
Abstract
Background:
Research suggests that microaggressions detrimentally impact the mental health of members of marginalized social groups.
Aims:
The aim of this systematic review was to assess the exposure to microaggressions and related implications on mental health of Lesbian, Gay, Bisexual, Transgender, Intersex, and Queer (LGBTIQ) people.
Method:
Medline, Scopus, PsycINFO, CINAHL, and EMBASE were searched until January 2023. Studies reporting data on the exposure to microaggressions toward LGBTIQ people were identified. Meta-analyses of rates of exposure to microaggression and of the association between microaggressions and mental health outcomes were based on odds ratio (OR) and standardized mean difference (SMD) with 95% confidence intervals (95% CI), estimated through inverse variance models with random effects.
Results:
The review process led to the selection of 17 studies, involving a total of 9036 LGBTIQ people, of which 6827 identifying as cisgenders, and 492 as heterosexuals, were included in the quantitative synthesis. Overall, LGBTIQ people showed an increased risk of microaggression (SMD: 0.89; 95% CI [0.28, 1.50]), with Transgender people having the highest risk (OR: 10.0; 95% CI [3.08, 32.4]). Microaggression resulted associated with risk of depression (SMD: 0.21; 95% CI [0.05, 0.37]), anxiety (SMD: 0.29; 95% CI [0.17, 0.40]), suicide attempts (OR: 1.13; 95% CI [1.08, 1.18]), alcohol abuse (OR: 1.32; 95% CI [1.13, 1.54]), but not to suicidal ideation (OR: 1.56; 95% CI [0.64, 3.81]) and cannabis abuse (OR: 1.44; 95% CI [0.82, 2.55]). The quality of the evidence was limited by the small number of studies.
Conclusions:
LGBTIQ people are at higher risk of microaggressions compared with their cisgender/heterosexual peers, which may lead to mental health consequences. This evidence may contribute to public awareness of LGBTIQ mental health needs and suggest supportive strategies as well as preventive interventions (e.g., supportive programs and destigmatizing efforts) as parts of tailored health-care planning aimed to reduce psychiatric morbidity in this population.
Introduction
Microaggression is a term used to describe subtle forms of discrimination to which marginalized social groups are subjected to, intentionally or unintentionally. Originally proposed by Pierce (1969) to describe insults and dismissals against African American people, microaggressions are currently conceptualized as every form of devaluation and humiliation toward members of marginalized social groups for their race, gender identity, sexual orientation, religion, economic status, disability, and other factors (Davis, 1989; Paludi & Denmark, 2010). Microaggressions can occur in different living contexts of a person such as the classroom (Winberg et al., 2019), the workplace (Davis & Mirick, 2022), the household (Gartner & Sterzing, 2018; Ryan et al., 2010), or they can take place at a more external level (e.g., state-level legal protections, religion, mass media) (Gartner & Sterzing, 2018; Nadal et al., 2016). Forms of microaggression can also occur in healthcare settings, and these have been linked to avoiding accessing healthcare as a response to anticipatory stigma (Mongelli et al., 2019).
Microaggressions have been classified in three primary forms: microassaults, microinsults, and microinvalidations (Nadal, 2013; Sue, 2010; Sue et al., 2007). Microassaults are overt verbal or nonverbal insults that the person who uses them is aware of, but ignores the detrimental effect on minority people; microinsults are attitudes that undermine the identity of marginalized people, frequently based on stereotypes, and often justified as ‘jokes’; and microinvalidations are statements that undervalue any experiential reality differing from the dominant one. The prefix micro- does not describe the quality or the impact of these aggressions, but rather the subtle way in which this type of discrimination occurs. An increasing number of studies identified a correlation between microaggressions and emotional, cognitive, and behavioral disturbances, such as chronic stress, depression, anxiety, and low self-esteem (Flentje et al., 2020; Marchi, Arcolin, et al., 2022; Mizock & Mueser, 2014; Nicholson et al., 2022).
Toward the lesbian, gay, bisexual, transgender, intersex, and queer (LGBTIQ) population, there are many ways in which microaggressions can occur (Nadal et al., 2012). Social environment plays a crucial role in mental health, and evidence, that microaggressive environments may lead to poorer mental health also among LGBTIQ people (Nadal et al., 2016), is mounting (Kattari, 2020; Nadal et al., 2012, 2014, 2015). In fact, a common feature of this kind of microaggression experience is the cumulative effect over time, which can erode one’s sense of identity, especially when there are other negative prognostic factors (Gartner & Sterzing, 2018), or in the case of a person belonging to multiple minority groups (e.g., ethnic, religious) (Nadal et al., 2014; Ryan et al., 2010), whereby sexual orientation and gender identity interact with other factors of vulnerability, within an intersectional understanding (Meyer et al., 2021) in the framework of the minority stress model (Meyer, 1995).
The aim of this study was to systematically review the available literature on microaggression, to provide a quantitative effect estimation of microaggression toward LGBTIQ people. Specifically, we aimed to estimate the risk to be exposed to microaggression for each LGBTIQ group, and to summarize the overall impact of microaggressions on the mental health outcomes reported in the literature.
Methods
This systematic review and meta-analysis was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Page et al., 2021). The protocol of this study was registered with PROSPERO (CRD42023399291).
Data sources and search strategy
We searched the PubMed (Medline), Scopus, PsycINFO, CINAHL, and EMBASE databases until January 31, 2023, using the strategy outlined in the Supplemental Table 1. No restrictions regarding language of publication or publication date were set.
Eligibility criteria
We included any observational or experimental study providing data on the exposure to microaggressions toward LGBTIQ people of any age, country, ethnicity, or setting of the enrollment.
We excluded reviews, qualitative studies, case-reports, case-series, and studies that did not report data for the measurements of the exposure in the targeted population. We only included studies published in peer-reviewed journals, excluding conference abstracts and dissertations. If data from the same sample were published in multiple works, we considered only that study reporting more exhaustive information. Sample overlap was ruled out through a careful check of the registration codes as well as the place and year(s) of sampling.
