
Abstract
Few studies have addressed gender differences in autism in relation to functioning and across cultures. We aimed to explore functional gender differences in autism from a multidisciplinary, global perspective using the International Classification of Functioning, Disability, and Health. Perceptions among professionals in high-income countries and middle-income countries were examined based on qualitative survey data from N = 225 professionals. Of these, n = 131 professionals provided information on functional gender differences in autism. Thirty-two professionals reported perceiving no gender differences. Remaining respondents (n = 99)—representing 31 countries, all World Health Organization regions, and 10 different professions—were included in a content analysis on functional gender differences, which generated three main categories and 13 subcategories. The subcategories were subsequently linked to International Classification of Functioning, Disability, and Health categories. Autistic males were described as displaying more externalizing behaviors, and females as having more internalizing problems and being more socially motivated. Thirty-two International Classification of Functioning, Disability, and Health categories were identified, of which 31 were covered by the comprehensive Core Set for autism. Gender differences in core symptoms and co-existing problems were acknowledged by professionals from both high-income countries and middle-income countries, while differences in social behaviors, including camouflaging, were more frequently described by experts from high-income countries.
Lay abstract
In this study, we explored if professionals working with autistic people in different regions of the world perceive differences between females and males diagnosed with the condition. A total of 131 professionals responded to a survey that included an open question about gender differences in autism. Of these, 32 responded that they do not perceive gender differences in autism. The information provided by the other 99 experts was analyzed to identify common patterns. Three main differences were found, (1) Matching the clinical conceptualization of autism where professionals described differences in core symptoms of autism, and that autistic females were less similar to the conceptualization of autism. In (2) Co-existing problems, professionals described that autistic males display more apparent problems including hyperactivity, while autistic females were perceived as having more internalizing issues such as anxiety and eating disorders. In the last category, (3) Navigating the social environment, experts perceived autistic females as more socially motivated, and more inclined to camouflage social difficulties, making their challenges less evident. Professionals also perceived differences in the social environment, for example, that autistic girls receive more support from their peers while autistic boys are more often bullied. Our results suggest that professionals working in different parts of the world acknowledge gender differences in autism, but also that there might be some regional differences. Finally, we found that gender differences reported by the international professionals could largely be assessed with a shortened version of the International Classification of Functioning by the World Health Organization, specifically developed for autism.
Keywords
Introduction
Autism spectrum conditions (henceforth autism) are associated with limited outcomes in a multitude of functional domains, including general adaptive capacities (Kenworthy et al., 2010), education, employment, and relationships (Howlin & Moss, 2012), as well as lower quality of life, somatic complications, and premature mortality (Hirvikoski et al., 2016; Jonsson et al., 2017; Pan et al., 2020). Increasing evidence suggests that gender influence underlying neurophysiology, behavioral phenotype, and functional outcomes in autism (Cauvet et al., 2019; Hull, Petrides, & Mandy, 2020; Lai et al., 2015; Van Wijngaarden-Cremers et al., 2014). Phenotypic gender differences in autism may to some extent mirror gender differences found in the general population. For example, neurotypical females exhibit higher social motivation than neurotypical males (Head et al., 2014), which has also been found among autistic females when compared to male equivalents (Head et al., 2014; Sedgewick et al., 2016); whereas males in the general population display more externalizing behavior than females (Zahn-Waxler et al., 2008), similar to what has been reported for autistic people (Hiller et al., 2014; Mandy et al., 2012).
Nevertheless, some gender-related findings in autism appear to not simply reflect findings in the general population, warranting further research into the relation between autism and gender. For example, autistic women do not display the social cognition advantages in mindreading in comparison to autistic men that are found for women in the neurotypical population (Baron-Cohen et al., 2015; Isaksson et al., 2019; Wacker et al., 2017). In addition, contrary to what is found in their siblings, autistic females appear to have an advantage in executive functioning, specifically in cognitive flexibility, compared to autistic males (Bölte et al., 2011). As executive functions are associated with restrictive and repetitive behaviors (Mostert-Kerckhoffs et al., 2015), this may partly explain that less of such behaviors is observed among autistic females (Van Wijngaarden-Cremers et al., 2014). Furthermore, the female preponderance in the general population regarding internalizing problems such as depression and anxiety disorders (Rutter et al., 2003; Van Oort et al., 2009) is not consistently found among autistic people (Hudson et al., 2019; Kirkovski et al., 2013). However, the elevated risks of both suicide and suicidal behavior for autistic people as a group appear to be especially pronounced among autistic females (Hirvikoski et al., 2016, 2020), contrasting findings in the general population where males are at higher risk to die from suicide (World Health Organization [WHO], 2019).
To date, most studies have focused on gender differences in clinical phenotypes, although autism might be differentially associated with a wide range of areas of everyday functioning in females and males. The influence of environmental factors on autistic people might be dependent on gender, as parents may expect more socially desired behavior from girls than from boys (Holtmann et al., 2007) or interpret social difficulties in females as an expression of gender-normative shyness (Amr et al., 2011). In addition, the interaction with neurotypical peers might differ. Autistic boys are at higher risk of being explicitly rejected by peers, while autistic girls rather are overlooked (Dean et al., 2014). Furthermore, autistic females are reported to camouflage, that is, mask or compensate for social difficulties, more than autistic males (Hull, Lai, et al., 2020; Lai et al., 2017). Camouflaging has been characterized as strategies to manage mismatched demands from the social environment (Mandy, 2019), and has been associated with negative outcomes in mental health and well-being for autistic people (Cage & Troxell-Whitman, 2019; Hull et al., 2019). The person–environment fit has been suggested to be an important factor determining functioning for autistic people in general, where environmental factors such as overly high social communication demands or bullying will increase disability, while a tolerant social surrounding or a fitting workplace instead will facilitate abilities (Lai & Baron-Cohen, 2015). Even though most autistic people live in low- and middle-income countries (LMICs) rather than high-income countries (HICs) (Hahler & Elsabbagh, 2015), autism research from LMICs is sparse, likely hampered by multiple social, political, and economic factors (Bölte et al., 2018). Consequently, little is known about the generalizability of gender findings in autism from HICs to low-income countries and middle-income countries (MICs) and how gender differences in autism are perceived worldwide.
In order to better understand individual challenges and strengths of females and males on the autism spectrum, the interplay between the condition, personal factors (including gender), and environmental factors must be considered. The International Classification of Functioning, Disability, and Health (ICF), which was developed by the WHO, provides a standardized framework to describe and understand functioning from a biopsychosocial perspective (WHO, 2001; see Figure 1). Specifically, the ICF views an individual’s ability to execute tasks or actions and to participate in important areas of life as outcomes not only determined by alterations in body structures and functions, but also hindering and facilitating environmental and personal factors. Environmental factors include external influences, such as other people’s attitudes, societal norms, and the availability of support, whereas personal factors are internal influences, comprising factors that are not part of the condition but nevertheless impact functioning, such as gender, age, and education. The ICF enables information on concrete needs and possibilities, improving communication between autistic individuals and professionals, and guiding individual interventions (Bölte et al., 2019). Importantly, for this study, the functional perspective of the ICF provides means to understand gender differences in autism beyond core symptoms, including identifying environmental aspects that may pose barriers for autistic females or males. In order to support the utility of the ICF in daily practice, shortlists of ICF categories (Core Sets) relevant to specific conditions, including autism, have been developed. The comprehensive ICF Core Set for autism consists of 111 second-level ICF categories: one body structure, 20 body functions, 59 activities and participation categories, and 31 environmental factors (Bölte et al., 2019) (see Supplementary Material for more information regarding the ICF and the Core Set for autism). While the ICF Core Set for Autism was developed using results from four preparatory studies, which included a large number of both males and females on the autism spectrum (Bölte et al., 2019), its usefulness in assessing functional gender differences in autism, and specifically its usefulness for assessing the female phenotype, is yet to be investigated.
