
Abstract
Background:
Currently, paradoxical findings exist regarding the level of functioning in individuals with Hikikomori (prolonged social withdrawal).
Aims:
This systematic review aimed to clarify the functioning, disability, and health of individuals with Hikikomori and their families in comparison to those without Hikikomori.
Method:
Relevant studies were searched from April 22 to 25, 2022, using MEDLINE, PsycINFO, Scopus, and two Japanese databases. Functions were categorized into ‘body functions”; “structure”; and “activity and participation’, which were further classified into subcategories.
Results:
Of the 8,181 studies screened, 24 studies with 1,769 individuals with Hikikomori were included. Twelve, three, and four indicators from six studies on depression and anxiety, three on addiction, and two on thought problem symptoms, respectively, were higher in the Hikikomori group than in the comparison group, with at least moderate effect sizes. Three indicators from three studies on interpersonal relationships were worse in the Hikikomori group, with at least moderate effect sizes. The meta-analyses showed that internalizing symptoms, externalizing symptoms, and thought disorders were significantly higher in the Hikikomori group than those in the comparison group with moderate-to-high effect sizes. Contrastingly, communication/interpersonal interactions were significantly lower in the Hikikomori group than those in the comparison group. No significant differences were observed in daily life/social life and the families’ communication/interpersonal interactions and relationship.
Conclusions:
The study limitations include a high risk of bias and heterogeneity. Overall, individuals with Hikikomori often have impaired mental and interpersonal interaction functions; thus, comorbidities of this condition should be carefully assessed.
PROSPERO: CRD42022320592.
Keywords
Introduction
Recently, Hikikomori, that is, prolonged social withdrawal or marked social isolation, has been added to the cultural concept of distress in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (American Psychiatric Association, 2022). Although no gold standard exists for defining it, Hikikomori is characterized by conditions such as not participating in school/work, not socializing outside one’s home, or staying home for most of the day, with all or some of these conditions persisting for a certain period (e.g. 6 months; Nonaka et al., 2022). Recently, definitions including the frequency of leaving home and significant functional impairment or distress have been proposed (Kato et al., 2019, 2020a), which were partially supported by a recent study (Nonaka & Sakai, 2023). A recent survey has reported the prevalence rates of Hikikomori to be 2.05% and 2.02% in the 15 to 39 and 40 to 64 year age groups, respectively (Japanese Cabinet Office, 2023). This phenomenon has been reported frequently in Japan (Nonaka & Sakai, 2022). However, it is not a Japanese culture-bound symptom. Furthermore, it has been reported in environments not only in Eastern countries such as those in Asia but also in Western countries such as European ones (American Psychiatric Association, 2022). Bowker et al. (2019) and Hamasaki et al. (2022) reported that hikikomori is not a culture-bound phenomenon and similar behavioral characteristics can be seen in other regions as well. However, more data is still needed to elucidate this phenomenon.
Although limited evidence is available, some studies have reviewed poor functioning in individuals with Hikikomori and their families, including mental function, social participation, interpersonal relationships, and family relationships (Funakoshi & Miyamoto, 2015; Kobayashi et al., 2003; Malagón-Amor et al., 2020; Ueda et al., 2004). Teo (2010) reported that Hikikomori cases showed characteristics such as disrupted family relationships, a sense of apathy, and a lack of desire and passion.
However, paradoxical findings exist regarding the psychological effects of Hikikomori. One report demonstrated that the longer the social withdrawal period was, the better the quality of life (QOL; Chan & Lo, 2014) was. Another study reported no significant correlation between Hikikomori duration and QOL (Nonaka & Sakai, 2014). Some studies have reported poor family functioning (Malagón-Amor et al., 2020), whereas others have reported different findings (Hata et al., 2004; Nonaka et al., 2019).
Thus, the level of functioning in individuals with Hikikomori and their families remains unclear. Furthermore, to date, no review has integrated existing knowledge about their functioning, which is crucial for understanding their treatment needs. Identifying the presence and extent of impairment is essential for developing psychiatric and psychosocial treatments. Consequently, this systematic review synthesizes data from the existing studies to clarify the level of functioning, disability, and health of individuals with Hikikomori and their families compared with non-Hikikomori patients. The International Classification of Functioning, Disability, and Health (ICF) is a comprehensive framework for understanding life functions; it defines functioning as including ‘body function’, ‘body structures’, and ‘activities and participation’ (World Health Organization, 2001). This review conducted exploratory research to determine whether lower functioning, including mental function and personality tendencies associated with hikikomori, could be found according to the ICF categories and subcategories.
Methods
Study design and participant selection
This study was pre-registered in PROSPERO (CRD42022320592) and was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines (Page et al., 2021).
Studies involving individuals with Hikikomori or their family members at the time of the study and those comparing functioning and disabilities between individuals with Hikikomori (or their families) and those without Hikikomori (or their families) were included. We also included studies: that mentioned the participants’ age and sex; with cross-sectional, case-control, cohort, or interventional study designs, including controls; that were peer-reviewed; and restricted to English or Japanese language. The following studies were excluded: (i) reviews, case series, or qualitative research designs and (ii) bulletin articles published by research institutions, such as universities. The included data were classified into a Hikikomori group (the group regarded as Hikikomori in the respective studies) including individuals with Hikikomori or their families, and a comparison group comprising non-Hikikomori individuals or their families. Individuals who had previously experienced Hikikomori but were not experiencing it at that time were categorized into the comparison group. We searched the electronic databases of MEDLINE, PsycINFO, and Scopus and two Japanese electronic databases (CiNii and ICHUSHI) from April 22 to April 25, 2022. The publication period was not restricted. The following search terms were used: ‘Hikikomori OR prolonged social withdrawal OR acute social withdrawal OR severe social withdrawal OR youth social withdrawal OR pathological social withdrawal OR primary social withdrawal’ in English, and ‘ひきこもり OR 引きこもり’ (‘Hikikomori’ with or without ‘Kanji’, respectively) in Japanese.
Data extraction
Two reviewers independently selected studies for the systematic review and extracted data by independently reviewing the full text; disagreements, if any, were resolved by a third party. Covidence software (https://app.covidence.org/) was used for study selection and recording. The following data were extracted: country where the study was conducted, definition and citation of Hikikomori, sample size, age of individuals with Hikikomori, sex ratio, and representative values (mean, median, or ratio) and standard deviations of the measures evaluating functioning and disability, medical diagnosis, and research design. The definition of Hikikomori was coded according to Nonaka et al. (2022).
Outcome measures
This study compared functioning and disability between the Hikikomori and non-Hikikomori cases according to the ICF, which consists of three categories: body function; structure; and activity and participation. Moreover, based on the World Health Organization (Geneva) classification (World Health Organization, 2001), the body function category was divided into the subcategories ‘mental functions’ and ‘temperament/personality’, while the activity and participation category was divided into subcategories communication/interpersonal interactions and relationship’ and daily life/social life’. We further classified the mental functions’ subcategory, which includes various psychiatric symptoms, into internalizing symptoms’, externalizing symptoms’, and thought disorder’ components (Caspi et al., 2014). Indicators not classified in these categories were considered as other categories’. In cases where the mean and standard deviation were reported but the between-group test statistic or p-value was not, the mean, standard deviation, and sample size were used to calculate the p-value in the analysis of individual indicators.
We integrated or selected data in the meta-analysis using the components following the listed procedures in Supplemental Appendix 1. In the meta-analysis, we excluded data of individuals who had previously experienced Hikikomori and those who were classified as having Hikikomori tendencies, such as high affinity (Watanabe et al., 2010). Nonaka et al. (2012) provided separate data of fathers and mothers; therefore, the data were integrated. Certain indices were reversed for the internalizing symptoms, externalizing symptoms, and thought disorder indices; therefore, the higher scores reflected lower functioning. In contrast, some of the communication/interpersonal interactions and relationship and daily/social life indices were reversed so that the higher scores reflected higher functioning.
Analysis
Statistical analyses were performed using SPSS version 27 (IBM) and R version 4.3 (R Core Team, 2023). Functioning comparisons between individuals with Hikikomori and non-Hikikomori individuals were made for indicators of each component. Effect sizes (Cohen’s d) and confidence intervals (CIs) were calculated for indicators for which previous studies provided means and standard deviations. Data from each literature study were tabulated and checked by the four authors to determine if they contained the necessary information to conduct the meta-analysis and check if each indicator was classified into the required categories of functioning and disability. We excluded FACES at Kwansein Gakuin-IV from the meta-analysis because it reflected family functioning in a quadratic curve and did not indicate that high (low) scores were high (low) functioning. The estimated average standardized mean difference (SMD) was calculated based on the random-effects model for the meta-analysis. The Q test and I2 index were used to identify statistical heterogeneity. Publication bias was investigated using failsafe numbers and funnel plot. Subgroup analyses were performed when the comparison group included clinical and non-clinical controls. Post-hoc sensitivity analyses were used to search the reasons for heterogeneity by sequentially excluding single studies.
Risk of bias assessment
The risk of bias (quality) was evaluated at the study level using the Joanna Briggs Institute Critical Appraisal Checklist (https://jbi.global/critical-appraisal-tools; Moola et al., 2020) for case-control studies. Two reviewers independently evaluated the risk of bias using the Covidence software. Furthermore, the certainty of evidence was evaluated based on the Grading of Recommendations, Assessment, Development and Evaluation (GRADE Working Group, 2004).
Results
Study selection
Tables 1 and 2 summarize the included studies and Table 3 provides the research locations and elements of the Hikikomori definitions. In total, 8,181 studies identified from the database were screened (Figure 1), of which 179 were assessed for eligibility. Of these, 154 were excluded, and one additional study (Hanashima & Kondo, 2007) was excluded for using a duplicate dataset. Finally, 24 studies were included in the review. Cohen’s Kappa for the ratings by the two independent reviewers was 0.75 or 0.55 for the title and abstract screening and 0.61 or 0.56 for the full-text review.
Summary of the studies included in the review.
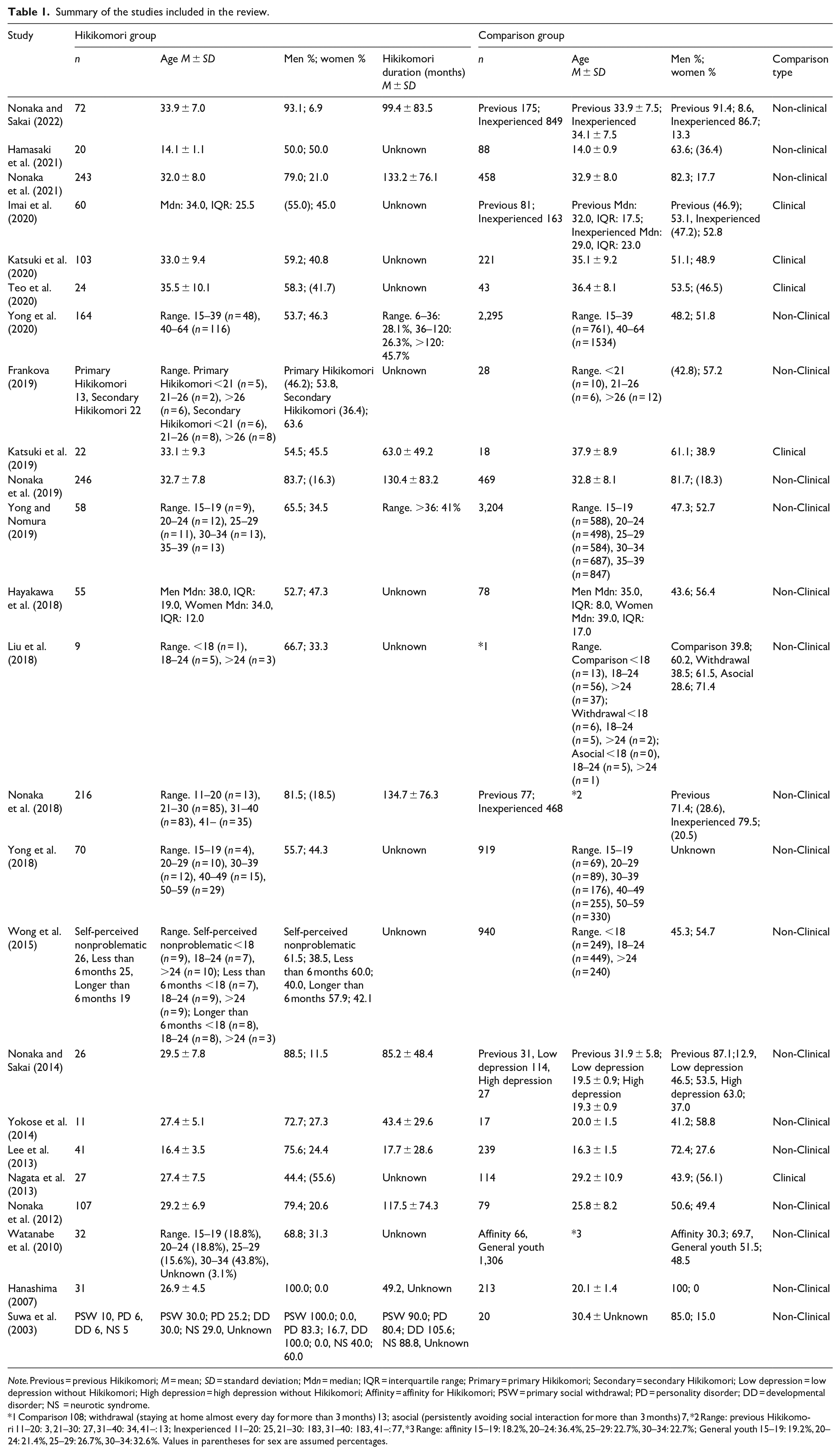
Note. Previous = previous Hikikomori; M = mean; SD = standard deviation; Mdn = median; IQR = interquartile range; Primary = primary Hikikomori; Secondary = secondary Hikikomori; Low depression = low depression without Hikikomori; High depression = high depression without Hikikomori; Affinity = affinity for Hikikomori; PSW = primary social withdrawal; PD = personality disorder; DD = developmental disorder; NS = neurotic syndrome.
