
Abstract
Objective:
Previous studies indicate that national traumatic events, particularly terror attacks, have a broad impact on the general population, including individuals not directly exposed. However, research on how such events affect inattention and hyperactivity/impulsivity symptoms in individuals with ADHD remains limited.
Method:
This study examined the impact of the October 7 terror attack in Israel on ADHD-related symptoms. Young adults with and without ADHD (43 ADHD and 42 control) completed assessments of current and childhood ADHD symptoms, as well as anxiety, at two time-points: before and after the national traumatic event. Participants also reported their level of exposure to the October 7 attack and the subsequent war.
Results:
The control group showed a substantial increase in inattention and hyperactivity/impulsivity symptoms after the attack, whereas the ADHD group exhibited no such increase and instead showed a slight reduction in symptom severity. Changes in symptoms in both groups were not influenced by direct exposure to an immediate threat. The increase in symptom severity tended to decline over time and was positively correlated with heightened anxiety symptoms.
Conclusion:
These results suggest that national traumatic events can temporarily increase inattention and hyperactivity/impulsivity symptoms among young adults without an ADHD diagnosis, even if they were not directly exposed to the events. This increase tends to return to baseline over time. Conversely, individuals diagnosed with ADHD did not experience a worsening of symptoms and instead showed a slight reduction in severity, particularly in inattention, following the traumatic event. Future research should further explore the functional capabilities of individuals with ADHD under acute stress to deepen the understanding of this relationship.
Introduction
National traumatic and catastrophic events, whether instigated by human actions such as warfare and terror attacks or triggered by natural disasters, represent a pervasive phenomenon with profound implications for societal well-being. The psychological impact of such events is thought to extend far beyond the immediate victims, affecting the broader population, including individuals who were not directly involved in the crisis (Hansen et al., 2016). The widespread impact of national traumatic events on large communities can significantly affect well-being, work, and academic function, potentially increasing societal burden (Schein et al., 2022). Research indicates that exposure to terror-related incidents can substantially elevate stress levels across communities, leading to heightened anxiety and depression (Gabriel et al., 2007; Salguero et al., 2011). However, much less is known about how such events influence psychiatric symptoms beyond anxiety and depression. Moreover, it remains unclear how these events affect vulnerable populations already experiencing elevated psychiatric symptoms. In this study, we examined the impact of national traumatic events (i.e., warfare and terror attacks) on young adults with and without ADHD. Specifically, we investigated whether the influence of national traumatic events extends beyond increased anxiety levels to also affect symptoms of inattention and hyperactivity/impulsivity in young adults with and without an ADHD diagnosis.
Psychological effects of war and terrorism can manifest in various forms, including posttraumatic stress disorder (PTSD), anxiety, and depression, which are exacerbated by the societal context in which these events occur (Joseph & Jaswal, 2014). The concept of psychological warfare underscores the intention behind terrorist acts, which aim to instill fear and manipulate public sentiment, thereby achieving broader political goals (Sarma et al., 2023). Therefore, it is not surprising that the psychological ramifications of national traumatic events are not confined to immediate those experiencing direct and immediate physical threats; they also encompass broader societal implications. The fear and uncertainty generated by terrorism can lead to a collective sense of insecurity, particularly pronounced in areas affected by ongoing conflict or violence (Charlson et al., 2012). For example, studies have shown that following the 9/11 attacks, even individuals who were only indirectly exposed to violence, such as through media coverage, report heightened levels of stress and avoidance behaviors, demonstrating the pervasive nature of trauma in the aftermath of terror attacks (Kristensen et al., 2016; Rigutto et al., 2021). Furthermore, a systematic review on the mental health of children and adolescents in conflict zones revealed that a significant percentage of youth reported exposure to terror-related media, which correlated with increased psychological distress, even among those who had not directly experienced violence (Comer et al., 2014; Hansen et al., 2017). This suggests that the emotional and cognitive appraisals of disaster events are influenced by various sources of information, including media portrayals, which can amplify feelings of fear and anxiety within the general population (Kristensen et al., 2016; Yasmeen & Kausar, 2022).
Despite extensive evidence on the impact of national trauma on stress and mood, little is known about how such events influence ADHD symptoms in individuals diagnosed with the condition. ADHD is characterized by two core symptom domains: (a) inattention, which involves difficulties in maintaining focus, sustaining attention, and organizing tasks, often manifesting as forgetfulness, distractibility, and a tendency to overlook details (Barkley, 2014); and (b) hyperactivity and impulsivity, which encompass excessive restlessness, fidgeting, difficulty waiting for one’s turn, and acting without forethought (American Psychiatric Association, 2013). ADHD affects approximately 5% to 7.5% of children and around 2% to 5% of adults worldwide (Polanczyk et al., 2007; Salari et al., 2023), with symptoms impairing various aspects of life, including academic performance, peer relationships, and overall quality of life (Faraone et al., 2021; Liu et al., 2018). Given these challenges, it is crucial to examine whether national traumatic events further exacerbate inattention and hyperactivity/impulsivity in individuals with ADHD.
National traumatic events may lead to an increase in ADHD symptoms, in part because stress can negatively impact executive functions, which are critical for goal-directed behavior. Indeed, it is well-documented that stress can impair executive functioning (Jurgens & Hayes, 2023; Shields et al., 2016). For example, a meta-analysis by Shields et al. (2016) demonstrated that stress disrupts working memory and cognitive flexibility (albeit with smaller effects on inhibition). Deficits in executive function have long been recognized as a core feature of ADHD (Barkley, 1997, 2012). Accordingly, individuals who already exhibit executive dysfunction—such as those with ADHD—may experience an even greater decline in these functions when exposed to stress, further exacerbating their ADHD symptoms.