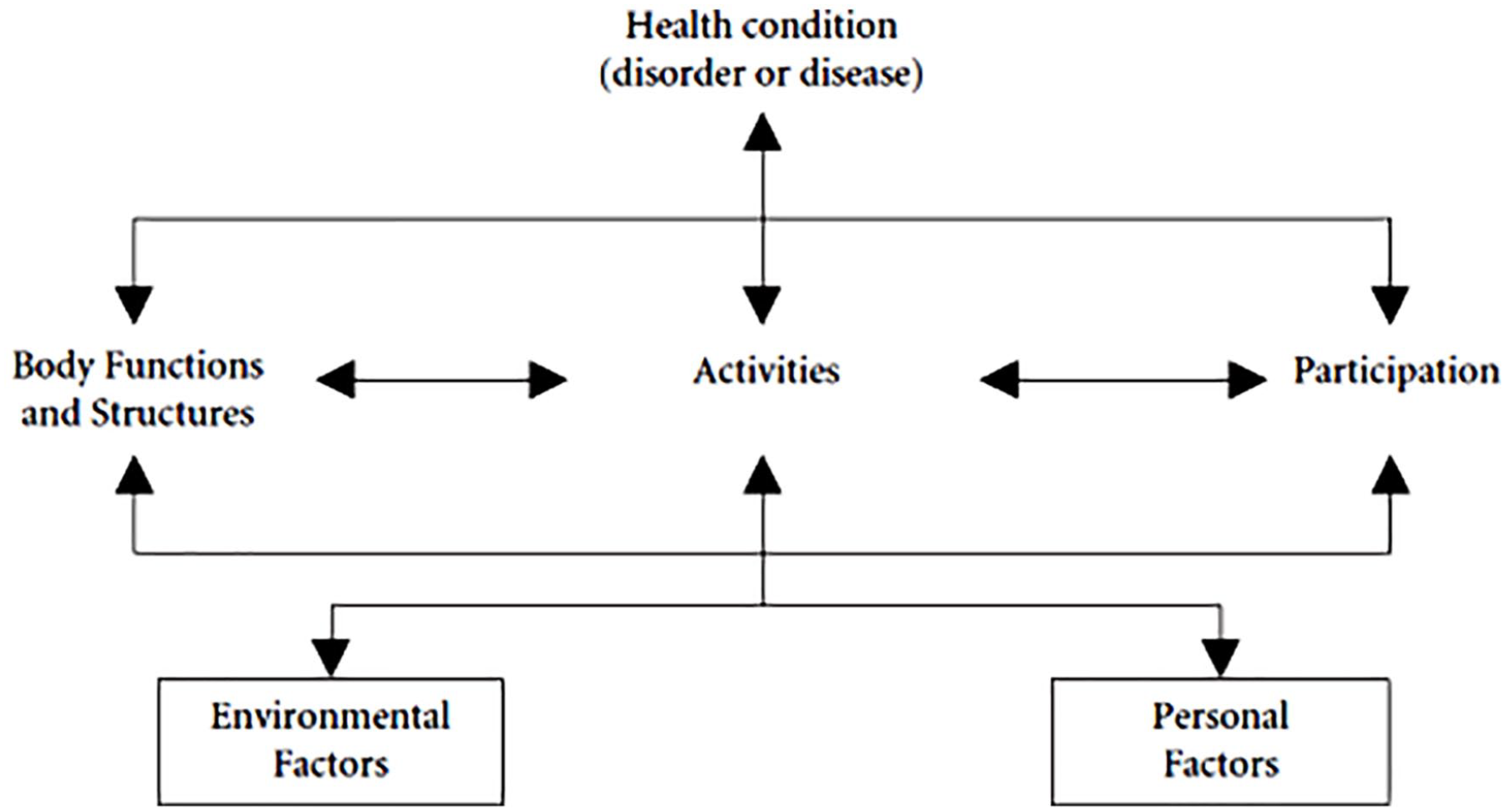
The ICF biopsychosocial model of functioning (WHO, 2007).
To conclude, gender differences in autism have attracted increasing research attention, yet there is a paucity of studies exploring gender differences in functioning, also taking into account the role of the environment in influencing autistic females and males. Furthermore, the majority of autism research has focused on data from HICs, while less is known about other parts of the world. Therefore, the aim of this study was threefold: first, to explore the perception of functional gender differences in autism in an international group of professionals; second, to investigate to what extent aspects of functioning pertaining to the female autism phenotype are covered in the ICF Core Sets for autism; and third, to explore similarities and differences in the perception of functional gender differences among professionals in HICs and MICs.
Method
Participants and procedure
This study was approved by the regional ethical review board in Stockholm. An international group of autism professionals participated in an email survey (collected from September 2013 to October 2014, see Supplementary Material for a further description) providing their perception of functioning among autistic individuals, as part of the development of the ICF Core Sets for autism (de Schipper et al., 2016). Contact information of autism experts was collected via the ICF Core Set steering committee (comprised of key opinion leaders in the field of autism from all six WHO regions), via an Internet search and via requests to academic or community-based centers, clinics, and university departments involved in autism education, treatment and research around the world. In addition, snowball sampling was used where contacted experts were requested to recommend other eligible autism experts. To be eligible for the survey professionals had to (1) practice one or more of the following occupations: coach, counselor, nurse, occupational therapist, physician, physiotherapist, psychologist, psychotherapist, social worker, special educator, or speech-language pathologist; (2) have a minimum of 5 years of experience working with autism; and (3) be fluent in English. In total, 225 experts responded to the survey and were included in the original study (de Schipper et al., 2016). The survey included an open question about gender differences in functioning in autism: “In your experience with individuals with ASD, are there any aspects of their functioning and impairment that are specific to gender? If yes, please type your answer below” to which 134 (59.6%) of all participants responded to. Among these, three experts were excluded, two for providing unclear responses, and one for reporting meeting too few autistic individuals, yielding a sample of 131 professionals. Of these, 32 professionals (24.4% of valid responders) explicitly responded not to perceive any gender differences in autism. The remaining 99 professionals (75.6% of valid responders) were included in the qualitative analysis, representing 31 countries and all six WHO regions: Africa (n = 9), Eastern Mediterranean (Middle East and Northern Africa) (n = 4), Europe (n = 38), the Americas (North, Central, and South America) (n = 22), Southeast Asia (n = 12), and Western Pacific (including Far East and Australia) (n = 14) (see Supplementary Table 1). Participants were aged between 26 and 74 years, with a mean age of 47.7 years (standard deviation (SD) = 11.0), and the majority of the included respondents were female (77.8%). The participants had a median of 15 years of experience working with autistic individuals (range: 5–43 years). Most experts reported either working mainly in the clinical field (45.5%), in education (15.2%), or in research (12.1%). A small proportion of experts (4.0%) reported working mainly in management (e.g. managing a clinic), or worked in other fields (4.0%), such as training or supervision of professionals. Remaining respondents (19.1%) worked in more than one field, often combining clinical work with another field. Experts worked mainly with children (34.3%), adolescents (1.0%), or both (45.5%), with both adolescents and adults (2.0%), adults (4.0%), or with autistic people across the lifespan (12.1%) (one participant did not report the age group he worked with).
To allow comparisons between HICs, low-income countries, and MICs, experts were grouped based on the country they worked in, using the World Bank classification of low-, lower-middle, upper-middle, and high-income economies (The World Bank, 2019). The World Bank data from calendar year 2013 were used in order to be most representative of the time point of the data collection. Among the 31 countries represented in this study, 23 were classified as HICs (n = 71 professionals, 71.7%), four as upper MICs (n = 14), and four as lower MICs (n = 14). Upper and lower MICs were collapsed into one MIC group (n = 28, 28.3%) (Table 1).
