
Abstract
This is a visual representation of the abstract created by Nichol Marsh.
Introduction
Indigenous Peoples to Turtle Island, also called Canada, have diverse, thriving cultures and healing practices (Ansloos et al., 2022; Redvers, 2020). Yet they continue to experience trauma from ongoing systemic racism within healthcare, social, education, and justice systems (Allan & Smylie, 2015; Fraser Salish Region First Nations Health Authority, 2022; In Plain Sight, 2020). The residential school system, one of many examples, was intended to assimilate Indigenous children into white, Christian society. The ongoing and intergenerational harms of these schools continue to be uncovered; including accounts of children being subjected to abuse, medical and nutritional experimentation (Mosby, 2013; Truth and Reconciliation Commission of Canada, 2015).
Institutional harm inflicted upon Indigenous Peoples is not a historical phenomenon. In 2020, claims of racism in British Columbia's provincial health care system led to an investigation resulting in the In Plain Sight report 1 (2020). This report found that anti-Indigenous racism within the British Columbia healthcare system leads to discomfort and fear Indigenous Peoples experience when interacting within the Canadian healthcare system (In Plain Sight, 2020). Systemic racism contributes to poorer outcomes experienced by Indigenous Peoples compared to non-Indigenous people, including but not limited to, higher prevalence of disability, diabetes, and substance use (Kim, 2019), poorer mental health (Boksa et al., 2015), and a lower life expectancy (Tjepkema et al., 2019).
Assessments are often a first point of contact between occupational therapists and service users. Assessments act as gatekeepers to funding and resources for Indigenous Peoples and inform occupational analysis and interventions (Byrne et al., 2020; Jacklin et al., 2020). Many assessments used by occupational therapists may not align with Indigenous Peoples’ cultural values (Price & Pride, 2023; White & Beagan, 2020). The western focus on deficits and problems to be “fixed” conflicts with various Indigenous ways of knowing that may value a person's strengths and relationships with people and the land (Kennedy et al., 2022). Occupational therapists often work in neoliberal influenced institutions, such as healthcare, that prioritize efficiency and standardized approaches over therapeutic relationships (Aldrich & Rudman, 2020; Trentham et al., 2021). In these contexts, clinicians may unintentionally reproduce trauma and health inequities for Indigenous Peoples; therefore, occupational therapists should facilitate the development of culturally safer assessment strategies (Byrne et al., 2020; CAOT, 2018; Jacklin et al., 2020). In this study, we refer to assessment strategies as the variety of ways occupational therapists approach information gathering to inform analysis and intervention. This may include how practitioners select and modify assessments such as adapting the assessment environment and the timing of assessments.
Cultural safety has emerged as an important component of addressing anti-Indigenous racism and its deleterious effects in healthcare (Allan & Smylie, 2015; Loppie & Wien, 2022). Culturally safer practice requires providers to critically examine and address power imbalances in healthcare to inform safe, respectful healthcare relationships and experiences (Curtis et al., 2019; First Nations Health Authority, n.d.). Indigenous Peoples have created frameworks and recommendations for culturally safer healthcare practices (CAOT, 2018; First Nations Health Authority, 2013; Swartz, 2015; TRC, 2015). In their final report and Calls to Action, the TRC states that all healthcare practitioners should collaborate with Indigenous Peoples and incorporate Indigenous ways of knowing into healthcare services (TRC, 2015), which we understand to include occupational therapy assessment strategies. In alignment, the Competencies for Occupational Therapists in Canada (2021) require all clinicians to promote anti-oppressive behaviour, contribute to a culturally safer practice, 2 and challenge social structures that marginalize people (ACOTRO, ACOTUP, & CAOT).
Few assessment tools have been developed in collaboration with Indigenous Peoples in Canada with the intention of being culturally relevant (Jacklin et al., 2020; Walker et al., 2020; White & Beagan, 2020; Young et al., 2013). These include the Aboriginal Children's Health and Well-being Measure (Young et al., 2013), the Canadian Indigenous Cognitive Assessment (Jacklin et al., 2020), the Northern Pain Scale (Baker & Giles, 2013; Ellis et al., 2011), and the Native Wellness Assessment (Fiedeldey-Van Dijk et al., 2017). These assessments may be a start towards culturally safer care; however, we argue that they are too few and are not necessarily generalizable to the diverse Indigenous Nations in Canada and diverse occupational therapy practice settings. Currently, clinicians rely on their own reasoning and experience to adapt assessments (Pidgeon, 2015; White & Beagan, 2020). We are concerned that this may lead to infiltration of the therapists’ own colonial values in the assessment process, regardless of good intent. Consequently, there is a need for further scholarship, ideally led by Indigenous Peoples, to be done in Canada to outline culturally safer occupational therapy assessment strategies.
Locating Ourselves and Our Work
This project emerged from multiple conversations held through the Canadian Occupational Therapy and Indigenous Health Network (OTIHN), where occupational therapists shared their challenges in navigating culturally safer practice. A group of occupational therapy clinicians from the OTIHN volunteered as community consultants throughout this project.
