping resources, especially within the Latino immigrant community (Ornelas & Perreira, 2011; Potochnick & Perreira, 2010; Priest & Denton, 2012). However, stressors like trauma exposure often deplete social resources by weakening social networks and intensifying feelings of isolation and alienation (Beck et al., 2009; Brewin et al., 2000). Trauma also strains family relationships by triggering stress responses in family members, leading to disrupted communication, shifting roles, and heightened conflict (Muldoon et al., 2019). Trauma survivors may develop insecure attachment styles, such as avoidant attachment, which further hinder their ability to form healthy relationships (Mikulincer & Shaver, 2007).
Latino families may also face “vicarious trauma,” where family members indirectly experience one another’s traumatic events (Goff et al., 2020; Molnar et al., 2017). This creates a cycle of stress as members share burdens and worry over one another’s well-being. Research by Punamäki et al. (2017) found that families with insecure or negative relationships exhibit greater trauma-related stress, underscoring how trauma ripples through the family unit.
Family Relationships and Mental Health: The Biobehavioral Family Model
Family relationships can either protect against or exacerbate health risks, depending on the quality of interaction (Carr & Springer, 2010; Woods et al., 2014). The Biobehavioral Family Model (BBFM; Priest & Woods, 2015) highlights the role of family emotional climate (FEC), often measured as a family function, in shaping health outcomes. A negative FEC characterized by strain, hostility, and conflict is linked to emotional dysregulation and psychological challenges, while a positive FEC characterized by support, respect, and warmth buffers stress and supports mental well-being (Priest & Denton, 2012; Woods et al., 2014).
Family relationships, however, rarely fall neatly at one end of this spectrum, as they are complex and have a mixture of both supportive and stressful elements. This complexity is particularly relevant when exploring the health effects of family relationships, as both positive and negative aspects of the relationship can uniquely influence mental health outcomes in Latino families (Priest & Denton, 2012; Priest & Woods, 2015; Rivera et al., 2008; Ross et al., 2019).
Trauma, Family Relationships, and Mental Health
BBFM provides a theoretical framework for understanding how family relationships affect mental health outcomes. Complementing BBFM, the stress process theory (Pearlin & Bierman, 2013) highlights the interconnected nature of a traumatic stressor, family dynamics, and mental health. Specifically, the stress proliferation hypothesis suggests that primary stressors, such as trauma exposure, can lead to secondary stressors like a family strain that amplify the psychological impact of the original trauma (Pearlin et al., 1997).
For Latino immigrants, family relationships are crucial sources of resilience and coping mechanisms, yet they can also be undermined by external stressors like discrimination, disorderly neighborhood conditions, and legal uncertainties (Kwon, 2020; Molina et al., 2016; Ornelas & Perreira, 2011; Zayas et al., 2015). Family separations due to immigration enforcement or financial strain can cause significant emotional distress and anxiety, challenging the cultural value of familismo (Zayas et al., 2015). Both pre-and post-migration traumas introduce stress that can strain family dynamics, often producing intergenerational impacts on mental health and chronic illness. Reese et al. (2022), for example, found that parental trauma was directly associated with greater adverse family experiences for their children, illustrating how trauma propagates across generations and affects family well-being. In light of these insights, this study hypothesizes that trauma exposure disrupts family relationships, which in turn increases the risk of psychological distress among Latino immigrants (H1).
The stress-exacerbating hypothesis suggests that strained family relationships amplify the psychological toll of trauma, increasing susceptibility to anxiety, depression, and physical health issues (Kwon, 2020; Mohanty et al., 2022; Priest & Woods, 2015). Thus, we further hypothesize that negative family relationships strengthen the link between trauma and psychological distress (H2).
In contrast, supportive family environments help individuals recover from trauma-related stress, lowering the risk of developing mental health issues such as depression and PTSD (Calhoun et al., 2022; Cohen & Wills, 1985; Thoits, 1982). This buffering effect is particularly notable for Latino immigrants, who often rely on family as a central source of social and emotional support. Strong family bonds can shield Latino immigrants and their children from experiencing trauma-related symptoms after migration (Masten & Narayan, 2012; Perreira & Ornelas, 2013). Accordingly, we hypothesize that positive family relationships buffer the negative impact of trauma on psychological distress (H3).
Methods
Data and Sample
The data for this study is drawn from the 2002 to 2003 National Latino and Asian American Study (NLAAS), a nationally representative household survey of Latino and Asian Americans based on a stratified area probability sample (Alegria et al., 2004; Heeringa et al., 2004). The NLAAS employed a three-stage sampling method, selecting primary sampling units with probabilities proportional to size. Data were collected by trained bilingual interviewers and aggregated by the University of Michigan’s Institute for Social Research (ISR). Details of this process have been described elsewhere (Alegria et al., 2004; Pennell et al., 2004). The analytic sample for this study includes 2,554 Latinos from four subgroups: 577 Cuban, 495 Puerto Rican, 868 Mexican, and 614 from other Latino backgrounds (e.g., Costa Rican, Ecuadoran, Guatemalan, Honduran). Interviews were conducted in Spanish for respondents who preferred it, and the final weighted response rate for the Latino sample was 75.5%. The present study focuses its analysis on 1,569 Latino immigrant adults born outside the United States, after excluding missing cases (3.74%), comprising 484 Cubans, 202 Puerto Ricans, 467 Mexicans, and 416 other Latinos. Weighted descriptive statistics of the variables included in the analyses are reported in Table 1.
