
Abstract
Introduction:
Mental health is essential for overall well-being, but it is affected by disorders such as depression and anxiety, which are highly prevalent both globally and regionally. The prevalence of these disorders has risen due to factors such as the SARS-CoV-2 pandemic, lack of adequate investment in mental health care, and the implementation of low-impact strategies.
Objective:
To establish the social determinants of health associated with the self-perception of sadness, depression, and/or anxiety in people in Colombia.
Results:
Heterogeneity was found in the predictive determinants between regions. The Amazon presented the regression model with the highest prediction (R2N = 0.650), while Orinoco had the lowest (R2N = 0.503).
Conclusion:
Among the social determinants associated with a greater risk of sadness, depression, and anxiety, those found to have a significant influence on emotional self-perception are female gender, stress, support networks, and social cohesion. Stress management and interpersonal relationship programs, comprehensive family care strategies, and community support should be strengthened. Furthermore, public policies should adopt comprehensive approaches that go beyond the biomedical paradigm.
Introduction
The World Health Organization (WHO, 2022) has defined mental health as ‘a state of mental well-being that enables people to cope with the stresses of life, realize their abilities, learn well and work well, and contribute to their community’. The global prevalence of mental disorders reached 13% in 2019, affecting 970 million people, with anxiety and depression being the most common conditions. Depression is characterized by affecting the way people feel, think, sleep, eat, and in general, how they perform in daily life (National Institute of Mental Health, 2024a), and anxiety consists of feelings of worry about different aspects of daily life, which can progress to a disorder when it occurs frequently and interferes with people’s daily lives (National Institute of Mental Health, 2024b).
Despite the impact of these disorders and the increase in their frequency in the 21st century, attributable not only to emerging environmental and technological factors but also as a subsequent effect of the COVID-19 pandemic (Expósito-Duque et al., 2024), investment in mental health worldwide represents on average less than 2% of national budgets. This ultimately leaves part of the population suffering from mental disorders without treatment, exacerbated by factors such as the quality of services, stigma, and discrimination (Pan American Health Organization, 2023).
In the Americas, the prevalence of mental disorders exceeds the world average, reaching 15.6%, which not only negatively affects people’s health and quality of life, as reflected in the years lost due to disability, but also generates economic losses for society, due both to the cost of care and the decrease in productivity (Pan American Health Organization, 2023).
In Colombia, the concept of mental health is defined by Law 1616 of 2013 as ‘a dynamic state that is expressed in daily life through behavior and interaction in such a way that it allows individual and collective subjects to deploy their emotional, cognitive, and mental resources to navigate daily life, to work, to establish meaningful relationships, and to contribute to the community’ (Ley 1616 de, 2013). The last National Mental Health Survey, which was carried out in 2015, revealed a prevalence of 2.4% of depressive disorders in the previous 12 months among adults aged 18 to 44 years and 1.3% in those aged 45 years or older (Ministerio de Salud, 2015). Subsequent research has indicated an increase in mental disorders in the country, highlighting the need to strengthen surveillance and monitoring. Although government efforts have been made to address this problem, gaps persist in regulations and care for people with mental illnesses (Cuellar Rivas, 2019; Rojas-Bernal et al., 2018).
People’s living conditions are directly related to their mental health (Handerer et al., 2022; Leiva-Peña et al., 2021), which underlines the importance of understanding the social determinants of health and their impact on the mental well-being of populations. Studies, such as ‘Clustering of Social Determinants of Health Among Patients’ (Schiltz et al., 2022), have pointed out how the social determinants of health are frequently grouped according to the demographic characteristics of individuals, highlighting the need to investigate how these groupings affect health.
Most of the existing research that seeks to understand the sociobiological interactions in mental health has been conducted in high-income countries, so its results cannot be extrapolated to Latin America. Given this, population studies are necessary to identify these situations in the biopsychosocial and community spheres. Only then can strategies be established that go beyond the biomedical paradigm and take into account the needs and characteristics of the population through mental health research, especially at the social level. Although progress has been made in this field in Latin America, there is still a long way to go (Gallego-Osorio et al., 2021; Holguín-Zuluaga et al., 2022; Leiva-Peña et al., 2021; Santamaría-García, 2023).
