
Abstract
Objective:
Postpartum mental disorders are twice as common among immigrant women compared to nonimmigrant women in developed countries. Immigrant women may experience barriers to access and use of postpartum mental health services, but little is known about their service use on a population level. We described postpartum mental health service use of immigrant mothers living in Ontario, Canada, comparing to a referent group of mothers who were either born in Canada or had lived in Ontario or another Canadian province since 1985.
Method:
Among all women in Ontario, Canada, delivering a live infant from 2008 to 2012 (n = 450,622), we described mental health service use within 1 year postpartum, including mental health physician visits, psychiatric emergency department visits, and psychiatric hospitalization. Adjusted odds ratios (aORs) and 95% confidence intervals (CIs) comparing immigrant women to the referent group were adjusted for maternal age, parity, income, rurality, mental health services in prior 2 years, and maternal and newborn health.
Results:
Immigrant women (n = 123,231; 27%) were less likely to use mental health services than women in the referent group (14.1% vs. 21.4%; aOR, 0.59; 95% CI, 0.58 to 0.61), including for physician-based (13.9% vs. 21.1%; aOR, 0.59; 95% CI, 0.58 to 0.61) and emergency department (0.6% vs. 1.3%; aOR, 0.63; 95% CI, 0.57 to 0.68) services. Hospitalization risk was lower among immigrants (0.20% vs. 0.33%) but became similar after covariate adjustment (aOR, 0.92; 95% CI, 0.79 to 1.06).
Conclusions:
Underuse of postpartum mental health services may be contributing to the high burden of postpartum mental disorders among immigrant women.
Clinical Implications
With 27% of births being to immigrant women, mental health service use in this population warrants consideration at the public health level. Low levels of outpatient postpartum mental health service use among immigrant women are of concern given other research demonstrating that immigrant women have a 2-fold increased risk for postpartum mental health problems. Immigrant and long-term resident women had similar psychiatric hospitalization risk, suggesting that immigrant women are accessing services when problems are severe.
Limitations
This study could not directly measure unmet need for postpartum mental health care. We were not able to measure postpartum mental health services delivered through the private system, in the community, or through informal networks or relationships. This study was not designed to address specific reasons for differential use of services by immigrant women.
The postpartum period is a high-risk time for new-onset and recurrent mental disorders, including depression, anxiety, mania, and psychosis, affecting up to 20% of women who have recently given birth. 1,2 These disorders can have a serious, negative, long-lasting impact on mothers, developing children, and families. 1,3 In the short term, postpartum mental disorders can affect maternal-child bonding and attachment and in the longer term are associated with delayed child development and child mental health conditions, especially when untreated or incompletely treated. 4 As such, effective treatment of postpartum mental disorders is a high priority from a public health perspective.
In several developed countries, including, Canada, the United Kingdom, and Australia, immigrants comprise nearly one-quarter of the population, and most recent immigrant women are of reproductive age. 5 –9 The “healthy immigrant effect” suggests that through factors such as self-selection, education requirements, and immigration criteria, immigrants are healthier than native-born populations at the time of arrival. 10 Importantly, however, the application of this healthy immigrant effect to perinatal health is more variable, with immigrant women in Canada having more small-for-gestational age infants and higher rates of postpartum pain, bleeding, and hypertensive disorders of pregnancy compared to long-term Canadian residents. 11,12 The mental health of immigrant mothers appears to be particularly poor. Research suggests that immigrant women to developed countries, including in Canada, are at high risk for postpartum mental disorders, with rates of postpartum depression increased up to 2-fold those of nonimmigrant women. 13 –17 In Canada, at least, the pattern for postpartum mental health symptoms among immigrant women appears to follow the opposite trend to the healthy immigrant effect, whereby more recent immigrant women are at highest risk. 18 The reasons for observed higher rates of mental disorders among immigrant women are likely multifactorial but may be partially due to higher rates of social risk factors, including low income, unemployment, intimate partner violence, and poor social support networks, compared to the nonimmigrant population. 2,10,16,19 –26 Our previous population-based Canadian studies showed that immigrant women have higher rates of postpartum depressive symptoms up to 14 months postpartum. 14,27 Since the common postpartum mental disorders such as depression and anxiety are highly treatable illnesses, this raises the possibility that their symptoms are not being identified and treated adequately. Qualitative research suggests that stigma, practical barriers, and issues related to gender roles such as emotional and economic dependence limit immigrant women’s abilities to access postpartum mental health services. 28 Small surveys and studies restricted to specific immigrant populations suggest that postpartum mental health services are indeed being underused. 29 –31 However, information about the extent to which immigrant women use postpartum mental health services on a population level is lacking.