Representation of experts in HICs and middle-income countries.
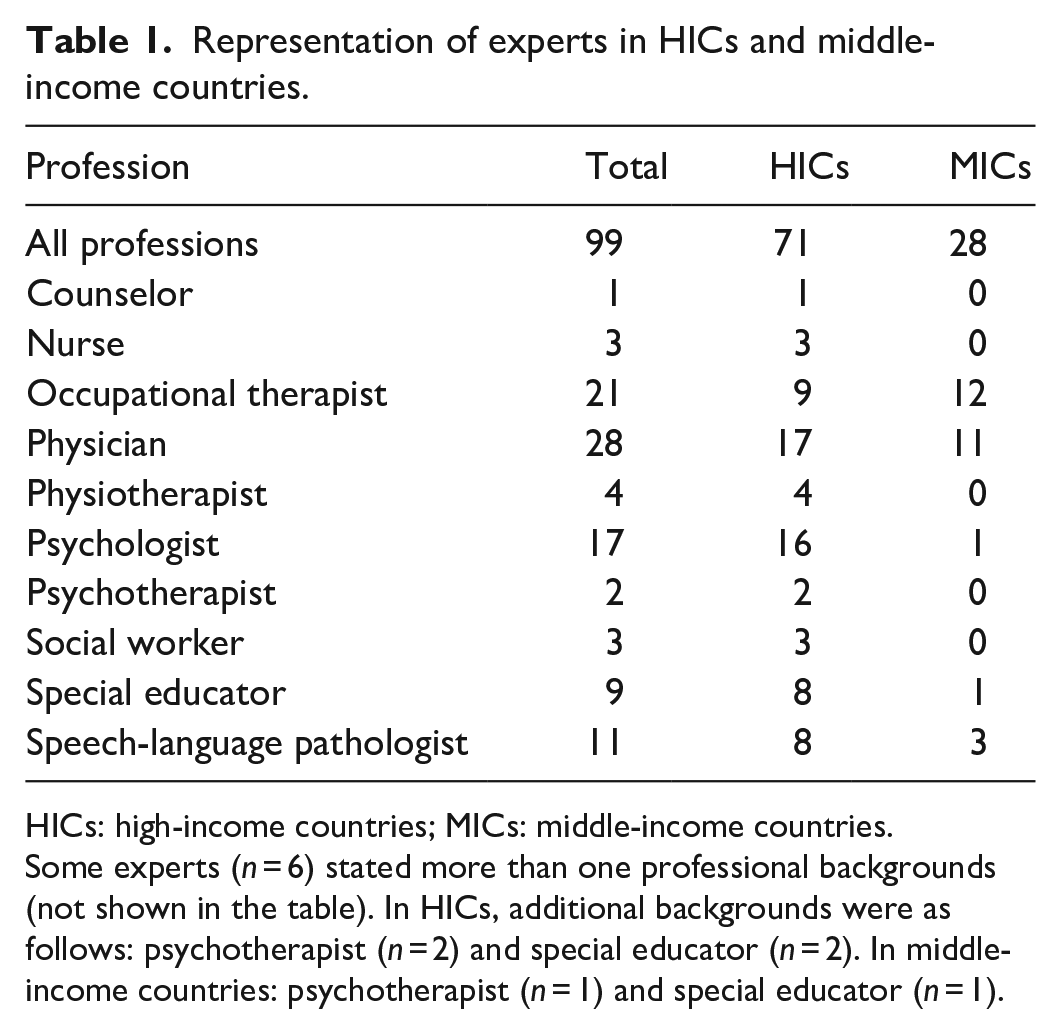
HICs: high-income countries; MICs: middle-income countries.
Some experts (n = 6) stated more than one professional backgrounds (not shown in the table). In HICs, additional backgrounds were as follows: psychotherapist (n = 2) and special educator (n = 2). In middle-income countries: psychotherapist (n = 1) and special educator (n = 1).
The 91 experts who did not respond to the gender question were comparable to the included experts regarding gender (76.9% females), mean age (47.3 years, SD = 10.8), years of experience (median: 15, range: 5–40 years), and profession, where the most common were physician (24.2%), occupational therapist (22.0%), physiotherapist (15.4%), and psychologist (14.3%). In this group, experts mainly worked with children (40.7%), adolescents (2.2%), or both age groups (34.1%). These experts mainly worked in the clinical field (46.2%), in education (15.4%), or in research (9.9%). The majority of these experts worked in HICs (67.0%), while a smaller proportion reported that they worked in MICs (25.3%) or a low-income country (1.1%) (6.6% did not provide a country that could be categorized).
Among the 32 experts responding no to the question, the majority were female (75.0%), the mean age was 45.4 years (SD = 10.5) and the median experience with autistic individuals was 13.5 years (range: 5–25 years). The most common professions were occupational therapist (28.1%), psychologist (18.8%), speech-language pathologist (15.6%), and physician (12.5%). Most experts in this group reported working with children (37.5%), adolescents (3.1%), or both age groups (37.5%). The majority of these experts reported that they worked in the clinical field (43.8%), in education (12.5%), or in research (9.4%). Of these experts, 59.4% worked in HICs and 40.6% in MICs.
Analysis
In the first step, a qualitative content analysis was conducted focusing on the manifest (explicit) level of the qualitative data (Bengtsson, 2016; Elo & Kyngäs, 2008). The analysis was conducted with an inductive approach, meaning categories were developed from the data as guided by the process of analysis described by Bengtsson (2016). Two of the authors (K.L. and S.M.) (1) read and re-read the material independently in order to familiarize with the qualitative data, and subsequently read through the data set word by word identifying meaning units, that is, sequences of text covering aspects related to the research question. The meaning units were labeled with codes (open coding). (2) The data set was read through alongside the list of codes in order to identify relevant sequences of text that were previously not coded. (3) Categories were developed by clustering codes with similar meanings, and based on similarity or dissimilarity, the subcategories were grouped under main categories. (4) Categories were refined, and renamed to describe their content. Any inconsistencies in interpretation throughout the analysis were solved through discussion until consensus was reached. (5) The categories were then checked against the entire data set to ensure that it represented the information in the data set, and to include any relevant data not previously covered in any category. (6) The two senior authors (J.I. and S.B.) audited the categories and coded data, and subsequently, the structure of categories was revised. In the results, coded meaning units are presented with added context when needed, and the quotes are labeled with the professionals’ study IDs (P01, P02, and so forth), occupation, and WHO region. To signify how many participants that referenced different aspects within subcategories, the following descriptive terms are used in the results: a few (2–4 participants), some (5–9), and several (10–20).
In the second step of the analysis, subcategories derived from the content analysis were linked to second-level ICF codes using a deductive approach in order to allow comparison with codes included in the ICF Core Set for autism (Bölte et al., 2019). Linking the results from the qualitative analysis to the ICF entails multiple advantages in our study. In addition to assessing the extent that gender differences in autism are covered in the ICF Core Set for autism, the ICF linking is a means for systemizing and standardizing information on functioning allowing comparison with results from other studies using the ICF framework. We used the Child and Youth version of the ICF, the ICF-CY, as it encompasses all categories of the ICF as well as additional categories pertinent to developing individuals (WHO, 2007). One author (S.M.) was trained in ICF linking by the ICF research branch. To avoid potential biases in interpretation, linking was conducted by two researchers (S.M. and K.L.) using a consensus approach. These authors read through all meaning units within the subcategories and discussed eligible ICF codes that represented each subcategory, linking subcategories to ICF codes. The ICF linking followed established linking rules from the ICF Research Branch (Cieza et al., 2002, 2005, 2019), that is, concepts within each category were linked to the most precise ICF code (ICF level 2 or 3), and when needed, converted to the second level code to allow comparisons with the ICF Core Set which consists of second level codes. Subsequently, the agreement of linked second level ICF categories with the Comprehensive Core Set for autism was examined.
