
Abstract
INTRODUCTION:
Research suggests that persons diagnosed with behavioral health illnesses can benefit from shared decision-making. On an inpatient behavioral health unit, low Press Ganey scores related to satisfaction with involvement in care triggered a root cause analysis that identified patients did not feel engaged by nursing during their time together; and discharge meetings with the health care team were not required.
AIMS:
The purpose of this quality improvement project was to improve patient perception of involvement in their care as evidenced by increased Press Ganey scores and increased number of patients involved in discharge meetings.
METHODS:
Nurses used an evidence-based model for nurse–patient communication: the Seeking information, Engaging in conversation, Exploring options, and Deciding on treatment (SEED) and use of a Control Preferences Scale (CPS) to increase communication about treatment and discharge decisions.
RESULTS:
A total of 120 patients engaged in the intervention. Patient presence at discharge meetings increased from 39% to 82% (p < .001), and Press Ganey scores evidenced minimal change.
CONCLUSIONS:
Use of the SEED model and CPS by nurses was effective in increasing patients’ involvement in their treatment. Although findings were limited due to COVID-19, the study suggests that improving patient involvement from admission through discharge throughout hospitalization can improve patient experience scores.
Keywords
Introduction
Problem Description
In November 2019, the behavioral health unit’s Press Ganey score for “the degree to which you felt included in decisions about your care” was 75% overall. This was lower than the hospital’s current benchmark of 88.7% for the psychiatry department. The Press Ganey (2021) patient survey provides health care organizations with the ability to benchmark internally and externally on different aspects of the patient experience to guide improvements. This triggered a root cause analysis which identified the following factors contributed to patients’ perception of low involvement with their care: (1) Meetings and treatment planning did not always include the patient, (2) Patients did not feel engaged by nursing during their time together, and (3) Discharge meetings with the health care team were not required. Although the Press Ganey scores were the trigger for the initiation of improvement in patient involvement on this unit, improving patient care and the patient experience was the priority.
Patient preference is the third cornerstone in evidence-based practice (Guyatt, 1991). Persons diagnosed with behavioral health illnesses who lack involvement in their care express lower satisfaction with their care (Agency for Healthcare Research and Quality, 2017; Chevalier et al., 2018; Tambuyzer et al., 2014). Poor interaction with nurses around care decisions is also associated with increased use of restraints and seclusion (Al-Maraira & Hayajneh, 2019). In addition, increased costs can occur when patients do not perceive active involvement in their care (Cosh et al., 2017).
Available Knowledge
To increase patient involvement and satisfaction within behavioral health, researchers have begun exploring shared decision-making (SDM; Dixon et al., 2016; Duncan et al., 2010). SDM is defined as a provider–patient partnership that encourages communication among both parties to reach a decision or determine the person’s treatment plan (Dixon et al., 2016; Duncan et al., 2010; Storm & Edwards, 2013). This approach involves the following steps to be taken by the provider and the patient: (1) define the problem, (2) present options for the problem, (3) clarify patient preferences and understanding, and (4) make or defer a decision (Slade, 2017). SDM is an integral component of patient participation, patient-centeredness, and the recovery model (Storm & Edwards, 2013).
However, implementing SDM can be uniquely challenging within behavioral health units: persons may not believe they have a mental illness, and providers may not think that patients can make a rational decision given their acute mental state (Chevalier et al., 2018; Drake et al., 2009). Nevertheless, studies show persons with behavioral health illness diagnoses still seek involvement in their care. If patients perceived SDM was used in their case, there was decreased decisional conflict (p = .00; Metz et al., 2019). Decreased decisional conflict was associated with better clinical outcomes (p = .001; Metz et al., 2019).
There have been two systematic reviews of studies that used SDM with patients who have mental illness; however, the total number of included studies was small. The evidence is equivocal that SDM supports improved outcomes, but it has demonstrated increased patient participation in care and satisfaction with care (Dixon et al., 2016; Duncan et al., 2010).
