
Abstract
The assist-as-needed technique in robotic rehabilitation is a popular technique that encourages patients’ active participation to promote motor recovery. It has been proven beneficial for patients with functional motor disability. However, its application in robotic therapy has been hindered by a poor estimation method of subjects’ functional or movement ability which is required for setting the appropriate robotic assistance. Moreover, there is also the need for consistency and repeatability of the functional ability estimation in line with the clinical procedure to facilitate a wider clinical adoption. In this study, we propose a new technique of estimation of subject’s functional ability based on the Wolf Motor Function Test. We called this estimation the functional ability index. The functional ability index enables the modulation of robotic assistance and gives a more consistent indication of subjects’ upper-limb movement ability during therapy session. Our baseline controller is an adaptive inertia-related controller, which is integrated with the functional ability index algorithm to provide movement assistance as when needed. Experimental studies are conducted on three hemiplegic patients with different levels of upper-limb impairments. Each patient is requested to perform reaching task of lifting a can from table-to-mouth according to the guidelines stipulated in the Wolf Motor Function Test. Data were collected using two inertial measurement unit sensors installed at the flexion/extension joints, and the functional ability score of each patient was rated by an experienced therapist. Results showed that the proposed functional ability index algorithm can estimate patients’ functional ability level consistently with clinical procedure and can modify generated robotic assistance in accordance with patients’ functional movement ability.
Keywords
Introduction
The assist-as-needed (AAN) robotic strategy is a popular strategy for encouraging patients’ active participation in robot-assisted rehabilitation therapy. Numerous clinical outcomes have suggested the effectiveness of the AAN scheme to induce neuroplasticity in patients with neurological impairment. 1 The AAN strategy focuses on providing the minimal amount of robotic assistance necessary for a patient to complete a movement, 2 thus a significant effort is required from the patient. If the patient can perform the task flawlessly, robotic assistance is withdrawn. However, if the patient cannot complete the given task, assistance is offered only as much as it is needed. 3
Deploying robotic assistance in accordance with the AAN strategy still come with many shortcomings.3,4 One major issue is how to appropriately estimate patients’ functional ability to set the correct level of robotic assistance. Another issue is the consistency of the estimated subject’s functional ability with clinical data and the repeatability across a wide range of subjects. An appropriate estimation of subject’s functional ability consistent with clinical data can give a realistic basis for deploying robotic assistance, since it gives a measure of subject’s actual disability level or recovery progress.5,6
A few strategies of AAN have been proposed recently which have attempted to address the challenges in the scheme. Wolbrecht et al. 7 proposed a model-based robotic assistance strategy which can enable a robot to learn the patients’ ability in real time based on a radial-basis function (RBF). The RBF is applied under an adaptive control framework.
Another AAN strategy was proposed by Pehlivan et al. 3 The authors introduced a minimal assist-as-needed (mAAN) strategy which uses a Kalman filter to estimate subjects’ functional inputs instead of the RBF technique that is a sensor-less force estimation strategy. Under the scheme, the ANN strategy is achieved in the following two ways: (1) by updating the derivative feedback gain to modify the bounds of allowable error on the desired trajectory and (2) by decaying a feed-forward disturbance rejection term which reduces the constraint on allowable quick movements. The combined effect could vary the robotic assistance according to the subjects’ capability. 8 The potential limitation of this approach is the reliance on the robot model for the estimation of subject’s capability. It is well known that model errors always exist and can significantly excite the disturbance term making it difficult to accurately estimate the subject’s input. There is the implication that different robot models would produce different functional ability estimates which will hinder an appropriate standardization or deployment of robotic assistance for clinical purpose.9,10
Pérez-Rodríguez et al. 11 also introduced an AAN strategy called anticipatory assistance-as-needed control algorithm capable of ensuring that the deviation from a patients’ desired trajectory is restored by giving an anticipated force assistance. This way, robotic assistance is always given as a restoring force to maintain the subject on the reference (desired) trajectory. With regards to the validity of this strategy, there are however no experimental studies till date.
Other noteworthy AAN strategies include the rule-based assistive strategy proposed by Wang et al., 12 which is applied in Physiotherabot; the hybrid impedance control for wrist and forearm rehabilitation proposed by Akdoğan and Adli, 13 which is applied on a 3-degree-of-freedom (3-DOF) upper-limb rehabilitation robot; and the visual error augmentation-based AAN proposed by Akdoğan et al., 14 which can provide robotic assistance as needed by amplifying tracking error to heighten the participant’s motivation.
Efforts in developing an appropriate estimation strategy for AAN robotic assistance are still on course; 15 however, there has been less focus on developing appropriate estimation techniques of subject’s functional ability that are consistent with the clinical procedure and that can be integrated in the control loop to provide robotic assistance.15,16
In this paper, we propose an ANN strategy to direct robotic assistance based on a novel functional ability index (FAI). The main originality of this work is the derivation of the new FAI estimation algorithm in accordance with the clinical procedure for the estimation of subject’s motor ability in movement task. As a preliminary investigation, we derive our FAI following the Wolf Motor Function Test (WMFT), a popular motor function test with consistency over a wide range of neurologically impaired patients. The FAI serves as input to a decay algorithm under the adaptive control law which consequently varies the robotic assistance according to the subject’s functional ability. The FAI is independent on the robot model or controller adaptation law and thus it is unaffected by modelling uncertainties.
