
Abstract
Stress and anxiety are pervasive concerns among American college students, posing detrimental effects to their well-being and academic performance. Physiologically based stress management programs have proven effective within university settings; however, limited research has investigated the impact of such interventions on university honors students. One promising tool is electrodermal biofeedback, which utilizes electrodermal activity as an indicator of psychophysiological stress-related phenomena. To address this research gap, we conducted a pre–post comparison electrodermal biofeedback intervention study involving five honors students. Across 18 time points, we recorded a total of 81 stress response control measurements per participant. Over a 6-week period, participants learned to control electrodermal activity, heart rate variability, and peripheral temperature. Visual analysis of the data revealed improved averages and trendlines in physiological stress response control for all five students, with an average effect size of d = 0.74. Moreover, participants demonstrated better average physiological stress response control post-treatment compared with pretreatment.
Plain Language Summary
College students in honors programs often face intense pressure to succeed. Although many of them perform well academically, they may struggle with stress, especially during examinations and periods of transition. In this study, we explored whether a tool called biofeedback could help honors students learn how to control their physical stress responses. Biofeedback uses sensors to measure signals from the body, such as sweating, temperature, and heart rate, and helps people practice techniques to manage these signals and feel calmer.
Five honors students participated in weekly sessions more than 6 weeks. During each session, they practiced controlling their breathing, muscle tension, and thoughts while monitoring their body’s signals. We tracked how well they learned to control stress across 18 time periods. The results showed that all five students improved their ability to control physiological signs of stress over time. For most students, these improvements were maintained even after the sessions ended.
This study shows that honors students, even though they are high-achieving, can benefit from support in managing stress. It also suggests that short-term, low-cost interventions like biofeedback could help students improve their ability to stay calm and focused in challenging academic settings.
Keywords
Colleges across the United States identify and recruit high-ability students for their honors programs with an aim to facilitate their academic growth (Rinn & Plucker, 2019). While some studies have explored the academic and psychosocial benefits of honors programs, including their potential role in fostering resilience and well-being (Rinn & Plucker, 2019), research on how these programs specifically assist students in managing stress and anxiety remains limited. Subotnik et al. (2011) criticized a prevailing misconception that students participating in talent development programs are emotionally more fragile due to alleged heightened sensitivities. This belief feeds into the assumption that such students are more vulnerable to stress-related pathologies. However, there is no clear consensus on whether gifted individuals experience more or less anxiety than their peers. Francis and colleagues (2016), in their systematic review, compared gifted students (i.e., students with IQ scores ≥125) and nongifted students (i.e., those with IQ scores ranging 90–110), finding that gifted students tended to exhibit slightly lower anxiety levels than their nongifted peers. But when Duplenne et al. (2023) undertook a meta-analysis comparing the effect sizes across multiple studies, they found that, on average, these differences were not statistically significant. Overall, the research is inconclusive on this front, and if a difference in anxiety levels between the gifted and nongifted exists, the difference is likely minimal. Still, this does not preclude context-specific vulnerabilities—particularly during academic transitions or under intense performance pressure—as shown in studies of honors students facing GPA-related stress, social comparison, and internalized expectations (Henfield et al., 2014; Mendaglio, 2013; Subotnik et al., 2011). Because anxiety rates among university students are rising worldwide across all continents (Tan et al., 2023), structured support and effective stress management strategies are essential for both groups.
Researchers in talent development underscore the ability to manage stressors as a fundamental skill pivotal to achievement (Subotnik et al., 2011). Siegle et al. (2017) emphasized self-regulation as a requisite element in fostering academic success. In fact, different studies provide evidence that self-regulated tools might be helpful when adopted in gifted programs (L. Orione et al., 2021; Reis & Greene, 2014). Gaesser and Karan (2017), in a randomized controlled trial, found that self-regulation tools, such as Emotional Freedom Techniques (EFT), effectively reduced anxiety in high-ability adolescents, with EFT showing a significant reduction in anxiety levels compared with a control group. In line with this, Portenga (2018) recommended that researchers explore methodologies to help students struggling with stress to effectively manage stress and anxiety during examinations.
Furthermore, Subotnik et al. (2011) advised educators assisting students in talent development programs to focus on building psychological resilience, a factor associated with superior performance and effective anxiety regulation. Other authors have highlighted that psychosocial support is particularly relevant during critical transitions, such as the shift to college, where students must navigate new academic expectations, social dynamics, and personal responsibilities (Kwan et al., 2021; Zhao et al., 2023). Ensuring that students develop effective stress management strategies during these transitions may be essential in preventing anxiety from hindering their long-term success (Fond et al., 2020). As Subotnik et al. contend, “It should not be assumed that students who possess developed ability also have these psychosocial skills, nor that such skills can be generated without direct guidance and teaching” (p. 40). However, it is important to note that educators do not feel typically equipped with the skills and tools to assist students in managing stress and anxiety effectively (Ekornes, 2015).
The outbreak of COVID-19 exacerbated stress and anxiety, particularly among school-aged students (American Psychological Association [APA], 2021). According to a survey conducted by the APA, between February 19 and 24, 2021, approximately 80% of individuals aged 18 to 26 exhibited elevated levels of stress-related behaviors potentially detrimental to their health. These behaviors included avoidance of physical activities, diminished sleep, and poor dietary habits. However, academic anxiety was a global problem for youth even before the pandemic. The Program for International Student Assessment (PISA) surveyed 540,000 students aged 15 to 16 across 72 countries (OECD, 2017). The survey found that two thirds of students experienced stress when contemplating grades and examinations, even when they felt well prepared.
A recent systematic review analyzed 68 different types of programs aimed at teaching university students how to cope with stress, anxiety, and depression, finding that several programs produced significant outcomes (Rith-Najarian et al., 2019). Therefore, there is some evidence that stress/anxiety reduction interventions in the academic field can pay off. Among the various strategies explored to mitigate academic stress and anxiety, physiologically based approaches have shown promising results. One such intervention, highlighted by Rith-Najarian and colleagues (2019), is biofeedback. Biofeedback interventions use noninvasive instruments that help people read and train physiological states. These states are associated with the human body’s responses to stressors, as measured by differences in aspects like temperature, heart rate variability (HRV), and muscle tension. Researchers can integrate biofeedback tools with smartphone apps that can train learners how to control stress and anxiety in a fast and autonomous way (De Witte et al., 2019).
Different modalities of biofeedback are related to different body signals. Electrodermal activity (EDA), also known as skin conductance, measures subtle changes in sweat gland activity, which are controlled by the autonomic nervous system. Since these changes occur in response to stress or emotional arousal, EDA is widely used as an objective indicator of physiological stress levels (Posada-Quintero & Chon, 2020). By controlling EDA, people can learn to control different stress-related physiological responses like HRV and body temperature (Sonkusare et al., 2019). Bhoja et al. (2020) described EDA as the most popular method for investigating human psychophysiology. Despite EDA being recognized by research as a reliable measure to control physiological stress responses, there have been no experimental studies using EDA biofeedback with college students on stress, anxiety, and achievement. There is a paucity of studies investigating the causal relationship between EDA biofeedback and reducing stress factors or increasing performance in honors program students. In fact, the few empirical studies on honors programs over the last 15 years that mentioned stress and anxiety focused more on describing the problem than on investigating solutions to help honors students deal with it (Rinn & Plucker, 2019). Given the potential benefits of biofeedback, alongside the recognition of EDA as a credible indicator of stress response within the scientific community, it becomes increasingly clear that more research is needed in this domain. This is particularly true when considering the significant role that stress and anxiety play in a student’s life, especially when transitioning into college. The dearth of empirical studies examining these elements within honors programs further underscores the need to explore the applicability of EDA biofeedback within such academic settings. Hence, an investigation into the use of EDA biofeedback within honors programs is both timely and warranted.
Literature Review
This literature review explores the relationship between stress, anxiety, and academic performance, particularly within the context of honors programs. It begins by defining stress and anxiety, highlighting their physiological and psychological components, and explaining how the autonomic nervous system regulates stress responses. The review then examines the prevalence of academic stress among students, discussing its impact on mental health, academic outcomes, and overall well-being with particular attention to critical academic transitions, such as the shift to college, where students must navigate new social and academic demands. Following this, research on biofeedback as a tool for stress management is introduced, with a focus on EDA and its role in regulating physiological arousal. In addition, the review considers the broader implications of talent development frameworks, emphasizing the importance of self-regulation for high-achieving students. Finally, the literature on stress and anxiety in honors programs is discussed, addressing both the challenges in existing research and the need for interventions tailored to this student population.
Stress and Anxiety: Definitions and Physiological Mechanisms
De Witte et al. (2019) defined stress as a complex phenomenon in which human beings respond to stressors that are present in the environment—things perceived as psychological, emotional, or physical threats to our equilibrium. Anxiety is characterized by excessive and persistent worries that do not subside, even when stressors are no longer present in the environment (APA, 2019). The APA suggested that the mental and physical symptoms of stress and anxiety are nearly identical, and these symptoms might impact people’s sleep, concentration, muscle tension, and irritability.