In primary care in the United Kingdom, 588 patients with mental health diagnoses and 206 staff members, reported that satisfaction with the level of SDM was associated with reduced costs (Cosh et al., 2017). In Belgium, Tambuyzer and Van Audenhove (2013) surveyed 111 patients in outpatient networks. They identified a positive association among patient involvement, satisfaction, and empowerment (p < .05). Unlike other approaches, SDM can be implemented even when a patient is acutely psychiatrically unstable, and its application is simple and requires few resources.
Rationale
How health care workers engage in communication with patients with mental health disorders, particularly those hospitalized, sets the tone for the admission. The Seeking information, Engaging in conversation, Exploring options, and Deciding on treatment (SEED) model is an evidence-based model for health care professional interaction with patients. It was developed from a study that included patients, family decision-makers, and health care providers (Ho et al., 2016). Often having an engaging yet straightforward conversation is essential to understand the treatment method or medications the patient would find beneficial. Although developed for use with patients at the end of life, it applies to all patients. This process can start on admission with the nursing assessment to seek collateral information and engage in conversation. The more the patient shares about their family, culture, socioeconomics, personal values, and views on health and healing, the better more information is available to the health care team for exploring options and preferences for decision-making with patients/families (Ho et al., 2017).
Exploration of preferences can enhance patient outcomes as well as patient satisfaction. The Control Preferences Scale (CPS) was initially developed for use with patients with a life-threatening disorder. To indicate their preference, patients are given five cards that each portray a different role in treatment decision-making, using a statement and an illustration (Degner et al., 1997). Patient preferences for involvement with decisions about their care are divided into choices of active, collaborative, and passive roles. The CPS has been used in patients with HIV (Kremer & Ironson, 2008) and cancer (Singh et al., 2010). Patients with mental disorders (N = 728), who provided their desired participation in care using the CPS, preferred a collaborative role in medical decisions. Self-efficacy was also measured in this study and correlated positively with a moderately autonomous role in decision-making (Michaelis et al., 2017).
Aims
The purpose of this quality improvement project was to improve patient perception of involvement in their care as evidenced by increased Press Ganey scores and increased number of patients involved in discharge meetings using the evidence-based bundle of the SEED model at admission and the CPS tool during a designated patient face time. The aims of the process were to (1) provide education on the SEED model and CPS tool to 100% of the nursing staff, (2) increase the number of patients who engaged with nursing on admission using the SEED model, and (3) increase the number of patients who designated a preference for decision-making using the CPS tool.
Method
Context
The inpatient behavioral health unit is located in a Southeastern hospital. The hospital has 369 beds. The specific unit involved in this project is a 23-bed acute crisis behavioral health unit. This unit admits any adult experiencing an exacerbation of mental illness. The care model on the unit consists of two health care teams, each with one psychiatrist, one nurse practitioner (NP), and one licensed clinical social worker. Each member of the nursing staff can be assigned up to eight patients. Participating staff included all registered nurses who engage in patient face time, including new graduate hires, those in orientation, the behavioral health trained-float pool, and experienced staff.
Nurses have face time with their patients during two designated times: (1) during their admission assessment and (2) during patient face time. Patient face time is 1 hr of the day that the nursing staff has individual conversations with two of their assigned patients. Information from patient face time is shared during treatment team meetings held every day with all members of the health care team (psychiatrist, nurse practitioners, social workers, and charge nurse).
Intervention and Study of the Intervention
The Academic Center for Evidenced-Based Star Model of Knowledge Transformation guided this quality improvement project. The five points of the star depict the steps in the transfer of knowledge to evidence-based practice: (1) discovery and research, (2) evidence summary, (3) translation into practice, (4) integration into practice, and (5) process, outcome, and evaluation (Stevens, 2004).
