
Abstract
Moral elevation is a positive emotion described as feeling inspired by others’ virtuous actions. Elevation has several psychosocial benefits, some of which may be relevant to trauma-related distress; however, past studies have primarily examined elevation in nonclinical, civilian populations or in naturalistic studies. This experimental study used mixed methods to assess if veterans with post-traumatic stress disorder (PTSD) experience elevation when exposed to elevation stimuli in a controlled setting. Participants included 47 veterans with significant PTSD symptoms. Following baseline measures and a written trauma narrative, veterans were randomized to an elevation or amusement condition where they viewed two videos intended to elicit the condition emotion. Veterans also provided a written journal response describing their reaction to the videos. Self-report measures were administered after each study task to assess state-level elevation and amusement. Veterans randomized to the elevation condition reported significantly higher levels of elevation after videos compared to veterans in the amusement condition. Qualitative results offered further support for differences between groups and identified unique themes related to the experience of elevation. Overall, findings indicate it is possible to induce elevation in veterans with significant PTSD symptoms. Additionally, qualitative results highlight specific benefits of elevation and potential targets for treatment integration and future exploration.
Introduction
Post-traumatic stress disorder (PTSD) is associated with significant distress and functional impairment. Veterans, in particular, are at increased risk for trauma exposure and subsequent PTSD symptoms (Hoge et al., 2004; Richardson et al., 2010). Given the prevalence and consequences of PTSD in veterans (Brockman et al., 2016; Rodriguez et al., 2012), novel approaches are needed to continue improving the delivery, retention, and effectiveness of trauma treatment (Steenkamp et al., 2015). One potential pathway that could address this need and facilitate trauma recovery in this clinical population is moral elevation.
Moral elevation definition and benefits
Moral elevation (hereafter, elevation) is a positive emotional state with features that are distinctive from other emotions such as what triggers it, the emotional and physical response, and the subsequent action tendency or motivation. First, elevation is triggered by witnessing another person perform an act you would consider incredibly virtuous, such as an act of remarkable generosity, compassion, or perseverance. This witnessed event can lead the observer to feel inspired and uplifted in response, accompanied by positive physical sensations that can include warmth in the chest, goosebumps (i.e., piloerection), tears, and a lump in the throat (Algoe & Haidt, 2009). This experience is typically followed by strong desires to emulate the witnessed virtuous behavior (e.g., “I want to act generously too”), become a better person, and engage with others (Aquino et al., 2011; Oliver et al., 2012).
Several studies have examined elevation in nonclinical, civilian populations and found multiple psychological and social benefits. As mentioned, after experiencing elevation, people often report motivations to become a better person themselves. People also report more affiliative behaviors, feeling more compassionate and connected to others, and show greater responsiveness in relationships (Cox, 2010; Erickson et al., 2017; Van de Vyver & Abrams, 2017). Several studies also found increased prosocial behavior following exposure to elevation stimuli (Schnall et al., 2010; Schnall & Roper, 2012; Van de Vyver & Abrams, 2015). Notably, several studies have demonstrated the unique benefits of elevation by comparing the effects of elevation stimuli to other positive-valenced emotions such as gratitude, amusement, and admiration (Algoe & Haidt, 2009; Diessner et al., 2013; Van Cappellen et al., 2013). For example, one study tested the effects of viewing brief, daily videos that elicited elevation or amusement in an undergraduate sample and found those who viewed elevation videos reported higher daily positive affect, compassionate goals, and social affiliation (Erickson et al., 2017). One gap in this area of research is that limited studies have examined elevation in clinical populations; however, there is some evidence that suggests the same benefits may be present—such as one study that found daily elevation was associated with lower daily symptoms of anxiety, dysphoria, and hostility in people with mild to moderate anxiety and depression (Erickson & Abelson, 2012).
Elevation and PTSD
Given the need to improve and expand upon PTSD treatment, and the known benefits of elevation to date, elevation may offer a unique contribution to trauma treatment. One reason this might be the case is because arguably, elevation and its benefits are antithetical to PTSD. For example, since elevation is triggered by witnessing someone perform a virtuous act, the observer is likely to perceive that person as moral, upstanding, or praiseworthy, whereas PTSD symptoms are associated with strong negative cognitions that can include negative beliefs about other people or the world (e.g., “People can’t be trusted”; Foa et al., 1999). Additionally, elevation is considered to be a strong, positive emotional experience that is also associated with involuntary physical reactions (e.g., tears of joy); on the other hand, people with PTSD often report difficulties with experiencing positive emotions or feeling numb when exposed to positive stimuli (Farnsworth et al., 2014; Kashdan et al., 2006). Lastly, PTSD is associated with avoidance behavior and isolation, whereas elevation is considered an approach-oriented emotion (Van de Vyver & Abrams, 2017) that often leads to increased desires to engage with others. In sum, the theoretical framework of elevation suggests it could potentially be used to facilitate or aid trauma recovery.
