
Abstract
Introduction
Individuals around the world have witnessed the findings of thousands of unrecovered graves of children who died in Canada's residential schools. From the mid-19th century until the last school closed in 1996, the Canadian government implemented policies attempting to (1) eliminate Indigenous Peoples’ governments, rights, and treaties and (2) through the process of assimilation, cause Indigenous Peoples to cease to exist as distinct peoples (Truth and Reconciliation Commission [TRC], 2015). In 2008, the Truth and Reconciliation Commission of Canada was established due to a class action lawsuit between the residential school survivors, the Government of Canada, and the churches running these schools. The TRC culminated in a final report outlining 94 Calls to Action essential for reconciliation with Indigenous Peoples in Canada (TRC, 2015). Several of the Calls to Action directly relate to health care, including increasing the number of Indigenous healthcare professionals, and providing culturally safer and trauma-informed education to address the ongoing impacts from intergenerational trauma wrought by residential schooling.
Indigenous Peoples in Canada continue to experience widespread health inequities in large part due to Canada's colonial history and the resulting inequities in the social determinants of health (Greenwood et al., 2015). Since the early days of colonization, a rapid decline in the overall health of Indigenous Peoples has been well documented by researchers and governments (Royal Commission of Aboriginal Peoples [RCAP], 1996; Reading & Wien, 2009; TRC, 2015). Access to health services is another significant concern for Indigenous communities in Canada, limited by socio-economic inequities, geographic location, lack of suitable staffing and infrastructure, language and cultural barriers (National Collaborating Center for Aboriginal Health [NCCAH], 2011), and experiences of individual and systemic racism (Allan & Smylie, 2015). Despite deliberate assimilation, genocide, and ongoing acts of colonialism, Indigenous Peoples have continued to live and thrive while reclaiming their own distinct culture, language, and ways of knowing. Indigenous Peoples continue to resist colonialism by asserting and protecting their human and treaty rights.
Occupational therapists in Canada must position themselves to respond to the Calls to Action and engage in the process of reconciliation: They can play a role in advancing Indigenous Peoples’ health via advocating for and applying culturally safer practices and policies on a local, provincial/territorial, and national level (Canadian Association of Occupational Therapists [CAOT], 2018a; Restall et al., 2016). However, to realize the potential of occupational therapists to engage in reconciliation, the profession must first examine, critically reflect, and change the ways our espoused core beliefs reflect Eurocentric values (Jull & Giles, 2012) and roots (Hojjati et al., 2018). Seminal occupational therapy theoretical frameworks and models are poorly suited to address Indigenous health and wellness as they impose a Western settler-colonial worldview (Fijal & Beagan, 2019; White & Beagan, 2020).
As one step towards reconciliation, the first unified set of competencies for all occupational therapists in Canada was released in November 2021 (Association of Canadian Occupational Therapy Regulatory Organizations [ACOTRO], Association of Canadian Occupational Therapy University Programs [ACOTUP], and CAOT, 2021). The document highlights a new domain acknowledging the presence and impact of racism in Canada, specifically stating that occupational therapists are expected to “identify the ongoing effects of colonization and settlement on occupational opportunities and services for Indigenous Peoples” (ACOTRO, ACOTUP & CAOT, 2021, pg.13). This competency indicator represents a critical step towards addressing knowledge and behaviour gaps related to Indigenous health and health services, placing the onus on occupational therapists and the profession at large to take action. Individually and collectively, occupational therapists must be accountable for responding to the TRC Calls to Action to engage the profession in ongoing reconciliation (Restall et al., 2016).
Study Purpose and Rationale
To inform responses to the TRC Calls to Action, it is important to identify the knowledge gaps of occupational therapists in relation to Indigenous health on both individual and system levels. The overarching aim of this research is to understand the present knowledge of occupational therapists regarding Indigenous health, identify steps to address knowledge gaps, and to inform responses to the TRC from the profession. To accomplish this goal, the research team undertook a three-phase approach of (1) literature review (Jacek et al., 2022), (2) seeking consensus from occupational therapists with membership in an Indigenous health network (Jacek et al., 2022), and (3) the development and implementation of a national survey of occupational therapists to determine knowledge gaps in relation to Indigenous health. This paper reports on the survey development process and survey findings.
An empirical understanding of the current knowledge of practicing occupational therapists will contribute to the growing body of literature within the profession related to occupational therapy and Indigenous health in Canada (Bauer et al., 2022; White & Beagan, 2020). Since the inception of this project in 2018, there has been a substantial increase of published research in this area (Bauer et al., 2022). However, there has not been a study identifying the present knowledge gaps of occupational therapists in Canada.
