
Abstract
Objectives:
To explore psychological distress levels, using the validated Kessler 6 (K6), as well as the relationship between demographics and K6 scores, and incidence of mental health crises in a cohort of community-dwelling people living with severe and persistent mental illness (SPMI).
Methods:
People living with SPMI taking antipsychotic or mood stabiliser medications were recruited from Australian community pharmacies between September 2020 and Februrary 2021 and completed an electronic survey, including the K6 scale. Pharmacists were interviewed and supplied written reports with details of the consultation when participants obtained ‘very high’ (⩾19/30) K6 scores. Records were reviewed and coded by an independent coder. Multivariate linear regression was used to determine predictors of K6 scores.
Results:
The median K6 score was 16/30 (IQR = 11,21; range = 6–30). Younger age, unemployment and multimorbid mental health diagnoses were significant predictors of higher K6 scores (p < .01; R2 = .24). Fifty-nine (39.3%) consumers scored ⩾19, of which 25/59 (42.4%) were reported to be exhibiting signs of psychological distress and none were experiencing mental health crises.
Conclusion:
People living with SPMI have high levels of psychological distress as measured by the K6. Further work is needed to understand the prevalence, extent, precipitating factors and impact of psychological distress in people living with SPMI.
Introduction
People living with severe and persistent mental illnesses (SPMI), including but not limited to schizophrenia, schizoaffective disorders, bipolar disorder and severe depression, may be susceptible to experiencing higher levels of psychological distress (Chittleborough et al., 2011). Higher levels of distress among people living with SPMI may be a result of managing mental illness and co-morbidities, complex medication regimens, stigma and social disconnect from their support networks and society. These factors were exacerbated during the novel coronavirus (COVID-19) pandemic, which diminished social contact and restricted access to members of the healthcare team, including general practitioners (GPs; family physicians) and psychiatrists (Muruganandam et al., 2020; Xiong et al., 2020).
Increased levels of psychological distress could potentially indicate worsening of SPMI and have been associated with increased mortality rates (Pratt, 2009; Puustinen et al., 2011). This risk of increased mortality is of particular concern in the SPMI population, who are at greater risk of premature death, not only by suicide, but also due to physical comorbidities such as complications of cardiovascular and respiratory diseases and diabetes (Liu et al., 2017). For example, in Australia the life expectancy gap between individuals living with SPMI and the general population is estimated to be between 14 and 23 years (National Mental Health Commission, 2016). The increased mortality in the SPMI population is driven by factors including higher rates of smoking and substance use, poor medication adherence, medication side effects and diagnostic overshadowing by treating practitioners (Jones et al., 2008; Liu et al., 2017; National Mental Health Commission, 2016).
The Kessler Psychological Distress Scale (K6) is a 6-item psychometrically valid instrument commonly used to both screen for, and measure the severity of, non-specific psychological distress; a diverse group of signs and symptoms that may be present among people living with a range of mental illnesses or experiencing distressing life events (Kessler et al., 2002). The K6 is an abbreviated version of the Kessler-10 (K10) and consists of six items rated on a 5-point Likert scale (1 = ‘None of the time’ to 5 = ‘All of the time’). Each of the six items begins with same item stem enquiring about feelings over the last month (i.e. ‘During the last 30 days how often did you feel. . .’). There is guidance for the use and scoring of the K6 in an Australian context, whereby the minimum and maximum scores are 6 and 30, respectively, with higher scores indicating higher levels of psychological distress (Australian Bureau of Statistics [ABS], 2012). The K6 has been used in multiple national and international health surveys as well as to screen for levels of distress after natural disasters such as Hurricane Katrina and the 2011 earthquake in Japan (Furukawa et al., 2003; Kessler et al., 2008; Pirraglia et al., 2011; Tachibana et al., 2014).