Despite the clear potential of a hypothesized link between elevation and trauma distress, few studies have tested this theory in clinical populations with PTSD. One study assessed elevation experienced by civilians reporting subclinical symptoms in the aftermath of a campus shooting and found higher elevation was associated with greater compassion and higher post-traumatic growth 4 months later (Tingey et al., 2019). A separate pilot study measured elevation experienced by veterans while participating in a residential PTSD treatment program and found weekly elevation was associated with greater weekly group engagement in the same week and future weeks, as well as large, negative correlations with avoidance symptoms at post-treatment (McGuire et al., 2019). The same study also found large, negative correlations with moral injury—significant distress after witnessing or performing a transgressive act that violates one’s personal values (Frankfurt & Frazier, 2016; Litz et al., 2009)—which could suggest that elevation has wider implications for other types of trauma distress in addition to PTSD symptoms. Overall, these select studies offer initial support to the potential utility of elevation in populations with PTSD with direct observations of possible benefits for veterans with significant PTSD symptoms.
Although preliminary research provides some valuable support given the demonstration of effects in naturalistic contexts, there are several limitations to previous studies that assessed clinical samples. To date, findings were based on self-report measures of elevation in the context of uncontrolled settings, which lacked internal validity. Therefore, it’s unclear if self-reports of elevation were in direct response of observed virtuous behavior—consistent with a core feature of this emotion—or if these measures captured general positive affect elicited by other positively valenced stimuli (e.g., something perceived as entertaining or amusing). Moreover, it’s still unknown if people with significant PTSD symptoms are capable of experiencing this emotion in the first place. The antithetical nature of elevation and PTSD could mean elevation might serve as an antidote to certain symptoms, but it could also indicate that characteristics of PTSD—such as strong negative beliefs about others and difficulties experiencing positive emotions—could significantly interfere with one’s ability to feel moved and touched by witnessing a virtuous act (i.e., to experience elevation). Further examination is needed that includes greater control of the stimulus that elicits elevation, as well as multimeasurement methods to expand our understanding of how this emotion is experienced in this clinical population. Doing so would further support the clinical utility of elevation by determining whether emotion induction is possible, and it might identify potential mechanisms by which the experience of elevation may be helpful for people struggling with PTSD.
Current study
The overall purpose of the reported study was to better understand the experience and benefits of elevation in veterans with significant PTSD symptoms. The primary aim of this study, and the objective of this article, is to assess whether veterans with significant PTSD symptoms report an elevation response consistent with findings in nonclinical, civilian populations as indicated by a distinct response to elevation stimuli versus other positive stimuli. We investigated this response using a mixed method approach. Specifically, we examined quantitative and qualitative data from veterans with significant symptoms of PTSD who were randomly assigned to view elevation-inducing video clips or amusement-inducing video clips. We hypothesized that participants viewing the elevation videos would report higher state elevation compared to those in the amusement condition. Qualitative data were also analyzed to contribute toward the understanding of observed differences in the quantitative data. Given the dearth of research regarding elevation responses in veterans with PTSD, qualitative analyses were largely exploratory; however, we hypothesized that qualitative responses would include distinct features that could be categorized as cognitive, emotional, physical, and motivation-based reactions to stimuli. Further, we expected qualitative responses would be consistent with quantitative data and previous research regarding differences in the reactions to elevation versus amusement stimuli. The process of examining specific subthemes for responses was considered exploratory as this pilot study aimed to learn from participants’ experiences by utilizing an inductive approach—identifying subthemes based on responses.
Method
Participants
We enrolled 48 veterans who endorsed significant PTSD symptoms. Recruitment methods included posting flyers on Veterans Health Administrations’ (VHA) medical center campuses, in-person recruitment in PTSD clinics, and direct referrals from VHA clinicians. One participant was excluded because of repeated disruptions in the experimental session that compromised the fidelity of session tasks. The final sample used for analysis included 47 veterans (M age = 48.60, SD = 12.71; 91.5% male). Participants identified as White (63.8%), Black (27.7%), American Indian (4.3%), Asian (2.1%), or other (2.1%); 19.1% identified as Hispanic or Latino/a. Most veterans served in the Army (78.7%), followed by the Marines (10.6%). The greatest proportion served in Iraq and/or Afghanistan (72.3%), followed by Vietnam (8.5%). All participants provided written informed consent and this study was approved by the local institutional review board.