Content analysis was conducted using version 11 of the NVivo software. R statistical software (version 3.6.3) was used for the quantitative analyses. In order to explore similarities and discrepancies in perceptions of functional gender differences in autism between professionals in HICs and MICs, the proportion of professionals in each group referencing main and subcategories was compared. Two-sided Fisher’s exact test was used for the comparisons, with a Bonferroni adjusted alpha level (α = 0.05) set to p = 0.003 (0.05/16) to account for multiple significance tests. In addition, the participants included in the content analysis (n = 99) were compared to the group of participants responding that they did not perceive any gender differences (n = 32), as well as to participants who did not respond to the question (n = 91), regarding age and years of experience, as well as proportion female or male, working in HICs or LMICs, working with children/adolescents or adults/across the lifespan, working in the clinical field or in other fields, and the proportion working in the three most commonly represented professions (physician, occupational therapist, psychologist). For continuous variables, an independent t-test was used for normally distributed data (expert age) and the Wilcoxon rank sum test for non-normally distributed data (years of experience). Chi-square tests were conducted to analyze the remaining categorical variables.
Results
The inductive content analysis yielded three main categories encompassing 13 subcategories that captured the professionals’ perception of gender differences in functioning among autistic individuals: (1) Matching the clinical conceptualization of autism, (2) Co-existing problems, and (3) Navigating the social environment (see Figure 2 for main categories and subcategories, and Supplementary Table 2 for examples of coded meaning units). The categories are described below with representative quotes.
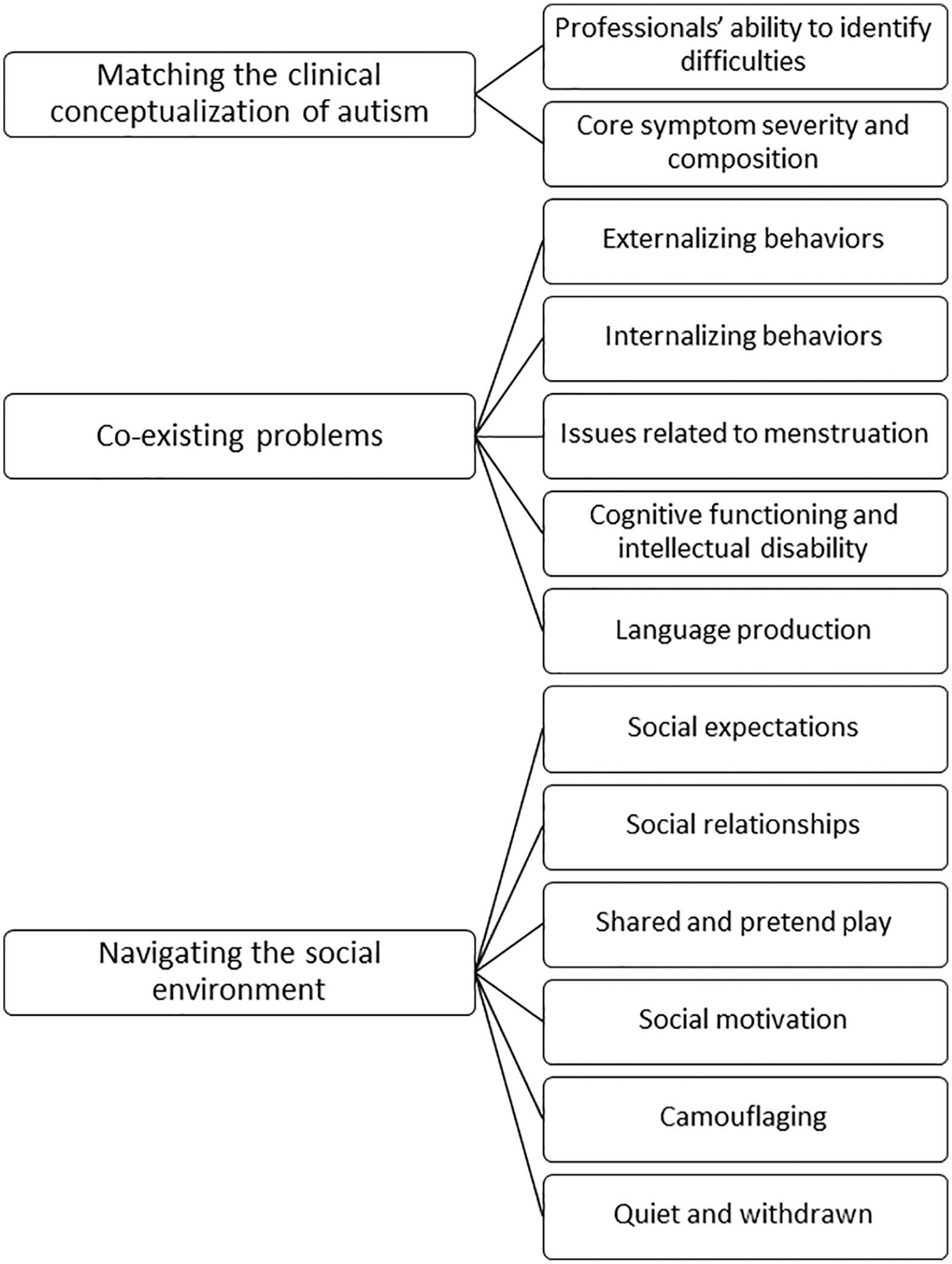
Main categories and subcategories.
Matching the clinical conceptualization of autism
This category reflects how respondents described their own and other professionals’ ability to identify autism in females and males, as well as how experts perceived gender differences in severity and presentation of the core symptoms of autism.
Professionals’ ability to identify difficulties
Participants described gender as a factor influencing the diagnostic process. Autism symptoms in females were seen as more difficult to recognize than symptoms in males, and some experts described that male behavioral phenotypes correspond better to the criteria outlined in diagnostic manuals and the common conceptualization of autism. Several professionals stated that difficulties often were not as apparent in females. Increased sociability along with superficial social skills and the use of social camouflaging were suggested to make formal diagnosis of autism more challenging:
I think that the symptoms are often more evident in boys, correspond better with the manual. In girls, it may be harder to see the symptoms and you need to be more observant and dig deeper to see all difficulties. (P07, Physiotherapist, Europe)
Core symptom severity and composition
Professionals noted gender differences in both the severity and the composition of core social communication symptoms of autism. However, reports of gender differences for this domain were mixed. Several respondents expressed that aspects of social communication difficulties were less pronounced among autistic females, describing advantages in to-and-fro conversations and in communicating emotions, while autistic males were described as displaying greater social impairment and less awareness of their difficulties. In contrast, a few participants experienced that autistic females had greater social difficulties and were socially more inappropriate than autistic males. One account suggested that observations of higher severity in autistic females may be explained by underidentification of females with average-to-high intellectual abilities:
Overall, girls seem to be more affected in social communication but there is over-representation of girls with intellectual disability so I am not at all convinced that this is not an artifact of under-referral and under-diagnosis of girls. (P31, Physician, the Americas)
Experts also described gender differences in restrictive and repetitive behaviors. A few stated that restrictive and repetitive behaviors are generally fewer among autistic females, while three other participants suggested that the special interests of autistic girls and women generally focused on “less peculiar” topics that are more often shared with their peers, making them less deviant:
In my experience it is more common, compared with boys, that the interests of girls are focused on topics that are more often shared with peers. Hence these interests can be disregarded as interests and not special interest if the intensity of the interest, and the often more narrowed focus of the interest are not picked up on. (P64, Special education teacher, Western Pacific)
In contrast, one respondent perceived that autistic boys often display gender-normative obsessions in video games while same-aged autistic girls show interests that are less similar to interests among peers. Some professionals described that the topics of special interests mirrored typical gender differences in the general population or ascribed gender-normative interests to autistic males: vehicles, dinosaurs and video games; and females: animals, dolls, and fashion. Furthermore, one participant described that autistic males keep the same interest for a longer period of time, while females were described as switching topics of interests more frequently.