Although the K6 has primarily been used for screening general populations (Furukawa et al., 2003; Kessler et al., 2003, 2010), it has potential application in screening for psychological distress in a population already diagnosed with mental illness (Sunderland et al., 2012). Consequently, the objectives of this study were to explore K6 scores, in a cohort of community-dwelling individuals diagnosed with SPMI across three Australian regions, determine the incidence of pharmacist-reported distress and mental health crises among people scoring ‘very high’ on the K6 (⩾19/30), and to explore the relationship between K6 scores and participant demographics, including age, gender and multimorbid mental illnesses.
Methods
Ethics approval
This study was approved by Griffith University Human Research Ethics Committee (HREC/2019/473).
Participants and setting
Consumer participants were recruited through community pharmacies as part of the Bridging the Gap Between Physical and Mental Illness (PharMIbridge) Randomised Controlled Trial (RCT) between September 2020 and February 2021. Detailed inclusion criteria for pharmacies and consumers are reported elsewhere (Wheeler et al., 2020). For the purpose of the RCT, consumer participants were eligible if they were: (1) aged 16 years or older and living in the community; and (2) had at least a 6-month history of use of an antipsychotic or mood stabiliser (such as lithium, carbamazepine and valproate) for the treatment of SPMI; and (3) had complex medication needs (for example, managing multiple medications or experiencing adverse effects of medications) or unmanaged physical health issues (e.g. weight gain). The first 150 consumer participants who consented to participate in the RCT were selected as a convenience sample for the study described in this manuscript.
Community pharmacies represented in this sample (n = 28 of 51 included in the RCT) were located across three regions of Australia (in order of progressive RCT rollout: Australian Capital Territory (ACT), Hunter New England, New South Wales (HNE) and regional Victoria (VIC)). All participating community pharmacists received training in study processes, including K6 use and scoring, as well as Mental Health First Aid training (Mental Health First Aid Australia, 2022) if they did not have current Mental Health First Aid accreditation, thereby enabling pharmacists to recognise and assess for mental health crises and assist consumers when needed, such as by referring the person to a medical practitioner, recommending appropriate supports and resources or seeking assistance from a mental health crisis team if the person was experiencing a mental health crisis.
Survey instrument (K6) and data collection
After providing informed consent, consumer participants were asked to complete an electronic survey as part of baseline data collection for the PharMIbridge RCT. The survey consisted of various validated and purpose-designed measurement instruments to collect data pertaining to consumer participant demographics, health and wellbeing, including quality of life, multimorbidity treatment burden, substance use and self-reported medication adherence, for the purpose of evaluating the impact of the PharMIbridge intervention (Wheeler et al., 2020). These findings will be reported elsewhere. The survey also consisted of mandatory questions to measure psychological distress using the K6. Scores of 19 or above were classified as being ‘very high’; derived from the Australian Bureau of Statistics (2012) K6 scoring guide (upper category for dichotomous grouping and two highest strata for polychotomous grouping). The primary aim of using the K6, as a component of baseline RCT data collection, was to determine whether potential consumer participants were experiencing distress in response to mental health crises, and needed immediate medical referral as per the published RCT protocol (Wheeler et al., 2020). The K6 was selected due to its brevity, validity and reliability in measuring psychological distress. K6 scores were flagged to pharmacists in clinical software to trigger the pharmacists to follow up with consumer participants scoring ‘very high’.
Research team members (SED, SM, JC and COR) monitored the incoming K6 data on a weekly basis as participants completed the baseline survey and directly contacted pharmacists by telephone whenever a consumer participant scored 19 or higher (‘very high’) on the K6. Detailed research notes were made by team members during these phone calls. The purpose of these phone calls were to: (1) discuss the score with the pharmacist; (2) assess whether the consumer was showing signs and symptoms of psychological distress and/or a mental health crisis (e.g. suicidal ideation and acute psychotic episode) and determine whether the consumer participant was well enough to continue to participate in the PharMIbridge RCT; (3) support and advise the pharmacist when needed; (4) discuss precipitating factors, and any ongoing care provided by the pharmacist and (5) ask the pharmacist to submit a written report using a research template provided to them, documenting their discussion with the participant, whether a support person, such as a carer or family member, was present during the consultation and any follow-up action/s taken. Research team members reviewed each submitted written report to identify if further actions were required to provide remote support to the pharmacist working with the consumer participant.