We are choosing to reflect on, and making our positionality known to situate ourselves within this work and our collective roles in reconciliation and decolonization (Kovach, 2021). Pamela Barnes, hereafter referred to as Pamela, is a Sylix knowledge keeper and Matriarch living in British Columbia and member of the Westbank First Nation. She is an educator and is an adjunct professor with the School of Nursing (University of British Columbia-Okanagan) and an Honorary Fellow (Okanagan College). Her academic background is in Aboriginal government. Her traditional Syilx education is a lifelong journey following her great-grandfather and other knowledge-keepers. In true Syilx tradition she strives to educate and mentor the next generations in all the work she does. As a Syilx educator, Pamela teaches cross-cultural awareness to all ages and backgrounds. Her guidance is sought after by organizations, boards, and advisory groups, both locally and nationally. Kaarina Valavaara is a Métis queer cisgender woman, occupational therapist, clinical instructor at Dalhousie University, and was the co-chair of the OTIHN at the time of this project. Jay MacDonald is a gay, white, cisgender, settler of Scottish descent, occupational therapist, and assistant professor of teaching at the University of British Columbia (UBC). The two student researchers have Euro-settler colonial heritage and identify as white, cisgender, able-bodied women who are graduate students in the Master of Occupational Therapy program at the UBC. Tal Jarus is a queer, white, ciswoman, settler of western Europe descent, who immigrated to Canada 17 years ago, occupational therapist and a professor at the UBC.
Objective and Research Questions
Our objective was to explore current culturally safer occupational therapy assessment strategies. We aimed to respond to two research questions:
What are the perspectives of Canadian occupational therapists working with Indigenous Peoples on the challenges they face during assessments? How are Canadian occupational therapists currently seeking to increase cultural safety of existing assessments?
Methods
Our study design was informed by principles of respectful and ethical research with Indigenous Peoples and critical theory. As the research relates to Indigenous Peoples, we sought guidance from our Sylix and Métis team members to decolonize our methodologies (Smith, 2021), strive towards allyship, and ensure relevance of this research to Indigenous Peoples.
Critical theory recognizes that there is more than one absolute truth, and that knowledge is affected by social groups, their historical background and geographical location (Taylor, 2017). It can provide a lens to expose the colonial history behind the development of occupational therapy assessments, and to challenge societal norms, assumptions, and biases of Euro-settler culture that are built into occupational therapy assessments. Critical theory has been critiqued for its lack of reflexivity and failure to liberate oppressed groups (Smith, 2021). Consequently, this project relied on knowledge from Indigenous team members and decolonizing research resources to inform how to engage with this work in the spirit of respect and reciprocity (Kilian et al., 2019; Marsh et al., 2015; Smith, 2021).
Data collection used a mixed-methods approach of surveys and storytelling groups. Researchers employed a trauma-informed approach (Substance Abuse and Mental Health Service Administrator, 2014) and engaged in member checking and transparency. Recognizing the history of extractive and exploitative research with Indigenous Peoples, the student researchers engaged in repeated iterative meetings and communication with Indigenous team members (in person and virtual) to ensure their perspectives and lived experiences were accurately reflected and respected through data collection, analysis, and knowledge dissemination (Kovach, 2021; Tsosie et al., 2022).
Storytelling
Participants were invited to share stories within storytelling groups as a means of sharing, creating knowledge, and generating discussion (Archibald, 2008; Kovach, 2021). Given the predominance of non-Indigenous researchers and participants, traditional Indigenous storytelling methodologies were not employed. Following guidance from Pamela, we followed elements of storytelling methodologies to respect Indigenous ways of creating and sharing knowledge (Archibald, 2008; Hunt & Young, 2021; Kovach, 2021). This hybrid approach allowed us to blend elements of qualitative focus groups and storytelling methodologies appropriate for the researchers and study participants (Hunt & Young, 2021).
Recruitment
With approval from the UBC Behavioural Research Ethics Board we recruited Canadian occupational therapists through Canadian occupational therapy national and provincial professional associations, provincial regulatory colleges and practice networks’ email lists or advertising platforms (e.g., websites, social media, newsletters), and team members’ professional networks.
Inclusion Criteria
Occupational therapists currently working with Indigenous Peoples in Canada.
At least 1 year of experience working with Indigenous Peoples.
English speaking.
Procedures
An introductory email, which included a brief description of the study purpose and a description of the methods, was sent to participants with a link to the survey. Participants consented to participate in the study by submitting their survey. Upon submission, participants were invited to take part in an optional storytelling group.
Interested participants were contacted directly through email. The storytelling groups were conducted on a UBC secure Zoom account. The group sessions were 45 to 90 min in duration. Storytelling groups were transcribed with Zoom transcription software and edited for clarity. We asked all participants in storytelling groups to keep what is shared in the groups within the groups. Participants were also offered to log in to Zoom with a pseudonym, or to turn off their camera and mute their microphone at any point during the storytelling group. Transcripts of the groups were anonymized, and we changed any places and names to protect participants’ privacy. All data from the survey is anonymized.
Survey
The 10-question survey included 6-point Likert questions to gauge participants’ perspectives on the sufficiency of cultural safety training they have received, and open-ended questions about participants’ assessment practices with Indigenous Peoples, including selection; modification; reflections on challenges; and promising actions to culturally safer assessment practices (Appendix). In addition, seven closed-ended questions on clinicians’ demographics and their practice settings were included.
Storytelling Groups
Participants were encouraged to share stories from provided prompts (Figure 1). Each participant had the opportunity to share a story. After each story, everyone was encouraged to reflect and discuss their thoughts. In line with storytelling methodologies and critical theory, group facilitators were active participants in the storytelling and their data was included, as appropriate, in thematic analysis (Kovach, 2021).