Another key reason to hypothesize that stress induced by national trauma may affect ADHD symptoms lies in the state regulation model, which is closely embedded in the Cognitive-Energetic Theory (Sergeant, 2000; Van der Meere & Sergeant, 1988). According to this model, individuals with ADHD are thought to be characterized by difficulties in regulating their level of arousal (e.g., underarousal or fluctuating arousal). Specifically, the state regulation model proposes that individuals with ADHD struggle to modulate their energetic states in response to changing contextual demands. In low-demand settings, they may appear underaroused or inattentive, whereas in high-simulation scenarios, they can become overstimulated or disorganized. Because stress can acutely elevate or destabilize physiological arousal, it has the potential to disrupt the already fragile balance of energetic states in individuals with ADHD. National traumatic events often create sudden, unpredictable changes in everyday contexts, requiring increased emotional and cognitive resources to cope. This rapid shift can overwhelm the already vulnerable regulatory systems of individuals with ADHD, resulting in exacerbated cognitive and behavioral symptoms. Consistent with these theoretical frameworks, studies have largely shown that individuals with ADHD are sensitive to stress, with numerous studies linking stressful life events to heightened ADHD symptoms across the lifespan (Hartman et al., 2019; Humphreys et al., 2019; Salla et al., 2019; Summerton et al., 2023).
However, somewhat counterintuitively, there are a few theoretical reasons to assume that national traumatic events might reduce ADHD symptoms, provided that the experienced stressor is very mild. Stress, defined as a response to perceived challenges or threats, involves both psychological (e.g., tension, worry) and physiological (e.g., elevated cortisol levels) changes. Moderate stress can increase arousal, leading a heightened state of alertness and cognitive control in the central nervous system. For example, studies in the general population have shown that exam-related stress improves task-switching and Stroop task performance (Kofman et al., 2006), and mild social evaluative stress enhances executive function in individuals with specific dopamine-related genetic variants (Zareyan et al., 2021). According to the state-regulation model, a slight increase in arousal can, in some cases, alleviate ADHD symptoms (Sergeant, 2000; Van der Meere & Sergeant, 1988). Accordingly, studies have shown that the increased arousal induced by fast incentives and a high event rate in computerized cognitive testing can improve the performance of individuals with ADHD (Isaac et al., 2024; James et al., 2016).
The present study aimed to assess the impact of national trauma and warfare on stress and ADHD-related symptoms in young adults with and without ADHD. On October 7, 2023, a terror attack in Israel targeted civilians across multiple locations, resulting in over 1,500 deaths and widespread kidnappings. The subsequent war led to large-scale military conscription. This study examined how these traumatic events affected stress levels and ADHD symptoms in young adults, both with and without ADHD who had little to no direct exposure to violence, in the immediate weeks following the war’s outbreak. We leveraged pre-existing data on anxiety and ADHD-related symptoms collected before the October 7, 2023, attack and reassessed participants afterward to evaluate changes in symptom levels. Our objective was to estimate the extent of the impact on both the general population and the more vulnerable ADHD group. We hypothesized that these events would substantially increase anxiety in both ADHD and non-ADHD individuals, acting as an acute stressor even in the absence of a direct physical threat. Furthermore, based on executive function and state regulation models, we predicted that increased stress would exacerbate ADHD symptoms in both groups, with a greater effect in the ADHD group.
Method
Participants