Data analysis
Data were imported into IBM SPSS V27.0 (IBM Corp, Armonk, USA) for analysis. Continuous variables (age, K6 score) were assessed for normality and reported using means and standard deviations (SD) for normally disturbed data or medians and interquartile ranges (IQR) for non-normally distributed data. Categorical variables (gender, highest level of completed education, employment status, self-reported mental illness and physical illness diagnoses) were reported as frequencies and percentages. Due to incomplete data for self-reported physical illnesses in this sample, a univariate linear regression model of comorbid (two or more) physical health conditions was initially produced to determine if this was predictive of K6 score. Age, gender, education level, employment status and comorbid (two or more) mental illness diagnoses were block entered into a multivariate linear regression model to determine if any of these characteristics were predictive of K6 score in this sample. Tolerance and variance inflation factors (VIF) were examined to assess for collinearity of independent variables.
A member of the research team (RN), who is a Mental Health First Aid-accredited pharmacist, independently assessed both written records, that is, the written records of the documented telephone interactions between the research team and pharmacists, as well as the distress reports provided by the pharmacists for all consumer participants with K6 scores ⩾19. The two records were reviewed for each participant and key variables were coded by the independent assessor: signs of psychological distress (e.g. stress, worry, feelings of anxiety or low mood, crying and explicitly stating distress) and signs of mental health crisis (e.g. expressing suicidal ideation or signs of acute psychosis), follow-up actions taken by pharmacists and potential precipitating factors. Precipitating factors were identified by a content analysis of the two written records and categories were derived inductively (Kyngäs, 2020). To determine accuracy in coding, a 50% random sample of records was independently coded (included distress, crisis, follow up actions and precipitating factors) by a second member of the research team (JC) who is also a MHFA-accredited pharmacist. Cohen’s kappa was calculated between the two coders to determine the level of interrater agreement for signs of psychological distress and/or crisis. Discrepancies were discussed with a third member of the research team (SED; a qualified MHFA instructor) to reach consensus on coding.
Results
Participant characteristics
Consumer participants’ demographics and number of self-reported physical health conditions are reported in Table 1. Consumer participants (n = 150) had a mean age of 47.72 years (SD = 13.47; range 17.96 – 81.72) and were predominantly female (n = 85, 56.7%). Fifty-four (36.0%) consumer participants reported participating in full-time, part-time or casual employment, while the remainder (n = 96, 64.0%) were not engaged in paid employment (e.g. studying, disability pension and volunteer work). Consumer participants most frequently reported Year 12 (High School) or lower as their highest level of education (n = 69, 46.0%), followed by a Certificate or Diploma (n = 43, 27.7%) and an Undergraduate or Postgraduate Degree (n = 38, 25.3%). Self-reported mental and physical illness diagnoses are shown in Table 2. The most frequently self-reported diagnosis was moderate to severe depression (n = 93, 62.0%), followed by moderate to severe anxiety (n = 70, 46.7%) and bipolar disorder (n = 69, 46.0%). More than two-thirds of consumer participants (n = 103, 68.7%) reported living with two or more co-morbid mental illness diagnoses (range: 1–7). More than half (n = 121, 61.1%) of consumer participants reported living with two or more physical health conditions, while 18.7% (n = 37) reported living with one physical illness. The presence of chronic health conditions in the remaining participants (n = 40, 20.2%) was not self-reported.
Consumer participants’ demographics (n = 150).

Participating in paid full-time, part-time or casual employment.
Consumer participants’ self-reported mental and physical illness diagnoses (n = 150).