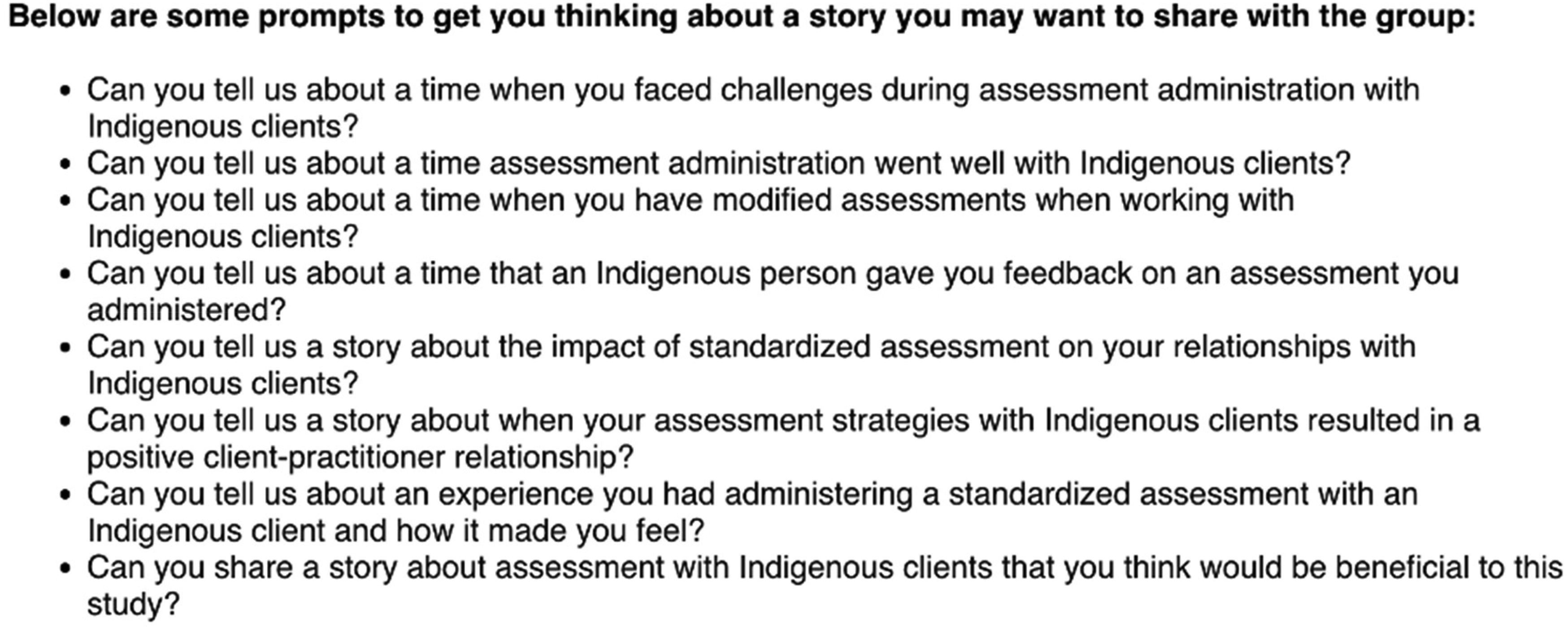
Storytelling group prompts.
Data Analysis
Analysis of survey and storytelling transcripts took place simultaneously. Closed-ended survey questions were analyzed with descriptive statistics. For open-ended survey questions and storytelling transcripts, we drew upon Braun and Clarke's reflexive thematic analysis where we creatively coded and collaboratively developed themes with our team members (Braun & Clarke, 2006). Open-ended survey questions and storytelling sessions were coded and themed initially by the two student researchers. Emerging themes were identified, and modifications were made to existing themes, returning to transcripts and surveys to ensure meaning was preserved. Indigenous team members were engaged during thematic analysis, for both surveys and storytelling groups, to confirm themes and highlight pertinent findings from their perspectives and experiences.
Once the research team came to consensus, we provided participants an opportunity to provide feedback on the themes via email to ensure research rigor (Braun & Clarke, 2006). Three participants responded by email to confirm agreement. Preliminary themes were also shared with Pamela who contextualized the themes into her own personal experience with the health system, during a recorded (and later transcribed) conversation on Zoom.
Findings
Participant Information
Forty-three occupational therapists completed the survey, with 39 (90.7%) of occupational therapy participants identified as female, similar to the national average of 90.8 (CIHI, 2024), two identified as nonbinary, and one did not respond. Their years of practice as an occupational therapist ranged from 1.5 to 38 years (M = 11.46, SD = 9.5). A similar range of 1–38 years was found among participants in their years practicing with Indigenous Peoples (M = 9.24, SD = 7.96). Participants represented a mix of rural, suburban, and urban practice locations (39.6%, 20.8%, and 39.6%, respectively) with a variety of practice settings (Table 1). Representation from urban and rural locations is important in the context of increased urbanization of Indigenous Peoples in Canada (Statistics Canada, 2023).