Terms and definitions
LGBTIQ status was defined as self-reported. Microaggressions referred to subtle forms of discrimination, often unconscious or unintentional, that communicate hostile or derogatory messages, particularly to and about members of historically marginalized social groups. Toward LGBTIQ groups, the three primary forms in which microaggressions may manifest are micro-assaults (which include overt verbal or nonverbal insults and behaviors), micro-insults (statements or actions that may slight or demean a person’s marginalized identity), and micro-invalidations (which exclude, negate, or nullify the psychological thoughts, feelings, or experiential reality of members of marginalized groups). We included studies where the exposure to microaggressions has been evaluated using validated questionnaires (Fisher et al., 2019), or through self-reporting on the three experiences listed above.
Data collection and extraction
Three authors (MM, FQ, and GL) preliminarily reviewed titles and abstracts of retrieved articles. The initial screening was followed by the analysis of full texts to check compliance with inclusion/exclusion criteria. All disagreements were explored until consensus was reached, and if consensus was not possible, another member of the team was consulted (GMG). A standardized form was used for data extraction. Information concerning the year of publication, country, setting, name of the study/cohort, characteristics of study participants (sample size, age, percentages of men and women), LGBTIQ status, microaggression exposure among the LGBTIQ groups and the controls were collected by two authors (MM and PG) independently. Where available, we also extracted data on mental health outcomes related to microaggression exposure. Preferentially, these should have been reported either as the frequency of people presenting that outcome or as the score on a validated scale for that mental health condition among microaggression exposed versus not exposed groups. To maximize the number of the included records, we considered also data derived from univariable regressions of mental health outcomes on microaggression exposure (i.e., odds ratio [OR] indicating the likelihood of mental health outcome between microaggression exposed and not exposed groups, and linear regression unstandardized beta coefficient [B] indicating the change in the psychometric score for microaggression experience). Extraction sheets for each study were cross-checked for consistency and any disagreement was resolved by discussion within the research group.
Statistical analyses
The meta-analysis was performed by comparing microaggression exposure rates between both controls versus overall LGBTIQ people and controls versus each LGBTIQ subgroup. Second, for each mental health outcome reported by at least two studies, a meta-analysis of the risk of that outcome by microaggression exposure was performed. Pooled ORs for dichotomous outcomes and standardized mean difference (SMD) for continuous outcomes, with respective 95% CIs, were generated using inverse variance models with random effects (DerSimonian & Laird, 1986). The results were summarized using forest plots. Standard Q tests and the I2 statistic (i.e., the percentage of variability in prevalence estimates attributable to heterogeneity rather than sampling error or chance, with values of I2 ⩾ 75% indicating high heterogeneity) were used to assess between-study heterogeneity (Higgins & Thompson, 2002). Leave-one-out analysis and meta-regression were performed to examine sources of between-study heterogeneity on a range of study prespecified characteristics (i.e., sex, age, country, year of publication, and assessment of microaggression applied – i.e., validated questionnaire, or self-reported).
If the meta-analysis included more than 10 studies (Sterne et al., 2011), funnel plot analysis and the Egger test were performed to test for publication bias. The Egger test quantifies bias captured in the funnel plot analysis using the value of effect sizes and their precision (i.e., the standard errors [SE]) and assumes that the quality of study conduct is independent of study size. If analyses showed a significant risk of publication bias, the ‘trim and fill’ method was employed to estimate the number of missing studies and the adjusted effect size (Duval & Tweedie, 2000; Sterne et al., 2008; Sutton et al., 2000; Terrin et al., 2003). All the analyses were performed in R (RStudio Team, 2021) using meta and metafor packages (Balduzzi et al., 2019; Viechtbauer, 2010). Statistical tests were two-sided and used a significance threshold of p value <.05.
Risk of bias assessment and the GRADE
Bias risk in the included studies was independently assessed by three reviewers (DU, EDM, and AT), using the Cochrane risk of bias tool (Higgins et al., 2011). All disagreements were discussed until consensus and, if necessary, another member of the team was consulted (GMG). Each item on the risk of bias assessment was scored as high, low, or unclear, and the GRADE tool was used to assess the overall certainty of evidence (Schünemann et al., 2013). Further information is available in the Supplemental Material.
Ethics approval
Ethics approval was not required for this systematic review because we collected and synthesized data from publications concerning previous studies in which ethical approval had already been obtained by the investigators in their respective local sites.
Results
Study characteristics
Figure 1 summarizes the selection process: from 157 records screened on title and abstract, 46 full texts were analyzed. The review process led to the selection of 17 studies (Austin et al., 2022; Bostwick et al., 2021; Carone et al., 2021; Davis & Mirick, 2022; Ehlke et al., 2022; Gartner & Sterzing, 2018; Gattis & Larson, 2017; Kalb et al., 2022; Mereish et al., 2022; Parr & Howe, 2019; Robinson & Rubin, 2016; Salim et al., 2019; Sarno & Wright, 2013; Sarno et al., 2020; Scharer & Taylor, 2018; Tsai et al., 2021; Winberg et al., 2019), referring to 17 different samples, corresponding to a total of 9036 LGBTIQ people, of which 6827 self-identifying as cisgenders, and 492 as heterosexuals, which were included in the quantitative synthesis.