1 Comparison 108; withdrawal (staying at home almost every day for more than 3 months) 13; asocial (persistently avoiding social interaction for more than 3 months) 7, *2 Range: previous Hikikomori 11–20: 3, 21–30: 27, 31–40: 34, 41–: 13; Inexperienced 11–20: 25, 21–30: 183, 31–40: 183, 41–: 77, *3 Range: affinity 15–19: 18.2%, 20–24: 36.4%, 25–29: 22.7%, 30–34: 22.7%; General youth 15–19: 19.2%, 20–24: 21.4%, 25–29: 26.7%, 30–34: 32.6%. Values in parentheses for sex are assumed percentages.
Summary of family information extracted from the studies included in the review.
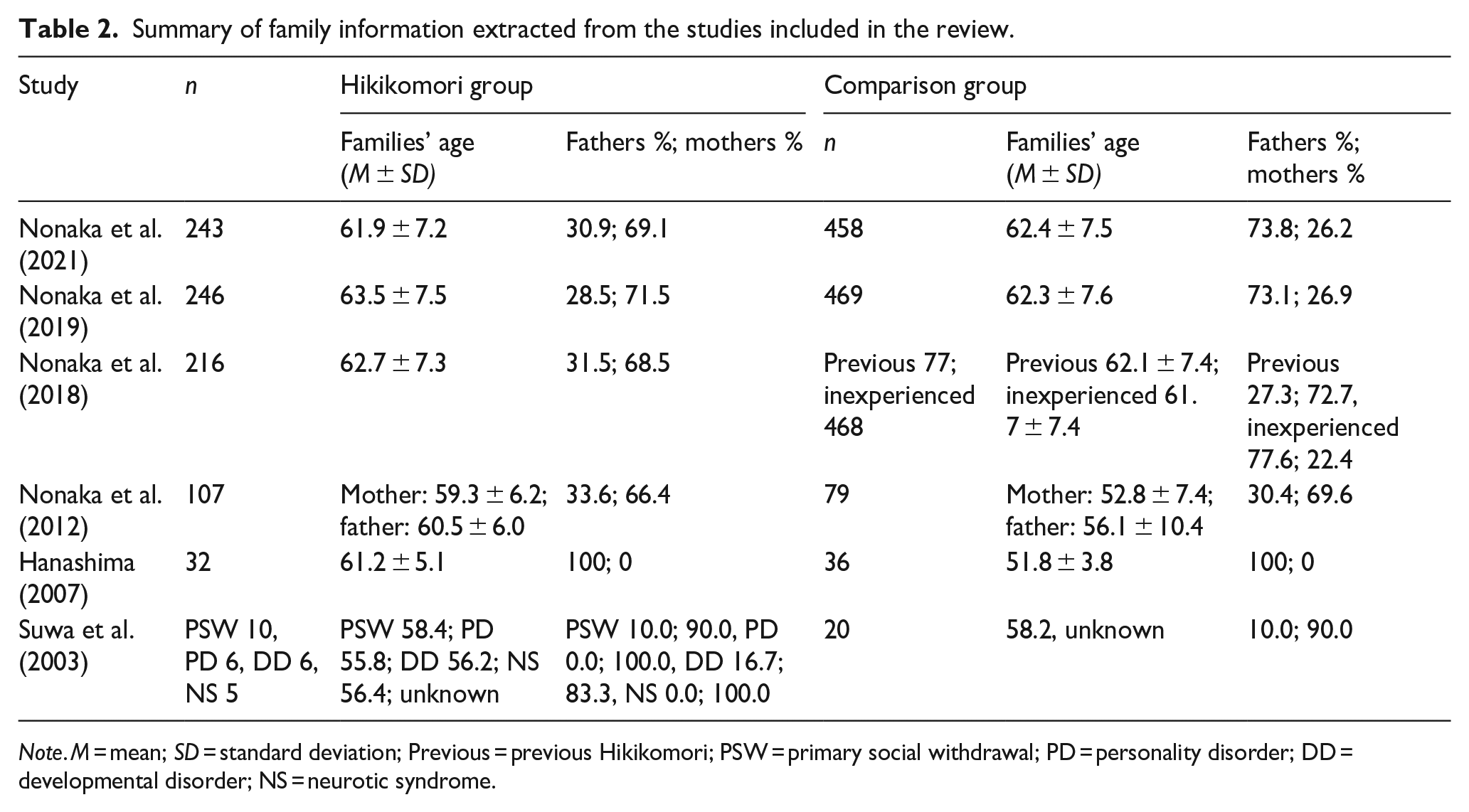
Note. M = mean; SD = standard deviation; Previous = previous Hikikomori; PSW = primary social withdrawal; PD = personality disorder; DD = developmental disorder; NS = neurotic syndrome.
Research location and elements of the Hikikomori definition used for each study.
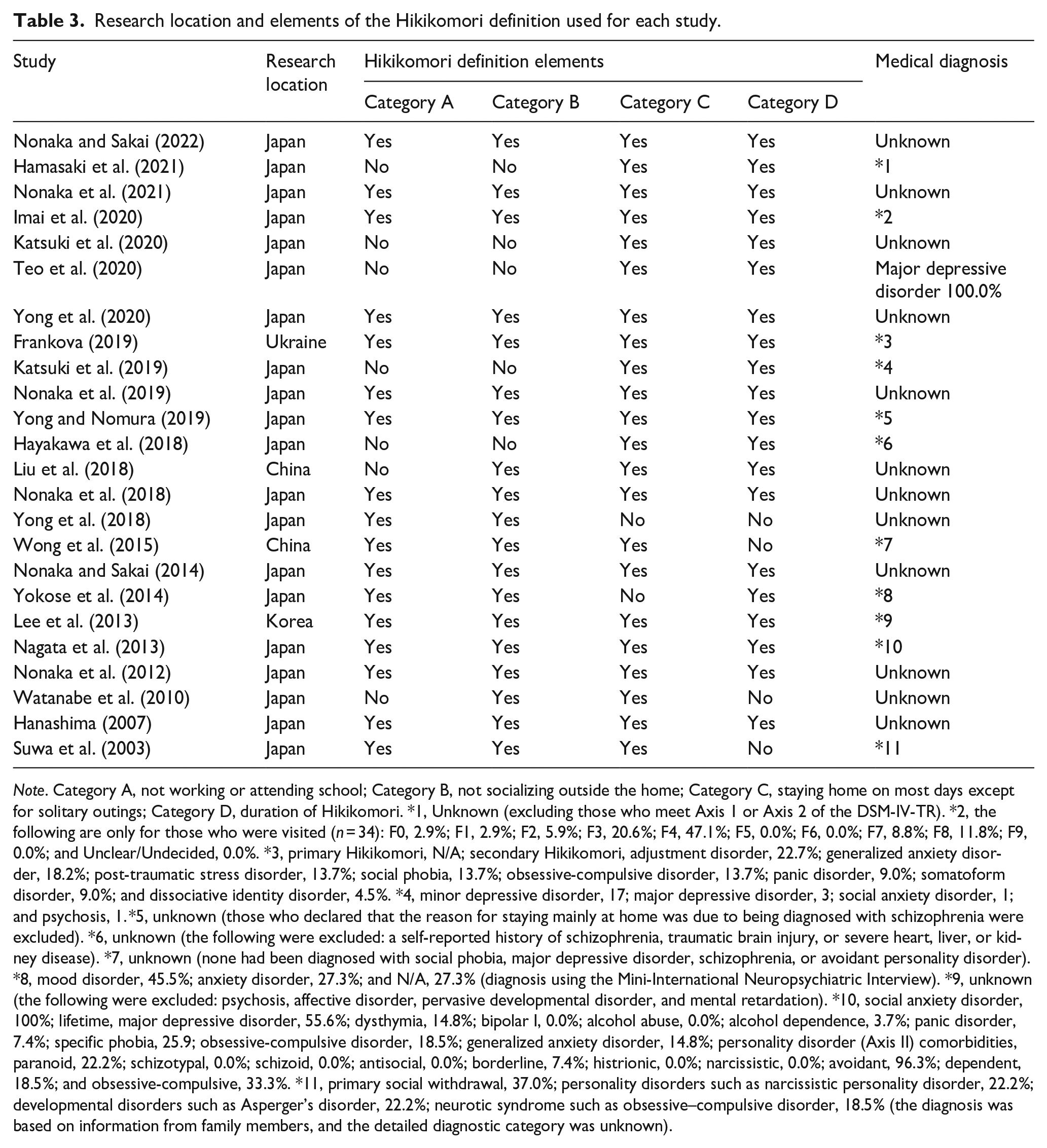
Note. Category A, not working or attending school; Category B, not socializing outside the home; Category C, staying home on most days except for solitary outings; Category D, duration of Hikikomori. *1, Unknown (excluding those who meet Axis 1 or Axis 2 of the DSM-IV-TR). *2, the following are only for those who were visited (n = 34): F0, 2.9%; F1, 2.9%; F2, 5.9%; F3, 20.6%; F4, 47.1%; F5, 0.0%; F6, 0.0%; F7, 8.8%; F8, 11.8%; F9, 0.0%; and Unclear/Undecided, 0.0%. *3, primary Hikikomori, N/A; secondary Hikikomori, adjustment disorder, 22.7%; generalized anxiety disorder, 18.2%; post-traumatic stress disorder, 13.7%; social phobia, 13.7%; obsessive-compulsive disorder, 13.7%; panic disorder, 9.0%; somatoform disorder, 9.0%; and dissociative identity disorder, 4.5%. *4, minor depressive disorder, 17; major depressive disorder, 3; social anxiety disorder, 1; and psychosis, 1. *5, unknown (those who declared that the reason for staying mainly at home was due to being diagnosed with schizophrenia were excluded). *6, unknown (the following were excluded: a self-reported history of schizophrenia, traumatic brain injury, or severe heart, liver, or kidney disease). *7, unknown (none had been diagnosed with social phobia, major depressive disorder, schizophrenia, or avoidant personality disorder). *8, mood disorder, 45.5%; anxiety disorder, 27.3%; and N/A, 27.3% (diagnosis using the Mini-International Neuropsychiatric Interview). *9, unknown (the following were excluded: psychosis, affective disorder, pervasive developmental disorder, and mental retardation). *10, social anxiety disorder, 100%; lifetime, major depressive disorder, 55.6%; dysthymia, 14.8%; bipolar I, 0.0%; alcohol abuse, 0.0%; alcohol dependence, 3.7%; panic disorder, 7.4%; specific phobia, 25.9; obsessive-compulsive disorder, 18.5%; generalized anxiety disorder, 14.8%; personality disorder (Axis II) comorbidities, paranoid, 22.2%; schizotypal, 0.0%; schizoid, 0.0%; antisocial, 0.0%; borderline, 7.4%; histrionic, 0.0%; narcissistic, 0.0%; avoidant, 96.3%; dependent, 18.5%; and obsessive-compulsive, 33.3%. *11, primary social withdrawal, 37.0%; personality disorders such as narcissistic personality disorder, 22.2%; developmental disorders such as Asperger’s disorder, 22.2%; neurotic syndrome such as obsessive–compulsive disorder, 18.5% (the diagnosis was based on information from family members, and the detailed diagnostic category was unknown).
