
Abstract
The incidence of Lyme disease (LD) has grown over time despite extensive awareness campaigns of disease risk. While previous research has explored public knowledge, perceptions, and attitudes toward tick-borne diseases, there is minimal research in understanding preventive behavior among individuals frequently engaging in outdoor recreation. This study addresses this gap by investigating the perceptions of LD preventive behavior, focusing on psychosocial factors influencing behavior. Utilizing an integrative framework incorporating the Health Belief Model and Social Cognitive Theory, we examined outdoor recreationist performance of three key preventive behaviors: tick checks, tick repellent use, and protective clothing. Data were collected through intercept surveys at Bradbury Mountain State Park (Maine, US). Findings indicate that tick-related knowledge and experience have a limited impact on preventive behavior, while efficacy beliefs and perceived benefits significantly influence behavior. In this paper we discuss the implications of these factors to both theory and practice in LD prevention studies.
Keywords
Introduction
Lyme disease (LD) is the most common tick-borne disease in the United States (CDC, 2022). LD is an infection caused by the spirochete bacterium Borrelia burgdorferi that is transmitted by the blacklegged tick, Ixodes scapularis (Acari: Ixodidae). Despite substantial underreporting, the US Centers for Disease Control and Prevention (CDC) estimates that between 300,000 and 476,000 people are impacted by LD every year causing a significant public health issue across the northeastern, upper midwestern and mid-Atlantic US (Kugeler et al., 2021; Schwartz et al., 2020). Research in tick ecology has shown that the life cycle of the blacklegged tick is tightly coupled with forest ecosystems, meaning that LD prevalence and pathogen transmission are common in deciduous forest landscapes (Conte et al., 2021; Ostfeld et al., 2018). Individuals spending time in forested areas, such as outdoor recreationists, have increased risk of exposure to the pathogen that causes LD (Brady et al., 2022; Donohoe et al., 2015; Richard & Oppliger, 2015).
To address the implications of LD and other tick-borne diseases (TBD) on human populations, public health providers and government agencies encourage the adoption of personal preventive behaviors (Aenishaenslin et al., 2017; Beck et al., 2022; Nawrocki & Hinckley, 2021). Such behaviors are traditionally promoted through educational programs and public awareness campaigns targeting individuals engaged in activities that are known to present unique disease risk, such as outdoor recreation (Porter et al., 2019). Given the lack of market-available options for human vaccination or prophylactic treatment, proactive prevention of tick bite exposure is crucial to community health (Aenishaenslin et al., 2017). Three major methods for tick bite prevention dominate the public health messaging surrounding LD: (a) tick checks, (b) use of tick repellent, and (c) use of protective clothing (Beaujean, Bults, et al., 2013; Cisak et al., 2012; Van Der Heijden et al., 2017). However, the adoption of tick bite preventive behaviors is low among residents in high LD incidence areas (Niesobecki et al., 2019; Valois et al., 2020). For example, Aenishaenslin et al. (2022) conducted an exploratory study on the adoption rate of several LD preventive behaviors among residents in Quebec, Canada. The authors found that respondents’ adoption rate for tick checks and use of tick repellent was 27% and 30%, respectively. These findings on the adoption rate of preventive behaviors in high LD incidence areas stress the importance of understanding why residents do not fully engage with preventive behavior by exploring the influences of psychosocial factors such as knowledge, experience, risk perception, and efficacy beliefs on individual behavior (Beaujean, Gassner, et al., 2013; Brady et al., 2022; Nawrocki & Hinckley, 2021). Responses to these questions are crucial for informing public health policies and campaigns and, ultimately, reduce human exposure to LD.
The adoption of LD preventive behaviors has been widely studied using different theoretical models such as the Health Belief Model (HBM), Theory of Risk Perception (TRP), Social Cognitive Theory (SCT) and Knowledge, Attitudes and Prevention Behaviors Model (KAP or KAB; Finch et al., 2014; Nawrocki & Hinckley, 2021). Studies have focused on analyzing the role of knowledge, attitudes, and experience in adopting tick bite preventive behaviors in LD endemic regions (Beck et al., 2022; Gupta et al., 2018; Herrington, 2004; Herrington et al., 1997), understanding changes in public awareness toward ticks and LD (Aenishaenslin et al., 2016), identifying knowledge needs about LD and preventive practices (St. Pierre et al., 2020), understanding the sociocultural and behavioral factors that increase human exposure to LD (Aenishaenslin et al., 2022; Marcu et al., 2011), and providing policy recommendations based on LD risk perception (Bouchard et al., 2018; Jacob et al., 2019).
Previous studies addressing the social and psychological dimension of LD prevention have largely focused their research on communities in disease affected areas. Several studies have evaluated the increased risk of exposure among foresters in Europe and found that those working in forest landscapes have a heightened risk of tick-borne disease exposure (Kurnatowski et al., 2011; Richard & Oppliger, 2015; Tokarska-Rodak et al., 2014). Research conducted in the US has pointed to the increased hazards outdoor recreationists face in regard to LD exposure (Donohoe et al., 2015, 2018; Piacentino & Schwartz, 2002). Nevertheless, research in the determinants of LD preventive behavior in outdoor recreationists is limited (Brady et al., 2022). In this paper we (1) propose a combined conceptual model to study LD preventive behavior and (2) explore the psychosocial determinants that predict preventive behaviors among outdoor recreationists in a LD endemic area.
Understanding the Psychosocial Constructs Behind LD Preventive Behavior
Government agencies, public health providers and epidemiologists recommend the adoption of tick bite preventive behavior that relies on an individual’s willingness to perform tick checks, use of insect repellent and/or insecticides, and wear protective clothing, among other preventive practices (Eisen & Stafford, 2021; Nawrocki & Hinckley, 2021). However, research has found that educational campaigns targeting behavior change fall short to address the multiple underlying factors that drive LD preventive behavior such as knowledge, experience, risk perceptions, and attitudes toward LD and ticks. Knowledge of LD and TBDs is often targeted by institutional campaigns as a means to improve individual preventive behavior. Gupta et al. (2018) found that, despite robust institutional campaigns, knowledge of TBD is poor among residents in Delaware, a state with one of the highest rates of LD, and few people perform tick bite preventive practices. Research has found that although knowledge is positively correlated with preventive behavior, targeting knowledge improvement alone is insufficient to impact behavior change (Puppo & Préau, 2018). Puppo and Préau (2018) found similar results to Gupta et al. among Long Island residents and emphasized the importance of exploring how other approaches differ from the “information deficit model” impact LD preventive practices.
Experience of LD, TBDs and preventive methods is considered a significant factor in influencing LD preventive behavior (Beaujean, Bults, et al., 2013). More than two decades ago, Herrington et al. (1997) found that previous experience with LD and tick bites was correlated to tick bite preventive behavior among residents from Montana, Maine, and Connecticut. Recently, Nawrocki and Hinckley (2021) used a nationally representative survey on health-related topics to understand individual experiences with TBD, tick bites and personal prevention methods in the US. Researchers found that survey respondents were most likely to perform LD preventive behaviors (e.g., perform tick checks, use insect repellent, and taking a shower after going to the outdoors) if they lived in a high LD incidence state (or in a neighboring state) and if they lived in a non-urban setting. However, researchers also found that approximately half of the survey respondents from high LD incidence states (~46.6%) and neighboring states (~53.9%) did not perform any type of LD preventive behaviors (Nawrocki & Hinckley, 2021).
Perceptions of disease severity and individual susceptibility have been explored to understand their role in encouraging or discouraging preventive behavior (Brady et al., 2022). Slunge and Boman (2018) studied risk perceptions and individual exposure to tick bites and TBDs using a nationally representative survey in Sweden with participants from high and low TBD incidence regions. The authors found that personal experience with tick bites was high for the last year (31%) and lifetime (68%) among residents in high TBD incidence areas and that knowledge, experience, risk perception and demographics were positively associated with some preventive practices, such as tick checks, wear protective clothing and use of insect repellent.
Efficacy beliefs have also been explored to understand how residents in high LD incidence areas are influenced by the perceived efficacy of preventive methods (Richardson et al., 2019). Efficacy beliefs influence how individuals assess potential threats to cognitively evaluate their own capability to control or respond to these threats. Efficacy beliefs may refer to the individual perception of the efficacy of a particular preventive method (i.e., method efficacy) or to the perceived ability to perform that method (i.e., self-efficacy). Beaujean, Bults, et al. (2013) investigated the social determinants of LD preventive behavior among 550 individuals in the Netherlands and found that knowledge, level of concern and perceived efficacy determined human preventive behavior. Tick checks was the most common and preferred method for mitigating the impact of contracting LD, while wearing protective clothing and using insect repellent showed lower levels of self-efficacy among research participants. Some studies in tick-borne disease prevention have used the KAP model to understand to what extent different populations adopt (or are willing to adopt) tick bite prevention methods in endemic areas (Beck et al., 2022; Lyons et al., 2022; Nawrocki & Hinckley, 2021). For example, Lyons et al. (2022) designed a training workshop to improve local health department employees’ knowledge, attitudes, and adoption of preventive behaviors by using the KAP approach. Researchers found that providing practical experience with tick identification and surveillance practices were key to create an impact on participants’ knowledge and attitudes toward LD prevention.