Procedures
First, veterans were screened for potential eligibility using the Posttraumatic Checklist Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (PCL-5; Weathers et al., 2013). Veterans with a total score of 32 or higher were viewed as experiencing significant symptoms of PTSD and therefore, deemed eligible and invited to participate in the study. Participation involved one, in-person appointment that included several study tasks and repeated measurements (see Figure 1). Some features of this study design are not relevant to the aims of this article and some planned analyses (i.e., secondary aims) require larger sample sizes before they can be tested; however, here we will describe all tasks and measurements completed by participants, so results can be appropriately interpreted in the context of the full experiment.

Study timeline of tasks and measurements associated with reported analyses.
Following informed consent, veterans completed baseline measures to assess demographics and trait-like constructs. 1 After baseline measures, veterans were asked to write about their worst traumatic event in detail for 15 minutes, followed by self-report measures of trauma-related thoughts and emotions. Those same measures were administered at the end of the experiment. This procedure served multiple purposes. First, a secondary aim of this study is to assess whether exposure to elevation stimuli reduces state-level distress relevant to PTSD symptoms. Therefore, eliciting trauma-related thoughts and emotions allows for future examination of the immediate impact of elevation on distress directly related to the trauma. A larger sample size is needed to conduct analyses for the secondary aim; thus, we have no findings to report to date. Beyond the secondary aim, the trauma narrative serves the objectives of this article by allowing us to measure the experience of elevation in the aftermath of any negative thoughts and/or emotions about one’s traumatic event that may arise after writing about it—a state that could conceivably inhibit someone from being moved or inspired by witnessing virtuous acts. This procedure allows for an assessment of a veteran’s capacity to experience elevation in the context of experiencing salient PTSD symptoms and/or negative mood, rather than examining elevation in the context of a neutral or positive emotional state. The former provides a better opportunity to capture the feasibility, and consequently, the clinical utility of elevation for this clinical population.
After writing a trauma narrative, participants were presented with three video clips. After each video, they were asked to complete brief measures to assess state-level emotional responses to each video. The first video was a neutral stimulus that was intended to lack any positive or negative valence and it was shown to all participants. The neutral video was 5 minutes in length and it demonstrated how flutes are made. Next, depending on the condition they were randomized to, veterans viewed either two elevation (n = 24) or two amusement (n = 23) videos to elicit the target emotion. Video selection was based on previous studies that aimed to elicit elevation and/or amusement (Erickson et al., 2017; Silvers & Haidt, 2008). For both conditions, the two videos were approximately 7 minutes in length, combined. Each pair of videos was displayed in random order within each condition. The elevation condition videos included a story about a man who saved another man’s life on a subway track (E1: Subway Hero), and a story about a father and his son with paraplegia who competed in marathons as the father carried, pushed, and pulled his son during the races (E2: Team Hoyt). The amusement condition included a video about a baby biting his brother’s finger (A1: Charlie Bit My Finger) and a Seinfeld stand-up comedy routine about taxi cabs and air travel (A2: Seinfeld; see Supplemental Materials for links to all videos). Immediately after each video, participants were asked to complete a brief self-report measure that assessed state-level emotions for a total of two repeated state assessments.
After viewing all three videos, participants were given 10 minutes to complete an open journal response describing their reactions to the condition videos. Participants were allowed to either type or write their response on paper. Participants were prompted to consider (1) what stood out to them in the video, (2) what reactions did they have or notice, and (3) what did they feel like doing after watching the video.
Measures
PTSD symptoms
The PCL-5 (Weathers et al., 2013) is a 20-item self-report measure that assessed PTSD symptom severity in the past month. In addition to characterizing the sample, we used the PCL-5 to determine whether there were significant differences in symptom severity between conditions after randomization. Items were rated on a scale from 0 (not at all) to 4 (extremely) and summed to create a total score. A cutoff score of 32 was selected based on previous findings that a probable PTSD diagnosis is strongly associated with PCL-5 cutoff scores ranging from 31 to 33 (Bovin et al., 2016). The PCL-5 has demonstrated good reliability and validity in previous studies (Bovin et al., 2016; Wortmann et al., 2016) and good reliability in this study (α = .89).