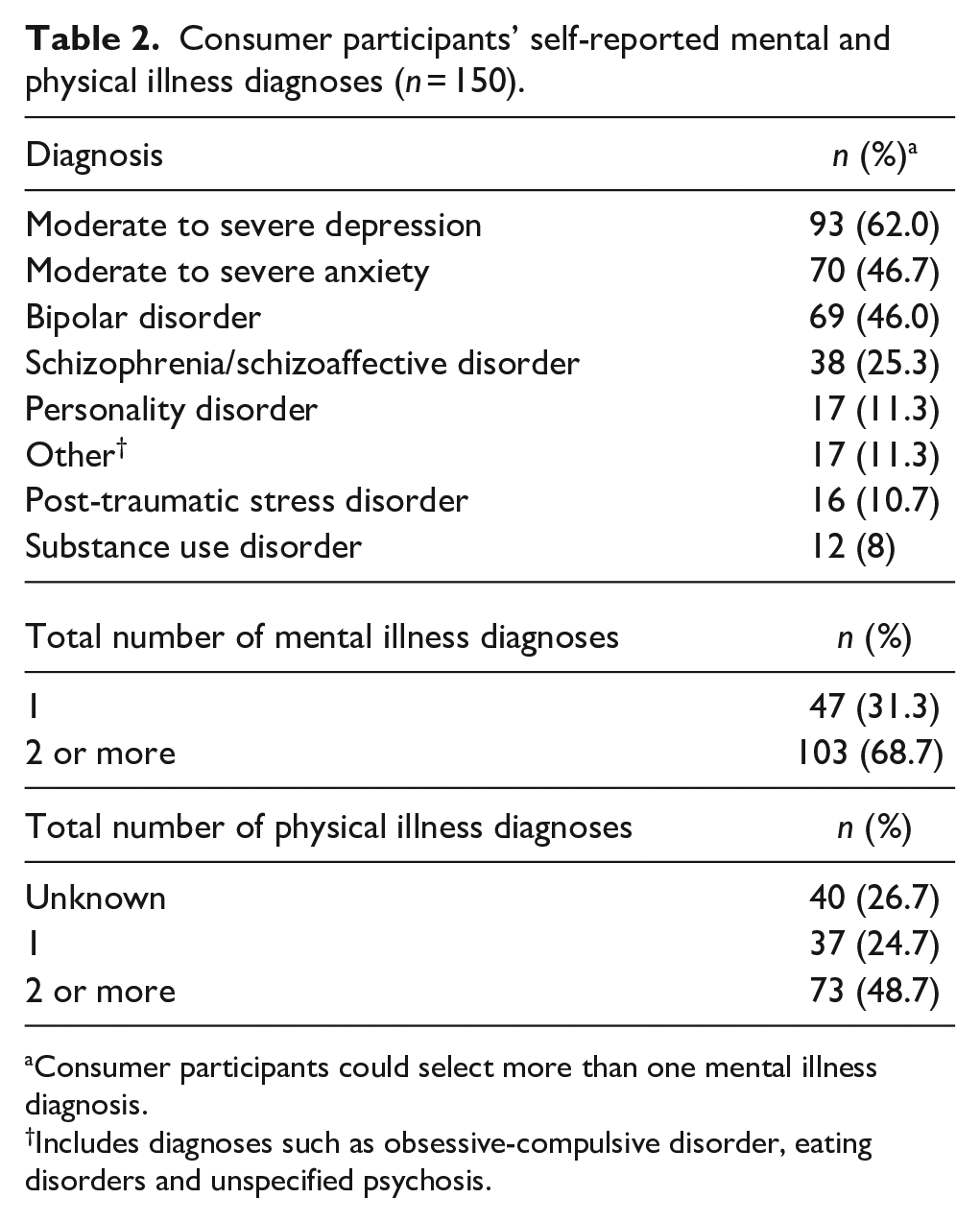
Consumer participants could select more than one mental illness diagnosis.
Includes diagnoses such as obsessive-compulsive disorder, eating disorders and unspecified psychosis.
K6 scores and associated factors
K6 scores ranged from the lowest possible score of 6 to the highest possible score of 30. The median K6 score was 16 (IQR = 11, 21). More than one-third of consumer participants (n = 59, 39.3%) scored 19 or higher, indicating potentially ‘very high’ levels of psychological distress. The distribution of scores using the Australian Bureau of Statistics polychotomous classification is presented in Table 3.