The autonomic nervous system plays a crucial role in regulating the body’s response to stress and is divided into two complementary branches: the sympathetic nervous system and the parasympathetic nervous system. The sympathetic nervous system is responsible for activating the body’s fight-or-flight response, increasing physiological arousal to help individuals respond to perceived threats. In contrast, the parasympathetic nervous system promotes the body’s rest-and-digest state, counteracting the effects of sympathetic activation.
The human sympathetic nervous system responds to stressors by producing a series of physiological responses to promote better adaptation to them. The goal of the sympathetic nervous system is to better prepare people for stressful environmental demands. It does so by accelerating heart rate, decreasing HRV, increasing blood pressure, dilating the bronchioles for improved oxygen intake, and stimulating sweat production to help regulate body temperature (Bhoja et al., 2020; Posada-Quintero & Chon, 2020; Sonkusare et al., 2019). When people need (or want) to lower the intensity of their stress responses, the parasympathetic nervous system triggers functions that slow those responses by reducing physiological arousal and promoting relaxation (Sandvik et al., 2020; Schach et al., 2022). The balance between these two systems is crucial for effective stress regulation, as dysregulation is often associated with heightened anxiety and difficulty in managing stress.
In the short term, our arousal responses associated with stress and anxiety might be beneficial in helping people cope with stressors (Shields et al., 2016). For instance, a small amount of stress and anxiety may lead people to study more for an examination because they anticipate it will be difficult, which might result in better grades. Besides that, sympathetic nervous system activity may have a positive association with our immunological activity, as long as people aren’t overly stressed for long periods of time (Dhabhar, 2014). However, when people can’t accomplish simple things like sleep well or can’t stop thinking about problems that are not present (e.g., getting too worried about grades), stress becomes negative. In these contexts, people might face clinical issues such as chronic anxiety.
Stress, Anxiety, and the College Transition
Unfortunately, students are at high risk of anxiety and stress symptoms (Rith-Najarian et al., 2019). A nationwide survey of 31,463 people found that anxiety was the most relevant mental illness for college students in the United States (American College Health Association, 2018). Students reported stress and anxiety as the main obstacles to their academic performance. Pascoe et al. (2020) identified several critical consequences of academic stress at both the high school and college levels, including mental health issues, depression, substance abuse, sleep disturbances, physical health problems, increased dropout rates, and lower academic achievement.
The link between academic stress and mental health is well documented. Studies show that self-reported stress correlates with higher anxiety levels, reduced well-being, and a lower quality of life (Ribeiro et al., 2018). Chronic stress is also associated with more severe mental health conditions such as depression and anxiety disorders (Hussenoeder et al., 2024). These symptoms can significantly hinder academic achievement, as students experiencing anxiety and depression often struggle with concentration, completing tasks, and maintaining strong academic performance (Harrison et al., 2022). Academic stress has also been linked to increased substance use, as students under high academic pressure may turn to alcohol or drugs as coping mechanisms (March-Amengual et al., 2022; Vargas-Ramos et al., 2021). However, protective factors such as positive coping strategies and social support from parents and faculty can help mitigate this effect (Boulton & O’Connell, 2017).
Beyond mental health concerns, academic stress also affects students’ sleep, physical health, and long-term academic trajectories. Sleep disruption is one of the most common consequences of academic-related stress, impairing attention, increasing stress levels, and ultimately affecting academic performance (Alhamed, 2023; Curcio et al., 2006). In addition, prolonged academic stress has been associated with unhealthy lifestyle habits, decreased physical activity, and conditions such as metabolic syndrome and obesity
The transition into college represents a critical period marked by heightened stress and adjustment challenges. A meta-analysis by Wu et al. (2021) found that many first-year students experience elevated stress during this adjustment period, with variations depending on individual mindsets and coping strategies. First-year students, in particular, face a dual transition: Not only are they moving into a new academic environment, but they are also navigating the developmental shift from adolescence to adulthood (Cheung et al., 2020). This period often involves adjusting to academic expectations, forming new social connections (Bojuwoye, 2002), and coping with the absence of familiar support systems such as family and long-standing friendships (Hudd et al., 2000). Emerging adulthood, the stage many first-year students are in is characterized by identity exploration, uncertainty, and instability (Kwan et al., 2021), further compounding stress levels. Research suggests that the experiences and coping strategies developed during this first year have long-term implications for students’ academic success and overall well-being throughout college (Fond et al., 2020). Reflecting these challenges, González-González et al. (2023) found that university dropout rates are highest during the first year, often due to academic, social, and personal adjustments that require significant effort from students as they adapt to their new environment.
Rith-Najarian et al. (2019) highlighted the high prevalence of anxiety symptoms among university students and emphasized the need for targeted mental health interventions. Several stress and anxiety reduction programs implemented in American colleges yielded significant positive outcomes, with 60% of adolescent and young adult prevention programs demonstrating symptom reduction (Christensen et al., 2010). Notably, Rith-Najarian et al. observed that 29% of these university-based programs reviewed produced large effect sizes, which is particularly promising given that prevention-level interventions typically yield smaller effects than treatment-level ones (Horowitz & Garber, 2006). While these findings support the value of stress management programs, more research is needed to determine which strategies are most effective for sustained anxiety reduction in college students. In this context, interventions that offer real-time monitoring of physiological stress responses have drawn increasing interest as potential tools for helping students develop long-term self-regulation skills (Rodrigues et al., 2022; Rydzik et al., 2023).
Biofeedback
The word biofeedback describes techniques using instruments that can help people understand and train their bodies’ physiological activity (L. Orione et al., 2021). People can use biofeedback for performance (Rodrigues et al., 2022) and clinical (Bergmann et al., 2020) improvement. It can help users understand that they can control biological electric signals (biosignals) associated with their psychophysiological states. These stress biosignals include HRV, EDA, skin temperature, and muscle activity.
As an example, researchers measure EDA, a reliable indicator of physiological arousal, in microsiemens (μS). One assumption in EDA biofeedback programs is that once learners understand how EDA biofeedback equipment shows their internal states related to stress, they trust it is possible to develop the skill to handle arousal using that equipment (Pop-Jordanova & Pop-Jordanov, 2020). First, people train how to change EDA levels in laboratory sessions. During these sessions, they learn how to diminish their arousal levels by visualizing their average EDA level dropping. After learning how to control EDA, users test their ability in real-life situations. At one point, learners no longer need the help of EDA equipment to transfer these techniques to personal life events, such as competitions and academic tests (De Witte et al., 2019; Rodrigues et al., 2022).
Biofeedback therapy focused on stress and anxiety is normally paired with other techniques traditionally used in clinical settings with the same purposes (Schlatter et al., 2022). During biofeedback sessions, users may practice breathing control by exhaling for longer periods of time or more vigorously than inhaling. People can learn to manage tension and thoughts through relaxation methods or by increasing states of mindfulness (Edwards, 2016).
When people are highly stressed and anxious, they tend to have elevated levels of cortisol. One type of breathing exercise called the “physiological sigh” is associated with diminished levels of cortisol in anxious people (Severs et al., 2022). This exercise consists of people exhaling more vigorously or for more time than inhaling. Researchers consider this type of respiration one of the fastest evidence-based ways to diminish sympathetic activity associated with stress and anxiety responses.
When people are stressed, they move and increase muscle tension, preparing to say or do something they would not normally say or do in calmer contexts. Therefore, another focus of successful therapies aimed at stress/anxiety control associated with biofeedback therapy is teaching people how to relax muscle tension and control their movements (McGinnis et al., 2005). Rith-Najarian et al. (2019) reported that relaxation methods had a large positive effect when teaching college students how to cope with anxiety and stress.
Since the 1800s, research has posited that thoughts, like expectations, might influence EDA, formerly called galvanic skin response (Peterson & Jung, 1907). Because of this, one function of biofeedback is to show learners that they can learn how to manage their thoughts and decrease EDA. Participants can practice how to diminish the intensity of the signals by using strategies like stopping stressful thoughts and focusing on things they perceive as more calming. In sum, students can learn how to diminish EDA by managing their thoughts, muscle tensions, and respiratory patterns.
Regarding EDA biofeedback use at universities, there are some distinct advantages and disadvantages (De Witte et al., 2019; L. Orione et al., 2021; Ratanasiripong et al., 2012; Rith-Najarian et al., 2019; Rodrigues et al., 2022; Tolin et al., 2020). Some advantages are as follows: (a) Biofeedback provides fast evidence for users in controlling bodily responses to stress; (b) different modalities of biofeedback have shown they work for stress/anxiety control in schools and sports; (c) studies have found a maximum Cohen’s Kappa in biofeedback research; and (d) biofeedback has been used for more than 50 years. Some disadvantages include (a) teachers do not receive training to offer this type of psychosocial support in the United States; (b) it uses individualized equipment (which raises costs, as biofeedback equipment can cost more than US$400); (c) users need a tablet, a smartphone, or a computer to engage with EDA biofeedback; and (d) there is a paucity of strong experimental research studying biofeedback at colleges to guide new studies.
Talent Development Frameworks: The Role of Stress and Anxiety Control
Since the 2010s, talent development conceptual frameworks have posited that achievement is a relevant outcome in the trajectories of successful high-ability individuals (F. Orione & Fleith, 2022). The Achievement Orientation Model (Siegle et al., 2017) and the Talent Development Megamodel (TDMM; Subotnik et al., 2011) consider specific abilities and psychosocial factors as fundamental elements of talent development. Both reinforce that people need to develop technical skills, but also that attitudes and self-regulation greatly influence achievement.