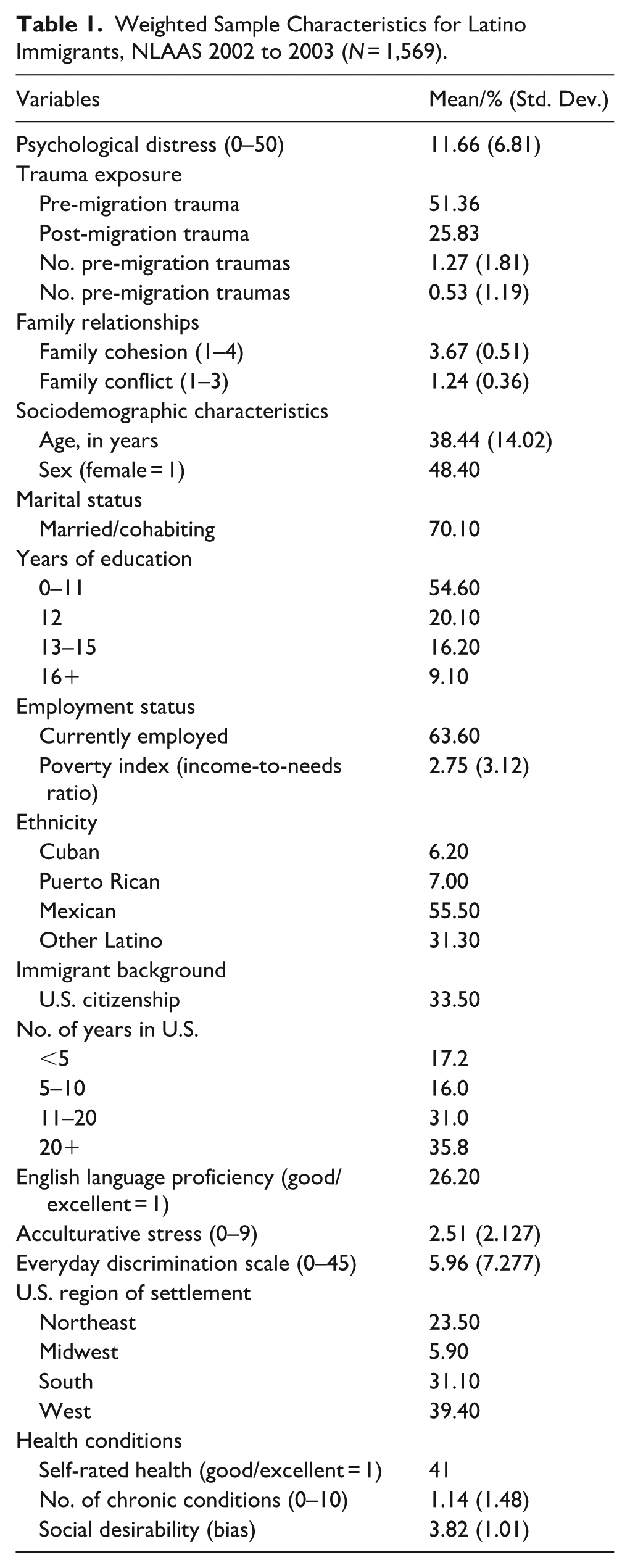
Weighted Sample Characteristics for Latino Immigrants, NLAAS 2002 to 2003 (N = 1,569).
Measures
Pre-migration trauma exposure was assessed using the WHO-CIDI trauma questionnaire from the Posttraumatic Stress Diagnostic Scale (PDS) in the NLAAS. Participants reported on 25 events (e.g. combat, refugee status, kidnapping, physical and sexual assault, disasters, domestic violence, life-threatening illness or accidents, and witnessing atrocities). Pre-migration trauma was coded as 1 for trauma experienced before moving to the U.S. and 0 otherwise. Post-migration trauma was similarly coded for events after immigration.
Family cohesion was measured with three items on closeness (e.g. “Family members enjoy spending free time together”), rated 1 to 4 (1 = strongly disagree, 4 = strongly agree; α = .93). Family conflict was assessed with five items from the Hispanic Stress Inventory (HSI; e.g. “Have your personal goals conflicted with your family’s expectations?”; Cervantes et al., 1991), rated 1 to 3 (1 = hardly ever or never, 3 = often; α = .76). Mean scores were calculated for both scales.
Psychological distress was measured with the 10-item Kessler Psychological Distress Scale (Kessler et al., 1998), assessing past-30-day distress (e.g. “How often did you feel depressed?”), rated 1 to 5 (1 = none of the time, 5 = all of the time). Total scores range from 10 to 50 (α = .91).