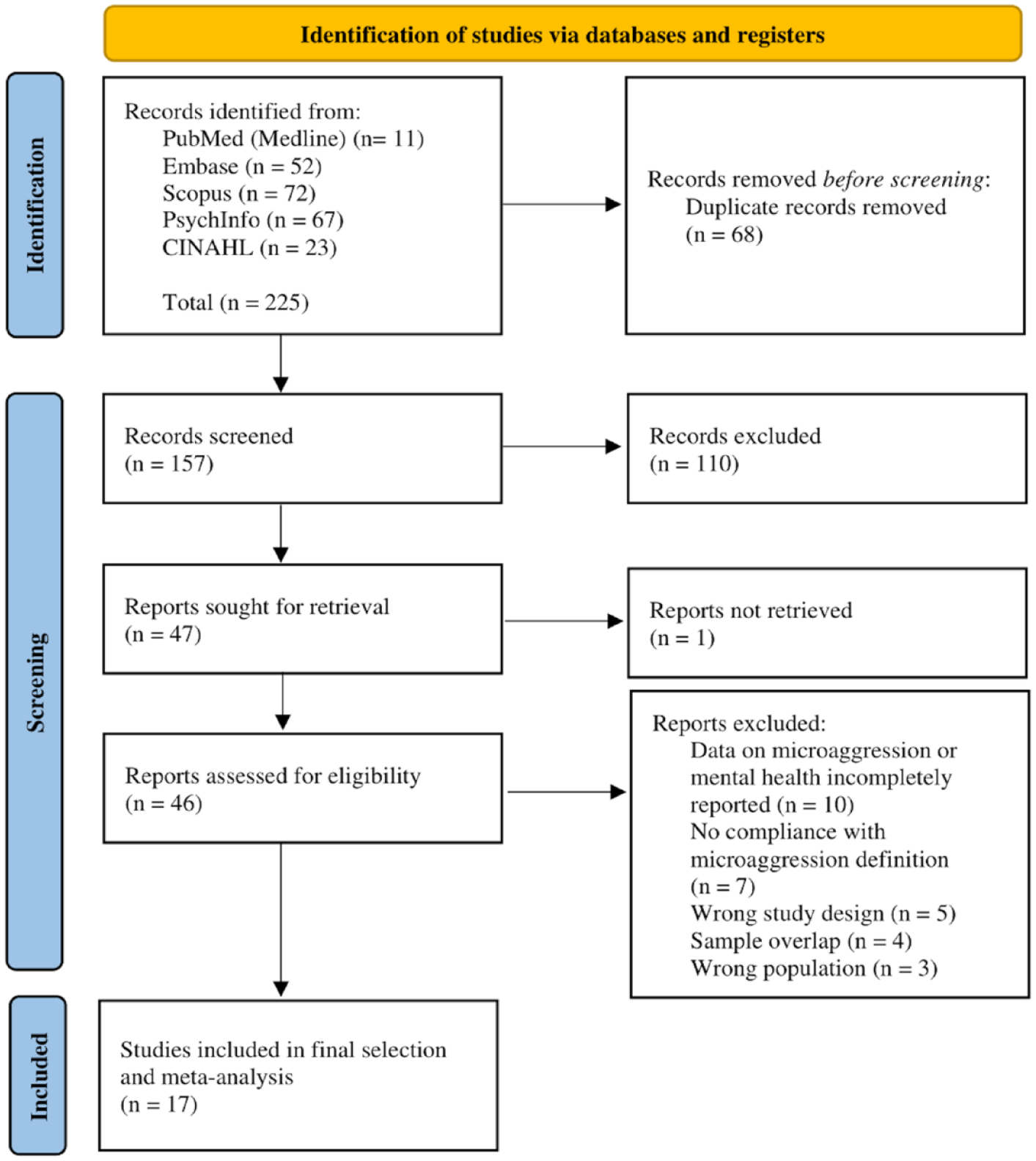
Preferred reporting items for systematic reviews and meta-analyses (PRISMA) flow diagram.
On average across the studies, the assigned sex at birth was female for 60.6% of participants (range: from 0% to 100%). The mean age of participants ranged from 14 to 65 years old (median age was 22.7). The selected studies were conducted in five countries: US (n = 11; 64.7%), Canada (n = 3; 17.7%), Puerto Rico, Taiwan, and Italy (n = 1 each; 5.9%). All the studies included were published in the last 10 years: 2022 (n = 5; 29.4%); 2021 and 2019 (n = 3 each; 17.7%); 2018 (n = 2; 11.8%); and 2020, 2017, 2016, and 2013 (n = 1 each; 5.9%). Overall, data collection covered the from October 2012 to July 2020, and it was not reported in seven studies (41.1%). Microaggression was measured through self-reporting (n = 4; 23.5%), or using the following validated scales: the Homonegative Microaggression Scale (HMS, n = 4; 23.5%), the LGBT People of Color Microaggression Scale (LGBT-PCMS, n = 3; 17.7%), the LGBT Microaggression Scale (LGBT-MCS, n = 2; 11.8%), the Sexual Orientation Microaggressions Inventory (SOMI, n = 2; 11.8%), the Racial and Ethnic Microaggressions Scale (REMS, n = 1; 5.9%), and the Bisexual Microaggression Scale for Women (BMSW, n = 1; 5.9%). The mental health outcomes reported were suicidal attempts (n = 2; 11.8%), suicidal ideation (n = 2; 11.8%), suicidality as attempt or ideation (n = 2; 11.8%), depression (n = 6; 35.3%), anxiety (n = 2; 11.8%), alcohol abuse (n = 6; 35.3%), and cannabis abuse (n = 2; 11.8%). Five studies (29.4%) did not investigate mental health outcomes but provided comparison of the microaggression exposure rate among LGBTIQ and controls (i.e., heterosexuals or cisgenders) or among LGBTIQ subgroups.
All studies characteristics are summarized in Table 1.
Characteristics of the included studies.
