
Abstract
Background:
Significant disparities in utilization of mental health services exist among immigrant and Canadian-born populations. These gaps may be associated with a ‘double stigma’ – stigma related to being from a racialized background exacerbated by mental health stigma. Immigrant young adults may be particularly susceptible to this phenomenon, given developmental and social transitions from adolescence to adulthood.
Aims:
To investigate the joint effects of racial microaggression and mental health stigma on mental health and service use among first-generation immigrant and Canadian-born university students.
Method:
We conducted an online cross-sectional study among first-generation immigrant and Canadian-born university students (N = 1,280, Mage = 19.10, SD = 1.50).
Results:
Despite no differences in anxiety or depression symptoms, first-generation (foreign-born) immigrants were less likely to have received therapy and to have taken medication for mental health issues compared to Canadian-born participants. First-generation immigrants also reported experiencing higher levels of racial microaggression and stigma toward service use. Results suggest the presence of a double stigma, mental health stigma and racial microaggression, each explained significant additional variance in symptoms of anxiety and depression and medication use. No effects of double stigma for therapy use were found – while higher mental health stigma predicted lower use of therapy, racial microaggression did not predict unique variance in therapy use.
Conclusions:
Our findings highlight the joint effects of racial microaggression and stigma toward mental health and service as barriers to help-seeking among immigrant young adults. Mental health intervention and outreach programmes should target overt and covert forms of racial discrimination while incorporating culturally sensitive anti-stigma approaches to help reduce disparities in mental health service use among immigrants in Canada.
Keywords
According to census data, close to one in four Canadians are foreign-born immigrants (Statistics Canada, 2021). Immigrant young adults, who also make up around 20% of Canadian universities’ populations (Statistics Canada, 2019), face unique and additive stressors such as adapting to a new country, learning a new language, and economic difficulties that can affect mental health (e.g., Kirmayer et al., 2011; Salami et al., 2019; Tulli et al., 2020). Immigrants from racialized backgrounds may also experience racial discrimination (Saechao et al., 2012; Thomson et al., 2015), including racial microaggression, which is a subtle, covert, and indirect form of racial discrimination (Sue et al., 2007; Williams, 2020). Despite heightened exposure to these stressors and potential mental health needs, there are significant gaps in mental health service use among immigrants: immigrants consistently report lower utilization of mental health care than Canadian-born individuals, even after accounting for self-reported mental health (Chiu et al., 2018; Mental Health Commission of Canada, 2016; Ng & Zhang, 2021; Urbanoski et al., 2017).
Underutilization of mental health services has been linked to complex and interacting factors, including cultural and linguistic barriers, financial challenges, and a lack of awareness of services (reviewed in Salam et al., 2022). Among individuals in marginalized communities, this underutilization might be exacerbated by a ‘double stigma’ – stigma related to being from a racialized or immigrant background exacerbated by a person’s perceived stigma toward mental health and service use (Gary, 2005). This double stigma has been shown to account for associations between racial discrimination, poorer mental health, and lower mental health services use (e.g., Krill Williston et al., 2019; Quinn et al., 2020). Accordingly, we examined the joint effects of racial microaggression and stigma in relation to (1) symptoms of depression and anxiety and (2) service use among first-generation immigrant and Canadian-born young adults.
The role of racial discrimination on physical and mental health is well-established. Through multiple pathways such as increased stress or maladaptive coping mechanisms, racial discrimination has been associated with negative mental health consequences including general distress, anxiety, and depression across genders, age groups, and racial/ethnic backgrounds (Paradies et al., 2015; Schmitt et al., 2014). Experiences of racial discrimination are multifaceted; they can include overt attacks or more subtle, brief and commonplace covert acts. These covert acts, defined as racial microaggression, may be equally or even more detrimental to racialized individuals because they can be hard to identify, leading to self-doubt and invalidations by victims, perpetuators, or outsiders (Sue et al., 2007; Williams, 2020). Research on overt forms of discrimination and the equally negative impact of racial microaggression on mental health have been more commonly examined among people of colour (Lui & Quezada, 2019; Nadal et al., 2014). However, there is a paucity of research on experiences with racial microaggression among racialized immigrants. The few available studies have focused on specific immigrant groups (e.g., West African immigrants) using qualitative methods, with virtually no quantitative data available (Otusanya & Bell, 2018; Zaami & Madibbo, 2021). Given the emphasis on multiculturalism in Canada, which often lends to a ‘colourblind’ approach to race (Williams et al., 2022), a form of microaggression in itself (Spanierman et al., 2021), it is especially important to investigate this phenomenon in a Canadian context.
Evidence on the relation between racial discrimination and service use has been more inconsistent. In a systematic review and meta-analysis on general health service use, Ben et al. (2017) found that self-reported racism was associated with more negative experiences of health services and lower healthcare-related trust, satisfaction, and communication, but there were no associations between direct health service use. Similarly, when examining mental health service use specifically, some studies showed associations between racial discrimination and more informal sources of help, but not formal mental health services (e.g., Spencer et al., 2010). In contrast, in a large multi-ethnic, community sample in the United States, Burgess et al. (2008) found that experiences of racial discrimination were associated with lower utilization of mental health services. Although research among immigrant young adults or adult populations is limited, this finding has been supported by a qualitative study by Tulli et al. (2020) in which immigrant mothers identified racial discrimination as a barrier to accessing mental health care for their children. Racial microaggression may play an even more important role in the context of mental health services, especially when coming from clinicians, as they have been linked to early termination, poor therapeutic alliance, and treatment outcomes among racialized clients and even lower callback rates for mental health service requests compared to White clients (reviewed in Williams, 2020). Although there is evidence showing the role of racial microaggression in Asian American college students’ attitudes toward help-seeking (Kim et al., 2017), there is less research on its associations with actual mental health service use, especially for immigrant populations in Canada.