Covariates
Four sets of covariates were included. Socio-demographics included gender (female = 1, male = 0), age, employment (employed = 1, otherwise = 0), education (years completed), poverty index (Census 2001 income-to-needs ratio), region of residence, and Latino ethnicity. Immigration factors included citizenship (U.S. citizen = 1, otherwise = 0), years in the U.S., English proficiency (excellent/very good/good = 1, fair/poor = 0), and acculturative stress (sum of nine items, α = .70). Perceived discrimination was measured by summing responses to nine items on a 6-point scale (0 = never, 5 = almost every day; α = .91).
Health conditions included the number of lifetime chronic conditions and self-rated health status (1 = excellent/very good/good, 0 = fair/poor). Chronic conditions assessed were arthritis, chronic pain, seasonal allergies, stroke, heart disease, high blood pressure, asthma, diabetes, ulcers, epilepsy, and cancer. Social desirability was measured using the 10-item Crowne–Marlowe scale (e.g. “I have never lost anything”), with higher scores indicating a tendency for socially desirable responses (Crowne & Marlowe, 1960).
Analytic Strategy
Multivariate regressions tested associations of trauma and family relationships with distress, controlling for covariates. Initial models assessed the impact of trauma exposure on distress, controlling for all covariates. Subsequent models included family relationship variables to test their roles. Due to moderate correlations between family cohesion and conflict (r = .441, p < .001), separate analyses were conducted to minimize multicollinearity. Mediation analyses tested whether family relationships mediated the link between trauma and distress with a bootstrapping procedure (MacKinnon, 2008), while interaction terms assessed whether relationship quality buffered or intensified mental health impacts of trauma exposure. Family relationship measures were mean-centered to address potential collinearity in the models with interaction terms (Aiken et al., 1991).
All analyses applied sampling weights to adjust for the multistage, non-random selection of respondents, ensuring that results accurately reflect the target population. Analyses were conducted using Stata 18.0 (Stata Press, 2019).
Results
Table 1 presents summary statistics for the variables in the analysis, based on the weighted sample. Approximately half of the respondents experienced pre-migration trauma and one-quarter post-migration trauma. Overall, immigrants reported a high level of family cohesion, with a mean score of 3.67 (SD = 0.51), and low levels of family conflict, with a mean score of 1.24 (SD = 0.36). Additionally, the sample had an average Kessler Psychological Distress score of 11.66.
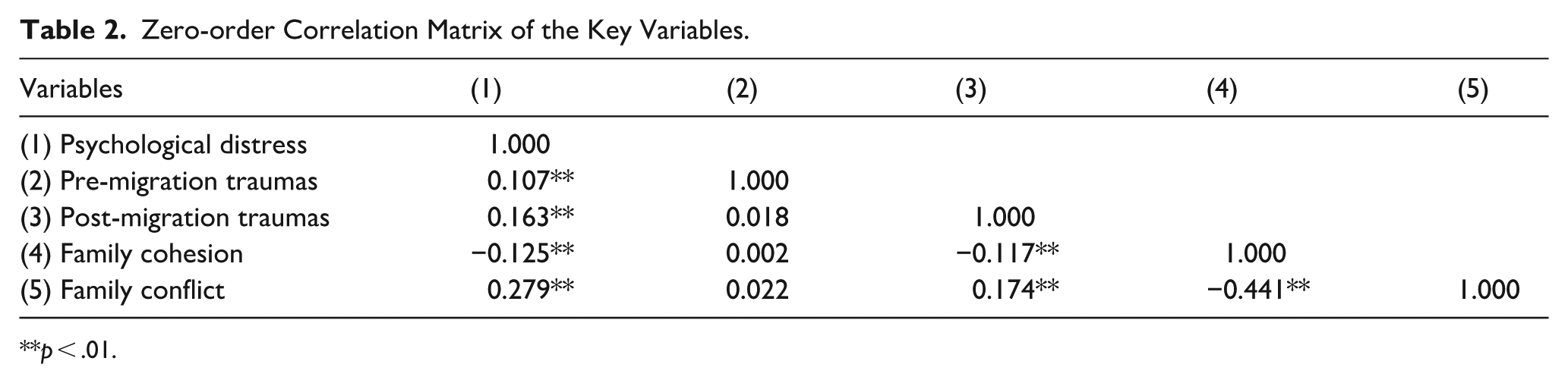
In the multivariate analyses, binary measures of pre- and post-migration trauma were used to focus on trauma exposure itself rather than the number of events. For illustrative purposes (Table 2), continuous measures of trauma exposure were used to calculate Pearson correlations among key variables. Results showed significant positive correlations between psychological distress and both pre- and post-migration trauma. Family conflict was positively correlated with distress, while family cohesion was negatively correlated. Pre-migration trauma was not significantly associated with family cohesion or conflict, whereas post-migration trauma was negatively correlated with family cohesion and positively correlated with family conflict.
Zero-order Correlation Matrix of the Key Variables.
p < .01.
