
Abstract
BACKGROUND:
Each year about one in five adults experiences mental illness. Although the independent physical and mental health consequences of alcohol misuse and cigarette smoking are well documented, little is known on how substance use moderates the relationship between physical and mental well-being.
AIM:
The purpose of this study was to examine whether substance use moderates the relationship between physical activity and mental health in adults.
METHODS:
This was a secondary analysis of data provided by the Behavioral Risk Factor Surveillance System (BRFSS).
RESULTS:
Participants (N = 450,016) were adults who completed the BRFSS in 2017. Those who did not drink alcohol had fewer mental health problems when they indicated greater amounts of time spent doing physical activities each week. Last, smokers’ number of mental health problems decreased as they engaged in more physical activity, whereas nonsmokers’ number of mental health problems increased as they engaged in more physical activity.
CONCLUSIONS:
The relationship between physical activity and mental health outcomes is well established and cannot be overemphasized. Nonetheless, substance abuse can moderate this relationship and should be routinely screened for by health care providers regardless of treatment setting.
Introduction
According to the Substance Abuse and Mental Health Services Administration (SAMHSA, 2018a) approximately 14.4 million adults aged 18 years and older have alcohol use disorder (AUD). The Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013) defines AUD as the presence of at least two of the 11 identified symptoms and is categorized based on severity as mild (presence of two to three symptoms), moderate (presence of four to five symptoms), or severe (six or more symptoms). Interestingly, among adults aged 18 years and older, 86% of this population in the United States report that they have been intoxicated at some point in their lifetime, 70% within the past year, and about 55% within the past month (SAMHSA, 2018b). More important, more than one in every four adults reports at least one episode of binge drinking, while slightly more than 6% report a heavy drinking episode in the past month (SAMHSA, 2018b).
Unfortunately, the negative effects of AUD cannot be overemphasized. For example, about 95,000 people die because of excessive alcohol use, which costs society approximately $249 billion annually (Centers for Disease Control and Prevention [CDC], 2020). The CDC (2018) defines excessive alcohol use as binge drinking, heavy drinking, or any type of drinking by individuals who are younger than 21 years or women who are pregnant. Thus, excessive alcohol use is the third leading cause of preventable death in the United States (National Institute on Alcohol abuse and Alcoholism, 2020). In fact, in 2014 alone, one in three motor vehicle fatalities were attributed to drunk driving (National Center for Statistics and Analysis, 2016). More important, it is estimated that more than 10% of children in the United States live in homes where a parent has alcohol problems (Lipari & Van Horn, 2017), which contributes to family instability, child abuse and neglect, and even other psychological problems such as depression, anxiety, and low self-esteem (Ewing et al., 2015; Solis et al., 2012). Of note, approximately 36% of children who entered the foster care system in 2018 did so due to parental drug abuse (Children’s Bureau, 2019).
In addition to AUD and excessive alcohol use, approximately 34.2 million adults in the United States smoke cigarettes, with the highest prevalence among those aged between 25 and 44 years (CDC, 2019. While the prevalence of cigarette smoking has declined over the past decade, cigarette smoking remains the leading cause of preventable deaths in the United States, accounting for almost 500,000 deaths per year (CDC, 2019). Although the independent physical and mental health consequences of alcohol misuse and cigarette smoking are well documented, little is known on how these substances moderate the relationship between physical and mental well-being. Therefore, the purpose of this study was to examine whether smoking or drinking alcohol moderated the relationship between physical activity and mental health in adults.
Background and Significance
Examining these relationships is important because each year about one in five adults experiences mental illness (National Alliance on Mental Illness [NAMI], n.d.-b). Specifically, approximately 16 million adults have major depression, and approximately 42 million adults have anxiety disorders (NAMI, n.d.-b). Additionally, adults with serious mental illness tend to die about 25 years earlier than others, primarily due to medical conditions that can be treated (NAMI, n.d.-b). Adults with mental illnesses are also more likely to smoke compared with their peers without mental illnesses (Ruggles et al., 2017) and more likely to engage in alcohol abuse (Dierker et al., 2018). For example, in 2018, approximately 21% of adults with a substance use disorder also reported major depressive disorder (NAMI, n.d.-a) and substance abuse, including alcohol consumption and cigarette smoking, and are frequently cited as contributing factors to mental health problems and well-being issues (Dierker et al., 2018; Kedzior & Laeber, 2014; Ruggles et al., 2017).