Several participants reported gender differences in overall autism severity. While one account specifically perceived that autistic females with comorbid intellectual disability display higher autism severity than their male counterparts, the others described that the autistic females they meet generally tend to be in “the more severe end of the spectrum”:
I have often observed that percentage of girls with ASD, having very severe form of autism is more than the boys even though more number of boys have autism. I have very rarely come across girls with mild features of autism. (P06, Occupational therapist, Southeast Asia)
Co-existing problems
Experts also described gender differences in co-occurring problems not part of the core autism behavioral phenotype, including externalizing/disruptive behaviors, internalizing problems, and intellectual disability.
Externalizing, internalizing, and issues related to menstruation
Males were described by several respondents to show more externalizing behavior patterns, including aggression and hyperactivity. One participant expressed that autistic females are at risk for going undetected due to acting well-behaved and displaying a lesser degree of challenging behavior. Furthermore, a few experts described autistic boys at higher risk for exhibiting inappropriate sexual behaviors such as self-stimulation of genitals among other people. The data also included mixed reports on self-harming, with a few respondents reporting higher incidence among autistic males while two participants reported the contrary. One expert expressed that increased externalizing behavior constituted a risk for negative consequences for autistic males, contributing to social isolation:
Boys tend to display more aggressive behavior and people find this extremely unacceptable socially. This results in them being more excluded from social environments. (P47, Physician, Africa)
Rather than acting out, some experts perceived that autistic females more often turn inwards and experience emotional distress, including anxiety and eating disorders. Problems related to menstruation were also described as an important area affecting functioning in autistic females by some respondents, with experts perceiving the menstrual cycle as challenging to manage for this group, sometimes leading to anxiety and even self-injury.
Cognitive functioning and intellectual disability
A few professionals described gender differences in the proportion of co-occurring intellectual disability, perceiving that autistic females more frequently have intellectual disability in addition to autism. Again, the survey revealed inconsistent perspectives here, with two other experts describing autistic females as to functioning higher intellectually.
Language production
A couple of experts expressed that autistic males display more difficulties in language production, being more affected in language development and speech, displaying slow speech and difficulties in finding words. Less pronounced problems with language and speech among females were also viewed as a barrier to the detection of autism in girls:
Boys seem to be more impaired related to language development and speech. I think that might be one reason girls may not be as readily diagnosed. (P41, Nurse, the Americas)
Navigating the social environment
This main category encompasses how professionals perceived the interaction between the social environment and female or male autistic individuals. The category comprises both factors that are environmental and those more related to the individual.
Social expectations
Professionals described that both autistic males and females struggle with fulfilling gender-related expectations. For autistic males, one account related the difficulties in fulfilling a male norm to performing physically in activities, and problems with clumsiness or dyspraxia. On the other hand, a few experts described that autistic females are subjected to higher expectations to act appropriately in social contexts and manage social interactions:
. . . social problems [among autistic females] are in many cases lesser than in males. On the other side social demands are higher on girls than on boys. (P80, Physician, Europe)
Social relationships
Professionals also described social relationships as an aspect of the social environment impacting autistic females and males differently. A few participants expressed that autistic girls were found to often have a friend and generally be better taken care of by their female peers, while autistic boys were characterized not only as more often lacking peer relationships, but also more frequently being subjected to bullying:
The girls have often some friend who take care for them at social aspect. I haven’t observed this behavior in male. This could be also the reason frequent cases of bullying of boys. The boys haven’t got their defender. (P66, Special educator, Europe)
Regarding intimate relationships, challenges faced by autistic males were characterized as difficulties in developing relationships and lacking intimate partners. For autistic females, problems in this area were related to the risk of being victim of sexual abuse, described by a few participants. These experts described that autistic females were at heightened risk due to increased motivation to search for intimate partners, for example, via the Internet, paired with difficulties in being assertive, uncertainties about how intimate relationships are formed, and in knowing when they are being subjected to abusive behavior:
Unfortunately we see many histories of chronic sexual abuse, often without the patients themselves even realizing that they are (unlawfully) abused. They have endured rape and sexual harassment because they were under the impression that this was one of the many other things in life that they don’t understand. (P13, Physician, Europe)
Shared and pretend play
Some participants reported differences in type of play and occurrence of shared play of autistic girls and boys. Autistic boys were described as engaging less in interactive play with others, while girls were perceived to be more interested in play with peers, and more likely to engage in pretend play, including play of social character. However, there was a discrepancy in how experts perceived the causes of these gender differences. While a few professionals argued that autistic females display behaviors that might look like pretend play by following learned play routines or acting out special interests in animals, another expert described that autistic girls may instinctively engage in pretend play with social elements:
Although we don’t see too many females with ASD it appears that the less severe children seem to have fairly intact pretend play skills especially with regards to dolls and activities of daily living routines. Many of the females almost instinctively “nurture” and pretend to care for dolls which is contradictory to the typical poor theory of mind and poor pretend play skills seen in children with ASD. The males don’t do this. (P04, Speech-language pathologist, Africa)
Social motivation
Autistic females were described by several professionals to display higher social motivation in comparison to male counterparts. Autistic females were reported to be more interested in people, show an urge to develop relationships, and find social interaction rewarding. The co-occurrence of an increased desire to take part in the social world along with the social difficulties associated with autism was reported to cause challenges for females on the autism spectrum:
We experience that females in general are more motivated towards social relationships than males. Females in general are not more competent in social interaction though. So it results often in more frustration and psychological distress when they do not succeed building relationships. (P51, Psychologist, Europe)
Camouflaging
Higher social demands from the environment and increased internal social motivation were described to contribute to autistic females using behaviors that mask or camouflage social difficulties. Several professionals described that females on the autism spectrum would imitate or copy social behavior conducted by others, such as classmates in school or fictional characters, and autistic girls were attributed with a higher capacity for imitation compared to autistic boys. Other reported behaviors included practicing facial expressions in front of the mirror or following inflexible patterns in conversations. Respondents argued that autistic females might be perceived as having less social difficulties due to the ability to present a more socially competent person on the surface level. Furthermore, a few respondents reported that camouflaging can lead to unwanted consequences for autistic females, resulting in exhaustion and experiences of presenting a false social self. When social difficulties were masked from other people, the expectations from the surrounding would not match the actual social ability of the autistic girl or woman, contributing to negative outcomes:
I can sometimes see girls who have social coping-strategies at a level that I seldom see in boys. These girls try hard to copy what others do (but without understanding why they do it) in order to fit in. They can play roles like an actor just because they are so eager to meet others expectations. This skill can make other people think that they have a better social ability than they have which make them vulnerable to stress and melt-downs when the social demands get too high. (P36, Special educator, Europe)
Quiet and withdrawn
Some experts also perceived autistic females as being more in the background, quiet and even passive in comparison with autistic males. In contrast, one account perceived females on the autism spectrum as talkative or even hyperverbal despite having equal levels of social communication difficulties as autistic males.