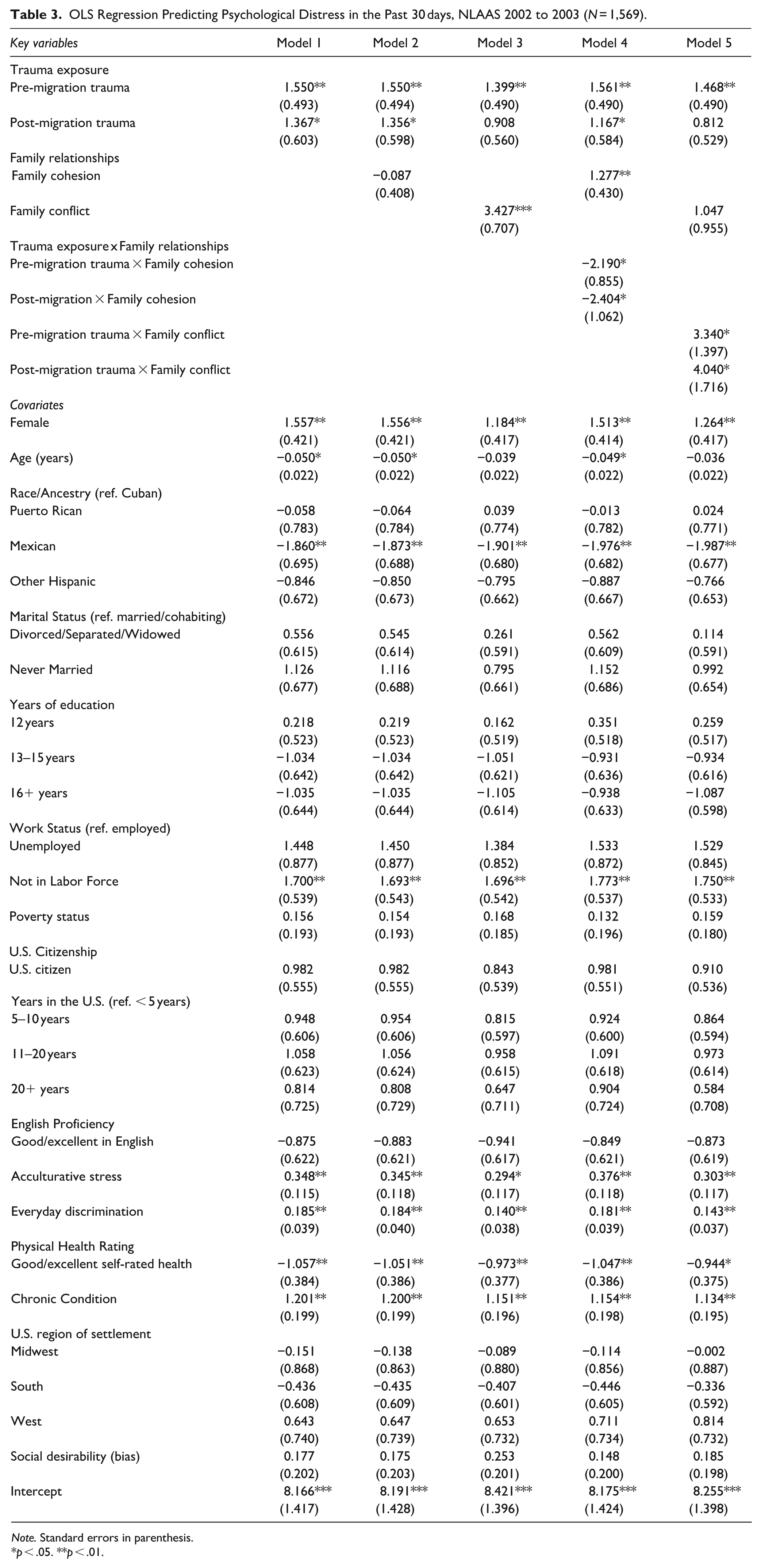
Table 3 presents the results of the multivariate regression models examining the effects of trauma exposure (both pre- and post-migration) and family relationships (family cohesion and family conflict) on psychological distress among Latino immigrants. In Model 1, both pre-migration trauma (b = 1.550, p < .01) and post-migration trauma (b = 1.367, p < .05) were positively associated with psychological distress. Adding family cohesion (Model 2) did not alter trauma effects. In contrast, family conflict, introduced in Model 4, had a significant positive association with psychological distress (b = 3.427, p < .001). Notably, adding family conflict in Model 3 reduced the effects of pre-migration trauma by 9.7% and post-migration trauma by 33.5%. Family conflict significantly mediated the relationship between post-migration trauma and distress, with an indirect effect of 0.458 (p < .05, 95% CI [0.104, 0.812]. No significant mediating effect was found for family cohesion.
OLS Regression Predicting Psychological Distress in the Past 30 days, NLAAS 2002 to 2003 (N = 1,569).
Note. Standard errors in parenthesis.
p < .05. **p < .01.
Several covariates were also significant (Table 3). Distress was higher among women, younger adults, those not in the labor force, and respondents reporting greater acculturative stress, discrimination, poorer health, or more chronic conditions. Mexican immigrants reported lower distress than Cubans, while Puerto Ricans and other subgroups did not differ. Education and citizenship were nonsignificant.