While these studies provide a foundational understanding of preventive behavior engagement, studies often lack a theoretical basis necessary to identify specific social and psychological factors influencing individuals’ preventive behaviors (Jacob et al., 2019). Our paper aims to address this gap by evaluating the predictive power of prominent health behavior determinants in a LD preventive behavior context. More specifically, this research examines the factors underlying three common personal preventive behaviors: tick checks, use of repellent/acaricide, and dress in protective apparel. To understand what psychosocial constructs determine LD preventive behavior among human populations in a LD endemic region, we developed a theoretical framework built on two prominent health behavior models: the Health Belief Model and Social Cognitive Theory.
An Integrative Framework to Study LD Preventive Behavior
Two of the most used theoretical frameworks in social psychology to study human health behavior are the Health Belief Model (HBM; Rosenstock, 1966, 1974) and Social Cognitive Theory (SCT) (Bandura, 1998, 2005). HBM was developed in the 1950s to explain people’s adoption of, and engagement with, disease prevention practices (Linke et al., 2014). HBM is also applied to predict action related to health screenings and symptom management (Heaney & Viswanath, 2008). HBM takes a value-expectancy approach to understand individual behavior, emphasizing the role of subjective cognition in decision-making (Champion & Skinner, 2008). In other words, the HBM describes action and inaction through an individual’s health issue or disease, and the perceived likelihood of being able to mitigate or avoid said affliction through personal action (Rosenstock, 1966, 1974).
The HBM draws on six behavioral determinants that are thought to predict behavior: perceived susceptibility, perceived severity, perceived benefits, perceived barriers, method efficacy, and cues to action (Figure 1; Carpenter, 2010; Champion & Skinner, 2008; Linke et al., 2014). Perceived susceptibility refers to an individual’s beliefs about their personal level of risk for contracting a condition or illness. Perceived severity indicates an individual’s beliefs about the implications of contracting a condition or illness. The combination of perceived susceptibility and perceived severity are called perceived threat. Perceived benefits refer to an individual’s opinion of the positive outcomes associated with a particular health action. Perceived barriers refer to an individual’s beliefs about the costs or limitations of performing a particular health action. Method efficacy indicates an individual’s assessment of the effectiveness of a particular behavior to promote positive health outcomes. Finally, cues to action refers to specific triggers that elicit engagement in a particular health action.
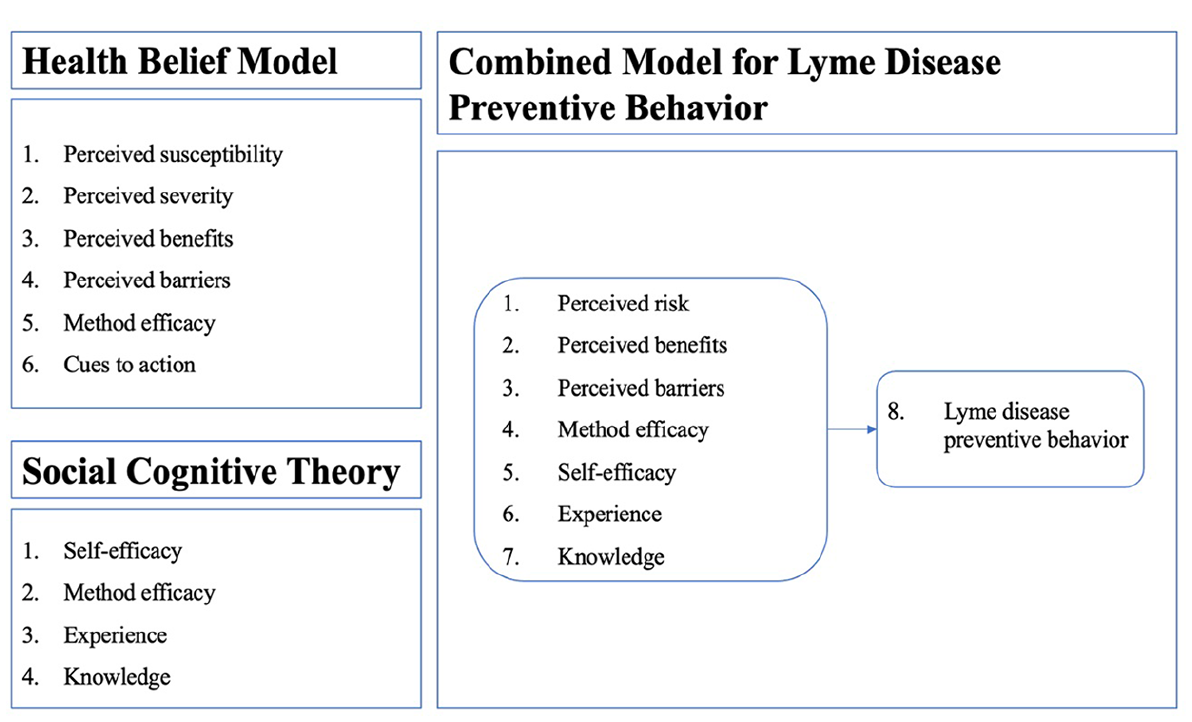
Psychosocial determinants or constructs in behavioral frameworks.
SCT has been used in health behavior research to study people’s knowledge of disease risk and transmission, previous experience with health issues or illnesses, and motivations to perform preventive practices (Heaney & Viswanath, 2008). SCT describes health-related behavior as a function of socio-cognitive determinants (Bandura, 1998), and is designed on the premise that learning and action reinforcement is influenced by dynamic and reciprocal relationships between an individual, their environment, and own behavior (Bandura, 1998, 2005). SCT applied to health behavior is built on four main behavioral determinants that drive human action: self-efficacy, method efficacy, experience, and knowledge (Figure 1; Heaney & Viswanath, 2008). Self-efficacy refers to an individual’s belief in their ability to engage in a particular health action. This variable is key to understand a person’s engagement with positive health behaviors that require repeated action (e.g., such as doing tick checks after going outdoors in LD endemic regions). Method efficacy, also known as response efficacy, refers to an individual’s opinion of the effectiveness of a particular behavior to promote positive health outcomes or reduce the likelihood of acquiring a disease. Experience refers to an individual’s previous exposure to a particular condition or illness. This variable considers both the personal experience of an individual as well as the witnesses experiences of those around them. The last variable, knowledge, refers to an individual’s awareness and understanding of a particular condition or illness. Knowledge also includes the understanding of medical treatments to manage symptoms and risk prevention practices (Bandura, 1998, 2005; Van Der Heijden et al., 2017).
HBM and SCT frameworks have shown promising results in understanding the social determinants of several illnesses and health conditions (Harrison et al., 1992; Linke et al., 2014; Mowbray et al., 2012; Schunk & DiBenedetto, 2020). Extensive literature has established the predictive value of each of the above behavioral determinants (Carpenter, 2010; Donohoe et al., 2018; Harrison et al., 1992; Overstreet et al., 2013). However, the strength of these predictors is inconsistent across health behavior scenarios, demonstrating the importance of multiple applications of theoretical models to diverse research topics and local contexts (Carpenter, 2010; Overstreet et al., 2013). To our knowledge, few studies have applied both theories to LD preventive behavior (Jacob et al., 2019). This paper aims to contribute to the understanding of psychosocial determinants of LD preventive behavior by combining the HBM and SCT framework in the context of a high LD risk exposure activity (i.e., outdoor recreation) in the northeastern US, one of the most impacted areas in North America.
Methods
Study Site
The state of Maine, located in the northeastern US, is well-known for its forest landscape which covers about 90% of the state (Goff et al., 2021). Maine’s forested landscape situates the state as one of the top nature-based tourism destination in the US (Munding & Daigle, 2007; Vail et al., 2019; Wilkins & de Urioste-Stone, 2018) where visitors engage in several outdoor recreation activities such as hiking, kayaking, wildlife watching, recreational hunting, and fishing (Wilkins & de Urioste-Stone, 2018). We investigated the psychosocial determinants of LD preventive behavior among outdoor recreationists at Bradbury Mountain State Park in Pownal, Maine, US. The state park is located in Maine’s most populous county, Cumberland County, of about 305,231 inhabitants (US Census Bureau, 2021). Bradbury Mountain State Park is a popular recreation destination for both in-state and out-of-state visitors. The 730-acre publicly owned recreation area features multi-use trails that are used for a variety of activities including, but not limited to, hiking, mountain biking, snowmobiling, and horseback riding. We surveyed outdoor recreationists using the state park’s trail system.
Research Design
Our study followed a correlational design (Lindley, 1990; Vaske, 2008) to determine what psychosocial factors drive human preventive behavior toward LD among outdoor recreationists (Brady et al., 2022; Donohoe et al., 2015, 2018). We used a combined HBM and SCT framework applied to LD preventive behavior to determine the extent of the relationship between psychosocial variables using statistical data (Bandura, 1998, 2005; Rosenstock, 1966, 1974). To adapt the HBM and SCT frameworks, we made the following decisions: First, HBM’s “cues to action” variable was not included. Literature that supports the predictive capability of “cues to action” is limited (Carpenter, 2010) and several authors warn about the practical challenges to measure this variable (Abraham & Sheeran, 2005, p. 28). Second, HBM’s perceived severity and perceived susceptibility were evaluated together in our analysis as a measure of perceived risk following previous studies in human preventive behavior (Guan & So, 2020; Rains et al., 2019). For this study, perceived risk was defined as a measure of “people’s subjective judgments about the likelihood of negative occurrences such as injury, illness, disease, and death” (Paek & Hove, 2017, p. 1). Our combined conceptual model for LD preventive behavior included eight constructs, as shown in Figure 1.