Several reasons underlying the associations between racial discrimination and utilization of mental health services have been identified in the literature, including mistrust of health care providers and institutions related to historical racial bias and abuse (Krill Williston et al., 2019; Tulli et al., 2020). Among racialized immigrants, these reasons can also include discriminatory comments and questioning targeted about their intersectional identities of gender, immigrant status, ethnicity, and language, which can negatively impact willingness to seek mental health services (Salam et al., 2022). Double stigma, or the additive and exacerbating effects of stigma related to being from a racialized background and stigma toward mental health and toward service use, has also been identified as a barrier to utilization of mental health services (Gary, 2005). On its own, mental health stigma has been linked with decreased help-seeking behaviour, intentions, and service use among adolescents (e.g., Nearchou et al., 2018; Yap et al., 2011, 2013) and university students (e.g., Schnyder et al., 2017; Tucker et al., 2013; Wu et al., 2017). It has also been associated with substantial underreporting of mental disorder symptoms in Australian adults (Bharadwaj et al., 2017). In conjunction with racial discrimination, double stigma is associated with more depressive symptoms, anticipated stigma for having a mental health problem, and negative beliefs about mental health problems among people of colour (Krill Williston et al., 2019; Quinn et al., 2020). However, to our knowledge, researchers have yet to investigate the effects of this double stigma on actual mental health service use, or among immigrant populations in a Canadian context.
First-generation immigrant young adults may be particularly susceptible to the negative consequences of double stigma. Marked by experiences of transitions, both at the developmental and social levels, this group is especially at risk for mental health difficulties and face additional barriers to mental health service use (Kessler et al., 2007; Li et al., 2016). On the one hand, from adolescence to adulthood, young adults continue to develop a sense of identity, which plays a role in well-being, internalizing and externalizing disorders, and health behaviour (Schwartz et al., 2015). This transition is often accompanied by simultaneous transitions from high school to university, which can lead to changes in living arrangements, academic demands, and social relationships that can subsequently also affect mental health (Howard et al., 2010). On the other hand, first-generation immigrant young adults also transition from their country of birth to a new one, facing additional challenges such as integrating into a new culture, managing multiple cultural identities, navigating new healthcare and education systems, and racial discrimination (e.g., Kirmayer et al., 2011; Saunders et al., 2018; Thomson et al., 2015). Given the unprecedented stressors linked to the COVID-19 pandemic that have amplified pre-existing disparities in mental health service use among immigrant communities (Sanford et al., 2022; Sieffien et al., 2020), it is crucial to investigate the factors affecting mental health and service use in this at-risk group.
Our aim was to address these gaps in the literature by investigating the joint effects of racial microaggression and mental health stigma (i.e. double stigma) on mental health and service use among first-generation immigrant young adults in Canada. Our work was guided by two main objectives: (1) How do first-generation immigrants and Canadian-born young adults differ in mental health, service use, experiences with racial microaggression, and perceived stigma toward mental health and service use? and (2) How does double stigma relate to mental health and mental health service use? We predicted that, consistent with prior literature (e.g., Ng & Zhang, 2021), there would be no differences in mental health outcomes between both groups, but first-generation immigrants would report lower use of mental health services than Canadian-born young adults. Next, we predicted that first-generation immigrants would report experiencing more racial microaggression and perceived stigma toward mental health and service use than their Canadian-born peers. Lastly, in line with prior research (Krill Williston et al., 2019; Quinn et al., 2020), we predicted that racial microaggression and perceived mental health stigma will contribute unique variance in predicting lower mental health outcomes and lower use of mental health services.
Methods
Procedure
Participants were recruited from diverse cultural and immigration backgrounds from September 2021 to April 2022 through a large Canadian university’s participant pool, student associations and clubs and classes in various academic departments. Participants were also recruited through public advertising (i.e., social media posts) targeting university students across Canada. The survey was administered online through Qualtrics and was available in English. Participants provided informed consent prior to completing the survey and were compensated course credit or were entered in a draw to win 1 of 20 $50 Visa gift cards after completion. All materials and procedures were approved by the University of Ottawa Research Ethics Board.
Participants
The sample consisted of 1,280 participants aged 17 to 24 years old (M = 19.10, SD = 1.50). Most participants self-identified as women (75.5%; n = 966). First-generation immigrants (i.e., born outside of Canada) constituted 39.2% (n = 502) of the sample, while Canadian-born young adults comprised 60.6% of the sample (n = 776). The racial/ethnic background of participants was as follows: 36.1% White (n = 462), 15.0% Black (n = 192), 2.5% Hispanic (n = 32), 1.0% Indigenous (n = 13), 16.7% East/Southeast Asian (n = 214), 10.8% South Asian (n = 138), 13.0% Middle Eastern (n = 166), 0.7% Other (n = 9), 3.6% Multiracial (n = 46) and 0.6% missing (n = 8). Additional demographic information is provided the results section (Table 1).