The main purpose of this study was to describe the proportion of immigrant women to Ontario, Canada, who used mental health services within the first postpartum year, with comparison to a referent group of women who were either born in Canada or were long-term residents of Canada, having lived in Ontario or another Canadian province since at least 1985.
Methods
Study Design
This was a population-based cohort study among female residents of Ontario, Canada, who delivered a live infant between April 1, 2008, and March 31, 2012. Outcomes were assessed up to 1 year from delivery for each woman, so the final follow-up date for the cohort was March 31, 2013. Ontario is Canada’s most populous province (population ∼13 million), and all residents receive universal health care benefits. Of relevance to the current study, this includes all antenatal, postnatal, and mental health care delivered by physicians in an outpatient setting as well as all hospital-based and emergency department care.
Data Sources
Data were accessed from the Institute for Clinical and Evaluative Sciences (ICES) in Toronto, Ontario, an independent nonprofit research organization that evaluates health care service utilization and their effectiveness in the province of Ontario, using a series of linked demographic and health administrative databases. At ICES, patient-level records are de-identified and linked with a unique identifier for each Ontario resident. To identify obstetrical deliveries, we used the MOMBABY data set, derived from the Canadian Institutes for Health Information Discharge Abstract Database (CIHI-DAD) that records all in-hospital obstetrical deliveries in Ontario (>98% of all deliveries in the province). 32 These data were linked to the Ontario segment of the Immigration, Refugees and Citizenship Canada (IRCC) database, which includes immigration records for all immigrants to Ontario since 1985. Information on postpartum mental health service utilization as well as past mental health and medical service utilization was obtained using physician billing claims for outpatient visits (Ontario Health Insurance Plan, OHIP), the National Ambulatory Care Reporting System (NACRS) for emergency department visits, and both the CIHI-DAD and the Ontario Mental Health Reporting system (that records information on all designated mental health admissions in the province) for inpatient hospitalizations. Limited funding is available in Ontario for private psychological services based on insurance coverage, but these services are not captured in our data sets. We also use the Registered Persons Database (RPDB), which contains information regarding sex, age, and postal code for all Ontario residents who have a provincial health care number for measurement of specific sociodemographic characteristics. The information in these data sources has been found to be complete and reliable, with excellent validity for primary diagnostic information in the emergency service and inpatient data sets. 33 –35 Physician billing claims are also complete and reliable with respect to the physician specialty and type of service provided, and the definition of mental health outpatient visits to a primary care provider used in the present study has been validated. 36 However, the validity of physician billing claims for specific diagnoses can be variable. The study received research ethics board approval from Sunnybrook Health Sciences Centre in Toronto, Ontario (ICES logged study: 2015 0904 321 000).
Participants
We considered all women who were residents of Ontario as of December 31, 2010, because this was the latest date for which IRCC data were available to classify women as immigrants versus long-term residents. Amongst this group, we identified all deliveries of a live-born infant between April 1, 2008, and March 31, 2012, using the MOMBABY data set (n = 527192). We excluded women younger than age 13 and older than age 55 at the time of delivery (n = 20) and those with an invalid health card number and/or those unable to be linked between databases (n = 66). For women who delivered more than once during the study period (n = 76484), we selected the first delivery for a total of 450622 unique women in the final cohort.