The rest of the paper is organized as follows: section ‘System dynamic and control’ presents the dynamics for the robotic rehabilitation system, the proposed FAI, and the proposed control algorithm. Section ‘Experimental study’ presents the data collection and simulation study; section ‘Results’ describes the results; section ‘Discussion’ presents the discussion; and section ‘Conclusion’ concludes the paper.
System dynamic and control
The mechanical system
The proposed prototype of the exoskeleton system is shown in Figure 1. The system is an upper-limb rehabilitation robotic device with two active degrees of freedom (DOFs) at the shoulder and elbow joint, respectively. If actively controlled, the exoskeleton can permit abduction/adduction (AA) movement of the shoulder joint and flexion/extension (FE) movement of the elbow, thus allowing the possibility of performing the table to mouth reaching task.
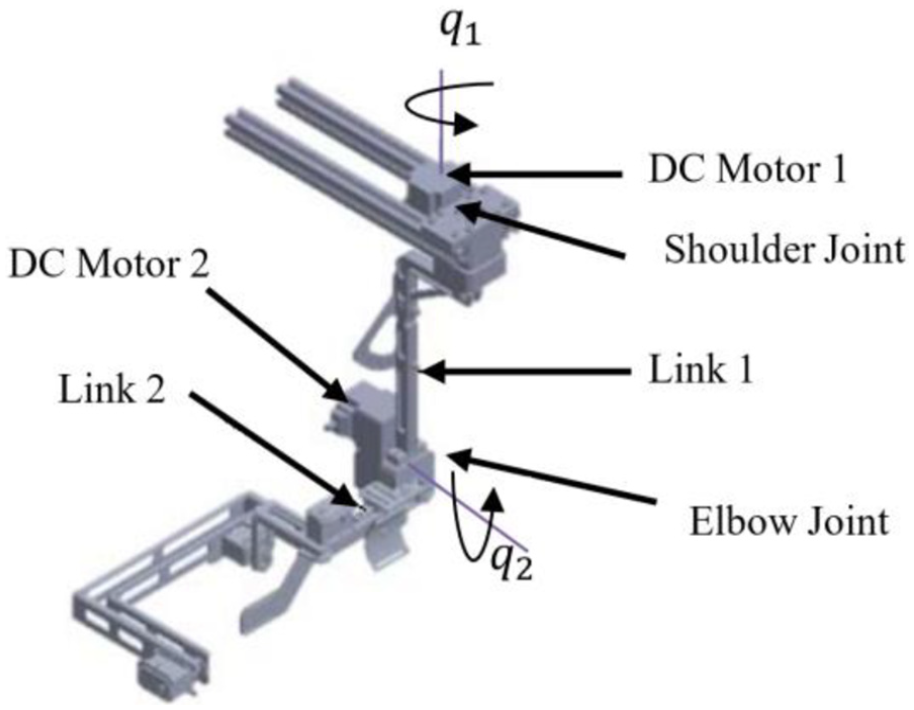
Exoskeleton device is of 2 degrees of freedom (DOFs).
The device employs back-drivable brushless DC motors for actuation, which are specially chosen to offer low noise, low friction, low backlash, and compact size. Torque sensor with strain gauge mechanism and potentiometer for position measurement are attached at each active joint. The active joint of the shoulder and elbow joint of the exoskeleton are actuated with a DC electrical motor (Maxon RE50, 370955, 200 W, 36 V) with a gear ratio of 1:113. The exoskeleton range of motion and permitted movements are shown in Table 1.
Proposed exoskeleton range of motion.
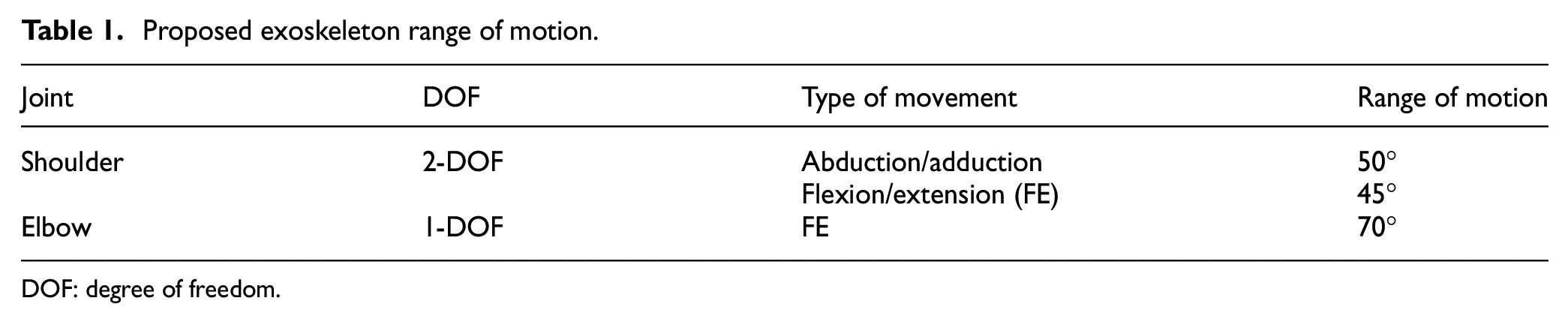
DOF: degree of freedom.