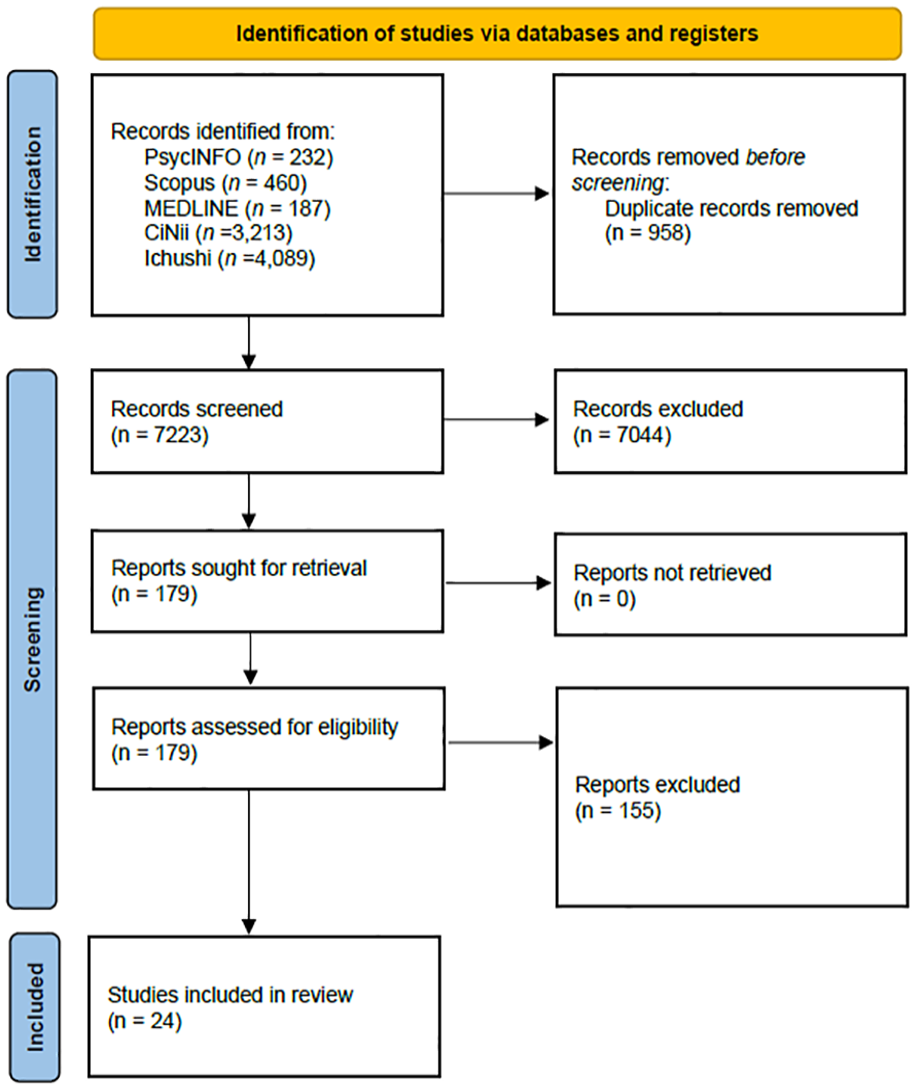
Flow diagram of the search process for this review.
Study characteristics
The total sample size comprised 1,769 Hikikomori and 12,928 non-Hikikomori individuals. Of the 24 included studies, 20 (83.3%) were conducted in Japan, two (8.3%) in China, and one each in Korea and Ukraine. Overall, 79.2% of the studies used non-clinical controls as participants for comparison, and 20.8% used clinical controls.
Functioning and disability of individuals with Hikikomori
Supplemental Appendix 2 presents the reported between-group comparisons for each component. Twelve indicators from six studies (Hamasaki et al., 2021; Imai et al., 2020; Lee et al., 2013; Nagata et al., 2013; Teo et al., 2020; Watanabe et al., 2010) on depression- and anxiety-related symptoms, three from three studies (Hamasaki et al., 2021; Lee et al., 2013; Wong et al., 2015) on dependence- and addiction-related symptoms, and four from two studies (Hamasaki et al., 2021; Lee et al., 2013) on thought-problem-related symptoms were higher in the Hikikomori group than those in the comparison group, with at least moderate effect sizes and 95% CIs that did not include 0. In contrast, no indicators showed fewer respective mental symptoms in the Hikikomori group compared with the comparison group. Three indicators from three studies (Hamasaki et al., 2021; Lee et al., 2013; Watanabe et al., 2010) on interpersonal relationship problems were worse in the Hikikomori group compared with the comparison group, with at least moderate effect sizes and 95% CIs that did not include 0. In contrast, no indicator showed that interpersonal problems were better in the Hikikomori group compared with the comparison group. Additionally, regarding Daily life/Social life component, offline bonding in social capital and motivation or illusion of a job were low in the Hikikomori group (Liu et al., 2018; Watanabe et al., 2010). The proportion of individuals with avoidant personality was consistently and significantly higher in the Hikikomori group than that in the comparison group across multiple studies (Hayakawa et al., 2018; Katsuki et al., 2019; Lee et al., 2013). The other temperaments and personality types showed less consistent differences.
The estimated average SMD using a random effects model was 0.78 (95% CI [0.45, 1.11]; p < .001, k = 9) for internalizing symptoms, 0.77 (95% CI [0.30, 1.24]; p = .001, k = 4) for externalizing symptoms, and 0.83 (95% CI [0.21, 1.44]; p = .01, k = 3) for thought disorder. These values were significantly higher in the Hikikomori group than that in the comparison group (Table 4, Figures 2–4). Conversely, communication/interpersonal interactions and relationship were significantly lower in the Hikikomori group (−0.74 [95% CI [−1.06, −0.42]]; p < .001, k = 7; Figure 5). However, there was no significant difference in their daily life/social life (−0.38 [95% CI [−0.91, 0.16]]; p = .17, k = 2; Figure 6).
Data by the groups included in the meta-analyses.
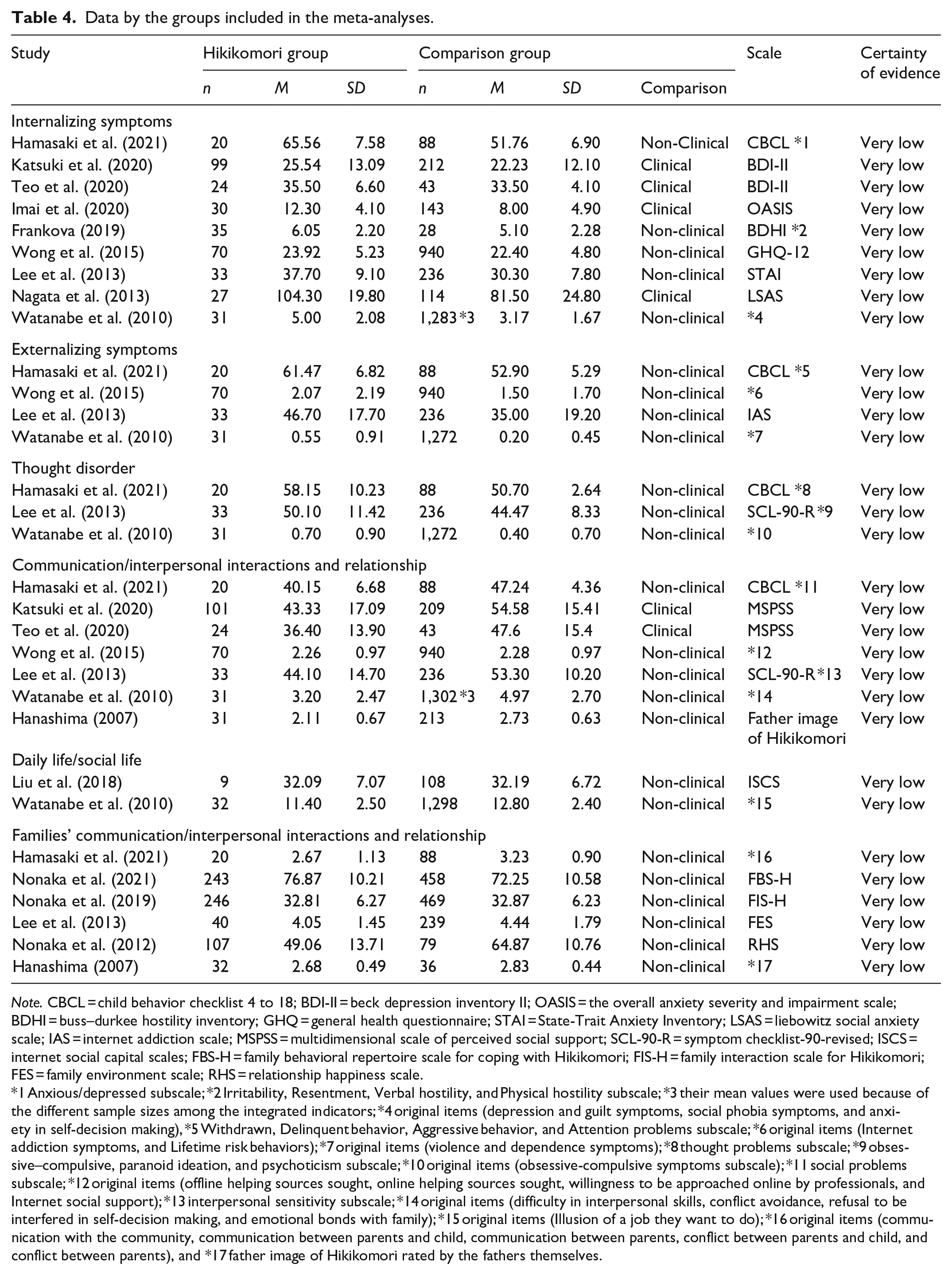
Note. CBCL = child behavior checklist 4 to 18; BDI-II = beck depression inventory II; OASIS = the overall anxiety severity and impairment scale; BDHI = buss–durkee hostility inventory; GHQ = general health questionnaire; STAI = State-Trait Anxiety Inventory; LSAS = liebowitz social anxiety scale; IAS = internet addiction scale; MSPSS = multidimensional scale of perceived social support; SCL-90-R = symptom checklist-90-revised; ISCS = internet social capital scales; FBS-H = family behavioral repertoire scale for coping with Hikikomori; FIS-H = family interaction scale for Hikikomori; FES = family environment scale; RHS = relationship happiness scale.
1 Anxious/depressed subscale; *2 Irritability, Resentment, Verbal hostility, and Physical hostility subscale; *3 their mean values were used because of the different sample sizes among the integrated indicators; *4 original items (depression and guilt symptoms, social phobia symptoms, and anxiety in self-decision making), *5 Withdrawn, Delinquent behavior, Aggressive behavior, and Attention problems subscale; *6 original items (Internet addiction symptoms, and Lifetime risk behaviors); *7 original items (violence and dependence symptoms); *8 thought problems subscale; *9 obsessive–compulsive, paranoid ideation, and psychoticism subscale; *10 original items (obsessive-compulsive symptoms subscale); *11 social problems subscale; *12 original items (offline helping sources sought, online helping sources sought, willingness to be approached online by professionals, and Internet social support); *13 interpersonal sensitivity subscale; *14 original items (difficulty in interpersonal skills, conflict avoidance, refusal to be interfered in self-decision making, and emotional bonds with family); *15 original items (Illusion of a job they want to do); *16 original items (communication with the community, communication between parents and child, communication between parents, conflict between parents and child, and conflict between parents), and *17 father image of Hikikomori rated by the fathers themselves.