State elevation
Currently, there are no standardized measures for assessing state elevation. The Elevation Scale (ES; Landis et al., 2009) or some version of it is widely used, but this scale assesses trait-like tendencies to experience elevation rather than a momentary state response. To capture state elevation in this study, we combined items adapted from the ES with items from a daily elevation measure previously used with a clinical population (i.e., mental health clinic outpatients with depression and anxiety; Erickson & Abelson, 2012). Instructions from the ES were altered by asking participants to rate the extent they experienced 12 items immediately after watching a video on a scale from 0 (not at all) to 4 (extremely). All items were summed to create a total score.
State amusement
We used 3 items (amused, entertained, laughing) to assess amusement following videos. Item selection was based on measures and findings from other studies that aimed to differentiate between elevation and amusement as distinct, positively valenced emotions (Algoe & Haidt, 2009; Erickson et al., 2017; Piper et al., 2015; Silvers & Haidt, 2008). The amusement items were randomly dispersed among the 12 elevation items with the same prompt and scale (i.e., a total of 15 items across amusement and elevation). The 3 items were summed to create a total score.
Data analysis
Quantitative
To test our first hypothesis that self-reported state elevation would differ across conditions, we used R (R Core Team, 2017) and the aov function of the base stats package to assess the main, between-person effect of experimental group using a two-way repeated measure analysis of variance. In this case, state elevation is measured twice for each participant (within-person effects) across both groups (between-person effects). State elevation was set as the outcome variable and condition or group was the predictor coded as 0 (amusement) or 1 (elevation).
Before testing the primary hypothesis, we conducted preliminary analyses of unconditional linear mixed effects models using the lme package (Pinheiro et al., 2019) to assess the reliability of state elevation and amusement measures. This multilevel method is recommended for nested data that violate the assumption of independence (Bonito et al., 2012; Nezlek, 2017). We used a three-level model structure with individual items for state elevation and amusement (Level 1) nested within each measure’s total score (Level 2) nested within each person (Level 3). Reliability estimates were calculated using the variance at item, total score, and person levels, providing a reliability estimate that is similar to Cronbach’s α while accounting for differences between repeated measurements and persons (Table 1).
Variance and reliability estimates for repeated measures.

Additionally, we conducted a manipulation check to verify that the condition videos elicited the desired emotion by using paired sample t tests to assess for within-person differences in the targeted emotion between the neutral video and the condition videos. Welch’s t test was used when Levene’s test indicated unequal variances. There was no missingness across all participants. Cohen’s d was calculated with the psych package (Revelle, 2020) and
Qualitative
Atlas.ti (v. 8.3, Atlas.ti Scientific Software Development GmbH, Berlin, Germany) software was used to support thematic analysis of the participants’ responses to the open-ended query of their reactions to the videos. Qualitative analysis occurred over three phases. Phase 1 was primarily deductive and employed direct content analysis (Hsieh & Shannon, 2005), using an a priori preliminary codebook to guide coding. This codebook was created with four main categories to reflect the distinct features of elevation as established by previous studies (e.g., Algoe & Haidt, 2009) that McGuire and colleagues (2019) developed into a model detailing the theorized link between distinct features of elevation and trauma-related distress. Specifically, the predefined deductive codes representing the four categories of distinct features of elevation included Thoughts and Reflections, Emotional Changes, Physical Changes, and Motivations (previously referred to as action tendencies). After the first author and an independent rater applied these codes to participants responses, the authors used an inductive approach (Phase 2) to identify subthemes based on participant responses that emerged under each of the four distinguishing features of elevation. The preliminary codebook was then updated with codes used to capture these additional emergent themes. The authors discussed the revised codebook with respect to specific participant responses to offer diverse interpretations of subthemes, which informed additional revisions to the codebook. In the third and final phase, the lead author used a deductive approach to recode all participant responses using the revised codebook.
Results
Quantitative results
On average, participants reported a PCL-5 score of 56.45 (SD = 11.85, range = 33–80). Despite randomization, veterans in the elevation condition endorsed significantly higher PTSD symptoms compared to those in the amusement condition (M diff = 8.00, t = −2.26, p = .029). Therefore, the main analysis also examined PCL-5 score as a covariate. Descriptive statistics for state elevation and amusement by video and condition are reported in Table 2. Notably, state elevation and amusement scores include a different number of items and ranges; therefore, comparisons of raw scores should be limited to comparing scores on a given state response between different stimuli (e.g., state elevation following an elevation video vs. state elevation following an amusement video). Figure 2 contains a scatterplot of all individual scores (standardized) for each video across both conditions.
