
Abstract
Background:
Shared decision making (SDM) is a health communication model promoting patient-centered care that has not been routinely utilized in mental health. Inconsistent definitions, models, measurement tools, and lack of sufficient evidence for the effectiveness of SDM interventions are potential contributors to the limited use of SDM in mental health.
Aims:
(1) Provide the first systematic analysis of global development trends and challenges of SDM research; (2) clarify the meaning, role, and measurement of SDM in mental health; (3) create a theoretical framework for key effective SDM components to guide future development and implementation of SDM interventions.
Methods:
A comprehensive search strategy was conducted in CINAHL, PubMed, Scopus, MEDLINE, EMBASE, Cochrane Library, Web of Science, Scopus, and PsycInfo. Included reviews focused on SDM interventions for prevention and/or treatment of mental illness in adults. A narrative synthesis was performed to capture the range of interventions, populations, measurement tools, comparisons, and outcomes.
Results:
10 systematic reviews of SDM in mental health were included with 100 nested studies spanning from 2006 to 2020. All reviews focused on dyadic and psychopharmacological decision-making. Primary outcomes of SDM in mental health interventions include treatment satisfaction, medication adherence, symptom severity, quality of life, and hospital readmissions. Participant-related factors unique to SDM in mental health, such as stigma and mental capacity, were not reported.
Conclusions:
The current landscape of SDM in mental health is overwhelmingly disconnected from the needs and experiences of potential end-users; clients, clinicians, and family members. Most SDM interventions and tools were adapted from physical health and are mainly geared to psychopharmacological decision-making. The SDM in Mental Health Framework (SDM-MH), developed here, expands the scope of decisions to non-psychopharmacological discussions, diversifies the pool of SDM participants and settings, and offers potential primary target outcomes of SDM in mental health to reduce heterogeneity across studies.
Introduction
“No decision about me, without me” reflects the importance of patient choices, values, and preferences in guiding healthcare decisions. Shared decision making (SDM) is a health communication approach that focuses on improving patient–clinician interactions around medical decisions in chronic conditions, with the goal of improving experience of care, clinical and functional outcomes (Zisman-Ilani, Roth et al., 2021). Clinicians and patients alike emphasize the importance of achieving a constructive therapeutic alliance and see this as essential (Kaminskiy et al., 2021). Moreover, decision-making may need to be negotiated between, and communicated to, multiple health and social care practitioners, as well as patients and their social networks (SNs) (Hamann & Heres, 2019; Zisman-Ilani, Roth et al., 2021). Strong SNs are crucial for the social integration and recovery of people with mental illness, who frequently experience difficulties in developing and maintaining social relationships and are more socially isolated, resulting in increased loneliness, compared to the general population (Chmielowska et al., 2021b).
In mental health, SDM has shown numerous benefits, such as increased knowledge of treatment options and conditions, involvement in decision-making, and satisfaction with psychiatric interactions (Deegan & Drake, 2006; Salyers & Zisman-Ilani, 2020). Yet, rates of SDM use and implementation in mental health are still very low compared to physical health (Zisman-Ilani, Barnett et al., 2017; Zisman-Ilani, Roth et al., 2021) with common challenges such as perceived stigma and self-stigma about patient decision-making capacity, and clinicians’ fear of liability and legal exposure (Hamann et al., 2017; Zisman-Ilani, Lysaker et al., 2021). However, the main barrier to SDM implementation in mental health is rarely discussed, namely the lack of a coherent, mental health-driven SDM model originally developed with and for people with mental illness, their care providers and families (Haugom et al., 2020; Ramon et al., 2021). SDM in mental health is characterized by inconsistent definitions and measurement tools, and there is a limited understanding of the key components of effective SDM interventions (Hamann & Heres, 2014). This novel umbrella review aims for the first time to clarify what is considered an effective SDM approach in mental health and to identify the core targets and elements required for successful utilization and implementation of SDM.
Methods
Design
Umbrella reviews, systematic overviews of systematic reviews and meta-analyses, gather evidence from multiple research syntheses to provide an overall examination of a body of information available for a given topic (Papatheodorou, 2019). This design was chosen because: (a) as the number of single studies focusing on SDM interventions, especially in mental health, increases, so does the number of published synthesis reviews; (b) an umbrella review provides means to report on the current direction and future priorities of SDM interventions in mental health (Aromataris et al., 2015). This review is based on the working definition of SDM as a health communication approach focusing on patient-clinician-family/carers interactions around treatment decisions, with the goals of improving clinical and functional outcomes via personalized care (Zisman-Ilani, Roth et al., 2021). It is reported using the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) 2020 statement (Page et al., 2021) (Supplemental Appendix 1), the protocol was a-priori registered (PROSPERO: CRD42020190700) and published (Chmielowska et al., 2021a).
Search strategy
A comprehensive search was performed using nine electronic databases: CINAHL, PubMed, Scopus, MEDLINE, EMBASE, Cochrane Library, Web of Science, Scopus, and PsycInfo. Some of the key terms included shared decision making, decision support system, decision aid, informed choice, and informed decision (Supplemental Appendix 2).
Inclusion criteria
All types of evidence were addressed matching the “PICO” (Participants, Intervention, Comparator, Outcome) criteria to capture the evidence from quantitative and qualitative reviews. Study inclusion and exclusion criteria are presented in Supplemental Appendix 3. An umbrella review’s key characteristic is that it only considers for inclusion the highest level of evidence, namely other systematic reviews, and meta-analyses (Aromataris et al., 2015). Most importantly, it offers a synthesis of two levels of evidence: systematic reviews and their primary research studies. Systematic and scoping review articles were included if they were published between 2010 and 2021 (Aromataris et al., 2015) and consisted of studies in which interventions were carried out by a wide range of healthcare professionals (e.g. psychiatrists, general practitioners, psychologists, nurses, and lay support staff) working in mental health settings. Interventions could target patients, healthcare professionals or both, and caregivers. The eligible reviews included primary research studies (i.e. studies which contain the original data and analysis conducted by their authors) that used quantitative (e.g. surveys), qualitative (e.g. interviews, focus groups) and mixed-methods methodologies and helped understand the variation in outcomes and the mechanism by which SDM interventions had an impact.