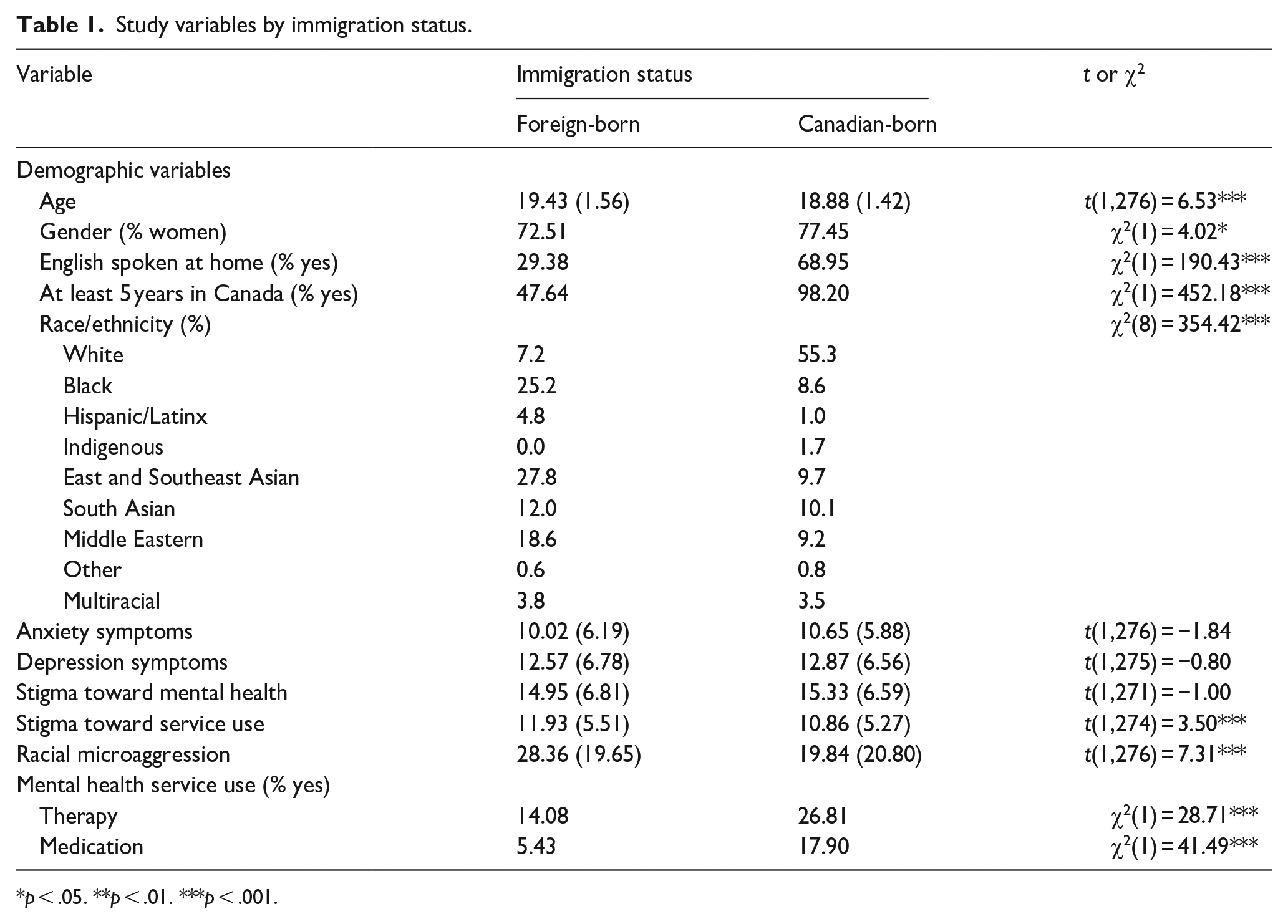
Study variables by immigration status.
p < .05. **p < .01. ***p < .001.
Measures
Demographics
An adapted version of existing demographic questionnaires (Statistics Canada, 2009; Vaillancourt et al., 2021) was used to assess participants’ general demographic information such as age, gender, racial/ethnic background, country of birth, length of time in Canada, and language spoken at home.
Perceived stigma toward mental health and toward service use
The Stigma-9 Questionnaire (STIG-9; Gierk et al., 2018) is a 9-item measure assessing cognitive, behavioural, and affective aspects of perceived stigma toward mental health. Items such as ‘I think most people consider mental illness to be a sign of personal weakness’ were rated on a 4-point scale (0 = disagree to 3 = agree), with high internal consistency in the current sample (α = .92). A higher score on the STIG-9 indicates more mental health stigma.
The Attitudes towards Seeking Professional Psychological Help (ATSPPH-Short Form; Fischer & Farina, 1995) is a 10-item questionnaire assessing general attitudes toward seeking professional psychological help. Items (e.g., ‘I might want to have psychological counselling in the future’) are rated on a 4-point scale (0 = disagree to 3 = agree), where higher scores indicate more positive attitudes toward using mental health services (i.e., lower stigma). For the purposes of the current analyses, we reverse-scored items to reflect stigma toward mental health services (i.e., higher scores indicate higher stigma). The ATSPPH-SF has been found to correlate well with the original 29-item scale (r = .87) and other measures of mental health seeking (Fischer & Farina, 1995). It also demonstrated adequate internal consistency in our sample (α = .77).
Experiences of racial microaggression
The Racial Microaggressions Scale (RMAS-32; Torres-Harding et al., 2012) is a 32-item scale that assesses different themes and categories of microinsults and microinvalidations (i.e., Invisibility, Criminality, Low-Achieving/Undesirable Culture, Sexualization, Foreigner/Not Belonging, Environmental Invalidations). We used the total score with all 32 items (e.g., ‘I feel invisible because of my race’), which were rated on a 5-point scale (0 = never to 4 = often). The RMAS-32 demonstrated excellent internal consistency in the current sample (α = .95).