In Models 4 and 5, interactions tested moderation effects. The interaction between pre-migration trauma and family cohesion was significant (b = −2.190, p < .05), and a similar pattern was observed for post-migration trauma and family cohesion (b = −2.404, p < .05). As shown in Model 5 (Table 3), the interactions between pre-migration trauma and family conflict (b = 3.340, p < .05), as well as post-migration trauma and family conflict (b = 4.040, p < .05), were both significant. Figure 1 illustrates how family cohesion and family conflict moderate the associations between mental distress and both pre- and post-migration trauma. For example, Panel A in Figure 1 depicts that among individuals with low family cohesion (2 SD below the mean), those exposed to pre-migration trauma have higher levels of psychological distress compared to those with no pre-migration trauma (16.75 vs. 10.29). For individuals with high family cohesion (2 SD above the mean), the pattern reverses, as illustrated in Panel B in Figure 1. Specifically, predicted levels of psychological distress are lower for those with post-migration trauma exposure (15.47) compared to those without (18.47). It should be noted that labeling low cohesion as 1 standard deviation below the mean and high cohesion as 1 standard deviation above the mean yields a consistent pattern.
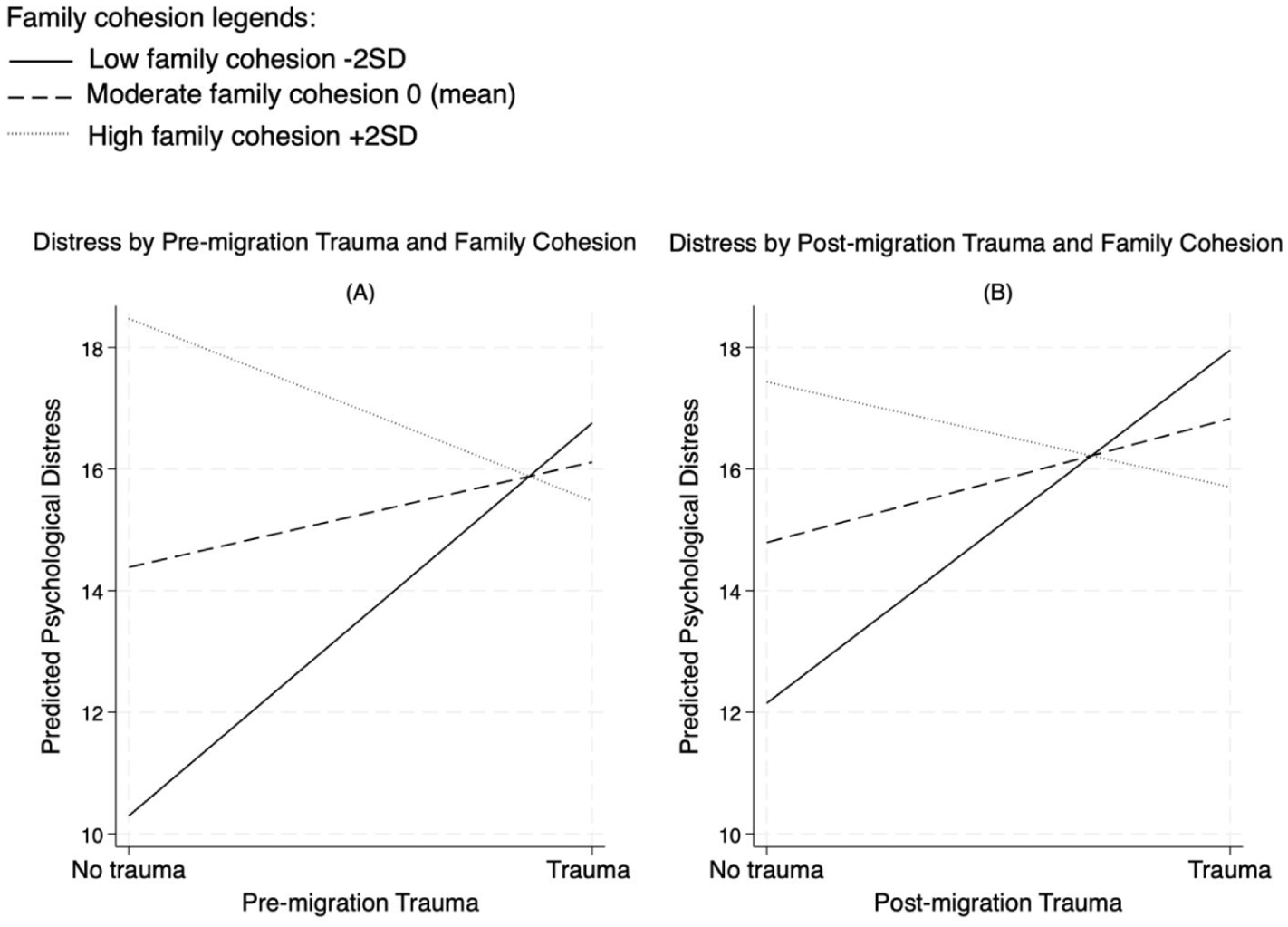
Buffering effects of family cohesion on trauma and psychological distress.