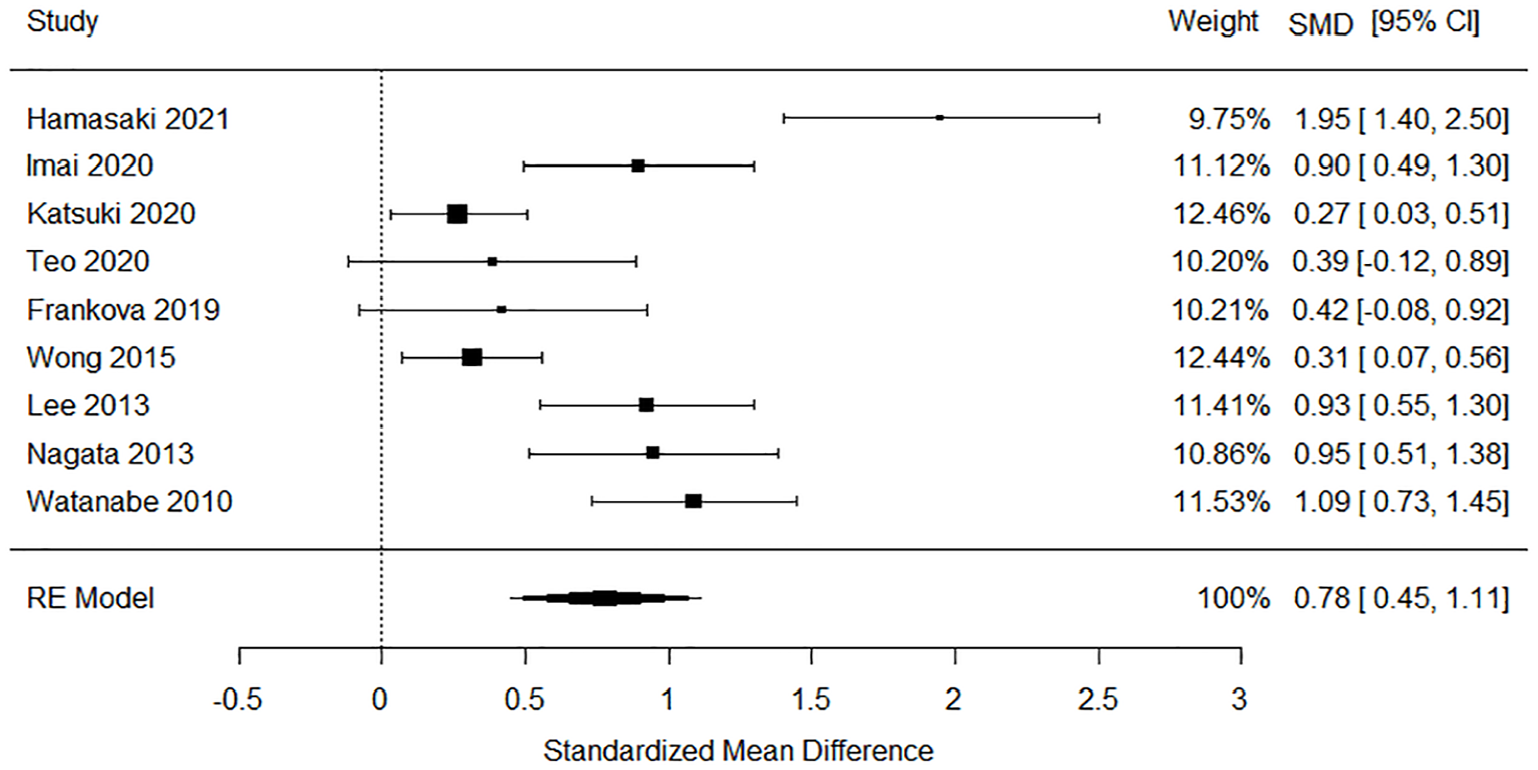
Forest plot of the internalizing symptom components.
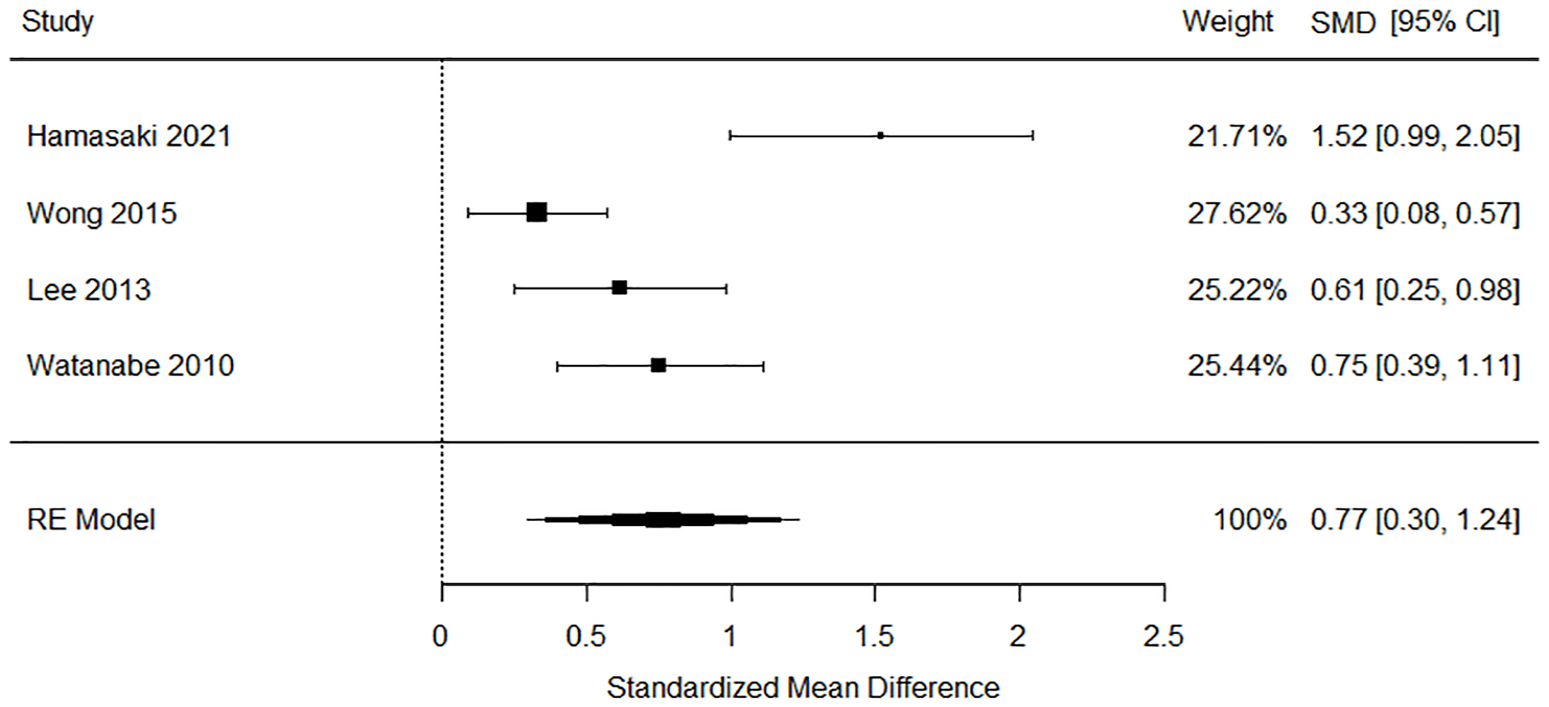
Forest plot of the externalizing symptom components.
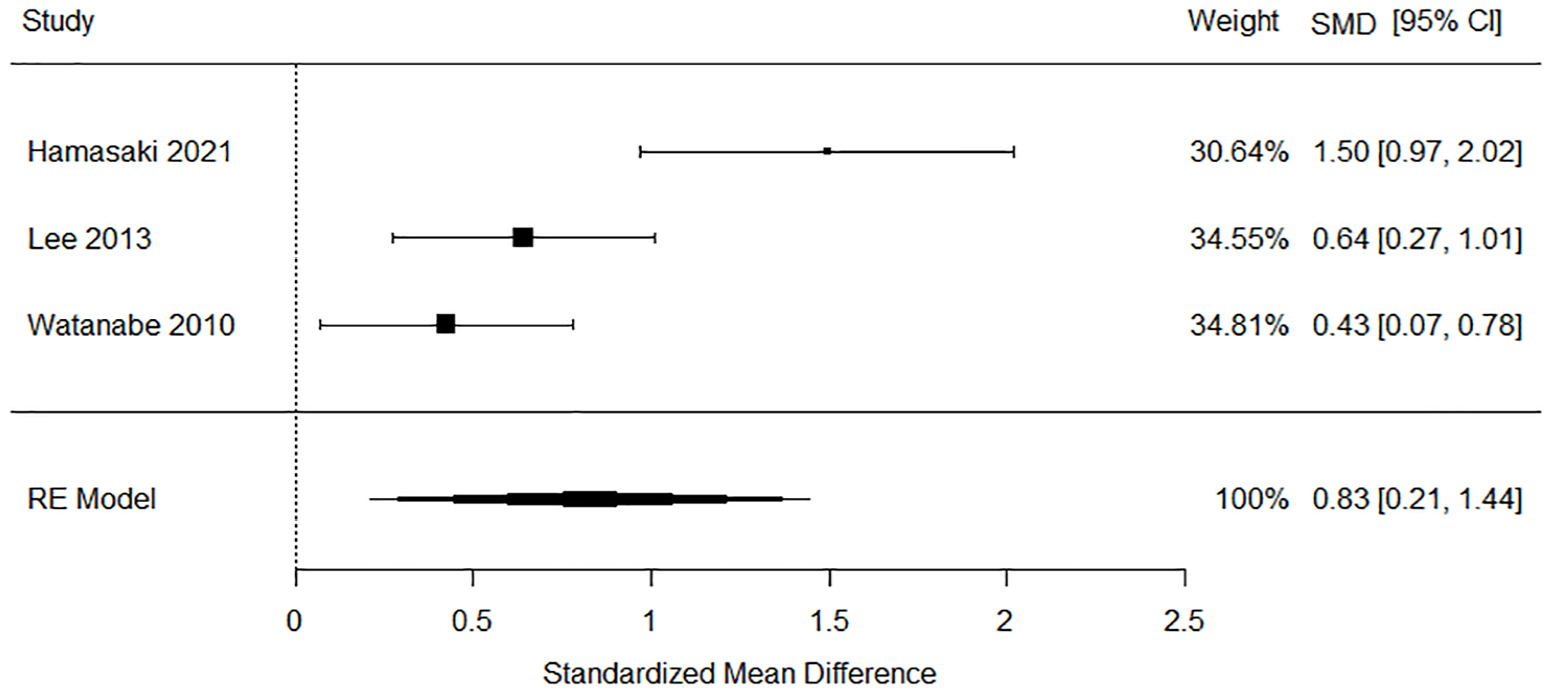
Forest plot of the thought disorder components.