The TDMM (Subotnik et al., 2011) and the Achievement Orientation Model (Siegle et al., 2017) provide key insights into the importance of self-regulation in motivating high-ability students and helping them achieve their goals. Pascoe et al. (2020) conducted a review of existing literature, illuminating the positive correlation between stress and underachievement in college settings. Xiao and Sun (2021) found that students who showed the highest math achievement and persistence on the PISA also reported the lowest levels of math anxiety and the highest levels of motivation. This is consistent with broader research showing a moderate negative correlation between math anxiety and math performance (Namkung et al., 2019). In other words, higher anxiety is often associated with lower achievement. Through this lens, it becomes clear that students must acquire strategies to manage stress and anxiety effectively to convert their potential into tangible academic outcomes.
The Achievement Orientation Model identifies self-efficacy, favorable environmental expectations, and meaningful goal valuation as pivotal beliefs within talent development contexts. Without robust support and conviction in these three areas, individuals may fail to engage in or attain significant career milestones (Siegle et al., 2017). Learners who exhibit self-efficacy, find tasks purposeful, and experience a supportive environment are more likely to employ self-regulation skills on their path to success. The model underscores the necessity for individuals to learn how to establish pragmatic expectations, as well as to develop and adjust strategies that can enhance their likelihood of success. This becomes particularly beneficial when individuals believe they have the capacity to accomplish tasks to the level of quality they desire or require.
Two components can potentially foster self-efficacy: (a) learners having acquired the technical skills necessary for proficient performance, and (b) learners possessing the confidence that they can apply what they have learned from instructional settings or evaluations. Viewed from this perspective, students’ ability to regulate their emotions, thoughts, and behaviors may play a meaningful role in differentiating those who reach high levels of achievement from those who do not. Therefore, self-regulation strategies could lead to improved performance. They could also serve as motivational tools, bolstering learners’ belief in their psychological resilience. As a result, learners may perform at a high level when required to attain their goals.
The TDMM (Subotnik et al., 2011) describes how talent develops in four progressive stages (technique, competence, expertise, and eminence). As an individual moves from one stage to another, the transitions become more difficult. Contexts become tenser as one moves from expertise to eminence, for example. During the last transition, the ability to self-regulate and cope with stressful psychosocial factors helps to determine who will achieve eminence. Therefore, Subotnik et al. write that psychosocial factors are of the utmost importance in highly talented people’s trajectories. To optimize psychosocial growth, they suggested that teachers learn to provide treatments that positively influence stress control, concentration, and high-level performance, something not traditionally implemented in modern schooling. Subotnik et al. (2011) reinforced that: This omission is especially glaring before graduate school, as academic talent during the school years and even in college is pursued mostly in classroom settings, as opposed to working with an individual teacher, mentor, or coach. It is also the case that school and college teachers receive no systematic training in this dimension of differentiated instruction. (p. 25)
The TDMM posits that psychosocial support is important for all students in talent development programs in all stages of their trajectories, especially for those in transitions to upper levels of production. Some gifted students struggle during the transitions into college, encountering heightened academic demands and social comparison pressures for the first time (Mendaglio, 2013). Subotnik et al. highlighted the role of the Big-Fish-Little-Pond Effect in this process, noting that students who were top performers in their previous environments may experience a decline in academic self-concept when surrounded by equally high-achieving peers.
In academia, there is no tradition of helping students learn to cope with pressure or providing psychosocial support (Subotnik et al., 2011). However, Subotnik et al. mentioned that fields like sports and arts have traditionally relied on the support of psychologists to help people perform well under pressure. Sports psychologists have used EDA biofeedback with successful world-level athletes for anxiety and stress management. L. Orione et al. (2021) documented that Olympic-level athletes who could not control anxiety before EDA biofeedback reported developing self-control and a feeling of knowing what to do under pressure after such training. Pusenjak et al. (2015) observed that athletes who could control EDA could also control HRV and anxiety. Subotnik and colleagues suggested investigating how to transfer methods from high-performance settings to gifted and talented education, like honors programs.
Stress and Anxiety in Honors Programs
Colleges often focus on identifying, recruiting, and supporting high-ability students to foster their personal development and societal contributions—two principal objectives of honors programs (Wechsler, 2014). Since their emergence in the early 1900s, honors programs have expanded significantly across the United States, evolving to address not only academic excellence but also the broader needs of high-achieving students. Given the growing recognition of the role psychosocial support plays in talent development, it is essential to examine how these programs assist students beyond academics. The National Collegiate Honors Council (NCHC) emphasizes that honors programs should balance academic rigor with student well-being. Their recommendations highlight the need for tailored support systems and proactive mentorship to help students manage demanding coursework, high expectations, and multiple commitments while fostering both academic success and emotional resilience.
There is encouraging research that underscores the positive outcomes associated with students’ participation in honors programs, linking participation to enhanced academic achievement and psychosocial benefits (Rinn & Plucker, 2019). Honors students often have stronger academic self-concept (Rinn, 2007) and higher retention and graduation rates (Keller & Lacy, 2013). These programs also foster social-emotional growth, as students build strong academic communities and gain specialized opportunities (Young et al., 2016). In addition, honors students engage more with faculty and co-curricular activities (Shushok, 2006). Psychosocial factors play a key role in their development, with honors students reporting higher levels of well-being than their nonhonors peers (Plominski & Burns, 2018). This aligns with research on the importance of self-regulation and resilience in talent development.
However, methodological challenges make it difficult to determine how stress management programs benefit these students. Establishing causality in gifted and honors programs is challenging, as students are assigned based on pre-established criteria rather than random selection, making it difficult to eliminate selection bias (Matthews et al., 2012). Inclusion criteria also vary widely, with some programs relying on IQ scores, whereas others incorporate additional measures such as the Naglieri Nonverbal Ability Test, teacher referrals, or academic performance (Card & Giuliano, 2016). In addition, stress management interventions vary significantly in structure and implementation, making it difficult to compare effectiveness across studies (Rith-Najarian et al., 2019). These methodological challenges hinder efforts to draw strong, generalizable conclusions about the impact of such programs. Furthermore, many experimental and quasi-experimental studies in the gifted education field have struggled to demonstrate clear benefits of participation in gifted and talented programs (Redding & Grissom, 2021; Warne, 2016).
A recent systematic review by Rinn and Plucker (2019) identified 52 empirical studies on honors programs conducted over a 15-year period. Few studies investigated the role of managing stress and anxiety in honors students’ trajectories. One study found that students who graduated from honors programs had higher scores on measurements of stress control than those who withdrew from honors programs (J. D. A. Parker et al., 2017). Henfield et al. (2014) interviewed four high-achieving Asian American honors students and identified several forces that were limiting factors in their social lives. These included high self-standards and pressure to maintain a high GPA. Despite interesting insights about unique social-cultural stressors in the lives of these students, it is difficult to generalize such findings for two reasons: First, all students had similar backgrounds, and second, the study had a small sample size. Rinn and Plucker (2019) lamented the problem of small sample sizes among these studies. Some studies in their investigation did not include sample size estimates. Finally, these studies were more associational and descriptive than causal.
Our literature review did not identify experimental studies focused on stress and anxiety control within honors programs. However, a randomized controlled trial by Ratanasiripong et al. (2012) demonstrated the benefits of biofeedback for college students. Ratanasiripong et al. investigated the effects of a 5-week HRV biofeedback program on stress and anxiety. The researchers observed 60 nursing students in college using two standardized tests (PSS and STAI-AD). People in the biofeedback group had a significant reduction in anxiety, whereas those in the control group had a moderate increase in anxiety. The .68 standard deviation impact indicates that HRV treatment positively influenced nursing students’ perceptions of anxiety. Studies with favorable results, such as the one conducted by Ratanasiripong et al. (2012), provide a direction for researchers keen on investigating the role of biofeedback within honors programs. However, it is important to note that their study only involved nursing students who were not part of an honors program, and the researchers used HRV as opposed to electrodermal EDA. These differences are important because stress experiences—and the mechanisms by which students regulate them—may differ by academic context and physiological training modality. Thus, our study extends the existing literature by examining EDA biofeedback specifically in the context of honors education, where experimental research remains scarce.
Given the particular stressors associated with academic transitions—especially for high-achieving students navigating new academic and social demands—EDA biofeedback may serve as a valuable tool for enhancing stress management skills during this critical period. This study explored the role of biofeedback in supporting honors students at the college level, specifically investigating whether it helped them regulate stress and anxiety responses more effectively and supported their academic performance.
Method
We conducted a single-subject study with five honors students to explore the role of EDA biofeedback in managing stress and anxiety. We used a single-subject A-B-A study design, which had the potential to show how the treatment effected change in small groups of people, illustrating how participants behaved before, during, and after treatment (Olive & Smith, 2005).