Participants were recruited through email lists and social media advertisements. A total of 173 individuals expressed interest in participating. Of these, 53 were excluded based on the following criteria: uncertainty regarding a community diagnosis (9 participants), scoring above the cutoff on a substance or alcohol addiction questionnaire (9 participants), neurological issues (1 participant), and reporting a psychiatric disorder or using psychiatric medication (34 participants). Additionally, two participants were excluded due to inconsistencies between their community diagnosis and the results of the Diagnostic Interview for ADHD in Adults (DIVA; Kooij et al., 2010). Thus, 118 participants remained and completed the measures at Time 1. At Time 2, the research team contacted all participants, and 85 responded. These 85 individuals comprised the final sample, with 43 participants in the ADHD group and 42 in the control group (see Table 1 for sample characteristics). The study was approved by the Research Ethics Council of Tel Aviv University, and all participants provided informed consent. All participants took part in the study voluntarily. At Time 1, participants received either monetary compensation (40 NIS/hr) or equivalent course credit for their participation. At Time 2, participation was uncompensated, with participants encouraged to contribute in the interest of advancing scientific understanding.
Sample Characteristics for ADHD and Control Groups at Time 1.
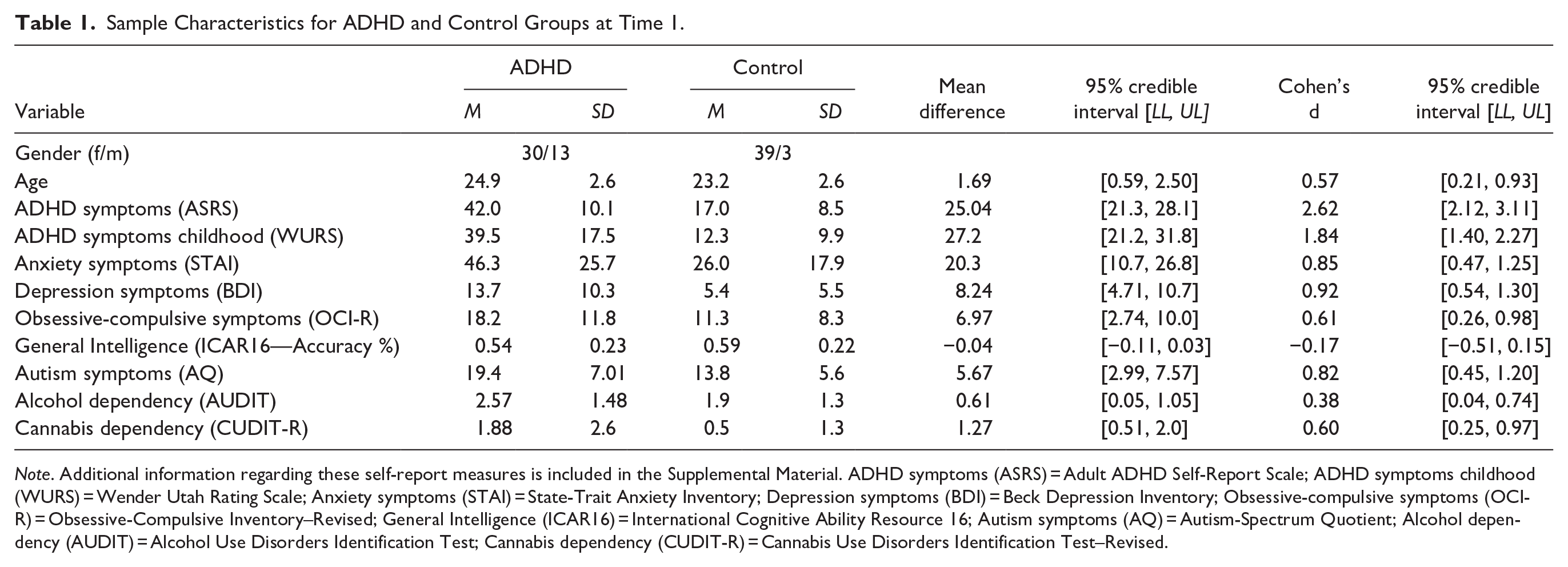
Note. Additional information regarding these self-report measures is included in the Supplemental Material. ADHD symptoms (ASRS) = Adult ADHD Self-Report Scale; ADHD symptoms childhood (WURS) = Wender Utah Rating Scale; Anxiety symptoms (STAI) = State-Trait Anxiety Inventory; Depression symptoms (BDI) = Beck Depression Inventory; Obsessive-compulsive symptoms (OCI-R) = Obsessive-Compulsive Inventory–Revised; General Intelligence (ICAR16) = International Cognitive Ability Resource 16; Autism symptoms (AQ) = Autism-Spectrum Quotient; Alcohol dependency (AUDIT) = Alcohol Use Disorders Identification Test; Cannabis dependency (CUDIT-R) = Cannabis Use Disorders Identification Test–Revised.
Procedure
At Time 1, between January 2022 and June 2023, recruitment was conducted for another study on decision-making in ADHD. At that time, all participants provided consent to be contacted for future studies. At Time 1, participants were screened to ensure they met inclusion criteria (i.e., absence of psychiatric disorders other than ADHD, no psychiatric medication consumption, no neurological conditions, epilepsy, genetic disorders, or substance or alcohol abuse). We ensured that all participants in the ADHD group, and none in the control group, had a formal ADHD diagnosis from a licensed mental health professional. To confirm the presence or absence of ADHD diagnosis at the time of testing, participants in both the ADHD and control groups underwent further assessment using a semi-structured interview for diagnosing adult ADHD (DIVA, Kooij et al., 2010). These interviews were conducted by well-trained psychology students under the direct supervision of a licensed clinical psychologist specializing in ADHD. Participants then completed a battery of self-report measures to assess the level of co-occurring psychiatric symptoms (see Table 1 and Supplemental Material). Additionally, participants completed the study’s primary measures, which evaluated current ADHD symptoms, childhood ADHD symptoms, and anxiety.
At Time 2, during the first 2 weeks of November 2023, following the October 7, 2023 terror attack, the research team contacted all participants who had taken part at Time 1. Those who showed interest were invited to participate in Time 2 assessment. Participants were reassessed for current ADHD symptoms, retrospective childhood ADHD symptoms, and anxiety levels. At Time 2, participants were also asked about their level of exposure to the October 7 events, which is reported in Table 2.
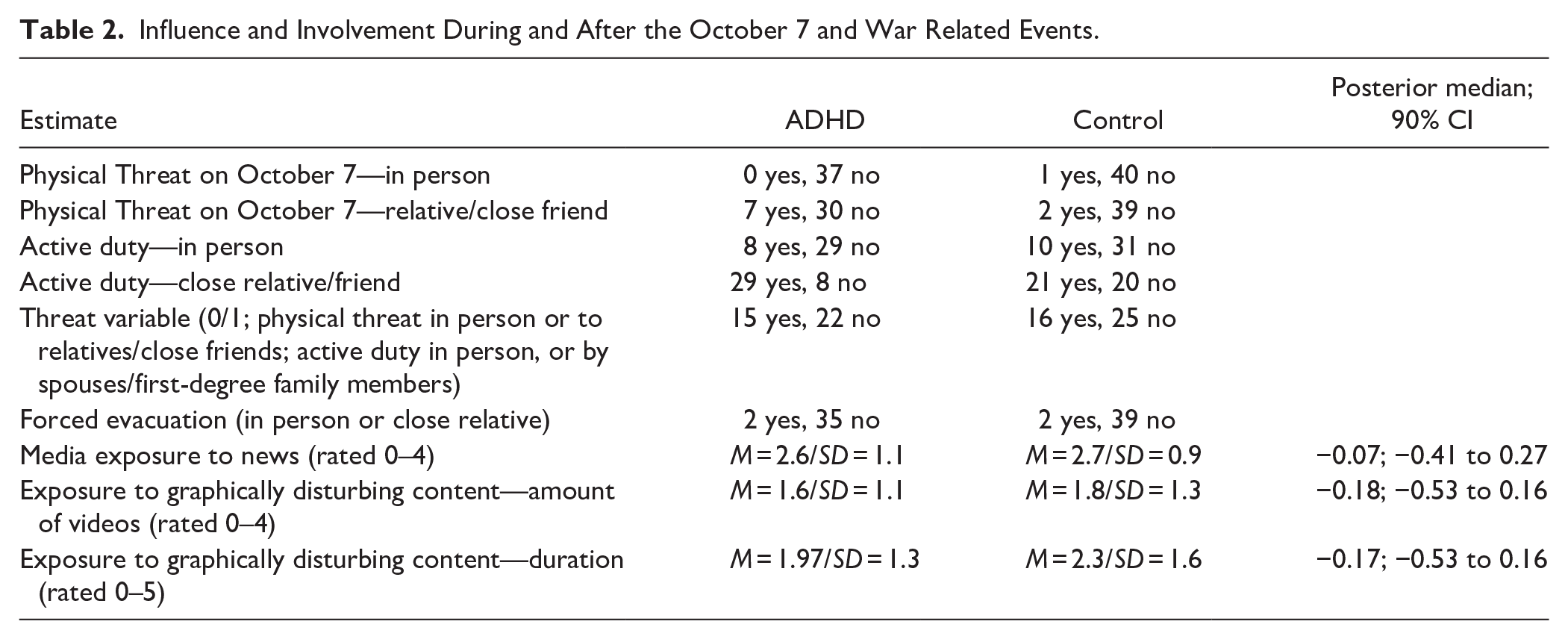
Influence and Involvement During and After the October 7 and War Related Events.