Discovery and Evidence Summary
The problem of perceived low involvement of patients in their care was the triggering discovery, and the project leader (PL) conducted a review of the evidence to address the problem. Improving patient perception of involvement in care and SDM was identified as a potential way to improve patient satisfaction with involvement in their care. The SEED model for guiding interaction between nurses and patients on admission and the CPS for communicating patients preferred level of involvement in their care were determined to be the best fit for this project.
Translation Into Practice
The CPS cards were adapted for the patient population to represent non-gendered and no race or ethnicity. Statements were slightly simplified but similar to Degner et al.’s (1997) cards, with the characters ranging as follows: Active—the individual making the treatment decisions only (Card 1), active-shared—individual decisions are made jointly with the health care team after information is provided (Card 2), Collaborative—individual desires to make decisions with health care provider (Card 3), Passive—individual defers to health care team for decisions (Card 4), and Passive-shared—the individual desires the provider to make the decisions but to have their opinion considered (Card 5).
Integration Into Practice
Integration into practice occurred in two stages. The first stage of implementation was nurse education and training led by the PL. These sessions took place via videoconference (because the PL was not allowed on the unit due to COVID-19 restrictions) in two phases. First, a leadership team which included nurse manager, clinical team leads, and nine charge nurses from both day and night shifts were trained. These leaders then became the coaches for the rest of the staff. Second, the leadership team trained day- and night-shift nursing staff. In training sessions, participants practiced using the SEED model and CPS by engaging in multiple mock patient sessions with the coaches. Attendance was measured by having a sign-in/out sheet at the beginning and end of the education and training. The leadership team then observed the nursing staff using the SEED model during the initial nursing admission assessment (Table 1).
Training of Leadership Team and Nursing Staff (Two 6-Hr Sessions Later Changed to Zoom Sessions).
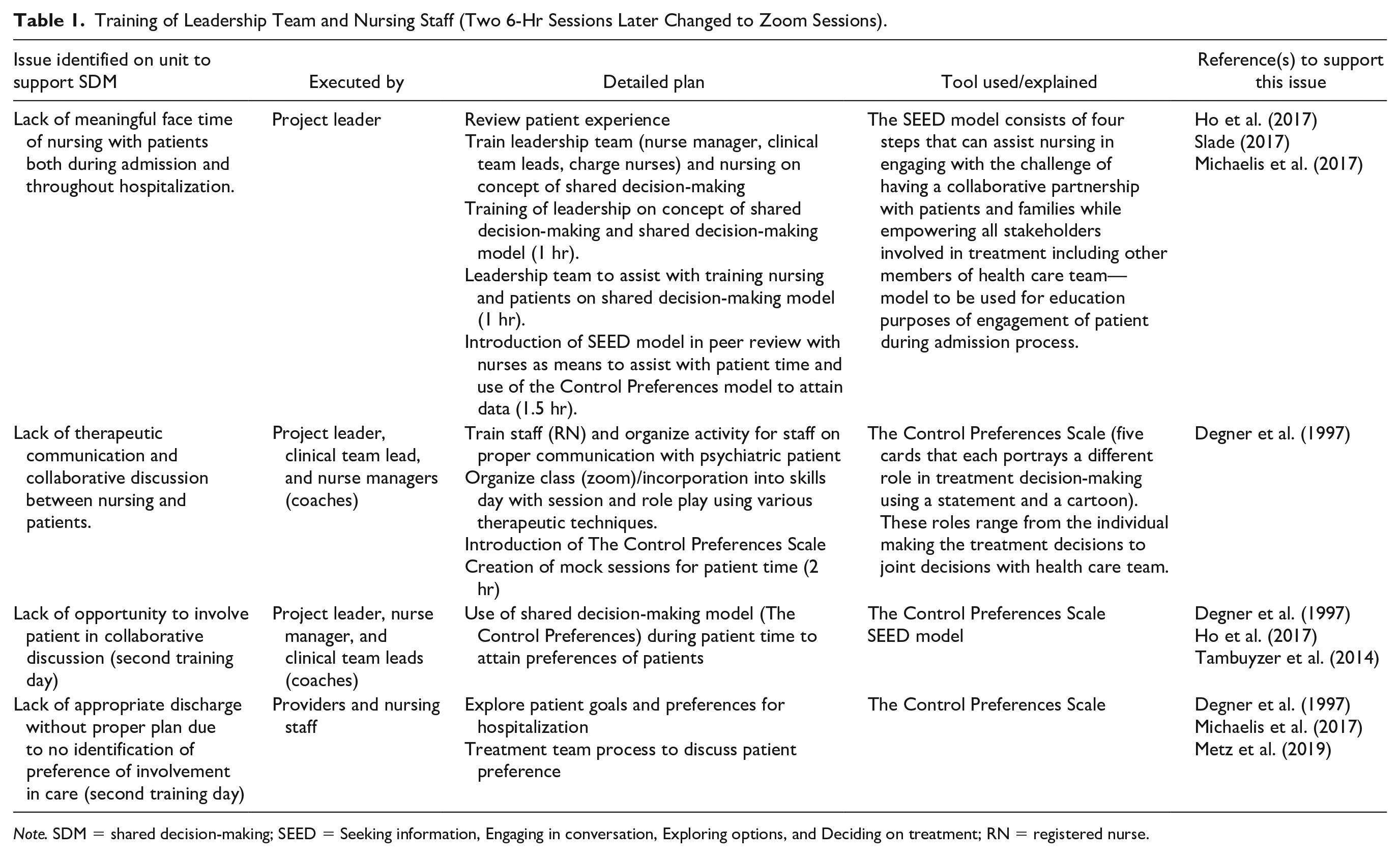
Note. SDM = shared decision-making; SEED = Seeking information, Engaging in conversation, Exploring options, and Deciding on treatment; RN = registered nurse.