Type of interventions and participants
Interventions could take place in any setting (e.g. inpatient, outpatient, primary care, community, and secure environment) and were not restricted by the mode, duration, or frequency of delivery. Included reviews may have assessed a single intervention/component or combination of interventions/components and compared them with other interventions with a similar purpose or with usual care. Participants of interest were adults aged 18 years and older diagnosed with a mental health disorder who faced a decision about their mental health treatment. A mental health disorder was defined as diagnosable psychological problems that could disrupt thinking, feeling, mood and behavior and cause significant impairments in daily functioning. Examples are mood disorders, anxiety disorders, personality disorders, eating disorders, alcohol use disorders (AUDs) and substance use disorders (SUDs), and psychotic disorders.
Outcome of interest
SDM outcomes fell into one of these categories: affective-cognitive, behavioral, and health. Affective-cognitive outcomes include knowledge, attitudinal and affective/emotional effects. Behavioral outcomes include adherence to recommended treatments and adoption of health behaviors. Health outcomes include measures of quality of life (QOL), self-rated health, and biological measures of health (Kreps et al., 1994).
Study screening and selection
MC performed the initial screen of titles and abstracts, with a random 10% sample screened by a secondary reviewer (YZI). Two reviewers then performed full text screening of any potentially relevant studies. Disagreements were resolved by discussion between the reviewers, with a senior reviewer (SP) acting as arbiter where necessary.
Assessment of methodological quality of included reviews
A measurement tool for the ‘assessment of multiple systematic reviews’ (AMSTAR) two tool (Shea et al., 2017) was used to assess the methodological quality of the included systematic reviews (Supplemental Appendix 4). The tool provided guidance to rate the overall confidence in the results of a review (high, moderate, low, or critically low, depending on the number of critical flaws, and/or non-critical weaknesses). The quality appraisal included a table that provided a breakdown of how each systematic review was rated on each question of the tool, the rationale behind the assessments, and an overall rating for each systematic review. The results of the quality/risk of bias (RoB) assessments were then used to contextualize the umbrella review’s evidence base (Supplemental Appendix 5). Two reviewers assessed the quality of each individual text. Discrepancies were resolved by consensus.
Assessment of the quality of the evidence in reviews
The Grading of Recommendations Assessment, Development and Evaluation (GRADE) ratings were extracted from each included review. Similar to previous umbrella reviews/overviews, the authors made judgments to downgrade or upgrade the quality of evidence based on the RoB using the criteria specified by the GRADE Working Group (Balshem et al., 2011). Discrepancies in the ratings of the quality of evidence were resolved by consensus between the authors and, if necessary, arbitration by a senior reviewer.
Data extraction
Two reviewers independently extracted data on the included reviews using a previously designed data extraction form. The authors summarized the review findings but did not re-synthesize the results of primary studies. Extraction information included: review characteristics: author, publication year, country, type of review; objectives; PICO; setting and context, number and study design of primary studies included in each review; SDM taxonomy; an assessment of the methodological quality of the included review; summary of results/findings.
Data summary and analysis
