
Abstract
Background:
The Hearing Voices Approach, a community-based peer-led support group model, is generating interest as a novel way to engage with psychosis. Hearing Voices (HV) groups are run by peers, ‘experts-by-experience’, and emphasize group ownership and community-building rather than adherence to a therapist-led, predetermined structure. Diverse beliefs about experiences are respected and viewed as potentially meaningful. Groups work within each individual’s explanatory framework to reframe understandings.
Aims:
This paper describes the effects of participation in Veteran Voices and Visions (VVV) groups, an adaptation of the HV approach, co-led by clinicians and Veteran peer support specialists, adapted for Veterans who have experienced psychosis and receive care at the VA, a large public health system in the United States.
Method:
This mixed methods pilot study has a convergent parallel design, integrating quantitative and qualitative data from participants in pre-intervention and post-intervention assessments.
Results:
Over 16 weeks, quantitative analysis showed a statistically significant reduction in distress, due to auditory hallucinations, as measured by the Psychotic Symptom Rating Scales (PSYRATS). The Beliefs about Voices Questionnaire- Revised (BAVQ-R) results showed a reduction in malevolence and omnipotence and an increase in benevolence related to auditory hallucinations, but no change in resistance. Engagement showed a trend-level reduction. Qualitative data from midpoint (Week 8) and endpoint (Week 16) interviews revealed several perceived benefits from groups: 1) normalization and camaraderie, 2) increased hope and confidence, 3) self-understanding and reframing of experiences, and 4) building relationships outside of groups. Overall, VVV groups reduced distress due to voices, negative beliefs about voices, and perceived power of voices.
Conclusions:
Study findings contribute to a growing body of literature indicating HV groups support those who have experienced psychosis by reducing social isolation and fostering community, which may facilitate social integration. Overall, our findings highlight the potential benefits of adapting HV groups to health systems.
Introduction
Psychosis is the clinical term referring to experiences of non-consensual reality, either sensory perceptions, such as hearing voices or seeing visions, having unusual beliefs, or extreme, intense emotional experiences. These experiences can be distressing and can lead to clinical diagnoses of serious mental illness (SMI), social isolation, and suicidality. Social isolation has well-documented impacts on mortality and health-related quality of life, comparable to smoking and greater than obesity and alcohol abuse (Grenawalt, 2023; Holt-Lunstad, 2015).
Medication is the first line of treatment for psychosis, but is not effective for many individuals and can have serious side effects leading to treatment discontinuation (Lieberman et al., 2005). A range of psychological interventions for psychosis exist. Cognitive-behavioral therapy for psychosis (CBTp) can reduce severity of positive symptoms (Sitko et al., 2020). Group CBTp has shown efficacy at improving social functioning (Wykes et al., 2005), reducing feelings of hopelessness and low self-esteem (Barrowclough et al., 2006), and reducing severity of psychotic symptoms overall (Lecomte et al., 2008; Penn et al., 2009).
The Hearing Voices Approach, a community-based peer-led support group model, is generating interest as a novel way to engage with psychosis (Branitsky et al., 2021; Corentin et al., 2023). Hearing Voices (HV) groups are run by peers, ‘experts-by-experience’, and emphasize group ownership and community-building rather than adherence to a therapist-led, predetermined structure. Diverse beliefs about experiences are respected and viewed as potentially meaningful in HV groups. Groups work within each individual’s explanatory framework to reframe understandings (Dillon & Hornstein, 2013). Participants value the safe space groups provide, reduced isolation, normalization, and the opportunity to learn from and help one another (Longden et al., 2018).
Veteran Voices and Visions (VVV) groups are an adaptation of the HV approach to Greater Los Angeles Veterans Affairs Health System (GLAVAHS). We piloted VVV groups and collected quantitative and qualitative data regarding the impacts of VVV on distress related to psychosis and to characterize benefits group members derived from groups.
Methods
Design
This mixed methods study has a convergent parallel design, as quantitative and qualitative strands were implemented during the same phase of research and were brought together for interpretation (Cresswell & Clark, 2010). Study assessments were made prior to the intervention and after 16 weeks. This was a single group observational study.
Site
VVV was offered in GLAVAHS mental health clinics. Veterans Affairs is one of the largest health systems in the United States, serving Veterans from all military branches. GLAVAHS serves 1.4 million patients in southern California, offering a range of services for those diagnosed with SMI, including housing support, intensive case management, and recovery and rehabilitative services. VA supports robust peer support specialist training and employment opportunities (Chinman et al., 2008).
Intervention
VVV groups were co-facilitated by a VA mental health clinician and a VA peer support specialist. Facilitators were trained at GLAVAHS by the Wildflower Alliance, in partnership with Hearing Voices Network USA. VVV groups met weekly for an hour on a virtual video platform due to COVID-19. Facilitators met twice-monthly for case consultation meetings.
As most HV groups are organized outside of clinical settings, adaptations were made to integrate these groups into this health system, including: incorporating Veteran trainers and Veteran-specific role-playing scenarios; training clinicians; and developing a clinical documentation approach consistent with HV values (Fletcher & Kalofonos, 2022). Following the HV ethos, VVV facilitators uphold a set of values emphasizing acceptance and making sense of unusual experiences, an openness to all explanatory frameworks (biomedical, psychological, spiritual, paranormal, etc.), sharing diverse pathways to coping and recovery, and exploring the role of psychosocial adversity in onset and persistence of unusual experiences (Hearing Voices Network USA, 2020; Longden et al., 2018). Rather than use clinical terminology to categorize participants, facilitators employ language participants themselves use to describe their experiences. VVV groups draw on tools and approaches disseminated through the HV movement (Parker et al., 2021; Schnackenberg et al., 2014).
