
Abstract
Objective:
Extended reality (XR) has emerged as an innovative educational modality that offers the potential for the creation of more interactive and engaging forms of patient education experiences and products. The purpose of this article is to describe the field of XR technologies and review its potential through a critical lens as well as its possible adoption as a mainstream technology for providing patient education in the future.
Method:
A review of the literature was undertaken to summarise the emerging evidence concerning the effectiveness of XR as a patient education modality. The findings of several reviews are summarised and a critical discussion of potential issues and challenges in the adoption and use of XR among particular marginalised populations are explored.
Results:
The emerging evidence suggests that different forms of XR technology applications have the potential to create immersive and engaging patient education experiences that can lead to enhanced patient satisfaction, positive educational outcomes and reduced patient anxiety. Nonetheless, there have been calls for greater consideration of how patient characteristics, including socioeconomic status, gender, cultural and generational differences, influence the learning effects of virtual reality educational applications, as well as its adoption and implementation for patient education purposes.
Conclusion:
The evidence surrounding the effectiveness of XR in patient education is growing; however, various factors could influence the successful adoption and implementation of XR in different patient populations who have traditionally experienced challenges with digital health literacy. The paper offers some recommendations for enhancing the evidence base and potential approaches to advance the design and evaluation of XR applications in patient education.
Introduction
Patient education is key to helping patients understand the information communicated by their healthcare providers. Patient education has been described as the process of influencing patient behaviour and affecting changes in knowledge, attitudes and skills to maintain or improve health (Slond et al., 2021). Effective patient education is an important aspect of patient-centred healthcare, a key goal being to empower patients with the knowledge for self-management and making good healthcare decisions (Adapa et al., 2020). Patients who are better informed about their medical condition are more likely to be satisfied with their healthcare, adhere to their treatment plan, experience better provider-patient relationships, and achieve more positive health outcomes (Adapa et al., 2020; van der Kruk et al., 2022; Urlings et al., 2022).
However, key barriers to achieving a high-level understanding of sometimes complex procedures include limitations in patients’ health literacy and healthcare providers’ ability to communicate this information clearly (Shepherd et al., 2022). There is often a generally low percentage of information recall among patients and widely diverging perspectives between patients and professionals. Health information that is too complex can lead to cognitive overload, resulting in patients being unable to process and remember the information being conveyed (van der Kruk et al., 2022). The causes of low information recall have been attributed to high levels of anxiety, patient age, low comprehensibility of the information provided, and low perceived importance of medical information (Urlings et al., 2022). Shepherd et al. (2022) have also suggested that clinicians often overestimate the ability of patients to understand medical and other health-related information.
The development of electronic health records and the more recent emergence of virtual care during the COVID-19 pandemic have led to increasing adoption of digital health tools. Digital health has expanded to include a wide variety of technologies, including health-related apps, wearable devices, and online medical resources to help people make informed decisions about self-management and health care (Canada Health Infoway, 2021). This increasing ‘digitisation’ of health systems, health information and access to health care has introduced new challenges for various segments of the patient population. Digital health literacy has become increasingly important and has been defined by the World Health Organisation as the ability to seek, find, understand and appraise health information from electronic sources and apply the knowledge gained to addressing or solving a health problem (World Health Organization [WHO], 2019).
Digital health literacy encompasses the application of both health and digital literacy skills to confidently and accurately use tools and information to manage health-related questions or care. However, lack of access to digital tools, usage patterns, and the ability to effectively use digital technologies has been shown to affect digital health literacy among patients (Estrela et al., 2023). Living in rural or remote communities, educational level, socioeconomic status and being older are other factors that also influence digital health literacy. Digital health literacy has important implications for the design, adoption and implementation of new digital health tools in healthcare delivery.
This article discusses the growth of extended reality (XR) as a new technological innovation in the patient education field. There is emerging evidence concerning the effectiveness of XR in patient education; however, digital health literacy and various characteristics of the patient population have important implications for how XR applications are designed and implemented to facilitate greater access, adoption and implementation in healthcare delivery. Using a critical lens, this paper offers some suggestions about strategies and principles that can be applied to advance the design and evaluation of XR applications in patient education.
XR and patient education
In recent years, there has been growing experimentation and adoption of different technological solutions to educating patients and promoting better health literacy (Adapa et al., 2020). Diverse ways to educate patients regarding health information are being explored, with XR emerging as a new innovative option. XR is an umbrella term referring to a wide range of immersive technologies including virtual reality (VR), augmented reality (AR), mixed reality (MR) and other computer-generated realities using head-mounted displays (HMDs) (Curran et al., 2022). Wearable devices such as HMDs (e.g. virtual headsets, smart glasses) can be used in XR simulations and are worn on one’s head as part of a helmet that has an optical display, allowing users to view projected imagery (Curran et al., 2022) (Figure 1). VR headsets produce the experience of total immersion in a three-dimensional (3D) space with stereoscopic views of a scene (i.e. by means of a pair of images, one for each eye) (Curran et al., 2022; Ros et al., 2017).