Measures
Current ADHD symptoms
ADHD symptoms at present were assessed using the Hebrew version of the Adult ADHD Self Report Scale (ASRS-v1.1; Kessler et al., 2005; Zohar & Konfortes, 2010). This questionnaire comprises 18 items designed to assess ADHD symptoms in alignment with DSM-IV diagnostic criteria. Items include questions such as, “How often do you misplace or have difficulty finding things at home or at work?”. Participants rated the frequency of symptom occurrence on a 5-point Likert scale, ranging from “Never” to “Very often.” The ASRS-v1.1 has shown strong internal consistency, typically ranging from .79 to .89 for the Hebrew version (Zohar & Konfortes, 2010), and from .85 to .89 in other populations (Kessler et al., 2006).
Childhood ADHD Symptoms
Childhood ADHD symptoms were assessed using the Hebrew version of the Wender Utah Rating Scale—25 item version (WURS-25; Kouros et al., 2018; Ward et al., 1993). The questionnaire assesses the presence and severity of childhood symptoms related to ADHD in adults and includes items such as: “As a child I had concentration problems and was easily distracted.” Participants provide responses on a 5-point Likert scale, ranging from “Not at all or slightly” to “Very much.” The WURS-25 has demonstrated high internal consistency, with estimates ranging from .86 to .92 (Taylor et al., 2011).
Anxiety Symptoms
Anxiety symptoms were assessed using the Hebrew version of the State-Trait Anxiety Inventory (STAI; Spielberger, 1983), comprising 40 items. In the STAI, 20 items are designed to assess trait anxiety, evaluating persistent feelings (e.g., “I feel nervous and restless”), and the other 20 items measure state anxiety, focusing on the current emotional state (e.g., “I am tense”). Participants rate all items on a 4-point Likert scale, ranging from “Almost Never” to “Almost Always.” The STAI exhibits excellent internal consistency, with alpha coefficients commonly reported between .86 and .95 in various populations (Barnes et al., 2002; Spielberger, 1983; Stojanović et al., 2020).
Exposure to the Events of October 7
At Time 2, we further evaluated the extent to which participants in the study were exposed to the October 7 attack and the subsequent war. The purpose was to gather information that would allow us to estimate the presence of Criterion A for Post-Traumatic Stress Disorder (PTSD) which involves direct or indirect (via close relationship) exposure to traumatic events. Specifically, we asked participants for details about their whereabouts during the October 7 attack (open-ended question). We further asked participants whether they or their close relatives and friends faced any physical threats during these events (yes/no question). If the answer was yes, we asked participants to elaborate in their own words to qualitatively evaluate their previous answer. We also inquired about involvement in active military duty by the participants or members of their immediate social circle. Based on this information, and in order to identify participants who may have been exposed to immediate trauma, we have created a “threat” variable. To gain a categorical coding for this variable (0/1), the authors (T.E. and G.K.) reviewed the participants’ responses and included as “1” individuals who faced physical threats in person, those whose relatives or close friends faced physical threats, and those who participated in active duty or had spouses or first-degree family members in active duty. In cases where discrepancies emerged between the two reviewers’ coding (5.2% of cases), a third independent researcher was consulted. The results are described in Table 2. In addition, within this questionnaire, we collected other variables that were not part of the “threat” variable. For example, participants were asked whether forced evacuation affected them or their close relatives. Additionally, we requested details about the extent of war news consumption, including the frequency and duration of exposure to graphically violent content spread online (see Table 2).
Analysis
Across all analyses, we used Bayesian linear regression, allowing us to describe the posterior distribution for the estimates of interest. We reported posterior distribution estimates including median, 95% credible interval, and probability of direction (noting the chance that the parameter is positive or negative in the population according to the posterior belief). We avoided hypothesis testing and complied with current guidelines asserting the need to describe in full extent the uncertainty in our regression coefficient estimates. Analysis was performed in R using “stan,” “brms,” and “cmdstan” packages (Bürkner, 2018; Gabry et al., 2023). We used weakly informative priors across all analyses. All regressions were estimated with four Markov Chain Monte Carlo (MCMC) chains, and we examined R hat estimates as well as trace plots to ensure good chain convergence. We further examined the chain effective size, and where required pair plots to ensure good coverage of the posterior space. Five participants from the ADHD group did not complete the STAI questionnaire, and the ICAR measurement at Time 1 (Table 1), and one did not complete the AUDIT and CUDIT scores (Table 1). Six participants from the ADHD group and one in the control group did not complete the exposure to the events of the October 7 questionnaire (Table 2). To handle missing values, we applied partial pooling in a hierarchical model, allowing individual estimates to be informed by both the participant’s available data and the group-level distribution. Consequently, missing observations were excluded, while available data from other time points for the same participant were retained. Data is publicly available on https://osf.io/v3anm/.
Results
We examined the effect of national catastrophic events (i.e., October 7) on inattention, hyperactivity/impulsivity, and anxiety in ADHD and control group participants. Using Bayesian analysis and data collected before and after October 7, we assessed the impact of these events on ADHD-related symptoms and anxiety symptoms.