Participants
The honors program at a large public university in New England collaborated with us for this research. The honors program participating in this study has existed for nearly six decades and enrolls approximately 2,300 students across multiple campuses and disciplines. Admission criteria differ by applicant type. First-year students are automatically considered based on GPA, class rank (if available), course rigor, extracurricular leadership, and demonstrated talents, with standardized test scores (SAT/ACT) being optional. Current students and transfer students must have a minimum 3.40 GPA and submit an application with an academic record review, personal essay, and résumé. Rising juniors need faculty honors advisor approval and must submit an honors preliminary plan of study. The program incorporates research, leadership, and community projects, requiring students to engage with faculty, interdisciplinary coursework, and hands-on experiences.
The honors program disseminated information about the study to its students via email, along with a dedicated email address for any inquiries. The student inclusion criteria were as follows: (a) They must be enrolled in the university’s honors program, and (b) they must be in the final 2 years of their degree program—a transitional phase from undergraduate to advanced levels of their education. We contacted the first five students who expressed interest, and we conducted individual meetings over WebEx to explain the study’s scope and details. Following these discussions, all participants agreed to partake in the intervention.
Participants were on campus for 2 months for summer jobs and coursework that included final examinations. Three of them were working in laboratories, and two of them were tutoring other students in summer classes. The intervention began at the outset of the summer session and finished before the week of their final summer examinations. Our sample included three 18-year-old female students (one Black [Participant 4], one White [Participant 5], and one Asian [Participant 1]) and two males (one Asian [Participant 3] and one White [Participant 2]).
Measures and Instruments
In this study, we explored the relationship between biofeedback training and students’ ability to control physiological stress responses. Aiming for replicability and reliability in recording the stress signals, we used Thought Technology’s EVu TPS finger instrument and accompanying software app. With this package, we tested, measured, and trained students to manage an index provided by the manufacturer based on three factors: (a) increasing skin temperature, (b) decreasing EDA, and (c) increasing HRV. These three biosignals tend to follow these patterns when people diminish stress responses (Sonkusare et al., 2019).
We calculated averages to determine the effects of our intervention. Each biosignal (e.g., HRV) awarded one potential point every 10 s. A point was given if the success index of the biosignal followed the expected pattern or remained stable after having followed it successfully. When it had recorded 10 s of good data (biosignal success index increased in the case of temperature and decreased in terms of EDA and HRV, and/or then remained stable after following the pattern), it recorded one point and restarted its internal count. Counting did not reset if no new points were awarded for a long duration of time. The maximum number of points that could be scored every 10 s was three: one for HRV, one for EDA, and one for body temperature.
Therefore, we used the physiological stress control index, based on controlling three biosignals (i.e., HRV, EDA, and temperature) provided by the software, as our outcome. Over the course of the sessions, participants were instructed to concentrate only on their EDA lines and were taught using only this measurement. The application we used allowed us to zoom in on this signal. The equipment recorded the physiological stress control index, although students could not see measurements of their HRV and were told to ignore skin temperature (as both EDA and temperature were visible on the screen because of the app layout).
A priori power analysis was not conducted due to the nature of the single-subject A-B-A design, which prioritizes functional relationships over conventional power calculations (Kratochwill et al., 2010). Instead, visual analysis and effect size estimation were used to evaluate intervention effects (R. I. Parker & Vannest, 2009). Session numbers were determined by feasibility rather than statistical power, aligning with single-subject research methods that focus on trend analysis and phase comparisons (Kazdin, 2019). The implications of sample size and statistical power will be addressed in the discussion.
Procedures
In total, we met with students at 18 different points in time. There was an interval of at least 2 days between these meetings. We generally held two meetings a week with each participant over the three phases. In pretreatment, we had three initial meetings to establish a baseline level of the physiological stress control index. This was followed by 12 treatment meetings and three final meetings after removing the treatment.
Pretreatment
This phase focused on three stress control meetings to measure a baseline for students’ physiological stress control index. To establish that baseline, we wanted to collect data when students were under some stress. Roos et al. (2021) conducted a meta-analysis that found a significant association between physiological arousal and test anxiety. Thus, during meetings, participants answered mock test questions from the GRE verbal and quantitative sections to raise their stress levels. Students were asked to perform well on the examinations and to diminish their stress responses without seeing their physiological data. We recorded 14 five-minute physiological stress control index sessions over the three pretreatment meetings: five on the first day, four on the second day, and five on the third day.
Intervention
This phase consisted of 12 30-minute protocols. We scheduled meetings twice a week with each student for 6 weeks. During these meetings, a tablet screen showed participants their EDA levels. At each meeting, we observed the initial EDA levels of each participant for 5 minutes. We used the final point of the initial daily EDA session as a threshold for each treatment. During the following 5-minute sessions, EDA instruments emitted pleasant sounds when participants reached EDA levels below the threshold and unpleasant sounds when participants kept EDA higher than the threshold. Over this 6-week phase, we taught learners how to (a) control movements (Protocol 1), (b) manage thoughts (Protocol 2), (c) control respiration patterns (Protocol 3), (d) diminish EDA (Protocols 4 and 5), (e) keep EDA low (Protocols 7 and 8), (f) diminish EDA rapidly (Protocols 9 and 10), (g) recognize signs of EDA change without the support of instruments (Protocol 11), and (h) practice what they learned to control EDA (Protocol 12). After each of these 12 intervention meetings, we recorded a final stress index measurement for 5 minutes. After each day’s measurements, we reviewed the meeting data with the participant, providing feedback and answering questions about the process. Treatment concluded the week before students’ summer finals. We recorded 53 five-minute physiological stress control index sessions over the three pretreatment meetings.
Post-Treatment
The week after finals, we repeated the baseline measurement process. We address the timing of post-treatment in the limitations section. We had 14 physiological stress control index measurement sessions more than 3 days using different GRE questions taken from the same manual.
Research Questions
Our first research question was whether students would improve their ability to manage stress from baseline to the post-treatment. Thus, we explored: Does participation in the biofeedback intervention lead to significant improvements in students’ ability to manage physiological stress responses from baseline to the end of the intervention phase?
The kind of trend we expect in a baseline phase should be in the opposite direction from the one we expect in the intervention, so that we might infer that the treatment is associated with a therapeutic pattern only after the treatment starts. The contra-therapeutic pattern is desirable in initial baselines in evidence-based single-subject designs (Byiers et al., 2012) for at least two reasons: (a) If it changes during the intervention, it allows us to infer the treatment worked; and (b) it is not ethical to provide unnecessary treatment when people’s ability to manage stress improves before the intervention. This led to our second question: Do students exhibit a contra-therapeutic trend in their physiological stress index during the first phase of the study?
Regarding the slope (the inclination of the dispersion), we wanted to see improvements marked by a negative to positive trajectory, or at least diminishing the severity of the negative slope. If the slope remained negative, we believed it would at least be less pronounced than the pretreatment slope. We hypothesized that students would show improvement on the stress control index after we compared the pre-intervention to the intervention because they would gradually become better at controlling the responses furnished by the equipment. That was our third hypothesis. Therefore, we analyzed: Does the intervention lead to improvements in the slope in the desired direction?
Our fourth hypothesis was that EDA biofeedback would help improve students’ level of stress control in the post-treatment to levels higher than in the pretreatment, despite the treatment ending. In sum, we believed that students’ ability to manage stress would increase from A to B and that, when we removed the treatment, the ability to manage stress would be better than in the pretreatment. As a result, we inquired: Do students maintain improved stress control levels in the post-treatment phase compared with their pretreatment baseline?
Design and Data Analysis
We implemented an A-B-A (i.e., pretreatment, intervention, and post-intervention) single-subject study design. One of the significant advantages of single-subject designs is their ability to facilitate the detection and replication of experimental effects. For example, if we discern that an intervention is effective for Person A, we can attempt to replicate it with other individuals. If the intervention proves successful for Person B and Person C, we gain more confidence in its potential applicability to a broader population (Sen, 2022). In the present era of evidence-based practices, the tools associated with single-subject designs are gaining popularity and are useful for both researchers and practitioners (Kraft, 2020).
Before the 2000s, researchers typically relied on visual analysis, rather than statistical analysis, to assess the effectiveness of interventions in single-subject studies. Olive and Smith (2005) proposed several reasons for this approach. One reason was the robust internal validity of these studies, which could determine the impact of a treatment on individuals within a specific context by examining factors such as level of change and variability. Furthermore, data from single-case designs often violate one or more assumptions required for various statistical procedures, making visual analysis a more fitting method. Olive and Smith (2005) also pointed out that the participants in single-subject studies might not fully represent the general population. Datchuk and Kubina (2011) noted that many research articles documented how visual analysis of single-subject studies can effectively and directly convey experimental results, thereby enhancing scientific communication. In our study, we initially employed visual inspection to analyze individual differences in level, trends, and slopes.
Considering the variability of visual analysis among researchers, some studies have suggested using the celeration line method to generate clear and rich presentation of experimental findings of single-subject studies in fields like health and education (Kenyon et al., 2024; Whiting et al., 2023). We used it to assess how meaningful the changes were from baseline to intervention. This method is normally used in single-subject studies to assess the null hypothesis that interventions have not changed the relative positions of the data points across phases in visual analyses (Rakap, 2015). We used the Split Middle Line and Binomial Test (at the .05 level) to describe level, trend, and slope changes. Specifically, we wanted to understand whether the intervention had changed the relative positions of the data points across phases (comparing the pretreatment with the intervention) so that we might say the proportion of points above the line in the treatment is different from the proportion of points below the line.