Immigration
The IRCC data set contains records for all immigrations since 1985, allowing us to classify all women in the cohort who immigrated to Canada from 1985 onward into the immigrant group. Women who met our inclusion criteria but did not appear in the IRCC data set were classified as long-term residents, as they were either born in Canada or would have immigrated to Ontario prior to 1985. Therefore, any foreign-born women classified into the long-term resident group would have lived in Canada for at minimum 23 years prior to the index birth for the current study (i.e., the first birth in the study was in 2008). Canadian data suggest that general health and health care utilization among immigrants approaches that of the general population by this time (and probably much earlier, at about 15 years from immigration). 37
Outcomes
Our primary outcome was mental health service utilization within 1 year postpartum, a standard time frame used in research and clinical practice for capturing postpartum mental disorders. 38 The primary outcome was defined as any of the following: 1) an outpatient ambulatory physician visit to either a psychiatrist (OHIP specialty code = 19) or a family physician for a mental health reason (using a validated algorithm requiring 1 mental health service code or a general service code with a mental health diagnostic code; sensitivity of 80.7%, specificity of 97%, and positive and negative predictive values of 84.9% and 96%, respectively, when applied in a primary care population in Ontario) 36 ; 2) an emergency department visit with International Classification of Diseases, 10th Revision, Canada (ICD-10-CA) codes in the primary diagnostic field for any psychiatric disorder, including addictions (F00-F99) or for a deliberate self-harm episode in any diagnostic field (X60-X84, Y10 to Y19, Y28) 39 ; or 3) a psychiatric inpatient admission to a designated mental health bed (Ontario Mental Health Reporting System [OMHRS] data set) or to a bed in an acute care hospital (as identified in CIHI-DAD) where the most responsible diagnosis (i.e., primary diagnosis) was for a mental health condition (ICD-10-CA: F00-F99). The latter includes psychiatric admissions to intensive care units after suicide attempts and psychiatric admissions to overflow medical beds, which are not captured in the OMHRS data set; these correspond to about 20% of psychiatric admissions in Ontario (source: ICES unpublished data). As secondary outcomes, we examined each type of service use separately.
Covariates
We considered covariates that could be considered either confounding factors or potential explanatory factors in the relationship between immigration status and postpartum mental health service use, based on previous postpartum mental health service use literature. We measured maternal age at delivery, parity, income quintile based on neighbourhood, and place of residence (urban vs. rural). 27 We captured pregnancy-related variables, including mode of delivery, infant sex, multiple versus singleton gestation, and selected newborn health complications, as well as extent and type of antenatal care received (i.e., obstetrician or family physician). 40,41 Medical comorbidity was measured by Johns Hopkins Adjusted Clinical Groups (ACG), 42 an approach to measuring morbidity using disease patterns in health administrative data, age, and gender. This system identifies individuals as falling into any of 11 possible major Ambulatory Diagnostic Groups (ADGs) characterizing different major medical conditions, 3 of which are considered psychosocial or mental health related. Individuals were categorized based on their health services utilization in the 2 years prior to pregnancy. The ADGs were summed to generate a comorbidity score that could range from 0 to 8 after excluding major ADGs associated with psychosocial issues. Prior mental health service use and diagnoses were captured using inpatient, emergency service, and outpatient data sets in the 2 years prior to the index delivery, allowing us to capture recent and active service use, including during pregnancy. Recent and active service use is one of the strongest predictors of subsequent use of mental health services in the postpartum. 43 We did not attempt to capture lifetime diagnoses of mental disorders given the variability in the number of years available per individual in the look-back period, especially given that we were not able to capture diagnoses given to immigrant women in their countries of origin. Within immigrant women, we also examined Canadian language ability, education level and marital status at the time of immigration, immigration class (i.e., refugee or nonrefugee), region of origin, and time since immigration. These variables were extracted from the IRCC data set and were therefore not available for the long-term resident referent group.
Analyses
Baseline participant characteristics are presented as means, medians, or proportions, and immigrant women were compared to long-term residents using summary statistics. Logistic regression was used to generate crude and adjusted odds ratios (aORs) and 95% confidence intervals (95% CIs) for the primary outcome and each of its components. Odds ratios were adjusted for age, parity, and other clinically significant differences between immigrant and nonimmigrant women observed in baseline characteristics that could be considered potential confounders in the relationship between immigrant status and postpartum mental health service use. We used SAS version 9.3 for Unix (SAS Institute, Cary, NC, USA). Cell sizes (i.e., the number of individuals who are in a certain category of a baseline or outcome variable) <6 were not reportable for privacy reasons under Ontario provincial regulations.
