
Abstract
Background:
Trauma exposure is associated with adverse health-related correlates, including physical comorbidities, and is highly prevalent among public safety personnel (PSP). The current study (1) examined the association between context of index trauma exposure (part of job vs. other) and physical conditions and (2) established the prevalence of physical conditions according to PSP category (e.g., police, paramedic) and index trauma type (e.g., serious accident, physical assault) in a large Canadian sample of PSP.
Methods:
PSP completed an online survey between September 2016 and January 2017. Multivariable logistic regressions examined associations between context of index trauma exposure (i.e., part of job vs. other) and physical condition categories. Cross-tabulations with chi-square analyses examined whether the prevalence of physical conditions significantly differed according to PSP category and index trauma type.
Results:
There were 5,267 PSP included in the current study. Results from the most stringent model of logistic regressions demonstrated that, compared to PSP who experienced their index trauma in any other context, PSP who experienced it as part of their job had reduced odds of “other” physical conditions (adjusted odds ratio = 0.73, 95% confidence interval, 0.57 to 0.94, P < 0.05). Results also revealed significant differences in the prevalence of physical conditions across all PSP categories and select index trauma types.
Conclusion:
Results highlight the relevance of trauma exposure outside of an occupational context among PSP and may have implications for the positive impact of stress inoculation and resiliency training programs for PSP.
Due to the nature of their work, public safety personnel (PSP; e.g., correctional workers, police officers, firefighters, paramedics, public safety communications officials [e.g., 911 call center operators/dispatchers]) are commonly exposed to potentially traumatic events. 1 –9 Studies across various samples demonstrate high estimates of trauma exposure among PSP, exceeding 85%; 1,3,7 –9 a recent study found that PSP reported exposure to 11 of the 16 types of traumatic events, on average. 1 Extant research has highlighted the negative health correlates associated with trauma exposure among PSP and the general population, including psychiatric illnesses 1,6–7,10,11 and, of particular relevance to the current study, physical conditions. 12 –16 Researchers suggest the latter association may be explained by physiological changes associated with the body’s response to traumatic stress. 17 Studies have shown that PSP have high rates of various physical conditions including respiratory, cardiovascular, autoimmune, gastrointestinal, chronic pain, and cancer; 18 –22 this may be, in part, related to their elevated rates of trauma exposure; however, this has not been directly investigated.
Research among the general population has examined the relevance of trauma characteristics in the association between trauma exposure and physical conditions, including number and type of traumatic events. For example, population-based studies by our group and others have found a “dose–response” relationship between number of traumatic events and increasing odds of physical conditions. 12–13,16 These studies also suggest that the association between trauma exposure and physical conditions may vary according to type of traumatic event and that these associations remain significant after controlling for psychiatric conditions. In particular, researchers 12–13 found associations between injurious traumas (particularly sexual assault) and witnessed traumas with a wide variety of physical conditions. However, associations between exposure to other trauma types and physical conditions, including war-related trauma, psychological trauma, and natural disasters, have been inconsistent. 12–13,16 The disparate results may stem from variations in covariates included within regression models across studies; nonetheless, further investigation is warranted to better understand the association between trauma characteristics and physical conditions, particularly in populations where trauma burden is high.
To our knowledge, no research to date has examined the association between trauma exposure and physical conditions among PSP despite elevated rates of both trauma exposure and physical conditions among this population. Recent research suggests that the prevalence of exposure to different types of traumatic events, cumulative number of types of traumatic events, and proportions of worst traumatic events endorsed may vary according to the type of PSP. 1 Accordingly, the prevalence of physical conditions may vary as a function of both type of trauma exposure experienced by PSP and type of PSP. Research that has examined either trauma exposure or physical health conditions individually among PSP has been limited to relatively homogenous samples of specific types of PSP (e.g., firefighters only). The available results limit our understanding of how differences in job requirements and work-related exposures according to PSP type may be related to trauma exposure and physical health. In addition, although studies have examined associations between trauma type and physical conditions, to our knowledge, no research to date has specifically examined the relationship between work-related traumatic events and physical conditions. This is particularly relevant to PSP who experience high rates of traumatic exposures as part of their jobs. Understanding the relationship between work-related trauma exposure and physical health among PSP represents a valuable area of investigation with important public health implications such as informing targeted intervention or prevention initiatives. Given the existing research gaps, the current study is designed to (1) examine the association between context of index trauma exposure (i.e., part of job as PSP vs. other contexts) and physical conditions and (2) establish the prevalence of physical conditions according to PSP category and index trauma type in a large, diverse sample of Canadian PSP.