Data Collection Instruments and Variables
To explore LD preventive behavior among outdoor recreationists, we designed a questionnaire following existing publications in HBM (Bosch et al., 2010; Donohoe et al., 2018), SCT (Van Der Heijden et al., 2017), and LD prevention (Valois et al., 2020). The questionnaire operationalized the eight constructs in our combined HBM-SCT conceptual model. The questionnaire combined Likert-type, dichotomous forced-choice, and demographic questions to collect data about participants’ perceptions of, experience with, and knowledge of ticks, LD, and tick bite prevention practices. The Likert-type questions assessed participants’ attitudes toward ticks and LD, and reasons for engagement in tick bite prevention practices. The dichotomous forced-choice questions assessed participants’ knowledge of and experience with ticks, LD, and tick bite prevention practices. The demographic questions asked for participants’ age, gender, place of residency, highest level of education, household income before taxes, frequency of visiting nature and time spent in the outdoors.
The first three combined conceptual model constructs were assessed through several items on a 5-point Likert-type scale from strongly disagree (−2) to strongly agree (+2) (Table 1). The first construct, perceived risk, was measured through seven items that contained three items to measure perceived susceptibility (e.g., “There is a high risk that I will be bitten by a tick if I visit nature”) and four items to measure perceived severity (e.g., “If I were to contract LD, it would have a significant impact on my life”). Statements representing perceived susceptibility and perceived severity were assessed together representing a measure of individual’s overall perceived risk. The second construct, perceived benefits of performing tick bite prevention practices was measured using two items that included statements about general preventive behavior benefits (e.g., “Adopting tick bite prevention practices is important for my health”). Considering that this research is focused on three main LD preventive practices (tick checks, use of insect repellent, and wear protective clothing), the items were designed to be representative of individual perceived benefits of tick bite prevention in general. The third construct, perceived barriers to performing preventive behavior, was measured using two types of items. The first type included two general statements that were deemed representative of individual perceived barriers to general tick bite prevention (e.g., “Adopting tick bite prevention practices is difficult”). The second type included several statements measuring barriers specific to each of the three preventive behaviors of interest (e.g., “I dislike having to fully undress to effectively perform a tick check”).
Behavioral Determinants of the Combined Model for Lyme Disease Preventive Behavior.
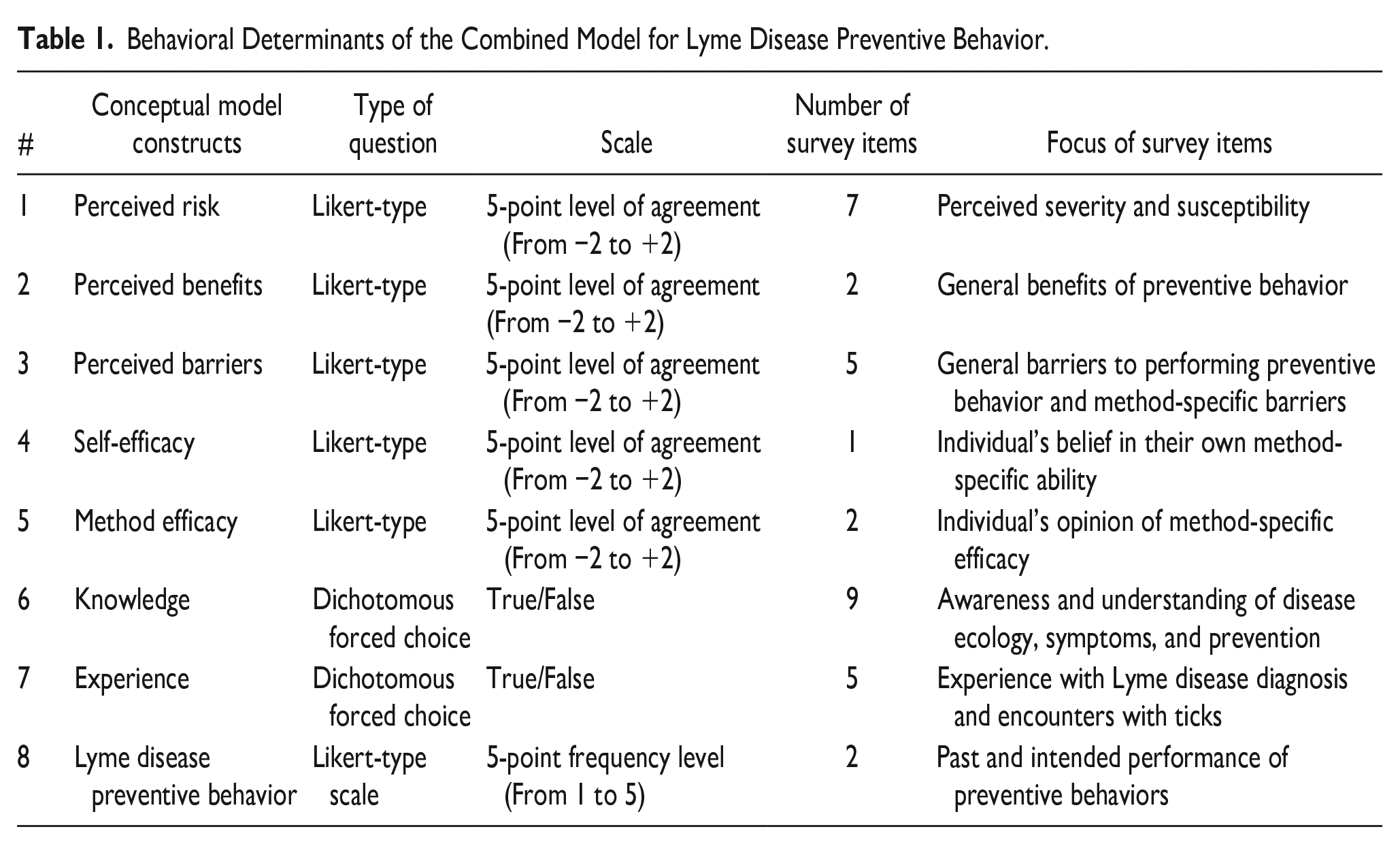
The fourth and fifth combined conceptual model constructs, efficacy beliefs, were measured through three items on a 5-point Likert-type scale from strongly disagree (-2) to strongly agree (+2). One of these three items measured self-efficacy while the remaining two targeted method efficacy. The three items were used to collect information about participants’ opinions on performing tick checks, use of insect repellent, and wear of protective clothing (e.g., “I am less likely to get LD if I wear protective clothing”). The questionnaire included statements that were behavior-specific meaning that the language used in these items was designed specifically for the preventive behavior of study.
The sixth and seventh combined conceptual model constructs, knowledge, and experience, were measured through dichotomous forced-choice questions. Cumulative scores were calculated within these two constructs as an additive scale. Participants were asked to indicate whether each statement was “true” or “not true” based on their current knowledge and experience of ticks, LD, and preventive behavior. Participants were also given the opportunity to indicate their lack of knowledge or uncertainty on the subject using the response category “don’t know”. To measure participants’ knowledge of ticks and LD, a set of nine items was used in an additive scale. Each correctly answered item was assigned a point, while incorrect or “don’t know” responses received zero points. The knowledge scores of individual respondents were determined by summing their correct answers. To measure participant’s experience with ticks and LD, a set of five items was used in an additive scale. Each affirmative answer (answering “true” to a question) was given one point in a summated score; “false” or “don’t know” responses received zero points. The experience scores of individual respondents were determined by summing their affirmative answers.
While the previous seven constructs in our conceptual model were considered independent variables, the eighth and last construct, LD preventive behavior, was assumed the dependent variable. LD preventive behavior was measured with two items on a 5-point Likert-type scale from “never” (1) to “always” (5). One item measured participant’s past performance of preventive behavior during the previous summer (summer of 2018) while the other measured participants’ intended performance of preventive behaviors during the current summer (summer of 2019).
Data Collection
Questionnaires were administered to participants via an in-person intercept surveying technique (Hallman et al., 1995). Potential participants were identified as outdoor recreationists utilizing Bradbury Mountain State Park’s trail system during summer of 2019. Research personnel approached potential participants and greeted adult-aged individuals at the beginning of the park’s Northern Loop Trail. We chose Northern Loop Trail as survey administration site because it is the main entrance to Bradbury Mountain State Park, and it receives nearly all visitor traffic. Individuals who were distracted with activities (e.g., on the phone, wearing headphones) or in large groups that would clearly be interrupted by a request to participate in research were not approached. Research staff greeted participants using an oral script describing the purposes of the research. Individuals who expressed interest in participating in the study then received a copy of a consent form outlining the details and requirements for participation. Eligibility for informed consent required that all participants were 18 years of age or older at the time of questionnaire completion. Once participants had read the form and communicated their consent, they were given a questionnaire to complete. Participants took 10 to 15 min to complete questionnaires on-site, and once finished, returned their completed questionnaires to the staff. The instrument format allowed for up to 10 questionnaires to be administered at a time, meaning that multiple individuals were able to complete their respective surveys simultaneously.
To determine an appropriate sample size for the linear regression analysis, we conducted a power analysis using GPower 3.1.9.6. The analysis considered an effect size of 0.15, a significance level of 0.05 and a desired power of 0.915. Based on these parameters, GPower recommended a sample size of 397 participants. We employed a random sampling approach in consideration of the park’s varying visitor counts during weekdays and weekends throughout the summer season. Based on an assessment of Bradbury Park’s annual visitor reported data, our primary aim was to attain the study sample over five days within each week of data collection. To ensure an equitable distribution across the days of the week, we employed random rotation of sample days and times. This approach facilitated a balanced representation of both weekends and weekdays, preventing any bias toward particular days. The sampling period spanned from July 11, 2019, to August 17, 2019, encompassing a total of 25 days. Research received IRB approval #2019-06-07.