Participants
Participants in VVV groups were referred by mental health clinicians. Eligibility criteria included: (1) mental health service receipt at GLAVAHS, (2) currently experiencing psychosis, and (3) willingness to attend weekly virtual group sessions.
Fifty-six Veterans were referred to VVV groups. All were invited to participate in the study. Thirteen of these referrals declined to participate in groups; six could not be contacted; two wanted to participate but had scheduling conflicts; one moved away during recruitment. Participants could attend via video conferencing platform or telephone. Of 34 who agreed to participate in groups and the study, 5 completed pre-intervention assessments but never attended a group. Of 29 who attended at least one group and completed a pre-intervention assessment (described below), 21 completed post-intervention assessments (Figure 1). Of eight who did not complete post-intervention assessments, one opted not to participate due to feeling unwell, one had scheduling conflicts, and six could not be contacted.
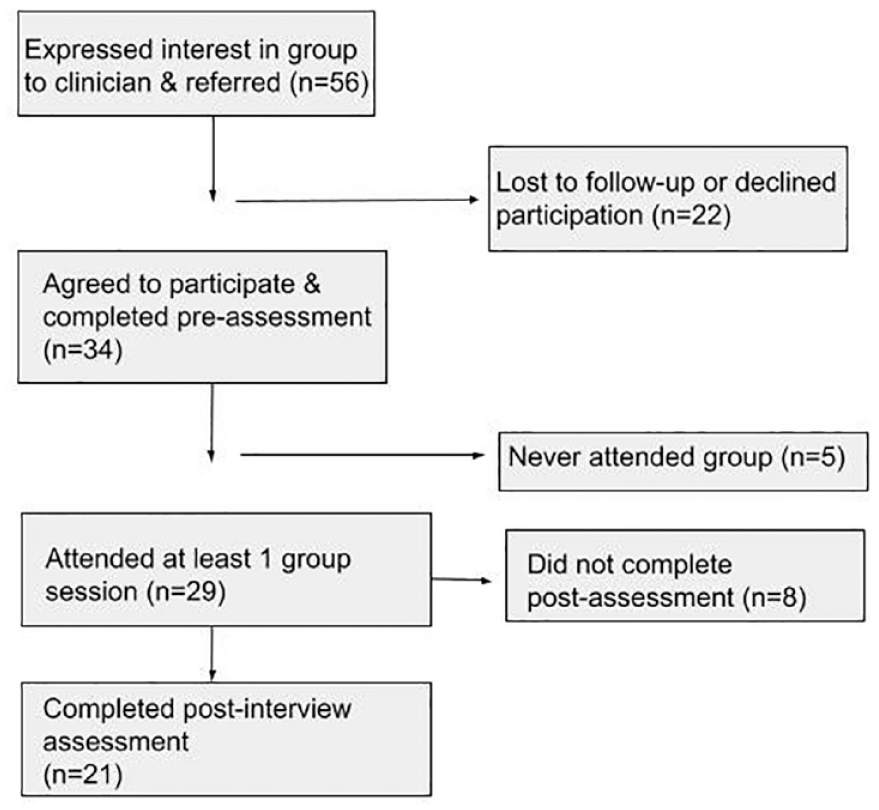
Research flow diagram of participant progression through the study.
Assessment measures
Primary outcome measures were selected to explore our hypothesis that participating in VVV would reduce distress and negative beliefs about voices and perceived power of voices. These measures have a demonstrated sensitivity to change in samples of people experiencing psychosis. Two primary outcome measures were collected at two points via video or telephone interview: pre-intervention, from 29 participants; and post-intervention (16 weeks) from 21 participants.
One primary outcome measure was overall Psychotic Symptoms Rating Scale (PSYRATS; Haddock et al., 1999) score. Secondary outcome measures from this scale included two subscales, rating auditory hallucinations (PSYRATS-AH) and delusions (PSYRATS-DS). PSYRATS has 17 items. PSYRATS-AH is an 11-item subscale assessing frequency, duration, severity, loudness, location, negative content, controllability of voices, intensity of distress, beliefs about origin of voices, and disruption, while PSYRATS-DS is a 6-item scale assessing preoccupation, distress, duration, conviction, intensity of distress, and disruption related to reported unusual beliefs. Items are rated on a five-point ordinal scale (0–4), range is 0 to 68. PSYRATS has strong inter-rater reliability (r ⩾ 0.9) (Haddock et al., 1999), test-retest reliability (0.55–0.74), and good validity (0.63–0.76) (Drake et al., 2006).
The second primary outcome was from the Revised Beliefs about Voices Questionnaire (BAVQ-R; Chadwick et al., 2000), a measure of a person’s beliefs, emotions and behavior in response to voices. Each item has a four-point response range (0–3). The 35-item questionnaire forms five sub-scales: three concerning beliefs about the dominant voice (malevolence, benevolence and omnipotence, range 0–18), and two concerning emotional and behavioral reactions (resistance, range 0–27, and engagement, range 0–24). The subscales demonstrate good psychometric properties. BAVQ-R shows acceptable levels of construct validity, there is a strong relationship between malevolence and resistance (r = 0.68, df = 69, p < .01) and benevolence and engagement (r = 0.80, df = 69, p < .1), with all other correlations between these subscales being strongly negative (Chadwick et al., 2000). We combined three subscales concerning beliefs about the dominant voice (malevolence, benevolence, and omnipotence) to create a single composite beliefs scale, with the benevolence subscale reverse-scored, so higher scores in every sub-scale reflected higher levels of negativity surrounding beliefs about voices. This composite scale was a secondary outcome.