The robot dynamic equation
The equation of motion of the proposed prototype robotic system based on the Euler–Lagrange equation 17 can be expressed as

where q is a 2 × 1 vector of joint position of the exoskeleton robot. M is the inertial matrix which is a 2 × 2 matrix, C is the 2 × 2 vector of Coriolis/centrifugal forces, G is a 2 x 1 vector which represents the gravity term,
FAI estimation
Functional ability is the capacity of an individual to perform activities and tasks involved in daily living. 18 Functional ability is needed to determine patients’ recovery progress or disability level. It also provides useful information that can guide therapists in prescribing appropriate treatment for patients. Measurement of functional ability is commonly done by assessing the ability of a patient to perform ‘activities of daily living’ (ADLs): by questioning the individual or by observing how an individual can carry out a given task.19,20 In robot-aided therapy, this procedure is however tedious, inconsistent, and time-consuming.
In this section, we introduce a standardized approach, consistent with the clinical procedure, to estimate the patients’ functional ability level based on a popular motor assessment strategy, namely, the WMFT. The WMFT quantifies upper-limb motor ability through timed and functional tasks 21 as shown in Table 2.
WMFT–Adapted functional ability scale
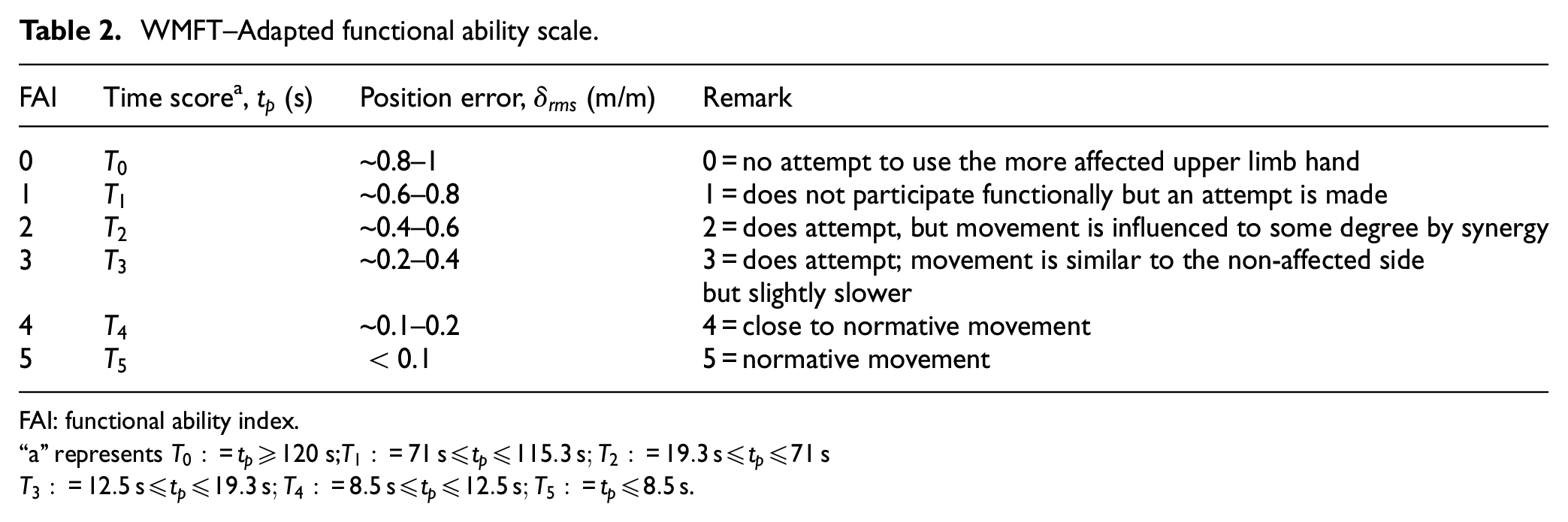
FAI: functional ability index.
“a” represents
Table 2 presents a modified WMFT scoring technique adapted from the work of Whitall et al.