Therefore, the objective of this work is to establish the social determinants of health associated with the self-perception of sadness, depression, and/or anxiety in people in Colombia.
Materials and methods
A quantitative, cross-sectional study was carried out with a correlational phase and multivariate analysis, involving 2,725 adults residing in the different natural regions of the Colombian territory (corresponding to areas with similar climatic, geological, geomorphic, and relief characteristics). These regions include the Andean, Amazon, Caribbean, Orinoco, and Pacific regions, representing 34.7%, 18.2%, 16%, 15.7%, and 15.5% respectively. Each of these areas is made up of departments and, in turn, cities or municipalities.
To establish the sample size, the data obtained from the last population census of the National Administrative Department of Statistics (DANE) were used, for which the population figures by department were taken to calculate the estimate by region (DANE, 2019).
The sample calculation was made by geographic region using the formula:

A maximum type 1 error of 5% was established and adjusted to a loss percentage of 10% so that the sample was finally homogenized in all regions, requiring a minimum sample of 422 participants per region. However, the maximum number of responses received when the collection was completed in all regions was accepted, which explains the higher percentage in some regions.
The selection of the sample was non-probabilistic, casual, or fortuitous, where each participant contributed to obtaining more participants consecutively.
Permission was obtained to use DESOSA81, which has a content validity index of 0.909 and an internal consistency score of 0.952, for the measurement of social determinants of health (Holguín Zuluaga et al., 2024), but has not yet been used in any other study. The tool consists of 81 questions designed to evaluate 19 structural determinants and 62 intermediate determinants through 7 general dimensions, such as sociodemographic characteristics, educational level, occupation, and economic income. In addition, it includes 30 specific dimensions that explore more detailed aspects, such as physical activity, stress, violence, caring for others, and residential security.
Information about the project was shared with individuals and researchers from different parts of the country who agreed to participate in the study. The questions were created in Google Forms, and the link to complete the form was sent to these contacts who were then asked to share it with other people in their networks and thus generate chain participation.
The participation criteria were being over 18 years of age, voluntary acceptance of participation, and availability of time to complete the questionnaire.
Data collection was carried out between the second half of 2023 and the first quarter of 2024. To avoid eliminating responses, a confidence level was used. The researcher’s email was provided as a means of contact to answer questions or discuss other topics related to the instrument or the investigative work.
Data processing and information analysis were carried out with the Jamovi software. A univariate analysis was conducted using contingency tables. Then, by region, the likelihood ratio omnibus test was used to establish significant associations between the study variable and the other variables, and, finally, binary logistic regression models were generated with the variables identified as significant. The results obtained by each geographic region were compared synchronously.
The ethical principles established in the Declaration of Helsinki (The World Medical Association [WMA], 2013) were adhered to, and the Colombian standards and regulations for health research were followed, in particular, Resolution 8430 of 1993 (Resolución 8430, 1993). The study was classified as low risk and approved by the Bioethics Committee of the University of Caldas Faculty of Health Sciences as recorded in Act No. 011 of 2023. Informed consent was obtained from all participants before completing the questionnaire.
Results
The results are presented in three sections, as established in the analysis plan. Initially, a descriptive analysis of the structural and intermediate determinants is presented, followed by the bivariate analysis and ending with the logistic regression by region.
Structural determinants
The average age of the participants was 36.5 ± 14.54 years, 67.8% were women and 91.6% lived in an urban area.
The most common age range was 27 to 59 years old, of which most were women. Of the survey respondents, 4.4% identified as LGBTIQ and 3.9% had some degree of ethnic identification. The highest educational level achieved by 29.1% of the participants was secondary school, followed by postgraduate and technical or technological. More than 50% of the participants were formally employed and 45% were single. In terms of economic income, 31.6% earned more than double the current legal minimum wage, which for Colombia in 2024 is 1,300,000 pesos, while 30.8% earned less than the current legal minimum wage.