The CPS was incorporated during patient face time. The nurse presented the five cards in random order to each patient. The patient ranked the cards from most preferred to least preferred. The nursing staff communicated this preference to the health care team during the treatment team meeting. Depending on the length of a patient’s stay, their preference could be assessed more than once and could change. Patients who preferred a collaborative role were scheduled a discharge meeting before discharge.
Each day, the coach assigned to the shift recorded how many patients had engaged in the intervention (SEED at assessment and CPS during patient face time) as reported by the nursing staff on the treatment team sheets. Patient presence at discharge meetings was also documented on the team sheets. After treatment team meetings, the team sheets were stored in the clinical team leaders’ office which was locked when not in use. Web conference meetings were conducted by the PL with coaches and nursing staff daily, and with the health care team at least weekly to maintain compliance and sustainability of the practice change. Patients were given the Press Ganey patient experience survey on the day of discharge, and completed surveys were collected prior to discharge.
Process Outcome and Evaluation
The primary outcomes were as follows: (1) the scores to the “the degree to which to you felt included in decisions about your care” on the Press Ganey survey and (2) the number of discharge meetings where patients were present. The process measures evaluated were the number of staff who attended the educational sessions and the number of patients who used the CPS.
Measures
The implementation process was measured by (1) number of staff attending training, via documentation on a training sign-in sheet; (2) number of patients the nurse was able to use the SEED model with on admission assessment; and (3) number of patients who used the CPS tool.
To evaluate the percentage of patients participating in discharge meetings, a run chart was used. To determine if the practice change increased engagement in care, the number of patients who reported satisfaction with “The degree to which you felt involved in your care” and the number of patients who participated in discharge meetings was collected. This project was reviewed by the Institutional Review Board (IRB) at the Medical University of South Carolina and received the determination of non-human subjects’ research.
Analysis
Data were analyzed with descriptive and inferential statistics. Descriptive statistics determined the percent of staff attending training and percent of patients who engaged in the SEED model with the nurse on admission and the percent of patients who used the CPS during their admission.