Descriptive statistics for state elevation and amusement after each video.

Note. State elevation includes 12 items with a range of 0–48 and state amusement includes 3 items with a range of 0–12.
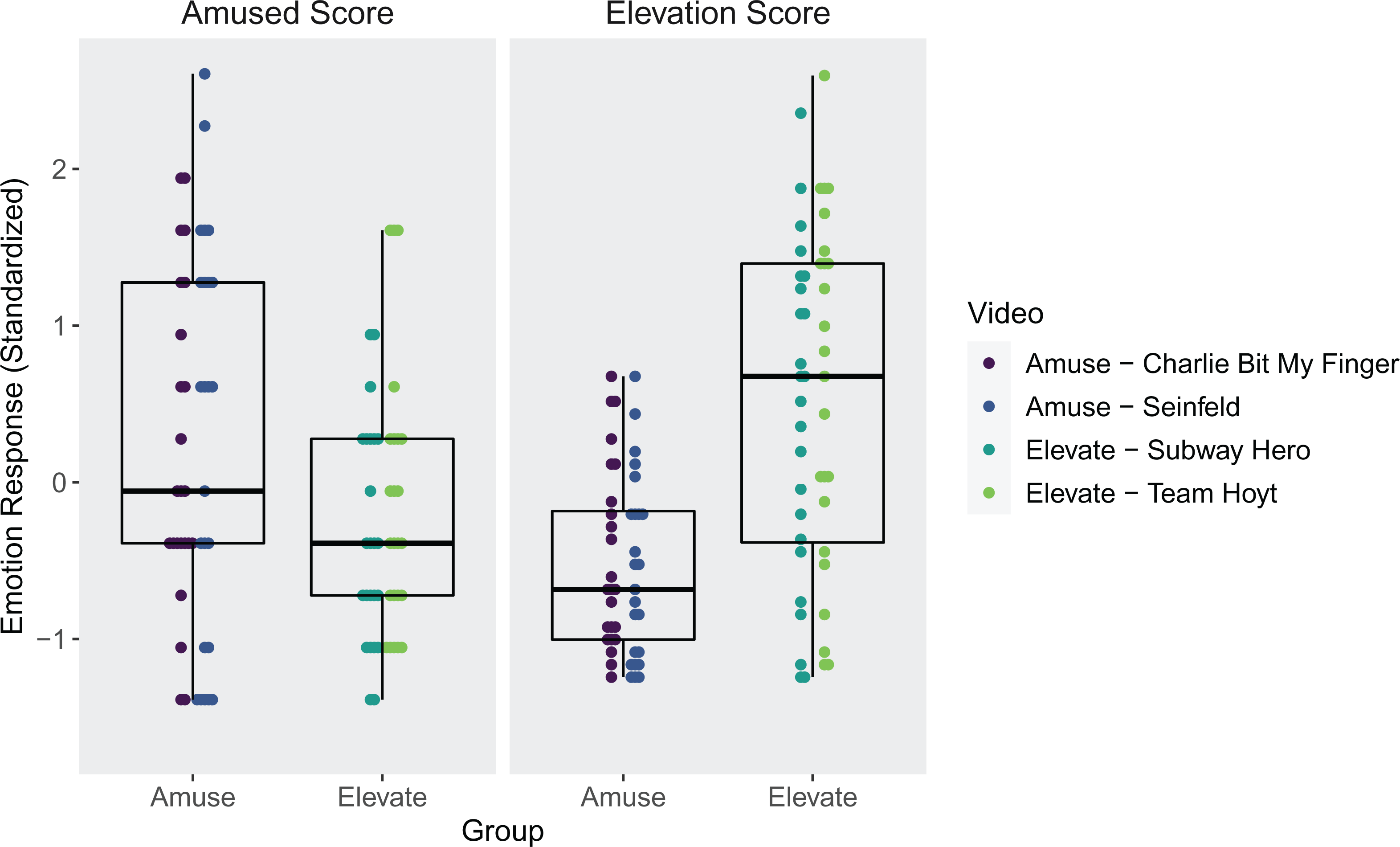
Scatterplot of state-level elevation and amusement following videos across both conditions with boxplot overlays that indicate 25th, 50th, and 75th percentile of score range.
Results from the manipulation check indicated that state elevation was significantly higher following both E1 (t = 5.45, p < .001, d = 1.57) and E2 (t = 7.45, p < .001, d = 2.15) videos compared to the neutral video. Similarly, state amusement was significantly higher following both A1 (t = 3.05, p = .006, d = 0.90) and A2 (t = 2.68, p = .014, d = 0.79) videos compared to the neutral video. It should be noted there was a wide range of elevation scores within the elevation condition (0–48) as highlighted by the scatterplot (Figure 2).
