
Abstract
Background:
Secure forensic hospital treatments are resource-intensive, aiming to rehabilitate offenders and enhance public safety. While these treatments consume significant portions of mental health budgets and show efficacy in some countries, their effectiveness in Czechia remains underexplored. Previous research has highlighted various factors influencing the likelihood of discharge from these institutions. Notably, the role of sociodemographic variables and the length of stay (LoS) in the context of forensic treatments has presented inconsistent findings across studies.
Methods:
The study, part of the ‘Deinstitutionalization project’ in Czechia, collected data from all inpatient forensic care hospitals. A total of 793 patients (711 male, 79 female and 3 unknown) were included. Data collection spanned 6 months, with tools like HoNOS, HoNOS-Secure, MOAS, HCR-20V3 and AQoL-8D employed to assess various aspects of patient health, behaviour, risk and quality of life.
Results:
The study revealed several determinants influencing patient discharge from forensic hospitals. Key assessment tools, such as HoNOS secure scores and the HCR-20 clinical subscale, showed that higher scores equated to lower chances of release. Furthermore, specific diagnoses like substance use disorder increased discharge odds, while a mental retardation diagnosis significantly reduced it. The type of index offense showed no influence on discharge decisions.
Conclusion:
Factors like reduced risk behaviours, absence of mental retardation diagnosis, social support and secure post-release housing plans played significant roles. The results underscored the importance of using standardized assessment tools over clinical judgement. A standout insight was the unique challenges faced by patients diagnosed with mental retardation, emphasizing a need for specialized care units or tailored programmes.
Keywords
Introduction
Treatment in secure forensic hospitals is a resource-intensive undertaking intended to rehabilitate those who have committed an offence, thereby increasing the general population’s security. For example, in the UK, 19% of the overall mental health budget is devoted to them and released patients show lower reoffending rates (Fazel et al., 2016). There needs to be more investigation into its effectiveness in Czechia as the total amount spent on forensic treatment is unknown. The current study addresses this by reporting on factors facilitating and impeding release from secure treatment.
Given the effort dedicated to forensic treatments, identification of critical variables that either contribute to or prevent discharge can help to maximize the effectiveness. Previous study on this topic in Czechia focused on only a sample of patients from one hospital in Prague (Páv, Sebalo, et al., 2022). The results showed that several patient-related variables, such as committing more than one violent crime, non-compliance with ward or therapeutic regimes, limited insight into mental health or high scores on HONOS secure scales, were associated with staying in treatment rather than being discharged. Although sociodemographic variables also differed between the released patients and those who were not, the results are very preliminary due to sample limitations and many tests. Given that the current study includes patients from all forensic hospitals in Czechia, we hope to validate and extend these results.
Similar patterns have been reported in other countries. In Germany, Ross et al. (2012) compared patients who were discharged from forensic psychiatric hospitals and those who were not. As expected, sociodemographic variables such as family and social life, work experience, lack of breaches in security and older age of first delinquency or admission were associated with the release. The analysis showed the difference between these two groups concerning the type of offence and diagnosis, with non-released patients having committed more severe crimes and a higher proportion of them having psychotic disorders. However, given the use of non-specific Chi-Square tests, the noted particularities of the differences require further confirmation. Likewise, In Sweden, Andreasson et al. (2014) have demonstrated that committing a violent index offence, being diagnosed with psychotic disorder, having a history of substance abuse, absconding and lower global functioning.
Crocker et al. (2014) reported similar results in in Canada. The severity of index offence, psychiatric history and non-compliance with medication was inversely associated with discharge. Furthermore, they investigated each diagnosis separately and found that having a psychotic spectrum disorder, non-mood spectrum axis one diagnosis, personality spectrum diagnosis and unspecified diagnosis increases the likelihood of continuing detention. Unlike Ross et al.’s (2012) study, where discharged and non-discharged patients did not differ in assaults on staff members or other patients, Crocker et al. (2014) found that violent behaviour significantly increased the likelihood of detention. Interestingly, the latter study also looked at the HCR-20 scales, which decreased the possibility of absolute discharge, but only historical and clinical had this effect on conditional discharge. Another study from Canada confirmed that violent behaviour in hospitals and worsening clinical presentation (e.g. unstable or inappropriate behaviour) were associated with remaining in secure hospitals (Hilton et al., 2022).