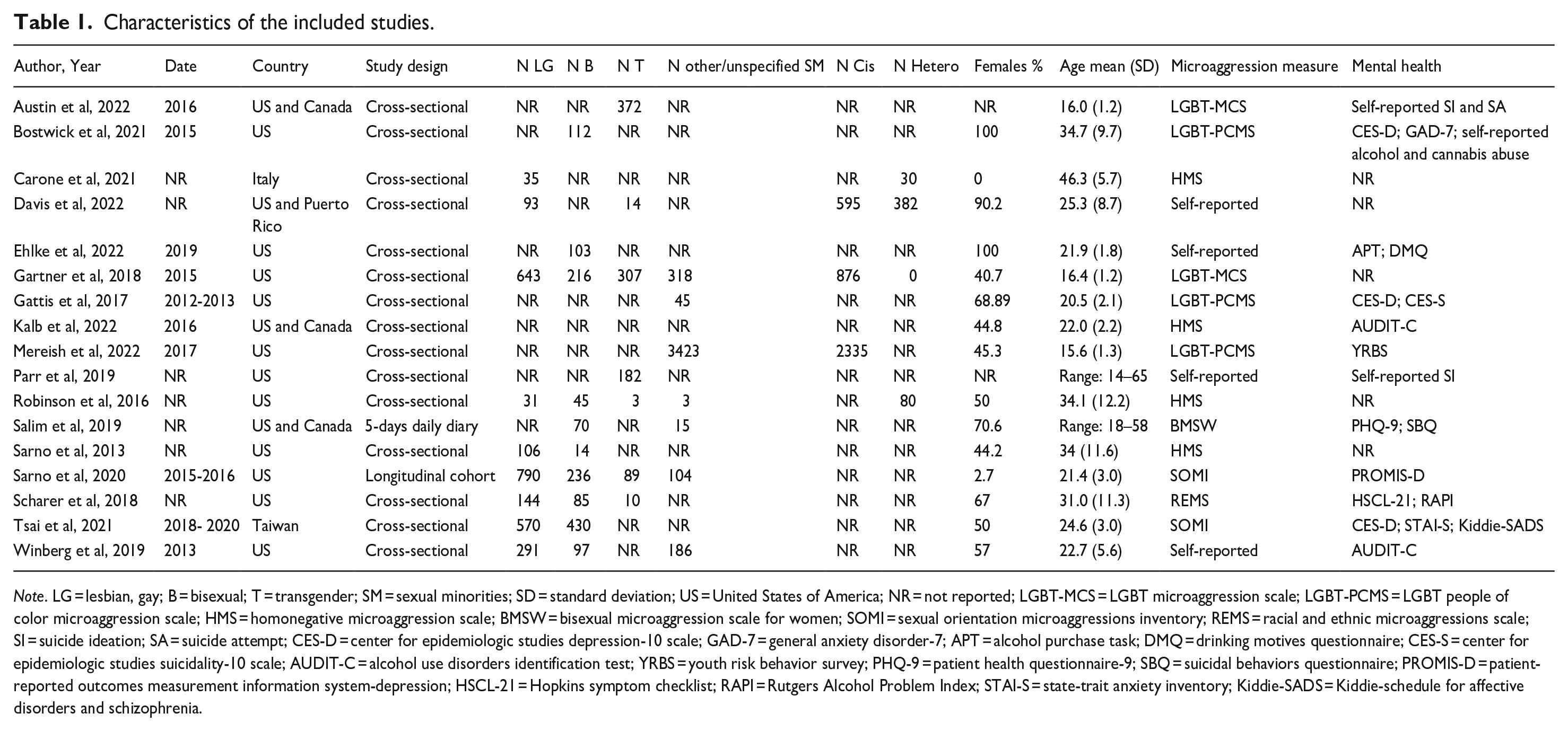
Note. LG = lesbian, gay; B = bisexual; T = transgender; SM = sexual minorities; SD = standard deviation; US = United States of America; NR = not reported; LGBT-MCS = LGBT microaggression scale; LGBT-PCMS = LGBT people of color microaggression scale; HMS = homonegative microaggression scale; BMSW = bisexual microaggression scale for women; SOMI = sexual orientation microaggressions inventory; REMS = racial and ethnic microaggressions scale; SI = suicide ideation; SA = suicide attempt; CES-D = center for epidemiologic studies depression-10 scale; GAD-7 = general anxiety disorder-7; APT = alcohol purchase task; DMQ = drinking motives questionnaire; CES-S = center for epidemiologic studies suicidality-10 scale; AUDIT-C = alcohol use disorders identification test; YRBS = youth risk behavior survey; PHQ-9 = patient health questionnaire-9; SBQ = suicidal behaviors questionnaire; PROMIS-D = patient-reported outcomes measurement information system-depression; HSCL-21 = Hopkins symptom checklist; RAPI = Rutgers Alcohol Problem Index; STAI-S = state-trait anxiety inventory; Kiddie-SADS = Kiddie-schedule for affective disorders and schizophrenia.
Analysis of microaggression rate among LGBTIQ and controls
Five studies (81.5%) reported data about exposure to microaggression among LGBTIQ and controls. Four studies measured exposure to microaggression using validated scales: three provided comparison between LGBTIQ and cisgender/heterosexual controls, and two between LG and B. As shown in Figure 2, the level of exposure to microaggression resulted higher for LGBTIQ than controls (SMD: 0.89; 95% CI [0.28, 1.50]), with high heterogeneity (I2 = 92%; p < .001). Interestingly, the study comparing T and cisgender (Gartner & Sterzing, 2018) showed the largest effect size, suggesting that gender minorities may be the group experiencing the highest level of microaggression. This study might be also the main source of heterogeneity of the effect size estimation.
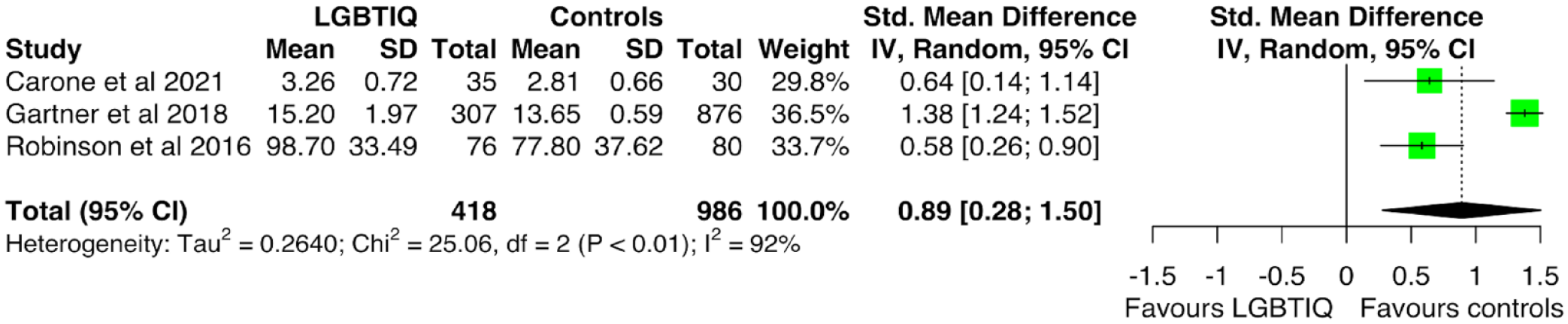
Forest plot of microaggression exposure for LGTIQ people compared with controls (heterosexual or cisgender).
Instead, the meta-analysis of the level of exposure to microaggression between LG and B found no significant difference between the two groups (SMD: 0.16; 95% CI [−2.08, 2.40]). The results are displayed in Figure 3.

Forest plot of microaggression exposure for LG compared with B.