Data Analysis
Research personnel approached 580 Bradbury Mountain State Park visitors in the sampling period. Of the 580 potential research participants, 401 people completed the questionnaire for a response rate of 69%. Following data collection, questionnaire responses were revised for completeness and legibility before analysis. Questionnaires missing 50% or more item responses within a specific construct were deemed ineligible and were removed from data analysis. We did not conduct a follow-up survey to address non-responses. In total 393 out of 401 questionnaire responses were included in data analysis for this paper. Data were entered into an electronic database on Microsoft Excel and then analyzed using IBM’s Statistical Package for Social Science 26.1 (SPSS).
To analyze the data, we first used frequency distributions to summarize the characteristics of the respondents and their responses to individual questionnaire items. This descriptive analysis established a preliminary understanding of recreationists’ attitudes and beliefs concerning ticks and LD. Second, we categorized research participants from Maine and those residing in other states to determine statistically significant differences between both groups of respondents. We used a paired sample t-test (Student’s t-test) and Chi-squared tests to compare sample means of age, gender and education level of participants (Campbell & Stanley, 1963; Sprinthall, 2011; Vaske, 2008). Calculating the difference in means between both types of respondents allowed us to determine if data could be treated as one single sample of outdoor recreationists.
Third, knowledge and experience questionnaire items were recorded into new variables that represented participants’ summed score for each latent construct. For instance, all nine questionnaire items measuring participants’ knowledge about ticks, LD and preventive behavior were combined into a new index that captured participants’ total knowledge accuracy score as described in the previous section. Similarly, all five experience questionnaire items measuring participants’ experience of ticks, LD and preventive behavior were combined into a new summated index that captured participants’ total experience score. These new two variables ranged from zero (0) to nine (9) and zero (0) to five (5) for knowledge and experience, respectively.
Fourth, Principal Component Analyses (PCA) with varimax rotation (Acal et al., 2020; Joliffe & Morgan, 1992) were performed on individual items representing perceived risk (seven items) and perceived barriers (five items). PCA were used to verify that the observed variables were separated into individual components that represent their respective latent constructs. Individual items with component loadings <0.4 were dropped from the subsequent analysis. Pearson’s correlation coefficient (Vaske, 2008) was calculated for two-item scales representing perceived benefits and method efficacy. Pearson’s correlation coefficient was employed to assess the linear relationship between the two items within a scale, examining the extent to which they varied together in measuring participants’ perceptions of LD prevention benefits and method efficacy. Based on the PCA results and Pearson’s r, single components were identified for all latent constructs and mean item scores were calculated by averaging the score of all items within the component. We used Cronbach’s alpha to measure the reliability of these latent construct composite scores. An alpha value >.60 was considered adequate for social science and human dimensions research (Jugessur, 2022; Vaske, 2008). Missing data points within a scale were substituted using a sample means solution (Raaijmakers, 1999). Assuming that missing data were random, the mean of the available data served as an appropriate estimate of the mean for the total sample, therefore, the mean of available item data was used as a substitute for missing values within the same scale.
Finally, we computed bivariate correlations to explore whether the seven constructs in our combined conceptual model were associated with LD preventive behavior (Figure 1). Results of bivariate correlations are not reported in this paper, but they can be accessed upon request to the corresponding author. Following confirmation of this association, multivariate relationships were assessed by means of regression analyses (Lindley, 1990; Vaske, 2008). Linear regression analyses were performed to assess the applicability of the proposed behavior models in a LD prevention context. More specifically, these analyses evaluated the predictive capabilities of seven constructs (self-efficacy, method efficacy, perceived risk, perceived benefits, perceived barriers, knowledge, and experience) in predicting each of the three LD preventive behaviors of interest. For these analyses, all determinants were treated as independent factors at the significance level of 0.05 (Lindley, 1990; Sprinthall, 2011; Vaske, 2008).
Results
Participant Demographics
Demographic data show that Maine residents accounted for 63.6% (n = 250) of the outdoor recreationist sample, while 35.8% (n = 141) of participants indicated that they were visiting the park from out of state (Table 2). At least 121 individuals (85.8%) of the 141 participants visiting the park from out of state indicated they were visiting from an area where LD is also endemic. The Student’s t-test showed no statistically significant differences in the age, gender, or education level between Maine residents and out-of-state visitors. Therefore, all 393 participants were examined as one sample of outdoor recreationists.
Demographic Characteristics of the Outdoor Recreationist Sample.
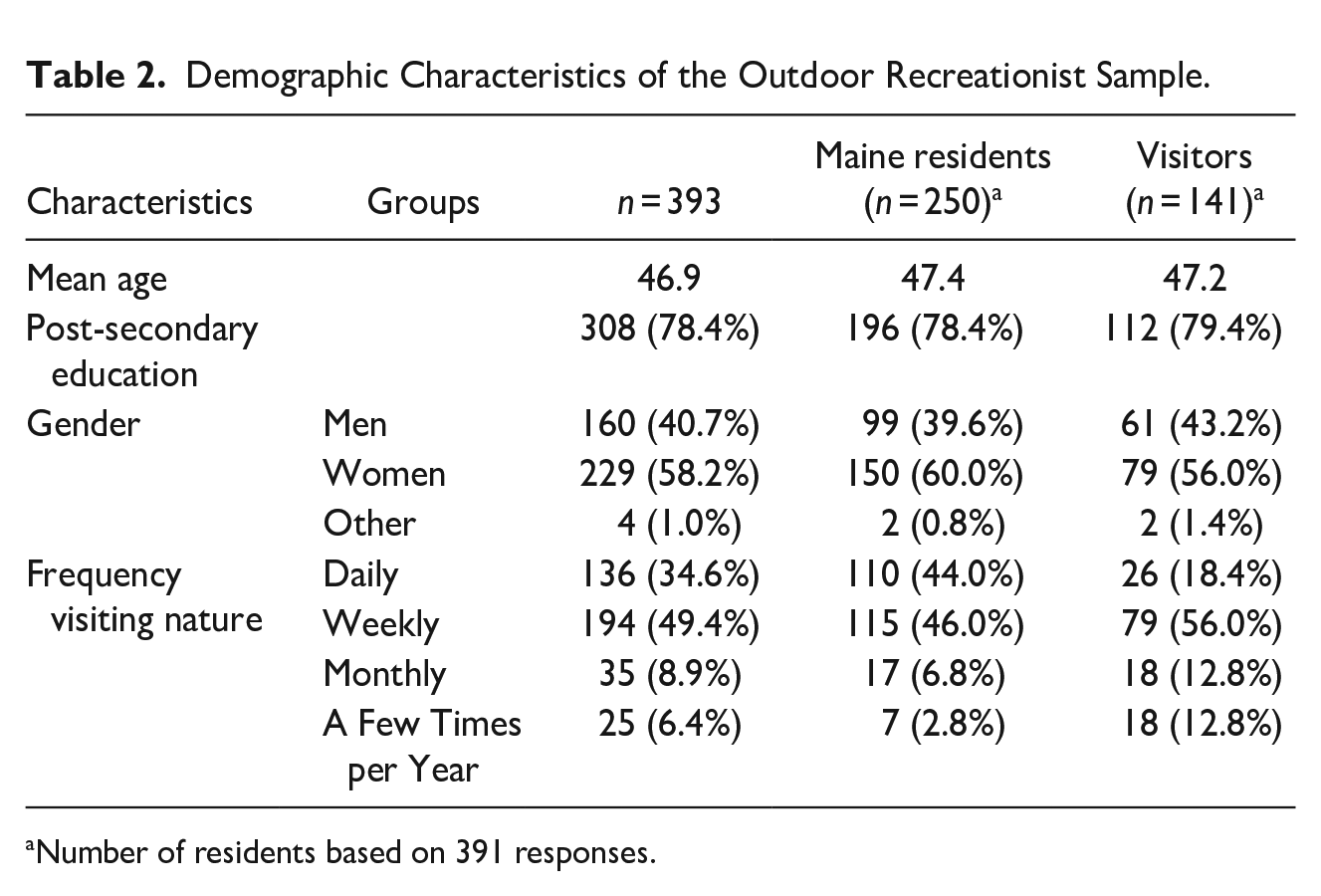
Number of residents based on 391 responses.
Demographic data also showed that 58% (n = 229) of the research participants identified themselves as female. The outdoor recreationist sample had an average age of 46.9 years (SD = 14.6), ranging from 18 years to 81 years. Most participants (82.2%) have received a post-secondary education, having pursued an undergraduate degree, graduate degree, or intermediate vocational training through terminal trade of technical school programs. For 3.3% of participants the highest level of education achieved was high school.