Regarding family conflict, Panel A in Figure 2 visualizes that for individuals with moderate family conflict (at the mean level), the difference in predicted levels of psychological distress between those with and without pre-migration trauma remains relatively small (14.15 vs. 15.72). However, for individuals experiencing high family conflict, the gap becomes much more pronounced. Those with pre-migration trauma report substantially higher distress levels (21.84) than those with no pre-migration trauma (16.11). These patterns become even more pronounced when examining the moderating effects of relationship quality on post-migration trauma, as illustrated in Panel B of Figure 2.
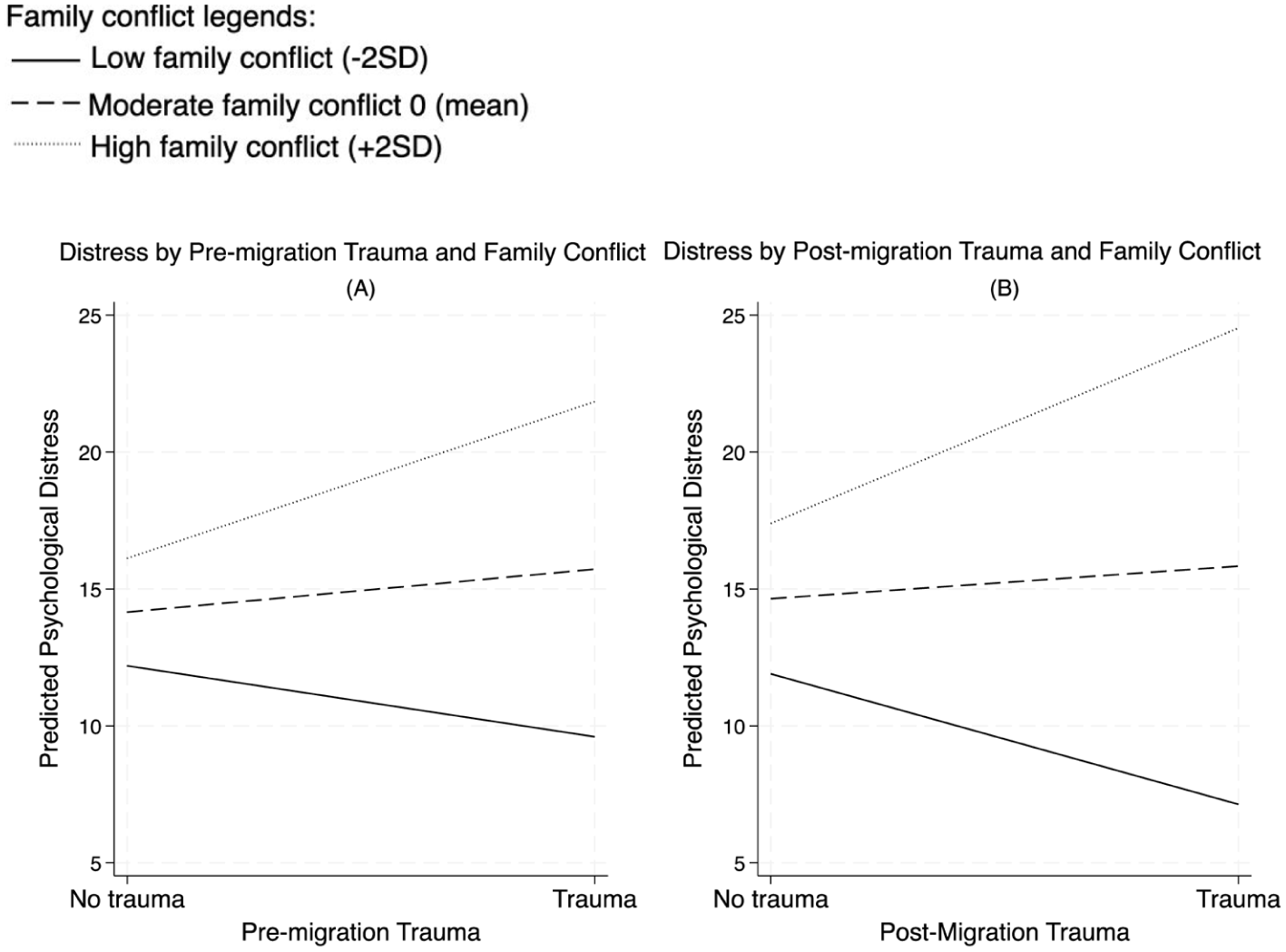
Exacerbating effects of family conflict on trauma and psychological distress.
Sensitivity Analyses and Subgroup Heterogeneity
To evaluate the robustness of the findings, we added measures of past-year and lifetime psychiatric disorder, perceived social support, and a coping proxy (religious comfort-seeking). We also conducted analyses excluding those with a past-year psychiatric diagnosis. These additions did not change the substantive conclusions (Tables S1–S3). While psychiatric history was consistently associated with higher distress, the buffering role of family cohesion and the exacerbating role of family conflict remained stable across all model specifications.