Older adult using an HMD and VR for patient education.
Patient understanding is a key factor in determining informed consent for procedures and treatment options. Informed consent demands a detailed discussion regarding the risks and possible side effects of treatments and alternative management approaches. However, promoting a high level of patient understanding of diagnostic and prognostic information is challenging due to multiple potential barriers including patient health literacy and the healthcare providers’ ability to communicate complex health information clearly. In addition, stress and anxiety have been shown to limit a patient’s ability to listen, learn and remember (Shepherd et al., 2022). Learning and understanding can be enhanced by adopting audiovisual tools such as XR and this may be important for enhancing communication between patients and healthcare professionals because it reduces literacy barriers (Slond et al., 2021).
Several VR concepts are believed to influence the effectiveness of these technologies when used for education and training. ‘Immersiveness, or feeling the sense of presence’ and ‘interactivity’ have been partially cited as key reasons for the adoption of VR in patient education (Slond et al., 2021). According to Witmer and Singer (1998), immersion refers to ‘a psychological state characterised by perceiving oneself to be enveloped by, included in, and interacting with an environment that provides a continuous stream of stimuli and experiences’ (p. 227). A high degree of immersion contributes to an increased level of presence, or ‘the subjective experience of being in one place or environment, even when one is physically situated in another’ (p. 225). Presence has been identified as a key factor in immersive learning experiences as well as a key feature of VR that is conducive to learning.
‘Co-presence’ is a significant concept also highlighted in the VR literature with implications for more meaningful user experiences. The term refers to the extent to which a user perceives a virtual human (VH) in a virtual environment while at the same time sensing that the ‘other’ can perceive the presence of the user (Kyrlitsias and Michael-Grigoriou, 2022). A VH is a perceivable digital representation of a human in a virtual environment and can be categorised as either an avatar or an agent (Kyrlitsias and Michael-Grigoriou, 2022). Avatars are VH representations where the behaviours are reflective of the actual human user, whereas an agent is a VH whose behaviours are determined by computer algorithms (Kyrlitsias and Michael-Grigoriou, 2022). Co-presence reflects the experience of being together in a virtual setting with another social being, whether an avatar or an agent.
Embodiment is another concept in the VR literature that refers to the use of gestures and body movements in virtual environments to enable multi-sensory forms of interaction, including possible tactile and auditory sensory experiences. It is believed that accented experiences of embodiment by the user can have important effects on learning and engagement in virtual learning environments (Ioannou et al., 2021). In their scoping review of HMDs in education and training, Jensen and Konradsen (2018) found HMDs were particularly useful for skills acquisition, such as cognitive skills related to remembering spatial and visual information and affective skills related to controlling emotional responses to stressful or difficult situations.
A number of different XR modalities exist including computer-generated VR (CGVR), 360° Virtual Reality Video, AR, MR and Smart Glasses.
Computer-generated VR
CGVR, or VR for short, is an interactive 3D simulation that enables users to experience a real-time interaction and immersion in a computer-generated virtual space that can stimulate multiple levels of sensory perception, including visual, auditory or haptic experiences simulating sights, sounds, orientation and motion (Curran et al., 2022). This virtual environment is experienced and visualised by looking into an HMD which enables the user to block out one’s immediate real-life environment and interact with the virtual objects in a simulated space (Curran et al., 2022). This artificial environment can either mimic and simulate the real-world or it can be a totally imaginary world (Curran et al., 2022).
360° virtual reality video
360° VR video incorporates video recordings of real-world scenes that enable a totally immersive, 3D experience using a virtual headset (Curran et al., 2022). These 360° cinematic images can change in real time as the person moves around and by looking in front, up, down or behind them, they can see the entire environment picked up by the 360° camera (Curran et al., 2022). However, unlike other XR types, such as VR and AR, users are unable to move within a simulated environment or interact directly with objects in virtual space (Curran et al., 2022).
Augmented reality
AR is an enhanced version of reality created by using technology to overlay digital information (texts, graphic images or 3D contents) onto the user’s direct vision of the real world (Curran et al., 2022). AR headsets use transparent screens and reflective lenses to enable the digital information to be overlaid in the real world in the wearer’s field of vision (Curran et al., 2022). AR differs from VR in that the user interaction provides a more realistic environment compared to a virtual one, resulting from the fact that some of the viewed objects are real and some are virtual, allowing the user to interact with virtual information in the context of their real-world surroundings (Curran et al., 2022).
Mixed reality
MR refers to a merging of real and virtual worlds combining the best features of both AR and VR such that physical and digital objects co-exist and interact in real-time, and the user can interact with both virtual and real-world environments using an HMD (Curran et al., 2022).