Methods
The research team is composed of white settler-descent occupational therapists and acknowledges that this positionality and privilege inherently bias the research process due to a lack of Indigenous representation. The research team practiced reflexivity individually and collectively to attend to this bias throughout the research process and continues to be committed to ongoing learning and purposeful professional development. In addition, the researchers completed the Tri-Council Policy Statement: Ethical Conduct for Research Involving Human Course on Research Ethics including the module on Research Involving the First Nations, Inuit, and Métis Peoples of Canada to support ethical research conduct. As a group, the team acknowledges that our ability to explicitly engage in a critical examination of positionality has grown throughout the research process in alignment with the advancement of knowledge and research within occupational therapy related to justice, equity, diversity, and inclusion. As this project lacks Indigenous authorship, a seminal element involved gathering and implementing feedback from the Occupational Therapy and Indigenous Health Network (OTIHN) through completion of a Delphi consensus exercise to validate and prioritize themes in preparation for survey item generation; this has previously been reported (Jacek et al., 2022). The study received approval from the local ethics board (Hamilton Integrated Research Ethics Board [HiREB] #4150).
Survey Development
Survey research is an ideal form of generating understanding of the knowledge, attitudes, and beliefs of a group, gathered from a representative sampling frame (Phillips et al., 2021). While it has been criticized for the potential to be highly influenced by researcher bias, literature synthesis and expert review during survey development can mitigate such bias (Burns et al., 2008).
The research team implemented a concurrent mixed methods survey (Creswell, 2014). The researchers acknowledge the critiques of this method, specifically the lack of consensus on the definition of mixed methods research, and often, the inferiority of qualitative findings (Mortenson & Oliffe, 2009). Despite this, the researchers chose to use this method because fixed choice and open-ended questions add precision to words and descriptions while creating space for comments to enrich the summary statistics with nuanced explanations of diverse perspectives (Johnstone, 2004). Survey questions were generated by using the priority themes confirmed by the Delphi method (Jacek et al., 2022) in conjunction with the "Profile of Practice of Occupational Therapists in Canada" (CAOT, 2012). Specifically, the Profile was used as a framework, with the competencies as the headings under which survey questions were organized (see Supplemental File A).
The survey was constructed using LimeSurvey, an anonymous internet-based survey platform hosted on a secure server at McMaster University. Multiple choice questions were used to assess knowledge gaps, including both positively and negatively worded questions using Likert scaling for agreement and frequency scaling for behaviours. The survey also included open-ended questions and areas for additional comments to capture individual attitudes, beliefs, and experiences. A draft of the survey was approved by HiREB prior to pilot testing for usability. Overall, the survey consisted of 11 demographic questions, followed by 20 main survey questions (see Supplemental File A). The questions were developed based on the priority themes established in a Delphi consensus exercise (Jacek et al., 2022); three questions were developed for each theme in the highest priority tier, two questions were developed for each theme in the second priority tier, and one question was developed for each theme in the lowest priority tier. See Jacek et al. (2022) for further detail on the weighting of questions based on priority themes. These questions were then reorganized and presented to respondents using the headings from the Profile (CAOT, 2012).
Pilot Testing
The survey was pilot tested with six key informants who were clinicians and researchers representing members (3) and non-members (3) of the OTIHN to receive feedback regarding the usability and readability of the survey. Informants were recruited through targeted emails. The research team reviewed responses and edited both the formatting and content of the survey based on feedback. Question order was randomized as it was postulated that this may influence survey completion. Specifically, informants highlighted that a respondent may be unlikely to complete the survey should a question using the term “genocide” appear too early in the survey. Therefore, the Profile headings were evenly divided into two sections. The first section to appear to any respondent was randomly assigned, while the question order within each section remained fixed. Additionally, an informant identified the inherent interconnectedness of the themes as a consideration for survey analysis.
Respondents
The online survey was intended to be completed by occupational therapists across Canada. The primary inclusion criteria were (a) an occupational therapist in Canada and (b) voluntary participation. The primary exclusion criterion was lack of proficiency in English, as only an English version of the survey was available due to time and resource limitations.
Data Collection
The online survey was posted on the CAOT Research Listing webpage and completed by occupational therapists across Canada. A link to the research webpage was available on weekly CAOT membership emails, though membership was not required to access this part of the website. Recruitment further employed snowball sampling, relying on respondents to recruit other potential respondents through their networks (Parker et al., 2019). The research team contacted representatives at provincial and territorial occupational therapy professional associations to request access to a member registrant list for survey distribution; the research team only received a list for British Columbia, with no responses from other provincial associations despite multiple attempts. A follow-up reminder email to complete the survey was sent to available contacts within 2–3 weeks of the first recruitment email, including British Columbia registrants and colleagues initially contacted by the researchers. A survey link was shared on the research team members’ social media (Twitter) and professional platforms (LinkedIn). The survey remained available for 13 weeks.