Knowledge and Experience of Ticks and LD
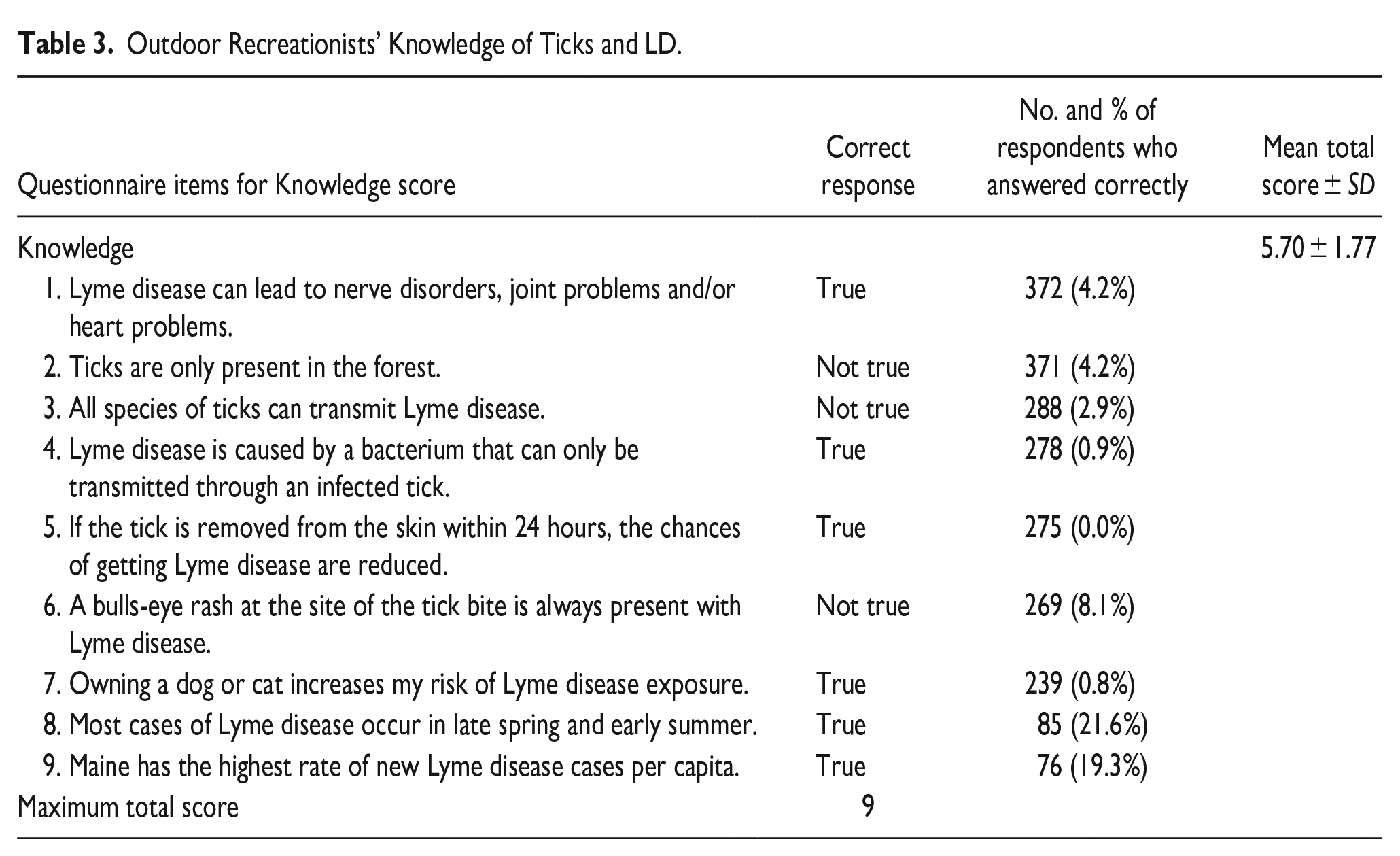
Overall, research participants’ mean knowledge score was high (5.70 ± 1.77) which indicates that on average participants correctly responded to more than half of the knowledge items presented in the questionnaire (Table 3). The most known facts were those relating to the health risks associated with the disease (94.2%) and the types of habitats that ticks inhabit (94.2%). The largest deficits in knowledge were observed in responses to items concerning the time of year most associated with LD transmission (21.6%) as well as the per capita impact of LD in the state of Maine (19.3%).
Outdoor Recreationists’ Knowledge of Ticks and LD.
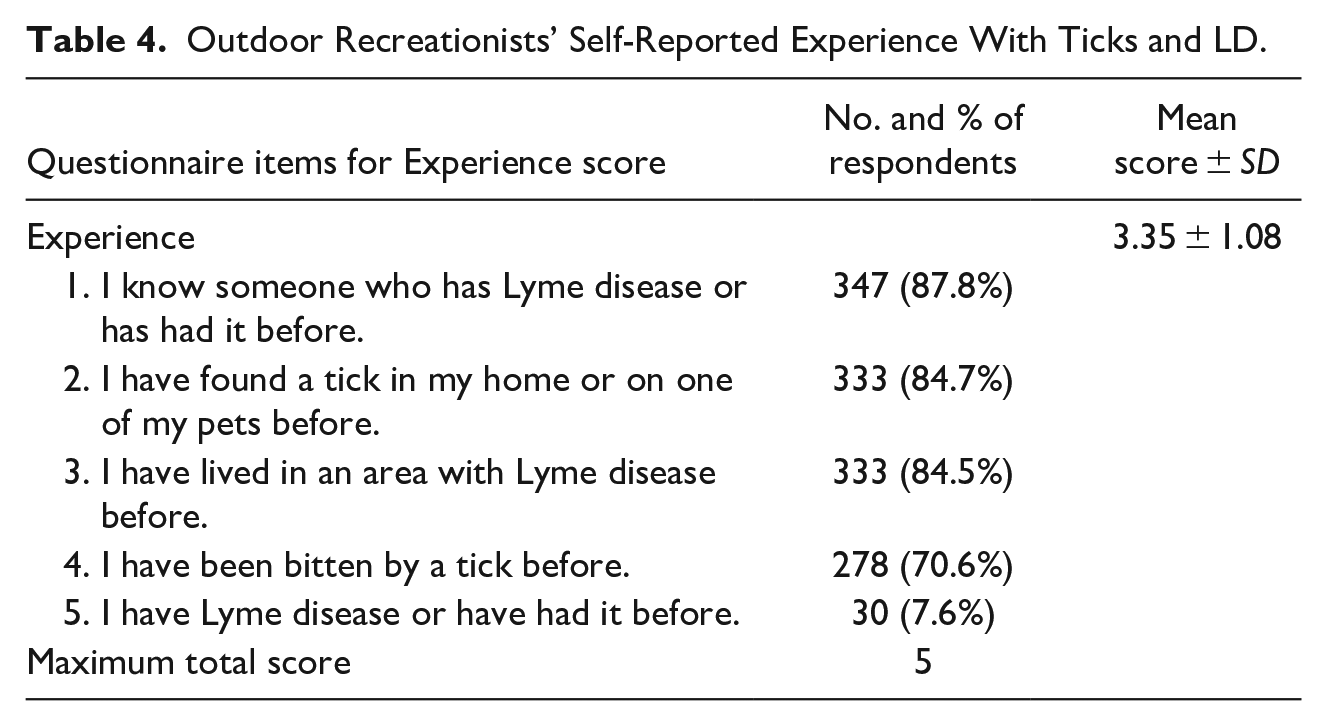
Research participants’ mean experience with ticks and LD score was also high (3.44 ± 1.08) which indicates that, on average, participants reported that they have experienced more than half of the scenarios in the questionnaire (Table 4). The most shared experiences among participants were knowing someone who has or has had LD (87.8%), having found a tick in one’s home or on one’s pets (84.7%), or having lived in an area with LD (84.5%). However, personal experience with LD was notably lower than other questionnaire items asking about experience, with only 7.6% of participants reporting having had LD.
Outdoor Recreationists’ Self-Reported Experience With Ticks and LD.
Perceptions of LD Risk and Benefits of Prevention Practices
Six out of the seven observed questionnaire items loaded with perceived risk, with component loadings >0.4 (Table 5). Therefore, the item “my risk of being bitten by a tick is equal to the risk of other people” was dropped from the analysis to improve the overall reliability of the perceived risk composite scale. A reliability analysis conducted on the six observed variables associated with perceived risk generated an acceptable Cronbach’s alpha value of 0.694 (Desselle, 2005). The perceived risk composite score was then calculated using the mean score of six questionnaire items. Analysis showed that participants reported moderate levels of perceived risk with an average level of risk perception of −0.82 (SD ± 0.33).
Outdoor Recreationists’ Perceived Risk and Perceived Benefits Mean Scales.