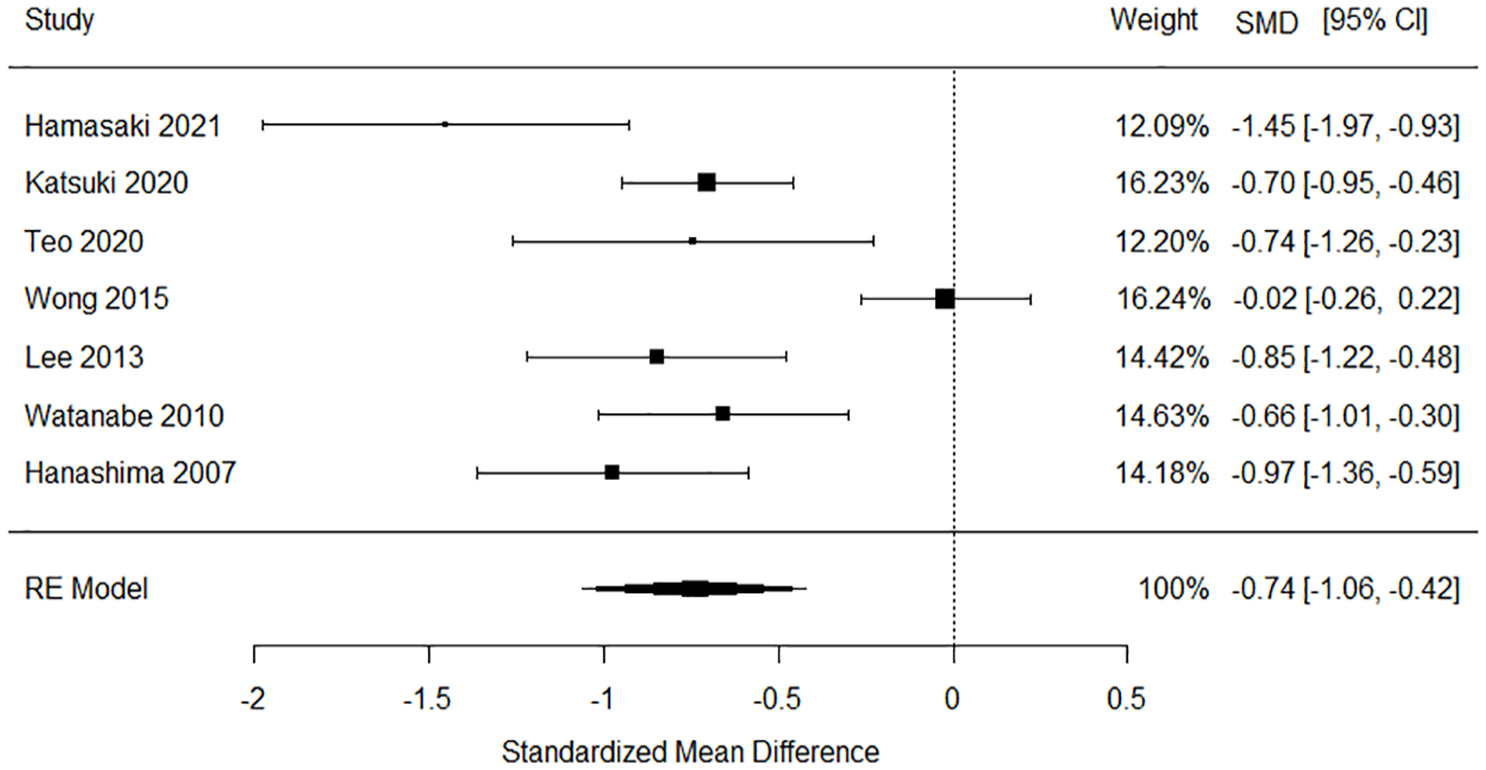
Forest plot of the communication/interpersonal interactions and relationship components.
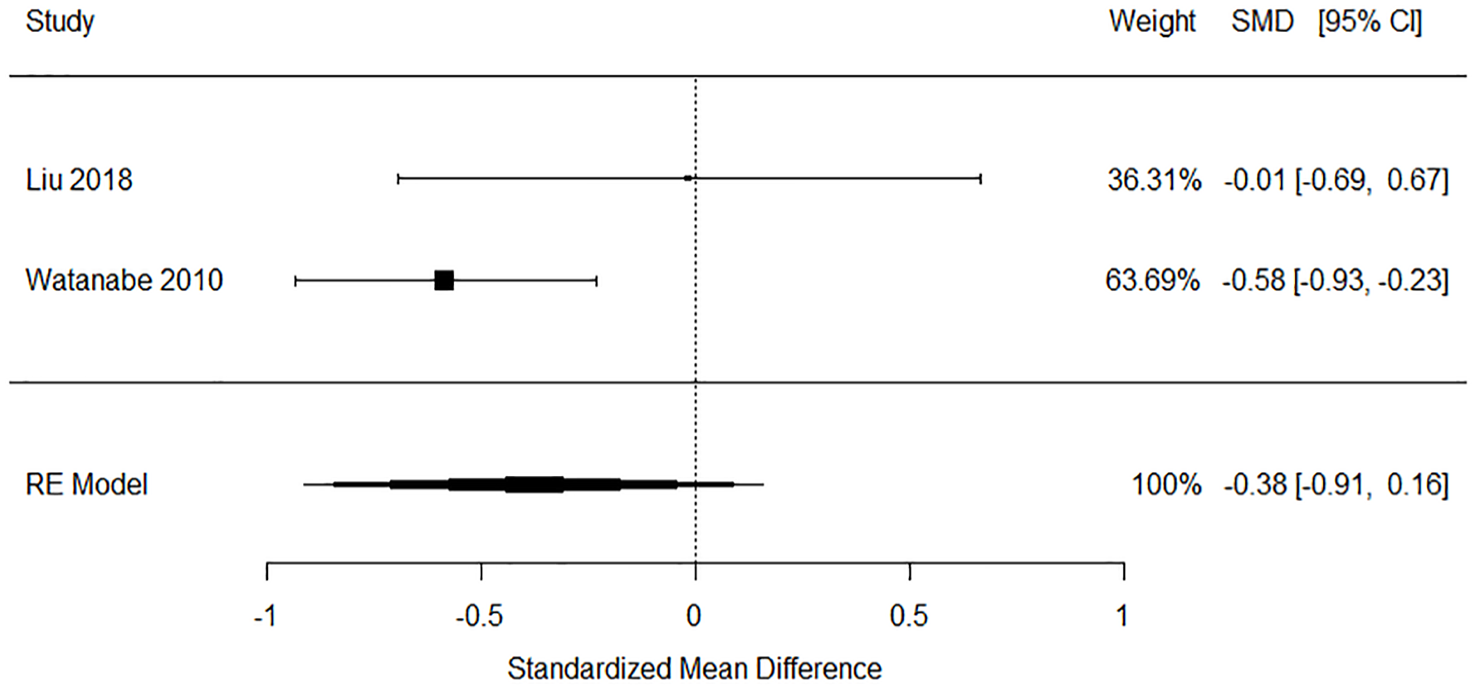
Forest plot of the daily life/social life components.
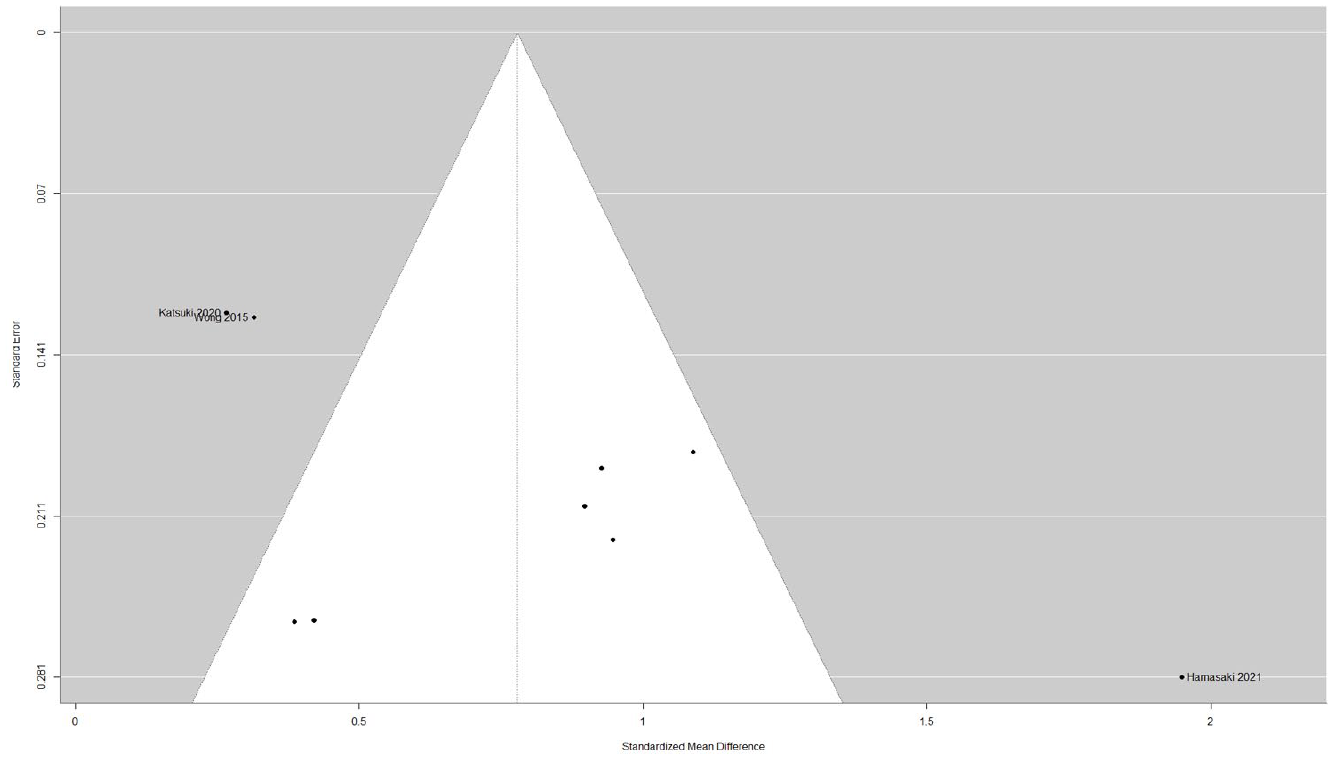
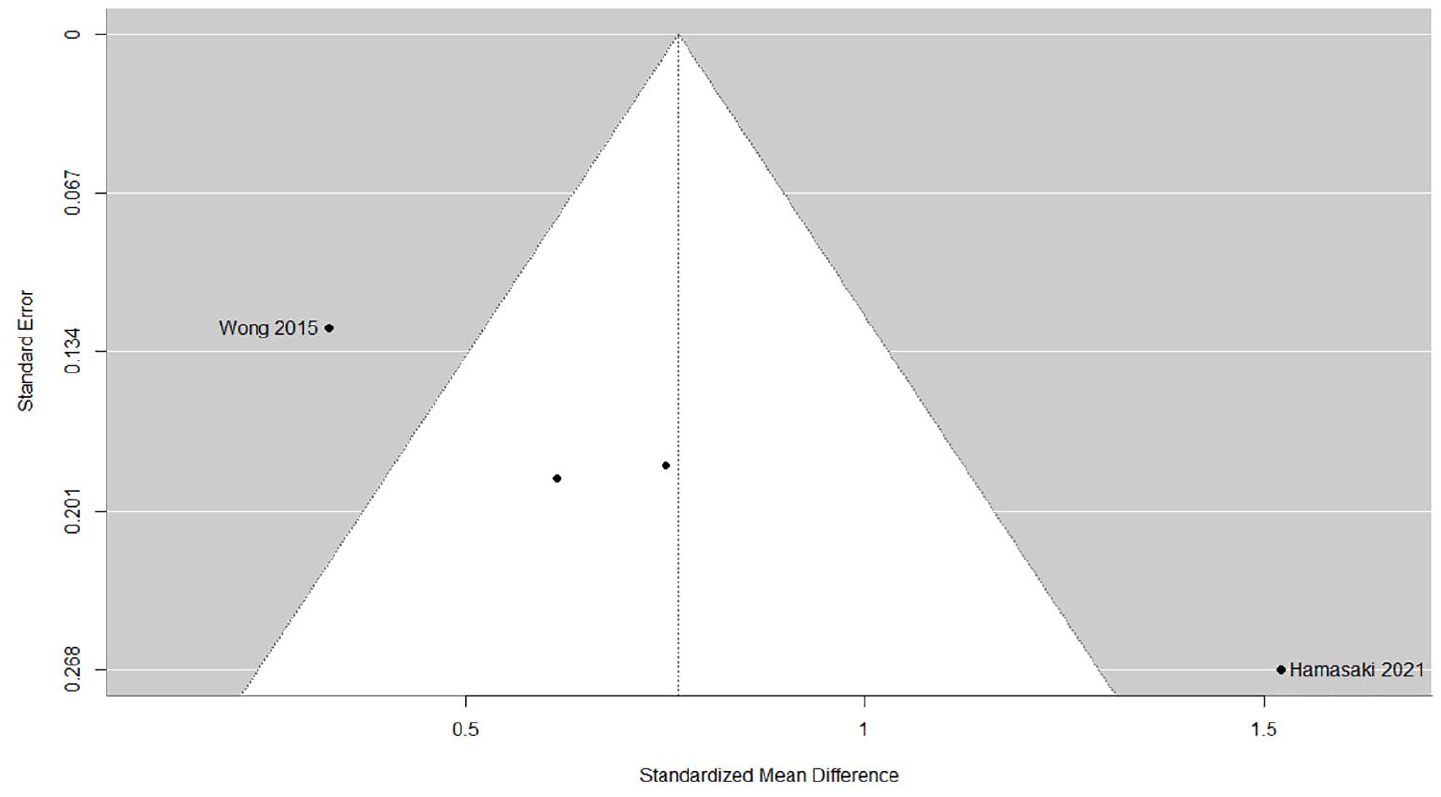
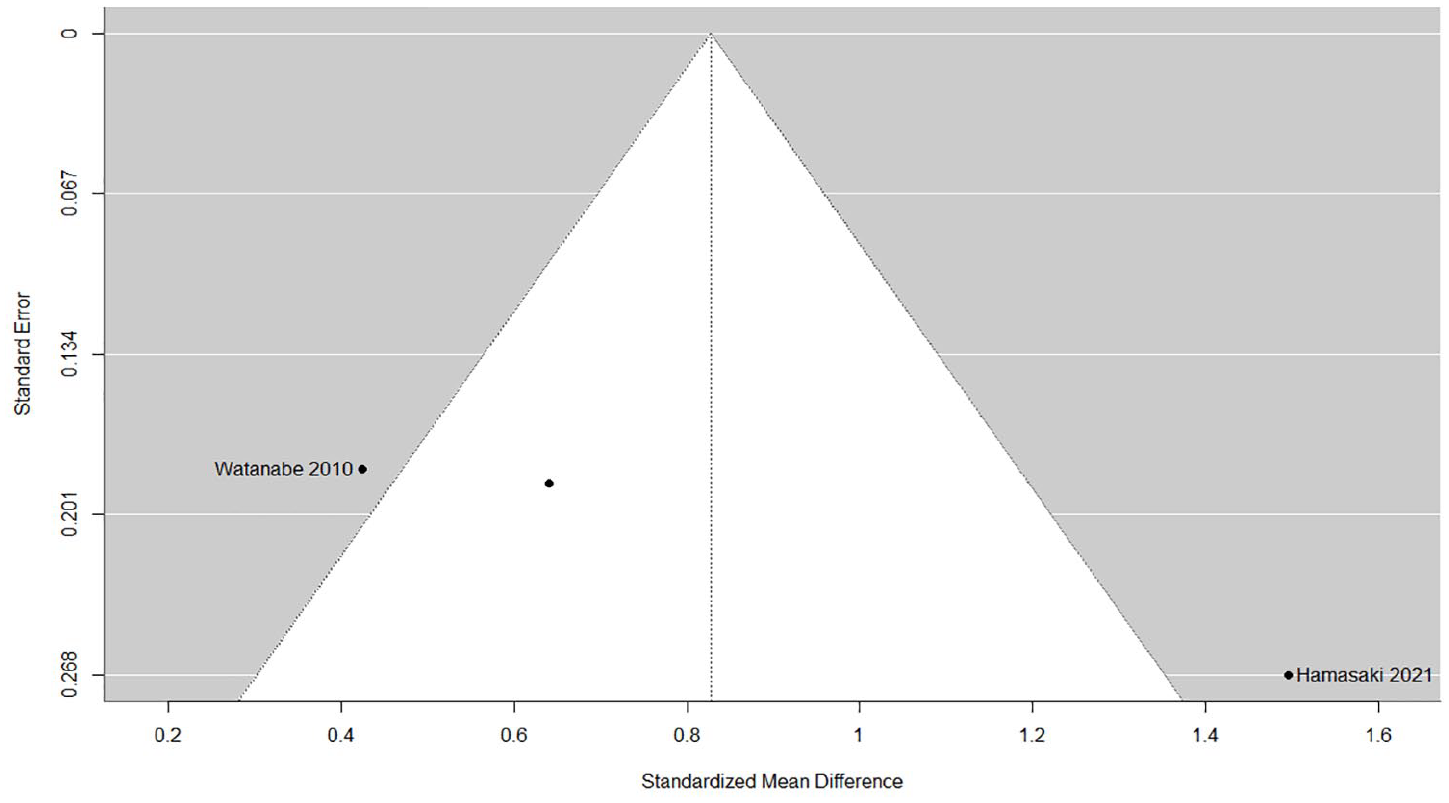
The heterogeneity between studies was high, and differences between the groups were inconsistent. The fail-safe numbers and funnel plots results indicated, at least partially, the possible existence of publication bias in externalizing symptoms, thought disorders, and communication/interpersonal interactions and relationship. Contrastingly, publication bias was not likely to exist in internalizing symptoms. Figures 7 to 11 show funnel plots.
Funnel plot of the internalizing symptom components.
Funnel plot of the externalizing symptom components.
Funnel plot of the thought disorder components.
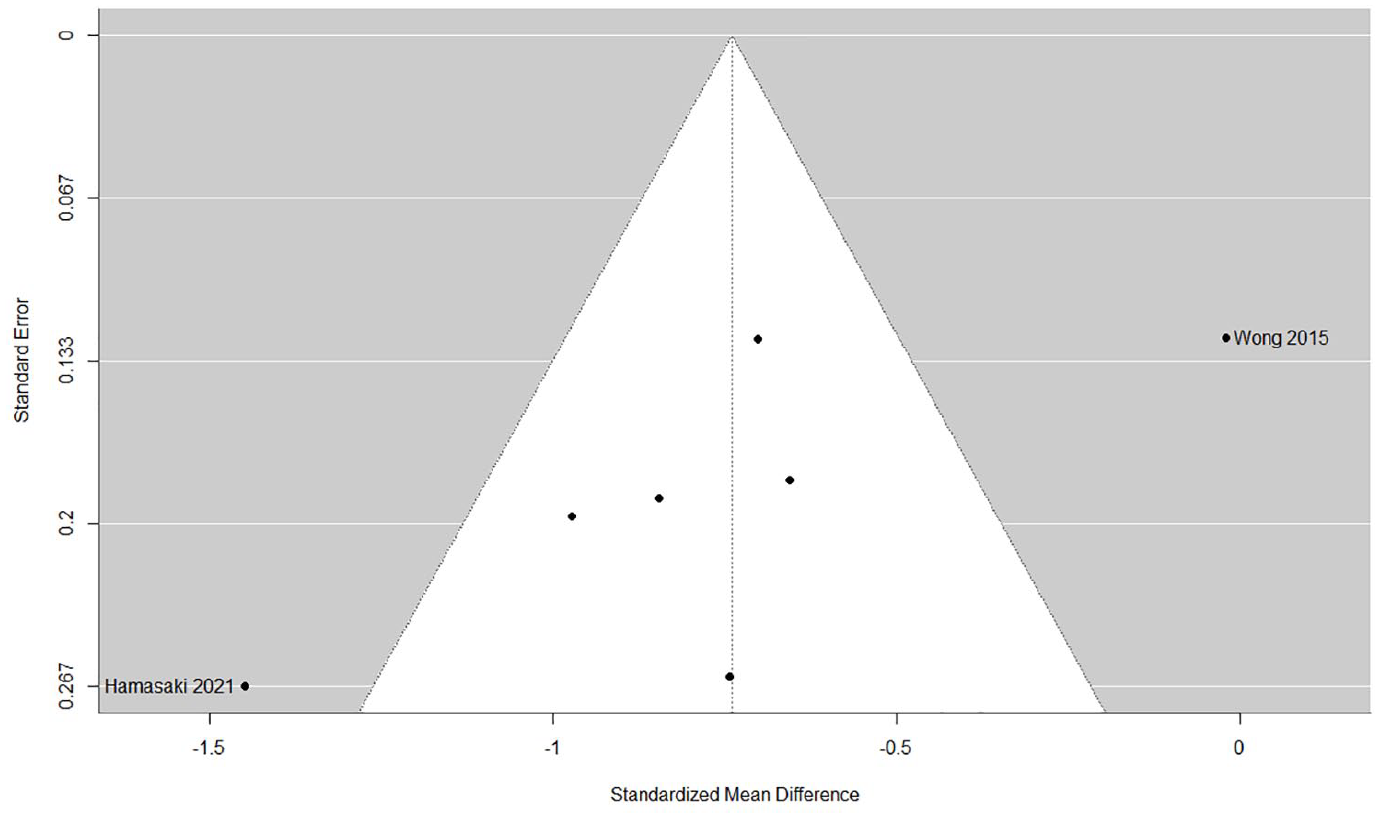
Funnel plot of the communication/interpersonal interactions and relationship components.
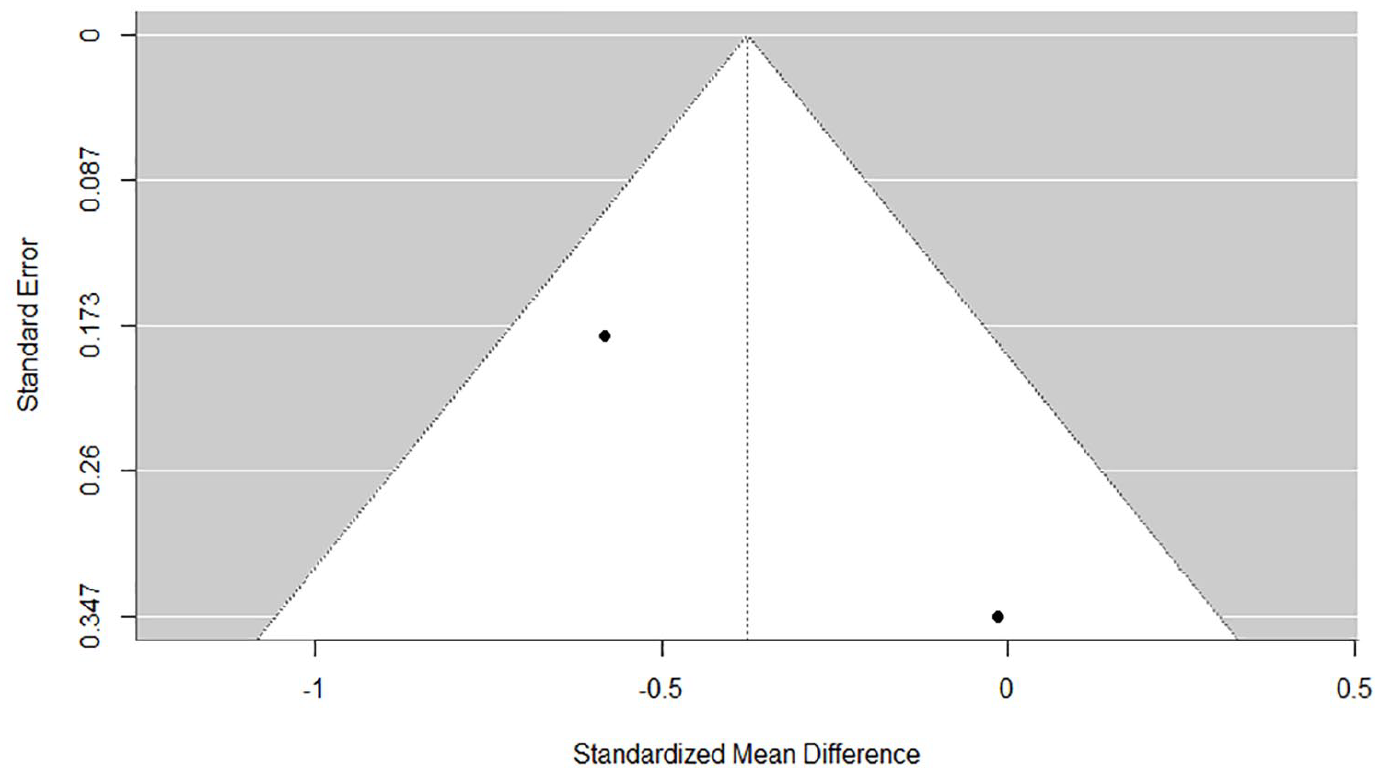
Funnel plot of the daily life/social life components.