Practice Setting (43 Participants)
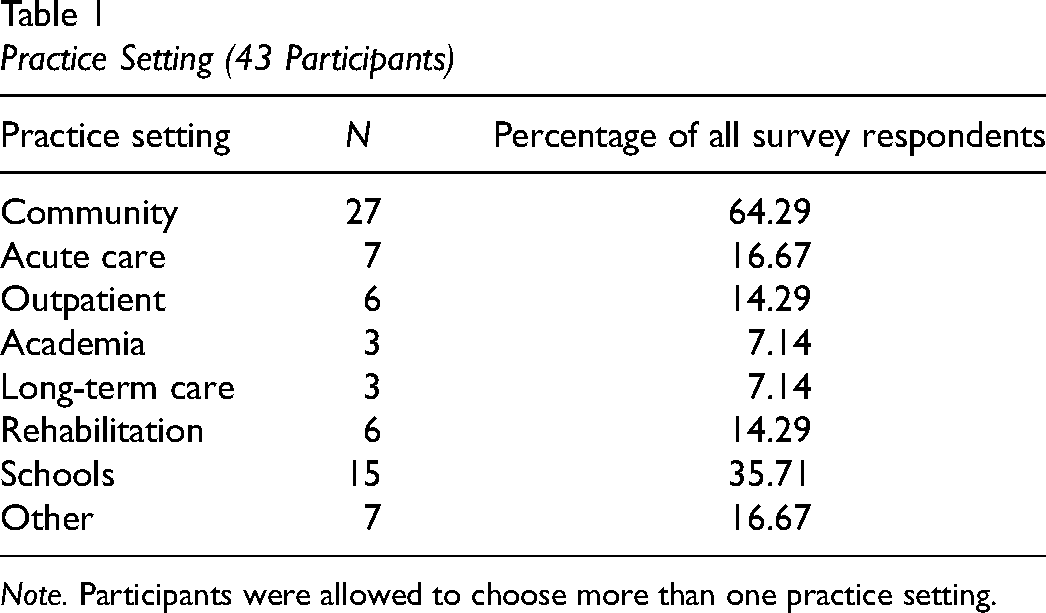
Note. Participants were allowed to choose more than one practice setting.
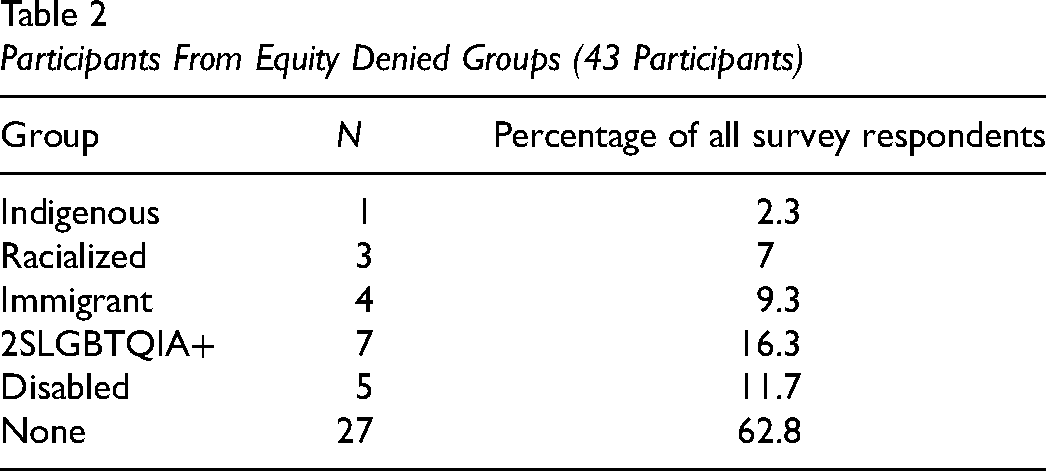
We decided to capture participant data reflective of multiple sources of identity, primarily those that have been historically underrepresented in the occupational therapy literature; hereafter referred to as equity denied groups (Table 2) (Interdepartmental Terminology Committee on Equity, Diversity and Inclusion, 2024). Survey responses were structured with the ability to self-describe to multiple identities rather than just be limited by predefined characteristics. Data was aggregated into common groups by the research team. Three participants (6.9%) marked more than one identity. Of the 43 total participants, 16 took part in four storytelling groups, each with two to five members.
Participants From Equity Denied Groups (43 Participants)
Emerging Themes
Three distinct, yet interconnected themes emerged, each with corresponding subthemes. Titles of themes are represented by emblematic quotations from occupational therapy participants or Pamela.
The first theme focused on systemic pressures—“All of our current systems are based in white colonialist processes…It would almost take dismantling the entire healthcare system to be truly culturally safe.” Participants shared frustrations with the number of systemic barriers to culturally safer assessment practices they encountered. They reported immense pressure to complete standardized assessments contradicting their efforts to build relationships with Indigenous service users and advocate for assessment approaches that could lead to culturally safer experiences. Sources of this pressure include: (i) physicians or other referring colleagues and (ii) third-party funders including insurance companies, health authorities, and government programs delivering medical equipment, supplies, and services. These pressures exist despite participants revealing that they knew of no, or very few, standardized assessments developed for and in collaboration with Indigenous Peoples that reflect Indigenous ways of knowing and doing. Participants shared strategies (Table 3) used to resist these systemic pressures in their assessments, analysis, and documentation.