Data Analysis
This mixed methods survey had an overarching qualitative focus. Quantitative survey data was analyzed using descriptive statistics for demographics of respondents and to highlight trends in the knowledge-based questions. Percentages were rounded as whole numbers to facilitate readability, and therefore may not sum to 100. Qualitative data was analyzed using inductive thematic analysis within an interpretive description approach, starting with a theoretical “scaffold,” and then iteratively expanding to a deeper thematic analysis driven by the data (Thorne, 2008).
In selecting a theoretical scaffold, the researchers sought a model addressing culture in occupational therapy practice, as the objective of the research is understanding the knowledge gaps related to Indigenous health in occupational therapy practice. In selecting a model, the research team acknowledged the ongoing evolution of the occupational therapy discourse to a focus on cultural humility and critical reflexivity (Beagan, 2015). However, at the time of engaging in the research process, the researchers were unaware of any model in occupational therapy for cultural humility and critical reflexivity. The researchers further acknowledge that a focus on culture is limited in capturing the broader systemic influences on Indigenous health, including colonialism. Despite these limitations, the Culturally Responsive Caring in Occupational Therapy model (Muñoz, 2007) was chosen as the theoretical scaffold to organize overarching themes and subthemes derived from the data. This model is comprised of five main components related to direct clinical practice that are situated within one component representing environmental factors (see Figure 1). Iterative analysis of the data through an interpretive description approach permitted findings to extend beyond the concepts captured in this theoretical scaffold, including those related to power relations and colonialism.
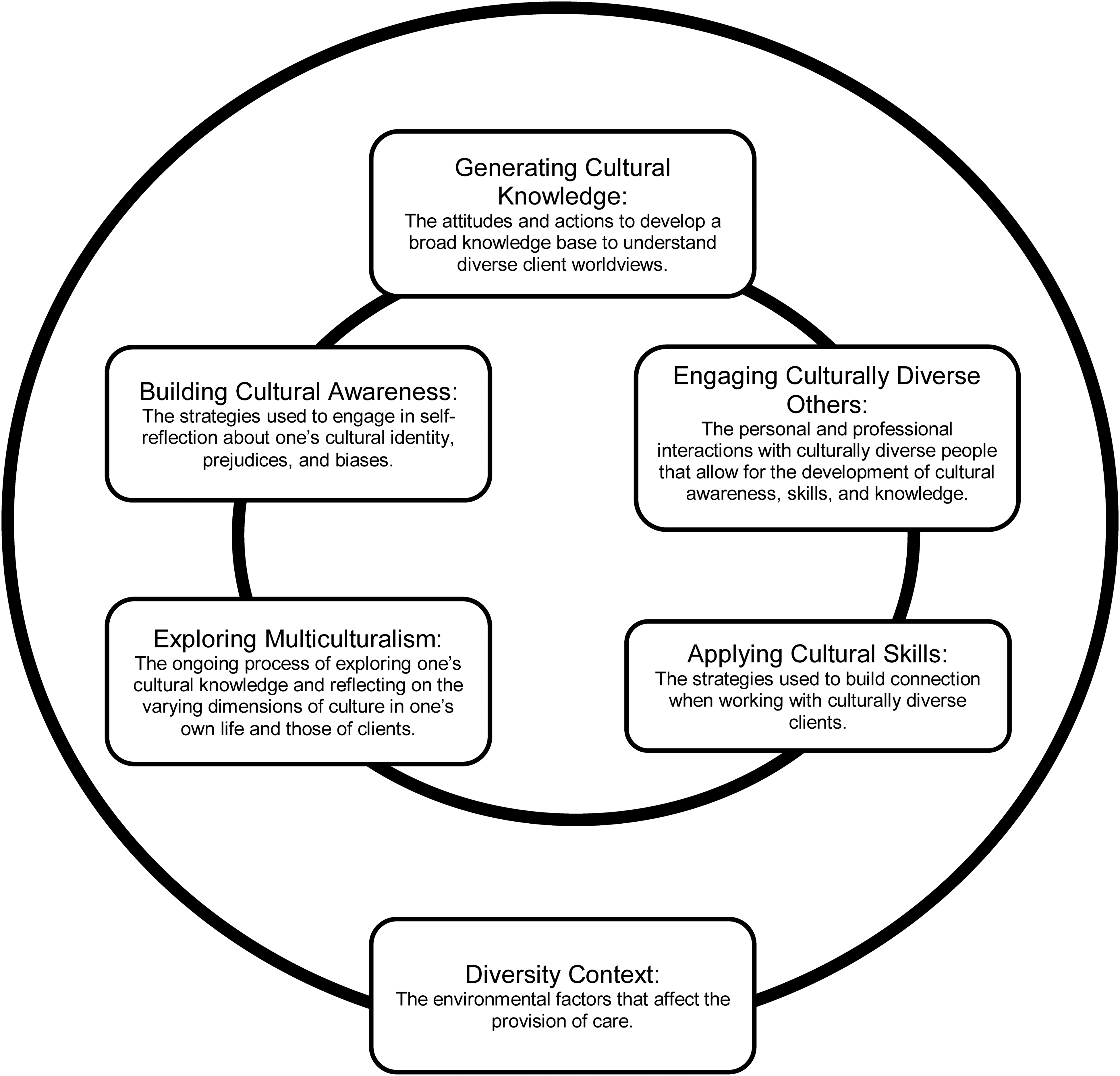
Culturally responsive caring in occupational therapy model, adapted from Muñoz (2007).