Smart glasses
Smart glasses are a type of HMD and wearable device that can display various information and incorporates a video camera that records what the wearer is viewing (Curran et al., 2022).
Emerging evidence for XR and patient education
XR has widely been used in the education and training of healthcare professionals, but it also has the potential to be of added value in patient education (Shepherd et al., 2022; Slond et al., 2021; van der Kruk et al., 2022). A growing body of evidence suggests that VR for treatment-related purposes is effective, such as in relation to phobias and anxiety disorders, and in pain management. It can also be used in rehabilitation to improve balance in patients with stroke (Baniasadi et al., 2020; van der Kruk et al., 2022; Shepherd et al., 2022). The application of VR in patient education to date suggests it is a promising technology, with patients reporting high satisfaction and enhanced understanding (Slond et al., 2021; Urlings et al., 2022; van der Kruk et al., 2022). However, research on the use of XR is only beginning to be reported on, and while its use as an educational tool in healthcare has been described as feasible and acceptable, there are opportunities to improve future directions in the field. A number of recent reviews of the literature and evidence surrounding the use of XR technologies for patient education have been published, and these are summarised below to highlight some of the key findings from its use in patient education to date.
Urlings et al. (2022) conducted a systematic review of the literature regarding the use of AR in patient education. Patient satisfaction and comfort were evaluated in five studies, of which three were randomised control trials (RCTs), with positive results being demonstrated in terms of (perceived) knowledge gain, patient satisfaction and usability. In one RCT, patients reported that the patient education they received on epilepsy surgery and stereotactic electrode implantation was significantly more comprehensible and imaginable when their physician used an AR application compared to a rubber model. Most studies and all RCTs reported high usability and likability, with patients reporting that applications were easy to use and would prefer the AR experience over regular patient education methods (Urlings et al., 2022).
In another review, Slond et al. (2021) undertook a scoping review of the use of VR in patient education related to medical somatic treatment. Seventeen (n = 17) studies published between 2015 and 2020 were included, with VR patient education tools being applied in the context of (paediatric) surgery and radiation therapy (RT) treatment. VR patient education tools were mainly developed to reduce anxiety and improve understanding of upcoming medical procedures. Anxiety reduction was demonstrated significantly in some studies, and patients reported VR education as promoting enhanced understanding and improved communication with healthcare professionals. It also encouraged treatment compliance (Slond et al., 2021). The majority of RT treatment studies reviewed by Slond et al. used the Virtual Environment for Radiotherapy Training system (VERT). VERT is a 3D immersive simulation system designed as an educational tool that can simulate the entire radiation treatment environment and process. It demonstrates virtual patients and provides a visualisation of internal anatomy and RT dose. Computed tomography (CT) data and RT treatment plans may be loaded into the system, offering multiple visualisation options of patient anatomy, tumour volumes, and dose and treatment techniques (Rizzetto et al., 2020).
Van der Kruk et al. (2022) also conducted a scoping review of the use of VR as a patient education tool in healthcare. Eighteen (n = 18) studies were identified that used VR to educate patients or to communicate medical knowledge to patients. The findings indicate that VR has the potential to be a positive means of patient education, promoting satisfaction and reducing anxiety. All studies reported an increase in knowledge on illness and/or treatment after using VR as a patient educational tool. The most common conditions studied were cancer (9/18, 50%), followed by atrial fibrillation (AF; 3/18, 17%), and stroke (2/18, 11%). Other conditions or topics studied included movement disorders (1/18, 6%), gastrointestinal conditions (1/18, 6%), abdominal aortic aneurysm (AAA; 1/18, 6%), and laparoscopic donor nephrectomy (1/18, 6%) (van der Kruk et al., 2022). Most studies were conducted with adult patients, and nine studies used CT and/or MRI scans to construct a 3D 360° VR model which was either generic or patient-specific. Most studies (14/18; 78%) reported that a key benefit of VR as a patient education tool was increased patient understanding, knowledge and comprehension (van der Kruk et al., 2022). Studies also reported increased satisfaction related to the use of VR or with the healthcare system (7/18; 39%) (van der Kruk et al., 2022). Other benefits included reduced anxiety (6/18; 33%), improved comfort with treatment plans (1/18; 6%), increased patient engagement and empowerment (2/18; 11%), and improved patient compliance (1/18; 6%) (van der Kruk et al., 2022). Findings from the five studies measuring anxiety showed an overall reduction in anxiety levels after using VR (van der Kruk et al., 2022).
Shepherd et al. (2022) undertook a scoping review of VR in the perioperative setting for patient education. The most commonly used VR headset was Oculus Rift (Meta Platforms, Menlo Park, CA), and the main educational intervention used VR to show patients 3D individualised anatomical models to improve understanding of procedures and pathology as part of the consent process perioperatively. Findings from this review support VR as both acceptable to patients and feasible to use in a clinical setting. Ten (n = 10) studies reported improved patient-reported understanding of their medical condition and of the procedure, which resulted in less concern over the procedure perioperatively (Shepherd et al., 2022).