Methods
Data and Sample
Data were collected using an online self-report survey from September 1, 2016, to January 31, 2017. The survey was available in English or French and was conducted in accordance with web-based survey guidelines. 23 Email invitations were distributed to PSP from the Public Safety Steering Committee of the Canadian Institute for Public Safety Research and Treatment, advocacy organizations, and public safety organizations, and a video invitation was prepared by the Minister of Public Safety and Emergency Preparedness in order to recruit participants. Additional details regarding data collection for this study have been published elsewhere. 24,25 The original sample consisted of 8,520 participants; however, the sample for the current study only included 5,267 (61.8%) participants who completed the psychiatric symptom modules and items pertaining to physical conditions. Ethical approval for the study was obtained from the University of Regina Institutional Research Ethics Board (file #2016-107).
Measures
Physical conditions
Following the psychiatric condition and chronic pain modules, participants were asked “Do you have any other diagnosed health conditions?” (i.e., aside from psychiatric conditions and chronic pain). If participants responded “yes,” they were asked to describe which diagnoses they had received. Responses describing physical conditions were grouped into categories based on physiological systems, clinical recommendation, 26 and prior research: 27 neurologic (e.g., migraine, concussion, epilepsy), digestive (e.g., inflammatory bowel disease, liver disease, pancreatitis), endocrine/metabolic (e.g., diabetes, high cholesterol, thyroid diseases), respiratory (e.g., asthma, bronchitis, sinusitis), cardiovascular (e.g., hypertension, cardiovascular disease, heart attack), and musculoskeletal/rheumatic (e.g., arthritis, fibromyalgia, lupus, osteoporosis). In order to obtain adequate cell sizes, we collapsed neoplastic, infectious, urogenital, hematologic, dermatologic, sensory conditions, sleep disorders, and other physical conditions into an “other” physical condition category (see Online Appendix A for a complete list of physical conditions in each category).
Trauma exposure
The Life Events Checklist for DSM-5 28 assessed trauma exposure. Participants were shown a list of 17 types of traumatic events and asked whether they had ever personally experienced or witnessed each event, learned that the event happened to a close friend or family member, or were exposed to the event as part of their job as a first responder. Participants were then asked to select which of the events was the worst trauma they had ever experienced (i.e., index trauma). We categorized index traumas into seven groups (i.e., life-threatening natural disaster/explosion, serious accident, physical assault, sexual assault, life-threatening illness/injury, witnessed trauma, and other trauma) on the basis of similarity and prior research 29,30 (see Online Appendix B for a complete list of index trauma types in each category).
Participants were then asked “What is the most stressful way you have experienced this event?” and were provided with 5 response options: (a) It happened to me directly, (b) I witnessed it, (c) I learned about it happening to a close family member or friend, (d) I was repeatedly exposed to details about it as part of my job, and (e) other (please specify). If participants specified within the “other” category that they directly experienced the event or witnessed the event as part of their job, these responses were categorized with response option “d.” We then dichotomized response options according to whether or not the participant was exposed to the event in the most stressful way as part of his or her job as a first responder (i.e., part of my job vs. other).
Sociodemographic and PSP characteristics
Participants were grouped into six PSP categories based on self-report: municipal/provincial police, federal police (i.e., Royal Canadian Mounted Police [RCMP]), correctional workers, firefighters, paramedics, and public safety communications officials; municipal/provincial police and RCMP were examined separately due to differences in their work setting and context. 25 We examined age and years of PSP service continuously and categorized sex (male, female), marital status (married/common-law, single, separated/divorced/widowed/remarried), ethnicity (White, other), and education (high school or less, some postsecondary, university/college degree or higher) in accordance with prior research. 25
Psychiatric screens and self-reported diagnoses
Well-validated and reliable self-report measures assessed positive screens for psychiatric conditions. The Posttraumatic Stress Disorder (PTSD) Checklist for DSM-5 (PCL-5) 31 assessed past month PTSD. A positive screen for PTSD required meeting the minimum criteria for each PTSD cluster and a total PCL-5 score >32. 32 The Patient Health Questionnaire 33,34 assessed major depressive disorder (MDD) over the past 14 days with a total score >9 indicating a positive screen. 35 The Generalized Anxiety Disorder (GAD) Scale (GAD-7) 36,37 assessed GAD over the past 14 days, wherein a total score >9 was indicative of a positive screen. 38 The Panic Disorder (PD) Symptoms Severity Scale–Self-Report (PDSS-SR) 39 assessed PD over the past 7 days. A total score >7 is suggestive of a positive screen. 40 The Social Interaction Phobia Scale 41 assessed social anxiety disorder (SAD) with a positive screen designated by a score >20. 42 Finally, the Alcohol Use Disorder (AUD) Identification Test 43 –45(AUDIT) assessed the presence of a past year AUD. A total score >15 is suggestive of a positive screen. 44
Participants self-reported lifetime psychiatric conditions that were not assessed by screening measures (outlined above), including obsessive-compulsive disorder (OCD), persistent depressive disorder (PDD), bipolar I, bipolar II, and cyclothymic disorder. They were asked whether they had ever been diagnosed with a mood/anxiety disorder (separately), and if they responded “yes,” they were asked to check all responses that applied. These disorders were categorized into composite variables with the psychiatric screens due to low prevalence; categories included “any anxiety disorder” (OCD, GAD, SAD, PD) and “any mood disorder” (MDD, PDD, bipolar I, bipolar II, cyclothymic disorder). These variables were included as covariates in analyses along with positive screens for PTSD and AUD.