For the main analysis, controlling for baseline PTSD symptoms did not change the results; therefore, we report findings without PCL-5 scores as a covariate. As hypothesized, veterans who watched elevation videos reported significantly higher state elevation compared to those who viewed amusement videos, F(1, 45) = 17.95, p < .001,
Comparisons of state elevation scores following elevation versus amusement videos.

Note. E1 = Subway Hero (elevation); E2 = Team Hoyt (elevation); A1 = Charlie Bit Finger (amusement); A2 = Seinfeld (amusement); Welch’s two sample t test was used after Levene’s test of homogeneity indicated unequal variances between the two groups.
Qualitative results
Thoughts and reflections
Responses of veterans in the elevation condition appeared to demonstrate more active engagement with the content of the videos as indicated by 77 coded responses in the thoughts and reflections category, compared to only 11 responses from the veterans in the amusement condition (see Table 4). Additionally, veterans in the elevation condition included positive attributions or reflections about others, whereas veterans in the amusement condition appeared to describe more passive and past-oriented thought processes as indicated by codes such as ruminating about their trauma and reminiscing about their own kids or family. Responses of those who watched the elevation videos most frequently reported thoughts and reflections about the virtue of selflessness. For example, one veteran wrote, It’s nice to recognize the selfless acts that normal people are capable of carrying out. Veterans in this condition also commonly made comments about the observed behavior being heroic. Additionally, these veterans commonly and exclusively to the elevation condition described thoughts about how there are good people in the world. One veteran wrote, This video let me know that there are still some good people in this world that care for other people. In contrast, relatively few veterans in the amusement condition remarked about any specific thoughts or reflections following the amusing videos. The few responses included reminiscing about past positive memories (e.g., family)—I remembered my kids growing up and playing—and ruminating about negative thoughts (i.e., trauma memories/reminders)—I couldn’t stop thinking about my trauma, negative thoughts of deployment, and shame.
Qualitative results: Coding counts and frequencies by experimental condition.

Note. The “[Unclear]” code was used when a participant recorded a statement that was clearly within a given category, but it was not clear how that statement fit with other codes.
Emotional and physical changes
Among those in the elevation condition, responses about emotional and physical changes in reaction to the video were positive. Most commonly, veterans reported feeling inspired and crying tears of joy. In contrast, responses in the amusement condition about emotional or physical changes suggested some of these veterans continued to be distracted by their trauma account, as these veterans reported negative emotions, such as sad, anger, shame, and feeling numb. Other responses about emotional or physical changes by veterans in this group indicated the manipulation effect worked as intended (e.g., laughter, funny, pleasant).
Motivations
Among those in the elevation condition, responses about motivations or the urge to act in a certain way were common. These responses were often about the desire to connect with others, to help others, or to engage in self-improvement. For example, I want to get closer to my boy and try to make a better life for him and I would like to help as many people as possible, in any way possible. Illustrative of one veterans desire to engage in self-improvement, she or he wrote: In the short term, I want to continue focusing on treatment and getting better. I want to focus on ridding myself of those toxic and incredibly negative feelings and emotions I have towards myself. I want to be able to think about the possibility of having children in the future and not be overcome with insurmountable fear.
Discussion
Consistent with our hypothesis, veterans reported higher elevation in response to videos of virtuous acts (i.e., elevation-inducing video clips) compared to videos that elicit amusement or general positive emotions. This is also consistent with findings from several studies that have similarly compared responses to elevation versus amusement stimuli in nonclinical, civilian populations (Algoe & Haidt, 2009; Erickson et al., 2017; Piper et al., 2015). However, prior to this study, it was unknown if this population had the ability to experience elevation given the significant shifts in cognitive schemas that often occur following a trauma, frequent experiences of strong negative emotions, and social impairment associated with PTSD. These results are important because they indicate veterans with PTSD have the capacity to be touched and moved by witnessing acts of exemplary moral value in spite of trauma-related distress and that such effects can be induced through targeted stimuli. Furthermore, it should be noted that veterans’ responses to elevation stimuli occurred in the context of recently completing a trauma narrative that was designed to elicit negative trauma-related thoughts and emotions. One might reasonably expect veterans to have significant difficulties experiencing a positive emotion following a trauma reminder, but that was not the case for many participants in the elevation condition. Therefore, the main results offer novel contributions by demonstrating (1) a general capacity to experience elevation in veterans with PTSD, (2) the potential to feel uplifted and inspired by the actions of others despite engaging in a trauma-reminder task that could present several cognitive and affective barriers to experiencing positive emotions, and (3) the ability to intentionally evoke elevation in veterans experiencing significant symptoms of PTSD.