22
and Edwards et al.,
23
where
The proposed FAI is developed by utilizing the statistical normalization function24–26 given as

where
The healthy subject has the maximum measurement for speed
By applying equation (2) (taken

Thus, by using equation (3), the FAI for only velocity index,

where
Similarly, by using equation (3), FAI for only time index

where
The FAI for position can similarly be derived from equation (3) but with slight adjustment as

where
The overall FAI

ANN decay algorithm
Similar to the work proposed by Pehlivan et al.,
3
we define a decay algorithm that relies on the modification of the error. This is achieved by modulating the gain,

where
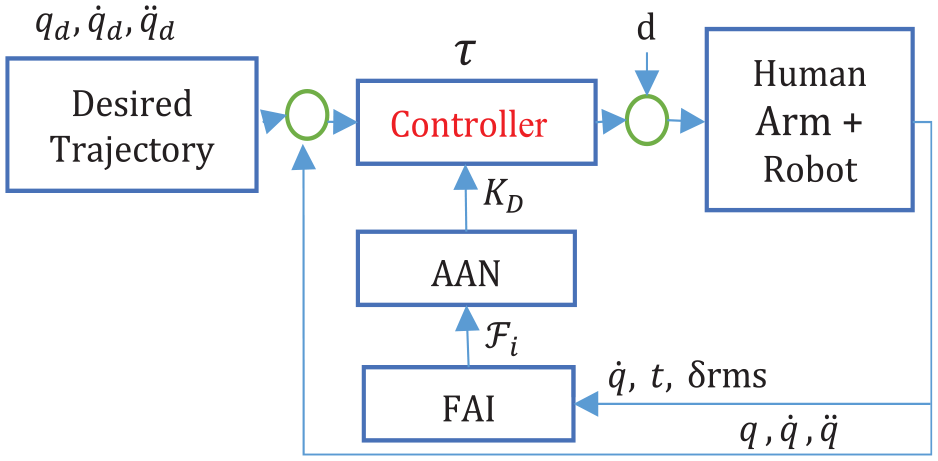
AAN adaptive controller framework.
Control architecture
Good tracking performance in the presence of uncertainty in the robot’s environment is often achieved using adaptive controllers. The robot environment in our case is the human upper limb whose mass and moment of inertia vary among different subjects. We apply the adaptive inertia-related torque controller in this study as the baseline controller to enable modification of the error bound and modulation of the assistive torque. In line with Van den Brand et al., 27 we define the control law as

where

For parameter adaptation, in accordance with the study by Lewis, 19 we adopt the updated rule given as

The designed AAN controller is intended to provide robotic assistance based on task 9 of the WMFT in an accurate manner. For this control strategy, an inner position loop is designed around the outer torque feedback loop. Therefore, the inner motion control guarantees the tracking of the reference trajectory. The desired torque is computed based on the
Experimental study
Experimental setup
The study is designed to follow task 9 of the WMFT 21 in which subjects are to perform a reaching task of grasping and moving a 340 g bottle from the table to the mouth. A table of suitable height with an adjustable chair is selected to enable the subjects to effectively perform table to mouth reaching task as shown in Figure 3. The main instrument used in the experiment is the inertial measurement unit (IMU) for determining angular position and velocity of the upper-limb joints (i.e. elbow and wrist joints). One sensor is fixed to the elbow base, and another one is attached to the user’s wrist as shown in Figure 3. All experiments were conducted on the flexion and extension joint using the two IMU sensors and MATLAB/Simulink (The MathWorks, Inc.) for computational analysis.
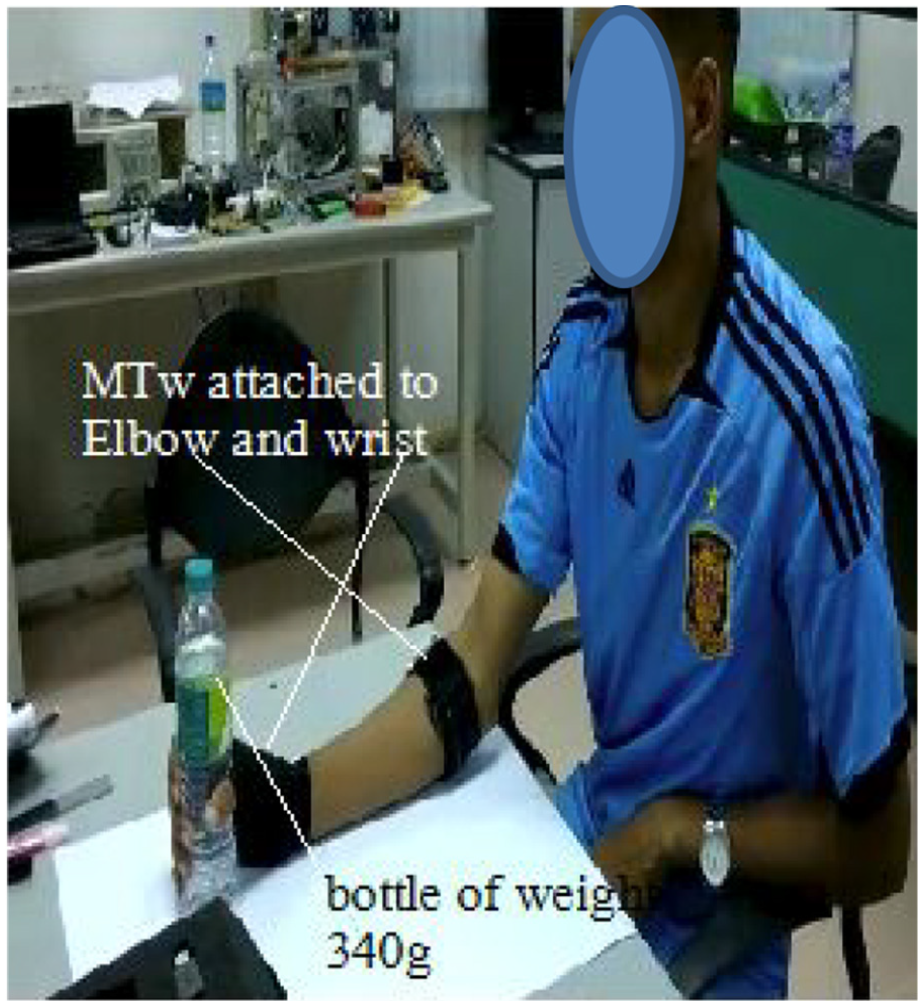
Experimental apparatus attached to the user’s hand.