Critical perspectives on advancing VR and patient education
Advancing evaluation research
While a growing body of evidence is emerging to support the efficacy and feasibility of XR use in patient education, a key limitation in the evaluative studies undertaken to date has been inconsistency across evaluation study designs and evaluative outcome measures. Future evaluation research surrounding XR technologies in patient education would benefit from greater standardisation in terms of intervention types and outcome measures to advance evaluation approaches and evaluative evidence in support of such technological innovations. Examples of this may be found in fields such as continuing professional development in the health professions (Moore et al., 2018) and interprofessional education (IPE) (Reeves et al., 2016), where models and frameworks have been proposed to guide the future design of evaluation studies employing standardised evaluation levels and outcome measures. Another factor to guide future evaluation studies of XR and patient education would be a focus on which devices or modalities are most optimal for patient education (Urlings et al., 2022). Comparative evaluation studies examining different XR modalities or types would be useful in improving our understanding of the modality types that foster the best patient education outcomes and are most feasible in particular settings. As one example, a modified version of Kirkpatrick’s model for summative evaluation, as described in Curran and Fleet’s (2005) work, could be adapted and applied to guide evaluation approaches going forward (Figure 2).
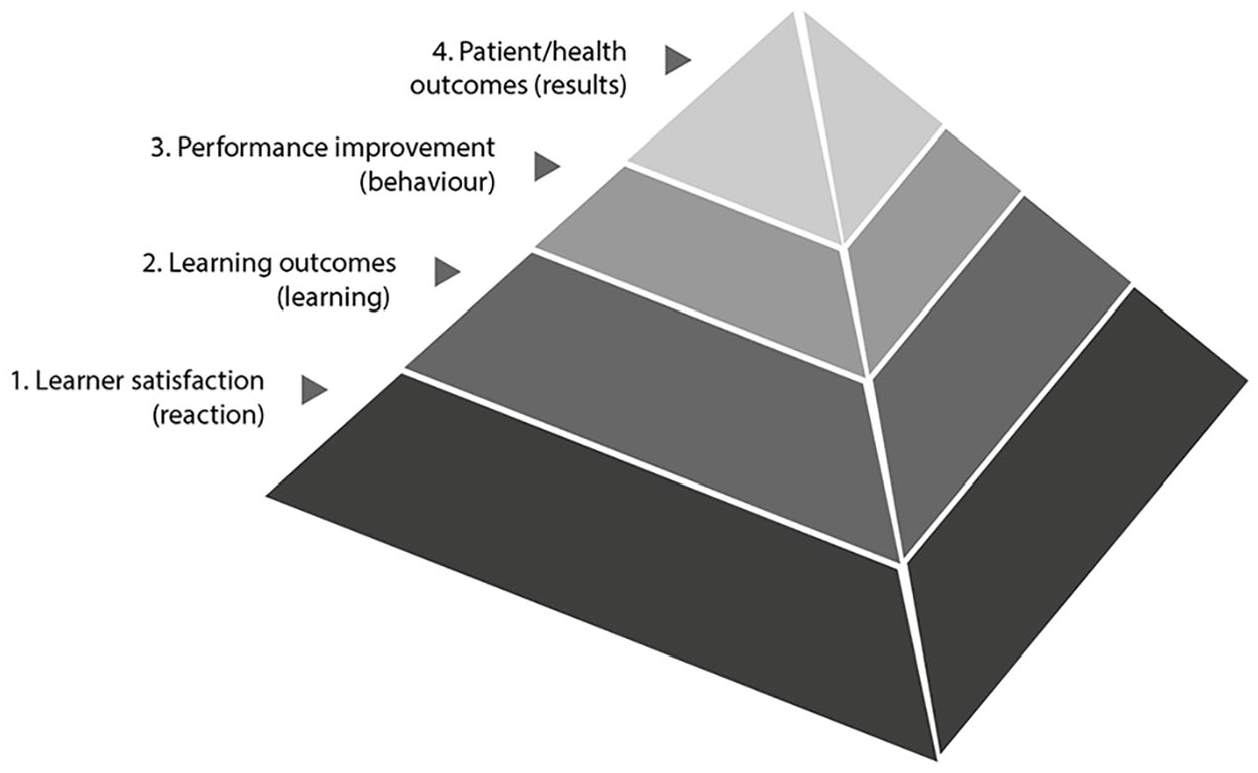
Modified model of Kirkpatrick’s levels of evaluation.