Subgroup analysis demonstrated that the estimated average SMD for internalizing symptoms was 0.61 (95% CI [0.25, 0.96], p < .001, k = 4) for the clinical control group and 0.92 (95% CI [0.37, 1.47], p = .001, k = 5) for the non-clinical comparison group. In the communication/interpersonal interactions and relationship, the estimated average SMD was −0.71 (95% CI [−0.93, −0.49], p < .001, k = 2) for the clinical control and −0.76 (95% CI [−1.22, −0.30], p = .001, k = 5) for the non-clinical control. Subgroup analyses focusing on the country in which the research was conducted (Japan vs. non-Japan), age, and Hikikomori duration were not performed due to the limited number of studies included in the meta-analysis. Considering the results of sensitivity analysis, excluding the study by Hamasaki et al. (2021), internalizing symptoms (Q = 28.23, p < .001, I2 = 73.49%; SMD 0.65, p < .001), externalizing symptoms (Q = 4.18, p = .12, I2 = 51.97%; SMD 0.54, p < .001), and thought disorder (Q = 0.68, p = .41, I2 = 0.00%; SMD 0.53, p < .001) showed the lowest heterogeneity index. However, heterogeneity was still high regarding internalizing and externalizing symptoms. Excluding the study by Wong et al. (2015), communication/interpersonal interactions and relationships (Q = 7.97, p = .16, I2 = 28.46%; SMD −0.84, p < .001) showed the lowest heterogeneity index.