ICF linking and comparison to the ICF Core Set for autism
The subcategories from the content analysis were linked to ICF codes to investigate if functional areas where autistic females were described as differing from autistic males were covered by the comprehensive ICF Core Set for Autism containing 111 second-level ICF categories (Bölte et al., 2019). In total, 32 second-level ICF categories were identified among the categories, comprising 11 body functions, 13 activities and participation, and 8 environmental factors (Supplementary Table 3). Of the 32 identified second-level categories, 31 (97%) were covered in the comprehensive ICF Core Set for Autism.
Similarities and differences between HICs and MICs
Comparing perceptions of functional gender differences in autism between experts from HICs and MICs revealed similarities and discrepancies, see Table 2. While the proportion of professionals referencing the two first main categories and their subcategories were similar (Matching the clinical conceptualization of autism and Co-existing problems), the third main category, Navigating the social environment, was referenced more frequently by professionals from HICs compared to professionals in MICs (52.1% vs 14.3%, p < 0.001), as was the subcategory Camouflaging (23.9% vs 0.0%, p < 0.003).
Proportion of experts from HICs and middle-income countries included in the content analysis referencing each category.
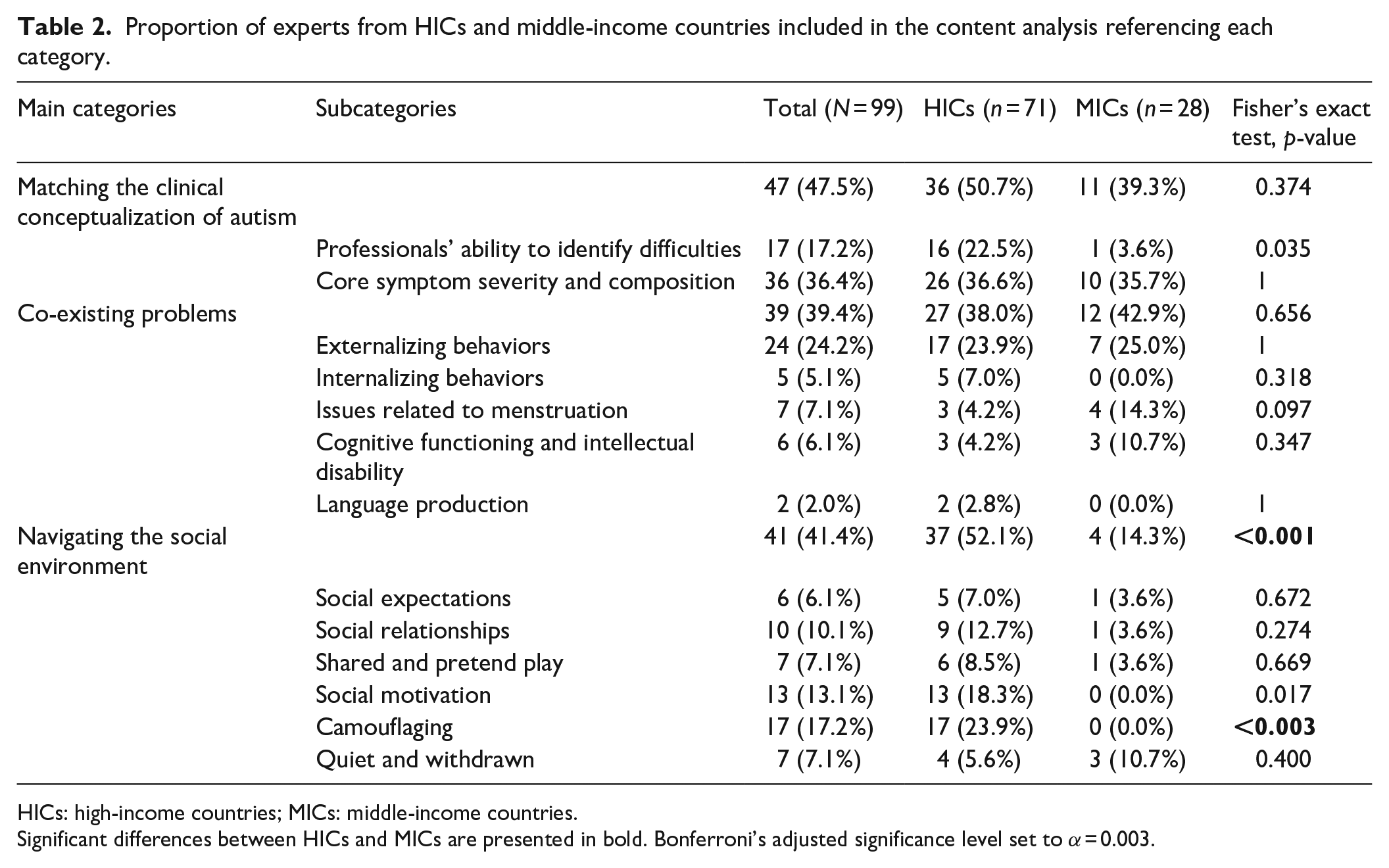
HICs: high-income countries; MICs: middle-income countries.
Significant differences between HICs and MICs are presented in bold. Bonferroni’s adjusted significance level set to α = 0.003.
Between-group comparisons
No differences were found when comparing the group included in the content analysis (n = 99) to experts responding that they did not perceive gender differences in autism (n = 32; denoted as comparison A), or experts who did not respond to the question (n = 91; comparison B) regarding group composition in proportion of females (A: 77.8% vs 75.0%, χ2 = 0.106, p = 0.745; B: 77.8% vs 76.9%, χ2 = 0.020, p = 0.888), proportion of experts working in HICs (A: 71.7% vs 59.4%, χ2 = 1.713, p = 0.191; B: 71.7% vs 67.0%, χ2 = 0.00005, p = 0.994), proportion of experts working with children and/or adolescents (A: 80.8% vs 78.1%, χ2 = 0.191, p = 0.662; B: 80.8% vs 77.0%, χ2 = 0.639 p = 0.424), or proportion working in the clinical field (A: 59.6% vs 59.4%, χ2 = 0.0005, p = 0.982; B: 59.6% vs 54.9%, χ2 = 0.419, p = 0.517). In addition, no differences were found regarding proportion working in the most commonly represented professions across groups: physician (A: 28.3% vs 12.5%, χ2 = 3.263, p = 0.071; B: 28.3% vs 24.2%, χ2 = 0.412, p = 0.521), occupational therapist (A: 21.2% vs 28.1%, χ2 = 0.655, p = 0.418; B: 21.2% vs 22.0%, χ2 = 0.016, p = 0.898), or psychologist (A: 17.2% vs 18.8%, χ2 = 0.042, p = 0.838; B: 17.2% vs 14.3%, χ2 = 0.297, p = 0.586). Also, groups did not significantly differ regarding mean age (A: 47.7 vs 45.4 years, t(124) = 0.973, p = 0.333; B: 47.7 vs 47.3 years, t(184) = −0.195, p = 0.846) or years of experience (A: median years: 15 vs 13.5, W = 1741, p = 0.053; B: 15 vs 15, W = 3978.5, p = 0.568).