ADHD Symptoms at Present
We hypothesized that the overall ASRS score will increase after October 7 events for both ADHD and control individuals. To examine this hypothesis, we conducted a Bayesian analysis where the association between Time (before vs. after October 7 events), Group (ADHD vs. control), and their paired interaction predicted ASRS scores (see Figure 1(A)). We found that the change in time, before, and after October 7 events, was associated with an increase of about 8 points in ASRS scores for the control group (posterior median = 8.06, 95% CI [5.72, 10.36], probability of direction (pd) ~ 100%), and a small decrease of about 2.4 points for the ADHD group (posterior median = −2.43, 95% CI [−4.66, −0.14], pd = 98.1%). This was evident in a positive ratio for the mean at Time 2 versus Time 1 for the control group (ratio posterior median = 1.47, 95% CI [1.31, 1.69], pd ~ 100%), and a negative ratio for the ADHD group (ratio posterior median = 0.94, 95% CI [0.89, 1.00], pd = 98.10%). The two-way interaction between Time and Group was substantial (posterior median of interaction = −10.49, 95% CI [−13.74, −7.22], pd ~ 100%) noting that the difference in the effect of Time was substantially smaller in the ADHD compared with the control group.
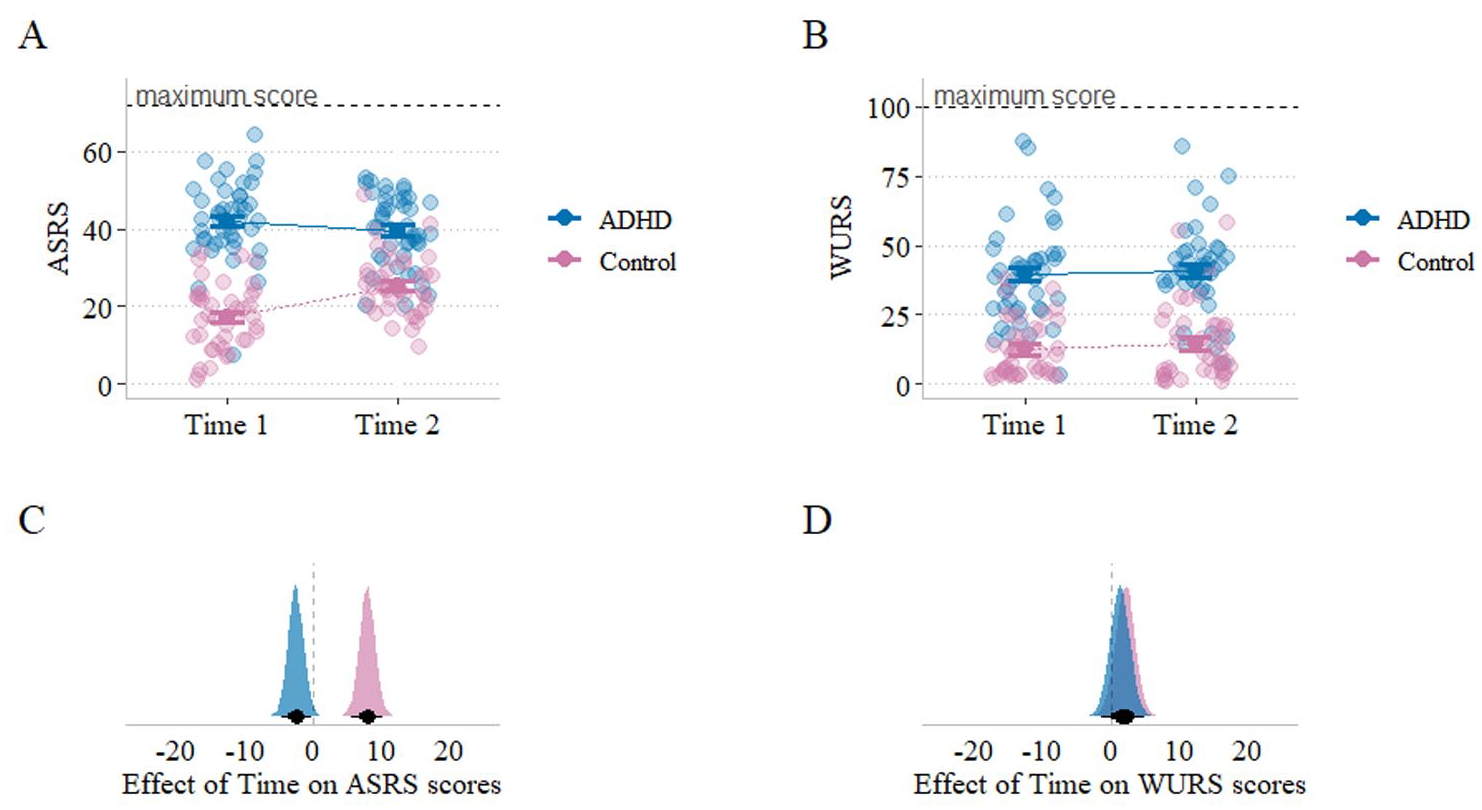
Estimation of ADHD symptoms at present and during childhood before and after national traumatic events: (A) current ADHD symptoms assessed using the ASRS in the control group (pink) and the ADHD group (blue) before and after a national traumatic event, (B) ADHD symptoms during childhood assessed using the WURS in the control group (pink) and the ADHD group (blue) before and after a national traumatic event, (C) posterior distribution showing the likelihood of each x-axis value being the population group difference in ASRS scores before and after a national traumatic event. Results indicate a significant increase of about 8 points in inattention and hyperactivity/impulsivity symptoms in participants without ADHD (control group). Conversely, participants with ADHD showed evidence against such an increase, with a slight tendency to report symptom relief, and (D) posterior distribution showing the likelihood of each x-axis value being the population mean group difference in WURS scores before and after a national traumatic event, showing no evidence in favor of substantial effect.
We repeated the same analysis, separately for inattentive and hyperactivity/impulsivity subscale and found similar results. Namely, for the control group, we found an increase in both inattentive (posterior median = 3.68, 95% CI [2.46, 4.89], pd ~ 100%] and hyperactivity/impulsivity (posterior median = 4.43, 95% CI [2.95, 5.97], pd ~ 100%]. For the ADHD group we found a small but certain decrease for inattentive scores (posterior median = −1.52, 95% CI [−2.73, −0.29], pd = 99.12] and no clear evidence for a change in hyperactivity/impulsivity (posterior median = −0.95, 95% CI [−2.38, 0.54], pd = 89.80%].