The importance of HCR-20 ratings was also confirmed by Kastner et al. (2022), who showed that clinical and risk management scales mainly predicted the board’s decision for provisional discharge. Davoren et al. (2013) investigated the predictive validity of different risk assessment tools, albeit in Ireland. Their results showed that higher global functioning of patients and lower symptom levels were predictive of conditional discharge. Interestingly, once separate items from HCR-20 were looked at, only some had a significant effect. Specifically, relationship and employment instability, mental illness and its acute symptoms, lack of treatment or supervision response, poor insight and absence of feasible plans were associated with detention rather than discharge.
The association of these variables with a probability of discharge is unsurprising. Symptoms of psychotic disorders, especially treatment-resistant ones as well as violent behaviour, have also been associated with longer stay in forensic hospitals (Andreasson et al., 2014; Davoren et al., 2015; Gosek et al., 2020, 2021; Páv, Vňuková, & Sebalo, 2022). The explanation for these findings is seemingly straightforward, as the aim of forensic hospitals is to rehabilitate both mental disorders and violent behaviour. Thus, non-remitting symptoms decrease the likelihood of discharge. However, these findings are not uniform. In the UK, Shah et al. (2011) found a direct association between psychotic symptoms and LoS but no association with a history of criminal behaviour. Most likely, this is due to the focus on past criminal behaviour rather than violent behaviour or non-compliance during the treatment. Concerning mental health symptoms, it is also important to note that prolonged LoS for patients with intellectual disabilities is not agreed upon. While Hare Duke et al. (2018) reported that patients with this diagnosis have more extended stays, Chester et al. (2018) found inverse results.
Given that both studies were conducted in the UK, the impact of intellectual disabilities on LoS and discharge should be investigated further. Especially, Gosek et al.’s (2020) study from Poland did not find any effect of this diagnosis. The need for closer inspection is echoed by Völlm et al. (2018), who note the inconsistencies in findings related to this variable yet point out that patients with intellectual disabilities often show more unmet needs than others, especially in non-specialized institutions.
The association of sociodemographic variables and LoS is slightly more transparent. The variables that reflect stability in the personal or future professional life of patients are associated with shorter LoS (Völlm et al., 2018). This trend explains why items from risk assessment tools indexing similar concepts, such as risk subscale from HCR-20, are higher in patients in the long term than in short-term treatments (Eckert et al., 2017). Such findings make intuitive sense as a stable environment is thought to provide positive support to patients upon release. However, other studies did not find this association (Andreasson et al., 2014; Davoren et al., 2015). Given the weight attributed to such items by parole boards (Kastner et al., 2022), this effect must be investigated further.
Consequently, the current study addresses these inconsistencies in previous research in Czechia. Thus, the study aims to identify the factors that facilitate and impede discharge from forensic treatment. Meanwhile, the secondary objective is to compare the functioning of forensic psychiatric institutions in Czechia and other countries.
Methods
Data collection process
This study was realized as part of the Department of Health’s ‘Deinstitutionalization project’, a ‘CENZUS’ survey. We gained data from all hospitals providing inpatient forensic care. We trained data-collecting staff in administering the HoNOS-secure and HCR-20 clinical item assessments. We used all available sources, including electronic hospital records, judgements and other health notes in patient files, patients and direct care staff information. There were two data collections 6 months apart.
Participants
To enrol the maximum number of participants, all inpatient forensic patients on 1.7.2021 got an offer to participate, and 36 refused. The original dataset included 841 patients from forensic psychiatric hospitals across Czechia. However, 48 patients had no data on their current disposition (discharged or remaining). Thus, the analysis was conducted on 793 patients (711 male, 79 female and 3 unknown). Within the Czech law system, only those with diminished or absent legal responsibility when committing a criminal act can be sentenced to forensic treatment (Páv et al., 2020).
Pathway definition
From the methodological point of view, enrolment of already community-transferred patients into the ‘discharge’ pathway is optimal. Our system requires no court approval to transfer patients between low or medium security levels within the hospital. Transfer to the community or the high security (in our conditions, ‘secure detention’) is a three-step process. First, the ward management level decides, followed by approval from the hospital consultant board. If these steps approve the transfer, a court proposal is filed and the transfer is realized with the court’s decision. According to Czech law, a reasoned proposal for continuation of treatment in the hospital, community transfer or another submission (transfer to security detention) must be presented every 2 years.