Participants
Three hemiplegic patients were recruited from the Heritage Physiotherapy Rehab Centre, Ampang, Kuala Lumpur, Malaysia, in January 2019, within the timeframe of study. The case file of each patient was documented before the experimental session. Details of the patients’ pathologies are given in Table 3. The reference group constitutes seven healthy participants with a mean age of 32 ± 6 years and weight 70 ± 7 kg earlier recruited at the Bio-mechatronics Research Laboratory, International Islamic University Malaysia (IIUM). All participants willingly gave their consent to participate in the experiment.
Post stroke patients’ details.
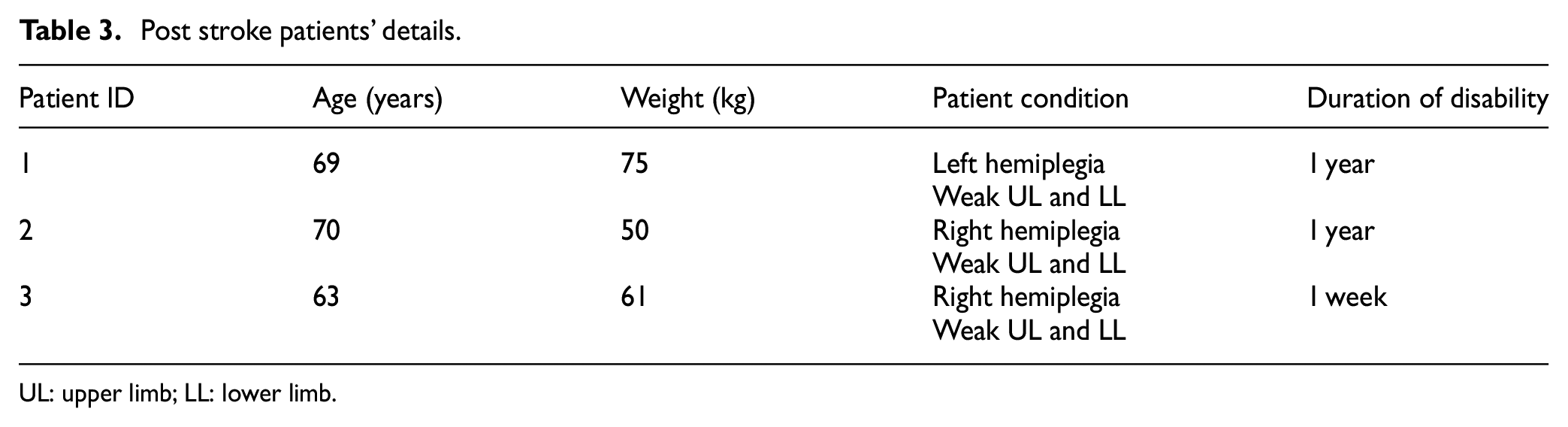
UL: upper limb; LL: lower limb.
Procedures
The experiment was performed to test and validate the feasibility of the proposed method. Participants were seated in an adjustable chair and asked to place their forearm on the table. Figure 4 shows one participant performing the table to mouth reaching task.

Three different positions of the participants.
Before the start of each training session, participants were given instructions to follow. Each participant was requested to perform a normal table-to-mouth reaching motion while grasping the 340 g bottle. The participant is instructed to repeat the task three times. The angular position and velocity of completion of each movement were recorded from the IMU. The time of completion of each task was recorded with a stop watch. If any participant could not complete the reaching task within 120 s, the experiment is terminated, and the participant is given a functional ability score (FAS) of zero.
Data collection and analysis
IMU sensor data for elbow and wrist joints were collected from the participants. Particularly, the pitch angle data for the joints, as shown in Figure 5, were utilized in the experimental analysis. The steeper curve with bold black represents the joint angular position measurement of the healthy participant, whereas the curve with the dotted line represents mean score from participants with severe disability. The slope of the curve gives indication of how fast a participant is able to perform the reaching task with relation to the disability level.