The Andean (44.6%) and Orinoco (16.5%) regions reported the highest percentage of LGBTIQ participants, while the Caribbean (33%) and Amazon (17.5%) stood out for their ethnic diversity. The Orinoco region had the highest percentage (42.9%) of participants with no education, while 49.8% of those with postgraduate studies were from the Andean region. The highest percentage of informal employment was reported in the Amazon and the Caribbean, while the Andean region presented the highest percentage of both formal employment and unemployment. In the Andean region, 40.2% of participants – the highest percentage of the group – had not received any economic income in the previous month (Table 1).
Structural social determinants of health in a study sample.

Source. Own elaboration.
Intermediate determinants
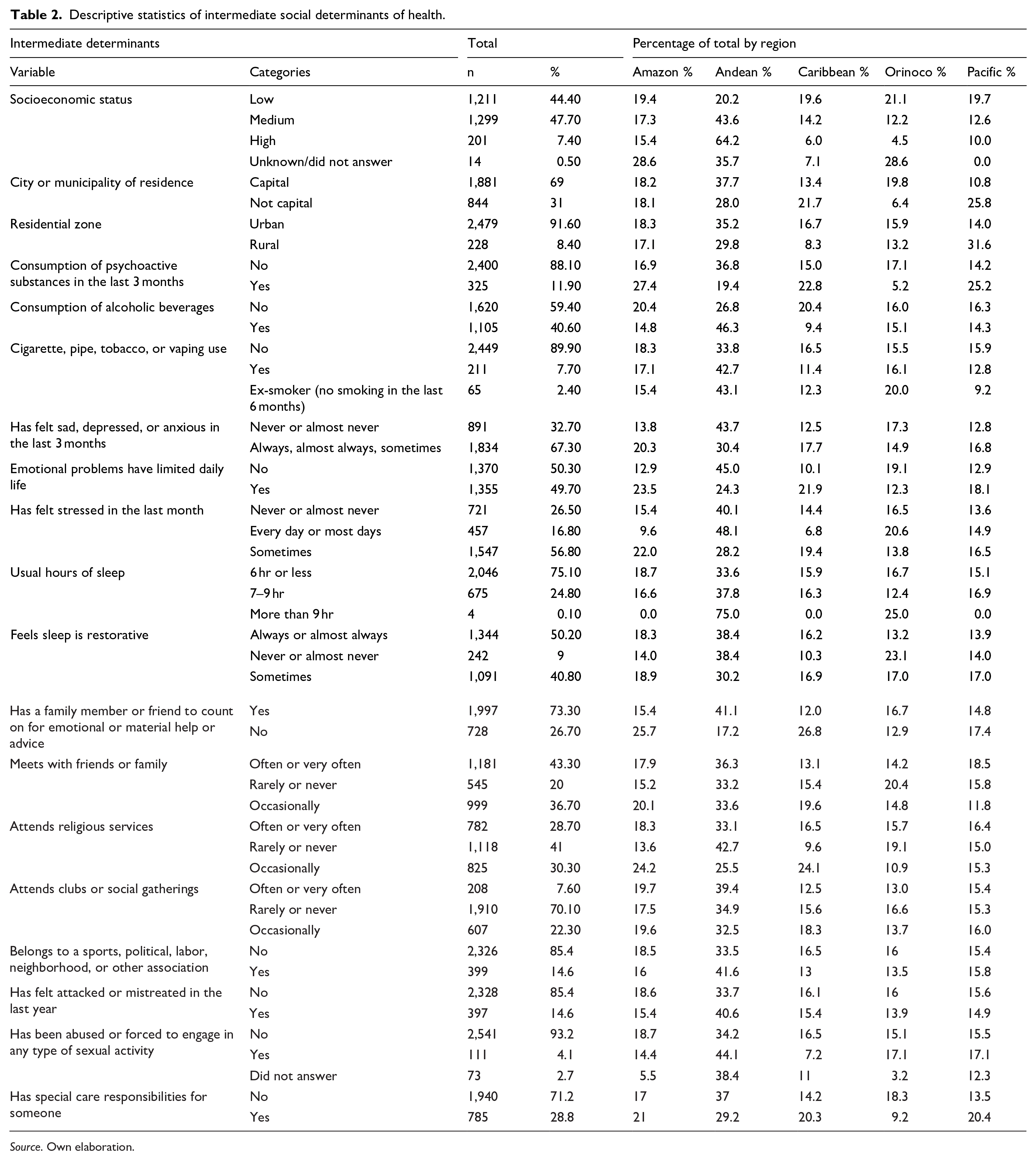
The predominant socioeconomic status was medium (47.6% of the sample), with 69% residing in capital cities and 91.6% residing in urban areas. The consumption of psychoactive substances exceeded 10%, the consumption of alcohol was below 50%, and the use of cigarettes, pipes, tobacco, or vaping was below 10%. The average sleep time for 75.1% of those surveyed was less than 7 hr a day, and 50.2% consider that their sleep is always or almost always restful. Regarding support networks, 73.3% had a close person to turn to if they needed help of any kind, 43.3% met frequently or very frequently with friends or family, while attendance at religious services or clubs occurred rarely or never (41% and 70.1% respectively). For 67.7% of the participants, feelings of sadness, depression, or anxiety occurred always, almost always, or sometimes in the last 3 months, while 49.7% reported that their emotional problems had limited their activities of daily living.