In the United States, adults who engage in regular physical activity are less likely to experience depressive symptoms and anxiety disorders (Goodwin, 2003). This relationship between physical activity, mental health, and well-being is adequately documented. In fact, in a review of 37 meta-analyses examining the effects of exercise on depression and anxiety, Wegner et al. (2014) found that exercise improved both anxiety and depressive symptoms, especially among patients within clinical settings. This relationship holds true even among individuals with serious psychiatric disorders, such as schizophrenia, with additional benefits of improvements in cognitive and brain functioning (Rimes et al., 2015). Additionally, both type and intensity of physical activity predicts depression, specifically the odds of having lower depressive scores increase with each additional hour of vigorous recreation-related physical activity, although some racial differences influence this relationship (Mumba et al., 2020). Last, the physical benefits of exercise among people with mood disorders are also documented (Mikkelsen et al., 2017).
Nonetheless, studies that have examined the relationship between substance abuse and physical activity have yielded mixed results. For example, in a study by Vidot et al. (2017) that examined the physical activity patterns among marijuana users (N = 12,618), the researchers found that the prevalence of physical activity is lower among marijuana users and that marijuana users have lower odds of moderate physical activity than those individuals who have never used marijuana. Additionally, as frequency of marijuana use increased, time spent on physical activity decreased. On the contrary, in a study that examined the relationship between physical activity and alcohol use, linear regression models did not show a significant interaction between physical activity and alcohol consumption (Kopp et al., 2015). These findings were also supported by Rawson et al. (2015) who found that although fewer participants in an exercise program returned to marijuana use after completion of the exercise program compared with those who only engaged in an education program about marijuana, this difference was not statistically significant.
Exercise and physical activity have further been utilized in smoking cessation intervention programs. For example, De Jesus and Prapavessis (2018) found that exercise decreased various outcome variables of a smoking cessation program. These included reductions in cigarette consumption, reductions in puff duration, reductions in smoking satisfaction, reductions in the psychological reward from smoking, reductions in nicotine cravings, and reductions in enjoyment of respiratory tract sensations from smoking. In another study that examined the relationship of exercise with smoking-related symptomology, Tosun et al. (2018) found that women exercised less compared with men and, thus, had more symptoms of negative affect, craving, and physical symptoms of withdrawal. Additionally, women on average smoked more cigarettes per day and exhibited more symptoms of nicotine dependency. Regardless of gender, exercise was positively associated with positive affect (Tosun et al., 2018).
Methods
Design and Dataset
This was a secondary analysis of data provided by the Behavioral Risk Factor Surveillance System (CDC, 2021). The BRFSS is administered and funded by the Population Health Surveillance Branch of the CDC, which is in the Division of Population Health at the National Center for Chronic Disease Prevention and Health Promotion. The BRFSS is a telephone survey created to collect health-related data from adults (≥18 years of age) in all 50 states, the District of Columbia, Guam, Puerto Rico, and the U.S. Virgin Islands. The median response rates for all states and territories in 2017, calculated using guidelines established by the American Association for Public Opinion Research, were 45.3% for calls directed to landlines and 44.5% for calls directed to cell phones. Since this is a secondary data analysis of a publicly available and de-identified data set, no institutional review board approval was required to conduct the research. The CDC approves all data collection and management procedures for BRFFS. Data are collected via telephone interviews, and interviewers request verbal informed consent from all participants prior to beginning the data collection procedures.