The PSYRATS and BAVQ-R questionnaires were delivered by a member of the research team via video or telephone at week 16. Qualitative, semi-structured interviews were conducted via video or telephone at week 8 and week 16. These interviews used open-ended questions prompting participants to reflect on their experiences in groups, insights about themselves or their experiences, life changes, motivations for participation, and recommendations for improvements.
Statistical analysis
Statistical analyses were conducted using SPSS v28. To examine effects of VVV group participation in terms of positive symptoms (PSYRATS) and beliefs about voices (BAVQ-R), a mixed linear model was used. One subject who did not endorse any psychotic symptoms pre-intervention was dropped from the PSYRATS analysis.
We employed a repeated measures (pre-post) linear mixed model to examine VVV groups’ effects on each variable. We used a random effects platform with compound symmetry-correlation metric. Time (baseline vs. post-experience) was the repeated-measure variable (wave); number of training sessions attended was entered as a covariate. We analyzed cohort as a between-subjects variable to determine if there were meaningful differences between specific VVV groups (i.e., cohorts). Two primary dependent variables were the composite scores from PSYRATS and BAVQ-R. For significant results on composite scores, follow-up analyses were conducted to determine which sub-scores drove overall effect. We also examined cohort-by-time interaction to assess whether any groups showed differential treatment effects.
Qualitative analysis
Qualitative interviews were audio recorded and professionally transcribed. Data were analyzed using a modified grounded theory approach (Strauss & Corbin, 1990), involving data coding, conceptual category development, analytic memoing, and summary of emerging constructs using Atlas.ti software. A preliminary coding framework was developed based on interview questions, codes, and their definitions. Data were separately coded by two authors (IK and EF) who discussed discrepancies and refined codes. They then identified themes and subthemes. Qualitative and quantitative data were analyzed separately and brought together to understand outcomes and participant experiences.
Results
The data for participants who attended at least 1 VVV group are included in analyses (N = 29). Mean number of sessions attended was 8 (SD 6.1; range = 1–16). Sixty-six percent of participants attended at least half of the sessions, and 31% attended at least 75% of the sessions. There were five groups and six to eight individuals were invited to each group. Session-by-session attendance varied from a low of one participant to a high of 6.
Sample characteristics
Demographic data were obtained from clinical charts and are provided in Table 1. Women were oversampled to form a women’s group. Single gender groups were a part of the study design. Patients at the GLAVAHS are 85% male, and we thought women Veterans might appreciate a group for women. All participants were diagnosed with a psychosis spectrum disorder and prescribed antipsychotic medication. The majority (83%) had experienced at least one psychiatric hospital admission.
Demographic data of study participants.
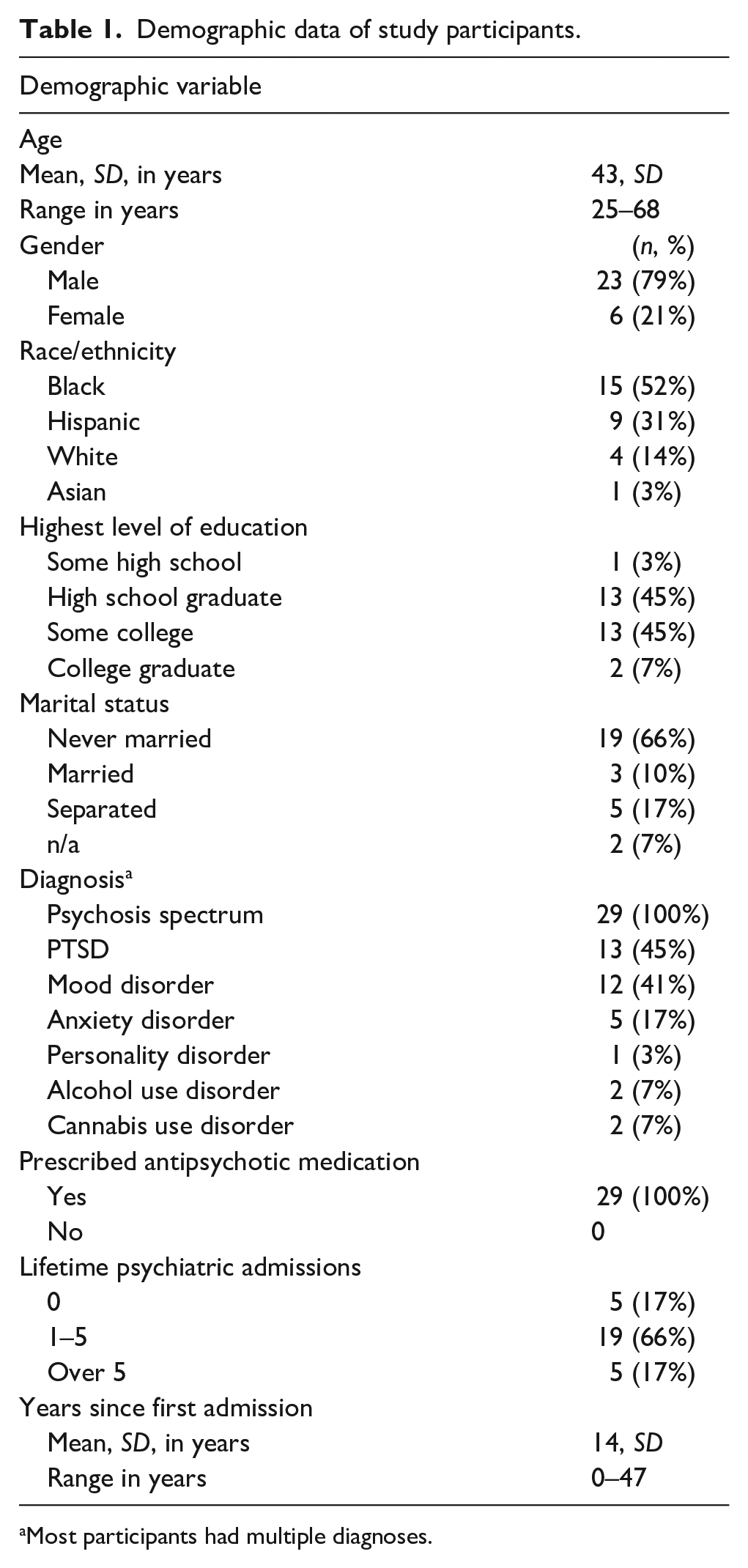
Most participants had multiple diagnoses.