Analytic Strategy
Descriptive statistics assessed sample characteristics among the total sample and among those who experienced their index trauma as part of their job as a PSP. Next, multivariable logistic regressions examined associations between context of exposure to index trauma (part of my job versus other [reference]) and physical conditions. We conducted an unadjusted model, in addition to a second model controlling for sociodemographics and PSP characteristics (i.e., age, sex, marital status, race, education, years of PSP service, PSP category) and a third model controlling for sociodemographics, PSP characteristics, and psychiatric conditions (i.e., positive screen for PTSD, any anxiety disorder, any mood disorder, AUD). Finally, although cell sizes and statistical power did not permit analyses examining the role of PSP category and index trauma type in associations between context of index trauma exposure and physical conditions, cross-tabulations with chi-square analyses assessed the prevalence of physical conditions according to PSP category and index trauma type among the entire sample. Analyses were conducted using SPSS (version 25) 46 and STATA (version 15) 47 statistical software.
Results
Sample Characteristics
PSP were 43.42 years old on average and primarily male (66.6%), married/common-law (75.2%), and White (90.4%) with some postsecondary education (52.5%). PSP served for 17.68 years on average, and the most common PSP category was municipal/provincial police (25.6%). The most frequently endorsed index trauma was witnessed trauma (42.3%), and PTSD, anxiety disorders, mood disorders, and AUDs were prevalent among 22.1%, 27.1%, 26.9%, and 5.7% of the sample, respectively. Participants who experienced their index trauma as part of their job (n = 1,649; 31.3%) had characteristics similar to the full sample, with an elevated proportion endorsing witnessed trauma as their index trauma (59.9%; see Table 1).
Sample Characteristics.