Distribution of Kessler-6 scores (n = 150).
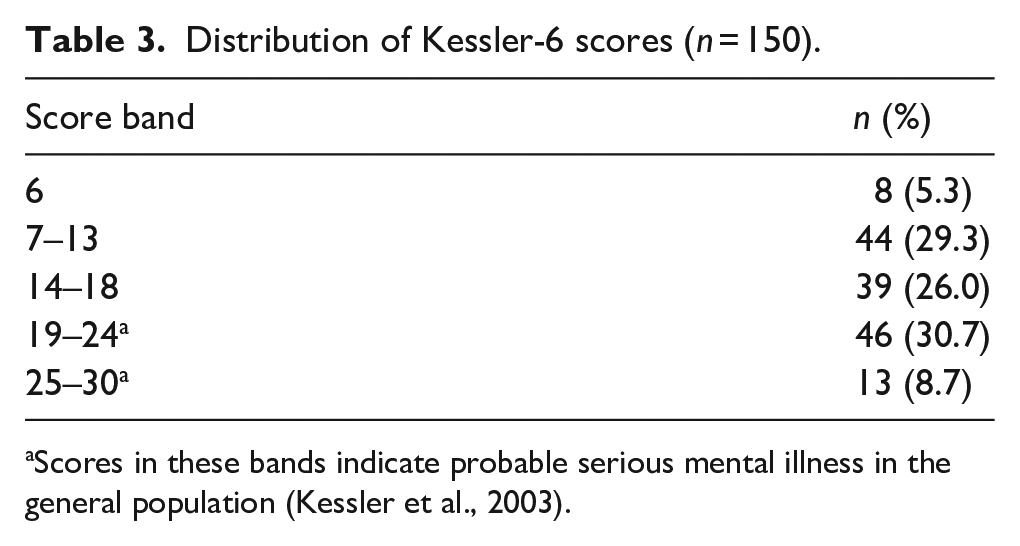
Scores in these bands indicate probable serious mental illness in the general population (Kessler et al., 2003).
The univariate regression model of multimorbid physical health conditions was not significant (p ⩾ .05) and this variable was therefore excluded from the multivariate model. A multivariate linear regression model (Table 4) including age, gender, level of education, employment status and multimorbid mental illness diagnoses returned an R2 value of .24 (F(5, 144) = 10.391; p < .001), accounting for approximately 24% of variance in score. Age (β = −.359; p < .001), participation in paid employment (β = −.248; p = .002) and multiple mental illness diagnoses (β = .261; p = .001) were significantly predictive of K6 score; indicating a positive association between two or more comorbid mental health diagnoses and K6 score and a negative association between paid employment and increasing age and K6 score. No collinearity was observed between independent variables (tolerance range: 0.789–0.991; VIF range: 1.009–1.268).
Consumer participants’ characteristics predicting Kessler-6 scores (linear regression output, n = 150, R2 = .24).
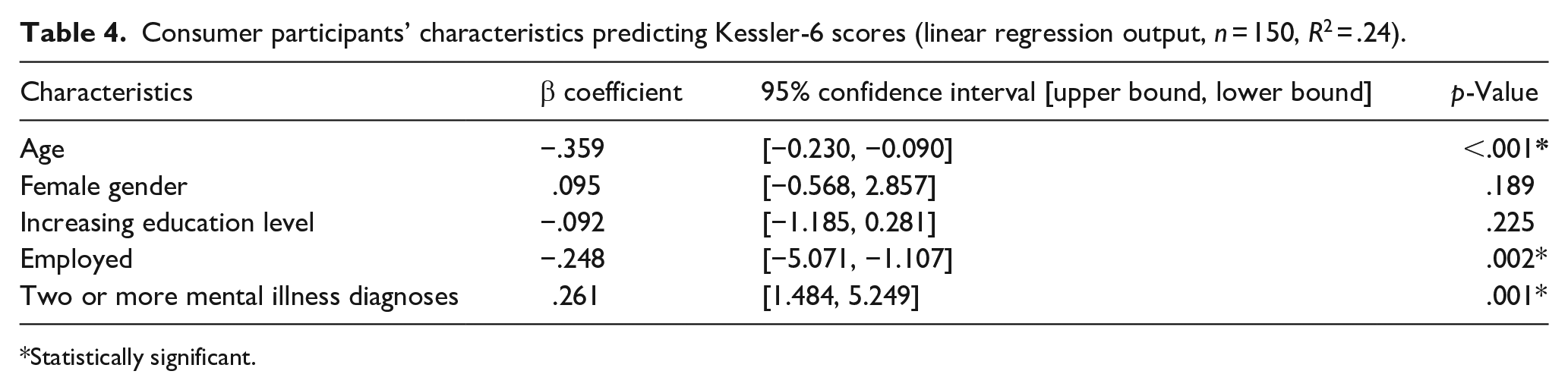
Statistically significant.