At baseline, 27 participants who completed PSYRATS total had a mean score of 43.5 (19–61.63, SD 10.7). For PSYRATS-AH, mean was 29.6 (11–40, SD 6.2) and for PSYRATS-D 13.9 (0–23, SD 6.3). These scores are comparable to those from clinical samples at non-VA settings (Woodward et al., 2014).
Primary outcome measures
PSYRATS
The results of the linear mixed model on psychotic symptoms revealed an 18% reduction in PSYRATS total score from pre-intervention to post-intervention assessment, F(1,19) = 5.3664; p = .032 (Figure 2). PSYRATS total is a composite score reflecting several dimensions of psychotic symptoms, with a reduction indicating subjective improvement. Follow-up analyses on PSYRATS subscore of hallucinations revealed a 21% reduction from pre-intervention to post-intervention assessment, F(1,21) = 9.050, p = .007 (Figure 3). In this analysis, there was also a nonsignificant trend level effect of cohort, F(4,23) = 2.675, p = .057. This indicates there may be differences in symptom severity between groups. Analyses of the four subscales of the hallucination subscore found significant reductions across time for distress (20% reduction, F[1,20] = 6.422, p = .020), attribution (24% reduction, F[1,16] = 10.530, p = .005), and loudness (36% reduction, F[1,18] = 7.810, p = .012), but not for frequency of unusual experiences (F[1,18] = 1.821, p = .194). PSYRATS subscore for delusions did not significantly change from pre-intervention to post-intervention assessment, F(1,18) = 1.017, p = .327.
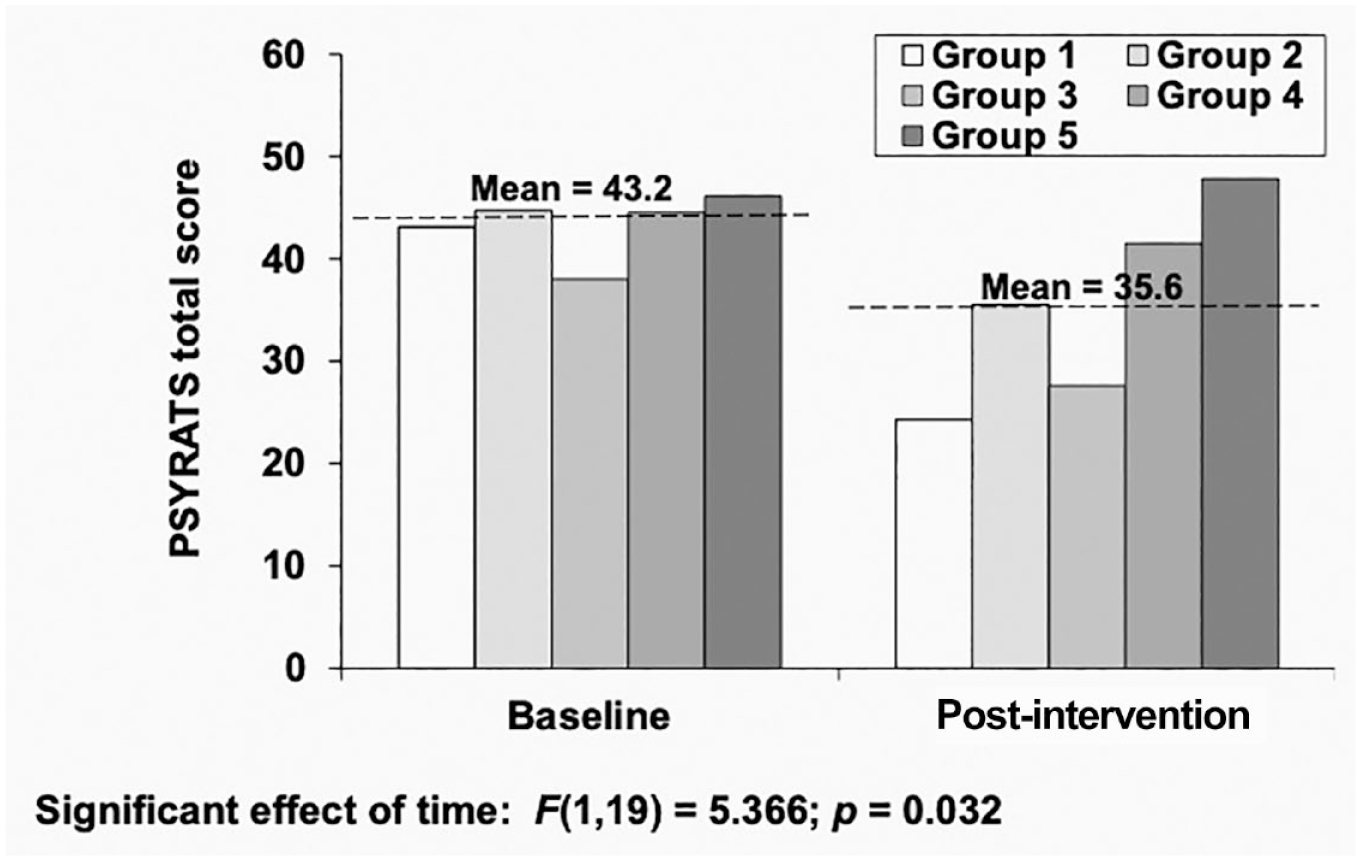
Veteran voices and visions effects on the PSYRATS.