The highest percentage (64.2%) of participants with high socioeconomic status were found in the Andean region, while most (21.1%) of those with low socioeconomic status were in Orinoco. The Amazon region recorded the highest percentage of psychoactive substance consumption (27.4%), while the Andean region had the highest percentages of people using cigarettes (42.7%) and alcohol (46.3%).
The Orinoco region reported the lowest percentage of people with self-perception of sadness, anxiety, or depression (14.9%), while in the Amazon region, 23.5% of people indicated limitations in their daily life as a result of their emotional problems. In the Andean and Orinoco regions, none of the participants slept more than 9 hr a day, and these same regions reported the highest percentage of poorly restful sleep (38.4% and 23.1% respectively). The Amazon and the Caribbean were the regions with the lowest support network (25.7% and 26.8%) (Table 2).
Descriptive statistics of intermediate social determinants of health.
Source. Own elaboration.
Bivariate analysis
A bivariate analysis was performed to establish the association between the social determinants of health and the variable of self-perception of sadness, depression, or anxiety, to thus define the variables with statistical significance (p < 0.05) for the logistic regression model. For this step, the Chi-square association test was used as an omnibus test within which all the variables for each region were included to establish homogeneity in the comparison. Subsequently, variables without significance were progressively removed, starting with those with the highest p values, until those with p < 0.05 were left. The final results of the test are presented in Table 3.
Association between social determinants of health with self-perception of sadness, depression, or anxiety.

Source. Own elaboration.
Binary logistic regression model
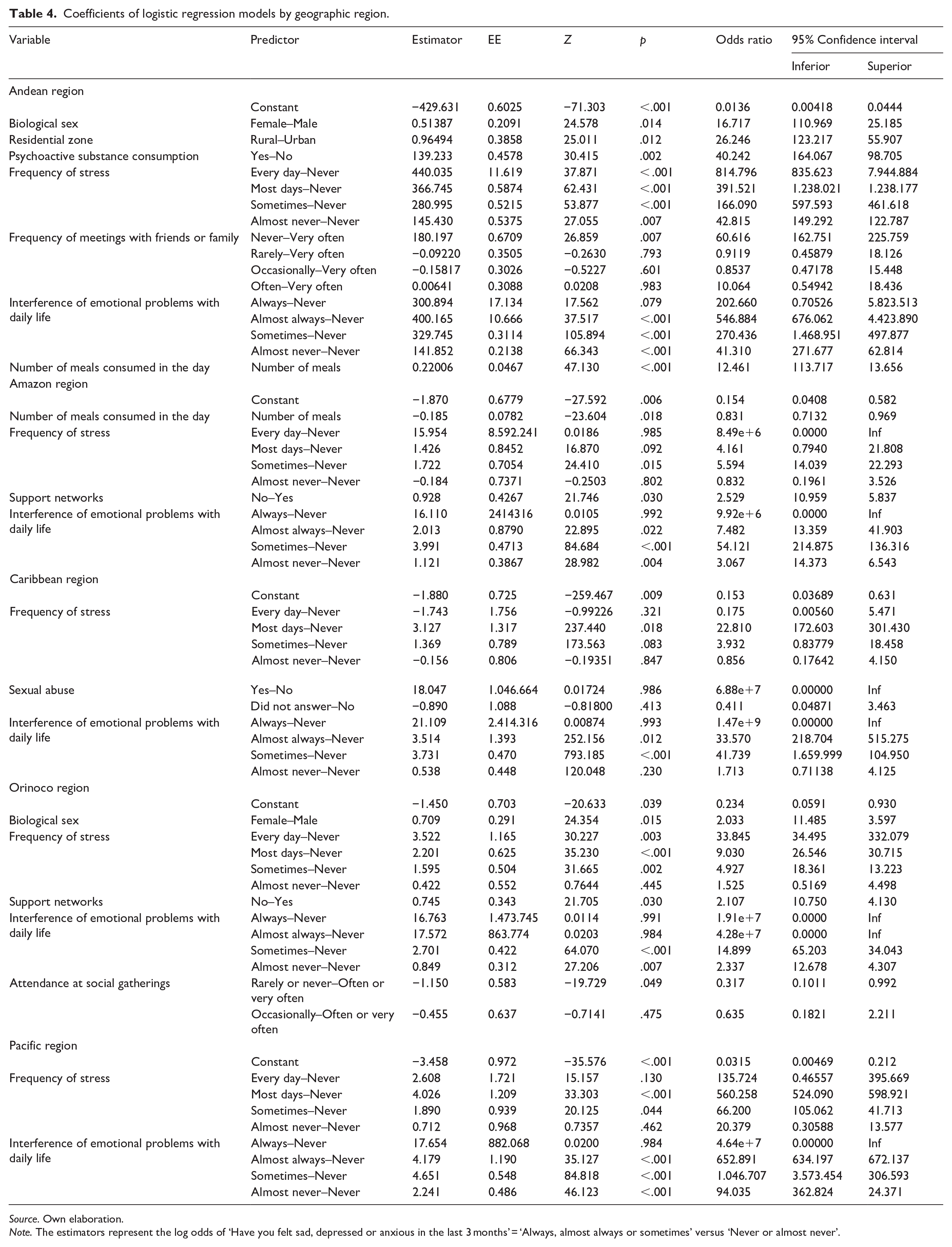