Pharmacist-reported psychological distress and mental health crises
Of the 59 consumer participants who scored 19 or higher on the K6, 25 (42.4%) consumer participants were exhibiting signs of psychological distress, such as crying or reporting to be highly stressed and anxious, but not an acute mental health crisis as determined by independent review and coding of pharmacists’ distress reports and documentation of telephone calls with pharmacists. The remaining 34 consumer participants (57.6%) were not reported to be exhibiting obvious signs of distress or crisis and were reported as presenting as their usual self at the time they met with the pharmacist for baseline data collection. The level of interrater agreement between the two research team members for the audited sample (n = 29) was ‘almost perfect’ (Cohen’s kappa = .861, p < .001) for distress and perfect (nil discrepancies) for crisis (Landis & Koch, 1977).
Where signs of psychological distress were reported (n = 25), the precipitating factors identified by independent coding included (may include more than one for each participant): family/personal circumstances (e.g. breakdown in relationship with family members, loss of employment, recent death in the family; n = 7, 28.0%); change in medicines or adverse effects of medicines (n = 6, 24.0%); substance use (n = 2, 8.0%); breakdown in relationship with doctor (n = 1, 4%); and recent suicide attempt (n = 1, 4.0%). For 10 consumer participants (40.0%) no precipitating factors were identified by the independent coder.
When asked to document the follow-up actions undertaken in response to consumer participants with Kessler scores ⩾19 in the written distressed participant reports, pharmacists most commonly reported taking no specific actions and continuing to provide usual care (n = 53, 89.8%), followed by contact with/referral to a psychiatrist (n = 3, 5.1%), GP (n = 2, 3.4%) or employment agency (n = 1, 1.7%).
Discussion
The findings of this study demonstrate that more than one-third of a community-dwelling sample of consumer participants living with SPMI obtained K6 scores indicating ‘very high’ levels of psychological distress. Of these consumer participants, approximately 40% were exhibiting signs of psychological distress during consultations as determined by independent coding of two written records. Personal events and medication-related changes and adverse events were the most common precipitating factors identified by the independent coder. However, most consumer participants who scored very high on the K6 presented as they usually would with no obvious signs of distress or need for concern, indicating that elevated levels of psychological distress may be a consistent experience for many who live with SPMI. This study identified that all consumer participants scoring in the very high distress range of the K6 were not reported to be experiencing mental health crises, such as suicidal thoughts or acute psychotic episodes, at the time of the consultation.
While feelings of distress are characteristic of poor quality of life among people experiencing mental health problems, indicators of good quality of life include feelings of being in control of one’s own distressing symptoms (Connell et al., 2012). People experiencing mental health symptoms often report experiencing distress due to these symptoms, which may include hallucinations, delusions and agitation (Connell et al., 2012). In this study, all participating consumers were living with SPMI, indicating that they had experienced symptoms of a mental illness for an extended period as a key inclusion criterion was that they had been receiving at least 6 months of treatment with a mood stabiliser or antipsychotic medication. The study findings demonstrate that most consumers who scored in the ‘very high’ distress range did not present to the pharmacy differently to how they usually would according to pharmacists, and pharmacists did not report recognising any signs of distress when interacting with them, despite discussing their distress specifically during these consults because of the K6 scores obtained. Consequently, further work is warranted to investigate the sensitivity and specificity of the K6 scale in identifying psychological distress in the SPMI population.