One study (5.9%) reported microaggression exposure as percentage of people self-reporting experience of microaggression from the LGB, T, cisgender, and heterosexual groups. The comparison of microaggression risk of sexual minority group yielded significantly higher level for SM compared to heterosexuals (OR = 2.08; 95% CI [1.27, 3.40]) and for T compared to cisgender (OR = 10.0; 95% CI [3.08, 32.4]), confirming the previous results of a higher risk of enduring microaggression for gender non-conformity individuals.
Analysis of depression by level of exposure to microaggression
Six (35.3%) studies provided data on the depression level among LGBTIQ people by exposure to microaggression. Interestingly, all the studies assessed microaggression exposure using validated questionnaires. Meta-analyses indicated that individuals exposed to microaggression reported also increased levels of depression (SMD: 0.21; 95% CI [0.05, 0.37]), with evidence of moderate between-study heterogeneity (I2 = 72%; p = .01). The results are displayed in Figure 4.
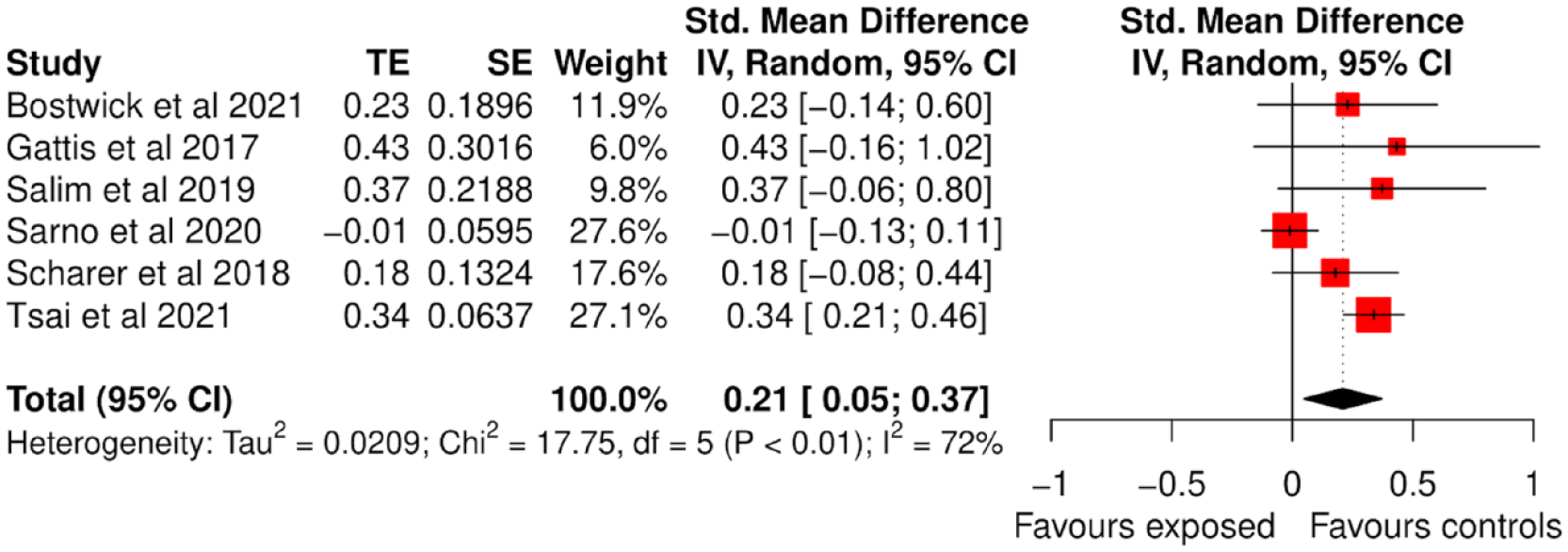
Forest plot of depression level by level of exposure to microaggression.
Interestingly, all the studies had confidence intervals crossing the line of no-effect, suggesting null effect from a frequentist framework. Leave-one out analysis, in which the meta-analysis of depression by microaggression exposure was serially repeated after the exclusion of each study, showed that two studies were potentially playing an outlier effect. In particular, by omitting the study from Sarno et al. (2020), there was a significant decrease in the amount of heterogeneity (i.e., the I2 = 0%) and increase in the effect size estimate (SMD: 0.31; 95% CI [0.21, 0.41]), whereas, by excluding the study from Tsai et al. (2021) the effect size resulted no longer statistically significant (SMD: 0.15; 95% CI [−0.02, 0.33]; I2 = 38.7%). Irrelevant changes in the pooled estimate were obtained by excluding each of the other studies (leave-one-out data available in Supplemental Table 2).
Analysis of anxiety by level of exposure to microaggression
Two studies (11.8%) provided data on anxiety level among LGBTIQ people by exposure to microaggression. Meta-analysis showed that individuals with higher levels of exposure to microaggression also reported higher levels of anxiety (SMD: 0.29; 95% CI [0.17, 0.40]). Although the estimate was based only on two studies, there were no evidence of significant between-study heterogeneity (I2 = 0%; p = .840). The results are displayed in Figure 5.
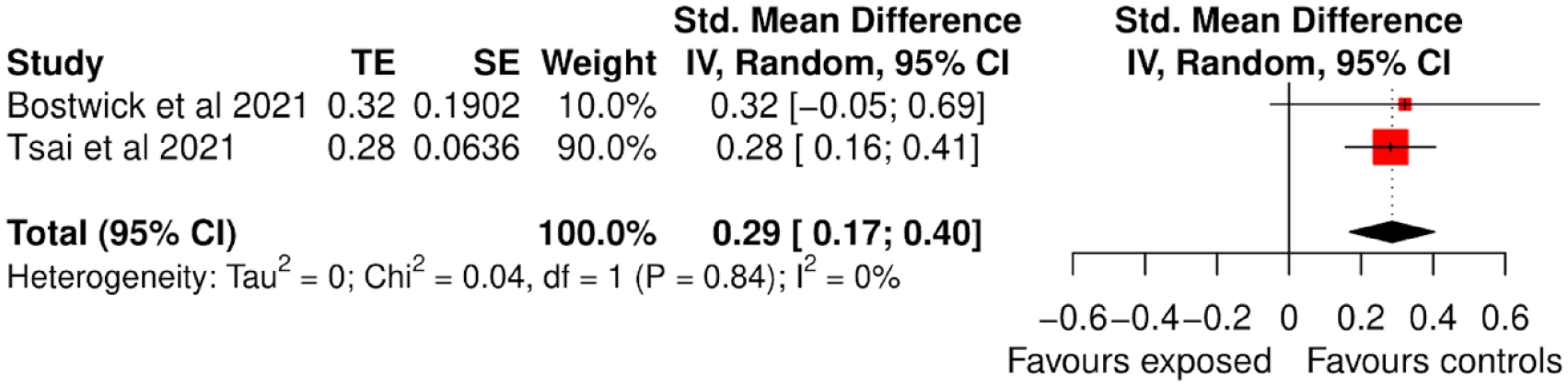
Forest plot of anxiety level by level of exposure to microaggression.