Functioning and disability of the family of individuals with Hikikomori
Supplemental Appendix 3 presents the reported between-group comparisons for each component. Ten indicators from five studies (Hamasaki et al., 2021; Hanashima, 2007; Lee et al., 2013; Nonaka et al., 2012, 2019) on bad communication within the family were higher in the Hikikomori group than that in the comparison group, with at least moderate effect sizes and 95% CIs that did not include 0. Some of these indicators also included bad communication between parents. In contrast, one indicator showed better communication within families in the Hikikomori group than that in the comparison group (Nonaka et al., 2019).
This meta-analysis indicated no significant difference in the families’ communication/interpersonal interactions and relationship (−0.31 95% CI [−0.78, 0.16]; p = .20, k = 6; Figure 12). The heterogeneity between studies was high; the differences between the groups were inconsistent (Figure 13). Regarding the results of sensitivity analysis, excluding the study by Nonaka et al. (2012), families’ communication/interpersonal interactions and relationship (Q = 33.97, p < .001, I2 = 88.71%; SMD −0.09, p = .60) showed the lowest heterogeneity index. However, heterogeneity was still high.
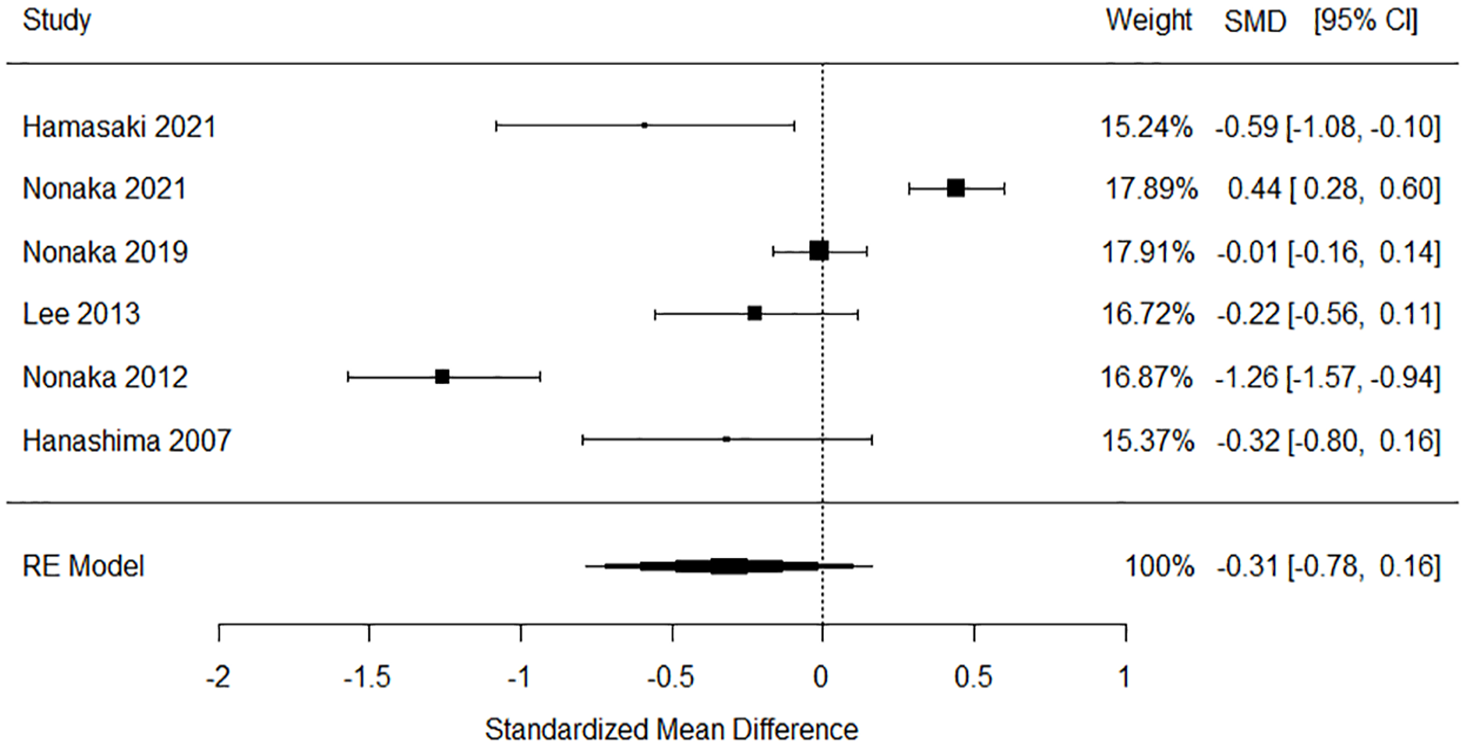
Forest plot of the families’ communication/interpersonal interactions and relationship components.
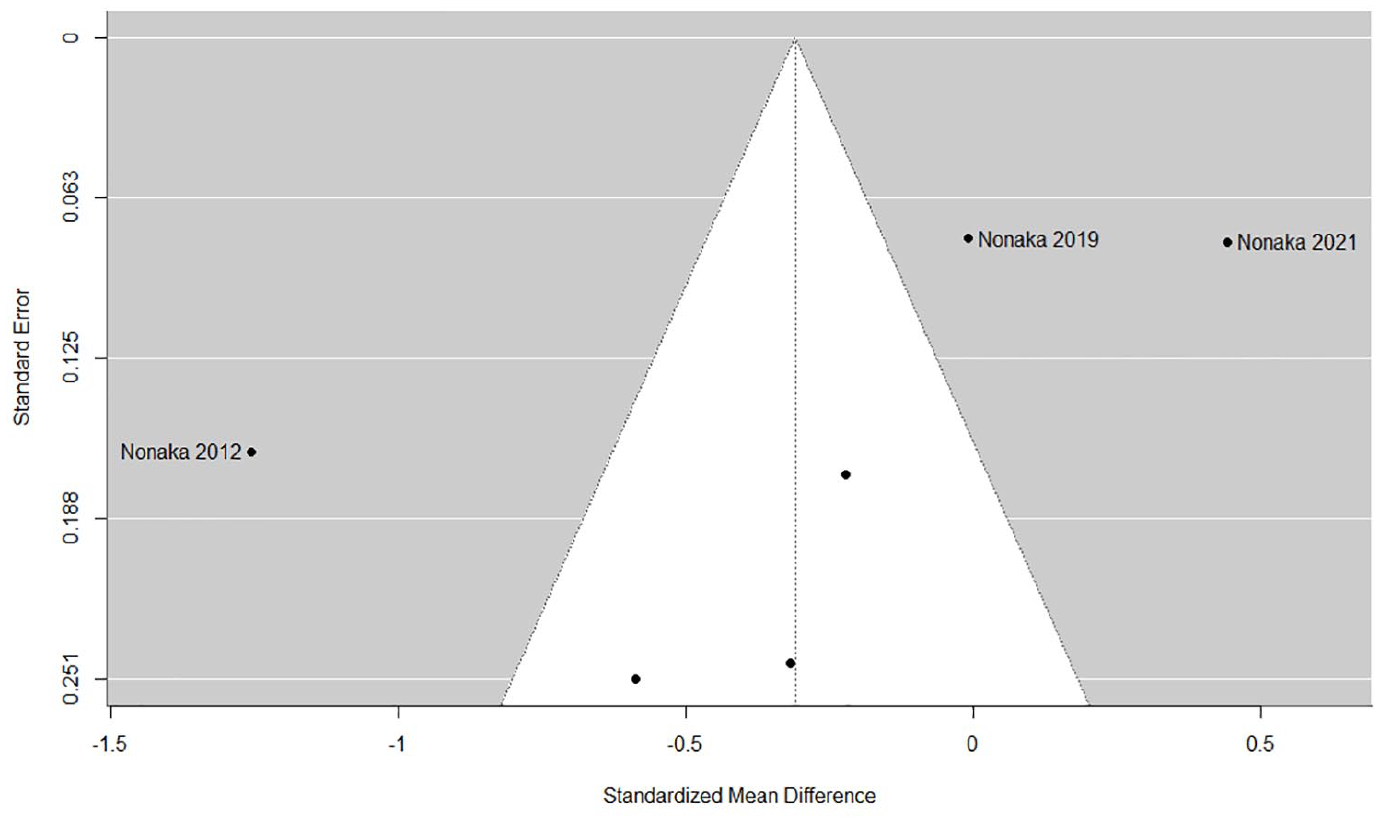
Funnel plot of the families’ communication/interpersonal interactions and relationship components.
Risk of bias assessment
The quality analysis demonstrated that, on average, each study met 55.0% of the criteria (range: 20%–70%) but did not meet 38.3% of the criteria (range: 20%–70%). Moreover, 6.7% (range: 0%–30%) of the observations were unclear (Table 5). The certainty of evidence for all studies was very low (Table 4).
Risk of Bias Assessment.
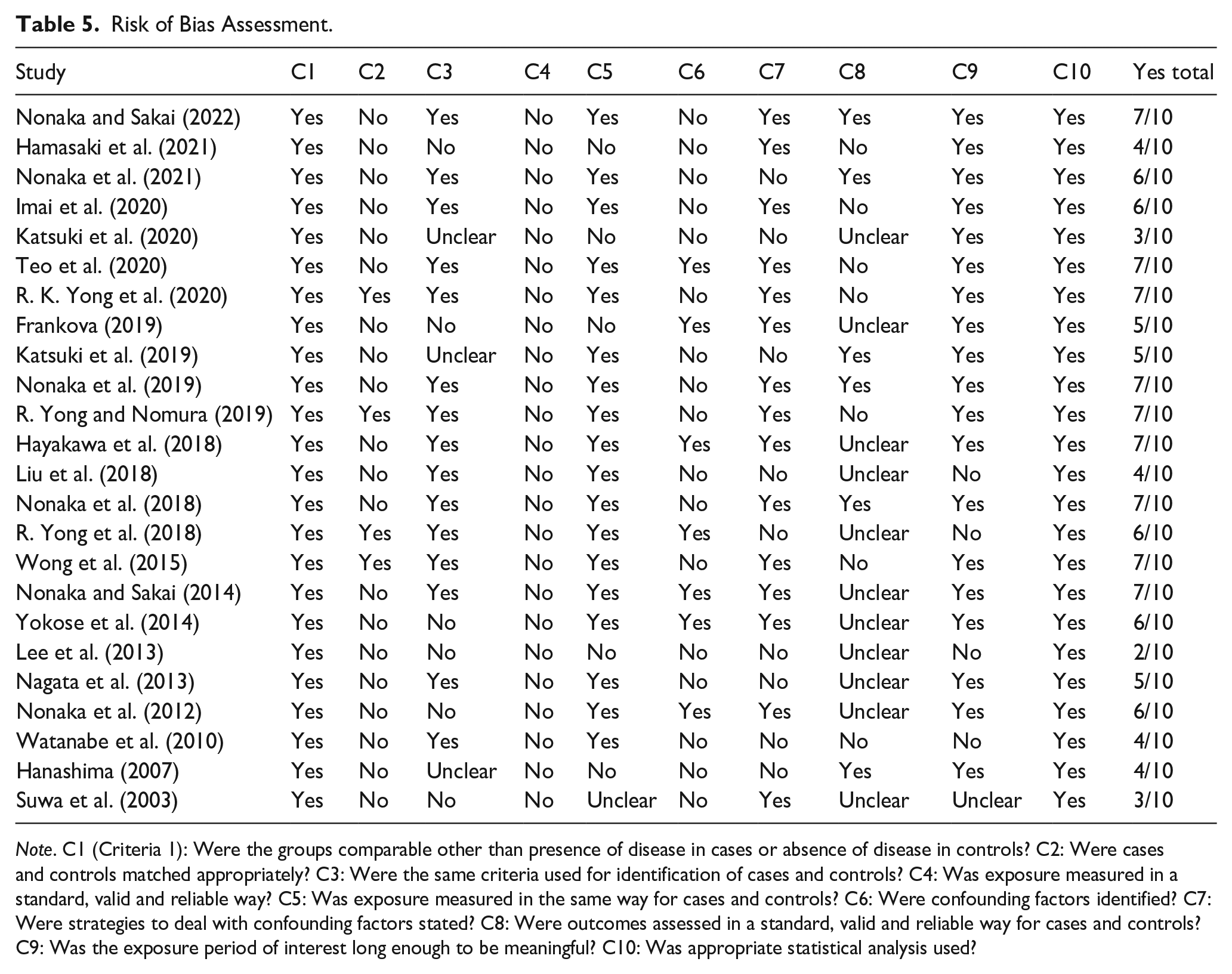
Note. C1 (Criteria 1): Were the groups comparable other than presence of disease in cases or absence of disease in controls? C2: Were cases and controls matched appropriately? C3: Were the same criteria used for identification of cases and controls? C4: Was exposure measured in a standard, valid and reliable way? C5: Was exposure measured in the same way for cases and controls? C6: Were confounding factors identified? C7: Were strategies to deal with confounding factors stated? C8: Were outcomes assessed in a standard, valid and reliable way for cases and controls? C9: Was the exposure period of interest long enough to be meaningful? C10: Was appropriate statistical analysis used?