Psychological distress can occur because of a range of precipitating factors, which impact individuals. However, study findings demonstrate that even among those who had visible signs of distress during consults with pharmacists, 40% did not report experiencing any precipitating factors. The DSM-V diagnostic criteria for mental illnesses, such as major depressive disorder, highlight the need to consider symptoms that may resemble mental illness symptoms but are accounted for by ‘normal responses’ to stressful events, such as loss, and to determine whether the person is experiencing ‘clinically significant distress or impairment in social, occupational or other important areas of function’ (American Psychiatric Association, 2013). These specified criteria indicate the need to recognise that the distress associated with living with a mental illness is ‘disproportionate to external stressful situations’ (Horwitz, 2007). Hence, for the majority of consumers living with SPMI distress may be intrinsic to living with their illness and not a reaction to external stressful events, in line with the understanding in the literature that distress associated with mental illness is persistent even in the absence or resolution of external stressors (Horwitz, 2007). In fact, this study demonstrates that psychological distress, as measured by a validated tool, was common among this population, in the absence of external stressors, which is not surprising given that all consumer participants self-reported being diagnosed with and receiving treatment for a SPMI.
Australian data published in 2018 indicated approximately 13% of the general population was scoring in the high/very high bands of the K10 (ABS, 2018). Consumer participants in this study reported higher levels of distress on the K6 if they were younger, unemployed or were living with multiple mental illness diagnoses. Similarly, 32.9% of adults living with disabilities in the US report mental distress, and mental distress was found to be higher among people living with co-morbidities or more than one type of disability, and those of younger age (Cree et al., 2020). These findings are also corroborated by a recent Italian study (Saita et al., 2021) and a systematic review which demonstrates that younger age and unemployment are associated with increased levels of distress, particularly during the COVID-19 pandemic (Xiong et al., 2020). Poor mental health has been associated with rates and duration of unemployment (Butterworth et al., 2012), and given that this is likely to contribute to distress levels, further consideration is needed on how to best to address employment issues in this population. Although younger age, unemployment and comorbid mental illnesses were associated with higher levels of psychological distress in the current study, it is interesting to note that female gender was not associated with K6 scores. This is in distinct contrast to previous Australian and international data which shows that female gender is associated with higher Kessler scores (ABS, 2018; Rahman et al., 2020; Xiong et al., 2020). Hence, further research exploring this association and potential reasons for difference across samples is warranted.
It is possible that the ongoing COVID-19 pandemic may have contributed to the levels of distress measured with the K6 in this sample as there have been reports of increased psychological distress in the general population during the pandemic, particularly during the early months (Pierce et al., 2020; Xiong et al., 2020). Furthermore, self-reported mental illness was associated with higher K10 scores in a 2020 Australian survey conducted during the pandemic (Rahman et al., 2020). The COVID-19 pandemic may have contributed to a worsening of psychiatric symptoms among consumer participants in this and other studies among the SPMI population (Kahl & Correll, 2020), which may have also resulted in elevated levels of distress. The pandemic may have impacted the ability of people living with SPMI to receive the continuous inpatient and outpatient care they need, further adding to distress and increasing the risk of mental illness relapse (Kahl & Correll, 2020). Moreover, COVID-19 outbreaks and the associated isolation and lockdowns may also have contributed to feelings of fear and stress (Sukut & Ayhan Balik, 2021). Research exploring the impact of COVID-19 on people living with SPMI in India reported that 80% of consumers had missed mental health appointments and 22% had been nonadherent to their psychotropic medications citing lack of availability of medications and health professionals, as well as lockdown and relapse of mental illness as reasons for non-adherence (Muruganandam et al., 2020). The effects of recent natural disasters may also have contributed to the elevated scores seen in this sample as some consumer participants were from regions affected by the 2019 to 2020 Australian bushfires. Elevated rates of mental health problems have been observed following previous bushfires in Australia (Bryant et al., 2017), while studies conducted in the United States after Hurricane Katrina and Japan after the 2011 earthquake demonstrated that distress levels increased after these events compared to distress levels reported prior to these disasters (Kessler et al., 2008; Tachibana et al., 2014). This highlights that while specific precipitating factors were not identified for a large proportion of consumer participants scoring very high on the K6 scale in the current study, significant events (i.e. the COVID-19 pandemic and Australian bushfires) at the time of the study may have contributed to distress levels.