Numerous benefits arising from the use of VR as a patient education tool are identified in the review studies previously summarised; however, very few studies highlight drawbacks. Yet, McKnight et al. (2020) report that multiple studies in the past have demonstrated that HMDs can cause side effects such as nausea, headaches and vertigo. However, this situation appears to have changed in recent years, with the severe effects found in the past becoming rarer nowadays, allowing XR users to spend much longer periods of time wearing HMDs than what was previously possible (McKnight et al., 2020). A main factor inducing simulator sickness (i.e., the delay between head motion and the corresponding visual update display) has been greatly reduced with state-of-the-art computer systems, graphics cards and HMDs. However, the evaluation of the side effects related to the use of XR in patient education must remain a consideration (Rizzetto et al., 2020). In addition, concerns about battery life, line of sight and secure network access have been raised (McKnight et al., 2020) and are being actively addressed by the developers of these technologies. Therefore, exploring the possible unintended consequences of VR as a patient education tool requires further research (van der Kruk et al., 2022). Patient sensitivity needs to be considered, including apprehensiveness about the use of HMDs, potential unintended psychological or emotional responses to VR environments, user’s capacity to act in a virtual environment, and the potential side effects (e.g. cybersickness) and how duration of use may influence this (Baniasadi et al., 2020).
Another limitation in the evaluative evidence to date derives from the lack of studies conducted specifically among populations known to have lower levels of health literacy and/or socioeconomic status (van der Kruk et al., 2022). The burden of digital health illiteracy can be significant for those patients who experience challenges in navigating health information, as they may also be more vulnerable to misinformation. Lower digital health literacy may also contribute to persistent social health inequalities and poorer health outcomes (Estrela et al., 2023). Research suggests that short and visually appealing medical information may be more effective in communications with populations of lower health literacy, and these patient groups could benefit the most from the use of VR as a patient education tool (van der Kruk et al., 2022). Similarly, people in rural areas far from health services are known to have lower levels of health literacy and worse health outcomes due to living in communities far from health resources (Aljassim and Ostini, 2020; Sui and Facca, 2020). More research is needed to determine whether XR technologies can be beneficial in overcoming the challenges to communicating healthcare information to these vulnerable groups.
There is also the need for research to better understand the influence of sociodemographic, economic, and cultural differences on digital health literacy and whether such factors may also present barriers or challenges to adoption and use of VR (Estrela et al., 2023). Chen et al. (2019) suggest that rural residents may also have lower access to and use of certain health information sources relative to urban residents and, with greater shortages of physicians and other healthcare providers and limited media exposure, rural residents may have more limited access to health information, especially those with limited health literacy. As a result, there is an opportunity to explore the potential role that VR could play in enhancing access to meaningful and timely health information for rural populations, thereby helping reduce some of the health inequities in access to impactful health education for rural communities.
Applying user-centred design
Feenberg’s (1991) ‘critical theory of technology’ offers a perspective that promotes an understanding of how social and historical factors impact technological use. Feenberg argues that technology is not ‘determinist’ by nature but is shaped by human agency and certain values and biases reflecting its own historical development and design. In Feenberg’s view, technology is a contested field in which individuals and social groups struggle to influence and change technological design, uses and meanings. Technology can also play an important role in societal democratisation, and, for Feenberg, technologies should contribute to helping produce a more egalitarian society. A key consideration of a critical theory of technology is that its construction is influenced by the interaction between its design and how it is appropriated by its users. According to Okan (2007), educational technology use, like VR, is influenced by the interaction of several elements such as the inherent characteristics of the technology, beliefs about its educational purpose, users’ own understandings of the potential of the technology, and the interplay between users and developers concerning how technology should be used for educational purposes.
A practical challenge considered by researchers is the usability of VR applications (Baniasadi et al., 2020), and the usability of a system is a key characteristic influencing system quality according to DeLone and McLean’s (2003) ‘Model of Information Systems Success’. Usability describes the quality of the user interfaces from the user’s point of view and the extent to which a system can be used by specific users with ‘effectiveness’, ‘efficacy’ and ‘satisfaction’ within a certain context. User-centred design (UCD) is a popular approach to designing effective user interfaces. Baniasadi et al. (2020) describe UCD as encompassing a design philosophy that stresses the importance of clearly understanding users and involving them in the design process to create a well-designed and usable system (Baniasadi et al., 2020; Hasani et al., 2020). By involving users and relying on their feedback, together with intuitive design, to ensure the quality of design, UCD aims to design user interfaces that increase satisfaction by aligning design with users’ expectations and goals (Ghazali et al., 2014).
Usable and user-friendly applications are essential, and most researchers agree that user participation in the design process will help to create a usable system (Baniasadi et al., 2020). There has been no single agreed definition nor way to implement UCD, although it has been described as a method with well-defined phases. Ghazali et al. (2014) describe these as follows: (1) specifying the context of use, (2) specifying user requirements, (3) designing the solution, and (4) evaluating the design. Alternatively, Sharp et al. (2019) describe UCD as encompassing four basic phases consisting of (1) requirements discovery, (2) solution design, (3) prototyping, and (4) evaluation.