Umbrella reviews often identify and synthesize systematic reviews on the same topic, which is likely to lead to overlap (i.e. duplication) in primary studies across the reviews (Lunny et al., 2021). To address this issue, the authors assessed and calculated the degree of overlap in primary studies via the corrected covered area (CCA) index method (Hennessy & Johnson, 2020). A CCA within the range 0%–5% indicates a slight overlap, 6%–10% indicates a moderate overlap, 11%–15% indicates a high overlap and >15% indicates a very high amount of overlap (Pieper et al., 2014). Data were grouped where possible according to the population, the type of intervention, and the outcome measure. Barriers and facilitators for implementation were identified across different articles and collated. Important limitations within the evidence base were presented and discussed. Any possible influence of publication/small study biases on review findings was also considered. Finally, a list of recommendations based on the data synthesis from all studies was compiled. Once the previous steps of the umbrella review were completed, the authors analyzed the included reviews to determine whether there were studies sufficiently similar in design, setting (e.g. in-patient, community mental health team, etc), age, intervention, and outcome measurement to allow their data to be combined for meta-analysis. This proved unfeasible due to heterogeneity of included reviews. The results of the umbrella review were reported using a narrative synthesis. First, each review was summarized. Then details of the research context, the review period, the objectives, and the primary studies identified within the review were presented.
Results
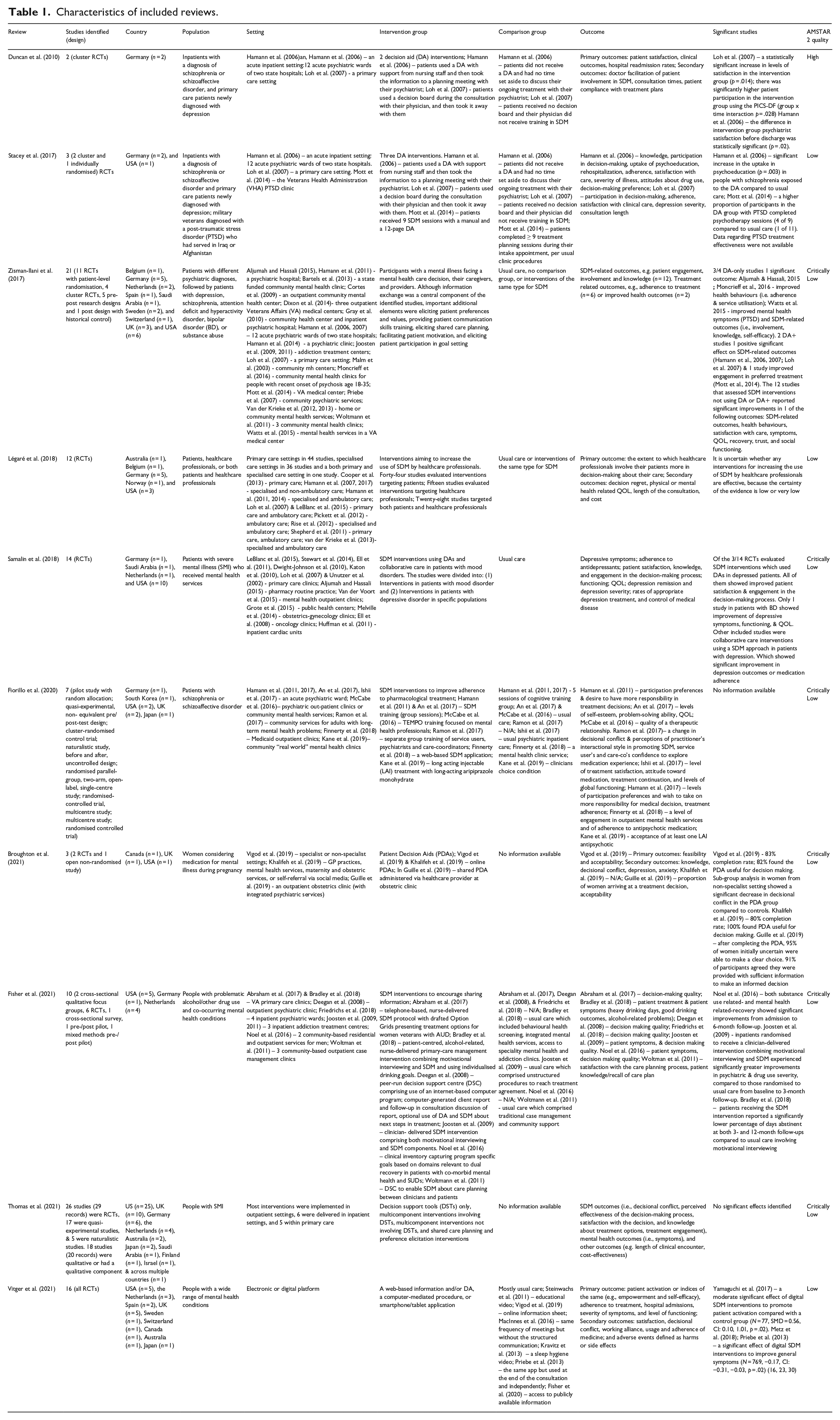
Searches yielded 7,383 records. After the duplicate removal and screening of titles and abstracts, 25 full-text reviews were assessed for eligibility through full-text screening. After this assessment, 10 systematic reviews (Broughton et al., 2021; Duncan et al., 2010; Fiorillo et al., 2020; Fisher et al., 2021; Légaré et al., 2018; Samalin et al., 2018; Stacey et al., 2017; Thomas et al., 2021; Vitger et al., 2021; Zisman-Ilani, Barnett et al., 2017) met the inclusion criteria (Figure 1). All 10 reviews evaluated SDM interventions and/or tools for dyadic patient-clinician psychopharmacological decision-making and included various mental health conditions, SDM intervention types and outcomes. A total of 168 studies were included in the 10 reviews. Of these, 68 studies (24 ineligible and 44 duplicates) were excluded from this umbrella review, resulting in 105 non-overlapping unique articles, of which 100 were the primary studies (n = 5/100 studies led to overlapping publications). The number of studies nested within individual reviews varied from 2 to 53. The included studies were conducted in 16 high-income countries: Australia, Belgium, Canada, Finland, Germany, Israel, Japan, the Netherlands, Norway, Saudi Arabia, South Korea, Spain, Sweden, Switzerland, UK, and USA. The first identified study was published in 1999 (Sutherby et al., 1999) and the most recent was published in 2020 (Fisher et al., 2020; Gibson et al., 2020; Treichler et al., 2020). In the 10 reviews, a total of 47,846 participants (47,071 patients, 676 clinicians, 5 family carers, 90 other carers, or 4 ‘other’) were included (Supplemental Appendix 6). Median total sample size was 167.5 (range 10–13,734). Details of the excluded reviews and the reasons (e.g. incorrect population characteristics, type of interventions, and outcomes) are provided in the Supplemental Appendix 7. Table 1 summarizes the characteristics of all reviews, including quality rating, study design and methodology, population and setting, intervention and comparison group, main outcome measures, and significant results. Details of the included/excluded primary studies and the reasons (e.g. incorrect population characteristics, study design, and overlapping publication) are provided in the Supplemental Appendix 8.
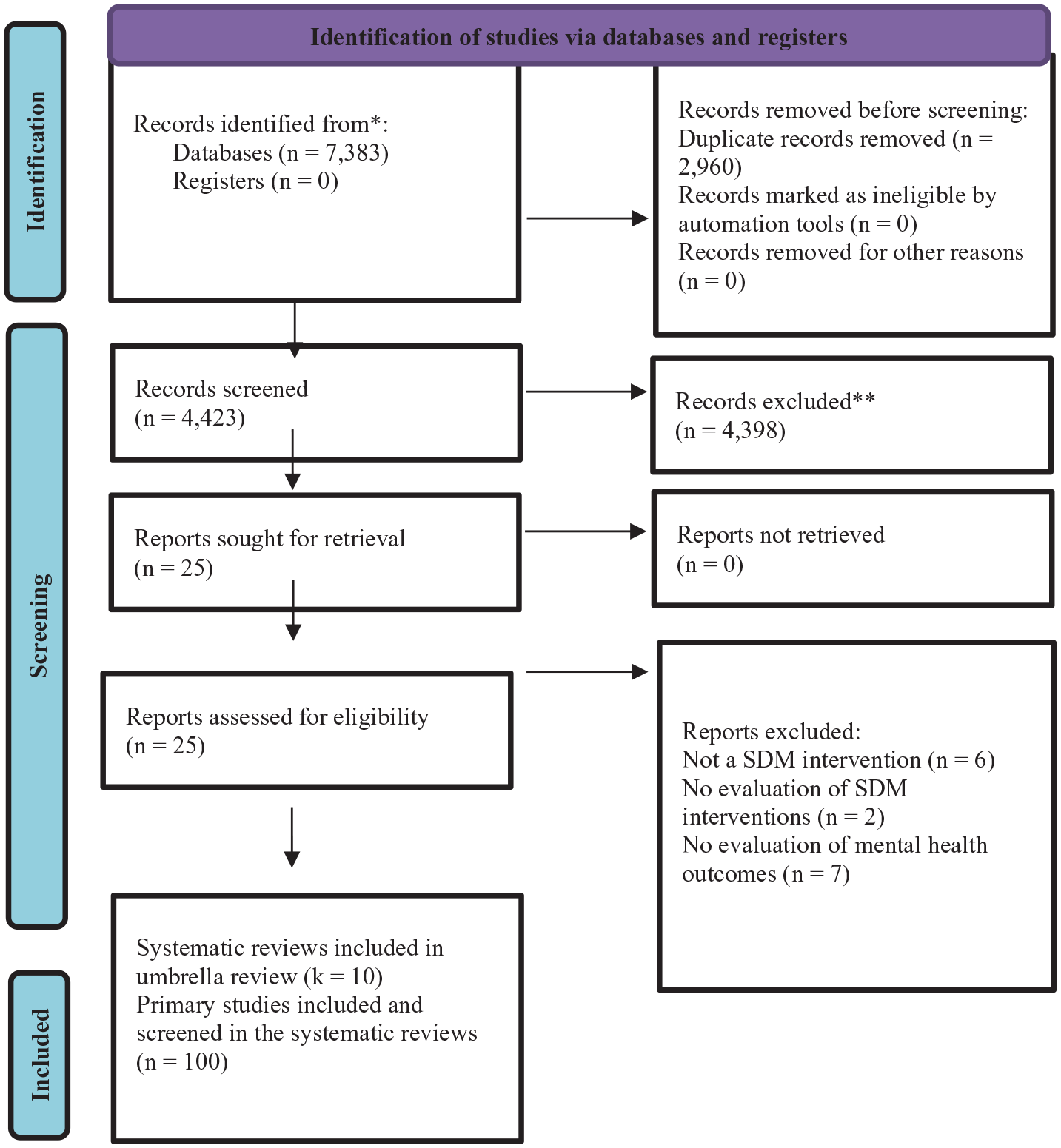
Flowchart of the literature search and evaluation process for 10 published systematic reviews.