Results
There were 450622 women who had a live birth in Ontario during the study period, of whom 123231 (27%) were immigrant women. Compared to long-term residents of Ontario, immigrant women were more likely to be multiparous and to reside in urban and low-income areas (Table 1). Prior to delivery, fewer had used mental health services, and they appeared to be in slightly better medical health. During their pregnancies, they were the most likely to receive antenatal care shared between an obstetrician and family physician, whereas long-term residents were more likely to receive care solely from family physicians or to receive nonphysician (i.e., midwife) care. More than half of immigrant mothers were originally from Asia, and more than one-third had immigrated within the preceding 5 years (Table 2). Almost 60% of immigrant women were married, and almost 75% had more than 10 years of schooling at the time of immigration, but about 36% spoke neither English nor French upon arrival. About 13% were refugees.
Baseline Characteristics of Immigrant Women and Long-Term Female Residents of Ontario Who Delivered a Live-Born Child between 2008 and 2012.a
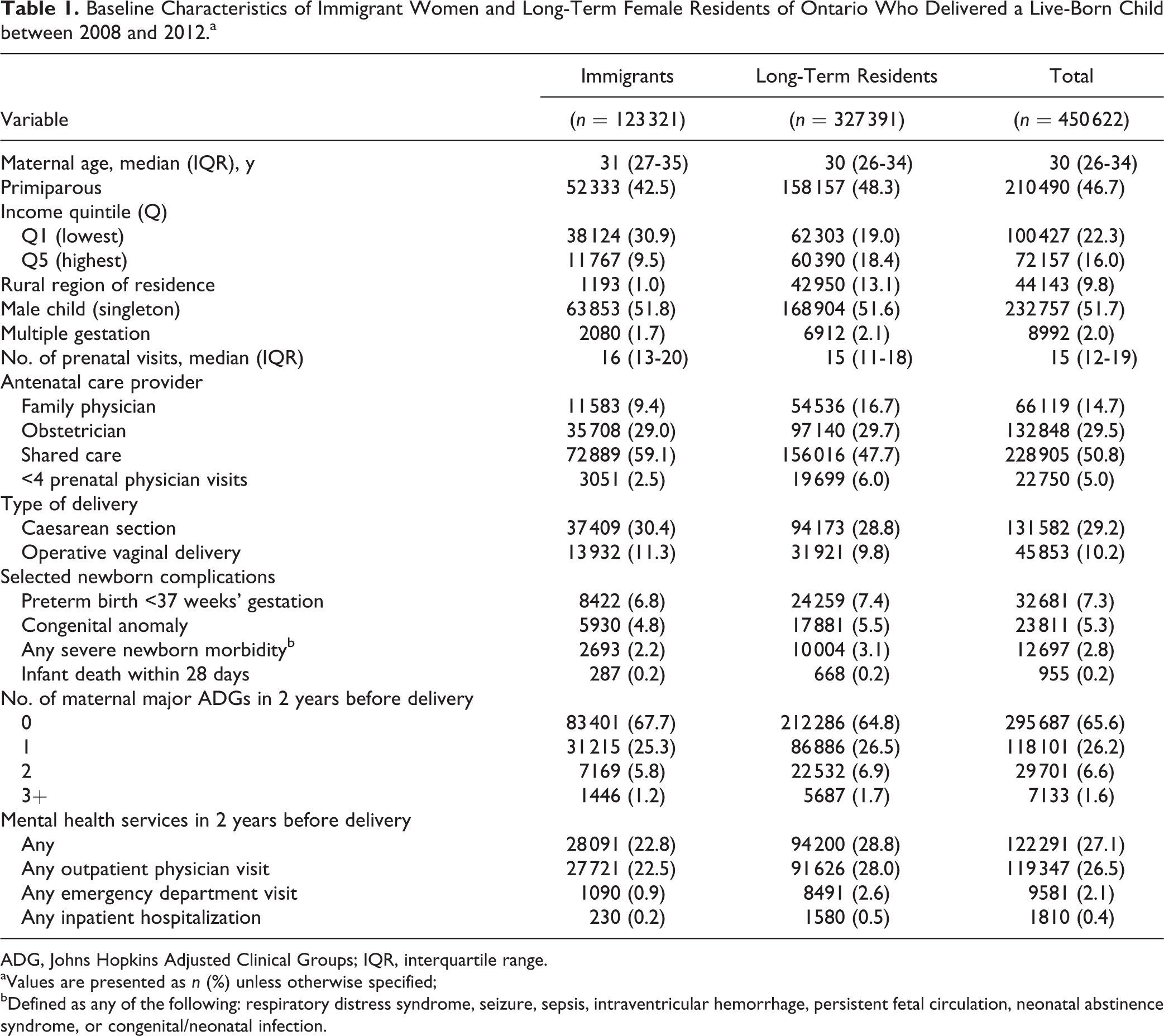
ADG, Johns Hopkins Adjusted Clinical Groups; IQR, interquartile range.