To account for the 6 months between data collections, we enrolled patients at any stage of the discharge process into the ‘discharge pathway’. The second pathway enrols all patients detained in the hospital, expecting prison or high-security transfer at any stage. Table 1 in the supplemental materials shows how this grouping was achieved.
Tools
The Health of the Nation Outcome Scales (HoNOS)
HoNOS is a widely used 12-scale instrument assessing patients’ behaviour, symptoms, impairment and social functioning (Wing et al., 1998). It has been used for several decades and has shown good reliability and validity as a short-screening instrument (James et al., 2018).
The Health of the Nation Outcome Scales Secure (HoNOS-Secure)
Clinicians use HoNOS-secure to assess patients’ health and functioning in different areas. HoNOS has four domains: behavioural problems, cognitive and physical impairment, symptomatic issues and social difficulties, rated on a scale from 0 to 4. The seven-item secure subscale, also placed on a scale from 0 to 4, requires advanced risk management if scored one or more.
MOAS
Clinicians use tools like the Modified Overt Aggression Scale (MOAS) to assess patients’ aggressive behaviour (Kay et al., 1988; Yudofsky et al., 1986). The MOAS measures the frequency and severity of aggression on a scale of 0 to 40, with a higher score indicating more aggression. This tool is often used in research settings to monitor changes over time.
HCR-20V3 clinical subscale
The Historical-Clinical-Risk Management-20 (HCR-20V3; Douglas et al., 2013) tool is a commonly used assessment tool for predicting violence risk, and it can also be used to evaluate treatment progress. When examining the effectiveness of interventions, the Clinical and Risk subscales that capture dynamic factors are more responsive to change. To assess our intervention, we examined four Clinical subscale items, including insight, symptoms of major mental disorder, instability and treatment or supervision response. We did not collect data on the violent ideation or intent item after the initial data collection because our data collectors found it challenging to assess.
AQoL-8D
The AQoL tool helps measure the quality of life (Maxwell et al., 2016; Richardson et al., 2014). It consists of 35 items, each with four to six reply options. The scores are then added to create a total score, divided into eight subscales or dimensions. The first three dimensions comprise the Physical Super Dimension, while the remaining five are grouped to form the Psychosocial Super Dimension.
Ethics
The study was realized under the Ethics Committee of Bohnice Psychiatric Hospital approval. Data collection and further handling were conducted per the national legislation and institutional requirements. All participants provided informed consent with the study realization. All data were pseudonymized and are solely identified by their treatment number and hospital identifier, kept confidential for external processing.
Data analysis
The data was analysed using R statistic software. In order to ensure the robustness of the results yielded from regression analysis, bootstrapped with 5,000 iterations, Confidence Intervals (CI) were added.
Results
As expected, length of stay (LoS) was associated with remaining in the hospital (Table 1). Specifically, every day spent in the hospital was associated with a 99.95% decrease in odds of being.
Effect of length of stay on discharge (n = 793).
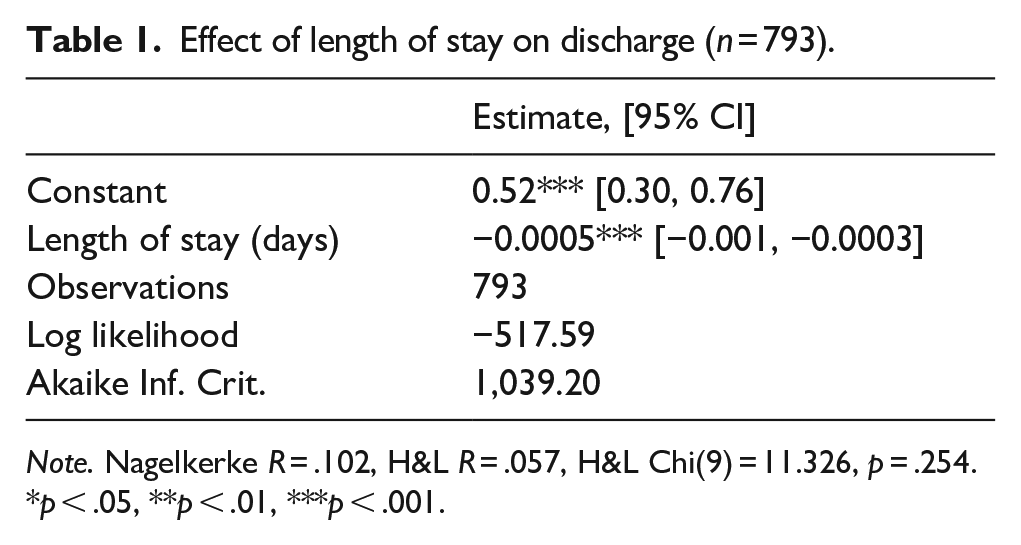
Note. Nagelkerke R = .102, H&L R = .057, H&L Chi(9) = 11.326, p = .254.
p < .05, **p < .01, ***p < .001.