Analysis of suicidality by level of exposure to microaggression
Five studies (29.4%) reported data on suicidality among LGBTIQ people in relation to exposure to microaggression. Specifically, three reported data on suicide attempts and suicide ideation, and two provided a general assessment of suicidality. Although the meta-analyses were based on a small number of studies, there is an indication that LGBTIQ people exposed to microaggression were at increased risk of suicide attempt (OR: 1.13; 95% CI [1.08, 1.18]) and displayed higher suicidality levels (SMD: 0.22; 95% CI [0.10, 0.34]), however this was not confirmed for suicidal ideation (OR: 1.56; 95% CI [0.64, 3.81]). The results are shown in Figure 6.
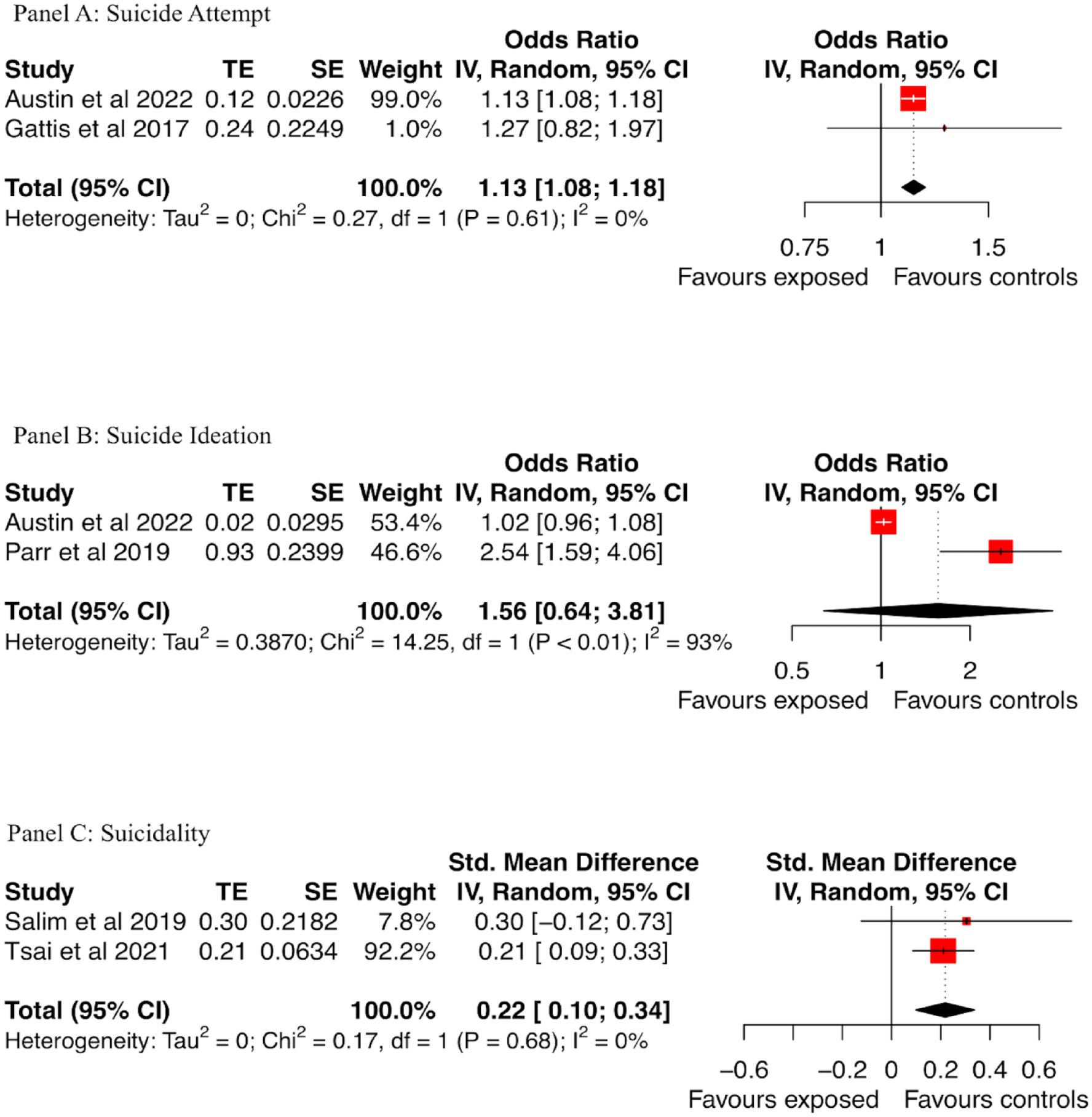
Forest plot of suicide attempt risk (Panel A), suicide ideation risk (Panel B), and suicidality level (Panel C) by exposure to microaggression.
Analysis of alcohol abuse by level of exposure to microaggression
Six studies (25.9%) provided data on alcohol abuse among LGBTIQ people by microaggression exposure level. Specifically, four of these reported OR as measure of association, whereas two as unstandardized univariable linear regression B. Therefore, two distinct meta-analysis were performed. Figure 7 presents the ORs meta-analysis showing an increased likelihood of alcohol abuse among LGBTIQ people when exposed to microaggression (OR: 1.32; 95% CI [1.13, 1.54]), with not significant between-study heterogeneity (I2 = 50%; p = .11). The association between microaggression exposure and alcohol abuse was not replicated in the meta-analysis of Betas (SMD: 0.14; 95% CI [−0.04, 0.32]), although the estimate was based only on two studies (see Supplemental Figure 1).