aValues are presented as n (%) unless otherwise specified;
bDefined as any of the following: respiratory distress syndrome, seizure, sepsis, intraventricular hemorrhage, persistent fetal circulation, neonatal abstinence syndrome, or congenital/neonatal infection.
Immigration Characteristics of 123 231 Immigrant Mothers in Ontario.a
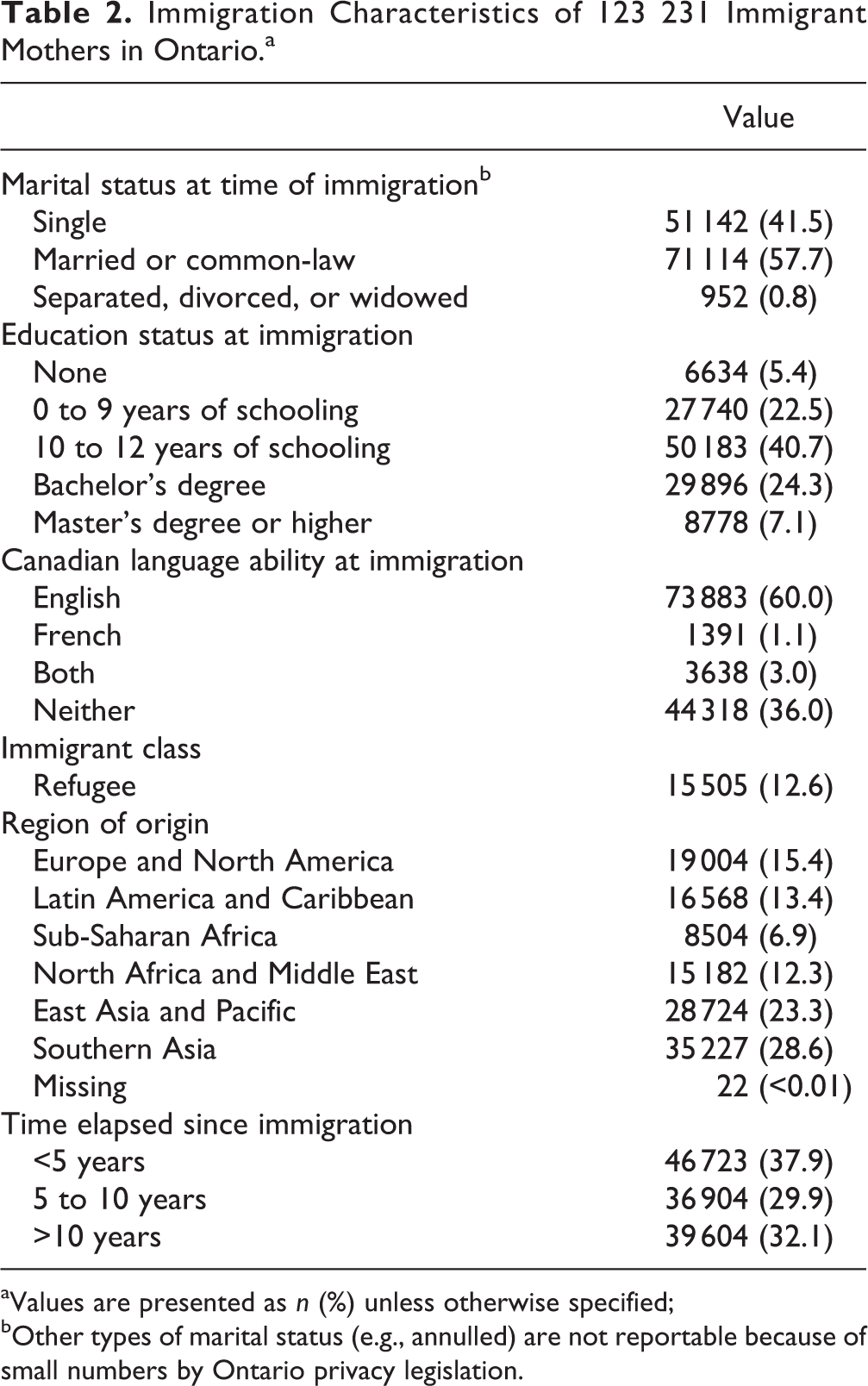
aValues are presented as n (%) unless otherwise specified;
bOther types of marital status (e.g., annulled) are not reportable because of small numbers by Ontario privacy legislation.