Next, we investigated whether changes in assessment measures such as HoNOS, HoNOS secure, MOAS, AQoL physical and psychosocial subscales and single rating of HCR-20 clinical subscale items were associated with patients’ current state. As Table 2 shows, only two of these were significant. Specifically, an increase in HoNOS secure scores over the past 6 months was associated with a 22% decrease in the odds of being discharged. The effect of the clinical subscale of HCR-20 was lower, as an increase in it was associated with a 47% decrease in the odds of being discharged.
Effect of assessment tools on discharge (n = 169).
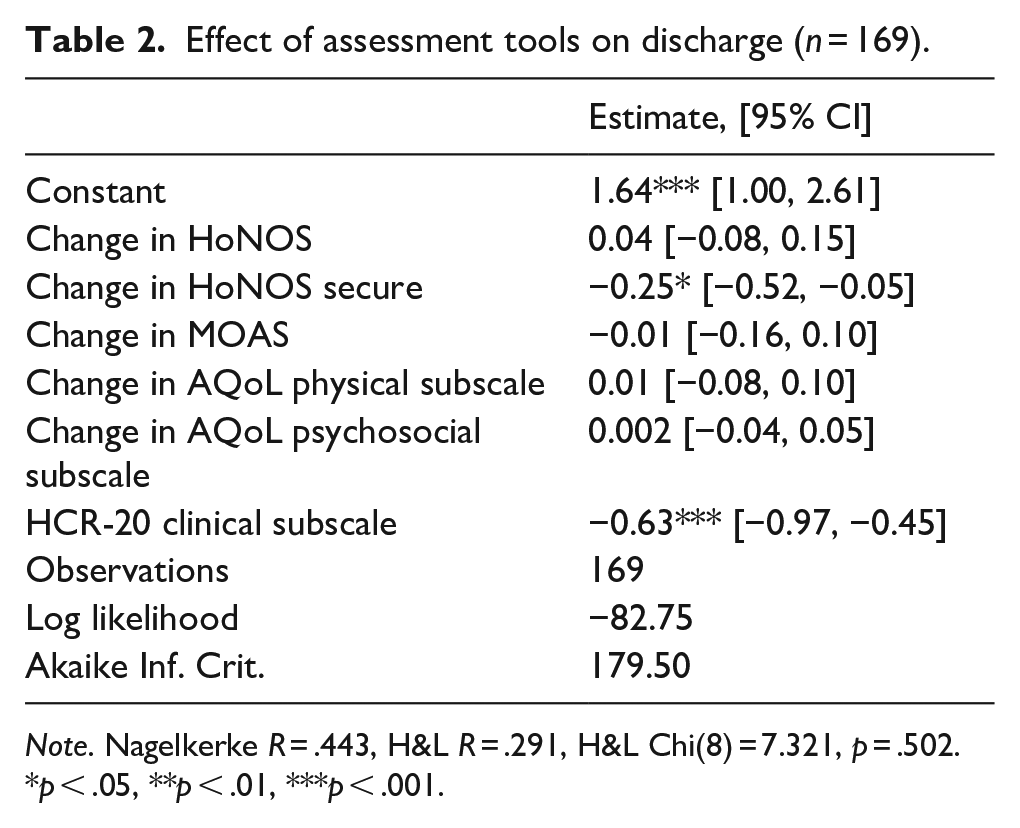
Note. Nagelkerke R = .443, H&L R = .291, H&L Chi(8) = 7.321, p = .502.
*p < .05, **p < .01, ***p < .001.