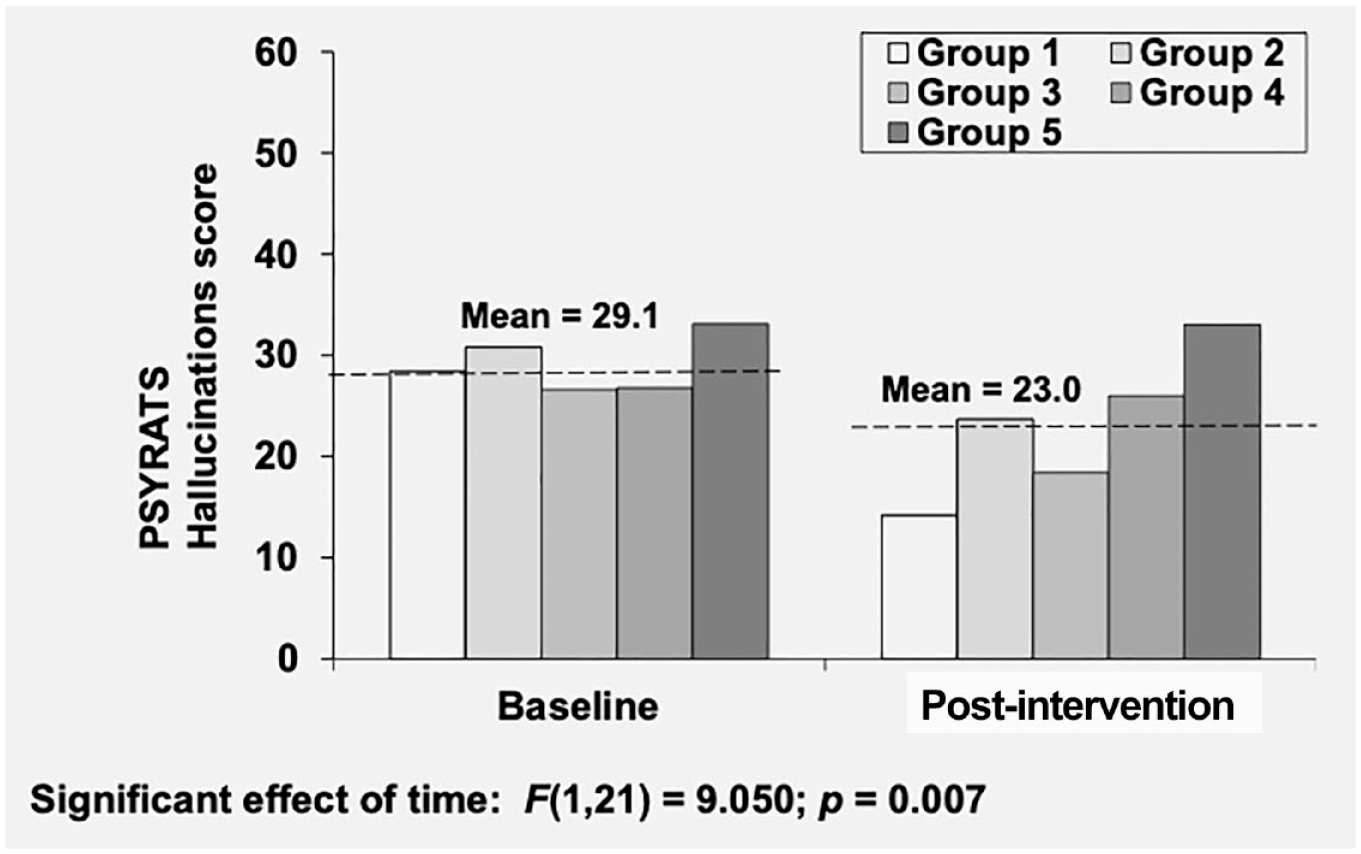
Veteran voices and visions effects on the PSYRATS hallucinations subscale.