A chi-square test determined if there was a difference in the percentage of patients who were satisfied with involvement in their care per the indicated question on the question Press Ganey survey. A chi-square test was also used to determine if there was a difference in the number of patients who attended discharge meetings in the 2 months before the intervention month compared to the 2 months afterward (the initial implementation month was not included). It is important to note that the number of patients who were admitted to the unit and therefore potentially able to participate with the nurse who used the SEED model for admission assessment was different than the number of patients who were hospitalized during the evaluation period and were able to use the CPS. The number of patients discharged during the evaluation period was also different. Therefore, the denominator for analysis of each measure is different.
Results
Process Measures
Training
Overall, 100% of the nursing staff completed the training on the SEED model and the CPS. Patients participated in the SEED model with their nurse on 50% of admission assessments (30 out of 60 admissions). And, 68% of patients also used the CPS to communicate their preferences for involvement in their care. Of the patients who used the CPS (N = 61), 76% preferred collaborative, active-shared, or active participation in decisions about their care.
Outcome Measures
Press Ganey Survey
Following implementation of the SEED model and CPS, the return rate of the Press Ganey survey remained low. For the 2 months before the intervention, it averaged 29%, and in the 2 months after the intervention, it was 36%. Responses to “the degree to which you felt involved in your care,” also demonstrated little change in satisfaction from 85% pre-implementation to 87% post-implementation (p = .12).
Involvement in Discharge Meetings
Discharge meetings with the presence of patients increased after the intervention, improving each month (Figure 1). Pre-intervention, 31% of discharge meetings included patients; following implementation, 53% of discharge meetings included patients (p < .00).
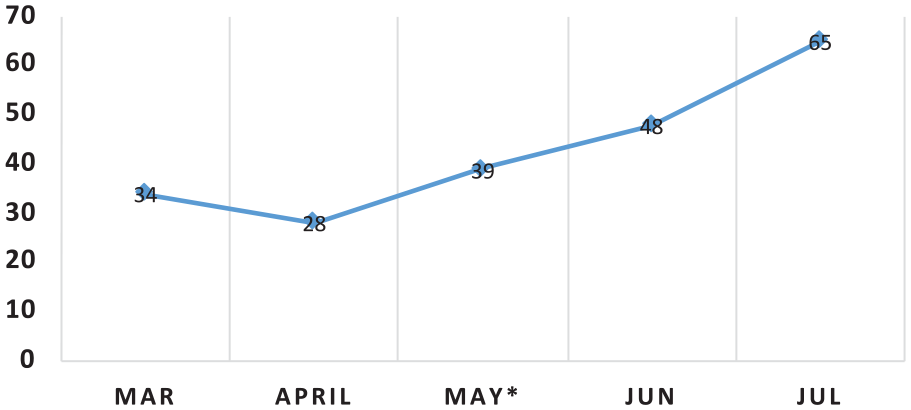
Percentage of Discharge Meetings with Patient Present
Discussion
Summary
Use of the SEED model and CPS by nurses was effective in increasing patients’ involvement in their treatment. Overall, 50% of patients were able to engage with nurses on admission and 68% of patients used the CPS during the 2-month evaluation period. Patient presence at discharge meetings increased significantly although Press Ganey scores evidenced minimal change.
Interpretation
Although Tambuyzer and Van Audenhove (2013) reported a correlation between increased patient involvement and patient satisfaction, the increase in patient satisfaction with perceived involvement in care scores on the Press Ganey survey in this study is small. It cannot be attributed to the practice change, especially with the continued low patient completion percentage. However, the significant increase in patient involvement in discharge meetings suggests the SEED model and CPS together were effective tools for incorporating SDM on our unit. Some patients were not able or chose not to engage with the nurse on admission or use the CPS tool. The CPS outcomes were consistent with previous studies that patient involvement can improve collaboration and engagement (Dixon et al., 2016; Duncan et al., 2010). The percentage of patients preferring collaborative involvement in decision-making was lower at 36% than in a previous report of patients with mental illness at 57.5% (Michaelis et al., 2017).