Discussion
In this study, key aspects of professionals’ perceptions of functional gender differences in autism were identified. Experts perceived differences in the severity of core symptoms and correspondence with diagnostic manuals, in co-existing issues, and in the interaction between autistic individuals and the social environment. The presentation of autism among females was suggested to be more difficult to identify as autistic, and our results indicate factors that contribute to autistic females being perceived as displaying a lower level of disability, including having special interests in normative topics, displaying fewer externalizing problems, higher social motivation, and a more extensive use of camouflaging behaviors. Our findings corroborate results from a recent qualitative study conducted in the United Kingdom (Muggleton et al., 2019), reporting that clinical psychologists perceived differences in the presentation of autism, finding that autistic girls may appear more neurotypical on the surface level, for example, due to use of social camouflaging and having special interests in topics shared by their peers. All findings must be interpreted in light of the large proportion of experts who did not respond to the question (n = 91) or responded “no” (n = 32), representing 55% of the 225 professionals who responded to other questions on functioning in autism in the survey (de Schipper et al., 2016). The causes for lacking responses can only be hypothesized, a proportion likely corresponds to “no” as the question instructed experts to only respond if they did perceive gender-specific aspects of functioning. Furthermore, a proportion (n = 21) of the 99 experts included in the content analysis were not coded in any category, for example, due to being too vague, describing topics that were not referenced by other experts or focusing on the proportion of females and males they meet in their profession rather than gender differences. The above suggests that a proportion of professionals in both HICs and MICs do not perceive functional gender differences in autism. Comparisons between groups did not yield any significant differences between participants included in the content analysis and participants who responded no or participants who did not respond, regarding demographic characteristics. However, one difference was approaching significance, suggesting that the experts who responded “no” had slightly fewer years of experience than included experts (13.5 vs 15 years, p = 0.053). This could indicate that more experience increases the likelihood of observing gender-related characteristics in autism for professionals working with autistic people. Still, it should be noted that this difference did not reach significance. Other unmeasured factors might have contributed to the relatively large proportion of participants that did not describe any gender differences. First, participants may differ in awareness of gender-related issues in autism, which might reflect differences in education and training, where professionals who are not previously aware of gender differences might be less inclined to observe differences in their daily work. Second, for some participants, inexperience with autistic females might have influenced their response. Two “no” responders also added that they primarily worked with males, and similar statements were found among the respondents that were included but not coded in any categories in the content analysis. Third, an influencing factor could be the age group that professionals meet, for instance, higher incidence of restricted and repetitive behavior in males is not found among autistic preschoolers (Van Wijngaarden-Cremers et al., 2014). Fourth, a proportion of the professionals may primarily meet autistic females with pronounced severity and/or intellectual disability, limiting their experience with female autism phenotypes, as exemplified by references to females mainly being in “the more severe end of the spectrum.” Fifth, some professionals may not perceive subtle gender differences as meaningful in the everyday lives of autistic people. Yet another explanation is that ascertainment bias result in that primarily autistic females who resemble male phenotypes are diagnosed, reducing gender differences.
In the first main category, Matching the clinical conceptualization of autism, professionals perceived that autistic females display less peculiar special interests, in topics that are often shared with their peers, for example, revolving around animals and dolls, and change fixations more often, compared to males. Even when special interests mirror gender-typical interests in the neurotypical population, interests among autistic girls and women might be perceived as less characteristic for the conceptualization of autism, while gender-normative interests among autistic boys, such as video games, might be more readily recognized. Accordingly, Hiller and colleagues (2014) found that autistic females were more commonly rated by clinicians as having seemingly random interests, for example in animals, potentially less likely to be identified as atypical, compared to interest in screen time and video games that were reported more often for autistic males.
Our data also included descriptions of autistic females having a more severe presentation overall, which could be related to a previous notion of a female protective effect resulting in a more severe disability when autism occurs in females (Tsai et al., 1981). Another possibility is that these descriptions indicate underidentification of milder presentation in females, in line with research findings suggesting that autistic females are less likely to receive a clinical diagnosis of autism even when presenting symptom levels equivalent to males (Russell et al., 2011), and required to display more co-existing problems in order to be diagnosed with autism (Duvekot et al., 2017; Dworzynski et al., 2012).
Regarding Co-existing problems, while professionals perceived that autistic males display more conspicuous co-existing issues, such as disruptive behaviors and speech problems, autistic females were associated with less salient problems with anxiety and eating disorders. This contrasts previous research often reporting no gender differences in internalizing problems in autism (Hudson et al., 2019; Kirkovski et al., 2013). The lack of gender differences in previous studies could reflect power limitations as has been discussed by Hudson and colleagues (2019), and our results highlight that further sufficiently powered research is needed in this area. Still, if this perception does not reflect true gender differences, it might be influenced by gender biases associating internalizing problems more readily with females. In addition, it could be an indication that the perception of the less sociable and more externalizing male autism phenotype described in our results masks internalizing symptoms in males. Importantly, externalizing behaviors have been found to be more prominent among autistic children with increased internalizing problems (Kim et al., 2000), and our results could also suggest that autistic males struggle with showing or reporting internalizing problems, in line with what has been suggested for neurotypical males (Callahan et al., 1997).
The professionals’ perceptions encompassed in our third main category endorse emerging research evidence relating the female autism phenotype to increased social motivation (Head et al., 2014; Sedgewick et al., 2016). Our results indicate elevated interest in and need for social interaction and relationships among autistic females across the lifespan as this was described by professionals working with children, adolescents, and adults. Higher social motivation in autistic girls and women can be hypothesized to increase the likelihood of social opportunities with peers and reduce social isolation, providing learning opportunities for social communication skills. However, experts also perceived that autistic females engaging in the social world may not only experience more social failures but also suffer more from such experiences, compared with autistic males. The potential drawbacks of high social motivation and the associated risk of social failures among autistic individuals without intellectual disability have been pointed out previously (Lai & Baron-Cohen, 2015), and our findings corroborate that this could contribute to negative outcomes especially for autistic females.
Experts also described increased use of camouflaging among females on the autism spectrum in a wide age range. While aspects of camouflaging have been reported among female children (Rynkiewicz et al., 2016), adolescents (Tierney et al., 2016), and adults with autism (Hull, Lai, et al., 2020; Lai et al., 2017), not much is known regarding its developmental course. Our data indicate that elements may be present in early childhood for some autistic females, as one respondent observed camouflaging among girls in preschool age. In addition, our results are in line with previous research relating camouflaging to negative consequences for females on the autism spectrum (Bargiela et al., 2016; Cage & Troxell-Whitman, 2019; Hull et al., 2019), including exhaustion and experiences of presenting a non-genuine social persona. Experts related camouflaging to an increased likelihood of not being diagnosed, and to the environment not understanding the social difficulties of autistic females and therefore not adjusting the social expectations appropriately, that is, a poor person–environment fit (Lai & Baron-Cohen, 2015), which might contribute to the reported associations between social camouflaging with internalizing problems (Hull et al., 2019) and suicidality (Cassidy et al., 2018). Exploring the impact of both social motivation and camouflaging on outcomes in more detail might provide a deeper understanding of the mechanisms leading to negative consequences, for example, is camouflaging in itself causing problems with mental health, or is camouflaging to some extent mediating detrimental effects of social motivation?
Both males and females with autism were reported to struggle with gender norms, where gender-related preferences in social activity may result in different barriers for autistic males and females. Females with autism were described as struggling with higher expectations on social competence, whereas males were suggested to be hindered by social norms related to physical ability. While only referenced by one expert, this potentially illustrates a struggle for autistic boys with motor challenges, as being able to perform in team sports might be valued higher in male groups. Furthermore, gendered aspects of the environment regarding the access to support from peers and risk of bullying as well as challenges and risks associated with intimate relations were described. Our results thereby underline the influence of the environment in determining functioning for autistic individuals, and the importance of taking environmental factors into account when studying gender differences in autism.
While topics of gender identity and gender dysphoria in autism are currently receiving increasing research attention, it was only referenced by one of the professionals in this study and thus not developed into a subcategory. Autism is related to an increased likelihood of not identifying with the sex assigned at birth (Strang et al., 2014), and future research in gender and autism should acknowledge the diversity in gender identification in this group.