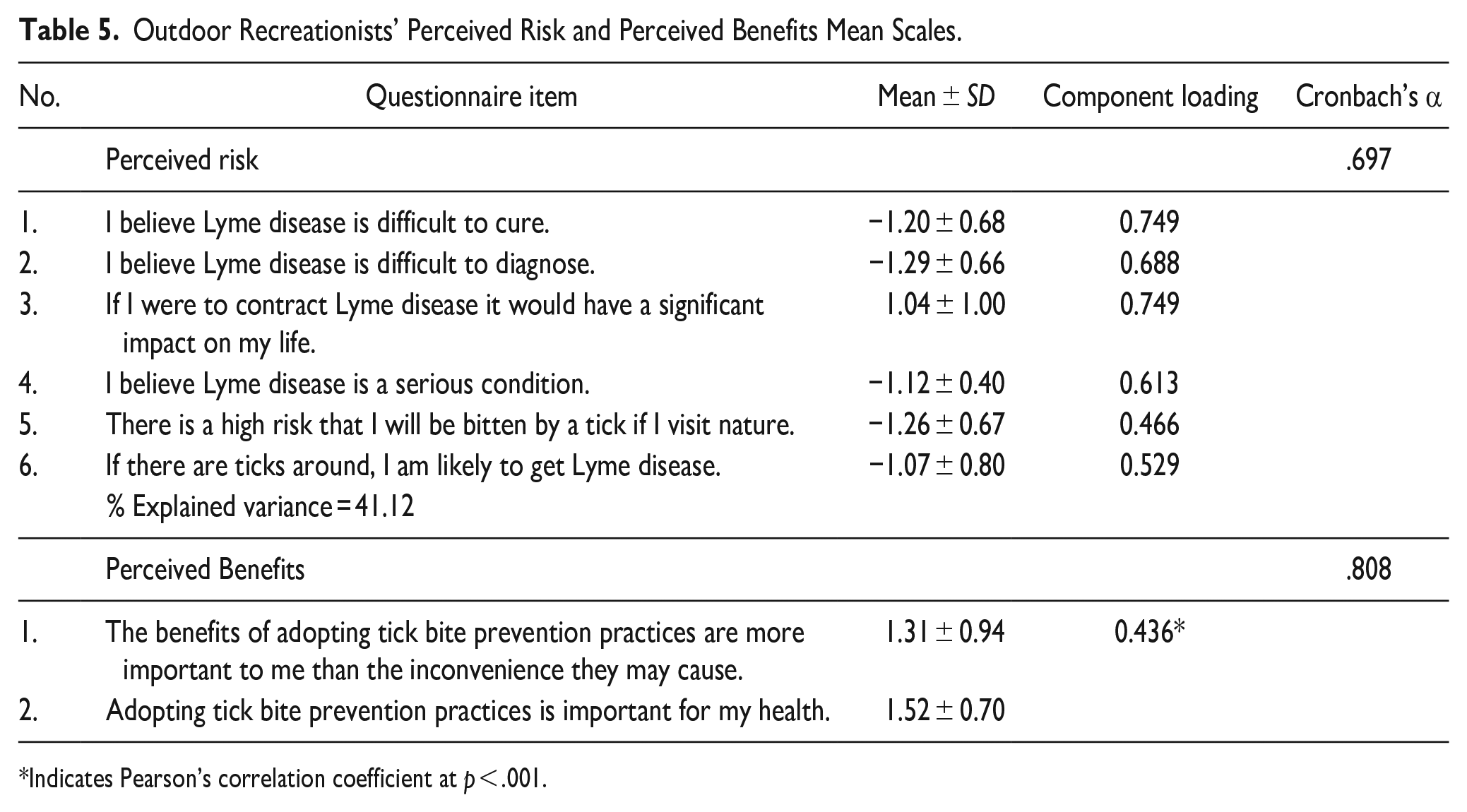
Indicates Pearson’s correlation coefficient at p < .001.
Regarding perceived benefits, the analysis revealed a statistically significant positive correlation (r = 0.44, p < .001), indicating a moderate association between the items. The perceived benefit composite score was then calculated using two questionnaire items (Table 5). The average level of perceived benefits among participants was 1.42 (SD ± 0.76).
Perceptions on Method Efficacy, Self-efficacy, and Barriers
As stated in the methods section, efficacy beliefs and perceived barriers to performing preventive behavior were measured through behavior-specific statements. The analysis on the method efficacy scale revealed a statistically significant positive correlation between the two questionnaire items across all types of preventive behavior (wear protective clothing, use of insect repellent and performing tick checks; Table 6). Cronbach’s alpha values for method efficacy items were >.60 in all three behavior models, signifying an acceptable internal consistency of these scales. According to research participants, the average level of method efficacy was 1.36 (SD ± 0.78) for use of protective clothing, 1.20 (SD ± 0.91) for use of insect repellent, and 1.57 (SD ± 0.70) for performing tick checks.
Outdoor Recreationists’ Efficacy Beliefs and Perceived Barriers Mean Scales.
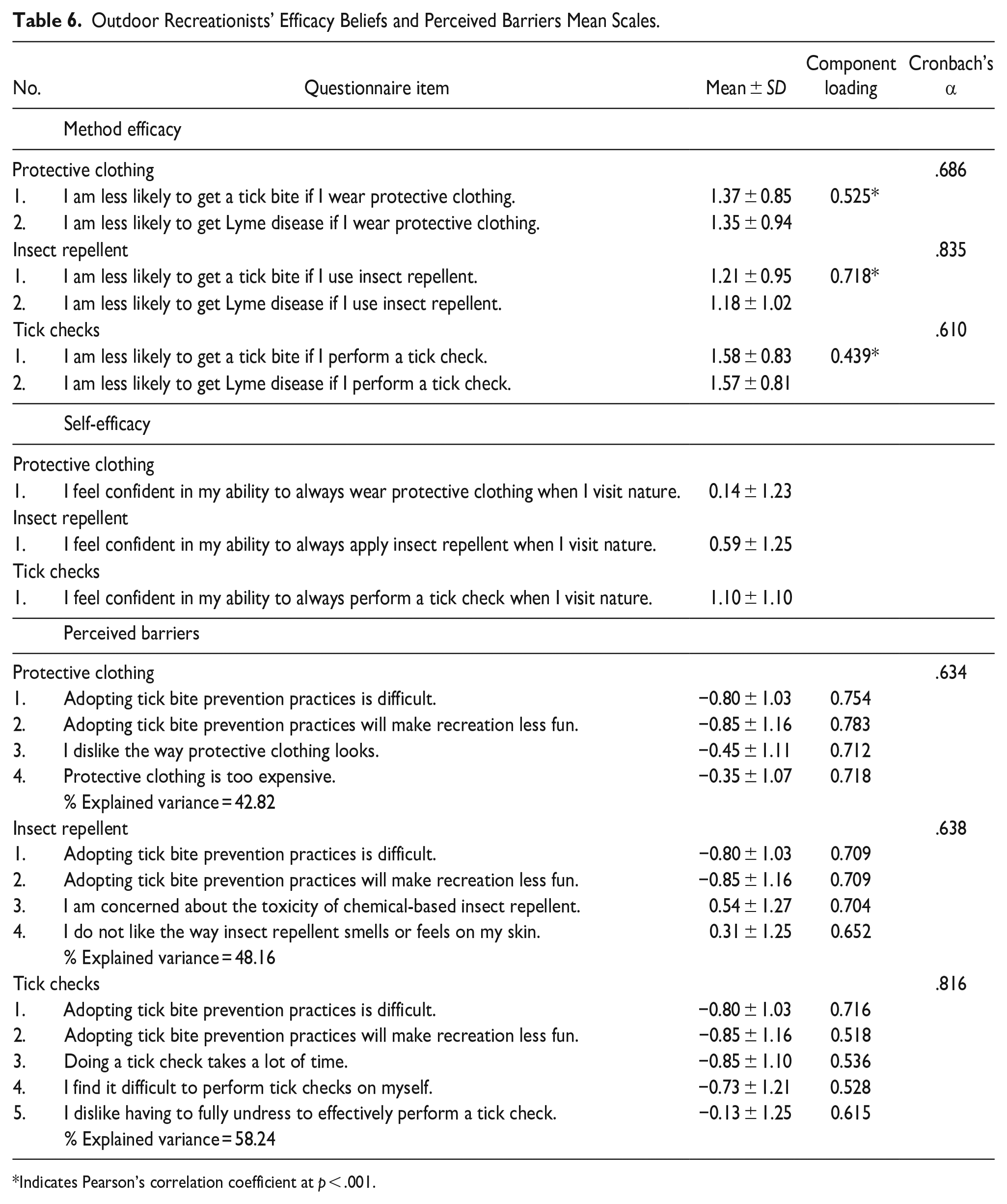
Indicates Pearson’s correlation coefficient at p < .001.
As self-efficacy was measured with one behavior-specific questionnaire item per model, no principal component, Person’s r or reliability analyses were necessary for this construct. However, we found that the average level of self-efficacy was 0.14 (SD ± 1.23) for use of protective clothing, 0.59 (SD ± 1.25) for use of insect repellent, and 1.10 (SD ± 1.10) for performing tick checks (Table 6).
Perceived barriers for each behavior model were assessed. The PCA for perceived barrier composite score showed component loadings >0.6 demonstrating that the construct was associated with each variable in the three models (Table 6). The reliability analysis showed a Cronbach’s alpha >0.6 meaning acceptable internal consistency of the three scales. Following these two analyses, the average level of perceived barriers to perform preventive behavior was −0.61 (SD ± 0.75) for use of protective clothing, −0.20 (SD ± 0.82) for use of insect repellent, and -0.67 (SD ± 0.87) for performing tick checks.