A logistic regression model was performed for each geographic region using the variables that presented statistical significance. The results are presented in Table 4. Note that the highest number of associated variables was observed in the Andean region, the frequency of stress occurred in all regions, and the Pacific region had the lowest number of variables with statistically significant associations.
Coefficients of logistic regression models by geographic region.
Source. Own elaboration.
Note. The estimators represent the log odds of ‘Have you felt sad, depressed or anxious in the last 3 months’ = ‘Always, almost always or sometimes’ versus ‘Never or almost never’.
In agreement with the bivariate analysis, the variables of stress and emotional interference with activities of daily living were found to have the highest odds ratio values in all regions. Notably, the latter variable was found to be the most dominant in terms of prediction, independent of the other variables. However, differences were noted in the other variables presented in each region. Thus, in the Andean region, people who consumed psychoactive substances in the last 3 months had approximately a 40 times greater risk of feeling sadness, depression, or anxiety compared to those who did not. There were no exclusive variables in the Amazon region, but the number of meals eaten during the day was a protective factor; for every meal eaten during the day, there was approximately 20% less risk of self-perceptions of sadness, depression, or anxiety. The Caribbean region was the only one to present statistical significance in the bivariate analysis with the sexual abuse variable; however, it loses significance within the model, as indicated by both the p-value and the confidence interval. In Orinoco, frequent attendance at social gatherings is a protective factor compared to non-attendance (RO = 0.317) and occasional attendance (RO = 0.635). Finally, in the Pacific region, no predictor variables other than those of stress and emotional interference with activities of daily living were identified.