Despite existing support for relying on visual analysis instead of statistical analysis with single-subject data, researchers cannot always guarantee the internal validity of single-case research studies (Lambert et al., 2024). Moreover, data derived from single-subject studies are not always linear, especially when studies use few baseline data points, and linearity is one of the assumptions of single-subject studies (Lobo et al., 2017). Furthermore, sometimes schedule limitations, lack of adherence, and attrition compromise the accuracy of observations in educational settings (Beintner et al., 2019; Weidmann & Miratrix, 2021). To ensure a robust baseline, we conducted 14 measurement sessions per participant and spread across 3 separate days within a 10-day span. This dense and structured data collection allowed us to estimate an initial contra-therapeutic trendline and calculate a celeration line to support our visual analysis. Despite these precautions, we also computed effect sizes to supplement and strengthen our interpretation of the intervention’s impact.
APA (2001) suggested that all articles submitted for publication include effect size computations to facilitate readers’ interpretations of the intervention outcome. Following this recommendation, researchers have developed several methods to report effect sizes in regression-based and nonregression-based computation and nonparametric methods. One issue with using different techniques to compute effect sizes of the same data set in single-subject studies is they result in different d values. Sen (2022) observed that the d values obtained from the same data set could estimate the effect size as 0.00, 0.36, 2.18, 3.47, and 2.11. Despite potential discrepancies, because effect sizes allow readers to interpret outcomes, and, above all, because researchers can seldom guarantee linearity in single-subject studies, different authors recommend reporting effect size using nonparametric models of single-subject designs (Rakap, 2015). We used four methods to compare effect size (to illustrate how discrepant they might be). We chose one of the nonregression methods reported by previous research as more suitable to evaluate our type of study.
Results
Our visual analysis compared the pretreatment, intervention, and post-treatment in terms of trend, slope, and level to examine change resulting from our intervention. We provide separate graphics for each participant to show how the stress control levels changed from pretreatment to the intervention and from the intervention to the post-treatment phase.
Participant 1
First, we analyzed level changes from baseline to treatment. The solid horizontal line over the different phases indicates level (see Figure 1). The mean line changed from 31.71 to 39.83. We also saw a change in trend and slope indicated by the dashed line. At pretreatment, we saw a decelerating trend and a negative slope (−2.71), which, in the context of this study, indicates a contra-therapeutic trend (indicating less stress control).
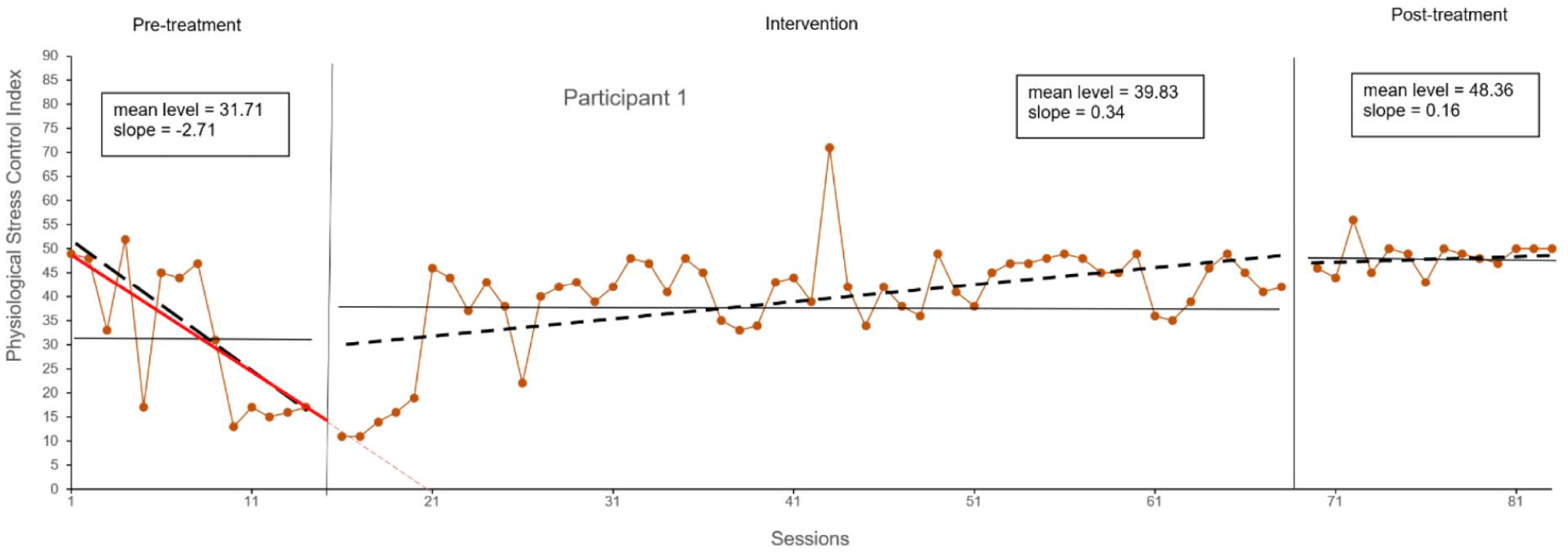
Participant 1’s Physiological Stress Response Control Index Over the Three Phases.
In the second phase (the intervention phase), the trend and the slope changed from negative to positive, thus showing a therapeutic effect (0.34). By therapeutic, we refer to the direction of the desired treatment outcome, indicating a higher physiological stress control index. Thus, the change from the negative/contra-therapeutic slope/trend to a positive therapeutic pattern associated with a difference in average (increasing the stress control index average from 31.71 to 39.83) provided evidence that the treatment was effective for Participant 1 in terms of controlling stress. After the withdrawal of the treatment (in the post-treatment phase), Participant 1 showed an increase in level (from 39.83 to 48.36) and kept the positive trend (slope reduced from 0.34 to 0.16). We used the celeration line method and did a binomial test associated with it that indicated the changes in the dispersion of the points from pretreatment to the interventions were significant (p < .001).
Participant 2
We saw a change in level from baseline to treatment, as the mean line changed from 35.64 to 39.56 (see Figure 2). We also saw a change in trend. During the pretreatment phase, we can see the dispersion had a negative, contra-therapeutic slope (−2.96).
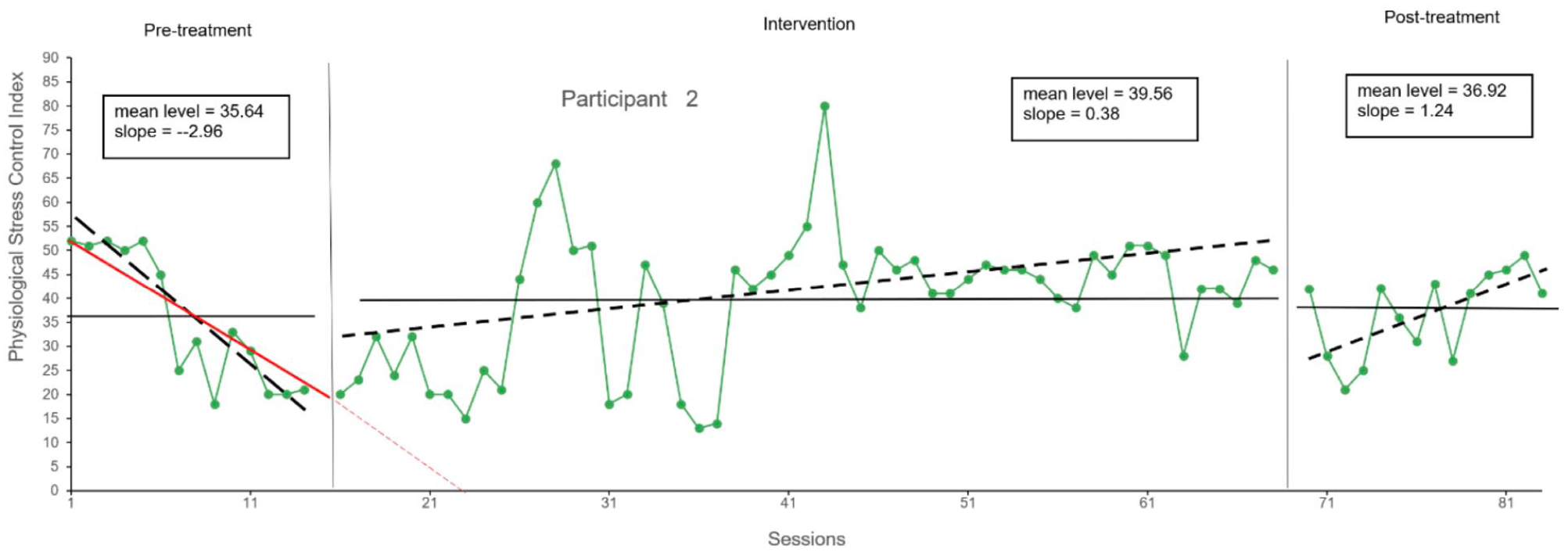
Participant 2’s Physiological Stress Response Control Index Over the Three Phases.