Characteristics of included reviews.
Degree of overlap between the included reviews
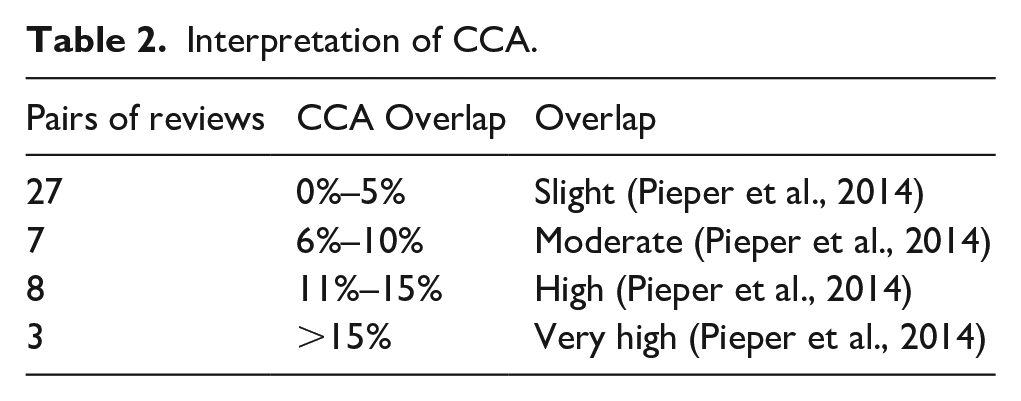
The CCA indicated overlap of 4% between the primary studies across reviews (Table 2). Fifth of the primary studies (n = 20/105) appeared in at least two reviews, and the degree of overlap between individual reviews varied from 0% to 60% (Figure 2).
Interpretation of CCA.
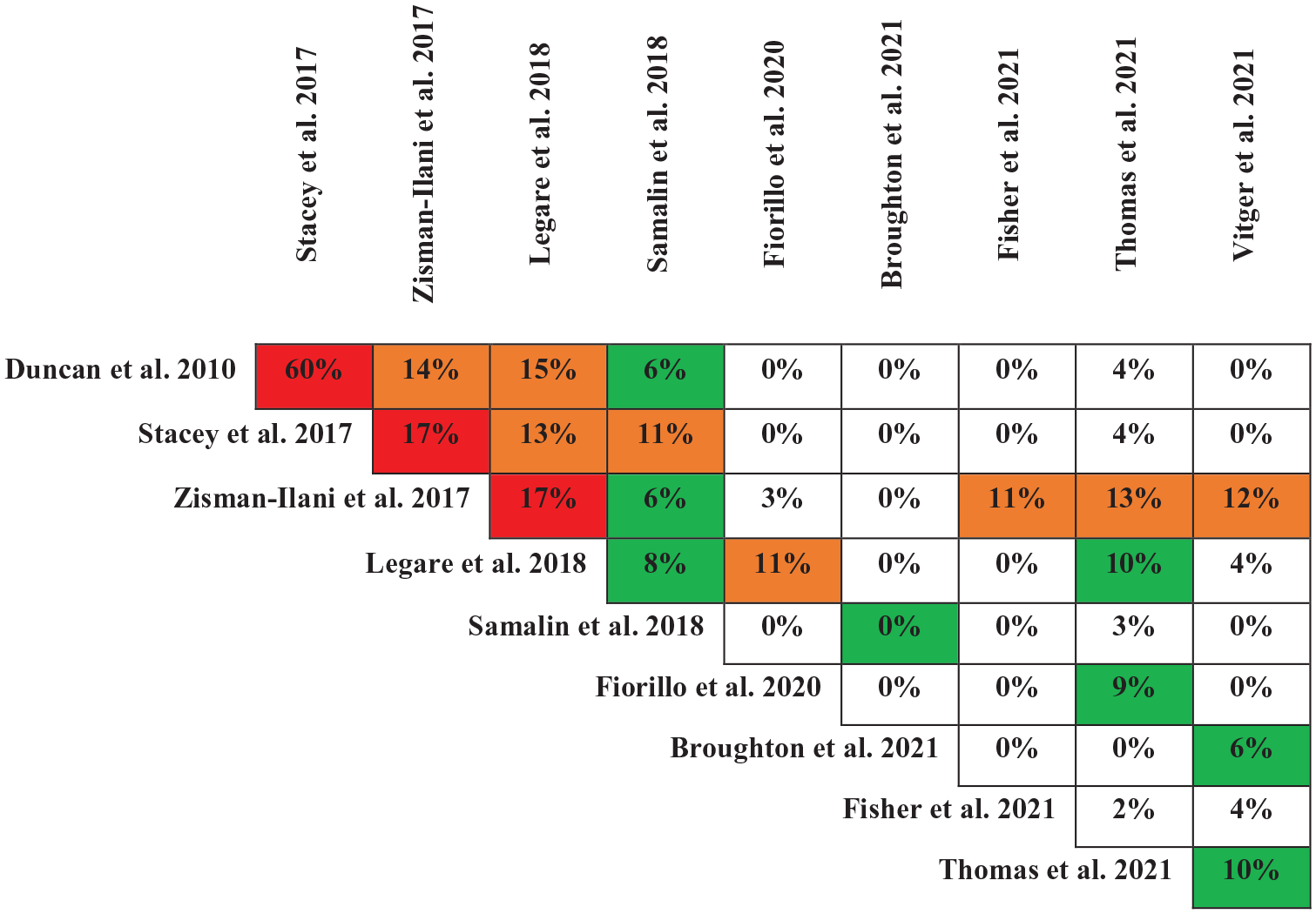
Degree of overlap between the reviews.