Overall, 19.4% of women in the cohort used any mental health service within 1 year postpartum (n = 87478 women). This was mostly accounted for by visits to primary care providers and psychiatrists (n = 86173, 19.1%), but some women also or uniquely used emergency department psychiatric services (n = 4891, 1.1%) and/or were hospitalized on an inpatient unit for psychiatric reasons (n = 1313, 0.3%). Some women received more than one diagnosis over time, with the majority of diagnoses being for anxiety and depressive disorders (n = 77025, 17.1% of the cohort), followed by bipolar disorder (n = 18838, 4.2%), substance and alcohol use disorders (n = 6881, 1.5%), and psychotic disorders (n = 1208, 0.27%).
Immigrant women were much less likely to use postpartum mental health services compared to long-term residents of Ontario (14.1% vs. 21.4%; crude OR, 0.60; 95% CI, 0.59 to 0.61) (Table 3). This did not change after adjustment for covariates (aOR, 0.59; 95% CI, 0.58 to 0.61). Similar observations were found for outpatient physician mental health visits (aOR, 0.59; 95% CI, 0.59 to 0.61) and for mental health emergency department visits (aOR, 0.63; 95% CI, 0.57 to 0.68). While immigrant women were less likely to require postpartum psychiatric hospitalization (0.20% vs. 0.33%; crude OR, 0.61; 95% CI, 0.54 to 0.71), the difference was not statistically significant after adjustment for covariates (aOR, 0.92; 95% CI, 0.79 to 1.06).
Mental Health Service Utilization Within 1 Year Postpartum.
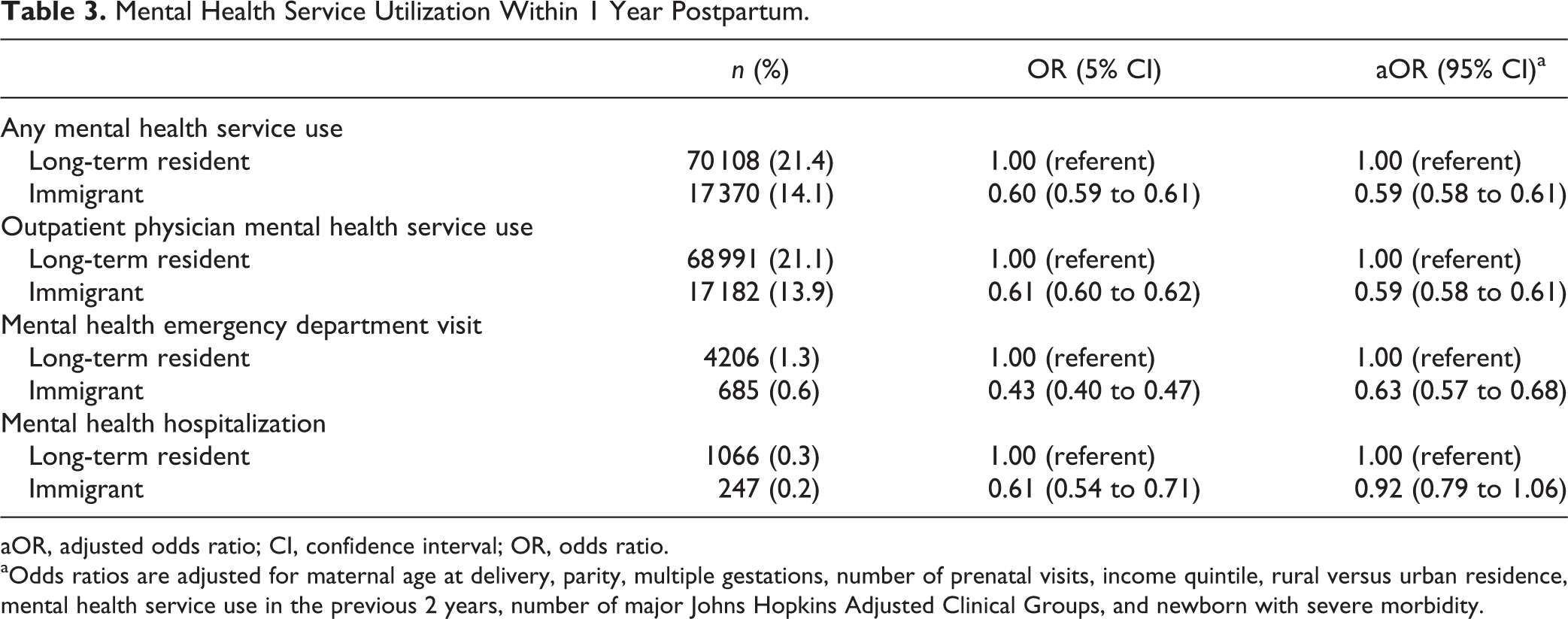
aOR, adjusted odds ratio; CI, confidence interval; OR, odds ratio.
aOdds ratios are adjusted for maternal age at delivery, parity, multiple gestations, number of prenatal visits, income quintile, rural versus urban residence, mental health service use in the previous 2 years, number of major Johns Hopkins Adjusted Clinical Groups, and newborn with severe morbidity.
Discussion
This study found that immigrant women in Ontario, Canada, were almost 40% less likely to use postpartum mental health outpatient physician services compared to long-term residents of the province. This difference was not explained by other sociodemographic characteristics, pregnancy-related characteristics, or differences in psychiatric history. Immigration was not independently associated with risk for psychiatric hospitalization, the most intensive form of mental health service use.
To our knowledge, this study is unique in its focus on postpartum mental health service use by immigrant women at a population level. Overall postpartum mental health service use rates were consistent with Canadian and international estimates for use of outpatient, emergency, and inpatient services in the postpartum period. 44 –46 The finding that immigrant women were 40% less likely to use postpartum mental health service fits with existing literature that demonstrates low mental health service utilization among immigrants. 