In the intervention phase, the trend changed from negative to positive, becoming therapeutic (0.12). Like Participant 1, the change from the negative/contra-therapeutic pattern to a positive, therapeutic pattern provided some evidence that the treatment worked for Participant 2. The celeration line indicated that pretreatment to intervention changes were significant (p < .001). When we removed the treatment, the trendline remained therapeutic (with a positive slope dropping from 0.34 to 0.16). The average mean decreased from 39.56 to 36.92 but was higher than in pretreatment.
Participant 3
Analyzing the data of Participant 3, we saw a clear change in level from baseline to treatment, as the mean line changed from 22.05 to 42.77 (see Figure 3). We also saw a change in trend from the initial baseline phase to the intervention phase. At the pretreatment phase, we saw a contra-therapeutic trend with a negative slope (−2.96). In the intervention phase, the trend and slope changed from contra-therapeutic/negative to therapeutic/positive (0.12). Similar to Participants 1 and 2, the change from the negative/contra-therapeutic pattern to a positive and therapeutic pattern provided evidence that the treatment worked for Participant 3 and was significant using the celeration line (p < .001).
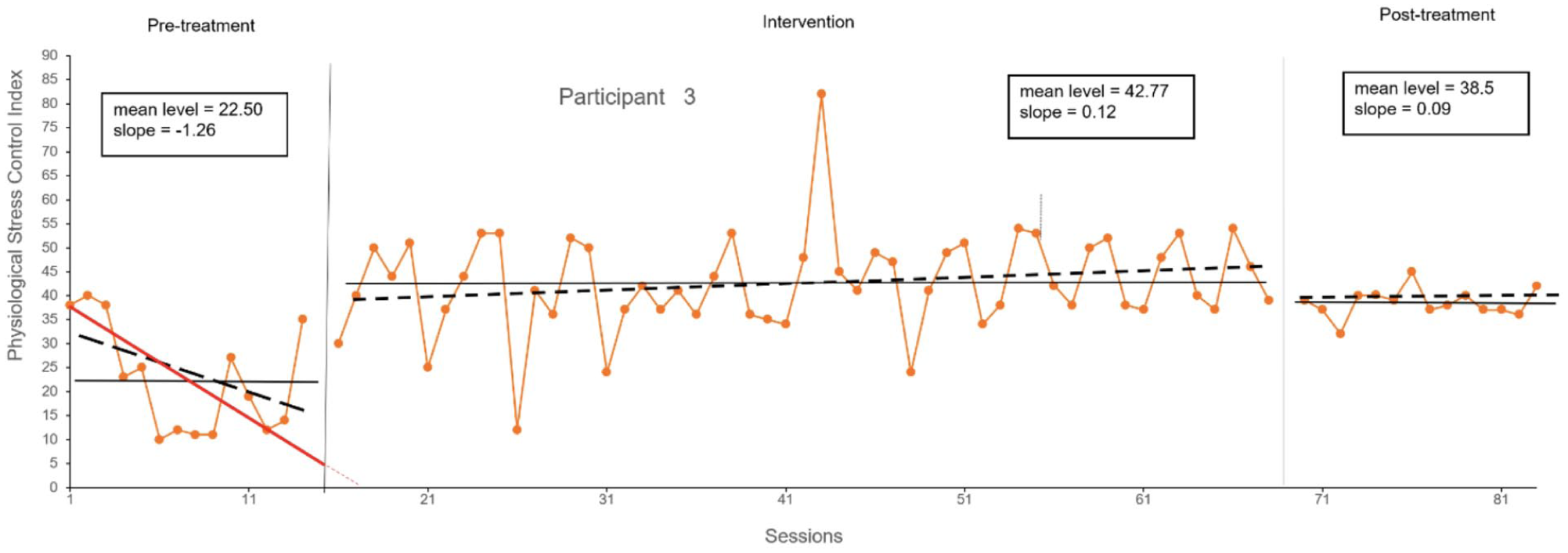
Participant 3’s Physiological Stress Response Control Index Over the Three Phases.
As with Participant 2, when we removed the treatment, the average mean decreased (42.77–38.5) but was higher than in the pretreatment phase. The trendline in the last phase stayed positive, despite slope magnitude decreasing from 0.12 in the intervention to 0.09 in post-treatment.
Participant 4
We saw a change in level comparing the averages in the pretreatment and intervention phases from 35.64 to 39.56 (see Figure 4). At the pretreatment phase, we observed a negative slope and contra-therapeutic trend (−1.64), indicating a decline in stress control. This negative trend continued during the treatment phase, although the slope reduced from −1.64 to −0.12, reflecting a slower rate of decline in stress control. The celeration line analysis revealed that the changes between the pre-intervention and treatment phases were statistically significant (p < .001). Upon the removal of the treatment, the average control level dropped slightly from 39.56 to 38.5. Notably, the post-treatment average remained higher than the pretreatment average of 34.5. In addition, the trendline and slope, which had been negative and contra-therapeutic, shifted to a slope of 0.00, indicating a stabilization of stress control after the intervention phase.
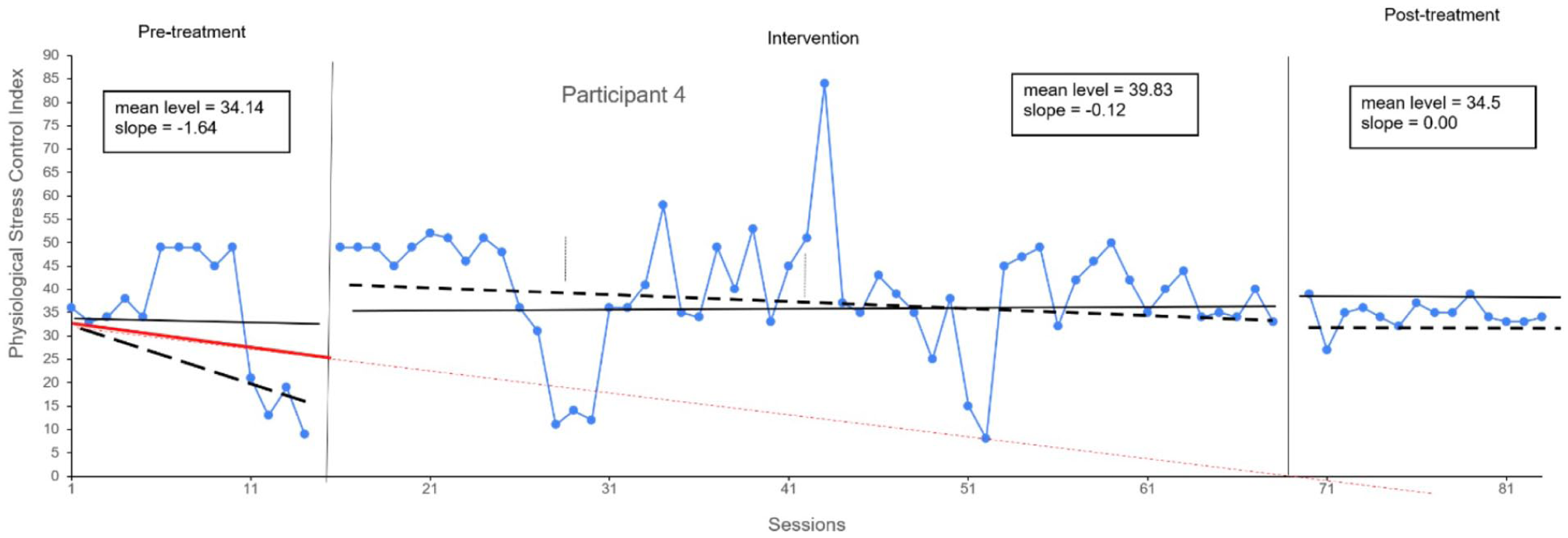
Participant 4’s Physiological Stress Response Control Index Over the Three Phases.
Participant 5
We saw a slight change in level comparing the averages in the pretreatment and intervention phases from 45.42 to 45.83 (see Figure 5). At the pretreatment phase, we saw a negative slope and contra-therapeutic trend (−0.15). As with Participant 4, the trend and slope stayed negative and contra-therapeutic over the course of treatment. Also similar to Participant 4, the inclination of the slope diminished from −0.15 to −0.03. The slight change in level and the slight reduction in the inclination of the slope from −0.12 to −0.03 seem to be a signal that the treatment worked for Participant 5 with some reservations. These changes seem visually to be small. The celeration line method indicated that changes were only marginally significant (p = .049). When we removed the treatment, the average mean increased from 45.83 to 49.57 (higher than in the pretreatment) and the trendline changed from −0.03 to a positive/therapeutic trend of 0.2. The fact that the initially contra-therapeutic trend became a therapeutic one in the post-treatment phase, with the final level higher than in the pretreatment phase, seemed to be a positive signal that participant developed stress control skills, especially in the context of the study. The self-regulatory intervention aimed at participants acquiring some level of knowledge compared with what they had before the treatment.