Methodological quality of the included reviews
The methodological quality of the included reviews was poor overall (critically low = 60%, low = 30%,and high = 10%); only 30% (k = 3/10) provided an a priori protocol, 80% (k = 8/10) conducted a ‘comprehensive’ literature search, 30% (k = 3/10) provided a list of excluded studies, and 30% (k = 3/10) performed meta-analyses. AMSTAR 2 scores for each review are presented in Supplemental Appendix 5.
Characteristics of the included reviews
All reviews referred to the broader SDM literature and cited at least one of the following SDM models: Charles et al. model of medical decision-making (Duncan et al., 2010; Fisher et al., 2021; Légaré et al., 2018; Stacey et al., 2017; Thomas et al., 2021; Vitger et al., 2021; Zisman-Ilani, Barnett et al., 2017), the Integrative model of SDM (Stacey et al., 2017), the Three Talk Model (Broughton et al., 2021; Fiorillo et al., 2020; Légaré et al., 2018; Samalin et al., 2018; Vitger et al., 2021; Zisman-Ilani, Barnett et al., 2017), the SDM 3 Circle model (Légaré et al., 2018; Vitger et al., 2021). However, not all reviews (k = 9/10) included a definition of SDM (Duncan et al., 2010; Fiorillo et al., 2020; Fisher et al., 2021; Légaré et al., 2018; Samalin et al., 2018; Stacey et al., 2017; Thomas et al., 2021; Vitger et al., 2021; Zisman-Ilani, Barnett et al., 2017). Each review listed at least half (7/14) of the SDM components extracted from the cited models: at least two participants are involved, both parties share information, both parties take steps to build consensus about the preferred treatment to implement, present options, discuss pros/cons, clarify understanding, discuss patient values/preferences, discuss doctor knowledge, make or explicitly defer a decision, establish a collaboration in a decision-relevant situation, check/enhance knowledge, enhance patient participation, and provide decision support. The most frequently listed SDM component was provide decision support (10/10) (Broughton et al., 2021; Duncan et al., 2010; Fiorillo et al., 2020; Fisher et al., 2021; Légaré et al., 2018; Samalin et al., 2018; Stacey et al., 2017; Thomas et al., 2021; Vitger et al., 2021; Zisman-Ilani, Barnett et al., 2017), and the least frequently listed one was check/clarify understanding/summarize (1/10) (Broughton et al., 2021). However, SDM components such as build trust, establish a therapeutic alliance, support personal recovery, activate, and empower, which are essential for clinical interaction in mental health, were not addressed by the models. All reviews presented a medical perspective on SDM in mental health and focused on inclusion of decision aids (DAs) to promote adherence to psychopharmacological treatment. Three reviews were broader in their scope and offered psycho-educational perspectives on SDM in mental health (Légaré et al., 2018; Thomas et al., 2021; Zisman-Ilani, Barnett et al., 2017). All reviews included several types of measurement tools (e.g. the Autonomy Preference Index, the Observing Patient Involvement in Decision Making, Patient’s perceived involvement in Care Scale, Decision Self-Efficacy, and Decisional Conflict Scale) and evaluated a wide range of outcomes, such as treatment satisfaction and knowledge, medication adherence, symptom severity, QOL, hospital readmissions, and recovery rates. Participant-related factors unique to SDM in mental health, such as stigma and mental capacity, were not available. None of the measurement tools were developed and validated for people with mental illness and there was no consensus on outcomes as primary targets of SDM research in mental health.
Characteristics of SDM interventions in primary studies
The primary studies were conducted across four different types of treatment settings (Figure 3): mental health hospital settings (N = 15), general hospital settings (N = 1), community mental health settings (N = 56), and community health settings (N = 28). SDM Interventions fell into the following categories: decision support tools (DSTs) only, multicomponent interventions involving DSTs, multicomponent interventions not involving DSTs, and shared care planning and preference elicitation interventions. SDM interventions were applied to a wide range of mental health conditions (Figure 3) and treatment-related decisions (Figure 3). Main diagnoses were schizophrenia-spectrum disorders (N = 31), SMI-related disorders (i.e. a mix of patients diagnosed with one of the following: schizophrenia-spectrum disorders, depressive disorders, anxiety disorders, BDs, SUDs, personality disorders, and PTSD (N = 29), and depressive disorders (N = 27). Far less addressed conditions were eating disorders (N = 1), and borderline personality disorders (N = 1). Main SDM components included: define goals and actions (N = 11), enhance patient participation/activate and empower patients (N = 37), discuss patient values/preferences (N = 32), establish a therapeutic alliance (N = 11), and make the decision (N = 9). A summary of all treatment settings, mental health diagnoses, and SDM components is presented in Supplemental Appendix 9.