Strategies Implemented by Participants to Increase Cultural Safety
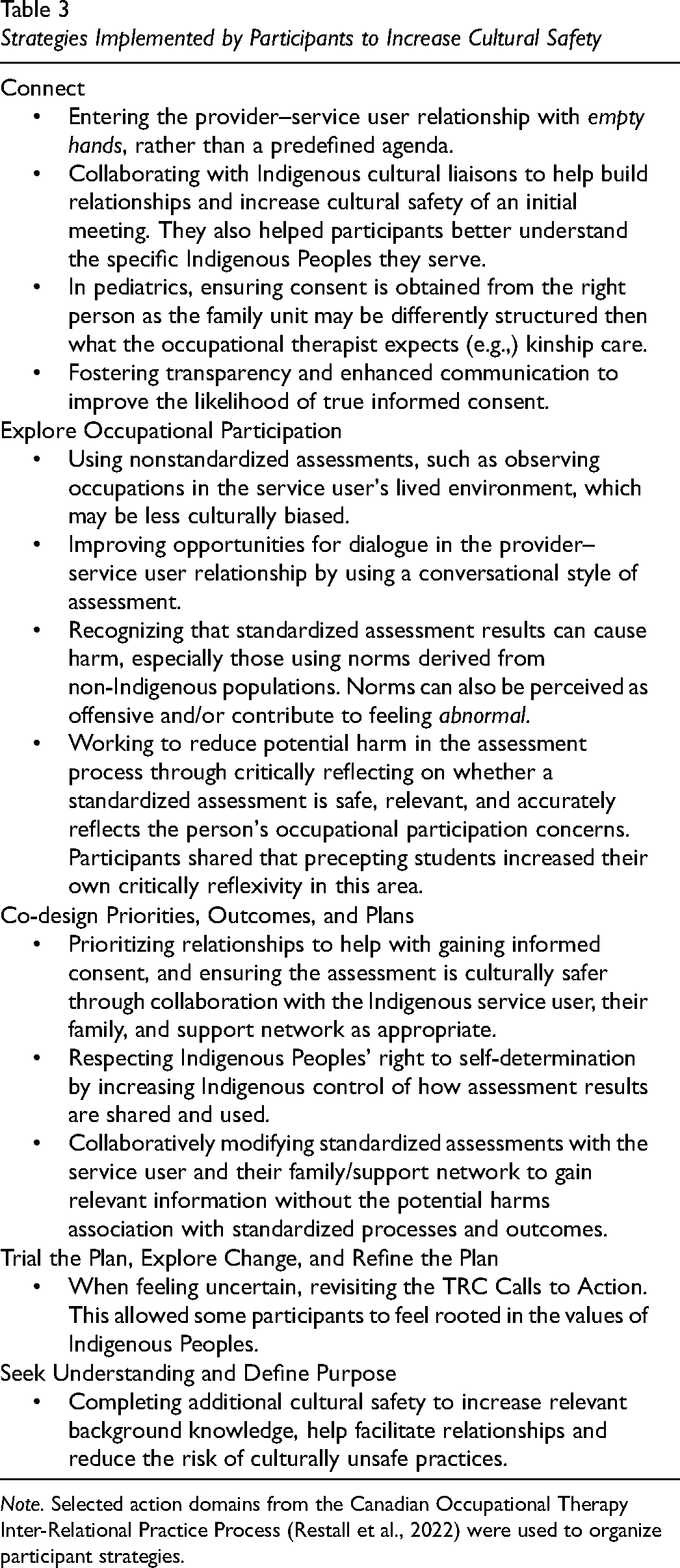
Note. Selected action domains from the Canadian Occupational Therapy Inter-Relational Practice Process (Restall et al., 2022) were used to organize participant strategies.
The second theme addresses the importance of connection and building relationship during the assessment process, “It comes right back down to trying to really make that human-to-human connection with people, and just how important that is in setting the tone for moving forward.” The participants shared that many standardized assessments were not created for or considerate of Indigenous ways of knowing or doing. However, they did feel that when there is an established relationship with the person and/or family it made introducing and completing these assessment tools, as imperfect as they are, a culturally safer experience. They stressed the limits of their knowledge on the lived experiences of Indigenous Peoples and shared practices of ongoing self-reflection of their own positionalities and assumptions in the assessment process. Similarly, when survey respondents were asked how confident they are with their Indigenous cultural safety training knowledge, and skills, they reported not feeling very confident (M = 4.13, SD = 0.87). Only 30% of respondents responded yes to “I have received Indigenous cultural safety training and feel that I have sufficient knowledge and skills in this area”; 66.7% of participants did, however, strongly agree they would feel comfortable if Indigenous Peoples receiving their services mentioned Indigenous teachings and practices during initial assessment (M = 5.49, SD = 0.96). This implies a level of openness and flexibility to multiple ways of knowing and doing within the therapeutic relationship building and process.
The final theme highlights the importance of consent, the right to say “no” as captured in Pamela's words, “Let's not lose sight of it's my health, and it's my body, and there might be the best drug in the world, but I might have reasons. It's still my body.” Many participants expressed uncertainty around their ability to obtain informed consent from Indigenous service users, particularly given the pressures of standardized assessments being required to fund services. They recognized the historical and ongoing colonial nature of the institutions they work in and how Indigenous Peoples may not feel they can refuse services without negative repercussions, like involvement of child and family services. Participants shared the importance of respecting self-determination of Indigenous Peoples when considering assessment. Participants expressed when services and assessment choices were led by Indigenous Peoples it could be a culturally safer process.
Throughout data analysis we realized that the emerging themes were interwoven, impacted one another, and we could not silo them as we discussed our findings without losing meaning. Guided by Indigenous team members and an intention to respect of the stories shared, we decided to present findings using a composite narrative in a conversational style. The conversation style reflects the relational approach central to Indigenous methodology, honoring orality as method of gathering knowledge through dialogic participation and maintaining a collectivist tradition (Kovach, 2021). Composite characters align with this approach by preserving the context and emotion of the stories, while supporting participant anonymity (Willis, 2019).