Measures
As a part of the larger study, participants completed an interview over the phone, which contained items addressing general demographics and health. The questionnaire took an average of 18 minutes to complete. Individual states were permitted to add their own questions to the interview, which typically added 5 to 10 minutes to the total interview time. Measures of interest for the present study included level of education, physical activity, alcohol consumption, smoking, and mental health problems. Level of education was coded on a 6-point Likert-type scale, with 1 = never attended school or only kindergarten,” 3 = grades 9 through 11 (some high school), and 6 = college 4 years or more (college graduate). Physical activity was measured by the total number of minutes of physical activity per week. Alcohol consumption was coded as a binary variable, with 0 = nondrinkers and 1 = drinkers. The smoking item asked participants the following: “Have you smoked at least 100 cigarettes in your entire life? (Note: 5 packs = 100 cigarettes).” If participants answered “yes,” this item was coded as 1; if participants answered “no,” this item was coded as 2. The mental health problems item of interest asked participants the following: “Now thinking about your mental health, which includes stress, depression, and problems with emotions, for how many days during the past 30 days was your mental health not good?” Thus, the mental health problems variable had a possible range of 0 to 30 days.
Results
Participants
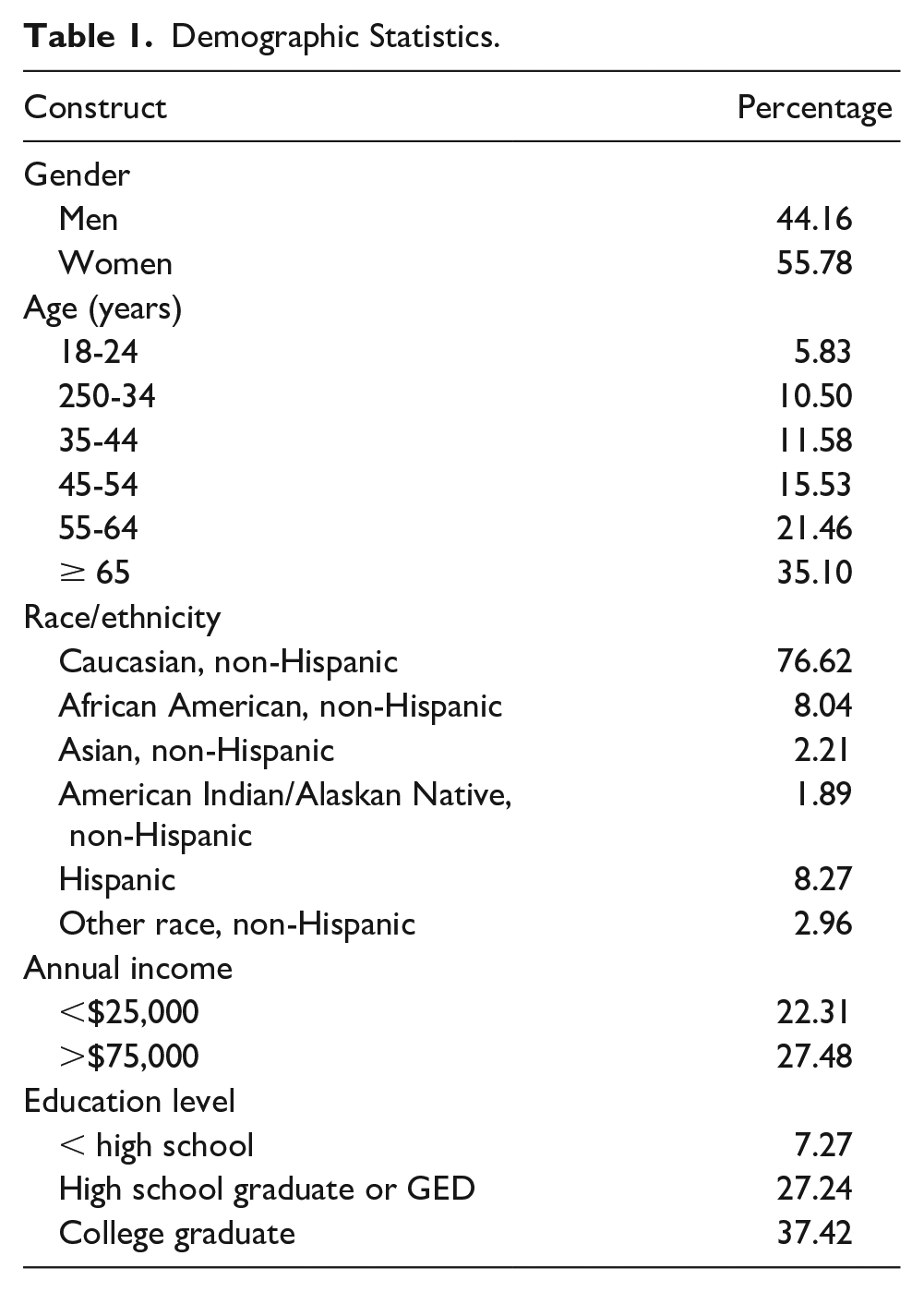