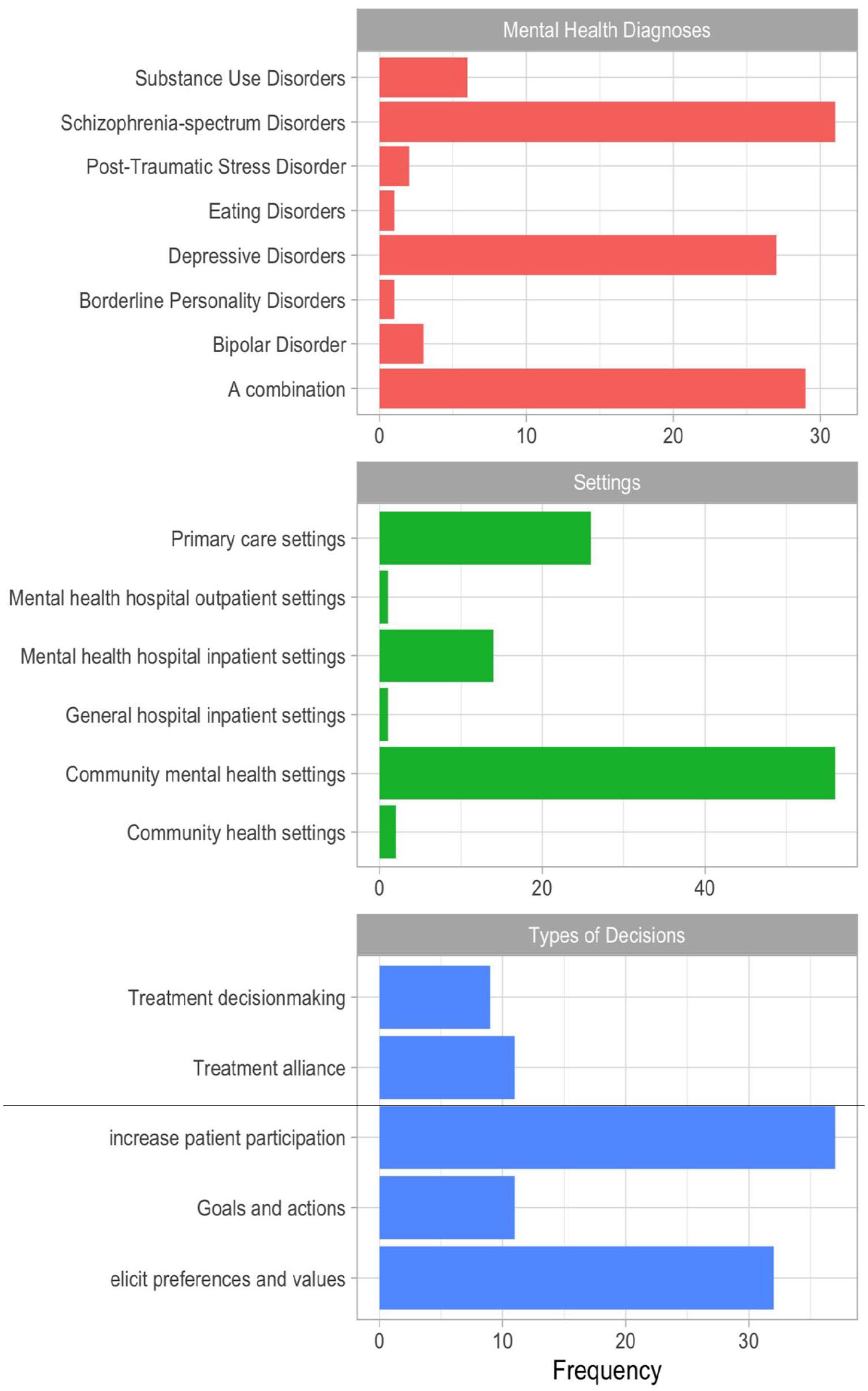
Treatment settings, diagnoses, and decision types across the included studies.
Global trends of SDM practices
Over the last two decades, the landscape of SDM research in mental health has established itself as a growing area of intellectual inquiry, with almost half of the primary studies (43%) published from 2015 to 2020 (Figure 4). Despite a rapid increase in peer-reviewed publications on SDM in mental health, much research has relied on SDM models applied in physical health and focused narrowly on psychopharmacological decision-making among patient-clinician dyads in community-based settings. None of the existing instruments to measure SDM in mental health have been developed and validated with and for people with mental illness, and there has been a lack of consensus on outcomes as primary targets of SDM mental health. The results of this umbrella review highlight the need to expand SDM mental health research to a broader range of decisions, participants, and settings, with a particular focus on family members, peer support workers, and non-psychiatric healthcare professionals (Hamann & Heres, 2019; Zisman-Ilani & Byrne, 2022). Directions for future research include the development and validation of SDM measures that acknowledge participant-related factors unique to SDM in mental health, such as stigma and mental capacity.
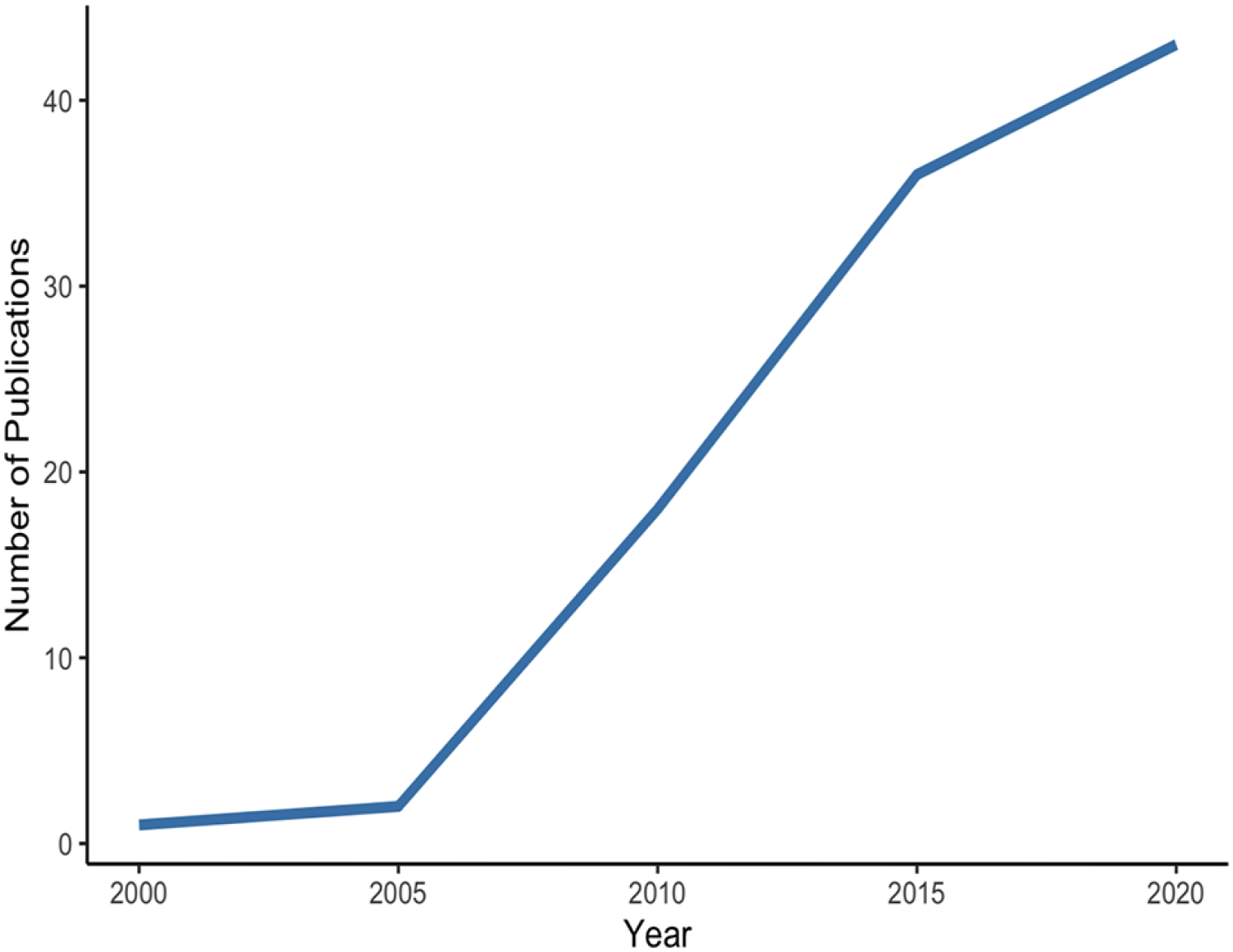
A two-decade output of SDM mental health studies in the included reviews.