Mental health outcomes
The Generalized Anxiety Disorder scale (GAD-7; Spitzer et al., 2006) is a measure of anxiety symptoms rated on a 4-point scale (0 = not at all to 3 = nearly every day) with 7 items such as ‘Trouble relaxing’. This scale is widely used both in research and clinical settings and has demonstrated high reliability in the current sample (α = .91).
The 10-item version of the Center for Epidemiologic Studies Depression Scale (CES-D-10; Andresen et al., 1994) was used to assess depression symptoms. Items (e.g., ‘I felt depressed’) were rated on a 4-point scale from 0 = Rarely or none of the time (less than 1 day) to 3 = Most or all of the time (5–7 days). This scale is also widely used in both research and clinical settings and has demonstrated good internal consistency in our sample (α = .84).
Mental health service use
We measured participants’ mental health service use for the past year using two binary questions (0 = no, 1 = yes) based on Downs and Eisenberg (2012): ‘In the past 12 months, have you received counselling or therapy for your mental or emotional health from a health professional?’ and ‘In the past 12 months, have you taken any prescription medications for your mental or emotional health?’.
Analytic plan
SPSS v.28 was used to analyse the data. Before conducting analyses, we excluded invalid responses (e.g., failing to correctly answer attention check questions, incompletion of survey) and screened data for violations of normality, including kurtosis and skewness. For Objective 1, t-tests and chi-squared tests were used to compare mental health, racial microaggression, perceived stigma toward mental health and service use, and actual service use between first-generation immigrant and Canadian-born students. Next, Pearson’s correlations were used to examine associations between continuous variables of interest (i.e., mental health, racial microaggression, perceived mental health, and service use stigma) in the total sample. The same correlations were conducted by immigration status. Fisher’s z transformations were applied on correlation coefficients, which were then compared using Fisher’s z test. Continuous predictors were mean centred before conducting the multiple regressions. For Objective 2, hierarchical regressions were conducted with mental health and service use as outcome variables, with Step 1 including demographics, Step 2 including perceived stigma toward mental health and seeking services, Step 3 including racial microaggression and Step 4 including interactions between immigration status and mental health stigma/racial microaggression.
Results
Comparing immigrant and Canadian-born young adults