Extending the quantitative findings that demonstrated a significant difference in self-reported elevation, distinct themes emerged in the journal responses across conditions to further support this difference. These divergent themes may highlight important differences in the experience of elevation versus amusement or general positive affect in this population.
Regarding the thoughts or reflections that were triggered by the video, veterans in the elevation condition reported positive attributions about the person featured in the video and demonstrated active reflections about the video content, whereas those in the amusement condition reported more passive reflections centered on reminiscing about events in the past including both positive (children/grandchildren) and negative topics (trauma). In the amusement condition, reminiscing about positive memories of children or grandchildren was likely elicited by the Charlie Bit My Finger video, which showcased an entertaining interaction between two young brothers. It should be noted that both entertaining videos were designed to avoid eliciting negative reactions and the content was unlikely to be related to most traumatic events. Therefore, incompatible responses to the amusement videos (e.g., ruminating about their trauma) could suggest veterans experienced difficulty letting go of trauma-related thoughts while trying to engage with generally positive stimuli. This phenomenon is common in people with PTSD and consistent with increased emotional reactivity, as well as intrusive, unwanted memories or thoughts about the traumatic event (American Psychiatric Association, 2013). In contrast, those in the elevation condition did not report difficulties with intrusive trauma-related thoughts and largely reported positive cognitive attributions about others’ behaviors.
The emotional and physical reactions suggest there was evidence across both conditions that the manipulation was effective in eliciting elevation and amusement, when intended. Notably, themes of negative emotional reactions were apparent in the amusement condition, but not the elevation condition. Similar to thoughts and reflections, some veterans who viewed amusement videos reported experiencing negative emotions that could be related to completing the trauma narrative (e.g., sadness, anger, shame), despite watching positive stimuli that typically elicit happiness, joy, and laughter. Veterans who viewed elevation videos, on the other hand, mostly reported a positive reaction such as feeling inspired and/or experiencing physical manifestations of positive emotions (i.e., tears of joy). These positive reactions are in direct opposition to the emotional sequela of PTSD, which include strong negative emotions and anhedonia or feeling numb to positive emotions.
Regarding motivations, a few veterans in the amusement condition reported a desire to reach out to their children or grandchildren, which was likely prompted by the video featuring the two young brothers; however, most did not report any motivations to act in a specified way. In contrast, the elevation condition elicited several motivations that could be described as approach-oriented motives or motives related to engaging in a specific activity to achieve a desired result. In this case, veterans reported a desire to connect with others and engage in prosocial behavior, consistent with the posited action tendencies of elevation. Additionally, a theme of self-improvement emerged such that this condition elicited desires to work on one’s own problems and strive to be a better person. The discrepancy between conditions could indicate that approach-oriented motives were more closely associated with the unique experience of elevation, rather than the experience of any positive emotion.
Potential Treatment Implications
Although this study did not test an intervention and it is limited in scope, the distinct elevation responses among veterans reporting significant PTSD symptoms could suggest ways in which inducing elevation might be useful in the context of treatment. In this final section, we propose hypothetical treatment implications that should be investigated in future research. First, given the positive attributions elicited by watching elevation videos, perhaps elevation could be used in conjunction with cognitive restructuring for strong negative beliefs about others or the world. Perhaps exposure to elevation stimuli (i.e., others’ virtuous acts) would provide veterans with an opportunity to recognize the good in others or in humanity as described by some in this study. This may aid the process of weighing the evidence for and against specific trauma-related beliefs.
Many veterans endorse limited positive affect or numbing of positive emotions (Armour et al., 2015; Kashdan et al., 2006). Perhaps it might be helpful to induce elevation in a veteran’s daily life if they report infrequent positive emotional experiences. If elevation is potent enough to move someone to tears, as experienced by some veterans in this study, maybe exposure to elevation stimuli could circumvent numbing tendencies. Intentionally eliciting elevation could take the form of occasionally watching videos similar to this experiment if someone’s daily routine does not create natural opportunities to be exposed to relevant, positive stimuli. Alternatively, treatment exercises could aim to help veterans increase their awareness of when virtuous acts occur in their daily life, resulting in increased opportunities to feel elevated.