Lyme Disease Preventive Behavior Among Outdoor Recreationists
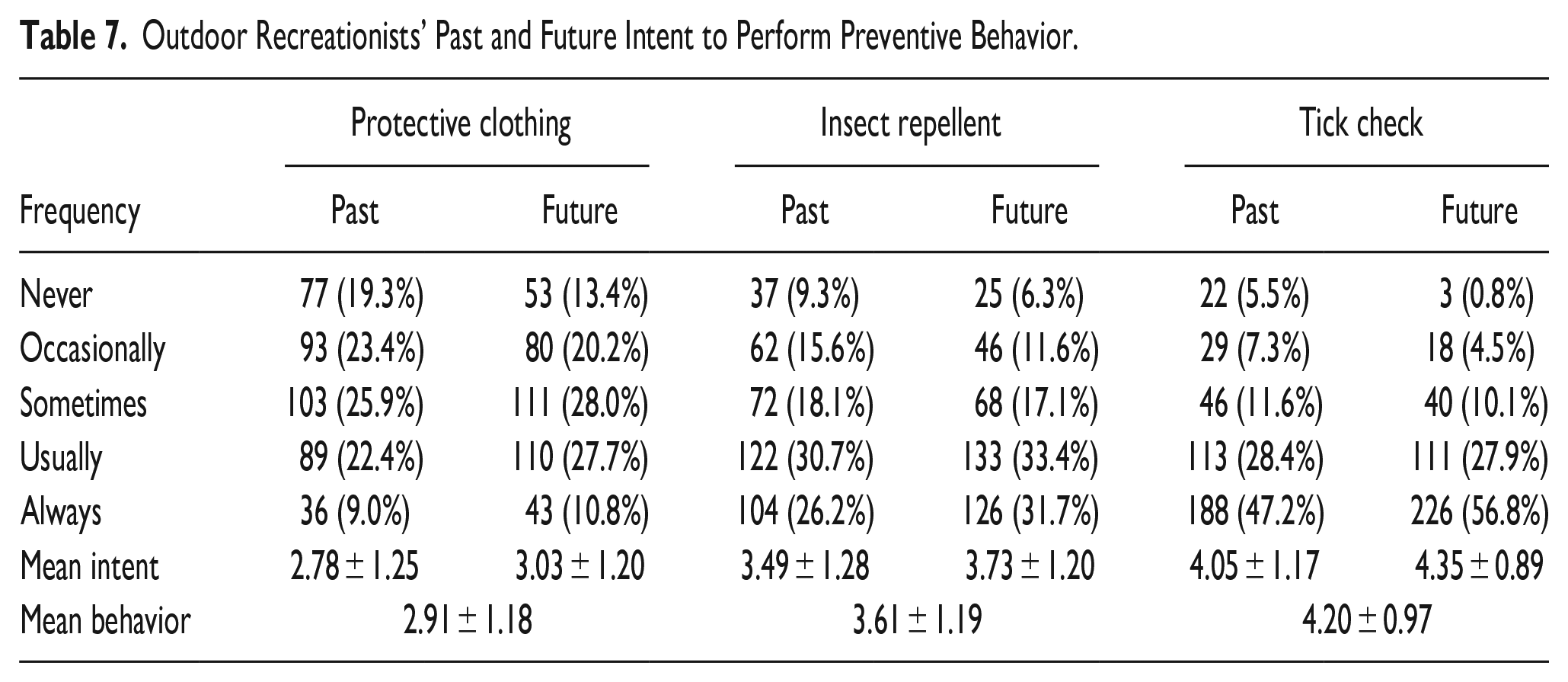
Overall, the most common LD preventive method reported by outdoor recreationists, both retrospectively (47.2%) and for future intent (56.8%), was the tick check (Table 7). Results also show that participants’ past and future intent of performing tick checks was 4.05 ± 1.17 and 4.35 ± 0.89 respectively. Tick checks was also the LD preventive method with the highest reported values for both method efficacy (i.e., how well will this preventive measure work) and self-efficacy (i.e., how capable I am to practice this behavior; Table 6).
Outdoor Recreationists’ Past and Future Intent to Perform Preventive Behavior.
The analysis of the last conceptual model construct, LD preventive behavior, through bivariate correlations and linear regression showed diverse results. When considering the protective clothing behavior as a dependent variable, four out of seven constructs were associated in the expected direction with the predicted behavior (Table 8); self-efficacy (β = .468, p < .001), perceived barriers to wear protective clothing (β = −.151, p < .001), method efficacy (β = .144, p < .001), and perceived benefits (β = .156, p < .001) were found statistically significant associated to protective clothing behavior. However, perceived risk, knowledge, and experience were not statistically significant associated to protective clothing behavior. The protective clothing method model explained 40.6% of the variance in protective clothing behavior among participants.
Linear Regression Analysis Predicting Lyme Disease Preventive Behavior.
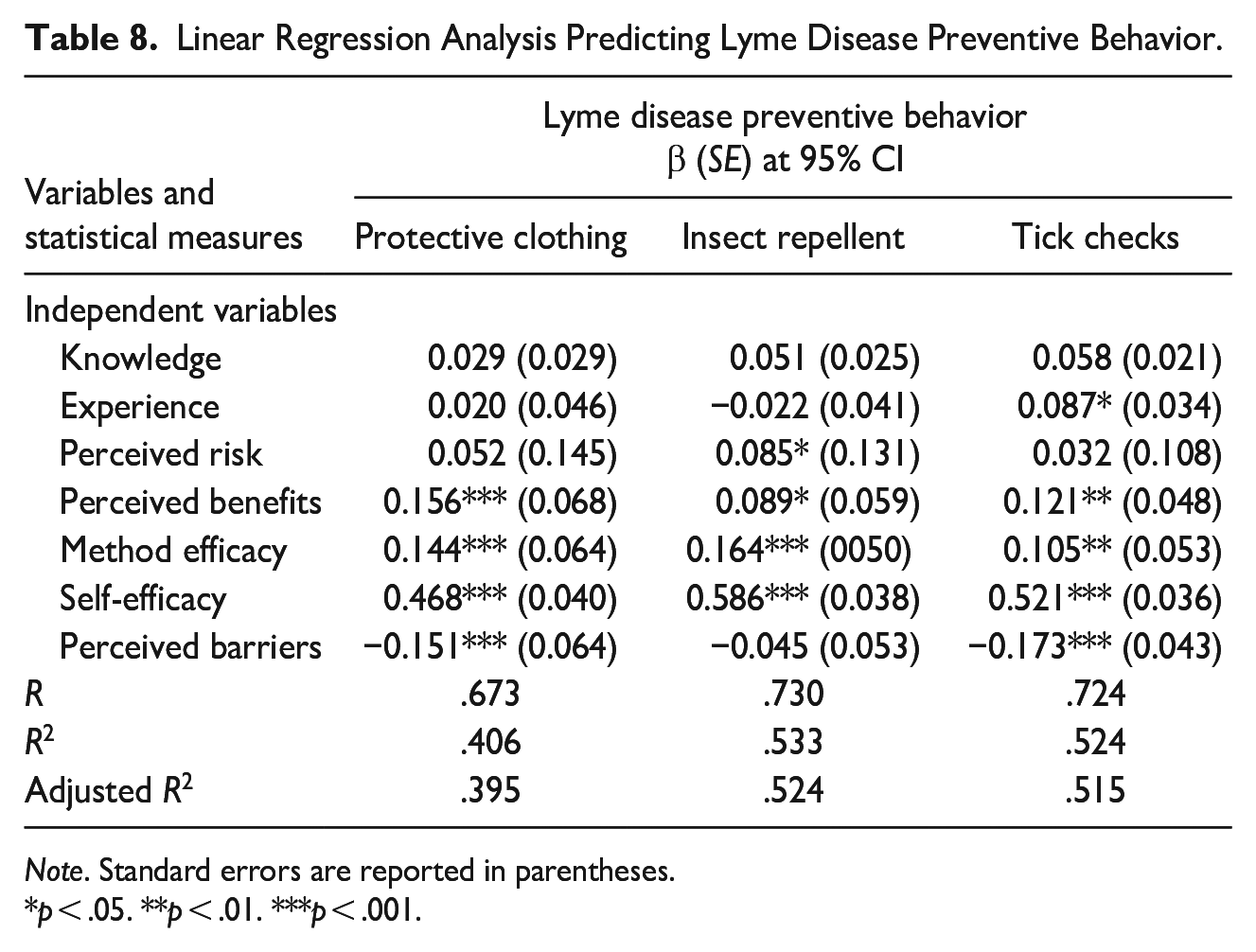
Note. Standard errors are reported in parentheses.
p < .05. **p < .01. ***p < .001.
When considering the repellent use behavior as a dependent variable, four out of seven determinants were associated in the expected direction with the predicted behavior (Table 8); self-efficacy (β = .586, p < .001), method efficacy (β = .164, p < .001), perceived risk (β = .085, p < .05), and perceived benefits (β = .089, p < .05) had a strong correlation with the dependent variable. However, perceived barriers to repellent use, knowledge and experience of ticks and LD did not have a statistically significant correlation with repellent use behavior. The repellent use method model explained 53.3% of the variance in repellent use.
Finally, five out of seven constructs were associated in the expected direction with tick check behavior (Table 8); self-efficacy (β = .521, p < .001), perceived barriers to perform tick checks (β = −.173, p < .001), method efficacy (β = .105, p < .01), perceived benefits (β = .121, p < .001), and experience with ticks and LD (β = .087, p < .05) had a statistically significant correlation with the dependent variable. Perceived risk and knowledge of ticks and LD had no statistically significant association with tick check behavior. This model explained 52.4% of the variance in tick check behavior.
Discussion
The increasing incidence of LD in the state of Maine has fostered diverse educational programs and outreach initiatives targeting communities in general due to their proximity to high tick density areas and TBD prevalence (Maine Center for Disease Control and Prevention, 2022a, 2022b). While the effectiveness of tick bite preventive behaviors (e.g., tick checks, using insect repellent and wearing protective clothing) is not extensively documented and the existing evidence my lack definitive consensus (Richardson et al., 2019; Vázquez et al., 2008), government agencies, epidemiologists and public health providers still encourage these practices among populations exposed to TBDs (Eisen & Stafford, 2021; Nawrocki & Hinckley, 2021; Puppo & Préau, 2018). We examined the psychosocial determinants of three prominent LD preventive behaviors among outdoor recreationists, a population highly exposed to tick bites due to the nature of outdoor recreation in the state of Maine. Data analysis suggests five important theoretical and practical findings.