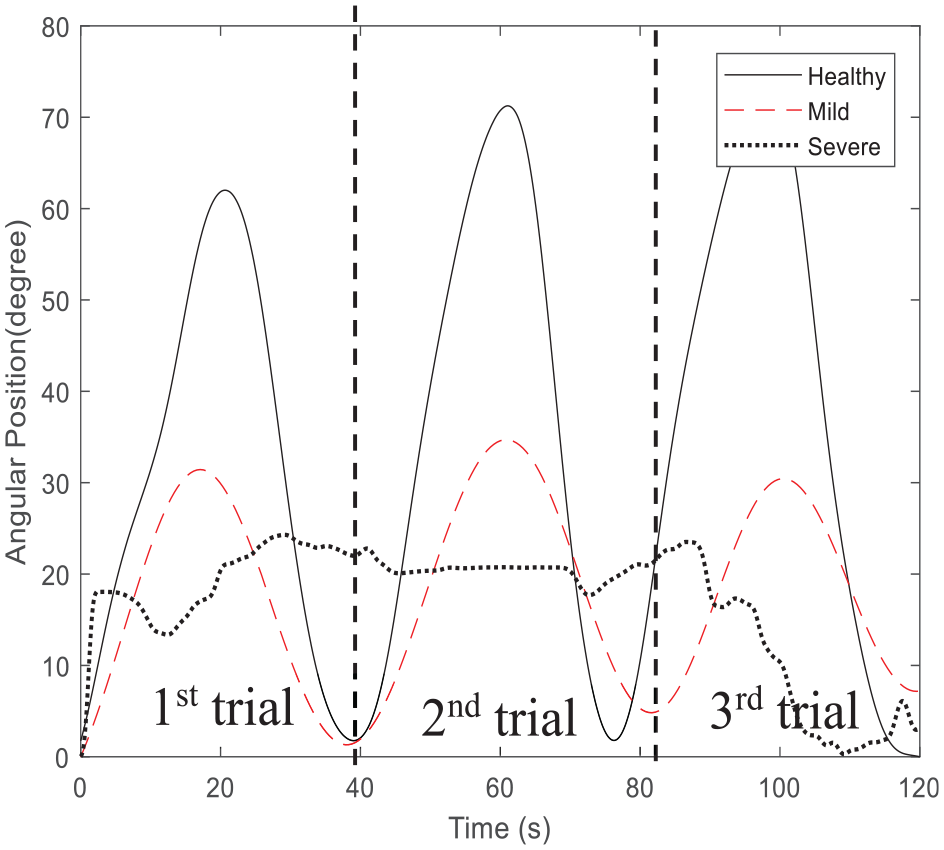
Position data: patients of healthy, mild, and severe participants.
Results
In this section, we present results of experimental verification of the proposed FAI-based AAN strategy. Three aspects are evaluated: real-time computation of the FAI, the corresponding derivative gain KD, and the generation of the controller assistance torques. Simulation is done in the MATLAB/ Simulink (The MathWorks, Inc.) for computational analysis.
FAI estimation
Based on the experimental procedure, we classify the outcome from the participants into three levels: healthy, mild and severe disability. The estimated FAIs for the healthy, mild, and severely-disabled subjects are shown in Figure 6. The figure gives the variation in the estimated subjects’ FAI for each trial.
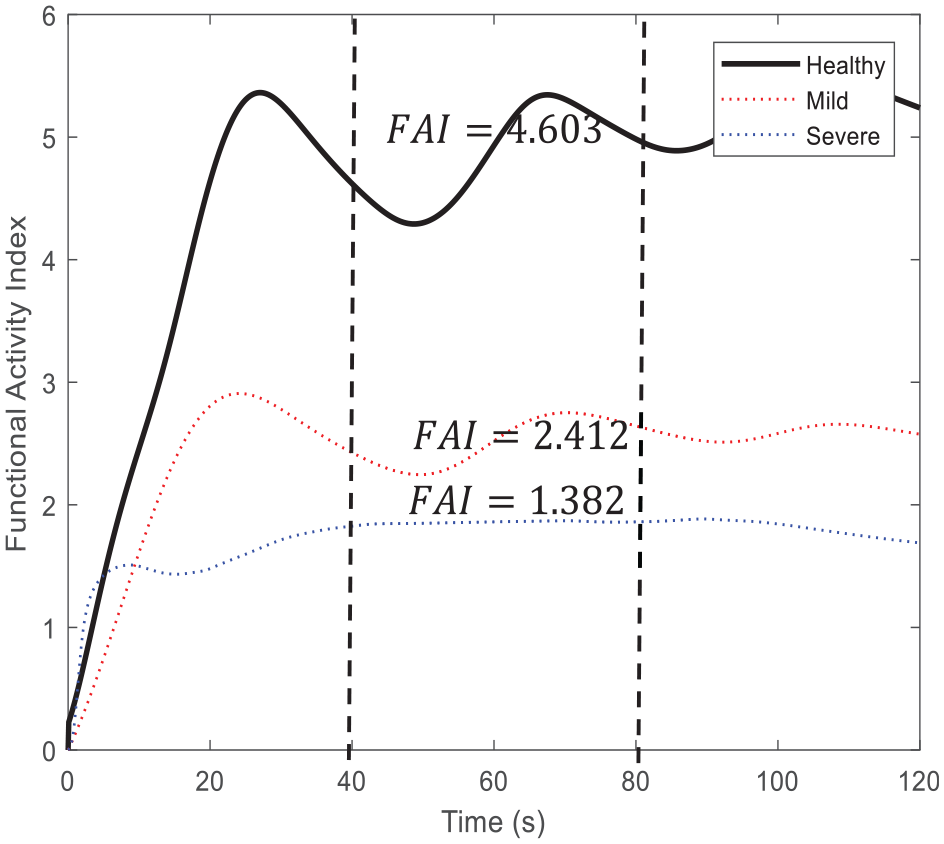
Functional ability index for the healthy, mild, and severe participants.