Bavq-r
Analysis of the BAVQ-R Benevolence-Malevolence-Omnipotence composite scale revealed significant reduction from pre-intervention to post-intervention assessment, F(1,15) = 6.486, p = .022, as well as a significant time-by-cohort interaction, F(4,15) = 5.928, p = .004 (Figure 4). This indicates participants reduced their negative beliefs about their voices. Groups 1, 2, and 3 contributed to this finding, while group 5 had a marginal reduction and group 4 increased across time. Any interpretation about characteristics of Veterans or group facilitators contributing to this reduction should be tempered due to the small number of participants and inability to do any formal follow-up statistical analyses. Follow-up examination of individual subscales found no other significant findings, Benevolence, F(1,14) = 0.267, p = .613; Malevolence, F(1,17) = 2.917, p = 0.106; Omnipotence, F(1,17) = 0.750, p = .398.
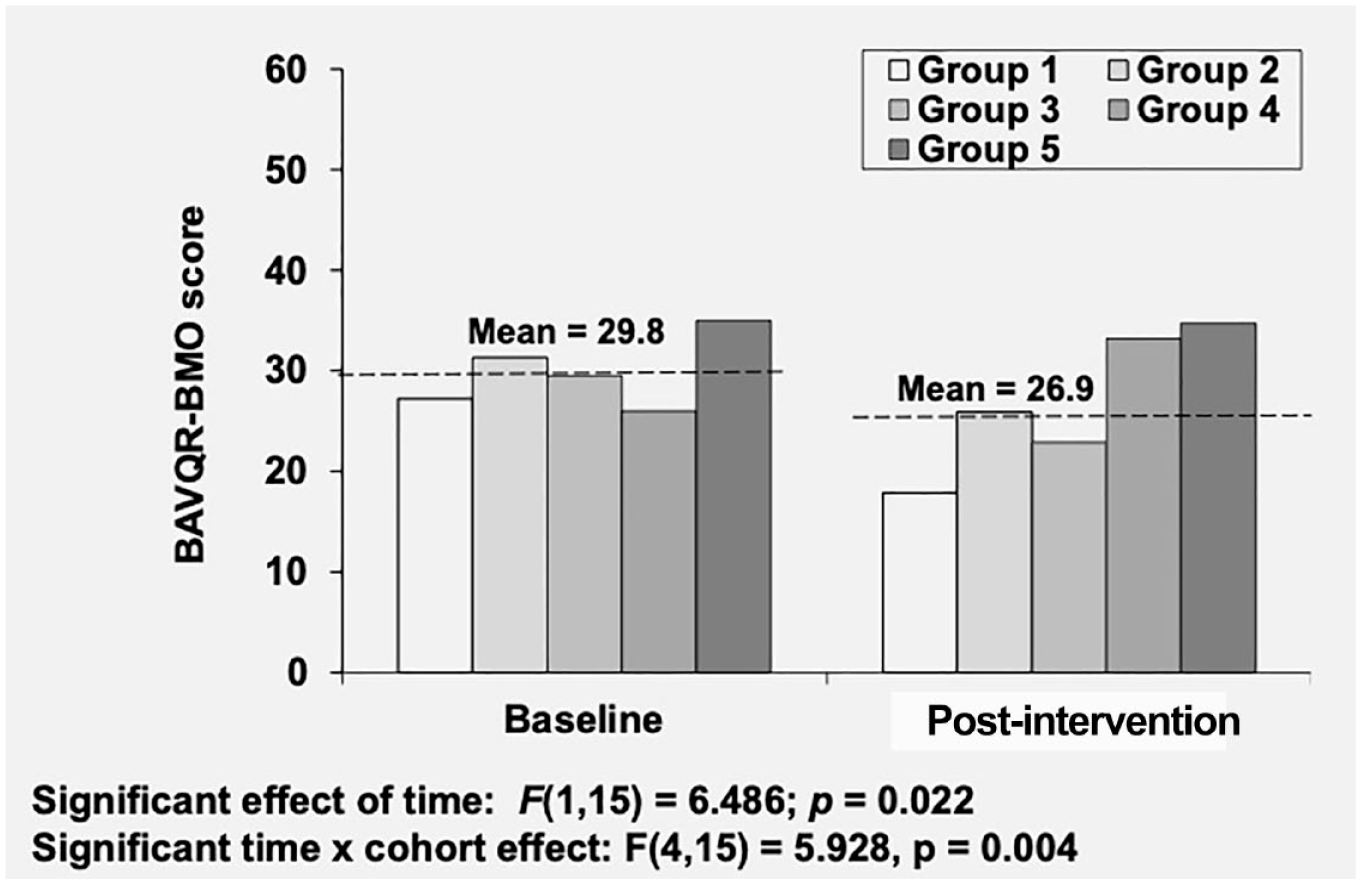
Veteran voices and visions effects on BAVQ-R – BMO composite score.
The analysis of BAVQ-R Resistance scale yielded non-significant results, F(1,16) = 3.040, p = .101. For the Engagement scale, there was a non-significant trend-level reduction across time, F(1,15) = 4.037; p = .063.
The quantitative findings show a significant reduction in distress related to voices, but not related to delusions as measured by PSYRATS. The BAVQ-R composite scale on beliefs regarding voices showed a significant change and the engagement scale showed a trend-level reduction. None of the BAVQ-R subscales showed significant results.