The majority of ICF categories (97%) identified in this study as being of relevance for gender differences in autism were covered in the ICF Core Set for autism, indicating its utility in covering important areas of functioning differing between autistic females and males. However, one ICF category identified in the linking process, “Strangers” (e345), was not covered in the Core Set. This environmental factor was linked to reports of autistic females being at risk for victimization when seeking to initiate relationships. This area is likely of importance for the safety of many autistic females, and might be related to the interaction of social motivation and social difficulties described in our data.
Two of the three main categories, Matching the clinical conceptualization of autism and Co-existing problems, were referenced by similar proportions of experts from HICs and MICs, indicating that professionals from both perceive common aspects of functional gender differences in autism. However, the third main theme, Navigating the social environment, revealed larger discrepancies. Here, the topic of camouflaging was referenced by a substantial proportion of experts from HICs (23.9%) indicating that they perceived this as an important aspect affecting functioning in autistic females, but was not described by experts from MICs. This might reflect actual differences in autism presentation between different regions, or that professionals working in HICs and MICs meet somewhat different groups of autistic people due to differences in identification and accessibility to services. Still, future research in female autism phenotypes needs to be conducted in other parts of the world in order to investigate whether previous findings generalize to low-income countries and MICs. The exploratory findings from our study should be interpreted with caution as the sample comprised substantially more experts from HICs, and in light of the limitations described below.
Limitations
Several limitations of our study need to be addressed. First, our results must be interpreted in light of the substantial proportion of experts who did not respond to, or responded “no,” the survey question. Second, although the sample included experts representing all six WHO regions and both HICs and MICs, there was a variation in the representation of each region. Potentially, a higher representation of professions, especially from MICs, could have provided perspectives that might be missing in our study. Still, the composition of our sample might to some degree reflect regional differences regarding which professions that meet autistic individuals in their profession. Furthermore, our qualitative analysis did not include experts from low-income countries, partly due to difficulties in identifying autism professionals, and the limited formal qualification status, in these countries. The generalizability of our findings to low-income countries is therefore uncertain. Also, while the sample represented professionals working with autistic children, adolescents, and adults, the majority of experts reported working with children and adolescents, potentially influencing the results to some extent, as autistic females are generally diagnosed later in life than autistic males (Giarelli et al., 2010). Thus, this could have limited the experience of autistic women in our sample. Third, we did not conduct member checks (respondent validation) to ensure credibility of the content analysis. However, we used multiple analysts and audits of the analysis to promote credibility in the interpretation of the data (Elliott et al., 1999). Furthermore, data saturation was not assessed during the recruitment process, yet as the analysis progressed we noticed that for several of the categories, additional responses did not convey new information. Fourth, the survey method yielded both limitations and strengths. The use of a single written question increases the risk of misinterpretation and unspecific responses that could have been clarified with follow-up questions in an interview. Potentially, the inclusion of additional questions could have clarified some of the responses that were included in the content analysis but not coded in any category due to being too vague. While it is true that a single survey question does not allow for deepened discussions with the respondents (hence influencing the depth of the qualitative data acquired), they are nevertheless deemed acceptable in qualitative content analysis (Bengtsson, 2016). Given the broad aim of our study, the email survey enabled us to collect information from a wider pool of international and multidisciplinary professionals, providing important and rare perspectives to gender research in autism. Potentially, participants might have been influenced by the wording of the question, asking for aspects of functioning specific to gender, in particular as a single survey question was used. Still, the qualitative data suggest that many of the experts interpreted the question as also covering subtle gender differences (e.g. autistic females “may be less likely to act out” or are in “general more competent in social imitation than males”). Fifth, as English was not the first language for several experts, proficiency in English has potentially influenced which professionals that participated in the survey, and the richness of the information participants provided. Finally, it should be noted that the professionals responded to the survey in 2013–2014, and perspectives among autism professionals might have changed slightly since then, for example, due to increasing awareness of the female autism phenotype and research interest in the topic.
On balance, our sample represents a rare cross-cultural professional perspective on functional gender differences in autism, encompassing not only professionals from HICs but also experts from lower and upper MICs. Furthermore, our study utilizes the experience of autism professionals working in different occupations with important roles in the services for autistic people, and provides a comprehensive view on gender differences, using a biopsychosocial perspective on functioning also comprising environmental aspects. Finally, ICF linking allowed systemization of the qualitative information and comparisons with the comprehensive ICF Core Set for autism.
Conclusion
In this study, we utilized international expert survey data to gain insights into professionals’ perception of functional gender differences in autism. We found in the content analysis that experts perceived the behavioral presentation of autistic females as harder to identify as autistic and not fully corresponding to the conceptualization of the condition outlined in the diagnostic criteria or to the common clinical understanding of autism. In addition, participants described several factors possibly contributing to autistic girls and women going undetected and being perceived as displaying less disability. Professionals expressed that autistic females, as compared to males, suffer more from internalizing behavioral problems, display fewer disruptive behaviors, behave more sociable, and often have some peer relations. In addition, they were described to display behaviors that make them blend into the social environment more, such as being quiet and withdrawn or by camouflaging. Professionals also expressed that autistic females and males face different facilitating and hindering environmental factors. The ICF linking revealed that nearly all of the linked categories were covered in the comprehensive ICF Core Set for autism, indicating that this shortlist of ICF categories can be used to assess functional differences between autistic females and males. The functional gender differences described were overall similar across HICs and MICs; however, references to the main category Navigating the social environment and subcategory Camouflaging were more frequently made by professionals from HICs.
Supplemental Material
sj-docx-1-aut-10.1177_1362361320975311 – Supplemental material for Functional gender differences in autism: An international, multidisciplinary expert survey using the International Classification of Functioning, Disability, and Health model
Supplemental material, sj-docx-1-aut-10.1177_1362361320975311 for Functional gender differences in autism: An international, multidisciplinary expert survey using the International Classification of Functioning, Disability, and Health model by Karl Lundin, Soheil Mahdi, Johan Isaksson and Sven Bölte in Autism
Supplemental Material
sj-pdf-2-aut-10.1177_1362361320975311 – Supplemental material for Functional gender differences in autism: An international, multidisciplinary expert survey using the International Classification of Functioning, Disability, and Health model
Supplemental material, sj-pdf-2-aut-10.1177_1362361320975311 for Functional gender differences in autism: An international, multidisciplinary expert survey using the International Classification of Functioning, Disability, and Health model by Karl Lundin, Soheil Mahdi, Johan Isaksson and Sven Bölte in Autism
Footnotes
Acknowledgements
The authors acknowledge the contributions made to the expert survey in the course of the development of the ICF Core Sets for autism that this study builds on. Contributions were made by the WHO, the ICF Research Branch, a partner of the WHO Collaboration Centre for the Family of International Classifications in Germany (at DIMDI), the International Society for Autism Research (INSAR), and colleagues at the Center of Neurodevelopmental Disorders at Karolinska Institutet (KIND) in Sweden, John E. Robison, Melissa Selb, Nidhi Singhal, Susan Swedo, Elles de Schipper, Petrus de Vries, Mats Granlund, Martin Holtmann, Sunil Karande, Omar Almodayfer, Cory Shulman, Bruce Tonge, Virginia V.C.N. Wong, and Lonnie Zwaigenbaum. The authors are grateful to all 225 international professionals who participated in the original survey.
Authors’ note
Sven Bölte is also affiliated to Region Stockholm, Sweden. Also, Bölte discloses that he has in the last 5 years acted as an author, consultant, or lecturer for Medice and Roche. He receives royalties for textbooks and diagnostic tools from Hogrefe, Kohlhammer, and UTB.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Swedish Research Council in partnership with FORTE, FORMAS, and VINNOVA (transdisciplinary research programs on child and youth mental health, grant no. 259-2012-24).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.