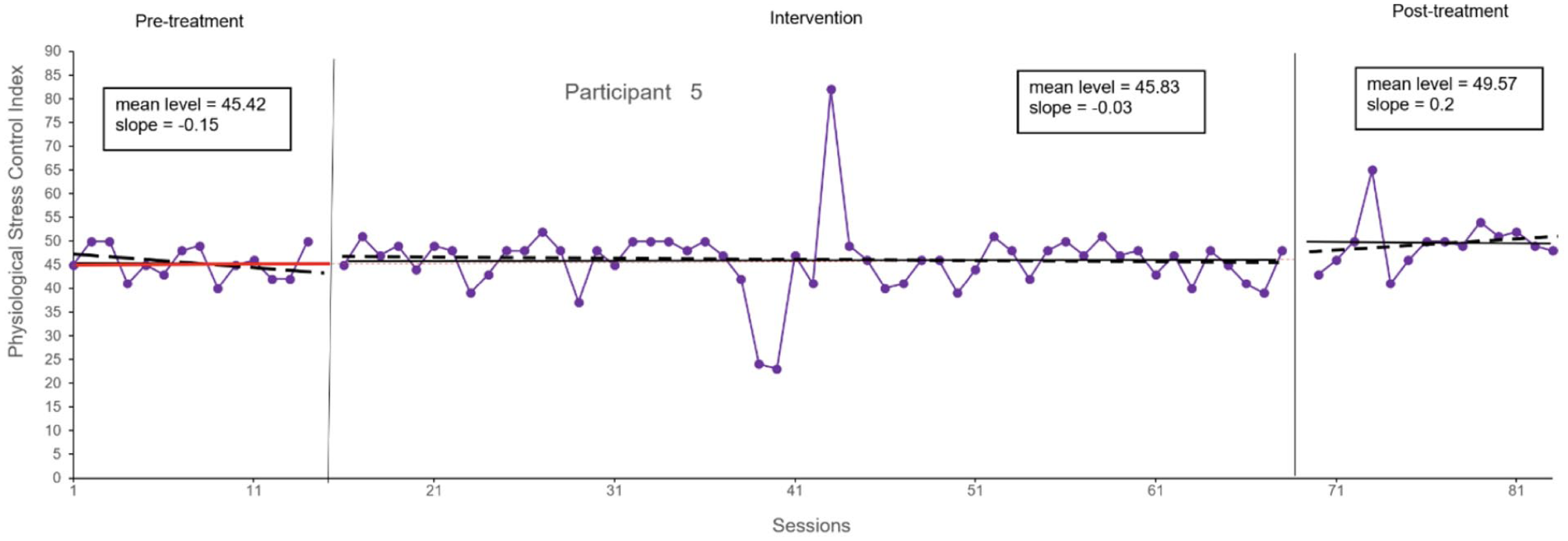
Participant 5’s Physiological Stress Response Control Index Over the Three Phases.
We hypothesized that participants’ average stress control index scores would increase from pretreatment to the intervention and that their averages would be higher than initial levels. All participants’ physiological stress control index averages increased from baseline to treatment (see Figure 6). Participants 2, 3, and 4 showed a reversed tendency from the intervention to the post-treatment phase with a decrease in their average control from intervention to post-treatment. Considering Participants 1 and 5, we see improvement from pretreatment to the intervention phase and further improvement from treatment to post-treatment. Their average stress response control improved continually. In sum, students’ average stress control during the post-treatment was on average higher than in the pretreatment for all students.
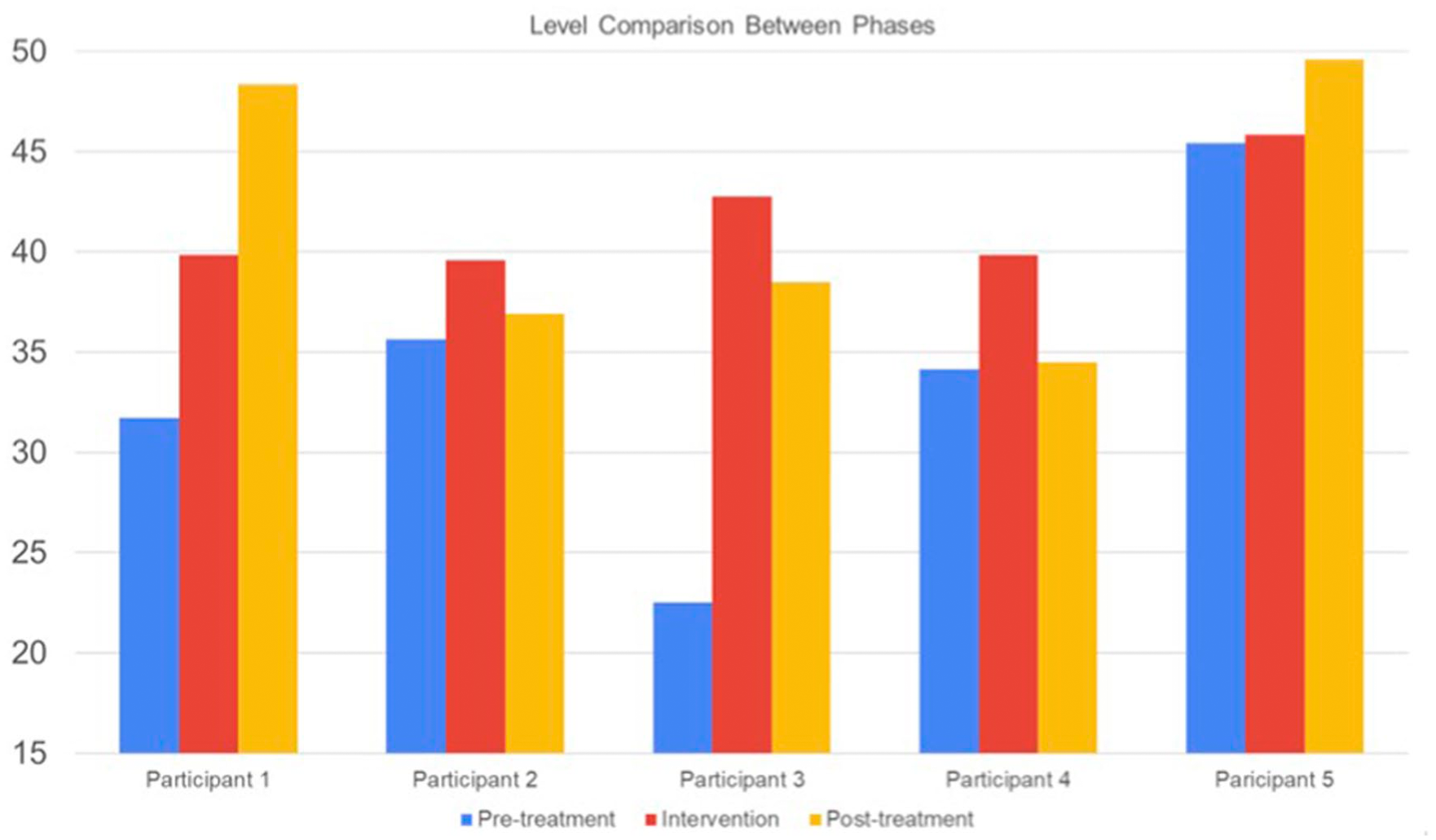
Average Physiological Stress Response Control Index Over the Three Phases.
Effect Size Computation
We used four methods to compute the effect size of our intervention (Rakap, 2015): (a) the percentage of nonoverlapping data (PND); (b) the mean baseline reduction (MBR); (c) the standardized mean difference using the last three data points from both the baseline and intervention phases, which we label as SMD-3; and (d) a version of the standardized mean difference using all data points from both phases, which we label as SMD-AD. We calculated the PND for each data set by counting the number of data points during the intervention phase that were higher than the highest pretreatment data point. We divided the result by the total number of data points in the intervention and pretreatment phases and multiplied it by 100. We use the average of the last three sessions of the intervention to calculate the MBR, which was multiplied by 100. To compute the SMD3 for each participant, we subtracted the last three intervention points minus the mean of the last three baseline points, divided by the standard deviation of the baseline. The average impact in this scenario was 0.62. We computed the SMD-AD considering the full baseline and intervention phases, which is more robust than using only the last three data points. We divided this number by the standard deviation of the pretreatment. The average impact in this scenario was 0.74 (see Table 1).
Effect Size Computations.

The interpretation of the program’s effect on students’ ability to increase stress control varied depending on the measurement method used. For instance, Participant 1 showed the highest improvement in stress control when assessed using MBR. However, if we compared his results with others using effect sizes, the treatment would appear to have had the smallest impact on him. Besides that, we can also see differences in terms of the direction of the effect. Participants 4 and 5 would have a positive effect size in three of the four methods, but, using SMB-AD, Participant 4 would have a negative effect. If we chose the MBR, Participant 5 would be the one with a negative effect, but none of the others would. Participants 1, 2, and 3 had positive effect sizes across all forms of computation.
Discussion
Research Question 1: Improvements in Stress Management From Baseline to Intervention
Visual inspection and effect size analysis revealed that all participants improved their ability to manage stress during the intervention phase. Our results converge with Ravada et al. (2023), who found that first-year medical undergraduates in biofeedback relaxation training experienced significant reductions in stress and anxiety. This parallel is particularly relevant because, like our participants, their study focused on first-year undergraduates navigating a critical academic transition—a period when effective stress regulation is especially important. De Witte et al. (2019), in a systematic review of 14 randomized controlled trials, likewise found that 75% of biofeedback interventions produced improvements in either physiological or psychological stress indicators. Our findings expand this evidence by demonstrating comparable outcomes with EDA-based interventions among honors students. Together, these results highlight that biofeedback may consistently improve stress management skills in student populations while extending this evidence base to the academically advanced honors context.