Slond et al. (2021) highlight the importance of involving patients, educationalists and technology professionals in the development of technology interventions such as VR. Users’ opinions and thoughts should be taken into account when designing a new XR application for patient education, and prior to clinical implementation, patients’ views on XR tools should be investigated. Designing systems, regardless of users’ feedback, can lead to user dissatisfaction, reduced performance and uselessness of the system. User acceptance problems often lead to the abandonment of systems by users or the refusal to learn how to use them (Baniasadi et al., 2020). That being said, Urlings et al. (2022) found in their recent review of the literature that patients were rarely involved in the designing of XR applications. Including patients more fully in this process could help construct patient-friendly, useful, and more effective XR applications. Previous work has shown that conducting qualitative research can result in identifying facilitators, barriers and positive and negative effects of new educational tool usage. Including these insights in application development can ensure that the use of technology will meet the needs of the patient in a more efficient way (Urlings et al., 2022).
Figure 3 outlines the key steps in a UCD approach adapted for developing XR for patient education. Initially, understanding the purpose and goals of the patient education activity is important, including understanding the nature of the context in which the XR application will be used by healthcare providers and patients. Will the provider be present to guide the patient in the use of the XR system, or will the patient be expected to use the application by themselves? The answer to this question has implications for instructions and guidance for the use of the product. Most times, a thorough needs assessment of both the patient and healthcare provider will be required to explore the context but also to define the specific knowledge, skills or perhaps attitudinal domains to be addressed by the patient education experience. The next steps would involve the design of the XR solution in collaboration with the end-users to seek feedback on the product as it is being designed and developed. Storyboards can be a useful tool to use at an early design stage to outline the nature of the XR experience, followed by a rapid prototype to pilot and test with the user audience before full production is undertaken. Finally, an evaluation of the XR system with end-users to gauge satisfaction with the patient education experience should be undertaken to check against the intended purpose and requirements for the product.
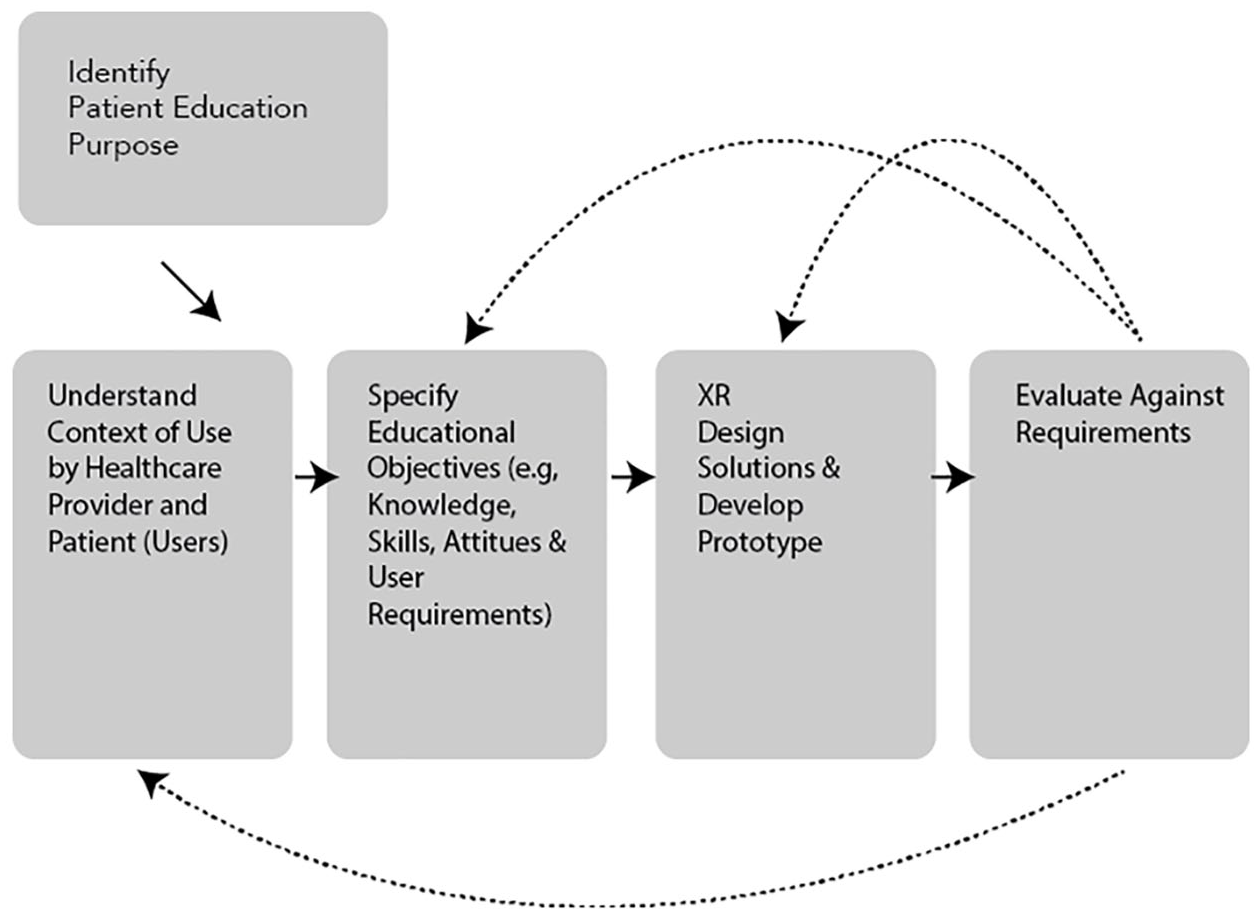
Modified UCD approach for patient education XR applications.