Participants (N = 450,016) who completed the BRFSS in 2017 were adults. The 2017 data set was utilized as it was the latest available data set at the time of the data analysis. Table 1 presents demographic characteristics of the total sample, including gender, age, race/ethnicity, annual income, and education level. Approximately 10% of the sample reported smoking every day, and 4.19% reported smoking on some days; 54.69% did not smoke at all. A total of 49.14% of participants reported drinking alcoholic beverages in the past 30 days. A total of 26.78% of the sample did not engage in any physical activity per week, whereas 29.42% were highly active (i.e., engaged in at least 300 minutes of aerobic exercise per week). Approximately 16% reported engaging in 150 to 300 minutes of physical activity per week, and 16.30% reported engaging in 11 to 149 minutes of physical activity per week. Last, about one in three participants reported experiencing poor mental health in the past 30 days, including stress, depression, and problems with emotions. See Table 1 for a breakdown of all demographic characteristics for the sample.
Demographic Statistics.
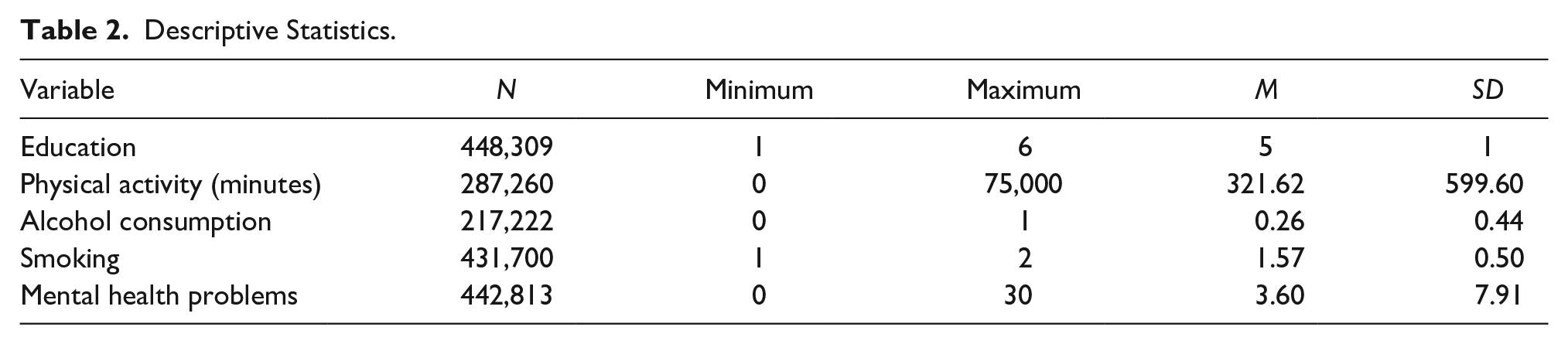
Descriptive statistics, including range, mean, and standard deviation, for each variable of interest are displayed in Table 2. Table 3 includes correlations between variables of interest, including education level, amount of physical activity per week (in minutes), alcohol consumption, smoking, and mental health problems. Mental health problems were analyzed based on the number of days in the month participants reported having mental health problems.
Descriptive Statistics.
Correlations Between Variables of Interest.