What follows is a fictional conversation between a composite character based on participant data and Pamela. The perspective of the occupational therapist represents quotations, ideas, and concepts that arose throughout the surveys and storytelling groups. Pamela's perspectives are from the conversation with the student researchers when presenting her with study findings. All italicized words are direct quotations. In some places they have been edited for clarity without changing meaning. Non-italicized sections are paraphrased information from the participant data or from conversations with Pamela. Presenting the findings in this manner allows us to incorporate and centre key teachings from Pamela that informed the research team throughout our process.
Summarized Presentation of Themes: An Indigenized Storytelling Approach
Mary is an occupational therapist who is currently working in an urban community-based centre and who worked rurally in a past position as a new graduate. Mary is a white, cisgender female of mixed European settler ancestry. She experiences complex barriers to culturally safer occupational therapy assessment with Indigenous Peoples. Following proper protocols, Mary meets with Pamela for guidance.
Mary: All of our current systems are based in white colonialist processes…It would almost take dismantling the entire healthcare system to be truly culturally safe. It seems like you can advocate as hard as you can. You can develop these relationships, and [Indigenous Peoples will] trust you, but then that just gets slammed down by the systems because we still have a lot, and I mean a lot, of work to do to address this. And I feel the pressure, especially in a hospital, to do standardized cognitive assessments. I hate standardized tools. There are no human beings that fit a standardized tool particularly well. Standardized assessments pretend to be neutral and value-free and culture-free, but that's an impossibility, because we're humans, living in human ecosystems.
Like one day, a physician was asking me to do an MoCA (Montreal Cognitive Assessment) 3 with an Indigenous person and she was like, “I need this MoCA done. I'm getting a geriatrician to consult, and it needs to be done.” And I was like, “It's not happening. I don't know what to tell you.” She was absolutely livid. And this was my first-year practicing as an OT, and I was called into my manager's office… and they sat me down and they were like, “look, you've been reported to HR…” I’ve heard some of my colleagues say they would try the Indigenous MoCA 4 … I think there's an older version, and one for Coastal First Nations too. But I’ve seen the Indigenous MoCA, and it's very surface level. Like you change the animals to be animals that Indigenous people recognize more and then you call it a day. I disagree with the idea that you can just paint a layer of Indigenous trimmings on it, and then it's going to be a relevant assessment…The foundation is still Western. Honestly, I’ve found observation of occupations in a real-life context is the best way to learn about how people are doing; however, this isn’t always respected by my colleagues or the systems where I work.
Pamela: I agree that colonial healthcare systems are a major issue when it comes to access for Indigenous Peoples. I think that part of the challenge in accessing services is that I feel like I have to prepare myself, be ready to deal with all these western colonial ways of doing things. It requires me preparing myself mentally and emotionally just to cope with it. [There's a] set standard as you walk in the door that just doesn’t fit. I truly often feel like an outsider in the healthcare system. Some of it is built into the way interactions are done and handled from a Western perspective but doesn’t always land well in Indigenous communities. Over time I would like the medical community to find ways to bridge that gap.
Mary: It's so hard because how can we decolonize a colonial institution? How can we make our healthcare system an inclusive and accessible space for Indigenous Peoples? One thing that I’ve been telling myself is that it's the relationship I create with people. And if I can't create that relationship, then the assessment isn't going to work. My workplace has offered some virtual cultural safety training, but it's not enough- I’m still not confident in how I take what I’ve learned there into making assessments less oppressive, less traumatic. I think it's necessary for occupational therapy school and workplaces to have mandatory education on Indigenous history, cultural safety, and antiracism, and to teach us how to combat the pressures to do standardized assessments.
Pamela: That's true. It comes right back down to trying to really make that human-to-human connection with people. And just how important that is, in setting the tone for moving forward. Those initial conversations, just how you approach someone right from the very beginning is really important. Because if it's super professional and not human, you're not gonna likely get very far.
Mary: Yes! Everything is a product of the relationships in which it's created. It's like don't even start with the interview or the pencil. Start with the “I'm a human. You're a human. Where are we together?” Some things I’ve been trying to do during assessment is to be reflective, empathetic, and authentic in my practice. I think [authenticity] is absolutely critical in our practice. And I mean it's just like making mistakes left and right, owning up to them, and then moving on and learning from them. I use humor a lot, and that seems to work for me too. I think the personal approach that OTs take is really important. And what you said about not being super professional, I’ve found it seems to help when I’m relaxed and acting authentically, like myself—not trying to be this “perfect” OT.
Pamela: Along similar lines sometimes, there is a strong attitude of others being the experts… as a client, you're not encouraged to question and get clarification… And I think, for many of us as Indigenous people, that is a trigger. Because you, the health professional, have some expertise, for sure. But, in order to get the best out of that relationship…It's a partnership and if you don't have both parties engaged then there's a limit to how far you can go. So, when any kind of a healthcare professional is focusing on their agenda. Right then, it just overrides all of that. And then for me, how am I going to be the next time I need to meet with my nurse practitioner, or doctor, or whatever, when I've felt…this kind of control way of handling things. With a message that “I'm clearly in control, as the nurse practitioner or doctor, and I will withhold your prescriptions until you comply and be a good patient.” For me, that's just a trigger. Instead of taking a more holistic approach, and maybe trying to have a better sense of why I am not rushing in.