Afterwards, we investigated whether different diagnoses affected the patient’s disposition. In order to create comparable groups, only diagnosis groups with 50 or more people were included in the analysis as separate predictors. Results displayed in Table 3 demonstrate that when mental retardation diagnosis (F70–F79) is grouped with other diagnoses, having diagnoses of substance use disorder (F10–F19) was associated with a 3.21-time increase in odds of being discharged, but diagnosis of personality disorder (F60–F69) was associated with a 1.89-time increase in odds of being discharged. However, once mental retardation diagnosis is looked at separately, it becomes the only significant factor associated with a 73% decrease in the odds of discharge. Given very similar LL and AIC values for both models, these results highlight that patients with mental retardation stay the longest in forensic hospitals.
Effect of diagnoses on discharge (n = 793).
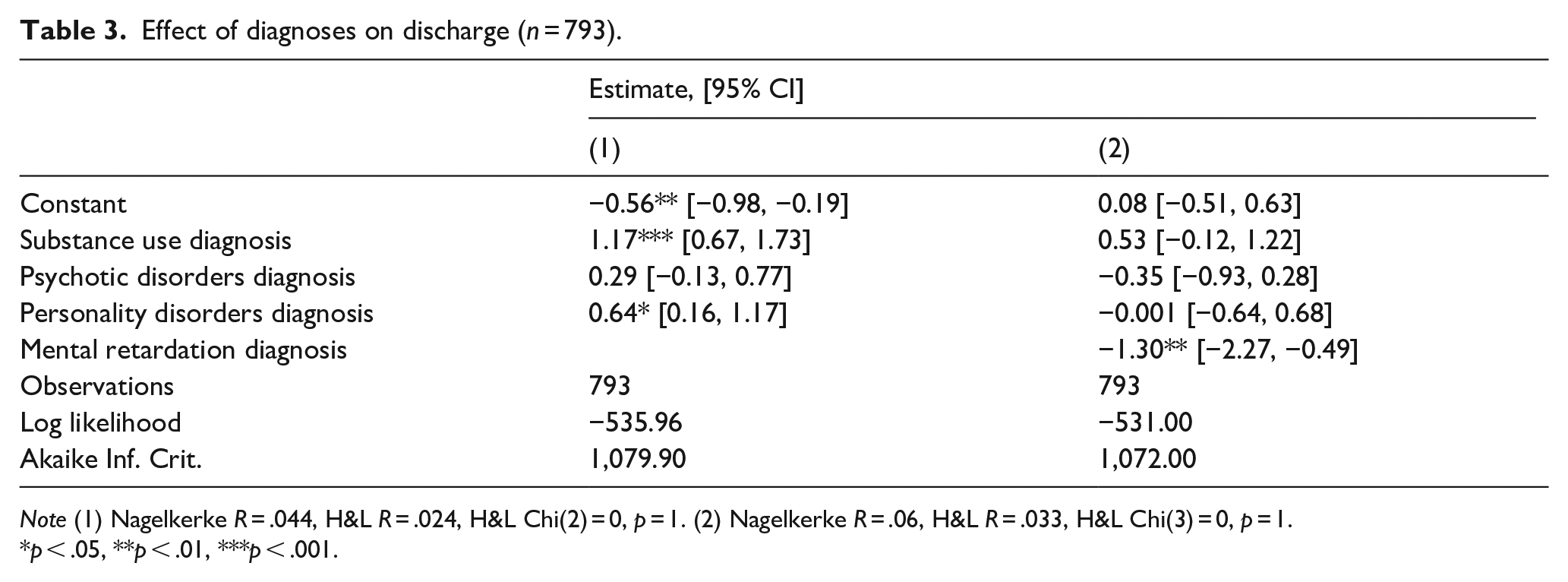
Note (1) Nagelkerke R = .044, H&L R = .024, H&L Chi(2) = 0, p = 1. (2) Nagelkerke R = .06, H&L R = .033, H&L Chi(3) = 0, p = 1.
p < .05, **p < .01, ***p < .001.
The next model investigated the effect of the type of index offence. Table 4 shows that the type of index offence was not associated with patients’ current disposition.
Effect of type of index offence on discharge (n = 793).