A common theme among veteran responses following elevation videos was the description of approach-oriented motives. Although we did not test behavioral outcomes directly, if the reported motivations have the potential to translate to behavior change, maybe elevation could be used to target specific behaviors that would positively impact trauma recovery. For example, elevation might be used to facilitate increased social engagement and connectedness to others for veterans who are isolated. Maybe elevation could also be used as a motivational enhancement tool to help veterans engage in trauma treatment activities, some of which can be difficult to complete. For example, maybe a veteran would feel more motivated to engage in a challenging exposure exercise if they felt elevated by watching the remarkable courage of another veteran who completed their most difficult exposure task. Overall, these qualitative responses highlight promising areas for potential treatment integration; however, because this study focused on the internal validity of elevation responses in this population, additional work is needed to determine whether these ideas are feasible and effective when implemented outside a controlled laboratory setting.
Limitations and future directions
Findings should be considered in light of limitations. In this preliminary investigation, we used a small sample size that was primarily male; however, it should be noted we found large effect sizes in self-reported elevation, as well as clear divergence in qualitative themes that support these results. Future studies should aim to expand our understanding of this phenomenon with larger and more diverse samples. Given that there are no standardized measures for assessing state elevation to date, the elevation measure used for this study is limited and further psychometric analyses are needed. Without developing and testing a new measure, we aimed to address this limitation by utilizing a combination of two, previously used elevation measures that demonstrated adequate reliability in past studies (Erickson & Abelson, 2012; Landis et al., 2009) and are consistent with the established theoretical underpinnings of elevation. Additionally, we found high internal consistency for our elevation measure across repeated measurements. Another possible limitation is that we only solicited brief written responses from veterans, which may have limited the scope of qualitative information collected. Future studies would benefit from soliciting verbal responses that allow for the opportunity to probe for additional information, which would likely provide a greater depth and potential for insight into veterans’ experiences, particularly in response to elevation stimuli. Last, after a codebook was established—which was based on subthemes of qualitative responses that were identified through an inductive approach—the lead author was the primary rater for the final phase of coding responses. Future studies that aim to replicate these qualitative results should utilize multiple independent raters.
Future research should also strive to expand on findings from this study in several ways. First, given the heterogeneous responses to elevation videos, future studies should aim to identify predictors for strong and weak elevation responses. Highlighting these predictors may provide insight into who has the best chance to derive benefits from elevation when integrated into treatment. Separately, it will be important to understand the predictors of who experiences the psychosocial benefits of elevation in daily life (e.g., increased connectedness) that could contribute to trauma recovery. Additional work is also needed to understand the within-person effects of exposure to elevation stimuli and how that directly relates to benefits relevant to PTSD symptoms. For example, the secondary aim of this study is designed to address that gap in part by examining changes in trauma-related cognitions and emotions (e.g., shame, guilt) before and after exposure to elevation stimuli. Data collection for that aim is ongoing. Most importantly, if elevation is to be used as a therapeutic tool, then additional research will be required to determine whether exposure to elevation leads to observable mechanisms as hypothesized (e.g., increased social engagement) and whether those mechanisms mediate decreased PTSD symptoms and increased well-being.
Conclusion
Findings from this study suggest that veterans with significant PTSD symptoms are capable of experiencing elevation, that elevation can be induced in this population, and an elevation response is distinct from responses to general positive stimuli such as amusement. Veterans’ subjective responses to elevation also highlight areas for future research and suggest ways in which exposure to elevation may aid in trauma recovery. Future studies should continue to explore these potential mechanisms and expand our understanding of the clinical utility of this unique positive emotion.
Supplemental Material
Supplemental Material, sj-pdf-1-epp-10.1177_2043808720982415 - Inducing moral elevation in veterans with PTSD: An experimental investigation using a mixed methods approach
Supplemental Material, sj-pdf-1-epp-10.1177_2043808720982415 for Inducing moral elevation in veterans with PTSD: An experimental investigation using a mixed methods approach by Adam P. McGuire and Joseph Mignogna in Journal of Experimental Psychopathology
Footnotes
Authors’ note
This material is the result of work with resources and the use of facilities at the VISN 17 Center of Excellence for Research on Returning War Veterans and the Central Texas Veterans Health Care System. The views expressed herein are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States Government or its affiliates.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This material was supported in part by a Veterans Affairs Small Projects in Rehabilitation Research Award to Dr. McGuire (I21-RX003035-01A1).
Supplemental Material
Supplemental material for this article is available online.
Note
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.