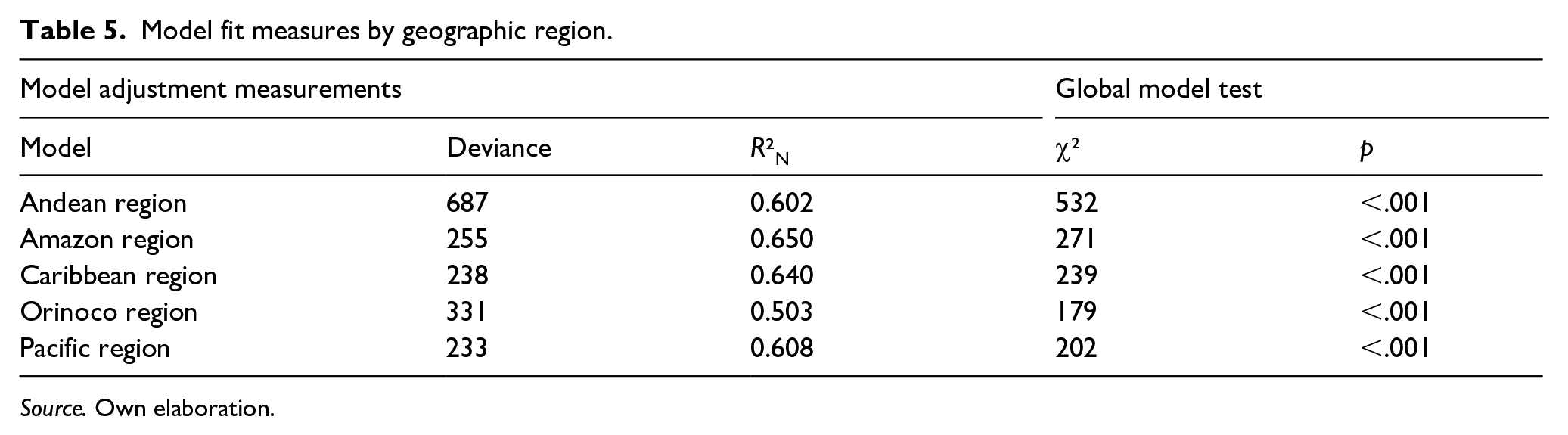
Despite the above, it must be considered that the degree of prediction is variable between each of the models (Nagelkerke’s R2), regardless of the number of variables included. Thus, the model with the highest percentage of prediction is that of the Amazon region (65%), while the lowest prediction occurs in Orinoco (50%). This is so, even though the Orinoco model includes five variables, compared to the Amazon region’s four. The results of the general model fit measures are presented in Table 5.
Model fit measures by geographic region.
Source. Own elaboration.
Discussion
The majority of research participants were female and of medium socioeconomic status with incomes more than double the legal minimum wage. Almost half of the participants (49.7%) indicated that emotional problems had limited their daily activities and 67.3% reported having experienced sadness, depression, or anxiety always, almost always, or sometimes in the last 3 months. These factors can be considered a risk for the diagnosis of depression, according to the criteria established by the DSM 5 Diagnostic Criteria Reference Guide (American Psychiatric Association, 2013/2014). However, it should be noted that these findings do not equate to a diagnosis of mental disorder, which must be made by a professional in the field. This study, with its social aspect, provides a preliminary approach to understanding the frequency of self-perceived depression or anxiety, as well as potential contributing factors.
Handerer et al. (2022) identified a series of factors that were considered social determinants of mental health, including safety and violence, food security, education, economic income, and social support, among others. Several of these variables were used in the present study to establish their relationship with self-perception of depression and anxiety.
Cabezas-Rodríguez et al. (2021) pointed out that the social determinants that influence mental health can vary between men and women, observing that men seem to be more influenced by employment, while, in women, marital status and domestic responsibilities are added. Coinciding with these findings, Cornejo-Espinoza et al. (2022) found that the suspicion of mental disorders was almost twice as high in women than in men, which was reflected in this research in the Orinoco and Andean regions (OR = 2,033 and 16,717 respectively). The results in the Cornejo-Espinoza study were attributed to the double workload present in the female group, a variable that was not included in this research, but which could be of interest for subsequent studies.
Zhou et al. (2023) found that women had a higher risk of depression compared to men. Likewise, they identified that unfavorable social determinants of health were associated with a greater risk of depression and that specific variables, such as employment and education, could account for this difference in the frequency of depression between men and women. These findings coincide with those reported by Peresini et al. (2024) in Argentina, who found a prevalence of depression or anxiety in women, especially those engaged in or exposed to physical or verbal violence. They also observed a lower risk among those with a higher educational level as well as among unemployed women.