Discussion
This umbrella review provides the first systematic analysis of global development trends, challenges, and priorities of SDM research in mental health. It offers a comprehensive overview of SDM interventions and tools for mental health based on 10 systematic reviews and 100 nested studies, with a total of 47,846 participants.
The scope and relevance of SDM interventions in mental health
All included reviews presented a medical perspective on SDM in mental health and focused on the inclusion of DAs to promote adherence to psychopharmacological treatment. Although DAs reflect significant advances in the effort to involve patients in decision-making, they tend to focus on one element of SDM – information exchange – and do not target other important components of the SDM process, such as deliberation and joint decision-making, or building rapport and trust (Wieringa et al., 2019). Therefore, focusing on the practice of exchanging information overlooks the possible broader contribution of SDM to such outcomes (Perestelo-Perez et al., 2017). The recovery model proposes the integration of people with mental illness into the community, and greater responsibility and involvement in decisions about their own lives. In this respect, one of the most important priorities for future research is to capture the complexity of SDM in mental health when decisions occur over multiple time periods, involve chronic and ongoing challenges, and often with significant shame or stigma (Perestelo-Perez et al., 2017). Future SDM interventions and tools should include, in addition to psychopharmacological decisions, social prescribing decisions and therapy decisions, such as psychosocial issues like work, lifestyle, housing, legal issues or social and leisure activities (Zisman-Ilani & Byrne, 2022; Zisman-Ilani et al., 2019; Zisman-Ilani, Lysaker et al., 2021). In studies using DAs, inherent training materials should be developed in co-production with clinicians, patients, and other potential members of SDM such as family members and carers.
Polyadic SDM in mental health
All included reviews evaluated SDM interventions and tools for psychiatric medication decisions in a dyadic context, with two participants, a patient, and a clinician. However, several studies have shown that the presence of a third person in the consultation significantly improves patient engagement and understanding, as well as the symmetrical power relationship between patients and clinicians (Basu et al., 2010; Keeling et al., 2015; Wolff et al., 2015). As such, polyadic consultations with more than two participants, offer not only the potential for cooperation, but also for long-term and recovery-oriented care. Most mental health guidelines encourage the involvement of patient SNs (i.e. family members, carers or peer support workers; PSWs) in treatment planning and decision-making (Dirik et al., 2017). Carers and family members can improve patient engagement with treatment, respond to early warning signs of relapse (Herz et al., 2000) and lead to better outcomes from both therapy and medication (Glick et al., 2011), leading to shorter hospital stays and better QOL (Schofield et al., 2001). Notably, because of their personal experience, PSWs often have credibility, especially with parents, and can build trust (Gyamfi et al., 2010) and promote family engagement in the recovery process (Wisdom et al., 2011). PSWs also challenge stigma and promote help-seeking behavior among patients with mental illness (Thornicroft et al., 2016; Yanos et al., 2015). Future research studies should focus on the involvement of PSWs and family members in SDM.
The conceptual landscape of SDM in mental health
All reviews included several types of measurement tools and evaluated a wide range of outcomes (Perestelo-Perez et al., 2017). However, none of the reviews included an assessment of mental capacity to make treatment-related decisions, which has become a key component of daily clinical practice (Harding & Taşcıoğlu, 2018; MacKay, 2006). This led to bias in the presentation of what is considered representative evidence of effective SDM research and practice in mental health, especially in SMI, where frequent fluctuation and variation in decision-making capacity and its implications for evolving research on SDM in mental health (Zisman-Ilani, Chmielowska et al., 2021). Currently, clinical outcomes such as psychiatric hospitalizations or psychiatric symptoms remain a focus of SDM research and contribute to a mixed evidence base for the effectiveness of SDM interventions in mental health, in which recovery-oriented outcomes such as empowerment, self-efficacy, and hopefulness are the main outcomes, especially in the mental health services field, which SDM is part of (Salyers & Zisman-Ilani, 2020; Zisman-Ilani, Chmielowska et al., 2021). The lack of validated SDM measures uniquely developed to assess SDM in mental health is a critical factor that contributes to the limited use of recovery-oriented SDM outcomes. SDM research is biased toward White and Western populations as most SDM interventions have not been developed with or for Black, Asian and minority ethnic groups, nor with people with mental illness or other disabilities (Treichler & Zisman-Ilani, 2022; Zisman-Ilani et al., in press; Zisman-Ilani, Chmielowska et al., 2021). As a result, early efforts to investigate SDM in mental health relied on existing tools and measures, with required tailoring and adaptation to mental health (Perestelo-Perez et al., 2017). There are many examples of adaptations of existing SDM measures to mental health, including the SDM-Q-9-Psy as revised version of the SDM-Q-9 (Zisman-Ilani, Roe et al., 2017), but no bottom-up person-centered care measure has been developed with and for people with mental illness. Since most existing measures for SDM in mental health have been adapted or borrowed from SDM studies in chronic physical illness (Perestelo-Perez et al., 2017), the measured SDM output is often less relevant and meaningful for assessing an SDM process in mental health (Zisman-Ilani, Lysaker et al., 2021). A useful strategy is to consider which outcomes are valued by the people who use services and to develop an evaluation approach based on these goals. Person-driven measurement approaches and more participatory research methods can improve both the quality and impact of mental health services. A way to bridge the gap between clinical outcomes and recovery-oriented outcomes is therefore to start with patients’ priorities (Barrenger et al., 2019). The measurement of personal outcomes identified by patients should include a recovery orientation and require participatory research methods. This is in line with the focus on agency as a component of recovery (Tang, 2019) by engaging people in recovery in defining their valued life goals. These personal outcomes include key aspects of QOL, such as social connections and feeling safe, change outcomes such as managing symptoms and improving morale, and process outcomes such as being listened to and treated with respect. The person-centered approach helps to overcome some identified tensions by combining different outcomes that include clinical concerns in a way that does not eclipse valued recovery outcomes, and process outcomes that can help to capture benefits associated with the working alliance (Rogers, 2017).