Table 1 shows proportions, means, and standard deviations for all study variables by immigration status. Chi-squared tests and t-tests revealed significant differences by age and gender – the average age of first-generation immigrant students was older than Canadian-born students and there were slightly more female Canadian-born students than their foreign-born counterparts. Chi-squared tests also revealed that first-generation immigrants were less likely than Canadian-born peers to report speaking English at home and to have lived at least five years in Canada. Moreover, the racial/ethnic background of participants also differed depending on immigration status. For example, 55.3% of Canadian-born participants reported being White, compared to 7.2% of foreign-born participants.
There were no statistical differences in anxiety and depression symptoms across immigration status, but first-generation immigrant participants were less likely to have received therapy or medication for their mental health needs. Moreover, while both groups did not differ significantly on perceived stigma toward mental health, first-generation immigrants reported more perceived stigma toward mental health service use and experiences of racial microaggression than their Canadian-born peers.
Correlational analyses
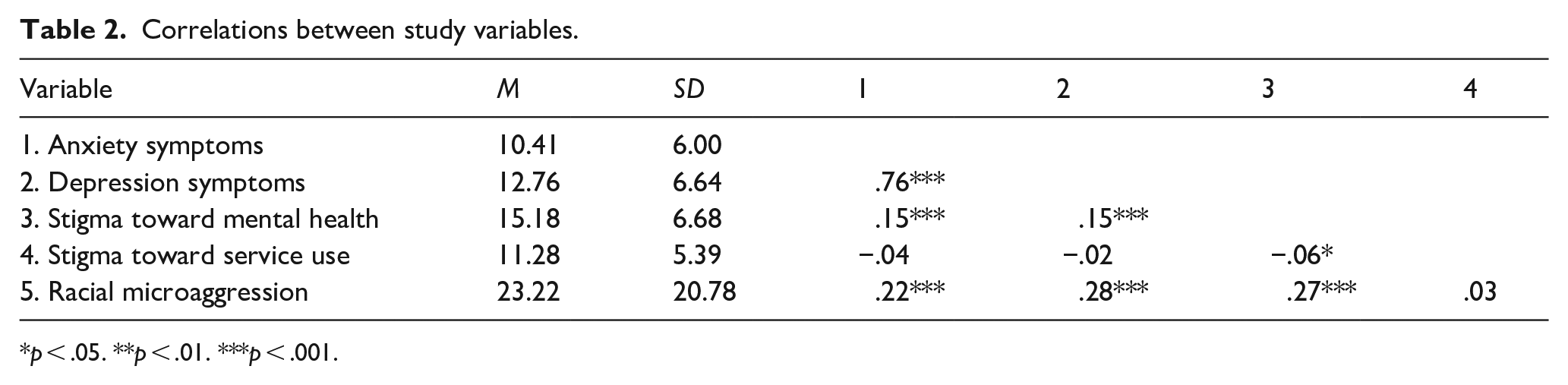
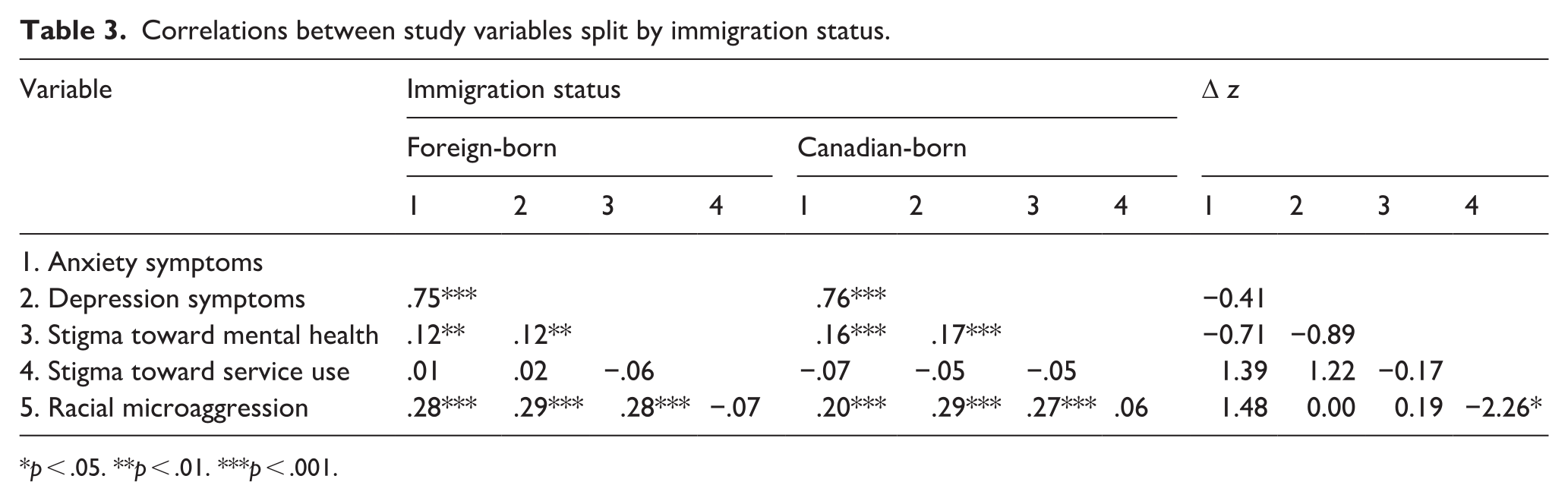
Table 2 shows Pearson correlations between all study variables. First, higher stigma toward mental health was significantly associated with higher anxiety symptoms, higher depression symptoms, and lower stigma toward service use. Experiences of racial microaggression were significantly correlated with higher anxiety and depression symptoms, as well as higher stigma toward mental health but not toward service use. Table 3 shows the same correlations split by immigration status, as well as the differences between groups by comparing Fisher’s Z transformed correlation coefficients. Results showed that associations between stigma toward service use and racial microaggression differed significantly by group (Δz = −2.26, p < .05). Specifically, racial microaggression was negatively correlated with stigma toward service use (r = −.07) for first-generation immigrants but positively correlated for Canadian-born participants (r = .06). No other correlations were significantly different across immigration status.
Correlations between study variables.
p < .05. **p < .01. ***p < .001.
Correlations between study variables split by immigration status.
p < .05. **p < .01. ***p < .001.
Double stigma and mental health
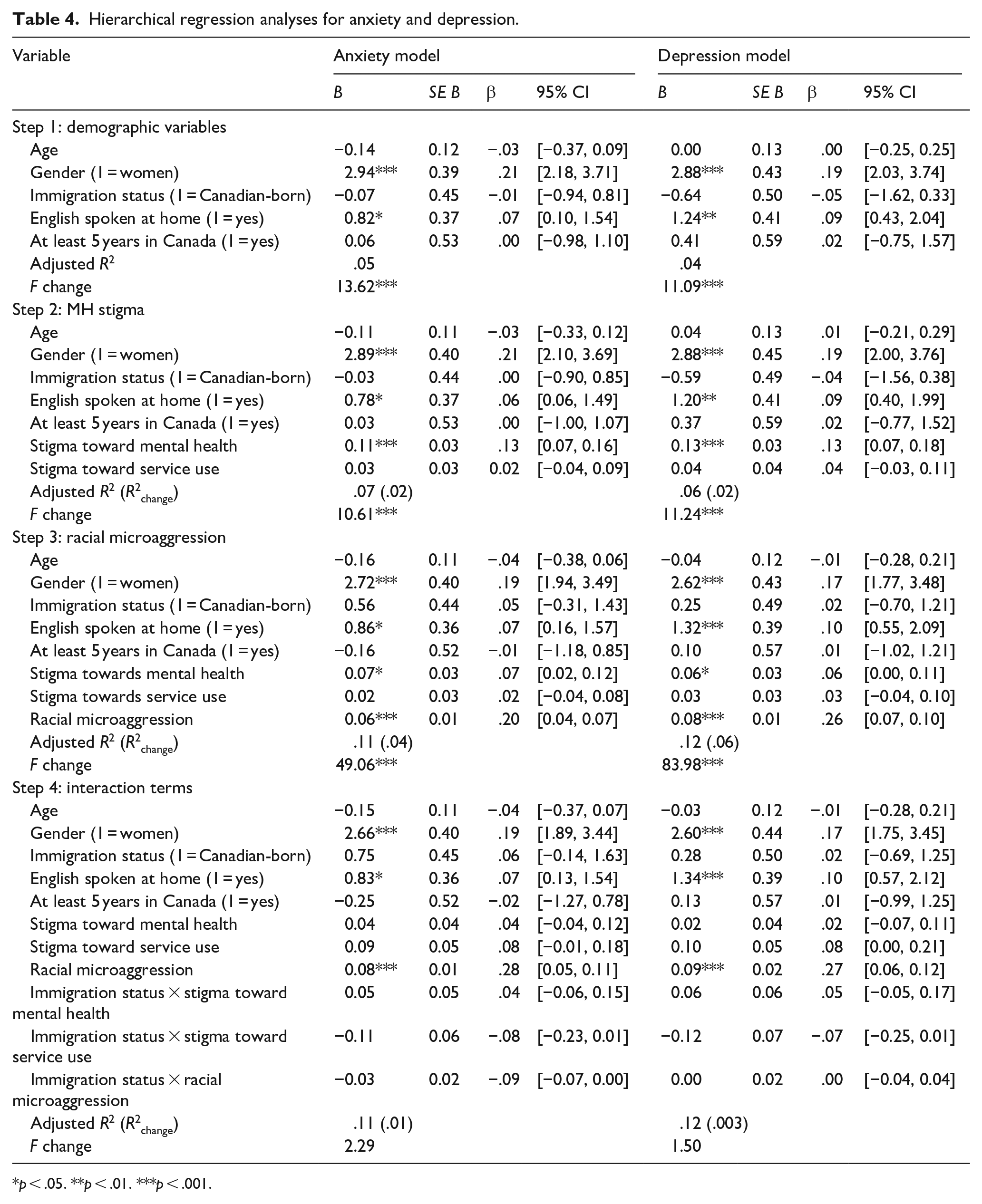
Table 4 displays hierarchical linear regressions with anxiety and depression symptoms as outcome variables, separately. Step 1 included demographic characteristics (i.e., age, gender, immigration status, length of time in Canada and language spoken at home), Step 2 included perceived stigma toward mental health and service use, Step 3 included racial microaggression and Step 4 included interaction terms between immigration status and mental health stigma/racial microaggression.