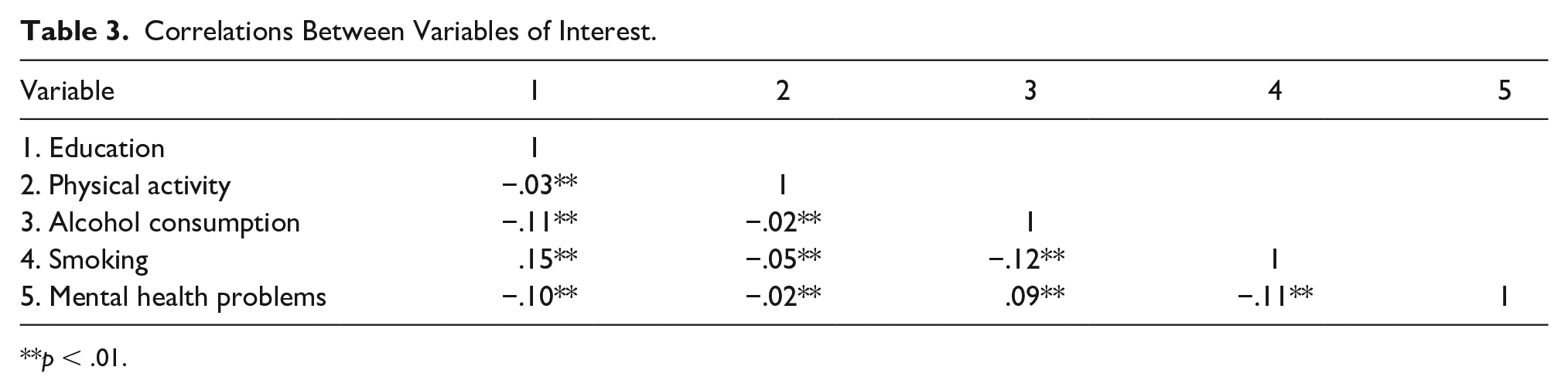
p < .01.
Two hierarchical linear regressions were performed to determine substance use moderators of the relation between physical activity and mental health problems. The first regression analysis revealed that alcohol consumption moderated the relation between physical activity and mental health problems, F(4, 160453) = 727.05, p < .001. Table 4 contains details of the first regression analysis. As depicted in Figure 1, those who did not drink alcohol had fewer mental health problems when they indicated greater amounts of time spent doing physical activities each week. The second regression analysis revealed that smoking