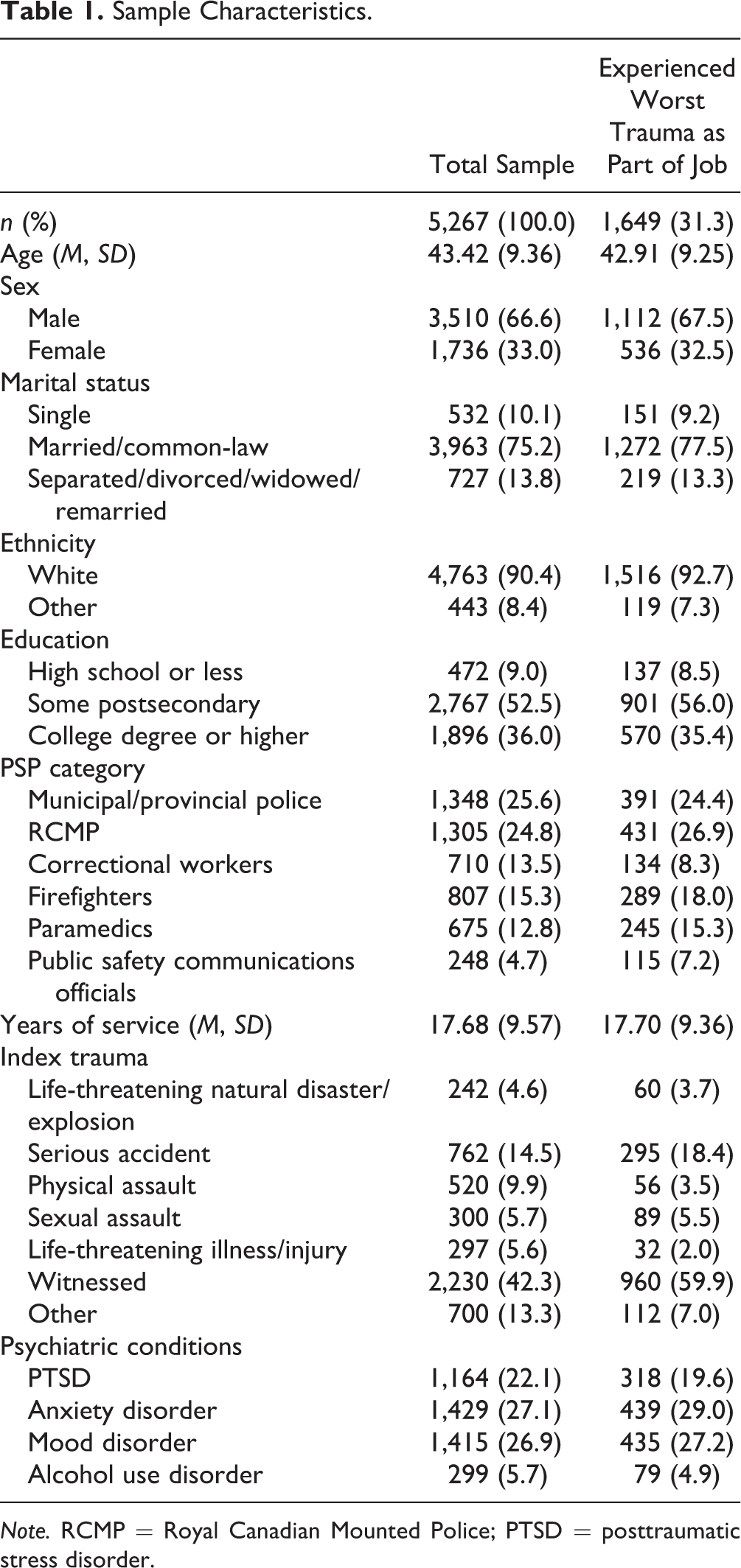
Note. RCMP = Royal Canadian Mounted Police; PTSD = posttraumatic stress disorder.
Associations between Context of Index Trauma and Physical Conditions
The multivariable logistic regression results are shown in Table 2. Compared to experiencing an index trauma in any other context, experiencing an index trauma as part of working as a PSP was associated with reduced odds of neurologic conditions (odds ratio [OR] = 0.64, 95% CI, 0.45 to 0.89, P < 0.01) and “other” physical conditions (OR = 0.79, 95% CI, 0.64 to 0.99, P < 0.05). Results remained consistent after controlling for sociodemographic and PSP characteristics. After additionally adjusting for psychiatric conditions, experiencing an index trauma as part of working as a PSP was associated with reduced odds only of “other” physical conditions (adjusted OR [AOR] = 0.73, 95% CI, 0.57 to 0.94, P < 0.05) compared to experiencing an index trauma in any other context. Post hoc analyses examined associations between context of index trauma exposure (part of working as PSP vs. other [reference]) and individual physical conditions within the “other” physical condition category. Results revealed no significant associations for any of the individual “other” physical conditions (AOR range: 0.90 to 1.01, P > 0.05).
Associations between Context of Index Trauma Exposure and Physical Conditions.
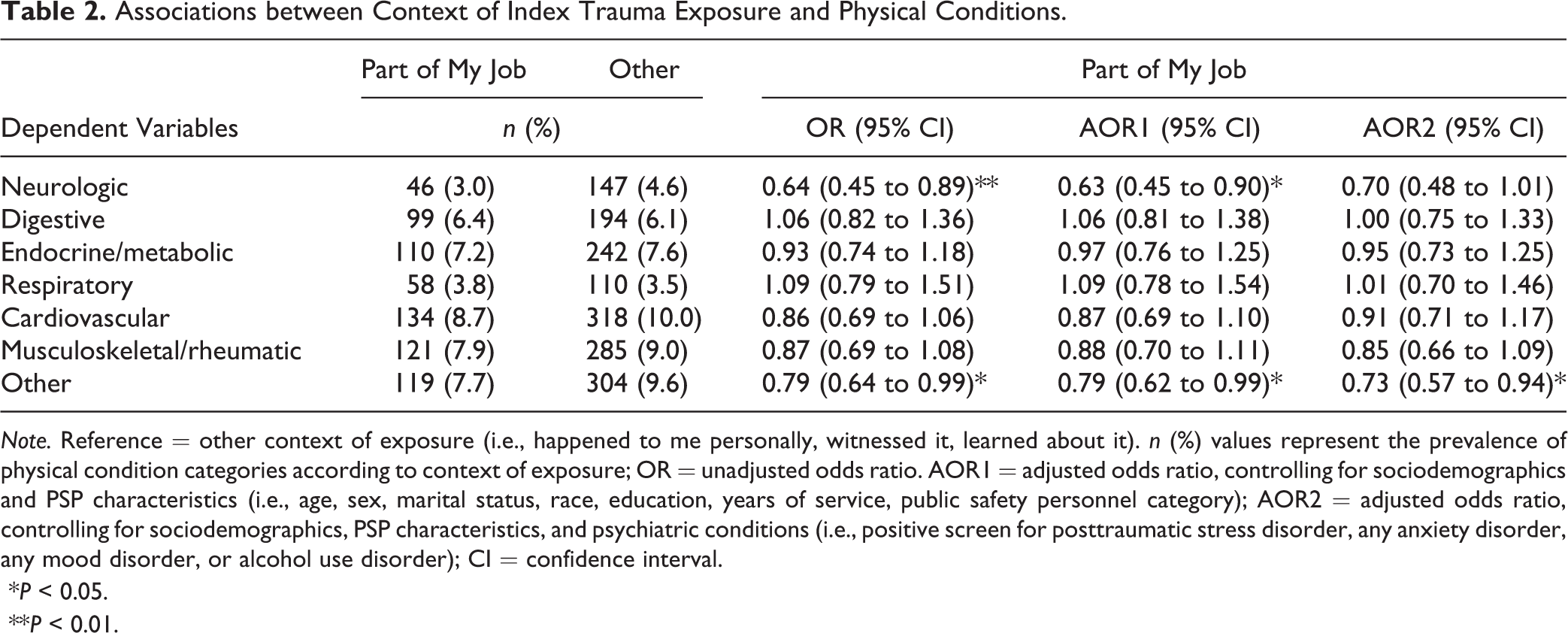
Note. Reference = other context of exposure (i.e., happened to me personally, witnessed it, learned about it). n (%) values represent the prevalence of physical condition categories according to context of exposure; OR = unadjusted odds ratio. AOR1 = adjusted odds ratio, controlling for sociodemographics and PSP characteristics (i.e., age, sex, marital status, race, education, years of service, public safety personnel category); AOR2 = adjusted odds ratio, controlling for sociodemographics, PSP characteristics, and psychiatric conditions (i.e., positive screen for posttraumatic stress disorder, any anxiety disorder, any mood disorder, or alcohol use disorder); CI = confidence interval.