Findings
Demographics of Respondents
The survey yielded 364 total responses, with 300 complete responses and 64 incomplete responses (46 partially complete, 18 containing no data). There were survey responses from all provinces and territories, except for the Yukon. The majority of respondents were from Ontario and British Columbia, with only one respondent from New Brunswick; see Table 1 for distribution of survey respondents compared with registered occupational therapists for each province/territory. There was a wide variety of respondent ages, practice years, client populations, and practice contexts and locations (see Table 2). The survey was intended for self-identified practicing occupational therapists; a single response from a retired therapist was also included. The majority of respondents (83%) identified their ethnicity as Caucasian, whereas 2% identified as Indigenous; see Table 2 for full demographic details.
Provincial and Territorial Distribution of Survey Respondents Versus Supply of Occupational Therapists in Canada (2019)
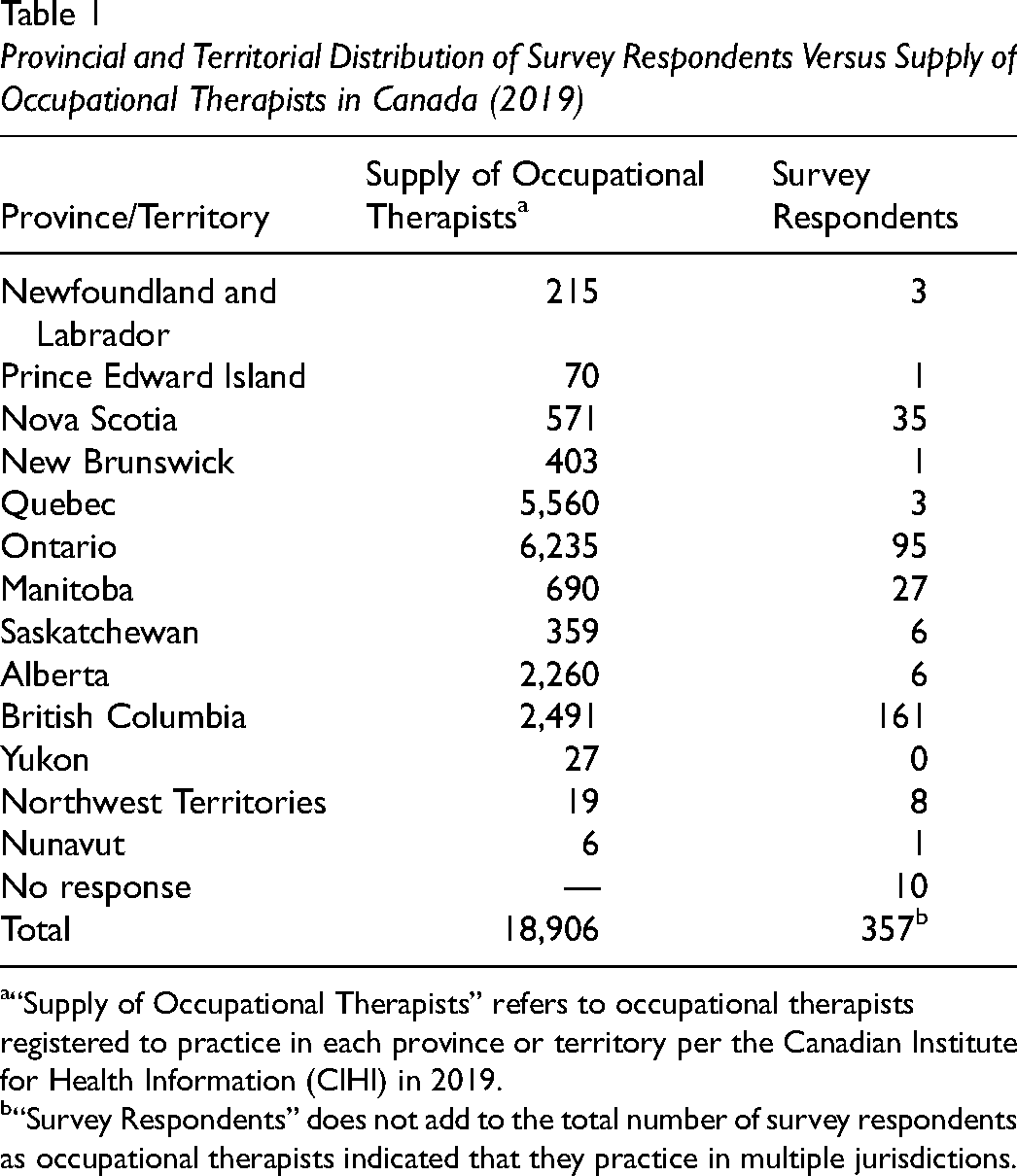
“Supply of Occupational Therapists” refers to occupational therapists registered to practice in each province or territory per the Canadian Institute for Health Information (CIHI) in 2019.
“Survey Respondents” does not add to the total number of survey respondents as occupational therapists indicated that they practice in multiple jurisdictions.
Participant Composition Table
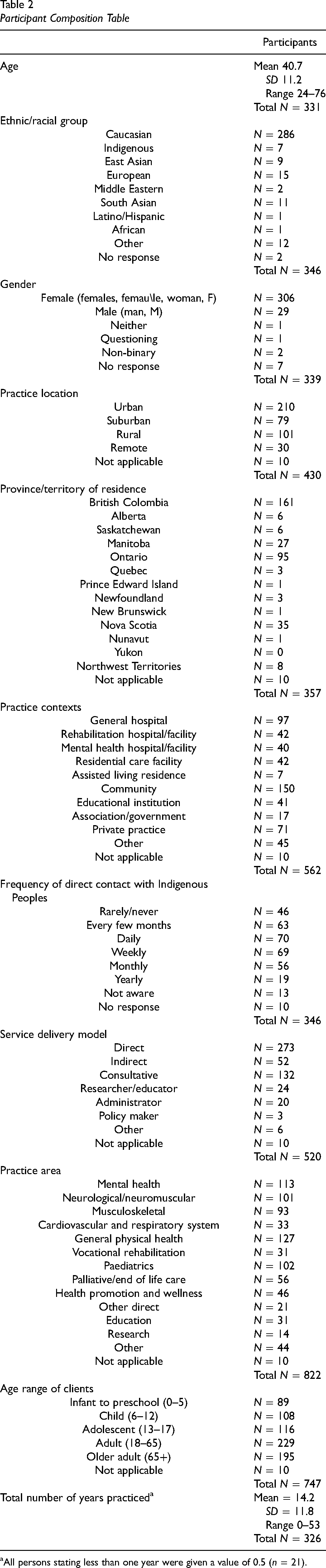
All persons stating less than one year were given a value of 0.5 (n = 21).