Applying educational design principles
Several reviews of the literature surrounding the use of VR use education suggest that educational studies generally lack consideration of learning theories in the development of virtual reality learning applications (Lui et al., 2023). However, a number of educational theoretical perspectives offer key premises to guide the design of potentially effective VR experiences. Constructivism, as a key learning theory, emphasises that knowledge, meanings and understandings are constructed through interactions with active and authentic learning activities that combine sensory input, existing knowledge, and new information (Chen, 2010; Merriam and Baumgartner, 2020). For constructivist theorists, knowledge is a function of how the individual creates meaning from his or her experiences. Each of us conceives of external reality somewhat differently, based on our unique experiences of the world and our beliefs about them. Learning is an active process that involves a personal interpretation of the world and the construction of meaning from these experiences. It is based on moving from creating prescriptive learning situations to developing environments that engage learners and require them to construct the most meaningful knowledge.
Generally, constructivists believe that learners can learn better when they are actively involved in constructing knowledge in a contextualised ‘learning-by-doing’ situation (Jonassen, 1999). An effective constructivist learning environment, therefore, offers adequate depiction of the contextual factors that surround an experience so the user can understand it. Constructivism also stresses the importance of authenticity in a learning experience, similar to that which exists in the real world (Jonassen, 1999). A key constructivist concept is that of ‘situated cognition’, which suggests learning occurs in a context, that our learning is situation-specific, and that the nature of the context structures the learning. Making learning as ‘authentic’ as possible by situating learning in the real world, or in simulated real-world experiences and in authentic learning tasks is a key principle. Situated cognition supports the use of specific activities or learning resources to create learning experiences in which users can acquire vivid and imaginative concrete representations (Ni, 2022). VR is believed to be a useful learning technology that can support constructive and situated learning experiences. VR technology can provide users with a vivid and realistic learning environment that simulates the characteristics of an actual situation, including the senses of sight, sound and touch. In this visualised VR simulation environment, users feel novel and interested in learning, thus thoroughly motivating them to learn (Chen, 2010).
Mayer’s Cognitive Theory of Multimedia Learning (Mayer, 2009) offers a further theoretical foundation for the learning benefits of VR. According to Mayer (2009), the ‘multimedia principle’ states that ‘people learn more deeply from words and pictures than from words alone’ (p. 47). However, simply adding words to pictures is not an effective way to achieve multimedia learning. Mayer proposes three main assumptions when it comes to learning with multimedia: there are two separate channels (auditory and visual) for processing information (also referred to as dual-coding theory); each channel has a limited (finite) capacity; and learning is an active process of filtering, selecting, organising and integrating information based upon prior knowledge. The key implications of Mayer’s work are for the design of multimedia-based learning environments like VR include providing coherent verbal, pictorial information, guiding learners to select relevant words and images, and reducing the load for a single processing channel (Mayer, 1997; Mayer and Moreno, 2003). Some research has revealed that the cognitive loads imposed by VR may be an impediment to effective learning outcomes, and as such key attention to the design of VR simulation environments is critical to optimise learning experiences (Lui et al., 2023).
The dual-coding theoretical perspective (Clark and Paivio, 1991) is also useful in understanding the significance of the audiovisual experiences that can be portrayed with VR technologies. Memory is a key function of the brain, and memory functions are seen as one of the primary mental processes associated with learning. Memory can be divided into sensory memory, working memory and long-term memory. Working memory–or short-term memory–(which takes place in the neocortex) is where the information one attends to (through the senses) is processed. Information that is processed in working memory enters long-term memory, where it is stored for future use. Moving memories into long-term memory involves encoding or the strategies we use to place information into long-term memory. Dual-coding theory, as depicted by Figure 4, suggests that working memory has two channels for information acquisition and processing: a visual/pictorial channel and an auditory/verbal processing channel (Clark and Paivio, 1991). The representation of both visual and verbal information in a complementary manner can create separate representations for information processed in each channel and enhance the quality and level of comprehension, facilitate the integration of new information into existing cognitive structures, and improve memorisation of the information (Sternberg and Mio, 2006).