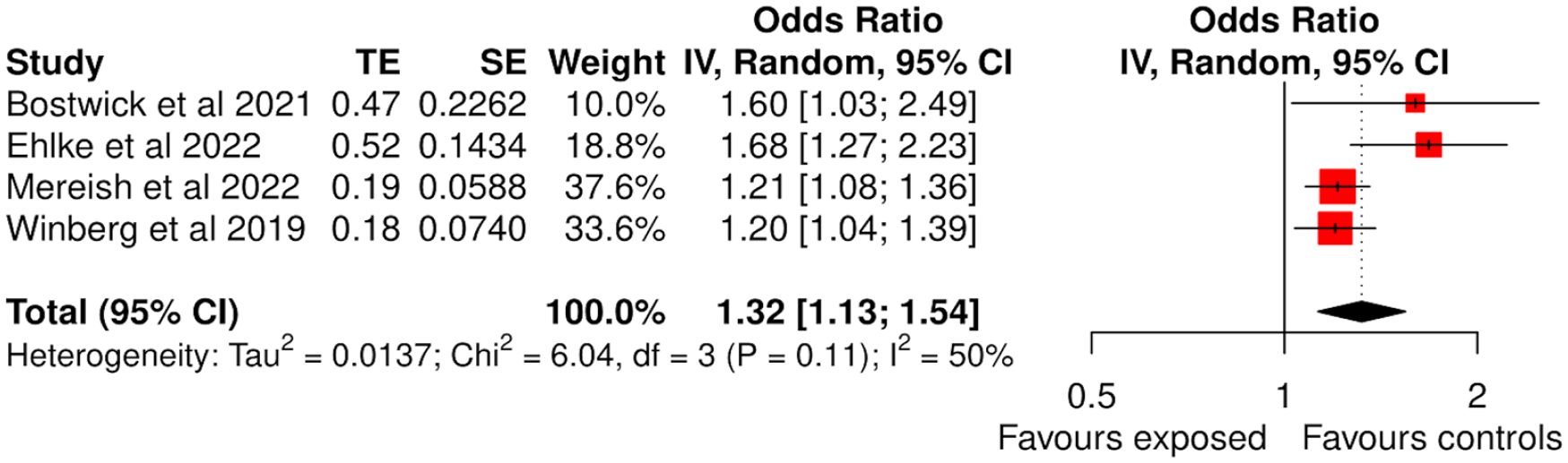
Forest plot of the risk of alcohol abuse by level of exposure to microaggression.
Analysis of cannabis abuse by level of exposure to microaggression
Two studies (11.8%) reported data on cannabis use and microaggression exposure among LGBTIQ people. Meta-analysis provided evidence supporting not significant association (OR: 1.44; 95% CI [0.82, 2.55]), with significant evidence of between-study heterogeneity (I2 = 81%). The results are displayed in Figure 8.
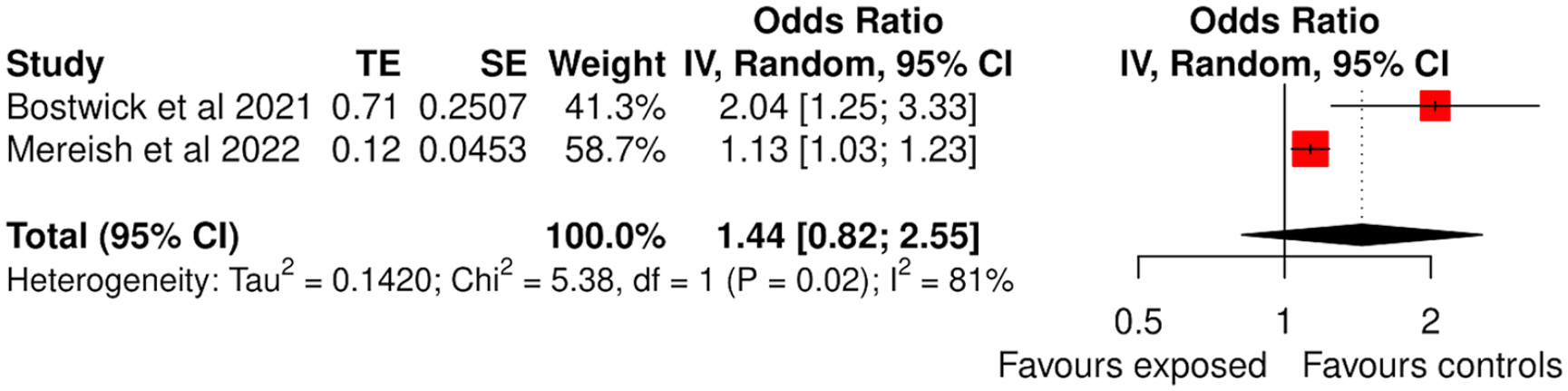
Forest plot of the risk of cannabis abuse by level of exposure to microaggression.
Publication bias and meta-regression
Publication bias evaluation is generally deemed meaningful when at least 10 studies are included in the meta-analysis (Sterne et al., 2011), yet none of our estimates were based on that number of studies. To get an impression of possible bias in publication and to inform future research, we decided to run it anyway on the estimate comprising the largest number of studies, that was the meta-analysis of the association between microaggression and depression (n = 6). As can be seen in the funnel plot presented in Supplemental Figure 2, and from Egger’s test results (p = .348), there was no evidence of publication bias.
Meta-regression analyses were performed only for the meta-analyses of the association between microaggression and depression and microaggression and alcohol abuse risk, because the number of studies in the other analyses was too low. The following variables, potentially associated with heterogeneity, have been investigated: (1) the percentage of females in the total sample; (2) the mean age of participants; (3) the country where the study was conducted; (4) year of publication; and (5) assessment of microaggression applied (i.e., validated questionnaire vs. self-reported, and intersectional vs. non-intersectional). In the univariable meta-regression model, the variable that resulted significantly correlated with the variance in the level of depression was the Taiwan country (B: 0.337; 95% CI [0.094, 0.580]), whereas the variance in the risk of alcohol abuse resulted significantly associated with the percentage of females (B: 0.006; 95% CI [0.001, 0.011]). Interestingly, no significant effect played by intersectional versus non intersectional microaggression was found both on depression and alcohol estimates (B: 0.030; 95% CI [−0.22, 0.28], and B: −0.034; 95% CI [0.33, 0.26], respectively). Univariable meta-regression results are displayed in Supplemental Table 3.