47 –51 Extensive research suggests that immigrant women are much more likely than nonimmigrants to suffer from postpartum mental disorders, so we do not believe lack of need explains the lower service use. 13,14,27 The observed sociodemographic characteristics of immigrant women in our sample further support this hypothesis. Immigrant women in our sample were more likely to be low income and live in urban areas, both of which have been shown to increase risk for postpartum mental disorders in our own work in Canadian populations. 27 They were also more likely to be multiparous, possibly increasing risk for childcare stress. This would also suggest that they are at higher risk for postpartum mental disorders compared to long-term residents. It is possible that immigrant women in our sample were preferentially accessing informal postpartum mental health supports, such as family, friends, clergy, or community-specific supports that were not captured in our data sets. However, given Canadian population-based survey data that report substantially reduced social support among immigrant women, this explanation is unlikely. 52
Stigma has been identified as a barrier to mental health service use in non-perinatal immigrant groups 53,54 and was also cited as a barrier to seeking mental health services in the postpartum among immigrant and first-generation women in several small studies. 29,30 Most immigrants in our study were from Asian countries, where women are less likely to disclose mental health symptomatology. 55 In fact, because of this issue, it has been suggested that the threshold for detection of postpartum depressive symptoms on standard scales such as the Edinburgh Postnatal Depression Scale (EPDS) be lowered for Chinese mothers. 55 Structural barriers associated with decreased mental health service use among immigrants identified in other studies include language barriers, high cost, and different cultural norms around service use. 56 –58 In the context of the Canadian health care system, where the cost of ambulatory mental health care is covered through public health insurance, cost is unlikely to be a barrier. Yet economic marginalization could be a factor that limits service utilization due to transportation costs or childcare—and 30% of immigrant women in our sample lived in the lowest income neighborhoods in the province. In addition, skepticism and distrust of Western medicine have also been acknowledged as reasons for lower mental health service use among immigrants and refugees to developed countries. 53,57,59 Of potential importance for future research is our finding that immigrant women were less likely to receive antenatal care solely from a primary care provider or nonphysician (i.e., a midwife). In these health care settings, the close follow-up provided after delivery by the health care provider might increase the detection of mental illness and facilitate referral for and uptake of mental health care.