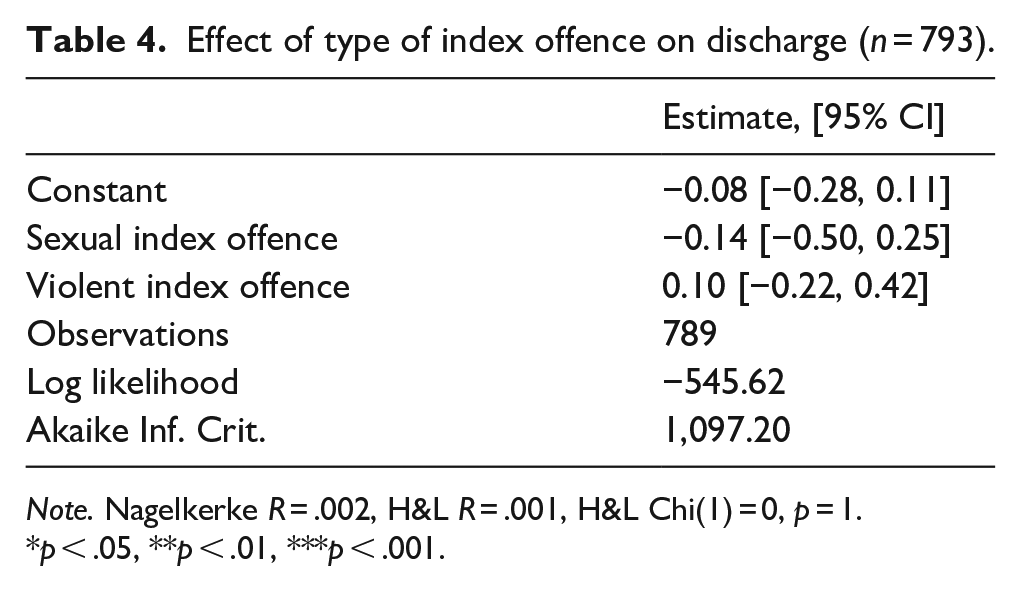
Note. Nagelkerke R = .002, H&L R = .001, H&L Chi(1) = 0, p = 1.
p < .05, **p < .01, ***p < .001.
Lastly, we analysed whether sociodemographic characteristics of patients affected their likelihood of being discharged. As model six in Table 5 shows, two variables had the effect, once others were controlled for. Specifically, having support and being in contact with relatives or friends was associated with a 2.47 times increase in odds of being discharged. Another influential variable was having living arrangements upon release from a hospital. Specifically, having an agreement to live in social housing was associated with an 8.75 times increase in odds of being released, while having a temporary or private residence prepared was associated with a 7.55 and 6.48 times increases. It is also noteworthy that although age, unemployment, education level and living arrangements before admission had significant associations with patients’ current disposition, this effect dissipated in the overall model.
Effect of Sociodemographic characteristics on discharge (n = 793).
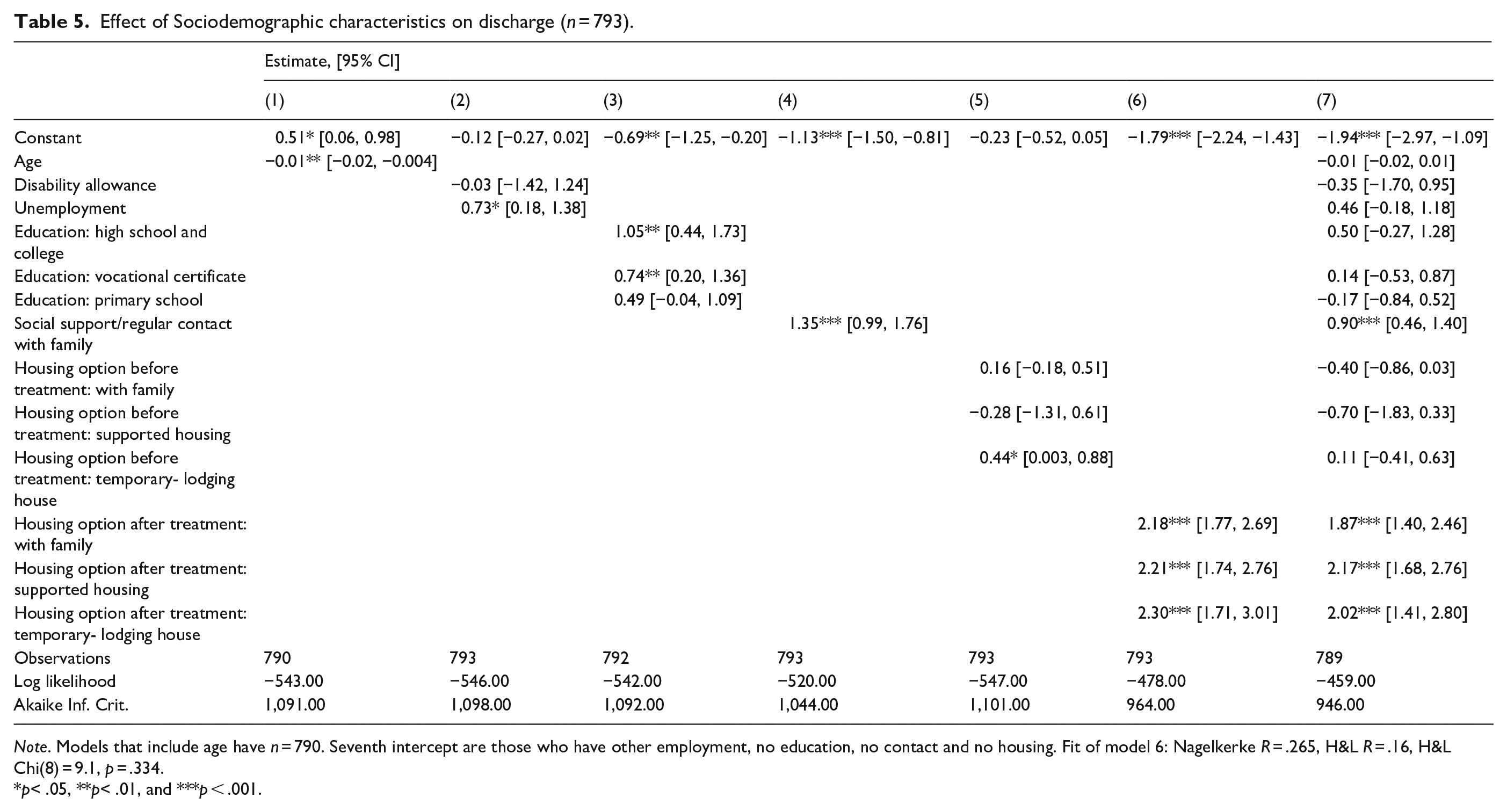
Note. Models that include age have n = 790. Seventh intercept are those who have other employment, no education, no contact and no housing. Fit of model 6: Nagelkerke R = .265, H&L R = .16, H&L Chi(8) = 9.1, p = .334.
p< .05, **p< .01, and ***p < .001.
Discussion
The current study aimed to provide an overview of patient characteristics contributing to discharge. The results yielded the following patient profile with the highest odds of being released. They show a low level of risk, as evidenced by the decrease in unstable behaviour, symptom severity, substance use and an increase in their insight. They also do not have a diagnosis of mental retardation and are likely to have been admitted due to the substance use. Importantly, they plan for a stable environment upon release, such as a positive support network through friends or relatives and a place to live. Interestingly, the type of index offence and perceived quality of life during the treatment play little role in affecting the odds of discharge.