*P < 0.05.
**P < 0.01.
Prevalence of Physical Conditions
Among the entire sample, the prevalence of each physical condition category significantly varied according to PSP category (see Table 3). Across PSP categories, paramedics had the highest prevalence of neurologic (6.1%), digestive (11.0%), endocrine/metabolic (10.5%), and respiratory conditions (7.2%); correctional workers had the highest prevalence of cardiovascular conditions (11.9%); RCMP had the highest prevalence of musculoskeletal/rheumatic conditions (12.2%); and communications officials had the highest prevalence of other physical conditions (12.9%). Firefighters had the lowest prevalence of each physical condition with the exception of cardiovascular conditions.
Prevalence of Physical Conditions according to Public Safety Personnel Category and Index Trauma Type.
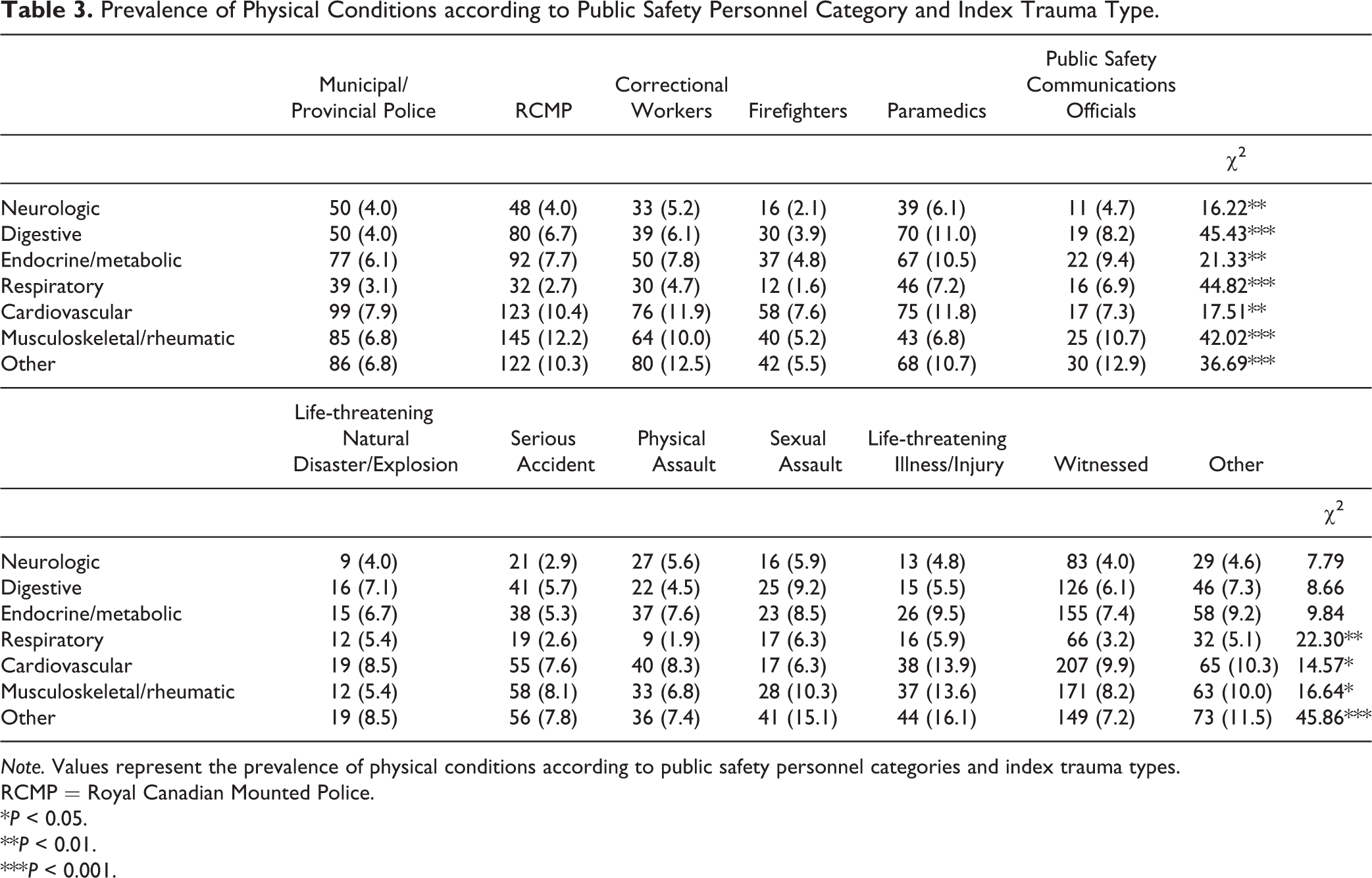
Note. Values represent the prevalence of physical conditions according to public safety personnel categories and index trauma types.
RCMP = Royal Canadian Mounted Police.
*P < 0.05.
**P < 0.01.
***P < 0.001.
The prevalence of respiratory, cardiovascular, musculoskeletal/rheumatic, and other physical conditions varied according to index trauma type among PSP (see Table 3). Cardiovascular (13.9%), musculoskeletal/rheumatic (13.6%), and other physical conditions (16.1%) were most prevalent among PSP who endorsed a life-threatening illness/injury as their index trauma. Respiratory conditions (6.3%) were most prevalent among those who endorsed sexual assault as their index trauma.
Discussion
The current study adds to the growing body of literature on trauma exposure and health-related correlates among PSP. The novel findings from this study outline that participants who experienced their index trauma as part of working as a PSP had reduced odds of certain physical conditions. In addition, results revealed variations in the prevalence of physical conditions according to both PSP type and index trauma. The current results have important implications for trauma-related care for PSP.