To explore variation across key demographic subgroups, we estimated models stratified by gender and age. Stratified analyses showed the overall pattern held across genders, with the exception that the trauma × family cohesion interaction was not significant among men. However, three-way terms involving gender were null, indicating no robust gender difference. Age-stratified models suggested that moderation was statistically evident in the youngest group, while effects in middle and older groups were directionally similar but less precise. Given reduced power for stratified interaction models and the exploratory nature of these tests, subgroup analyses were interpreted cautiously. Pooled covariate-adjusted results reflect population-average moderation.
Discussion
Our findings contribute to ongoing discussions about structural determinants and family systems in immigrant health, showing that the mental-health consequences of trauma are shaped by family emotional climate as well as individual risk. This study examined the effects of pre- and post-migration trauma on psychological distress among Latino immigrants, with a focus on the mediating and moderating role of family relationships. The results align with stress process theory and the Biobehavioral Family Model (BBFM).
Both pre-and post-migration trauma increase the risk of psychological distress, consistent with prior research (Li & Anderson, 2016; Sangalang et al., 2019). However, in the full model only pre-migration trauma remained significant, while post-migration trauma was not. One plausible explanation is that severe exposures such as war, political repression, and cartel threats may leave durable psychological scars that erode resilience long after resettlement (Theisen-Womersley, 2021). Traumas rooted in home-country contexts may also carry deeper emotional weight than those experienced post-migration. In today’s climate of continued displacement from Central and South America—driven by violence, instability, and economic crisis—the salience of premigration histories is likely even greater (Bueno & Müller, 2025; Isacson, 2022; Noe-Bustamante et al., 2020). These findings highlight the clinical need to screen for premigration trauma early in care. Future research should disaggregate trauma type, severity, and chronicity to clarify mechanisms and inform tailored interventions.
Family conflict was both a direct predictor and mediator of distress, indicating that conflict reflects and reinforces the burden of trauma in the post-migration context. Stressors such as acculturative strain, financial hardship, and shifting roles may exacerbate tensions or create new conflicts, making them plausible pathways through which trauma translates into distress. By contrast, pre-migration trauma might be internalized differently, with its effects more independently rooted in the individual’s experience (Sangalang et al., 2019; Theisen-Womersley, 2021). Although our data are historical, this mechanism arguably remains salient in today’s policy climate, where deterrence-oriented programs, parole restrictions, and enforcement create legal precarity, separations, and chronic uncertainty (Hill et al., 2023). These conditions heighten role strain, disrupt caregiving, and may suppress help-seeking out of fear, thereby amplifying stress proliferation (Pearlin et al., 1997). In such environments, conflictual family climates magnify trauma’s effects, while cohesion may be difficult to sustain without structural supports. This interpretation echoes prior work showing that family conflict exacerbates, and supportive relationships buffer, the impact of stress (Kwon, 2020; Priest & Woods, 2015).
Aligned with the stress-buffering hypothesis (Cohen & Wills, 1985; Thoits, 1982) and the BBFM, family cohesion buffered the adverse effects of trauma. Similar findings have shown that cohesion reduced trauma’s impact among immigrant youth (Barton et al., 2021) and that social support buffers migration-related stressors for Latino adolescents(Ornelas & Perreira, 2011). These findings highlight the dual role of family as protective and stress-inducing, and reinforce calls to move beyond individualistic approaches by incorporating family-level processes in immigrant mental health (Slobodin & de Jong, 2015).
Covariates also showed meaningful associations. Women and younger adults reported higher distress, consistent with demographic vulnerabilities. Mexican immigrants reported lower distress compared to Cubans, echoing subgroup differences noted in national surveys (Alegria et al., 2004; Rojas et al., 2021), while Puerto Rican and other subgroups showed no differences. Discrimination, acculturative stress, poor self-rated health, and chronic conditions were positively associated with distress, reinforcing the multifaceted burden of structural and health-related stressors on immigrant well-being (Alegria et al., 2004; Kwon, 2020; Molina et al., 2016). These results highlight the need to address both social and health determinants when considering pathways of distress among Latino immigrants.
This study has several limitations. The cross-sectional design precludes causal inferences about the relationships among trauma, family dynamics, and mental health outcomes. The mediation results should be interpreted as statistical indirect associations rather than causal mechanisms. While these findings point to possible pathways linking trauma, family conflict, and distress, longitudinal studies are needed to establish temporal ordering. Although past-year and lifetime psychiatric diagnoses were included in sensitivity analyses—and results were unchanged—they do not establish temporal precedence over past-30-day distress. Thus, “prior” psychiatric history should be interpreted cautiously. Likewise, the NLAAS lacks a standardized coping inventory; our coping proxy (religious comfort-seeking) may not capture the breadth of coping strategies. While the sensitivity analyses reassure that our main findings are robust, the absence of validated coping measures and time-anchored psychiatric history remains a limitation.