moderated the relation between physical activity and mental health problems, F(4, 282366) = 1109.07, p < .001. Table 5 contains details of the second regression analysis. As depicted in Figure 2, smokers’ number of mental health problems decreased as they engaged in more physical activity, whereas nonsmokers’ number of mental health problems increased as they engaged in more physical activity.
Alcohol Consumption Moderation Regression Results.
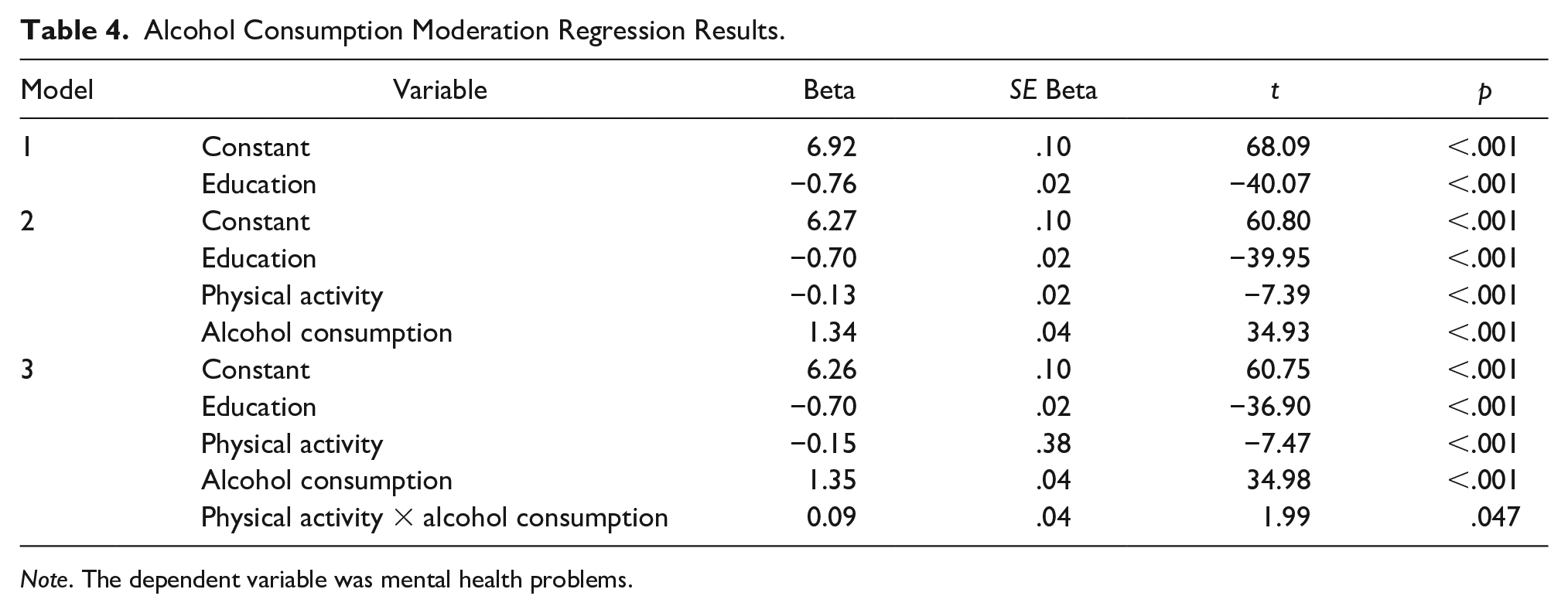
Note. The dependent variable was mental health problems.
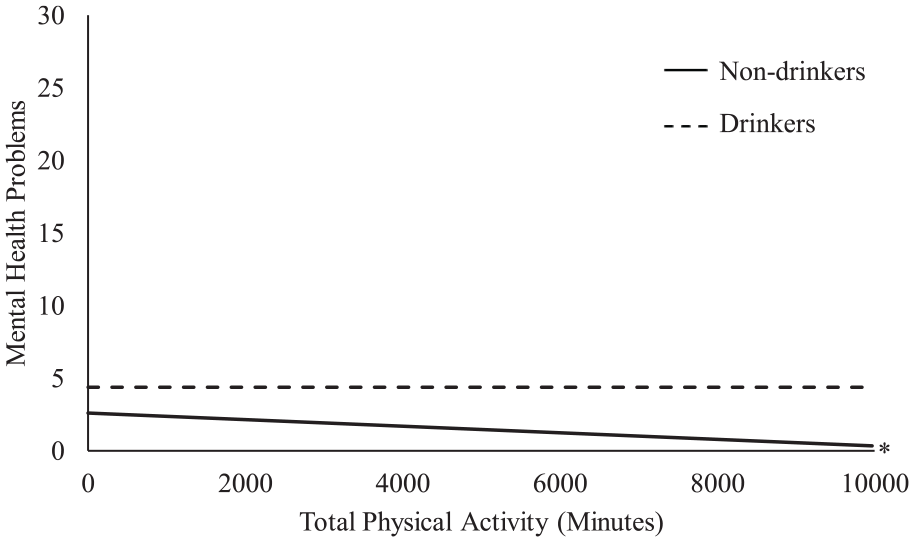
Physical activity and alcohol consumption interaction.
Smoking Moderation Regression Results.