Furthermore, we suspected that the influence of October 7 events on ASRS measures might be driven by physical exposure to threat and a mental trauma reaction that can elevate ADHD-like symptoms (e.g., due to recurrent intrusive memories). We repeated the same regressions analyses while also controlling for “exposure to threat” by including it as an additional predictor. We first conducted a Bayesian analysis estimating the association between Threat (no vs. yes), Time (before and after national trauma), Group (ADHD vs. control), and their paired and triple interactions predicting ASRS scores. For both the control (posterior median = 8.22, 95% CI [5.76, 10.59], pd ~ 100%) and ADHD (posterior median = −2.05, 95% CI [−4.62, 0.44], pd ~ 100%) we found very similar effects compared to when threat was not controlled for. Therefore, we can conclude that the increase in ASRS scores for the control group, and the decrease for the ADHD were not influenced extensively by exposure to immediate threat.
These results suggest that the control group experienced a significant increase in inattention and hyperactivity/impulsivity symptoms from Time 1 to Time 2. In contrast, the ADHD group did not show a similar increase and instead displayed a slight reduction in symptom severity, particularly for inattention. Although a ceiling effect could have limited our ability to detect an increase in the ADHD group, an examination of individual variability at baseline indicates that the ADHD group had ample room for deterioration in the ASRS assessment (Figure 1(A)).
ADHD Symptoms During Childhood
We hypothesized no change in WURS scores before and after October 7 events, as the WURS is designed to assess symptoms during childhood. Therefore, this analysis serves as a control analysis ensuring that participants did not simply emphasize symptom severity indistinctly (e.g., due to overall distress following October 7 events). We sampled posterior estimates from a Bayesian regression with Time (before vs. after October 7 events), Group (ADHD vs. control), and their paired interaction, predicting WURS scores (see Figure 1(B)). For the control group we found a slight increase in WURS scores (posterior median = 2.19, 95% CI [−0.68, 4.99], pd = 93.40%). For the ADHD there is no evidence for an effect of time on WURS (posterior median = 1.43, 95% CI [−1.43, 4.34], pd = 83.76%). Figure 1 clearly shows that the major effect of time on ADHD symptoms at present were not mimicked in the WURS.
Anxiety Symptoms
We hypothesized that the overall STAI scores will increase after October 7 events for both ADHD and control individuals. A Bayesian regression analysis estimated the influence of Time (before vs. after October 7 events), Group (ADHD vs. control), and their paired interaction on STAI scores (see Figure 2). We found that a change in time, before and after October 7 events, was associated with an increase of about 27 points in STAI scores for the control group (posterior median = 27.72, 95% CI [22.01, 33.29], pd ~ 100%), and an increase of about 16 points for the ADHD group [posterior median = 16.18, 95% CI [10.44, 22.05], pd ~ 100%). This was further reflected in the estimate of the two-way interaction between Time and Group showing that the effect of time on STAI scores was higher for control compared to ADHD (posterior median of time × group = −11.51, 95% CI [−19.54, −3.30], pd = 99.60%; Figure 2(A)).
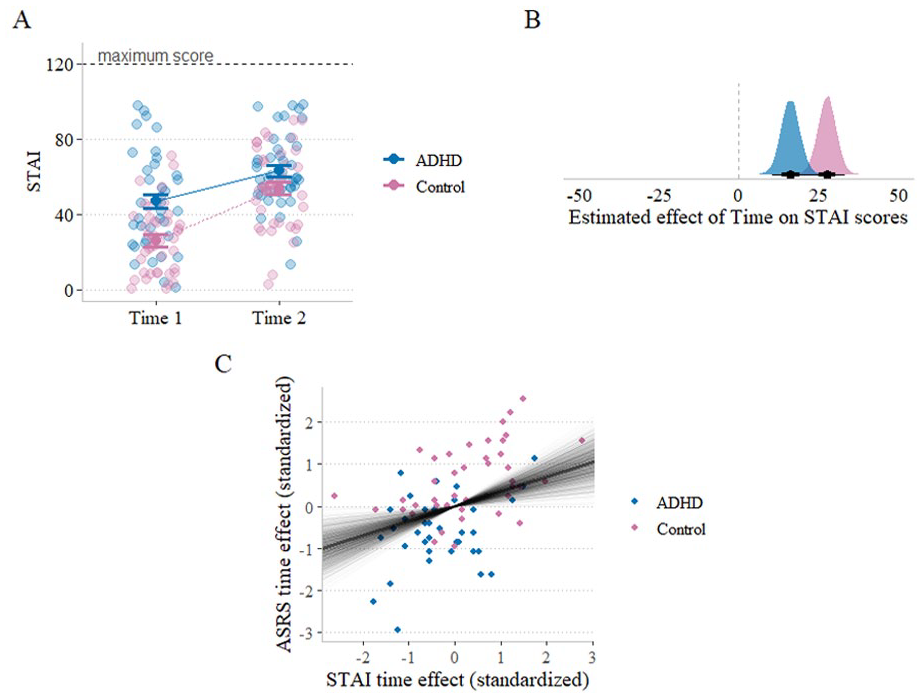
Estimation of anxiety symptoms before and after national traumatic events: (A) anxiety symptoms assessed using the STAI in the control group (pink) and the ADHD group (blue) before and after a national traumatic event, (B) posterior distribution showing the likelihood of each x-axis value being the population group difference in STAI scores before and after a national traumatic event, and (C) positive association between the change before/after October 7 on anxiety (STAI) and ADHD (ASRS) estimates, for both ADHD and control groups.
We performed a similar analysis separately for trait-anxiety and state-anxiety subscores in STAI. For the control group we found that state (posterior median = 20.69, 95% CI [16.75, 24.65], pd ~ 100%) and to a lesser extent trait anxiety (posterior median = 6.91, 95% CI [4.30, 9.37], pd = 100%), increased overtime. For the ADHD group we found an increase for state anxiety (posterior median = 14.02, 95% CI [9.86, 18.08], pd ~ 100%), and a small increase for trait anxiety (posterior median = 2.31, 95% CI [−0.25, 4.79], pd = 96.29%). Therefore, overall, we found substantial increase in anxiety symptoms for both groups.