Hierarchical regression analyses for anxiety and depression.
p < .05. **p < .01. ***p < .001.
Results showed that although age, immigration status and length of time in Canada did not significantly predict anxiety or depression, gender, and language spoken at home were associated with both outcomes. Women and those who did not speak English at home reported higher anxiety and depression symptoms than men and those who did speak English at home, respectively.
We also found evidence of double stigma for both outcomes: for anxiety, stigma toward mental health in Step 2 (B = 0.11, SE = 0.03, β = .13, p < .001, R2change = .02) and experiences of racial microaggression in Step 3 (B = 0.06, SE = 0.01, β = .20, p < .001, R2change = .04) predicted unique variance in anxiety symptoms, such that higher stigma toward mental health and more experiences of racial microaggression were associated with higher anxiety. Similarly, for depression, stigma toward mental health (B = 0.14, SE = 0.03, β = .13, p < .001, R2change = .02) and racial microaggression (B = 0.08, SE = 0.01, β = .26, p < .001, R2change = .06) also predicted unique variance in depression symptoms, such that higher stigma toward mental health and more experiences of racial microaggression were associated with higher depression. These results indicated that stigma toward mental health and stigma related to being from a racialized background (in the form of racial microaggression) both contributed to anxiety and depression above and beyond demographic variables. No other main or interaction effects were significant.
Double stigma and mental health service use
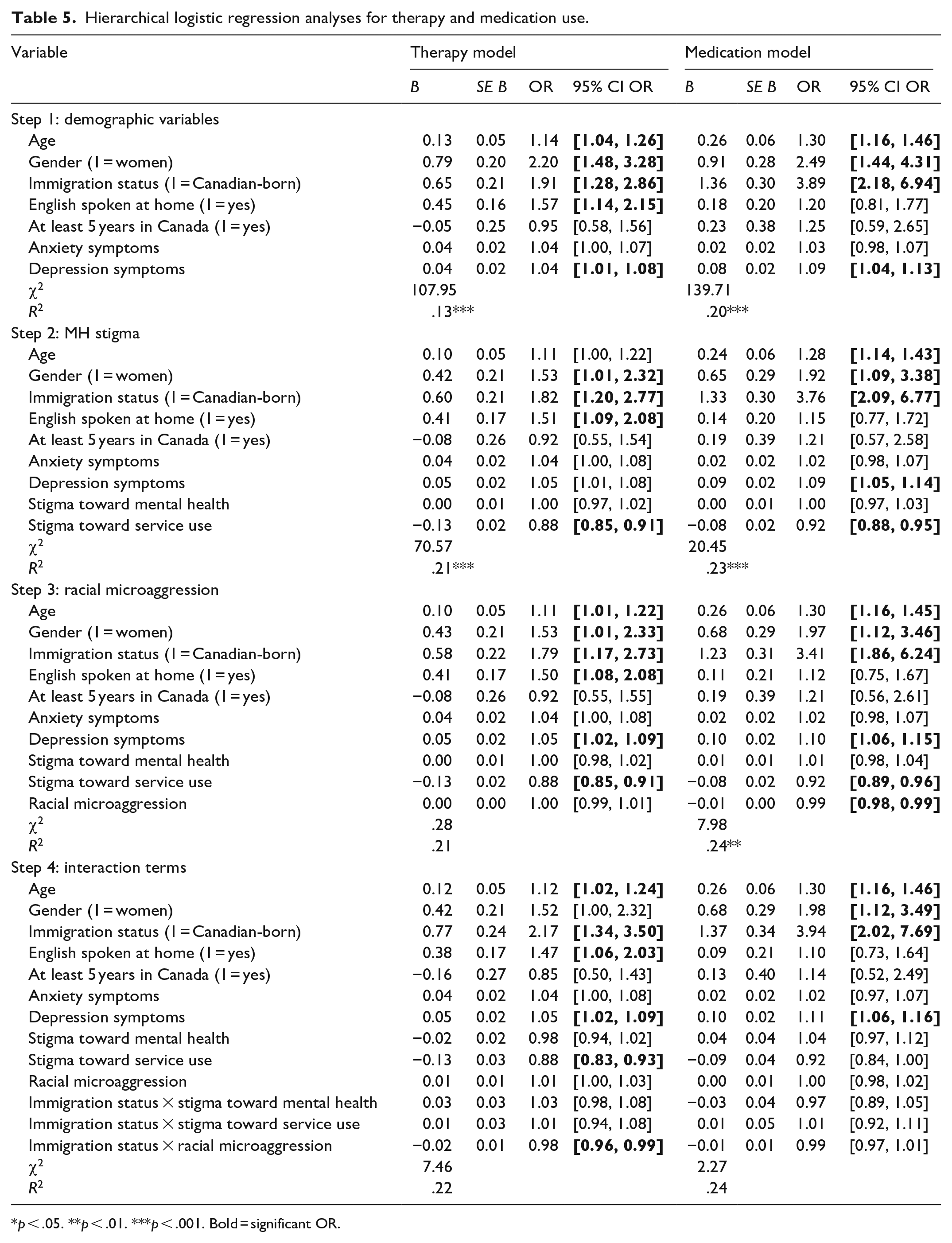
Table 5 shows hierarchical logistic regressions with anxiety and depression symptoms as outcome variables, separately. Step 1 included demographic characteristics (i.e., age, gender, immigration status, length of time in Canada, and language spoken at home) and mental health (i.e., anxiety, depression), Step 2 included perceived stigma toward mental health and service use, Step 3 included racial microaggression and Step 4 included interaction terms between immigration status and mental health stigma/racial microaggression.