Research Question 2: Contra-Therapeutic Trends During Baseline
Participants displayed contra-therapeutic or negative slopes during baseline, which then reversed once the intervention began. This pattern is not unexpected in academic contexts, as stress often escalates in the weeks leading up to final examinations. In our study, participants completed the treatment just 1 week before their summer course finals, a period when academic stress is typically at its peak. Roos et al. (2021), in their meta-analysis, showed that physiological arousal is strongly associated with student test anxiety, underscoring why untreated baselines may naturally deteriorate as examination period approach. Ratanasiripong et al. (2012) further demonstrated that biofeedback training significantly reduced anxiety among nursing students, underscoring that once intervention is introduced, contra-therapeutic trends can be effectively reversed. Byiers et al. (2012) similarly noted that negative slopes are common in baseline phases of single-case designs and that successful interventions typically reverse this trajectory. Our results expand this literature by demonstrating the same baseline-to-treatment reversal among honors students, a population rarely examined in stress management trials. Furthermore, Olive and Smith (2005) emphasized that reversal of contra-therapeutic baseline trends is a methodological hallmark of well-controlled single-case interventions. Our findings support this view, showing that baseline deterioration was not incidental but part of a replicable pattern that strengthens causal inference.
Research Question 3: Changes in Slope and Trajectory
Our third question was whether the intervention led to improvements in the slope in the desired direction, increasing the stress control index. All trendlines shifted from pretreatment to intervention. Students showed negative slopes during baseline, which then changed to positive slopes once the intervention began, while others showed a clear reduction in the steepness of their negative slopes. This pattern converges with Rodrigues et al. (2022), whose systematic review reported consistent improvements in stress trajectories among university students following biofeedback interventions. It also aligns with other studies that reported improvements in stress trajectories after biofeedback therapies were implemented in educational settings (Aritzeta et al., 2022; Meier & Welch, 2016). These results suggest that the slope changes we observed are not incidental but reflect a meaningful acquisition of stress regulation skills. As Byiers et al. (2012) noted, negative slopes are often observed during baseline in single-case designs and tend to reverse once an effective intervention is applied. Our findings expand this evidence by showing that EDA biofeedback produces comparable slope improvements among honors students, a group rarely examined in experimental stress management research.
Research Question 4: Post-Treatment Maintenance of Stress Control
Finally, we asked whether students would maintain improved stress control levels in the post-treatment phase compared with their pretreatment baseline. The increase in the physiological stress control index score by Participants 1 and 2, observed after removal of the treatment, can be interpreted in two ways. First, in line with our Hypothesis 4, this suggests that students may have internalized stress regulation strategies and continued to apply them autonomously, indicating a sustained effect. Evidence for such maintenance has been observed in prior research: Rith-Najarian et al. (2019), in a systematic review of 68 prevention programs, found that many physiologically based interventions produced effects that extended beyond the treatment phase. Our findings expand this evidence by showing similar post-treatment maintenance in honors students, a group rarely included in stress management trials. At the same time, not all participants maintained their gains to the same extent, with some showing partial declines. This variability mirrors patterns described by Rith-Najarian et al. and highlights that sustained benefits may depend on individual differences and contextual support. Second, the observed stability also aligns with educational perspectives on self-regulated learning. Oates (2019) emphasized that one of the goals of effective instruction is to help learners acquire autonomy in applying strategies after explicit guidance. From this perspective, maintenance of gains is not incidental but reflects the broader educational aim of equipping students with enduring self-regulation skills.
On the contrary, from an evaluative perspective of the treatment, some researchers might contend that we cannot definitively attribute their improved physiological stress control to the treatment. Nevertheless, we posit that within the context of this study, it is encouraging to observe an enduring effect post-treatment. This aligns with the overarching aim of self-regulation interventions, which is to equip students with long-term autonomous capabilities. However, it is important to note that other participants (Participants 3 and 4) did not exhibit the same pattern, as the effect diminished after the treatment was withdrawn. In classic A-B-A interventions, such a decline might be seen as evidence that the treatment had the intended effect while it was administered. However, in the context of self-regulation, sustained improvements are the desired outcome, making a lasting effect more favorable.
Effect Size
Different forms of effect size computation suggested by the literature change the interpretation of effects. Depending on the method, students in our study appear to have different levels of improvement. Also, despite showing a general positive effect size in all our measurements, two of them would have a negative overall effect, if we chose those methods. We provide the effect sizes from different computation methods in Table 1, so that the reader can compare them (Sen, 2022). Here, we opted to focus on SMD-AD for several reasons. First, the SMD-AD is “d” itself, using simple computations that others can easily check and are familiar with. It is recommended as a better option to compute the effect size of a single-subject study than the PND or the MBR (Olive & Smith, 2005; Rakap, 2015). This is especially important in reversal designs, where the interpretation depends on observing consistent patterns across multiple phases. By incorporating all data points, SMD-AD captures the full trajectory of change and any return to baseline, rather than anchoring the effect size on isolated time points that may not represent phase-wide behavior.
Thus, the average effect size using the SMD-AD was d = 0.74. This impact is considered moderate by some authors, but for others, especially in education, this is a large impact for a 2-month intervention. Individually, Participant 1 (d = 0.67), Participant 2 (d = 0.74), Participant 3 (d = 1.44), and Participant 5 (d = 0.73) showed an increase in their average control of physiological stress responses. Only Participant 4 (d = −0.08) had a small negative effect size on the control of physiological stress responses over the treatment.
Limitations and Recommendations for Future Research
We conducted this study in one university’s honors program with a small sample, which limits our ability to generalize these results. This study meets two of the four What Works Clearinghouse Single-Case Design criteria (Kratochwill et al., 2010). It satisfies the requirement for systematic manipulation of the independent variable and includes at least three data points per phase. However, it does not meet the criteria for multiple assessors, as data collection relied on a single implementer, nor does it demonstrate the intervention effect at three distinct points. The study used an A-B-A design, which does not meet the WWC standard requiring A-B-A-B, multiple baseline, or similar designs. Thus, we cannot assume causality and state that the treatment effect occurred solely because of the treatment, despite being associated with it and having a moderate-to-large effect size. Future studies should consider replicating this research in different locations with larger samples. We recommend future researchers consider conducting a larger, randomized control group design with the relaxation strategies we used. We also recommend comparing the effectiveness of biofeedback with honors students and nonhonors students to understand whether it impacts honors students differently. Finally, future researchers might consider including additional measures of stress beyond a physiological stress control index when measuring the effectiveness of biofeedback. This might include the use of self-reported stress rating scales and actual improvements in academic performance.
We also would have benefited from biofeedback equipment that displayed students’ averages on EDA, HRV, and temperature independently and not simply in the overall success index calculated by the instrument. However, the equipment and software needed to do so are prohibitively expensive and would limit general application of the techniques we tested for this study.
An additional limitation to acknowledge is that we did not evaluate the stability of the data points. Gerstorf et al. (2009) noted that the within-person variability of state-anxiety tends to be substantial, particularly among those not trained in its control. The literature is still unclear on the causes of this phenomenon. However, given the significant variability of state-anxiety—the type of stress potentially most significantly influenced by biofeedback, as suggested by Ratanasiripong et al. (2012)—we decided that evaluating stability in such a context might not yield meaningful insights. We recognize that more stable baselines could facilitate our understanding of the changes in patterns observed among students from the pretreatment phase to the intervention phase in this study.
Finally, we collected our post-treatment data shortly after the formal examination period had ended. Although participants were still in an academic setting and engaged with GRE-like tasks during data collection, it is possible that the absence of real-time academic consequences (such as actual grades) reduced their stress levels compared with the treatment phase. This timing may have influenced their ability to regulate stress, potentially confounding the interpretation of sustained treatment effects.
Conclusion
Stress and anxiety are relevant problems for college students in the United States. Students in honors programs are not immune to their effects. Despite physiologically based programs being positively associated with improving stress and anxiety control among college students, talent development researchers have few studies guiding them how to use these tools with honors students. All students in our study showed a negative trend in physiological stress response control before treatment, yet all of them were able to change the pattern after engaging in EDA biofeedback treatment and demonstrated better stress control in the intervention compared with the pre-intervention phase. Ultimately, all of them also had better stress control in post-treatment than in pretreatment. Despite these two positive findings and a d = 0.74 average effect size (which some would consider strong for a 2-month intervention), our limited sample does not allow us to generalize. However, given the paucity of empirical studies that show the positive aspects of this technique in talent development programs, this study provides an important piece of evidence in understanding the impact of EDA biofeedback on improving honors students’ stress control.
Footnotes
Ethical Considerations
Ethical approval for this study was obtained from the University of Connecticut, Department of Educational Psychology Institutional Review Board (approval no. H22-0042) on May 22, 2022.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Open Science Disclosure Statement
The data analyzed in this study are not available for purposes of reproducing the results. The code or protocol used to generate the findings reported in the article is not available for purposes of reproducing the results or replicating the study. There are no other newly created, unique materials used to conduct the research.
Artificial Intelligence Use
The authors confirm that no generative AI tools were used in the development of this article.