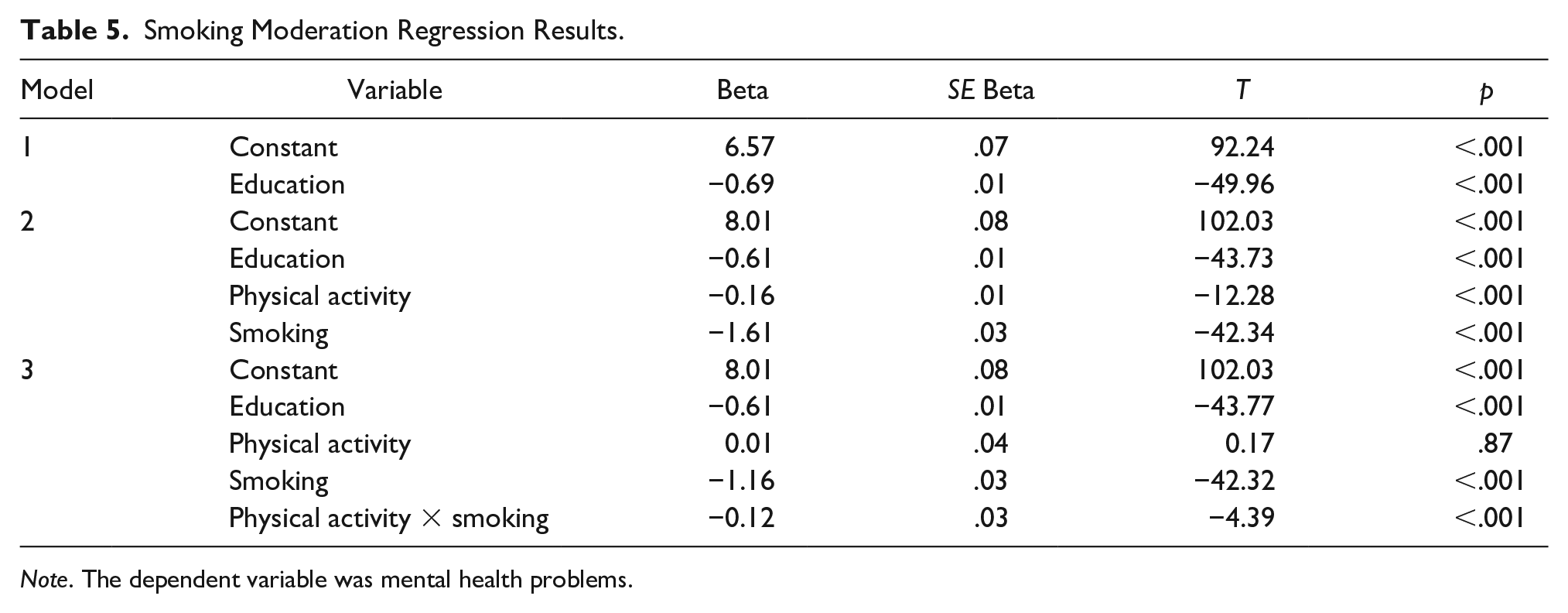
Note. The dependent variable was mental health problems.
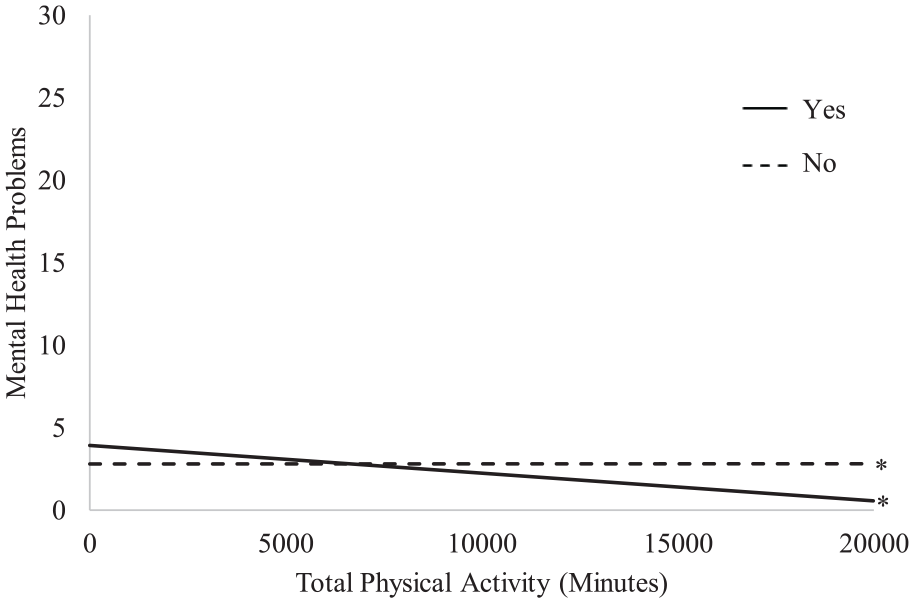
Physical activity and smoking interaction.