Qualitative results
Qualitative findings centered around four major themes: (1) normalization and camaraderie; (2) increased hope and confidence; (3) self-understanding and reframing experiences; (4) relationship-building outside groups.
Normalization and camaraderie
At baseline, participants reported social isolation. They felt uncomfortable talking about their experiences with friends and family members. Most participants had not developed relationships with others who heard voices, and several stated they learned to keep voice-hearing a secret because self-disclosure tended to result in exclusion and rejection. Groups created spaces to share what many considered to be shameful experiences with others, and most of those interviewed (16 of 21, 76%) felt as though they had benefited from connecting with other participants. Groups instilled a sense of shared experience: I truly know now that I’m not alone. And if you can get through it, I can, too. I think about my brothers all week long when I’m going through what I’m going through. I can’t wait ‘til [group], so we can talk about it. It makes me feel more normal, because there’s other people that I’m able to relate to, and so it’s sort of helped me learn to accept things about myself more.
These responses provide evidence that the emergence of camaraderie and normalization facilitated self-acceptance for participants. This was often linked to increased ability to successfully live with their voices. Normalization did not necessarily lead to building close relationships between participants, but it helped improve how they related to themselves. Some participants talked about an altruistic desire to support each other by regularly attending groups.
Increased hope and confidence
Hearing about how other Veterans continue to live their lives despite the presence of psychosis gave participants hope and confidence in their own ability to establish and maintain social roles. Tied to this hope was a sense it was possible to have a better relationship with unusual experiences, including more control over responses to voices. Fourteen of 21 (67%) participants mentioned increased hope, confidence, and/or happiness because of joining groups: I’m a little less terrified of life, a little less depressed. It’s nice to see a light at the end of the tunnel. I think I could have a happy life. Things don’t have to be so hard. That’s what I’ve been thinking, just dealing with everything and figuring out what everything means and seeing people have some control over this thing that seems like it’s uncontrollable. It’s nice because you get to hear [other] perspectives and some of the people who have been dealing with this longer, what they do to cope with things. It just opened me up to new ideas and new ways of handling the situation.
Increased hope and confidence may have come from participants sharing their own coping strategies and serving as role models for each other in successfully navigating difficult experiences.
Self-understanding and reframing unusual experiences
Most participants had learned to view their experiences as symptoms related to mental illness, and many ignored or distracted themselves from their experiences and took medication. Most also held personally meaningful interpretations of their experiences, such as religious, spiritual, or psychological frameworks. Groups provided a unique opportunity to share and explore these frameworks. Listening to others talk about their voices and becoming more curious about the origin and meaning of voices also inspired participants to describe specific characteristics about their voices and situations when they appear. For most participants (13 of 21, 62%), this resulted in increased self-understanding and a positive reframing of experiences: I don’t feel too many negative emotions towards them [the voices] anymore. . . being able to talk about it without people wanting to run away, and people taking interest in what I’m experiencing makes me want to fully explain it all. Just being able to get it off my chest. I’ve never been able to explain that to anybody. We’re talking so much about the specifics, which I’ve never really done with anyone at all . . . and I’ve had realizations about myself . . . I think that some of the reasons that I have these voices and visions are to do with trauma.
The ability to share details of experiences, such as tenor, gender, or age of a voice, helped participants reframe their experiences. Some connected past trauma to current experiences. For others, their voices reminded them of deceased loved ones whose presence guided and protected them. Some Veterans shifted negative associations they had with their experiences towards a more neutral or even positive perspective.
Relationship-building outside groups
Fourteen of 21 (67%) mentioned group involvement resulted in relationship-building outside of groups. This included both deepening existing relationships and creating new ones. Examples included: socializing more with friends and family, sharing struggles with others and receiving additional support, participating more in community events like church, and taking on new challenges like applying for employment, educational, and housing opportunities. For some, these activities were major life goals requiring courage and persistence to address: I can say that being in the group has helped me to be able to function better and communicate better with my mom, for me to listen more because everybody needs somebody to listen to when they get full of knowledge or whatever it may be, that they may need to get off their chest. I would say the group made me confident in taking this [new] job. It made me more open.
Because most participants had tenuous social relationships and experienced social isolation at the start of groups, shifts in their confidence and ability to form relationships outside groups had a profound impact on their daily lives.
Discussion
This is the first US-based study to adapt the HV approach to a large healthcare system, using clinical assessments to identify changes in how people relate to their unusual experiences. We observed reductions in distress associated with voices, as well as a reduction in negativity surrounding beliefs about voices. Previous studies of US-based HV groups have involved qualitative interviews of group members (Hornstein et al., 2022) and a survey of group facilitators (Jones et al., 2015), largely outside of health services. Most literature on HV groups consists of small-scale cross-sectional studies and surveys of groups located both within and outside of health services, with most from the UK, Australia, and Netherlands (Branitsky et al., 2021; Schaefer et al., 2021).
One exception to this literature is an Australian quasi-experimental design study employing mixed-methods to assess outcomes of a group approach combining aspects of HV with CBTp in a mental health system (Kay et al., 2022). This study found a statistically significant reduction in PSYRATS-AH score. BAVQ-R subscales showed statistically significant increases in engagement and benevolence scores and statistically significant decreases in malevolence, omnipotence, and resistance scores. These findings align with our study’s outcomes on the efficacy of VVV groups to reduce distress and negative associations related to voices. Like the current study, it is an adaptation to a mental health system, but our adaptation draws exclusively on the HV model without incorporating CBTp.