Sociocultural influences on SDM in mental health
All reviews included studies conducted in high-income countries, and none of the SDM interventions in mental health addressed socio-cultural backgrounds and experiences, treatment needs and expectations of patients. Illness narratives are often closely linked to social adversity or trauma, and hold a specific meaning within the local cultural context (Jacob & Patel, 2014). They can include theories of mystical, animistic, and magical causalities (e.g. fate, soul loss, sprit regression, sorcery, and witchcraft), which are predominantly addressed by traditional and faith-based healing treatment (Kirmayer & Bhugra, 2009).There is widespread concern that existing SDM interventions in mental health do not fully promote the key principles and values of person-centered care and personal recovery from mental illness (Matthews et al., 2022; Zisman-Ilani, Chmielowska et al., 2021). Consequently, there is a gap between what services prioritize in terms of SDM outcomes and what matters to patients and their families, especially for marginalized and health-disparity groups, who often experience inequalities in access to mental health services due to perceived discrimination and systemic and cultural barriers (Bansal et al., 2014; Chen & Yang, 2014). Expanding the definition of SDM in mental health to additional outcomes, decisions, and populations will broaden the scope, thereby enabling a better representation of cultural and ethnic diversity in SDM research in mental health (Zisman-Ilani, Barnett et al., 2017).
Limitations
This umbrella review was subject to several limitations. First, the heterogeneity of measures, settings, and sample characteristics prevented the use of meta-analysis on the full data set (McKenzie & Brennan, 2019). To address this, we provided a descriptive account of the SDM literature in mental health and did not synthesize data for analysis. Consequently, judgments about effectiveness were based on the detection of statistically significant differences in outcomes and did not account for effect size. Other limitations include the exclusion of studies published not in English or those conducted with children under 18 years of age.
Recommendations for practice
Although early definitions of SDM suggest some form of family, friend, or carer involvement in patients’ mental healthcare (Charles et al., 1997), most interventions do not explicitly address SNs in SDM. Polyadic SDM provides opportunities for both the person with mental illness and members of their SN to express values or preferences in connection with specific decisions (Hamann & Heres, 2019). To support the involvement of SNs in SDM, it will be valuable to conduct focus groups with different stakeholders, including patients and their families, and discuss the fundamentals of why SN involvement is conducted, how it is experienced by patients and members of their SN, and how this relates to the perspective of clinicians. We encourage discussion of the differences and similarities between the different SDM models and theories, considering different ideas about the nature of mental health and the purpose of involving SNs in these contexts. Exploring and acknowledging such concerns through open but non-judgmental communication could facilitate the establishment of a therapeutic alliance between clinicians, patients, and their SNs.
Recommendations for research
Although there are many instruments to measure SDM in mental health, none of them have been developed and validated with and for people with mental illness, and there was no consensus on outcomes as primary targets of SDM research in mental health. This led to a mixed evidence base for the effectiveness of SDM interventions in mental health, where key aspects of recovery-oriented care, such as empowerment, self-determination, and hope, are the main priorities. In addition, the existing instruments focus only on dyadic patient-clinician consultations, and do not include the values and preferences of SNs in treatment decision-making. Recognition and contribution of polyadic SDM to the treatment of mental illness requires consideration of family members, carers, and PSWs in the evaluation of SDM interventions and treatments. Future research studies are therefore needed to develop and co-produce SDM measurement tools, interventions, and DAs for mental health that focus on personal outcomes that include a recovery orientation and require participatory research methods.
Conclusion
This umbrella review advocates for going beyond the traditional dyad of patient-clinician consultations and recognizes that engagement in mental health is increasingly polyadic. We provide the first framework for SDM in mental health that emphasizes the need for multiple decision-makers, including family members, PSWs, and non-psychiatric health professionals. Our framework puts SDM at the center of person-cantered care and personal recovery from mental illness, where person-driven measurement approaches and participatory research methods are the top priority. It sets a new direction for SDM research in mental health, with the focus on developing and validating SDM measures with and for people with mental illness.
Supplemental Material
sj-docx-1-isp-10.1177_00207640221140291 – Supplemental material for Trends, challenges, and priorities for shared decision making in mental health: The first umbrella review
Supplemental material, sj-docx-1-isp-10.1177_00207640221140291 for Trends, challenges, and priorities for shared decision making in mental health: The first umbrella review by Marta Chmielowska, Yaara Zisman-Ilani, Rob Saunders and Stephen Pilling in International Journal of Social Psychiatry
Footnotes
Acknowledgements
The protocol of the current umbrella review was registered in the PROSPERO database: CRD42020190700.
Conflict of interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Zisman-Ilani is a member of the Patient-Centered Outcomes Research Institute’s (PCORI’S) Advisory Panel on Clinical Effectiveness and Decision Science. The views in this commentary represent the opinions of the authors and not necessarily those of the PCORI. The authors report no financial relationships with commercial interests.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Ms. Marta Chmielowska’s work was supported by the National Institute for Health Research (NIHR, RP-PG-0615-2002). Dr. Zisman-Ilani’s work was supported by funding from National Institute of Mental Health (NIMH, R34 MH-128497). The views in this commentary represent the opinions of the authors and not necessarily those of the NIHR or NIMH.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.