Correlation Between Increase in Anxiety Levels and Increase in ADHD Symptoms
We aimed to examine the extent to which changes in ADHD symptoms co-occur with changes in anxiety symptoms. For this end, we calculated the difference in ADHD symptoms (ASRS) and anxiety (STAI) symptoms estimates for each participant between Time 1 and Time 2 measurements. Overall, we found a positive association between ASRS difference and STAI difference (Pearson’s correlation = .49, 95% CI [0.29, 0.69], pd ~ 100%; see Figure 2(C)). Next, we found a positive association in both groups, with evidence of no difference between the groups (posterior median of Pearson’s correlation for control = .35, 95% CI [0.13, 0.58], pd = 99.9%; posterior median of Pearson’s correlation for ADHD = .30, 95% CI [−0.03, 0.62], pd = 96.46%).
Moderation of Temporal Time Lag From Onset of National Traumatic Events
We examined whether the temporal distance from a national traumatic event was associated with changes in ADHD and Anxiety symptoms. Specifically, we examined whether greater temporal distance from the traumatic event would be associated with smaller changes in these symptoms. To test this, we calculated the number of days that had passed since October 7, designated as the national catastrophic event, and the difference between Time 1 and Time 2 in both ADHD symptoms (ASRS) and anxiety (STAI). A Bayesian correlation analysis revealed a negative correlation (Pearson’s r posterior median = −.33, 95% CI [−0.53, −0.12], pd = 99.91%), indicating that participants tested at Time 2 more days after the traumatic event showed a smaller increase in ASRS scores (see Figure 3). A similar analysis with anxiety symptoms (STAI) produced consistent results, with temporal distance from the onset of national traumatic events being associated with a smaller change in anxiety symptoms (r = −.24, 95% CI [−0.46, −0.02], pd = 98.15%; see Supplemental Material Figure S1).
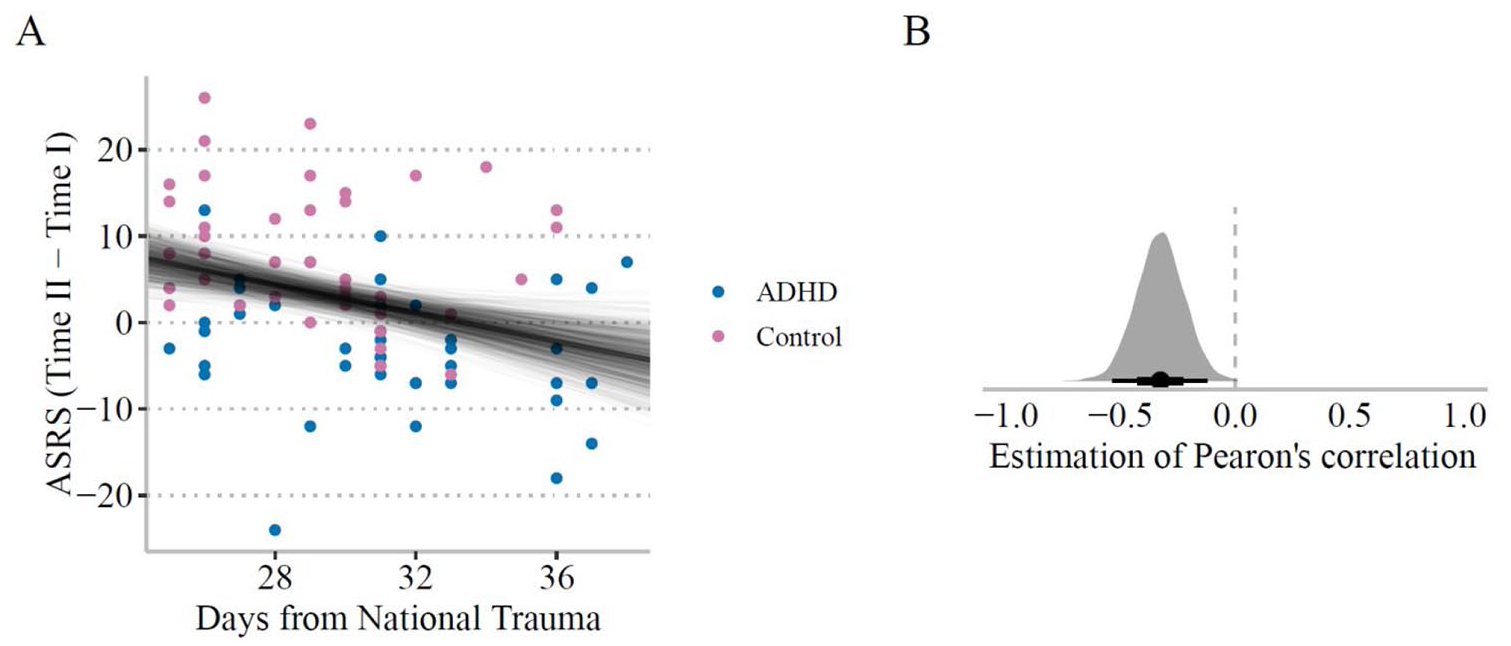
Change in ADHD symptoms as a function of the number of days since the onset of national traumatic events: (A) Scatter plot of the difference in ASRS scores as a function of days from October 7 to the second measure. Solid lines represent coefficient samples from the posterior distribution denoting the uncertainty in the association. (B) Posterior estimation of Pearson’s correlation for the temporal difference from October 7 and change in ASRS score (Time 2–Time 1). Overall, we found that the increase in ASRS score was mostly evident in temporal proximity to the national traumatic events.