In addition to the primary and secondary outcomes, nursing staff disclosed in informal meetings that they learned more about their patients through their participation in this project and felt empowered by the change in practice. Patients were also empowered to share in their care as evidenced by the increase in participation in discharge meetings. More research is needed to investigate if these tools can improve patients’ adherence to their treatment plans.
One unexpected result of the project anecdotally reported by nurses was how patient preference changed from admission to discharge. Although 68% of the patients ultimately chose active, active-shared, or collaborative preferences, many of them had chosen passive or no preference at all when first admitted to the unit. This shift in preference might be a reflection of their illness and how as their mental status improved, they were better able to assume a more active role in their treatment.
Limitations
The PL was not allowed to be physically present on the unit per hospital policy. Therefore, the PL could only provide implementation support and guidance via videoconferencing. Videoconferencing was a novel way to provide leadership and was probably accepted by the unit leaders and staff because of the PL’s prior role as the lead PMHNP on the unit. This frequent contact during implementation kept the leadership and staff motivated and informed.
The number of patients on the unit was also smaller than anticipated to have rooms available for COVID-19 patients. Some patients were not able to engage in logical conversation and were experiencing psychosis or catatonia. Therefore, they did not participate in the admission assessment using the SEED model or the CPS. Thus, the total sample size was 140 patients (80 in the 2 months before the intervention and 60 in the 2 months after the implementation).
The low survey response rates make any association between a practice change on the unit and Press Ganey survey results tenuous. Efforts to increase the completion of the survey by patients and collection for at least one quarter (3 months) could provide stronger evidence of a true change in this outcome related to the practice change. As a quality improvement project, patients were not “enrolled,” and data were not collected in an identifiable way so that connecting who completed the tools and whether they completed the Press Ganey surveys could not be made. This limits the ability to determine the association between the practice change and the patient satisfaction scores. However, as a quality improvement project, the results were not intended to be generalizable, but it is hoped that the processes can be transferable and adapted to other similar settings and populations.
While COVID-19 moved training online and limited the amount of time available for data collection, the pandemic did not appear to affect the project’s quality or results. The training was still fully executed, and staff and leadership remained highly supportive of and compliant with the intervention.
Conclusion
While the low Press Ganey satisfaction scores were the impetus for the administrative support of interventions to improve patient engagement and satisfaction, the outcome that reflects real change was the increased participation by patients in their care evidenced by the increase in attendance at discharge meetings. This project challenged the culture of this behavioral health unit. Some health care team members may assume that patients who are in acute crisis do not want to be involved in their care. However, by implementing engagement tools, members of the health care team found that these patients seek involvement regardless of their diagnoses. Providers changed their approach to patient treatment and discharge plans and sought to understand more about the use of SDM.
The project is sustainable due to ongoing support from the patient–family advisory committee and administration. The leadership team continues to discuss expanding this intervention following the pandemic and in the care model for the planned grand opening of a new 42-bed behavioral health department. Recognizing the effectiveness of SDM gives our patients a voice and is a first step toward improved patient engagement in their care. The next steps will be to learn to nurture and critically listen to that voice to evolve patient care.
Footnotes
Acknowledgements
Shana Williams is no longer affiliated from Recovery Innovations International, Phoenix, AZ, USA.
Authors Note
Shana Williams is no longer affiliated from Recovery Innovations International, Phoenix, AZ, USA.
Author Roles
All authors contributed to the conception or design of the study or to the acquisition, analysis, or interpretation of the data. All authors drafted the manuscript, or critically revised the manuscript, and gave final approval of the version that was submitted for publication. All authors agree to be accountable for all aspects of the work, ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.