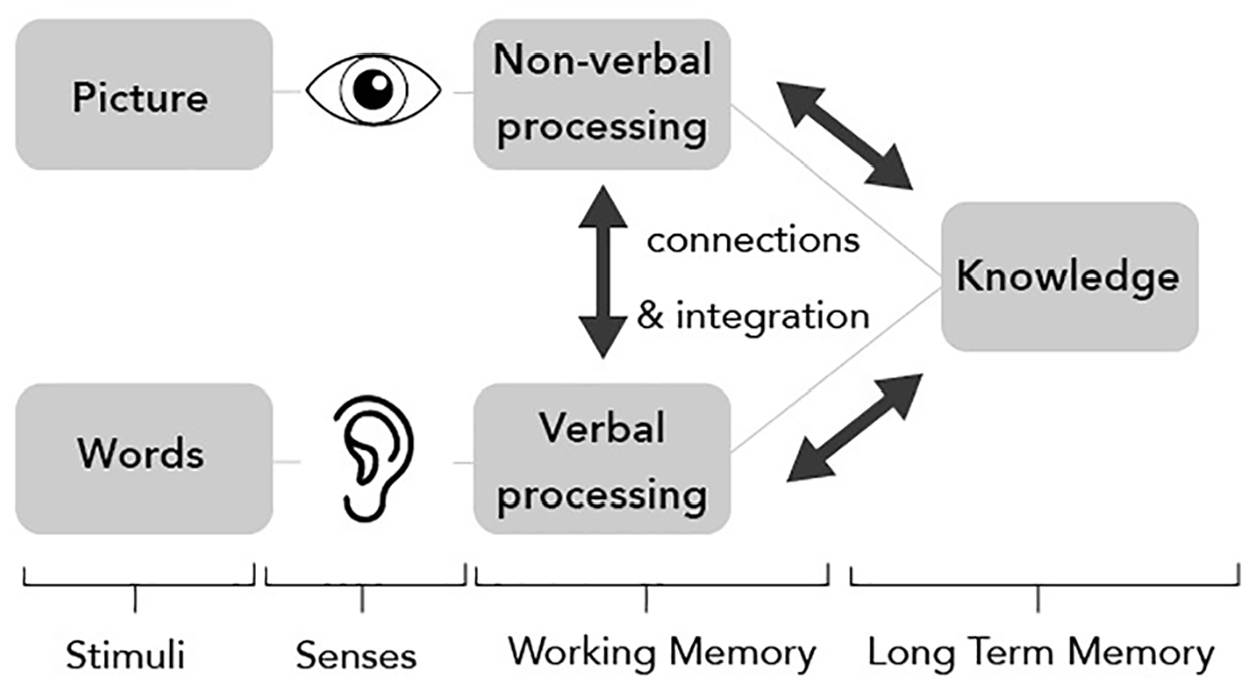
Depiction of dual-coding theoretical perspective.
Further work to explore the best mix of visual and/or auditory information in the design of VR experiences, whether through 360 video or interactive VR simulation is needed. Evidence-based principles in designing immersive XR experiences, such as those developed for other technology-based learning environments, will help to advance the use of XR for patient education (Cook and Skrupky, 2023). In line with this perspective, Slond et al. (2021) suggest that key learning principles that promote patient education are ‘interactivity’ and ‘involving different senses’ to better remember the information provided. Urlings et al. (2022) also propose that improvement of low information recall could be accomplished by using explicit categorisation techniques and supporting spoken information with written or visual material.
Conclusions
XR technology has emerged as a new and innovative way to provide patient education in a range of health domains. The nature and extent of evaluative evidence is growing as well, as new opportunities for applying XR technologies across different clinical and healthcare areas emerge. The growing evidence suggests that different forms of XR technology applications have potential in creating immersive patient education experiences that are engaging and can lead to enhanced patient satisfaction, positive educational outcomes and reduced patient anxiety about medical procedures and treatments. It is possible that XR may also have important implications for better patient compliance, healthy behaviours and lifestyle modifications, and ultimately, better health outcomes. Nonetheless, there have also been growing calls for greater consideration of how learners’ characteristics, including socioeconomic status, gender, cultural and generational differences, influence the learning effects of VR educational applications, as well as its adoption and implementation for patient education purposes. Technology acceptance may also be another important learner characteristic that could affect adoption and learning effects of XR. Given the effect of these different learner characteristics on digital health literacy as well, the design and implementation of XR modalities for patient education will require greater attention to tailored interventions that consider these nuances more closely. Despite this, opportunities for adopting and using XR technologies in diverse areas of patient education are numerous, and in some areas, XR platforms may offer more accessible and cost-effective means for patient education delivery. Further research to explore the effectiveness of XR use in patient education and across different patient populations is needed to support effective design approaches as well as potential applications of this innovative technology.