The mean time score, FAS, and the estimated FAI score for the (seven) healthy participants were found to be
Mean FAI estimation of the participants.
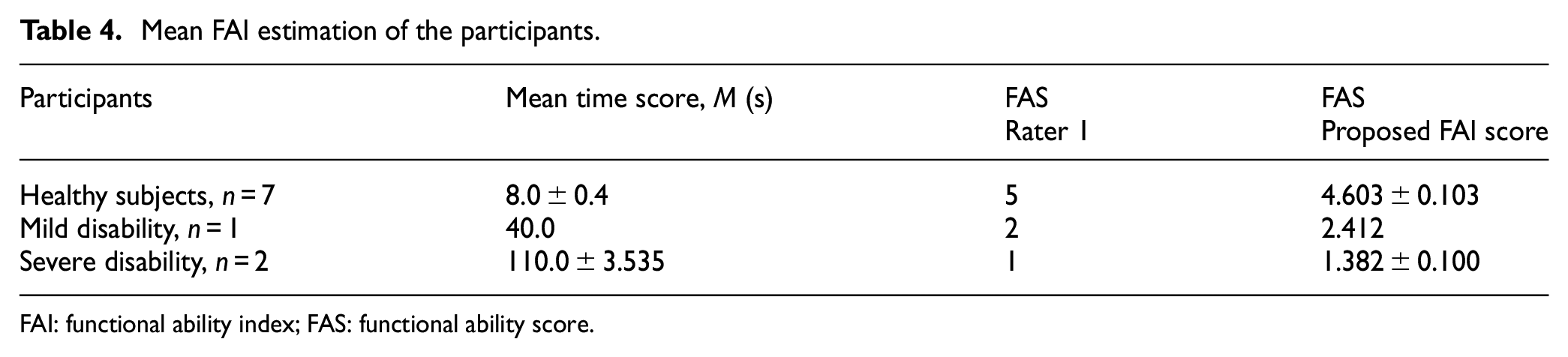
FAI: functional ability index; FAS: functional ability score.
Computation of the KD
The result of computation of the derivative gain, KD, based on equation (10) is shown in Figure 7. The adjusted feedback gain KD is computed concurrently with the FAI for each trial. For this experiment, the adjusted KD for the severe, mild, and healthy participants were 119, 81, and 45 N m s/degree, respectively.
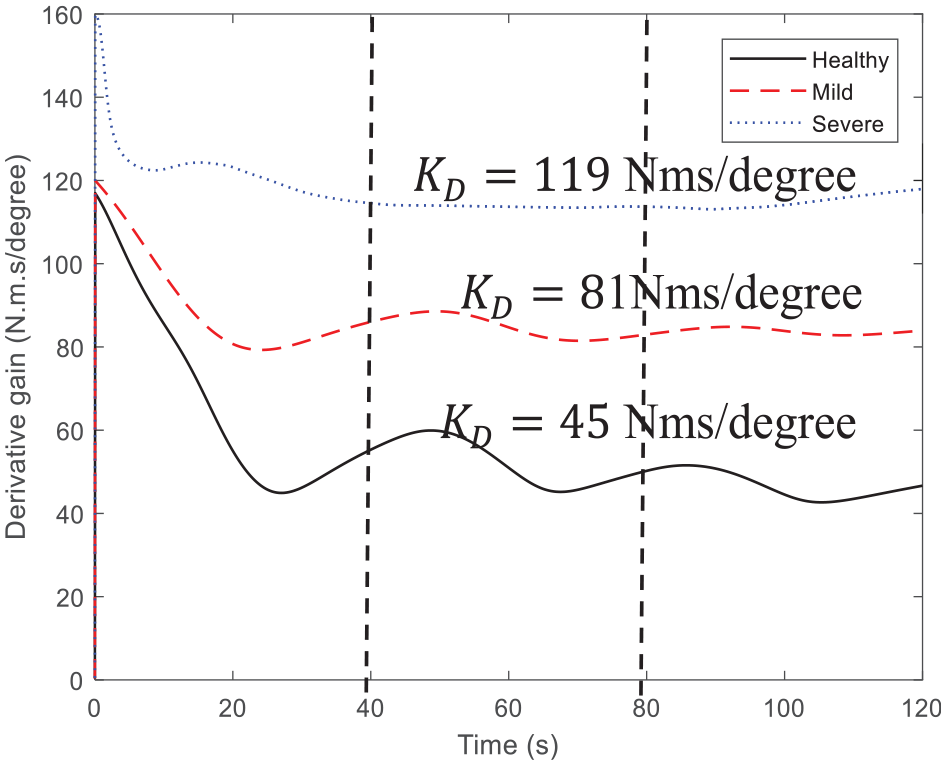
Derivative gain for healthy, mild, and severe participants.