Discussion
This study systematically reviewed the existing literature to identify the levels of functioning, disability, and health of individuals with Hikikomori and their families compared with those without Hikikomori. Although substantial heterogeneity existed among the included studies, drawing some generalizations were possible. The qualitative and meta-analysis results revealed that individuals with Hikikomori had lower mental function and communication or interpersonal interactions and relationship than non-Hikikomori individuals, with moderate-to-high effect sizes. The level of difference was moderate, even when compared with clinical controls. This meta-analysis included studies that excluded individuals with Hikikomori with comorbid psychiatric disorders. The results showing poor mental function in individuals with Hikikomori indicated that mental health problems should not be ignored, even being comorbid subthreshold mental disorders. This study is the first systematic evidence of the poor psychosocial functioning in individuals with Hikikomori. It could provide an important basis for facilitating psychiatric understanding and developing necessary treatment.
Herein, individual indicators did not reveal any potential moderators of functioning, including age or sex. For example, with respect to internalizing symptoms, no significant difference was observed between the Hamilton Rating Scale for Depression used by Katsuki et al. (2020) and the Patient Health Questionnaire 9 and Beck Depression Inventory II (BDI-II) used by Teo et al. (2020). However, significant differences were observed in other indices that reflected the same or similar concepts in the studies. Thus, the results were not always consistent within studies. The same was true regarding externalizing symptoms.
Our results demonstrating impairments in mental function are consistent with previously reported findings. Social distancing caused by non-disclosure of depression and social withdrawal caused by poor mental health were found to be associated with loneliness and persistent symptoms (Achterbergh et al., 2020); moreover, social isolation has been associated with social anxiety disorder (Teo et al., 2013). Furthermore, lower perceived social support was associated with poorer symptoms, recovery, and social functioning, and loneliness results in poorer depression outcomes in patients with depression, bipolar disorder, and social anxiety disorders (Wang et al., 2018). Loneliness was associated with common mental disorders, including depression, phobias, and obsessive-compulsive disorder (Meltzer et al., 2013); additionally, in a study by Erzen and Çikrikci (2018), loneliness was associated with depression at moderate levels. Although few reports have been published on Internet addiction and overuse in externalizing symptoms, there is a study on college students (Tateno et al., 2019), a literature review (Stip et al., 2016), and a systematic review (Sales-Filho et al., 2023) on this topic. The results of the present study at least partially support these findings. However, further robust study designs, including case-control studies, are warranted. An overview of reports from multiple individual studies has revealed a consistent trend toward high levels of avoidant personality traits in individuals with Hikikomori. Avoidant personality disorder is more likely to be comorbid with major depressive disorder (16%; Friborg et al., 2014) and various anxiety disorders, including social phobia (46%; Friborg et al., 2013), and it has a higher prevalence of comorbidity than other personality disorders. Thus, the tendency of individuals with Hikikomori to have poor mental function may be affected by their highly avoidant personalities.
Many studies have reported maladaptive communication and interpersonal relationships among individuals with Hikikomori. Coping strategies to seek support from others under stress were associated with lower severity of Hikikomori (Nonaka & Sakai, 2021), whereas interpersonal anxiety and difficulties were associated with Hikikomori (R. Yong & Nomura, 2019). The results of the present meta-analysis support these previous findings and another finding by Nonaka and Sakai (2023) where a lower frequency of going out with others is a condition for Hikikomori, thereby indicating that disabilities in communication and interpersonal relationships are the primary characteristics of Hikikomori. However, some studies demonstrated contradictory results: Wong et al. (2015) observed internet social support, and Watanabe et al. (2010) noted a refusal to interfere with self-decision-making, suggesting that communication and interpersonal interactions were better in individuals with Hikikomori than those in non-Hikikomori individuals. However, it is noteworthy that Watanabe et al. (2010) assessed the differences by comparing individuals with higher Hikikomori affinity, that is, individuals with Hikikomori having desire and empathy; both studies found that individuals with Hikikomori fared worse on other measures that reflected slightly related concepts. The variability of results is more marked in the families’ communication and interpersonal interactions. Effect sizes for each indicator demonstrated that Hikikomori cases had poorer communication functioning within family than non-Hikikomori cases regarding many indicators. Contrastingly, the opposite has been reported for some indicators including parental behavioral repertoires (Nonaka et al., 2021), parental cognition of contingency, and behavior theory-based family interaction (Nonaka et al., 2019). In both studies, Hikikomori cases were Hikikomori family group participants. These contradictory results may reflect an improvement in the parental behavioral repertoire and intra-family interactions through family group participation. Two possible explanations could be: (i) large individual variations in the cognitive-behavioral indicators of parent-child relationships and (ii) improvement in the parental behavioral repertoire or family interactions does not always lead to recovery from Hikikomori. The finding that nearly some of families’ communication/interpersonal interactions and relationship indicators demonstrated no significant differences between the groups (Hamasaki et al., 2021; Hanashima, 2007; Lee et al., 2013) supports the former explanation. A study reported that a significant increase in perceived parental skills did not significantly increase (but partially increased) the overall adaptive behavior of children with Hikikomori, thereby supporting the latter explanation (Kubo et al., 2020). However, a pattern of cognitive-behavioral changes in parents that alters the behavior of their children with Hikikomori has also been reported in an intervention study with small sample size (Nonaka et al., 2023).
There were no clear differences in the daily or social life, temperament or personality, and families’ communication/interpersonal interactions and relationship. Meta-analyses of daily or social life included indicators of social capital and work-related attitudes. According to the individual studies included, compared with non-Hikikomori individuals, Hikikomori individuals had worse social capital, which refers to a network of relationships, as reported by one study (R. Yong et al., 2018), whereas another study reported no significant difference (Liu et al., 2018). The reasons for these inconsistent findings could be attributed to the differences in the countries in which the surveys were conducted (Japan and China), differences in the research methods (face-to-face vs. social media), and the fact that Liu et al. (2018) included online social capital. The significant variability in the results of certain components suggests the need for assessing individual variability. Furthermore, given the results of post-hoc sensitivity analysis in communication/interpersonal interactions and relationships component, the results by Wong et al. (2015) differed from those of other studies in that they included indicators related to online communication. Thus, the tendency of functioning regarding communication and interpersonal relationships in individuals with Hikikomori may differ depending on whether their means of communication were online or offline.
Overall, the studies included in this research had a higher proportion of men than of women. The sex ratio of individuals with Hikikomori differed between Japan and other countries (Nonaka & Sakai, 2022), indicating potential cultural differences. Moreover, this inconsistency in the sex ratio may be attributed to overlapping psychiatric disorders. Autism spectrum disorder (ASD) and social anxiety are the main psychiatric disorders overlapping with Hikikomori (Kondo et al., 2013; Nagata et al., 2013; Umeda et al., 2021), with ASD being approximately four times more prevalent in boys than in girls (Maenner et al., 2020), whereas social anxiety is more likely to be experienced by women than by men (Asher & Aderka, 2018). Thus, the sample included in our study may be biased because of overlapping psychiatric disorders and cultural influences, which could have influenced the findings regarding their functioning. For example, a recent report has shown that individuals with Hikikomori and ASD exhibited significantly higher levels of depressive and social anxiety symptoms, sensory sensitivity, and sensory avoidance than did those with only ASD (Yamada et al., 2023). At the same time, an association between ASD and anxiety disorders has also been reported. Over one-third of adolescents to older individuals with ASD have clinically significant anxiety (Uljarević et al., 2020). A systematic review found a 42% lifetime prevalence of anxiety disorder, including social anxiety, in adults with ASD (Hollocks et al., 2019). However, little is known about the association between ASD and comorbid (social) anxiety disorders and Hikikomori.
This study has several limitations. First, the variety of Hikikomori definitions may have resulted in the high heterogeneity among the studies. Given the lack of systematic findings, this study used more tolerant conditions for the analysis. However, further research using more rigorous Hikikomori conditions is warranted to understand the functioning in individuals with Hikikomori. Second, although the inclusion of non-standardized measures in the meta-analysis allowed us to examine the trends in functioning in many studies, it may have reduced the quality of the studies. Thus, researchers should conduct case-control studies to identify trends in Hikikomori functioning. Importantly, the study results do not necessarily indicate a causal relationship between Hikikomori and disabilities in daily functioning. Due to the purpose of this study, which was to examine a wide variety of functioning in individuals with Hikikomori and lack of previous studies, a detailed examination of temperament/personality and daily life/social life in more subcategories could not be performed.
Conclusion
Individuals with Hikikomori had significantly higher psychiatric symptom levels with moderate-to-high effect sizes than did individuals without Hikikomori and even clinical controls alone. However, the results should be interpreted with caution due to the high heterogeneity among the studies. Furthermore, the communication and interpersonal interactions among individuals with Hikikomori were significantly maladaptive, with moderate effect sizes. Daily life, social life, and family communication and interpersonal interactions did not show clear differences between the groups. Clinicians’ attention to assessing whether patients with psychiatric disorders would have comorbid Hikikomori conditions could help understand their level of functioning, including mental and interpersonal functioning.
Supplemental Material
sj-docx-1-isp-10.1177_00207640241310189 – Supplemental material for Functioning, disability, and health of individuals with Hikikomori (prolonged social withdrawal) and their families: A systematic review and meta-analysis of case-control studies
Supplemental material, sj-docx-1-isp-10.1177_00207640241310189 for Functioning, disability, and health of individuals with Hikikomori (prolonged social withdrawal) and their families: A systematic review and meta-analysis of case-control studies by Shunsuke Nonaka, Hiroaki Kubo, Tomoya Takeda and Motohiro Sakai in International Journal of Social Psychiatry
Supplemental Material
sj-docx-2-isp-10.1177_00207640241310189 – Supplemental material for Functioning, disability, and health of individuals with Hikikomori (prolonged social withdrawal) and their families: A systematic review and meta-analysis of case-control studies
Supplemental material, sj-docx-2-isp-10.1177_00207640241310189 for Functioning, disability, and health of individuals with Hikikomori (prolonged social withdrawal) and their families: A systematic review and meta-analysis of case-control studies by Shunsuke Nonaka, Hiroaki Kubo, Tomoya Takeda and Motohiro Sakai in International Journal of Social Psychiatry
Supplemental Material
sj-docx-3-isp-10.1177_00207640241310189 – Supplemental material for Functioning, disability, and health of individuals with Hikikomori (prolonged social withdrawal) and their families: A systematic review and meta-analysis of case-control studies
Supplemental material, sj-docx-3-isp-10.1177_00207640241310189 for Functioning, disability, and health of individuals with Hikikomori (prolonged social withdrawal) and their families: A systematic review and meta-analysis of case-control studies by Shunsuke Nonaka, Hiroaki Kubo, Tomoya Takeda and Motohiro Sakai in International Journal of Social Psychiatry
Footnotes
Author contributions
Nonaka Shunsuke: conceptualization, data curation, formal analysis, funding acquisition, investigation; methodology, project administration, resources, visualization, writing–original draft; writing–review, and editing; Hiroaki Kubo: conceptualization, investigation, methodology, resources, writing–review, and editing; Tomoya Takeda: conceptualization, investigation, methodology, resources, writing–review, and editing; and Motohiro Sakai: conceptualization, funding acquisition, investigation, methodology, resources, supervision, writing–review, and editing. All authors have read and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by JSPS KAKENHI grants (grant numbers 20K14199, 21H00951, and 23K12922). The funding source played no role in the study design; collection, analysis, and interpretation of data; writing of the report; or decision to submit the article for publication.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.