GRADE of the evidence
A summary on the risk of bias in all 17 trials has been reported in Supplemental Figures 3 and 4, along with an assessment of the quality of the evidence (Supplemental Table 4). In the GRADE system, the evidence from observational studies is initially set to low, there are then criteria that can be used either to downgrade or upgrade (see further information in the Supplemental Material). The quality of the evidence was rated very low for all the estimates, mainly due to the small number of studies included and the risk of bias linked to the sample selection.
Discussion
To our best knowledge, this is the first meta-analysis aimed at investigating the impact of microaggressions on the mental health of LGBTIQ people. Our findings confirm that microaggressions affect LGBTIQ individuals, particularly transgender ones. We also provided a quantitative estimate of the negative impact that microaggression can have on mental health, highlighting the increased risk of depression, anxiety, suicide attempts, and alcohol abuse. The findings on depression and alcohol abuse were particularly relevant, as they were based on a larger number of studies. Previous research has shown that microaggression is associated with low self-esteem, depressive symptoms, and alcohol abuse, which is sometimes used as a coping mechanism (Mereish et al., 2022; Salim et al., 2019; Scharer & Taylor, 2018). Studies have also investigated the additive effects of intersectional factors, such as the minority stress experienced by LGBTIQ individuals who belong to minority ethnic groups (Mereish et al., 2022; Vaccaro & Koob, 2019). However, based on the assessment used to target microaggression or intersectional microaggression, our meta-regression analysis did not find significant differences in depression risk and alcohol abuse. This findings may be due to the small number of studies included in our review. It is important to mention here the atypical nature of some of the studies in terms of sex ratio especially as rates of women are higher and lesbians may face more micro-aggression than others. Indeed, we found an increased risk of alcohol abuse and microaggression level, depending on the number of females in the sample, which can be viewed as consistent with intersectionality theory, in most countries the dominant gender is male. We also found an association between microaggression and suicide attempts, which is consistent with the estimate reported in this review on the risk of depression, and in line with previous evidence on increased risk of suicidality among LGBTIQ people (Marchi, Arcolin, et al., 2022; Parr & Howe, 2019). According to the interpersonal theory of suicide, the simultaneous presence of thwarted belongingness and perceived burdensomeness can prompt the desire for suicide. Therefore, family and peer support may be highly important in reducing the risk of suicidality among LGBTIQ people (Craig & Smith, 2014; Menvielle & Rodnan, 2011). The experience of microaggression was also associated with anxiety, consistently with previous evidence showing the negative psychological effects of discrimination on marginalized ethnic groups (Marchi, Magarini, et al., 2022). Research has found that individuals who conceal a stigmatized social identity are more likely to focus on keeping that identity hidden during their social interactions, which may lead to social phobia (Gattis & Larson, 2017). LGBTIQ individuals may feel threatened in general social interactions, as their sexual orientation may be challenged or questioned (Pachankis et al., 2020). Interventions that focus on personal skills to cope with negative interpersonal encounters may help creating an affirmative interpersonal world, promoting self-compassion. Longitudinal studies are needed to investigate patterns of transition from psychopathological symptoms to clinical diagnoses, and research on protective factors may have implications for policy makers. Qualitative studies are also needed to better understand the experiential component of microaggression. Educational and intervention programs grounded in equity and compassion should be implemented in schools and workplaces to address these issues.
Limitations
First, mental health outcomes assessed varied across the included studies, which translated into many meta-analyses (i.e., one for each mental health outcome), each including a small number of studies, with a reduction of statistical power in the analysis. Second, most of the studies reported the association between microaggression and mental health using measures of association rather than frequencies or mean scores. Increasingly, there are available tools to perform meta-analysis using pre-calculated effect sizes (Harrer et al., 2021), however, it is required that these are from univariable regression models, and that was not always easy to verify. The inclusion of these data is both a strength and a limitation of this review, as it allowed us to maximize the number of included studies, though the data collected may be of lower quality. Third, although our results suggest a strong relationship between microaggressions and mental health outcomes, the cross-sectional nature of the studies included in this meta-analysis did not allow us to clarify causality. There may be alternative mechanisms at play, such as reverse causality, whereby a depressive state could influence perceptions of aggression, or residual confounding, as the exposure to microaggressions could be also associated with exposure to major traumas. Therefore, caution should be exercised when interpreting the causal relationship between microaggressions and mental health outcomes based on our findings. Fourth, most of the studies reported information on either sexual orientation or gender identity, hindering to detail the risk across the LGBTIQ groups. More thorough reporting of information about sex assigned at birth, sexual orientation, and gender identity should be considered in future research, also in light of our findings in the meta-regression analyses that alcohol abuse was significantly associated with the percentage of persons with female sex assigned at birth. Finally, the number of studies included in the meta-analyses was <10, which is a questionable number for a reliable assessment of the presence of a publication bias (Sterne et al., 2011).
Conclusions
LGBTIQ people are likely exposed to microaggression, which may lead to mental health consequences. This evidence may contribute to public awareness on LGBTIQ mental health needs and suggest supportive strategies as well as preventive interventions (e.g., supportive programs and destigmatizing efforts) as parts of tailored health-care planning aimed to reduce psychiatric morbidity in this vulnerable population.
Supplemental Material
sj-docx-1-isp-10.1177_00207640231194478 – Supplemental material for Microaggression toward LGBTIQ people and implications for mental health: A systematic review
Supplemental material, sj-docx-1-isp-10.1177_00207640231194478 for Microaggression toward LGBTIQ people and implications for mental health: A systematic review by Mattia Marchi, Antonio Travascio, Daniele Uberti, Edoardo De Micheli, Fabio Quartaroli, Giuseppe Laquatra, Pietro Grenzi, Luca Pingani, Silvia Ferrari, Andrea Fiorillo, Manlio Converti, Federica Pinna, Francesco Amaddeo, Antonio Ventriglio, Massimo Mirandola and Gian M Galeazzi in International Journal of Social Psychiatry
Footnotes
Availability of data and materials
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.