Results indicate that experiencing one’s worst trauma as part of working as a PSP was associated with reduced odds of neurologic and “other” physical conditions compared to experiencing the worst trauma in any other context. The lower odds remained statistically significant for “other” physical conditions after controlling for sociodemographics, years of service as a PSP, type of PSP, and psychiatric conditions. These results may suggest that PSP are able to cope with work-related trauma more effectively than trauma experienced in other contexts and subsequently are less likely to experience adverse physical health correlates related to occupational trauma. The current results may provide preliminary support for the positive impact of stress inoculation and resiliency training programs for PSP (e.g., mental health first aid, critical incident stress management, the Road to Mental Readiness, mindfulness-based resilience training), 48 –54 which are designed to mitigate negative impacts of repeated work-related trauma exposure; however, additional investigation is warranted to explore this hypothesis further. Relatedly, PSP resilience toward work-related trauma may stem from reduced uncertainty promoted by job-specific training and expectations formed about deployment experiences. In contrast, nonoccupational trauma may be associated with greater uncertainty and reduced support, which may be related to increased vulnerability to trauma-related sequelae 55,56 including physical comorbidity. In addition, work-related trauma may be associated with fewer adverse health-related correlates in light of greater access to treatment services (e.g., through the Workplace Safety and Insurance Board) compared to non-work-related trauma.