Hierarchical logistic regression analyses for therapy and medication use.
p < .05. **p < .01. ***p < .001. Bold = significant OR.
Results indicated that several demographic variables in Step 1 were significantly related to mental health service use. For both therapy and medication use, higher use was associated with older age, identifying as a woman, being born in Canada, and higher depression symptoms. Moreover, speaking English at home was associated with higher likelihood to seek therapy, but not medication use.
For mental health service use, effects of this ‘double stigma’ were present for medication use but not therapy use, after controlling for anxiety and depression. Although those with higher stigma toward mental health service use were more less to have used therapy in the last year (OR = 0.88, 95% CI [0.85, 0.91]), experiences of racial microaggression were not significantly associated with therapy use. Conversely, stigma toward service use (OR = 0.92, 95% CI [0.88,0.95]) and experiences of racial microaggression (OR = 0.99, 95% CI [.98,.99]) both contributed unique variance in medication use. These results indicated that participants who reported higher stigma toward service use and who experienced less racial microaggression were less likely to have used medication in the last year. No other main or interaction effects were significant.
Discussion
In the present study, we examined how experiences of racial microaggression and mental health stigma (i.e., double stigma) jointly affected mental health outcomes and utilization of mental health services among first-generation immigrant and Canadian-born young adults.
Our results highlight the significant gap in utilization of mental health care services among first-generation immigrant young adults in Canada, which is consistent with nationally representative Canadian samples (Ng & Zhang, 2021). Importantly, consistent with our hypotheses, first-generation immigrant and Canadian-born young adults did not differ in anxiety or depressive symptoms. Although this might reflect an ‘immigrant paradox’, or immigrant individuals having better or similar mental health outcomes as non-immigrant individuals despite increased socioeconomic disadvantages and stress (Yang, 2021), this finding also suggests that immigrant young adults who do experience mental health problems are not seeking or receiving the appropriate mental health supports. Moreover, we found that first-generation immigrant young adults reported higher stigma toward service use than their Canadian-born peers but did not differ in stigma toward mental health, which did not align with our predictions and the existing literature (e.g., Nadeem et al., 2007; Saechao et al., 2012). This finding may be due to our measurement of mental health stigma. It is possible that given recent efforts of mental health awareness in Canada (e.g., Bell Let’s Talk), there has been a decline in the explicit reporting of negative attitudes toward mental health combined with potential social desirability bias. Given that we used a self-report measure of explicit stigma (Gierk et al., 2018), we may have not captured differences in mental health stigma that are more indirect, unconscious, and automatic (i.e., implicit attitudes; Peris et al., 2008). Researchers may want to investigate the role of implicit mental health stigma as a barrier to help-seeking and service use among immigrant populations.
Consistent with our predictions, first-generation immigrants reported more experiences of racial microaggression, which interacted with mental health stigma to jointly contribute to mental health and service use. Researchers have hypothesized that the effects of double stigma may be attributed to perceptions of holding multiple stigmatizing identities related to being from a racialized background and experiencing mental health difficulties (Krill Williston et al., 2019). For example, racialized immigrants who experience discrimination related to their background may be especially reluctant to seek mental health services out of fear of experiencing even more discrimination and stigma from their health care providers or members of their communities. Other researchers (Quinn et al., 2020) have posited that experiences of discrimination related to a visible stigmatized identity (i.e. race) may sensitize individuals to anticipate more stigma based on a concealable identity (i.e. having mental health difficulties). In other words, it may be possible that racial discrimination experiences based on race can lead individuals to expect more discrimination based on other social identities such as mental state or immigration status. Although we did not measure specific immigration-related discrimination or stigma, researchers may want to consider how stigma related to these other concealable social identities can have additive effects on mental health and service use.