Mary: That is a good reminder that I'm not the expert on what your life looks like and what your background is…. I am a very privileged white person, who has experienced very little discrimination in the grand scheme of things. I have no clue what you have gone through.
Pamela: I think your awareness of OTs not being the experts on Indigenous Peoples’ lives is a step towards better resolution…in at least starting to recognize that there is this gap, or whatever it is, right? I think that's the first step, recognizing it. Sometimes, it takes a long time to get to that place of just recognizing. But we cannot make change without awareness first.
Mary: Yeah, you are right, awareness is the first step…Something else I wanted to ask you about, is this tension that I’m seeing recently, where families will consent to services for their children, but seem disengaged or disinterested in collaboratively setting goals and a therapy plan. [It seems like] many families simply don't have the time or capacity to heavily involve themselves in therapy but still want to make sure that their child receives the services that they need. I think that this sometimes leads to a “willingness” for [healthcare providers] to be involved, without a true consent in a way that respects their values and other commitments.
Pamela: Well, I think this is closely tied to the history of healthcare providers acting like the experts, and not respecting Indigenous Peoples’ Rights, which we discussed earlier. And that belief that they have the right to just override everything is alive and well, you know? It's like let's not lose sight of it's my health, and it's my body, and there might be the best drug in the world, but I might have reasons [not to take it]. It's still my body. You know the whole reason that the government were able to conduct experiments on our children. It's that whole idea that we are not in control of ourselves, our destination, our lives, anything. And it is possible that the families you work with who seems to you as if they are disengaged—might not feel like they have many options since there are so many barriers to even accessing care. I often want to say—You have no idea the crisis I put aside to make sure to come to this appointment, or the crisis that caused multiple cancellations…most of the time there isn’t going to be communication about it, especially in a setting where you are feeling so judged.”
Mary: Hearing you say that makes me realize that I need to examine my own biases more. I am constantly thinking about—how I can decrease that power imbalance. I’m trying some things, like being as flexible as possible by providing choice and ensuring they know that they are in control…explaining in depth the purpose of the assessment and what [I] will be doing, offering clarification, giving space for questions, and ensuring they fully understand the task at hand. I’ve started to ask some people if they would like a cultural liaison present for our sessions.
Pamela: Yes, and I think it would be especially important [to] work with [your] client in really trying to help them understand the [healthcare] system better…I think for a lot of us it might be a place where we're more in a deficit because we have just been administered to on a very, take it or leave it kind of basis. Because of that, we may not be as familiar with the system overall. Again, after all, don’t forget, it's my body.
Discussion
This study explored perspectives of occupational therapists on the challenges they face during assessment with Indigenous Peoples and their current assessment strategies used in pursuit of increased cultural safety. Our findings revealed three emerging, interconnected themes.
Overall, participants perceived multiple system level pressures as a barrier to culturally safer assessment processes. In response, participants reported seeking Indigenized versions of standardized cognitive assessments (e.g., CICA, Indigenous versions of the MoCA), but presented varying opinions about the appropriateness of such tools. These tools may still be grounded in western, colonial values and further research is needed on the appropriateness of these Indigenized versions within occupational therapy practice (Price & Pride, 2023; White & Beagan, 2020). There was no consensus among participants of what a culturally safer assessment approach entails and how standardized assessments fit into this approach; however, participants overwhelmingly preferred occupation centred, nonstandardized assessment approaches when possible. We agree with participants who expressed concern regarding external pressures asserted upon therapists to complete standardized assessments. Emerging interprofessional research is demonstrating that inappropriate use of standardized assessments can cause harm to Indigenous service users (Jacklin et al., 2020; O’Connell et al., 2021, 2022; Ouellet et al., 2022). This pressure also potentially undermines occupational therapy professional autonomy and reasoning on assessment practices.
This research reinforces the importance of relationship building and authentic connection throughout the assessments process. Participants report improved outcomes for Indigenous service users when they were able to draw upon their core occupational therapy values and skills through relationship building, authentically listening to the Indigenous service user, and centring them and their meaningful occupations in the practice process. This aligns with Bauer and colleagues (2022) scoping review of Indigenous Peoples and occupational therapy practice, research, and education in Canada, commenting on the need for occupational therapists to actively dismantle systemic barriers that exist for Indigenous Peoples in colonial healthcare institutions to build authentic partnerships in practice.
Participants desired to practice in a manner that supports culturally safer interactions and facilitates participation in meaningful occupation; but experienced substantial, complex resistance from others in systems and institutions in doing so. Our study revealed that when occupational therapists solely viewed themselves as experts, it was harmful to the assessment process. They felt unprepared from their entry to practice occupational therapy programs to challenge these complex, systemic barriers. The participants in this study had, instead, developed a level of expertise in working respectfully and collaboratively with Indigenous service users through learning from Indigenous Peoples. They unlearned much of what was taught to them in academic programs about evidence-based practice and the role of standardized assessments in their occupational therapy practice.
Many participants identified the importance of power-sharing, recognizing that Indigenous service users are the expert in their own lives. Participants suggested mandatory Indigenous history, colonization, cultural safety, and antiracism education in occupational therapy curriculum and workplaces. This echoes TRC Call to Action #24, which calls for mandatory antiracism and cultural competency training for health care providers (TRC, 2015). Indigenous health researchers such as Ouellet and colleagues (2022), have also indicated the importance of healthcare providers having background understanding of Indigenous Peoples’ history, their culture, and their present day lives to support therapeutic relationships.