Knowledge Gaps
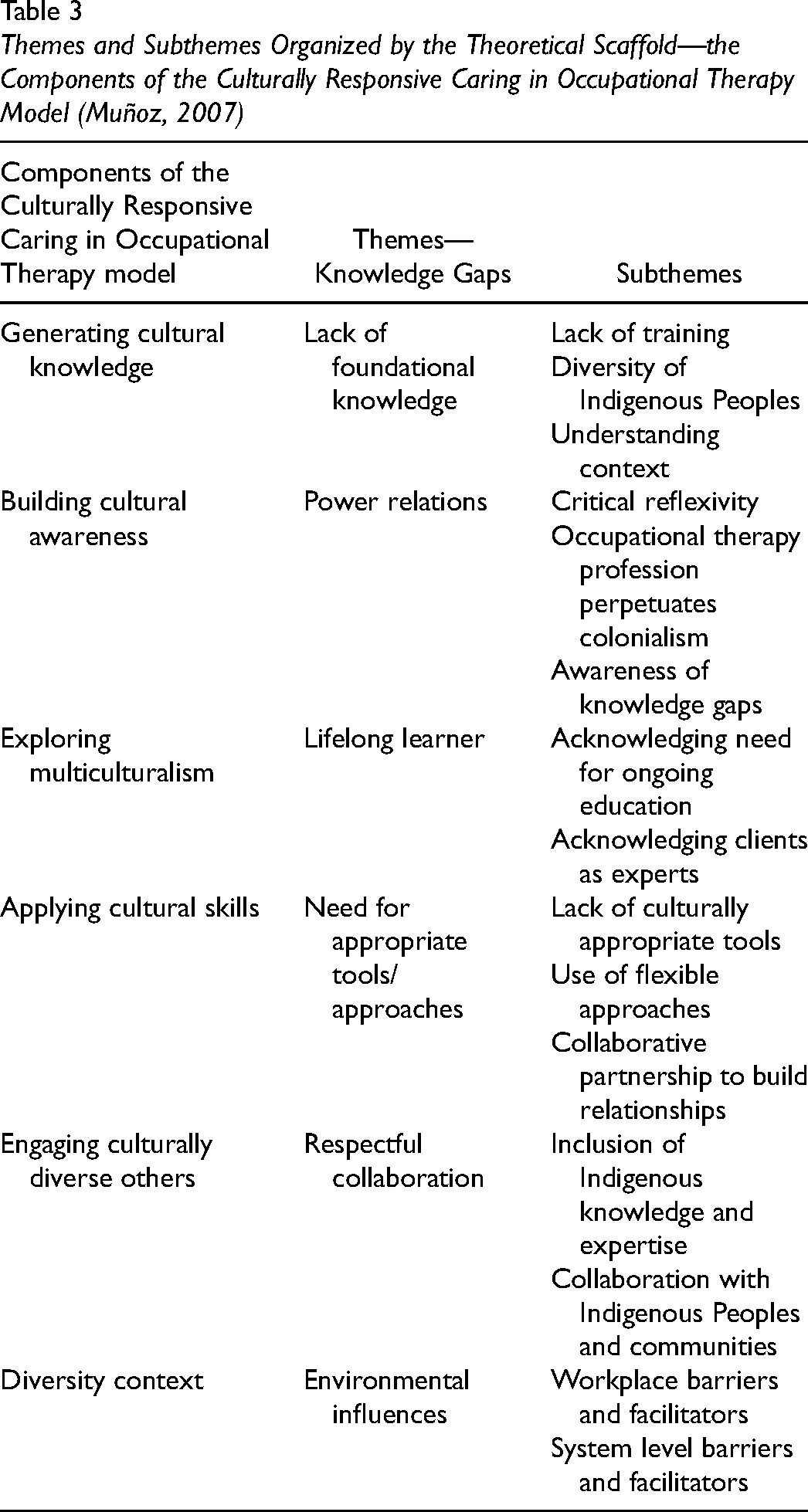
Six overarching knowledge gaps were characterized through data analysis and organized using the above model (Muñoz, 2007) as a theoretical scaffold. Each of these six knowledge gaps represents themes which are further composed of unique subthemes (see Table 3). See Supplemental File B for Frequency Table.
Themes and Subthemes Organized by the Theoretical Scaffold—the Components of the Culturally Responsive Caring in Occupational Therapy Model (Muñoz, 2007)
Knowledge Gap #1: Lack of Foundational Knowledge
The first knowledge gap identified includes a lack of adequate training, lack of acknowledgment of the diversity of Indigenous Peoples in training, and lack of awareness of the historical and contemporary impact of colonialism.
Lack of Training
Respondents described having taken training of various formats and content (e.g., cultural competence versus cultural safety training). A total of 58% of respondents reported that they had completed training related to Indigenous health: 17% of these respondents accessed this training outside of their workplace. Respondent 113 expressed that “unfortunately the course was voluntary, as I felt some of my colleagues could have benefited from it.” Additionally, 48% of respondents who had completed training indicated their training was 1–10 hours in length, with an additional 13% indicating the training was under 1 hour.
Diversity of Indigenous Peoples
Respondents stated that Indigenous Peoples are diverse, and knowledge cannot be generalized. For example, “Indigenous peoples are not a homogeneous group” (respondent 250); and “there is no ‘one’ Indigenous culture, of course” (respondent 264). Many respondents desired training and formal learning opportunities to address the unique practices and traditions of local Indigenous Peoples. However, many of the training opportunities reported by respondents were pan-Indigenous, and respondents found this difficult to apply to their local context.