The emergent associations may also relate to the nature of the specific types of work-related and non-work-related traumatic events. For example, it is possible that work-related traumas may more often include events such as serious accidents and life-threatening natural disasters, whereas non-work-related traumas may more often include interpersonal traumas involving victimization, such as sexual assault. Previous research has demonstrated differences in the odds of physical conditions according to the type of traumatic event; in particular, sexual assault has been associated with increased odds of several physical conditions across multiple studies. 12,13 The duration of time since the index trauma, and subsequently the chronicity of traumatic stress, may also play a role in the current results. Work-related index traumas likely would have occurred within the previous two decades on average, considering PSP’s average number of years of service (∼18), whereas non-work-related traumas may date back to participants’ childhood. The association between chronic stress and allostatic overload with maladaptive physiological changes is well-established. 57 This may translate to increased vulnerability to physical conditions among those who experienced earlier index traumas and thus may be implicated in the “protective” association between more recent work-related trauma and physical conditions in the current study. Of note, however, due to the cross-sectional nature of this survey, we are unable to determine the temporal and causal nature of the emergent associations. It is also possible that those with certain physical conditions are more or less likely to experience certain types of traumas. For example, an individual with functional limitations related to a chronic condition may be at increased risk of victimization; alternatively, an individual with poor physical health may have reduced risk of being exposed to work-related trauma due to multiple medical leaves. Future longitudinal research should explore this further.
Interestingly, however, post hoc analyses revealed no significant associations between context of index trauma and individual “other” physical conditions. This may suggest the emergent result captures an association between work-related trauma and reduced odds of physical multimorbidity as opposed to individual conditions. Future research should examine this hypothesis further. Nonetheless, the current results highlight the potential importance of monitoring trauma exposure that occurs outside of an occupational context among PSP (both prior to and during employment) and the possible associated impact on mental and physical health. In addition, it may be beneficial for stress inoculation, resiliency, and other training programs for PSP to incorporate training focused on nonoccupational trauma or emphasize the generalizability of skills included to nonoccupational contexts.
To further understand factors associated with physical conditions among PSP, cross-tabulations with chi-square analyses assessed differences in the prevalence of physical conditions according to PSP category and index trauma type. Prevalence estimates for each of the seven physical condition categories varied significantly by PSP category with the lowest estimates among firefighters across nearly all physical conditions. This pattern of results is in line with the “healthy worker effect” 58 found among samples of firefighters, 59 which suggests that certain employment groups, such as firefighters, have lower mortality risk compared to the general population. Choi 59 outlines various possible explanations for the healthy worker effect, including beneficial health effects of a certain job (e.g., positive physical impact of high physical exertion for firefighters) or a selection bias wherein those who are physically healthier are selected for a certain job, among others. The reduced rates of physical conditions among firefighters are also consistent with recent studies that found the lowest rates of chronic pain among firefighters compared to other types of PSP. 24,60 Previous research has also found evidence that firefighters have the lowest estimates of any mental health condition compared to other PSP, 25 though some studies included the same participants as the current study. There are several possibilities for the relatively positive physical and mental health specific to firefighters when compared to other PSP; for example, there may be a variety of systemic or organizational variables that support firefighter resilience or there may be an implicit systematic selection bias in the current sample. In any case, further investigation is warranted to determine whether the pattern generalizes to other large samples that facilitate comparisons across PSP.
In contrast to firefighters, paramedics reported the highest estimates of most physical conditions including neurologic, digestive, endocrine/metabolic, and respiratory conditions. Recent research focused on paramedics found declines in participant physical health status across the duration of approximately a decade; 61 specifically, an increasing proportion of the participating paramedics endorsed “fair/poor” overall health (i.e., 5.5% in 1999 vs. 8.2% in 2008) and “fair/poor” physical fitness (i.e., 17.5% in 1999 vs. 23.6% in 2008). The same study also found sleep difficulties were highly prevalent (20% to 27%) among their entirely paramedic sample. 61 Accordingly, the established association between sleep difficulties and poor physical health 62-64 may partially explain the elevated prevalence of physical conditions in the current study; however, further investigations with large samples that include diverse PSP for comparisons appear warranted to better understand any physical health disparities.