This study adds to the growing body of evidence pertaining to primary care providers’ roles in mental healthcare. As evidenced by this study, and others (Chan et al., 2008; McMillan et al., 2018; O’Reilly et al., 2015; Uecok et al., 2006), with appropriate training, frontline primary care providers are willing and enable to engage with mental health consumers, including those living with SPMI, and have conversations around distress and mental health crises. Hence, it is evident from this study that consumers living with SPMI are willing to have conversations with primary care providers about personal life events and mental health symptoms.
Limitations
This study examined psychological distress using the validated K6 scale and secondary sources of data (i.e. written and verbal reports); however, it is not without limitations. Firstly, consumer participants were recruited from three Australian regions, with the majority of the sample from one region, and, hence, the study sample may not be representative of the entire population living with SPMI nationally or internationally. Secondly, the written records analysed in this study were documented by pharmacists and research team members and may be subject to recall bias and not necessarily reflect consumer participants’ own perceptions of their distress. Future studies involving consumers’ perceptions of their experiences of psychological distress are warranted. Nonetheless, this study is strengthened by the analysis of two separate written records, as well as the use of an independent coder. Furthermore, the high Kappa values indicate sound interrater reliability among two coder, lending evidence to the robustness of the coding process. Furthermore, consumers’ mental and physical health diagnoses were self-reported and may not reflect clinical diagnoses documented by healthcare practitioners. The presence of physical health conditions was not stated for 40 participants in this sample, and this may have impacted the univariate regression model. Further work is needed to explore whether co-morbid physical illnesses impact psychological distress, along with other factors that could not be explored in this study, such as living with a disability and time since diagnosis of mental illness, among people living with SPMI.
Finally, despite including 150 consumer participants in this study, only pharmacists who recruited consumer participants with scores ⩾19 was required to submit distress reports and complete phone interviews with research team members; hence, there were no written records to analyse for those who scored <19. It is therefore possible that consumers who scored <19 were experiencing psychological distress and/or a mental health crisis and were not captured. However, the K6 scale is a validated and reliable tool with high sensitivity and specificity and was chosen due to its accuracy in detecting psychological distress (Kessler et al., 2002). Despite these potential limitations, this study is an important addition to the current literature and contributes to the evidence surrounding the levels of distress and needs of people living with SPMI, particularly given the limited evidence exploring pharmacist-delivered care for this vulnerable population.
Conclusion
More than one-third of individuals living with SPMI in this study scored ‘very high’ on the validated K6 psychological distress scale. Most of those surveyed were not reported to be displaying obvious signs of psychological distress, indicating that psychological distress may go undetected in this population. Younger age, unemployment and co-morbid mental illnesses were associated with higher psychological distress scores among the community-dwelling sample living with SPMI. Further work is warranted to understand the prevalence, extent and impact of psychological distress in people living with SPMI, how to best manage this distress and to explore the reliability and validity of the K6 scale in populations living with SPMI.
Footnotes
Acknowledgements
The authors wish to acknowledge the consumer participants and pharmacy staff involved in the RCT.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This activity received grant funding from the Australian Government Department of Health and Aged Care. The researchers were independent from the funder. This article contains the opinions of the authors and does not in any way reflect the views of the Department of Health and Aged Care or the Australian Government. The funding provided must not be taken as endorsement of the contents of this paper.