Understanding Context
Respondents identified the need to be aware of the historical and contemporary impact of colonialism and highlighted the importance of understanding the impact of social determinants of health for Indigenous clients. Respondent 43 stated that they “try to consider the impact of colonialism on relationships with Indigenous peoples and recognize that difficulties with rapport building may arise from power imbalances or abuses of power that relate to our colonialist history.” Additionally, 55% of respondents reported that they were not aware of the health and education-specific recommendations presented by the TRC, while 32% indicated they were aware of these specific recommendations.
Knowledge Gap #2: Power Relations
The second theme identified the need to use critical reflexivity to bring awareness to the influence of unconscious biases in one's own practice and the underlying assumptions within the occupational therapy profession perpetuating colonialism.
Critical Reflexivity
Respondents indicated the need to use critical reflexivity to examine the occupational therapy profession and the ways in which it reinforces power imbalances. Respondents further reported an ongoing need to reflect on their own biases and privilege, including being aware of how their unconscious biases may influence their practice. Respondent 250 posited “a single solution for all is further colonialism. Good OT is meeting each individual where they are, placing our options and biases outside of our work.” Furthermore, 81% of respondents indicated that they were aware of the position of power they hold within the healthcare setting when working with Indigenous clients.
Occupational Therapy Profession Perpetuates Colonialism
Respondents reported the need to reflect on the values and assumptions underpinning the theories and practice tools in occupational therapy in Canada. “We are at a critical juncture in terms of exploring how much of us are a product of colonialism and how we perpetuate it, versus being part of the healing” (respondent 302). Respondents were asked if they believed that occupational therapy, based on mainstream cultural norms and practices, contributes to the ongoing cultural genocide of Indigenous Peoples through colonialism: 36% supported this statement, 28% indicated that they do not believe this statement, and 36% of respondents indicated a neutral response.
Awareness of Knowledge Gaps
Respondents differed in how they recognized and addressed their knowledge gaps when working with Indigenous clients. Some respondents described treating all clients the same regardless of their culture. Respondent 343 stated “I don’t believe there is a power dynamic. I treat all people equally.” Other respondents stated that they always practiced in a client-centered way, and by doing so, they were doing enough to address culture in practice.
Knowledge Gap #3: Lifelong Learner
There was an acknowledgement that occupational therapists must not become complacent with their current state of knowledge, in order to remain a competent clinician.
Acknowledging the Need for Ongoing Education
Respondents identified the need to attend ongoing education related to Indigenous health. A total of 58% of respondents agreed or strongly agreed to feeling confident in advocating for increased training for practitioners to work in culturally appropriate ways. Respondent 9 stated “Our workplaces need to be prioritizing this kind of training in both health and education.” Respondents identified continuing support and guidance from national and provincial occupational therapy bodies helps to provide direction and formal opportunities to address their knowledge gaps and support lifelong learning.
Acknowledging Clients as Experts
Respondents acknowledged occupational therapists should avoid making unexamined assumptions about a client's culture and the influence it has on their occupations and should strive to be curious and learn from each client's unique perspective. Respondents noted that clients are experts in their own lives and wellness. Respondent 290 stated “I approach each client with humility and inquisition of understanding their world and their struggles. [. . .] I describe my role as an OT as being a partner, with client as expert.”
Knowledge Gap #4: Need for Appropriate Tools/Approaches
The fourth knowledge gap identified needing to incorporate appropriate strategies and to build collaborative partnerships with an intentional respect for a client's culture.
Lack of Culturally Appropriate Tools
Respondents reported the need for culturally appropriate tools and the importance of choosing not to use standardized tools with Indigenous populations due to the inherent bias of these tools and measures. Respondent 128 stated “I tend to not use standardized assessments unless totally necessary because they aren’t appropriate for on-reserve clients in remote communities. [. . .] We need better assessment tools.” When asked if respondents think that there are currently sufficient culturally appropriate tools (e.g., theories, models, and assessment measures), less than 1% stated yes, 59% stated no, and 40% stated that they did not know. Respondents stated that it was important to use a critical lens when choosing to use or not to use a specific tool in practice; for example, “I rely more heavily on development of rapport, and clinical observations” (respondent 278).
Use of Flexible Approaches
Respondents shared a variety of flexible approaches that they implement to build culturally safer relationships with clients, including flexibility in meeting location, using strength-based approaches, and not using a formal or professional title. For example, respondent 42 stated “I allow for flexibility for any visits I book, [. . .] so that I may have time for more conversation with clients/caregivers.”