Effects of Media Exposure
We examined the association change in ASRS and STAI before (Time 1) and after (Time 2) national traumatic events and media exposure. We hypothesized that those that were exposed to higher amounts of war news reports (in terms of number of reports and amount of time) would exhibit higher levels of ADHD symptoms. We found a mild positive correlation, such that the amount of war news report exposures was associated with stronger increase in ADHD symptoms (Pearson’s r posterior median = .16, 95% CI [−0.04, 0.40], pd = 94.25%). We found no evidence for a difference in this correlation between ADHD and control groups (Median posterior for the difference in Pearson’s correlation = .13, 95% CI [−0.24, 0.51], pd = 75.74%).
Discussion
In this study, we examined whether national traumatic events affected inattention and hyperactivity/impulsivity symptoms in young adults with or without an ADHD diagnosis. To do so, we analyzed data from an existing cohort that had completed our measures before the October 7 attack and compared it to a subsequent set of assessments completed by the same cohort after the attack.
As predicted, we observed a significant increase in ADHD-related symptoms among the control group following the national traumatic event. This increase was associated with a corresponding rise in anxiety symptoms and tended to diminish over time after the October 7 attack. The increase in ADHD-related symptoms for the control group persisted even when controlling for a “threat” variable, indicating that the national trauma had a broad impact on anxiety and ADHD-related symptom severity in individuals without ADHD diagnosis, even in the absence of a direct threat exposure. This finding aligns with studies that found stress induced by lockdowns during the COVID-19 pandemic increased inattention symptoms, even among individuals without an ADHD diagnosis (Breaux et al., 2021). It suggests that ADHD-related symptoms are sensitive to environmental stressors, even in populations without an ADHD diagnosis, and may fluctuate depending on external factors such as national crises or stressful events. The association we found between the increase in ADHD symptoms (ASRS) and the rise in anxiety symptoms (STAI) provides further support for the intertwined relationship between ADHD-related symptoms and stress, even among the general population.
Surprisingly, contrary to our hypothesis, which stated that the national traumatic events should lead to increased symptomatology in ADHD individuals, the ADHD group did not exhibit an increase in ADHD symptoms following October 7 events. Instead, they showed a slight reduction in symptom severity, particularly in inattention. As in the control group, this change was not influenced by exposure to immediate threat. A few possible explanations may account for the slight relief in symptoms observed within the ADHD group. First, in the month following the October 7 attack, expectations for performance and professional functioning were generally lower, as universities and workplaces were closed. This reduction in expectations may have made symptoms, especially those related to inattention, less pronounced (Melegari et al., 2021). Second, according to the state-regulation model (Sergeant, 2000; Van der Meere & Sergeant, 1988), individuals with ADHD exhibit altered arousal regulation tendencies that hinder their ability to adjust to varying levels of environmental engagement. If the national events functioned as only a moderate stressor (e.g., due to the lack of direct involvement in the events), this may have facilitated a shift toward a more optimal arousal level in individuals with ADHD. This speculation resonates to some extent with controlled lab experiments, which indicate that a slow event rate (believed to induce lower arousal levels) is associated with poorer performance in individuals with ADHD, whereas faster event rates are thought to elevate arousal, leading to enhanced attention and improved task performance (Isaac et al., 2024).
Several limitations should be noted. First, consistent with previous research (Faraone et al., 2021), the ADHD and control groups differed on various non-ADHD psychiatric scales (Table 1), potentially introducing confounds. However, the differences in ADHD-specific measures (ASRS/WURS, see Table 1) were much larger. Moreover, while higher psychopathology in the ADHD group would typically predict greater vulnerability following traumatic events, we observed the opposite: despite higher baseline psychopathology, the ADHD group showed a reduction in ADHD symptoms after October 7, whereas the control group, with lower baseline psychopathology, exhibited an increase. These findings suggest that baseline differences in general psychopathology are unlikely to account for our results.
Second, at Time 2, while the crisis was ongoing, we focused on ADHD symptoms, anxiety, and exposure to the October 7 events to avoid overburdening participants. While this approach ensured feasibility during the stressful period, the omission of additional variables (e.g., depression, substance use) limits our ability to fully understand the broader psychological impact of national trauma. It also constrains our capacity to identify potential mediators of the symptoms patterns observed in this study. Future research should incorporate broader measures and proactively plan for data collection following national disasters.
Third, self-report measures may be influenced by the assumption that individuals with ADHD are less reliable in recollecting events (e.g., reporting media exposure). This potential bias could have influenced the mild positive correlation observed between war-related news consumption and the increase in ADHD-like symptoms. As such, future studies should consider incorporating momentary or real-time assessments to reduce recall bias and better isolate the effects of national traumatic events when comparing data collected before and after such events.
Finally, our findings may not generalize broadly. We studied high-functioning students without coexisting psychiatric diagnoses (e.g., depression, anxiety) which is less typical of the broader ADHD population (Faraone et al., 2021). Moreover, men were underrepresented (3/42 in controls, 13/43 in ADHD), making our results more applicable to women. This is important given known sex differences in stress responses, especially the higher prevalence of internalizing disorders (Kessler, 2003) and anxiety (McLean & Anderson, 2009) among women.
Our study adds to the growing body of evidence supporting the assumption that national traumatic events, particularly terror attacks, have a widespread impact on the general population, including individuals not directly involved (Hansen et al., 2016, 2017; Rigutto et al., 2021). To the best of our knowledge, this is the first study to specifically investigate the effect of such events on ADHD-related symptoms in both individuals with and without a diagnosis of ADHD. Future research should further explore the functional capabilities of individuals with ADHD under acute stress to deepen the understanding of this relationship.
Supplemental Material
sj-docx-1-jad-10.1177_10870547251351442 – Supplemental material for Influence of National Traumatic Events on Inattention and Hyperactivity/Impulsivity Symptoms in Young Adults With and Without ADHD
Supplemental material, sj-docx-1-jad-10.1177_10870547251351442 for Influence of National Traumatic Events on Inattention and Hyperactivity/Impulsivity Symptoms in Young Adults With and Without ADHD by Tal Erdinast, Gili Katabi, Abraham Weizman, Iris Manor and Nitzan Shahar in Journal of Attention Disorders
Footnotes
Acknowledgements
We would like to extend our deepest gratitude to Shira Amir, Ofir Cohen, and Yuval Levy for their dedicated assistance with data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.