Further, our study contributes to existing literature on double stigma by considering covert forms of racial discrimination (i.e., racial microaggression), which may play an especially important role in utilization of mental health services. Compared to overt or more direct racial discrimination, racial microaggressions may be equally or even more detrimental because they can be hard to identify for both perpetrators and victims (Sue et al., 2007). In the context of mental health care, given that treatment revolves around interactions and relationships between mental health professionals and clients, there has been an increasing attention to the negative consequences of racial microaggressions. Mental health professionals, who are more mostly White in Canada (Statistics Canada, 2016), may inadvertently perpetuate culturally insensitive acts by not noticing acts of racial microaggressions or minimizing its harm. Simultaneously, racialized clients may also question the validity of their feelings of discomfort or disrespect, given the subtle nature of microaggressions. Therefore, previous experiences of racial microaggression may lead racialized immigrants to avoid seeking mental health services despite their needs, exacerbating pre-existing mental health stigma and resulting in lower use of services.
Interestingly, while we did find effects of double stigma on medication use, racial microaggression was not a significant predictor of therapy use above and beyond stigma toward mental health service use. Although previous studies have not shown a difference in therapy versus medication use when only examining mental health stigma (Downs & Eisenberg, 2012; Eisenberg et al., 2009), a qualitative study among immigrants suggested that most had negative attitudes toward medication and that perceived over-prescription of psychiatric medication was a barrier to seeking mental health services (Whitley et al., 2006). One possible explanation underlying more negative attitudes toward using medications versus therapy could relate to their relative perceived seriousness. Participants may have perceived that individuals taking medication for their mental health issues have more serious mental issues compared to those using therapy, which in turn could lead to higher stigma and reluctance to seek mental health services. The literature on this possible reason is still limited. A qualitative study among adolescents found that participants perceive that medications are for people who are ‘psycho’ (Kranke et al., 2011). Consequently, the exacerbating effects of racial microaggression may be higher for medication than therapy use, which may explain our null effects of double stigma on therapy use.
Limitations
Several limitations need to be considered when interpreting our findings. To start, the cross-sectional design of our study prevents inferences of causality and directionality. Future longitudinal studies should be conducted to clarify these findings, which would benefit designs of anti-stigma interventions and mental health promotion programmes among immigrant young adults.
Next, our sample consisted of university students, which precludes us from generalizing our findings to immigrant young adults who may already be in the workforce. Our survey was also only available in English, which limited participation from those who were not comfortable in this language. Given that language spoken at home seems to play a significant role in use of mental health services (especially therapy), future work may use sampling procedures that capture immigrant young adults in Canada who do not attend university or who do not speak English fluently.
Another limitation was that we were unable to untangle ethnicity from immigration, given a large overlap in our sample – more than 94% of first-generation immigrants identified as non-White. Similarly, given our sample size, we were unable to consider specific ethnic/racial groups or immigration statuses (e.g., refugees, second-generation immigrants). Further, when we examined subscales in the RMAS (e.g., Invisibility, Criminality), we found that immigrant participants consistently reported higher rates than their Canadian-born peers, but we were unable to detect any race- or ethnicity-related patterns. Given the heterogeneity that exists within each group in terms of cultural values, norms and practices, future research should consider examining double stigma among specific racialized immigrant communities and investigating different types of racial microaggression to better target future intervention programmes. However, we believe that our collapsed approach allows us to provide initial and general evidence that racial microaggression does play a role in mental health stigma, outcomes, and service use.
We were also unable to consider the intersectional identities of our participants. Particularly, given that more than 75% of our sample identified as women, we were unable to include gender in our analyses. Because men are simultaneously less likely to seek help and less likely to participate in psychological research compared to women (Chatmon, 2020), future research may examine mental health stigma and service use using an intersectional lens (e.g., examining experiences of immigrant women versus immigrant men).
Lastly, we did not consider cultural processes such as ethnic identity and acculturation. Although we examined the length of time in Canada, which can relate to these cultural processes, and found that it did not significantly play a role in our outcomes, future work may include a more direct measurement of ethnic identity and acculturation. Given that these factors have been shown to independently both buffer and exacerbate the effects of racial discrimination and mental health stigma on mental health and help-seeking (Cheng et al., 2013; Woo et al., 2019), further research on this topic would be critical. Future work may also consider pre-migration experiences and country of birth, given existing literature on refugee mental health and service use (Ng & Zhang, 2021).
Conclusion and implications
Given the increasing global proportion of immigrants, especially in Canada, as well as the multitude of immigration-related stressors faced by these communities, it is important to understand potential barriers to mental health service use. To our knowledge, our study is the first to investigate the joint effects of racial microaggression and stigma toward mental health and service use (i.e., double stigma) among first-generation immigrant and Canadian-born young adults.
These findings contribute to a fuller understanding of how stigma may contribute to mental health, while highlighting the importance of incorporating overt and covert racial discrimination within anti-stigma programmes and interventions. Additionally, they may also inform public health policies, such as increasing mental health services in diverse languages other than English and incorporating psychoeducation on the benefits of medication use for certain disorders. They may also inform government and school policies more broadly, highlighting that even though immigrants are found to have similar mental health than those born in Canada, they do experience challenges with mental health stigma and racial microaggressions as part of their resettlement process, which can in turn be risks to their mental health and integration. Finally, the results of our study may inform mental health treatment and interventions for clinicians, which may address current service use disparities and contribute to better well-being for immigrant young adults in Canada.
Footnotes
Acknowledgements
We are grateful to all participants for their valuable time and energy completing our study.
We thank the members of the Culture, Diversity, & Youth Development Lab and the Brain and Behaviour Lab at the University of Ottawa for their feedback and support throughout the project. We also thank volunteers and research assistants for their help with implementing and recruiting for our study: Cloudia Rodriguez, Marilou Poitras, Sahej Kaur, Tiana Rangoussis, and Zoe Campbell (in alphabetical order).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Seed Funding Opportunity (SFO) from the University of Ottawa Faculty of Social Sciences awarded to Irene Vitoroulis, Ph.D.