The strengths of this study include the use of a population-based sample of immigrant women such that almost all immigrant women in our jurisdiction were captured, as well as the complete coverage of physician-based, emergency department, and hospital-based mental health services available using our linked health administrative data sets. Several study limitations are of note. The referent group for these analyses is heterogeneous and possibly includes non-Canadian-born women who immigrated prior to 1985, the earliest date of our immigration records. However, with the first cohort birth in 2008, this would mean that any non-Canadian-born women classified into the referent group would have been living in Canada for at least 23 years. Canadian data show that both general health and health care utilization among immigrants approach that of the general population by this time, and probably much earlier, at about 15 years from immigration. 37 As such, a referent group of long-term residents remains appropriate for understanding health service use patterns of immigrant women. Furthermore, since any misclassification of immigrant women into the referent group would bring the health service utilization of the referent group closer to that of the immigrant exposure group (i.e., bias toward the null), then observed differences in our study are likely to underestimated, not overestimated, if there is such a bias at play. Because we used health administrative data, we could measure mental health services that were used (and for which diagnoses) but could not directly measure what proportion of postpartum mental health needs were going unmet or were being met through the private system (e.g., psychologists), in the community (e.g., postpartum support groups delivered by public health nurses), or through informal networks or relationships. Our inability to measure these supports and services, however, is unlikely to explain the observed differences in utilization between immigrant women and the referent group since Canadian population-based survey data demonstrate that postpartum immigrant women report receiving significantly less social support than Canadian-born women. 52 Additional limitations include limited availability of individual-level covariates that could help explain the relationship between immigration status and postpartum mental health service use, such as marital status, education, and perceived social support.
Conclusion
Our findings are of importance given recent evidence that immigrant women are at 2-fold risk for postpartum mental disorders, even in studies measuring symptoms late into the first postpartum year. 13,27 With a high proportion of births in developed countries being to immigrant women, attention to services and supports that optimize engagement of immigrant mothers with acceptable and effective postpartum mental health services is warranted. Postpartum mental health care research still lacks a full understanding of the influence of cultural factors, social support, and institutional structures on help-seeking behaviours and access to mental health services. 28 Future research can focus on identifying specific populations of immigrant women at risk for underusing postpartum physician health services, as well as understanding the barriers and facilitators of mental health service utilization within those groups that can be addressed in efforts to reduce the burden of postpartum mental disorders on mothers, children, and families.
Footnotes
Authors’ Note
This article was presented as an Abstract Poster Presentation at the 2015 CAPE Annual Scientific Symposium, Vancouver, BC, September 2015. It was also presented as part of a plenary presentation at the 2nd Bienniel Perinatal Mental Health Meeting, Chicago, Illinois, November 2015.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received support from the Institute for Clinical Evaluative Sciences (ICES), which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care (MOHLTC). The opinions, results, and conclusions reported in this article are those of the authors and are independent from the funding sources. No endorsement by the ICES or the Ontario MOHLTC is intended or should be inferred. Parts of this material are based on data and information compiled and provided by Canadian Institutes for Health Research (CIHI). However, the analyses, conclusions, opinions, and statements expressed herein are those of the author and not necessarily those of CIHI.