These findings partially agreed with a previous study with patients from only one hospital in Prague (Páv, Sebalo, et al., 2022). Across all hospitals in Czechia, improvement in presentation and insight increased the likelihood of discharge. Given that in earlier studies, sociodemographic variables did not include those about plans, their significance only in the current research is understandable. Mainly as it corresponds to findings from other countries ((Eckert et al., 2017; Kastner et al., 2022; Ross et al., 2012; Völlm et al., 2018); however, it is essential to point out that relevant variables are those that correspond to the patient’s social support currently or relate to their future. The sociodemographic variables related to their past do not affect the likelihood of discharge.
This unimportance of specific aspects of history is an important finding. It also extends to the need for significance of the type of index offence. These findings also match the focus of parole boards in the US on clinical and risk subscales of HCR-20 rather than on historical ones (Kastner et al., 2022) and studies in other countries (Andreasson et al., 2014; Völlm et al., 2018). However, this finding does not correspond to all studies. For instance, Ross et al. (2012) reported that patients with severe crimes such as violence or sexual assault stayed longer in forensic hospitals.
Similarly, Crocker et al. (2014) found that the severity of index offence was associated with a lower likelihood of discharge. Given the descriptive nature of the study, these differences likely reflect different practices. Any debate of whether the history of violent behaviour should influence patients’ discharge results from the extent to which past behaviour can predict recidivism.