In line with previous research, the prevalence of certain physical conditions varied according to trauma type. 12,13,30 In particular, the prevalence of respiratory, cardiovascular, musculoskeletal/rheumatic, and “other” physical conditions varied according to trauma type. The current results suggest that across trauma types, life-threatening illness/injury is associated with the highest prevalence of cardiovascular, musculoskeletal/rheumatic, and “other” physical conditions; it is possible that in many cases, the physical condition itself may be considered the life-threatening illness/injury trauma. A growing body of research has examined illness-induced PTSD 64,65 including cardiac disease–induced 66,67 and cancer-related PTSD. 68,69 Evidence from the extant literature suggests that certain physical conditions may be perceived as traumatic and are capable of triggering the onset of PTSD. 70 Alternatively, life-threatening illnesses and injuries may be associated with greater medical comorbidity compared to other traumas, which may explain the elevated prevalence of physical conditions among individuals endorsing these index traumas. In support, prior research from our group found that among individuals with PTSD, those who endorsed a life-threatening illness as their index trauma had a higher mean number of physical conditions and a higher prevalence of both acute and chronic physical conditions compared to those endorsing any other index trauma. 64 The current study’s result that sexual assault was associated with the highest prevalence of respiratory conditions is consistent with previous research that has established an association between sexual assault and poor physical health including respiratory conditions. 12,71,72 Further investigation is warranted to understand why only certain physical conditions varied according to trauma type, or whether this trend is a consequence of limited power and small cell sizes in the current study.
The current study results benefit from using a large, diverse PSP sample; nevertheless, the study has limitations that provide important directions for future research. First, psychiatric conditions were assessed using self-report screening measures, and physical conditions were assessed using a single self-report question. These methods of assessment may be less reliable than clinician-ascertained diagnoses and may be susceptible to response biases. In addition, physical conditions were not assessed using condition-specific targeted questions; rather, participants were asked to report any other diagnosed health conditions. This method of assessment may be associated with additional recall bias. Further, although some participants reported conditions associated with chronic pain, participants responded to specific questions directly assessing chronic pain prior to the item assessing physical conditions in the current study (i.e., “Do you have any other diagnosed health conditions?”). As such, chronic pain conditions are most likely underrepresented in the current analyses (see Carleton et al. 24 for additional information on chronic pain in the current sample). Second, psychiatric symptoms may have been underreported in the current study; although responses were anonymous, research suggests there are concerns with stigma related to mental health among PSP. 73,74 Third, the current sample was not randomly selected and may not be representative of all Canadian PSP; however, demographic proportions for sex, age, and provincial region in the overall data collection were comparable to data provided by Statistics Canada for PSP using the 2011 National Household Survey and the National Occupational Classification. 75 Similarly, trends in the proportions of PSP categories were also comparable to those listed in the National Occupational Classification. 75 Fourth, due to the cross-sectional nature of this study, temporal and causal assumptions cannot be made regarding the emergent associations; in particular, we are unable to determine whether the onset of physical conditions occurred before or after (or concurrently with) index trauma exposure. Finally, due to small cell sizes for certain physical conditions, some of the analyses may have been underpowered.
Conclusion
Despite the limitations, the current results are a novel contribution to the literature on trauma exposure among PSP. Results highlight the importance of considering PSP trauma exposure beyond that which occurs in an occupational setting. Future research should examine the associations between occupational trauma and physical conditions longitudinally in order to understand the temporal nature of these associations. In addition, further investigation is warranted to elucidate the mechanisms driving the associations between trauma characteristics and physical conditions among PSP, for whom potentially traumatic or injurious events are part of their work.
Supplemental Material
Supplementary_material - Associations between Trauma Exposure and Physical Conditions among Public Safety Personnel: Associations entre l’exposition à un traumatisme et les problèmes physiques chez le personnel de la santé publique
Supplementary_material for Associations between Trauma Exposure and Physical Conditions among Public Safety Personnel: Associations entre l’exposition à un traumatisme et les problèmes physiques chez le personnel de la santé publique by Jordana L. Sommer, Renée El-Gabalawy, Tamara Taillieu, Tracie O. Afifi and R. Nicholas Carleton in The Canadian Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This research was supported by the Canadian Institute of Public Safety Research and Treatment (CIPSRT) supported by the Canadian Institutes of Health Research (CIHR) through a New Investigator Award (FRN: 285489) and a Catalyst Grant (FRN: 162545). Tracie O. Afifi’s research is supported by a CIHR Foundation Award, CIHR Gold Leaf Award, and the Royal-Mach-Gaensslen Prize for Mental Health Research. Renée El-Gabalawy’s research is supported by Max Rady Faculty of Medicine Start-Up Funding (University of Manitoba) and a CIHR Strategy for Patient-Oriented Research (SPOR) Chronic Pain Network operating grant (#320095 340100). This research was also funded in part by the Ministry of Public Safety and Emergency Preparedness through the Policy Development Contribution Program.
Supplemental Material
The supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.