We also note limitations related to subgroup heterogeneity. Although age and gender were included as covariates in all models, we conducted exploratory stratified analyses to gage public-health–relevant variation. The overall pattern of findings was consistent across subgroups; moderation was significant in the youngest age group and generally consistent across gender, except that the pre-migration trauma × family cohesion interaction was not significant among men. However, three-way interaction tests were null, and stratified models were underpowered with wide confidence intervals. These subgroup patterns should therefore be interpreted cautiously and viewed as exploratory. Larger samples and designs specifically powered for subgroup moderation are needed to determine whether cohesion and conflict effects differ systematically by age or gender.
Additionally, the measures of psychological distress in this study are based on symptoms experienced in the past 30 days, which may not fully capture more severe or chronic mental health outcomes such as PTSD, depression, or anxiety. However, the focus on recent psychological distress was methodologically intentional, as it serves the purpose of testing the moderating and mediating roles of family relationships. Longitudinal designs in future research could further build on these findings to explore how more chronic mental health outcomes interact with family dynamics over time. Another limitation is that trauma exposure was operationalized as a binary variable (presence or absence) rather than a continuous measure that could account for the varying intensity or frequency of traumatic experiences. While this binary approach allowed for a clear and parsimonious analysis of the trauma-exposed versus non-trauma-exposed groups, it does not capture the nuanced effects of trauma severity. Future studies should use continuous or multidimensional trauma measures to better account for the heterogeneity of trauma experiences and their impact on mental health. Finally, while this study highlights the importance of understanding family dynamics in the mental health consequences of trauma, it is limited by its reliance on individual-level data rather than families as the units of analysis. Future research could benefit from incorporating family or dyadic-level data to capture family dynamics and the mental health consequences of trauma exposure.
Another limitation is the age of the dataset (2002–2003). As such, estimates may not reflect current prevalence or policy-specific exposures among contemporary Latino immigrants (e.g. recent changes in border enforcement or humanitarian pathways). Nevertheless, we view the core processes examined—linkages between trauma, family relationship quality, and psychological distress—as relatively stable mechanisms. What may differ across cohorts are the magnitude of effects and the distribution of exposures, shaped by shifting sociopolitical conditions. Replication with contemporary, longitudinal samples that explicitly capture policy context and cohort effects is therefore needed to assess generalizability and further situate family processes within today’s sociopolitical landscape.
Conclusions and Implications
This study advances understanding of how family conflict, cohesion, and trauma exposures jointly shape the mental health of Latino immigrants. By distinguishing pre- and post-migration trauma and identifying family dynamics as cross-cutting mechanisms, findings highlight intervention targets at individual, family, and structural levels. At the individual level, culturally adapted evidence-based treatments (e.g. trauma-focused CBT, narrative exposure therapy, interpersonal psychotherapy) can support immigrants with PTSD, depression, or anxiety (L. Fortuna et al., 2025). For severe premigration trauma, sequenced care beginning with stabilization should precede trauma processing, with brief family modules to strengthen cohesion and reduce conflict. For post-migration stressors, treatment should be paired with conflict management and acculturation support.
At the family level, targeting cohesion and conflict through BBFM-informed therapy, multi-family groups, or brief programs (e.g. WHO Problem Management Plus) offers scalable approaches. Delivering these services in primary care and community settings by bilingual/bicultural providers can enhance access and engagement. In addition, clinicians should routinely screen for both trauma history and family climate when working with Latino immigrants, while public health practitioners and community organizations can integrate family-centered behavioral health services into immigrant-serving clinics and community programs.
At the structural level, policies that prioritize family unity, expand legal stability, and strengthen anti-discrimination protections can mitigate distress (L. Fortuna et al., 2025). Expanding culturally and linguistically tailored services—including reimbursement for family therapy and interpreter services—is critical for equitable care.
In sum, care for pre-migration trauma should prioritize processing earlier exposures and rebuilding resilience, whereas interventions for post-migration trauma involve support systems to tackle migration adjustment challenges that strain the family environment. Pairing disorder-specific treatments with transdiagnostic, family-focused approaches offer a practical path to reducing distress and fostering resilience within the Latino immigrant community. Overall, the findings advocate for culturally tailored, family-centered interventions that enhance family bonds and manage conflicts and promote durable mental well-being of this community.
Supplemental Material
sj-docx-1-isp-10.1177_00207640251394881 – Supplemental material for Family as a Buffer or Burden: Trauma Exposure and Mental Health Among Latino Immigrants in the U.S
Supplemental material, sj-docx-1-isp-10.1177_00207640251394881 for Family as a Buffer or Burden: Trauma Exposure and Mental Health Among Latino Immigrants in the U.S by Soyoung Kwon, Timothy Oblad and Chethani M. Perera in International Journal of Social Psychiatry
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article. The National Latino and Asian American Study data collection was supported by the National Institute of Mental Health (NIMH; U01 MH062209 and U01 MH62207), with additional support from the Office of Behavioral and Social Sciences Research, the Substance Abuse and Mental Health Services Administration, and the Latino Research Program Project (P01 MH059876).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
This study utilized publicly available data from the National Latino and Asian American Study (NLAAS), 2002-2003. The dataset is accessible through the Inter-university Consortium for Political and Social Research (ICPSR) at the University of Michigan. Researchers can obtain the data by submitting a request through the ICPSR website: ![]() .
.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.