First, we found that outdoor recreationists did not regularly engage in the tick bite preventive behaviors of interest. Performing tick checks was the most widely adopted preventive behavior among recreationists who perform a tick bite preventive method, followed by using insect repellent and, lastly, dressing in protective clothing. Beaujean, Bults, et al.’s (2013) study on public perceptions and LD preventive practices among residents in the Netherlands found that research participants were most likely to perform a tick check. However, when looking at past behavior data, it was found that wearing protective clothing was the most common practice (37%), followed by tick checks (32%) and using insect repellent (6%; Beaujean, Bults, et al., 2013). Overall, the authors found lower levels of preventive practices among survey respondent compared to other studies (e.g., Phillips et al., 2001) which require a deeper understanding of why people do not fully engage in preventive behaviors in high LD incidence regions. In our study, given the permanent messaging from Maine agencies and public health providers about the implications of TBD and the importance of performing tick bite preventive practices, we would have expected higher levels of current practice and future intent reported by outdoor recreationists (Donohoe et al., 2018; St. Pierre et al., 2020). This finding is consistent with previous studies in LD preventive behavior among residents in LD endemic and emerging areas such as Connecticut, Maryland, Minnesota, Wisconsin, and Quebec (Canada) where low levels of LD preventive behavior adoption were found despite institutional messaging and risk of exposure (Aenishaenslin et al., 2015; Beck et al., 2022; Niesobecki et al., 2019). We suggest that public messaging must consider other psychosocial factors associated with LD preventive behavior that can contribute to behavioral change among outdoor recreationists as discussed in Aenishaenslin et al. (2022).
Second, the combined conceptual model to study the determinants of LD preventive behavior (Figure 1) applied in this paper indicated that individual perceptions of self-efficacy, method efficacy, and perceived benefits contributed significantly to prevention practice in each of the three behavior models studied. Among these determinants, self-efficacy showed the most significant association with the three preventive behaviors. Our results echo what previous research in TBD preventive behavior has found on psychosocial determinants of health preventive behavior (Aenishaenslin et al., 2015, 2017). For instance, Donohoe et al.’s (2018) study on demographic and psychosocial predictors of TBD preventive behaviors among State Parks employees showed that study participants were most likely to perform tick checks due to their increased confidence or perceived ability for taking action to prevent tick bites. Self- efficacy has also found to be a strong predictor of tick bite preventive behavior among residents in Canada and Switzerland (Aenishaenslin et al., 2015, 2017) and the Netherlands (Beaujean, Bults, et al., 2013).
Third, as efficacy beliefs (i.e., self-efficacy and method efficacy) were strongly correlated with the three LD preventive behaviors, it is imperative to stress the need of integrating a novel approach for LD prevention and awareness programs targeting communities with high occupational risk (Connally et al., 2009; Donohoe et al., 2018; Kurnatowski et al., 2011; St. Pierre et al., 2020). By creating experiential learning and/or hands-on activities to successfully perform LD preventive behaviors, individuals can acquire new skills and gain confidence in their ability to perform certain health behaviors (Beaujean, Gassner, et al., 2013; Richardson et al., 2019). Following our findings, health promotion organizations can integrate activities to foster self-efficacy around tick bite preventive behavior, especially tick checks, to minimize perceived barriers to performing this method. McAlister et al. (2002) provide a comprehensive list of additional strategies to increase self-efficacy, such as guided practice, verbal persuasion, and planning coping responses.
Fourth, contrary to what has been reported in prior research (Brady et al., 2022; Donohoe et al., 2018; Slunge & Boman, 2018), our study found a weak association between risk perception and use of insect repellent and no association of this construct and the remaining two preventive behaviors. Therefore, we suggest that interventions focused solely on increasing LD risk perceptions should be approached with caution (Decker et al., 2012; Fogel & Chawla, 2017; Peters et al., 2013; Slunge & Boman, 2018). As previous research has found, threatening- or fear-arousing messages (e.g., fear appeals) may only have an impact on changing health behavior under high self-efficacy conditions (Peters et al., 2013). While it is important to acknowledge the association between fear appeals and tick bite preventive behavior, it is essential to consider a more nuanced approach that emphasizes both the emotional aspect and the individual’s capability to perform tick bite preventive practices. As described previously, our study found that efficacy beliefs are strongly associated with preventive behavior. Therefore, an integrative approach that targets risk perception, efficacy beliefs and preventive behavior may improve outcomes of educational campaigns. For example, public health intervention approaches could provide factual information about proximity to tick habitat, share personal stories and testimonials about LD exposure and preventive methods, offer support networks, and reinforce positive outcomes. These strategies may contribute to minimize anxiety or fear while encouraging tick bite prevention.
Fifth, we found that experience and knowledge were not associated with LD prevention as expected. Although experience had a statistically significant association with the tick check behavior model only, overall, our findings do not show that this construct was key in determining LD preventive behavior. Similarly, knowledge did not show association with any of the LD preventive behavior models. Our findings contrast what has been found in Beaujean, Bults, et al. (2013), Herrington (2004), Herrington et al. (1997) and Nawrocki and Hinckley (2021) where knowledge and experience were found to be strong predictors of some tick bite preventive methods. Instead, our results echo Van Der Heijden et al.’s (2017) research, who found no association between individual knowledge and performance of the tick check. Previous research in determinants of preventive behaviors has suggested that residents of high LD incidence regions become habituated to the occurrence of tick bites and TBDs, resulting in lower levels of preventive behavior (Slunge & Boman, 2018; Van Der Heijden et al., 2017). In our study population, a combination of contextual factors (i.e., high LD incidence rate in the state of Maine) and outdoor recreationists’ level of knowledge and experience of ticks and LD may be contributing to lower levels of preventive practices. The association between knowledge, experience and preventive behavior requires further exploration among residents and visitors of high LD incidence regions. Our findings also bring into question the prioritization of awareness initiatives by health authorities and local governments. Among current strategies in place for promoting LD prevention in communities, education is often at the forefront. However, the immaterial influence of individual knowledge and experience on preventive behavior brings into question the efficacy of this public health approach.
Finally, we want to draw attention to the high levels of explained variance observed in each of the LD preventive behavior models. Our findings underscore the significance of novel hybrid health behavior approaches in identifying the underlying psychosocial factors that drive LD preventive behavior (Jacob et al., 2019). Previous research found that a SCT model applied to tick checks explained 25% of the variance in individual’s tick check behavior (Van Der Heijden et al., 2017). Our combined conceptual model to study LD preventive behavior shows promising applications to TBDs and other zoonotic diseases that require both theoretical models and contextual applications to fully contribute to the understanding of the human dimensions of zoonotic diseases and, potentially, informing health policies and educational programs (Jacob et al., 2019; Valois et al., 2020).
The combined conceptual model to study LD preventive behavior was successful in explaining key psychosocial determinants of the most used (and recommended) tick bite preventive behaviors. However, we need to acknowledge some limitations of our study. The in-person surveying of outdoor recreationists in a LD endemic area, during a high-risk season, was designed to limit the effect of recall bias on the self-reported behavior responses. However, the self-reported nature of this data still presents potential biases. Self-reporting of health behaviors could have led some participants to overestimate the extent to which they engage in prevention measures. Another limitation is related to the research instrument design. First, the questionnaire combined general health preventive behavior questions and behavior-specific questions (statements focused on ticks and LD) that may have been so widely reported among participants that the predictive power of some constructs (experience and knowledge) was artificially diminished. Future research is needed to understand the influence of knowledge and experience on LD preventive behavior. Second, the number of survey items within a construct scale to measure efficacy beliefs and perceived barriers may have dropped the internal consistency of these scales. We suggest using more than five survey items within a construct scale to impact reliability (Vaske et al., 2017). Another limitation is the exclusion of the HBM’s construct “cues to action” in our study. While this variable was not included in the included in the final theoretical framework for this research, state agencies and municipal recreation areas dedicate time and resources each year into generating notices and educational materials aimed at increasing awareness of local LD risks. Future research can assess the influence of cues to action on determining individual’s LD preventive behavior. Finally, we recommend experimental testing of the models examined in this study in other high-risk populations. In 2021, Maine was the state with the highest incidence rate (110 cases per 100,000 people) and extending this research to other high-risk states like Rhode Island, New Jersey, and Wisconsin with 2021 incidence rates of 89, 38, and 37 respectively would be a useful next step (CDC, 2022). Future research should focus on diverse occupational groups, including outdoor workers like wildlife biologists, foresters, and park rangers. Additionally, it would be valuable to examine other categories of individuals engaged in outdoor recreational activities, such as golfers, backcountry campers, and hunters. By expanding the scope of these investigations, a comprehensive understanding of the models' effectiveness and applicability can be attained across various contexts.
Conclusion
The goal of this research was to provide a preliminary understanding of the human dimensions of LD and offer insights into the ways in which outdoor recreationists think about and respond to the current landscape of LD risk. While the current literature has documented the knowledge, attitudes, and beliefs of general populations in endemic communities, minimal research has been conducted among populations that frequently engage with forest landscapes for recreational or occupational purposes. This research aimed to fill that gap by characterizing the psychosocial determinants of outdoor recreationists’ preventive behaviors. Our findings demonstrate the importance of integrating psychosocial factors such as efficacy beliefs, perceived risk and perceived benefits in public health programs that target communities in LD endemic regions. By understanding what psychosocial factors, besides knowledge of and experience with ticks and LD, can influence people’s preventive behaviors, researchers, practitioners, and public health organizations may improve the impact of health behavior campaigns. Further exploration of the human dimensions of LD will inform future education and extension initiatives aimed at managing the spread and persistence of the disease in forest landscapes across the northeastern US.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a USDA National Institute of Food and Agriculture grant (No. ME012450318) and two Maine Agricultural and Forest Experiment Station projects (No. ME021826 and ME021905).