Consequently, the current findings show that while the simple offence was unrelated to patients’ disposition, specific assessment tools such as the clinical subscale of HCR-20 and HoNOS secure indicate reliance on verified instruments rather than clinical judgement. The importance of risk-indicating behaviour and improvement in presentation echoes research from other countries (Crocker et al., 2014; Davoren et al., 2013; Hilton et al., 2022). However, surprisingly, the change in violent behaviour indexed by MOAS during the past 6 months did not influence the odds of being discharged. This does not correspond to the studies above. Furthermore, these findings are counterintuitive to the forensic hospitals as institutions. The reason for this is the inclusion of several tools simultaneously. The first item of HoNOS secure assesses physical aggression and agitated behaviour. While MOAS did not have a significant effect, HoNOS secure did. Thus, it is likely that the current results speak more about the effectiveness of one scale over the other rather than discounting patients’ behaviour when considering their release. Another finding related to the scale rather than practice is the non-significant effect of AQoL subscales. Given that this scale reflects subjective well-being, a dubious construct in predicting rehabilitation efficiency, the current finding suggests that this scale has limited application in forensic settings.
The primary disagreement between the results of the current study and other research pertained to the importance of diagnosis. First, similar to the patients described by Hare Duke et al. (2018), Völlm et al. (2018) and (Ross et al., 2012), but unlike those reported by Chester et al. (2018) and Gosek et al. (2020) patients in Czechia diagnosed with mental retardation were less likely to be released. A possible explanation is the lack of specific forensic units for these patients that can effectively meet their unique needs. Second, the model where mental retardation was not split into a separate group showed that patients diagnosed with substance use or personality disorders were more likely to be discharged. Not only is this counterintuitive, but these results are also inconsistent with practices in other countries (Crocker et al., 2014; Ross et al., 2012). The most straightforward explanation is the high importance of the mental retardation diagnosis, as once it was not grouped with other diagnoses, the unexpected results lost significance. Thus, it appears that in Czechia, the diagnosis that is most relevant to the likelihood of release is mental retardation. The lack of commonly found effects of psychotic symptoms (Andreasson et al., 2014; Crocker et al., 2014; Gosek et al., 2020, 2021; Páv, Sebalo, et al., 2022; Páv, Vňuková, & Sebalo, 2022), once intellectual disability is accounted for also supports the importance of the latter.
Limitations
The present study has limitations. First, the number of analyses employed naturally increases the likelihood of fictitious results. However, to ensure maximum robustness of the results, all comments were supplemented with bootstrapped 95% confidence intervals. Second, while the current study is representative of the population of patients from forensic psychiatric hospitals in Czechia, its results cannot be extrapolated to other countries. The third limitation of the study was the inability to access the detailed criminal history of patients, which would have provided a more in-depth analysis of the effect that past behaviour can have on discharge.
Furthermore, rather than relying on detailed coding of patients’ behaviour during treatment, the current study relied on a retrospective assessment done at two-time points. Similarly, it was impossible to incorporate information about the specific treatments that patients have undergone in the data collection. Lastly, another critical set of limitations stems from the inability to access the data about the hospitals and respective districts that could influence the decision to discharge and the effect of patient-centred variables. It is possible that for some patients, where, for example, a proposal to community transfer is submitted, the court will not grant this proposal or determine an extension of treatment.
Conclusion
The current study is the first wide-scale investigation into factors facilitating and impeding discharge from forensic psychiatric hospitals in Czechia. The results have shown that they are similar to those identified in other countries. Specifically, improvements in behaviour during treatment, which include a decrease in aggressive behaviour, overt symptoms of mental health issues, cognitive problems, lack of problems with treatment and increase in insight as well as the creation of a stable future in the form of strong support networks and a place to live increases the odds of being discharged. However, the results have also demonstrated that patients with mental retardation are likely to remain in the forensic settings. This, in turn, indicates the necessity to create either specialized units or at least programmes that address their unique needs.
Supplemental Material
sj-docx-1-isp-10.1177_00207640241255575 – Supplemental material for Markers of predicting discharge from forensic psychiatric hospitals in Czechia
Supplemental material, sj-docx-1-isp-10.1177_00207640241255575 for Markers of predicting discharge from forensic psychiatric hospitals in Czechia by Ivan Sebalo, Martina Sebalo Vňuková, Martin Anders, Radek Ptáček and Marek Páv in International Journal of Social Psychiatry
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Cooperatio grant 207 038, Research area : Neurosciences and Health sciences, and the project MH CZ – DRO VFN64165
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.