Pamela highlighted that health professions have little understanding of the harms caused by colonial systems, including the healthcare system, which often fails to provide a comfortable space for Indigenous Peoples to share their experiences. Indigenous Peoples report barriers to accessing health professions services caused by racism, judgment, and communication issues (Allan & Smylie, 2015; Boivin & MacLachlan, 2019; In Plain Sight, 2020) While participants’ personal reflection on the lack of their expertise on Indigenous experiences is crucial, addressing the inherent service provider–service receiver power imbalance also calls upon systemic change from a broader professional level (Bauer et al., 2022).
The complex nature of consent during assessment emerged when participants queried if true consent is obtainable within colonial systems. In an OT Now article, Lisa Boivin, a Dene woman, reported her experiences as a young mother who had lived through the Sixties Scoop consenting to medical services, while fearing of her child being taken away (Boivin & MacLachlan, 2019). Similarly, Pamela's story reveals when she had to defend the right to her own choices around her body and when healthcare providers pressured her to accept health services that did not align with her values. This power imbalance can reinforce feelings of powerlessness while receiving occupational therapy services (Boivin & MacLachlan, 2019). This may result in Indigenous service users being fearful of the repercussions of refusing recommended assessments. Given the historical harmful impact of health and other professionals on Indigenous Peoples, occupational therapists need to address the power imbalance and the difficulty they might experience enacting their rights to consent to assessments in a colonial system.
Limitations and Indications for Further Research
This study is an important first step in documenting the experiences of occupational therapists who are attempting to practice in a culturally safer manner with Indigenous Peoples. Our occupational therapy participants were primarily settlers. Our participants are presumed to be largely reflective of the occupational therapy workforce which is overwhelmingly of settler origin; however, this data is not currently collected by most regulatory colleges or professional associations in Canada and there is no reliable data on such. One critically important perspective missing is the experiences of Indigenous occupational therapists. Further research of their perspectives and experiences should be led by Indigenous occupational therapy scholars and clinicians. This project did not seek the perspectives of Indigenous service users, due to our 18-month project timeframe, which did not allow for adequate relationship building and reciprocity needed to complete research in an ethical manner. Future research is needed from Indigenous occupational therapy service users, in a way that prioritizes relationships and reciprocity. Additionally, while career long learning is expected as an occupational therapist, our findings indicate that there is a need for Canadian academic entry to practice programs to consider how much of the educational burden of (un)learning is being placed on Indigenous communities and the individual therapists. Therefore, future research could explore how entry to practice occupational therapy programs are preparing students for culturally safer assessment practices and how to incorporate recommendations of occupational therapy clinicians in assessment curriculum.
Conclusion
Occupational therapists in Canada are required to “act on situations and systems of inequity and oppression within their sphere of influence,” which include occupational therapy assessment practices (ACOTRO, ACOTUP, & CAOT, 2021, p. 13). Research on this topic is intended to help decrease the disproportionate health inequities that Indigenous Peoples face (Kim, 2019; Young et al., 2013). Currently, occupational therapists are facing systemic barriers to conducting culturally safer assessment with Indigenous Peoples. These barriers are resulting in challenges for occupational therapists when building relationship with Indigenous Peoples and leave many occupational therapists unsure whether they are gaining informed consent throughout their practice process. Despite systemic pressures towards efficiency and standardized approaches, occupational therapists are attempting efforts towards culturally safer assessment by advocating for occupation-based, culturally relevant, and flexible assessment processes that respect the autonomy of the Indigenous service recipients.
It will take a committed, comprehensive response from the occupational therapy profession—educators, researchers, leaders, and clinicians—to further understand and respond to the multiple barriers presented by these participants when striving for culturally safer practice. Clinicians require resources and evidence to support their professional reasoning and professional autonomy in the face of systemic pressures such as limited time; colonial consent policies; pressure from interdisciplinary colleagues; and processes that prioritize standardized assessments at the expense of culturally safer outcomes.
Supplemental Material
sj-docx-1-cjo-10.1177_00084174251336547 - Supplemental material for Occupational Therapists’ Experiences of Assessments With Indigenous Peoples: A Storytelling Approach
Supplemental material, sj-docx-1-cjo-10.1177_00084174251336547 for Occupational Therapists’ Experiences of Assessments With Indigenous Peoples: A Storytelling Approach by Kaarina Valavaara, Jay MacDonald, Pamela Barnes, Emilie Bourque, Sierra Rowe and Tal Jarus in Canadian Journal of Occupational Therapy
Footnotes
Occupational therapists are facing systemic barriers to culturally safer assessment practices, which negatively impacts their ability to build trusting relationships with Indigenous Peoples grounded in informed consent. Occupational therapists feel unprepared from their entry to practice education on culturally safer assessment approaches, including skills in challenging systemic pressures. Research on occupational therapy assessment practices with Indigenous Peoples needs to be done collaboratively and in a way that ensures reciprocal benefit to Indigenous Peoples.
Acknowledgments
We would like to acknowledge the contributions from and collaborative work with Pamela Barnes, and our community consultants: Caitlyn Debruyne, Carmen Gendron, Molly Flindall-Hanna, Monique Lizon, and Elizabeth Pooley.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received funding through a Scholarship of Teaching and Learning Grant from the UBC Institute for the Scholarship of Teaching and Learning to support the publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.