According to HV values, individuals are free to attend group sessions as often as they wish, thus attendance was not mandatory, nor were group members pressured to attend beyond being sent weekly reminders of the group meeting time. We did not have a predetermined idea of the minimal number likely to be helpful, beyond the supposition that the more groups attended, the stronger the likely outcome. Based on our experience, we believe that even a single group attended could have a significant effect, and our qualitative data did reflect this to some degree as a few individuals we interviewed who had attended only one or two groups did comment on feeling camaraderie with fellow voice-hearers, feeling accepted and ‘normal’, as well as feeling increased hope and confidence. In qualitative interviews, we also asked Veterans if they had a preference regarding groups that were single or mixed gender, and most participants did not express a preference for single-gender groups.
Our study found a statistically significant reduction in distress due to auditory hallucinations, as measured by PSYRATS, but not in their frequency. This is in keeping with HV values advocating for accepting rather than eliminating voices or other experiences. It may indicate participants developed a greater understanding and familiarity with their voices, learning to live with them. Our qualitative findings supported this, as 62% reported increased self-understanding and reframing helping them better live with their experiences. This is consistent with literature indicating many interventions reducing distress related to voices do so without changing frequency of voices (Branitsky et al., 2021; Sitko et al., 2020). Normalization and camaraderie and increased hope and confidence reported by participants may also have contributed to reduced distress. These findings may be related to increased relationship-building outside groups.
Our BAVQ-R composite scale combining benevolence, malevolence, and omnipotence measures showed an overall improvement despite no change in individual subscales. In contrast to Kay et al., engagement showed a trend-level reduction, contradicting our goal of increasing engagement with voices. This may reflect that the dominant coping strategies individuals came to groups with involved distraction and attempts to eliminate voices. Our qualitative findings suggested Veterans gained a greater sense of self-determination in relation to their voices. For example, they learned they did not have to do what voices told them to do, but rather examined emotions underlying voices’ demands.
Our findings suggest VVV groups contribute to recovery by reducing social isolation and creating a supportive community in ways consistent with existing research on peer support groups indicating they offer solidarity, provide an accepting and supportive environment for sharing experiences, exchanging coping strategies, and developing social connections (Corentin et al., 2023). Our findings also resonate with international research showing HV groups help individuals understand their own experiences, gain a sense of agency, and increase confidence in sharing their experiences with people outside groups (Branitsky et al., 2021). Likewise, Hornstein et al. (2020) suggest processes of discovery, growth, and change are crucial components of how people engage with HV groups over time. These findings highlight groups as a resource for individuals living with unusual experiences, offering an opportunity for meaning-making, personal growth, and collective healing.
Limitations
This was a small pilot study, limiting generalizability. The lack of a comparison group makes it difficult to conclusively attribute changes to group participation. As the questionnaires were administered by the research team, there was the possibility of rater bias. However, the uneven pattern of results and sufficiently wide range of scores across test variables suggest otherwise. The relatively short duration of this 16-week study may underestimate the approach’s potential. In traditional HV groups, members may attend for several months or years before noticing meaningful changes (Branitsky et al., 2021). While we demonstrated a reduction in distress and a shift in how participants viewed their voices, we did not assess broader outcomes of holistic recovery using standardized scales. Groups do address delusions and sensory experiences beyond voices, but we did not thoroughly assess distress due to these experiences.
Conclusion
Future research should assess distress related to other aspects of experience as well as assess for social functioning and overall recovery while continuing to explore the effectiveness of the HV approach in a variety of populations and settings in ways that preserve the movement’s core values.
HV researchers have been cautious about making outcome-oriented assessments, preferring to center subjective testimonies as measures of success (Corstens et al., 2014). Should HV groups become instrumentalized as a part of clinical services, HV researchers and advocates fear explicitly peer-based approaches to valuing experiences of self-reported recovery and growth may be lost to clinical definitions of functional recovery, and mission creep may erode unique, user-driven qualities of HV groups (Styron et al., 2017). To prevent this, HV researchers advocate for leadership of researchers with lived experience throughout the research process, along with ongoing community engagement with HV groups (Jones et al., 2021; Longden et al., 2018).
We have consulted and collaborated with researchers and HV trainers with lived experience. Our research team, who – at the time of this study’s completion – did not include any members with lived experience, recognizes these critiques, even as we see value to adapting the HV approach to the VA healthcare system, making it accessible to Veterans via standardized, outcome-oriented measures. As we continue this project, we aim to: include Veterans with lived experience, preserve the values and ethos of the HV approach to work across differences, and find common ground within and outside of traditional mental health epistemologies and care. These efforts seek to continue the legacy of voice hearer and clinician/researcher partnerships on which the Hearing Voices movement was founded (Bullimore & Carson, 2022).
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by an Agency for Healthcare Research and Quality (AHRQ) – Patient-Centered Outcomes Research Institute (PCORI) Stakeholder-Partnered Implementation Research and Innovation Translation (SPIRIT) K12 Award, a VA Research Enhancement Award Program (REAP) on Enhancing Community Integration for Homeless Veterans Pilot Grant, and a Greater Los Angeles VA/UCLA Center of Excellence for Veteran Resilience and Recovery Pilot Grant.