Torque assistance
The assistive torque from the adaptive inertia controller for the three groups is depicted in Figure 8. The torque assistance also increases correspondingly with the estimated subjects’ FAI. The highest torque is produced for the participants with severe case of disability, while the least is given for the healthy subjects. This variability proves the capability of the FAI-based controller to provide assistance in accordance with the estimated disability levels.
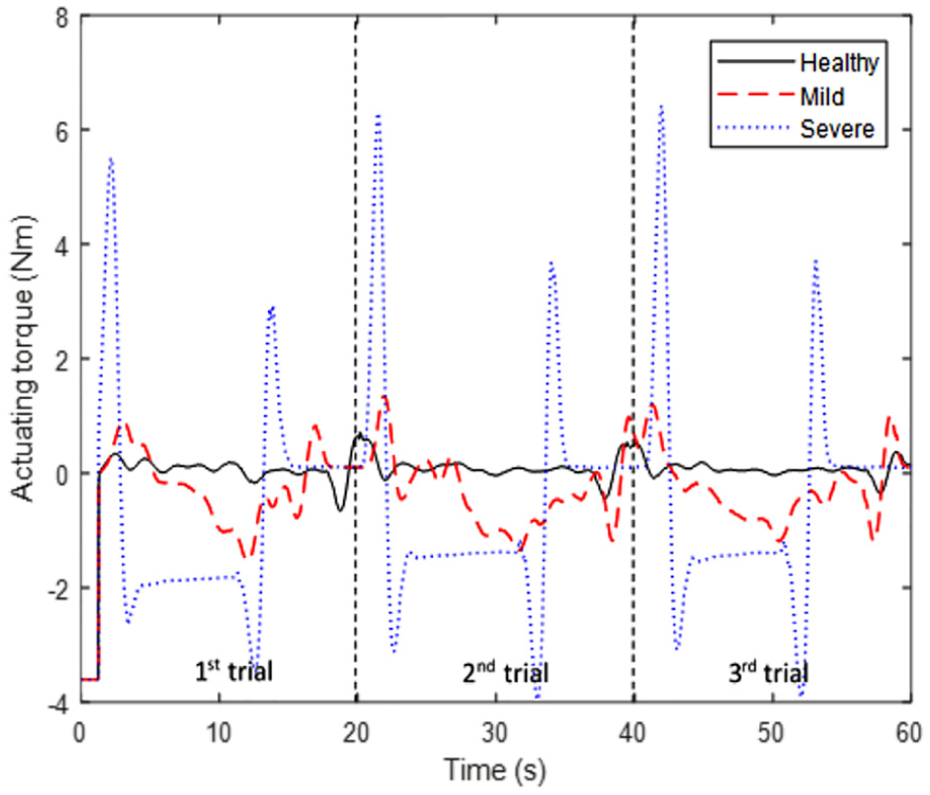
Joint actuating torque.
Discussion
The results of the experiment show that the proposed FAI algorithm can estimate patient’s disability level consistently with clinical method (i.e. WMFT). The estimated FAI decreases correspondingly with the subjects’ disability level, the more severely disabled having FAI = 1. Based on Figure 6, the healthy subjects produced the highest mean FAI score of approximately 4.603 ± 0.103 during the table-to-mouth reaching task, whereas the participants with severe disability achieved the least mean FAI score of approximately 1.382 ± 0.100, as shown in Figure 6. These values were consistent with the rating of patients’ disability level by experienced therapist (Table 4). The results also show that the proposed FAI-based AAN control can vary the assistive torque in accordance with the participants’ functional ability. The torque assistance is automatically adjusted by the computed derivative gain
Conclusion
In this article, we have proposed an AAN control strategy based on subjects’ FAI. Preliminary experiments have been conducted on three clinically identified hemiplegic patients with different degrees of disabilities and seven healthy participants used as the reference group.
The estimated FAI and torque assistance based on data from IMUs (position, velocity, and time) show consistency in the patients’ level of disability, which indicates the suitability of this estimation technique for AAN robotic application in clinical settings.
Future work will involve implementing the proposed control strategy on an actual robotic platform for upper-limb rehabilitation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received financial support from International Islamic University Malaysia P-RIGS Grant (grant number: P-RIGS18-019-0019) for the research and publication of this article.