Discussion
We know that independently, physical activity and substance use are each associated with mental health outcomes. However, understanding how the relationship between physical activity and mental health is moderated by substance use necessitated further examination. Findings of this study indicate that nondrinkers had fewer mental health problems when they reported more minutes of physical activity per week. Therefore, although physical activity is beneficial in improving mental health, when evaluating comparisons of nondrinkers and drinkers, nondrinkers exhibited better mental health with increasing physical activity. Vidot et al. (2017) found that studies that examined the relationship between physical activity and mental health were inconclusive, perhaps because this relationship is moderated by substance use as found in this study. Alcohol is considered a central nervous system depressant, which may further explain why drinkers who are engaging in physical activity may not necessarily yield similar mental health results compared with their nondrinker counterparts. These findings supporting a positive relationship between physical activity and mental health outcomes are also consistent with findings by Mikkelsen et al. (2017).
Other findings from this study indicate that smokers’ mental health problems decreased as they engaged in more physical activity. Additionally, nonsmokers’ mental health improved as they engaged in more physical activity. This is consistent with findings by De Jesus and Prapavessis (2018) who found that exercise can be utilized as a smoking cessation intervention because it decreases cigarette consumption, decreases the satisfaction gained from smoking, decreases cravings for nicotine, and decreases the psychological reward gained from smoking, all of which are important in contributing to smoking cessation. This relationship can be explained by the fact that engaging in physical activity releases endorphins, which are hormones that reduce stress, a major trigger for cigarette smoking. These results can be further explained by the fact that research has shown that physical activity positively affects mental health outcomes such as depression among diverse individuals (Mumba et al., 2020; Rimes et al., 2015).
Health care providers, regardless of setting, should be vigilant and intentional with routinely screening for substance abuse, specifically alcohol and nicotine use disorders; they should also provide educational materials and resources to mitigate the negative effects of these problems on overall health and well-being. For example, the SBIRT (screening, brief intervention, and referral to treatment) model should be adopted by health care providers in various settings, but more especially in mental health settings. Health care providers should also educate their patients on the benefits of exercise as a nonpharmacological cost-effective intervention that improves mental health outcomes and can assist patients with smoking cessation efforts. Although this is a population-based study, this moderated effect should be examined in a longitudinal study to ascertain the long-term interaction and directionality of effects. Specifically, future studies should longitudinally examine the relationships among physical activity, substance use, and mental health to determine mechanisms across the life span that contribute to mental health problems in adults. Last, further studies are necessary to examine whether differences exist in this moderation effect based on severity of substance misuse.
Limitations
Some limitations regarding the measures utilized in this database should be considered when interpreting the results. The dependent variable, mental health problems, was assessed via one question rather than a previously validated questionnaire. This question asked participants to report if they had experienced a set of mental health problems, including stress, depression, and problems with emotions. Therefore, conclusions drawn about mental health problems in this study are limited to an aggregate of different conditions. Additionally, because the smoking variable asked participants whether they had smoked at least 100 cigarettes in their lives, it was unclear whether participants were currently smoking at the time they provided their responses to the survey. The last limitation related to measures is that alcohol consumption was a binary outcome, with only yes or no responses. Therefore, we are not able to ascertain the severity of alcohol consumption.
Conclusion
About 20% of adults in the United States report a mental health problem each year, and more than 14 million of adults have an AUD. The relationship between physical activity and mental health outcomes is well established and cannot be overemphasized. Nonetheless, substance abuse can moderate this relationship and should be routinely screened for by health care providers regardless of treatment setting. Longitudinal studies are needed to further understand this moderation effect and the long-term implications of substance use on physical and mental well-being of adults in the United States. Last, future studies are needed that utilize well-established and validated measures of alcohol and nicotine use to examine whether severity of these substance use disorders, rather than mere presence of the substance use disorder, still moderates this relationship.
Footnotes
Author Roles
All authors contributed to the conception or design of the study or to the acquisition, analysis, or interpretation of the data. All authors drafted the manuscript, or critically revised the manuscript, and gave final approval of the version that was submitted for publication. All authors agree to be accountable for all aspects of the work, ensuring integrity and accuracy.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received support from the Population Health Surveillance Branch of the Center for Disease Control.