Califf et al. (2022) sought to establish the association between the Patient Health Questionnaire-9 (PHQ-9) and social determinants of health, identifying that in addition to clinical and biological factors, other elements related to social determinants of health were associated with higher scores on the questionnaire. These included female sex, younger ages, people of color, low socioeconomic status, unemployment, and not being married. In this study, similar results were observed with the female sex as a prognostic factor in the Orinoco and Andean regions. However, other demographic and socioeconomic variables were not significant in the models and were consequently discarded.
King et al. (2022) found that none of the standard demographic variables were significantly associated with depressive symptoms, while variables such as self-reported health status, urban disturbance and neighborhood safety, and stress did present an association. These findings partially coincide with the results of this study, where stress was found to be a predictor variable in all regions, while among the demographic variables, only biological sex had priority in two of five regions. Similarly, Motsamai and Mhaka-Mutepfa (2022) did not find a significant association with sociodemographic factors, which is consistent with the King et al. study as well as this one.
Choi and Lee (2022) found indirect effects between socioeconomic level and depression, while interpersonal reserves such as self-esteem and self-perception of health status showed a stronger association, leading to the conclusion that it is important to develop actions to promote self-esteem and self-perceived health in general. In this study, self-perception of health status was one of the last variables to be eliminated from the models, so it could be considered to have some level of relationship. However, the presence of the stress variable in all regions suggests that promoting actions and programs that promote self-perception of health and stress management could contribute to reducing the self-perception of sadness, depression, or anxiety.
Sánchez-Moreno et al. (2024) found that older adults with less education and economic difficulties had a higher risk of depression. However, by incorporating variables associated with loneliness into their regression, they found that the other risks were significantly reduced, which is why they concluded that loneliness could help explain the role of economic inequalities in depression among older adults. This research supports those findings, as it identified the presence of support networks and the frequency of such contact as protective factors for the self-perception of sadness, depression, or anxiety in three of five regions. However, unlike the aforementioned study, this one was not limited to older adults. Similarly, according to Liang et al. (2012), divorced, separated, or widowed people had a greater risk of suffering from depression, as did those people with poor self-perceived health and little social cohesion. This reinforces the idea of working on pillars such as general self-perception and the formation and maintenance of support networks, for which Agudelo-Hernández et al. (2024) propose the implementation of support groups as a methodology for continuity in care and provision of mental health services.
Alibudbud (2023) found higher rates of depression and anxiety in the LGBTI population, and identified age as a protective factor for anxiety in this population, whereas for cisgender men, age was a risk factor. In contrast, none of the models in this study identified gender identity as a predictor variable.
Through a narrative review, Bernal Rodríguez et al. (2021) looked at social determinants of health associated with depressive symptoms or depression in older adults in Colombia, finding that low educational level, being a woman, low social cohesion, and chronic diseases were risk factors. These results agree with the findings of this research, which identifies female sex and low social cohesion as risk factors in the self-perception of sadness, depression, or anxiety.
Finally, and as Pathare (2023) reports, it is imperative to establish a global approach focused specifically on the social determinants of mental health, not only to meet political goals but to efficiently address the resulting disorders and their consequences on the general health of people, their families, and communities.
Conclusion
The study identifies and analyzes the social determinants of health associated with self-perception of sadness, depression, and anxiety in Colombia, revealing significant heterogeneity between regions. In general, female sex, elements of social cohesion, and self-perception of health are presented as predictive factors.
These findings underscore the need to develop sustainable program strategies that address the entire course of people’s lives and promote a positive self-perception of health and stress management at the individual level, family care, and strengthening of community support networks. Furthermore, public policies should adopt comprehensive approaches that go beyond the biomedical paradigm. This study not only contributes to science but also reflects the impact of inequities and social determinants of health on the mental well-being of populations.
Footnotes
Acknowledgements
This research derives from the macroproject of the University of Caldas, ‘Psychometric properties of the instrument for measuring the Social Determinants of Health, DESOSA 81’. The authors wish to thank the University of Caldas for its commitment to education by supporting research not only at the local level but also nationally, in line with global demands.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors wish to acknowledge that they have received financial support from the University of Caldas for the research and publication of this article.