Collaborative Partnership to Build Relationships
Respondents reported a variety of strategies to build rapport and relationships with Indigenous clients, including as follows: (a) focusing on mutual goal setting; (b) building trust as an essential foundation; (c) applying principles of Indigenous self-determination; and (d) using client- and family-centered approaches. The primacy of trust and partnership is illustrated by respondent 278: “Without a therapeutic relationship, there is no trust. And without trust, there is no room for providing beneficial supports.” Most respondents (72%) either agreed or strongly agreed with feeling confident in their ability to build trust and a working relationship with an Indigenous client.
Knowledge Gap #5: Respectful Collaboration
The fifth knowledge gap centered on respect and collaboration, identifying a need for occupational therapists to learn about and then access and connect with available supports, to acknowledge Indigenous ways of knowing, and to collaborate with Indigenous communities.
Inclusion of Indigenous Knowledge and Expertise
Within the survey, 9% of the survey respondents were aware of the traditional healing practices used within their healthcare region, whereas 43% indicated that they were not aware. Respondents shared the importance of incorporating or acknowledging traditional healing practices to work with Indigenous Peoples in a culturally safer manner. For example, respondent 70 stated, “Evidence informed practices include evidence from indigenous knowledge and expertise.”
Collaboration with Indigenous Peoples and Communities
Respondents reported the need to collaborate with supports in a client's environment: specifically, learning and engaging with local Indigenous communities, including incorporating Elders and family members into sessions, and collaborating with Indigenous patient navigators in hospital settings and in the community. A total of 46% of the respondents indicated that they understood how to support a client in connecting with a traditional healer and/or Indigenous organization in their healthcare region. Respondent 256 suggested “ongoing education, including first nations programming in local hospitals, inviting elders into our workplaces to provide education.”
Knowledge Gap #6: Environmental Influences
The sixth knowledge gap highlighted that occupational therapists need to develop awareness of environmental factors impacting practice to create safer spaces for engaging in the therapeutic relationship with Indigenous clients and populations.
Workplace Barriers and Facilitators
Within the survey, 45% of respondents indicated that their workplace has implemented strategies to create a welcoming, respectful, and inclusive space for Indigenous clients. These included available sacred places to participate in smudging ceremonies, displaying Indigenous art, inclusive signage, written information or brochures available in at least one local language, websites including acknowledgement of traditional territories, and the ability to access an Indigenous navigator. In contrast, 56% of respondents indicated that their workplace has not implemented strategies, or they are unaware of strategies in place. Respondent 26 shared “whether my workplace has specific practices for indigenous patients isn’t obvious. There are general practices for recognizing and respecting diversity, but I haven’t seen an indigenous focused program or approach.”
System Level Barriers and Facilitators
92% of respondents agreed or strongly agreed that the mainstream healthcare system is inaccessible to some Indigenous Peoples. Respondent 212 shared “additional services time for relationship development & administrative support to the family/community” are available. As well, other workplaces have supported staff education/in-service opportunities specific to Indigenous needs. In contrast, a few respondents shared that their workplaces or management had not done much in relation to working with Indigenous clients and communities. Respondent 183 noted “they have not done much beyond encouraging employees to take cultural safety classes, it is hard to ‘bend the rules’ to better fit our services to our indigenous clients.”
Discussion
This national survey of occupational therapists in Canada represents the efforts of settler-descent occupational therapists to engage our profession in self-reflection to support a response to the Calls to Action of the TRC. The research team constructed six unique themes exposing critical knowledge gaps. While the team did not achieve our goal of representative participation from every province and territory, the findings support a nuanced description of the current state of the knowledge gaps of occupational therapists in Canada.
Decolonizing Occupational Therapy
The findings suggest that there is a need to work towards the decolonization of occupational therapy as a profession via engaging in critical reflexivity and examining the cultural assumptions of the profession's theories, models, and assessment measures.
Critical reflexivity is needed to bring awareness to unconscious biases born of power and privilege in individuals’ practice and the underlying assumptions within the overarching occupational therapy profession perpetuating colonialism (Gerlach, 2015). Respondents endorsed the desire to continue to work on dismantling colonialism and the perpetuation of power imbalances. If occupational therapy continues to be positioned as “culturally neutral,” the conceptual foundations of the profession will continue to be unknowingly imposed (Hammell, 2011). A total of 36% of survey respondents believed that occupational therapy, based on mainstream cultural norms and practices, contributes to the ongoing cultural genocide of Indigenous Peoples through colonialism. In contrast, 28% of respondents disagreed with the above statement, revealing ongoing tensions and the need for active and conscious decolonization to move towards reconciliation. Occupational therapists must be critically reflexive, understand their own biases, and acknowledge how they may be unintentionally perpetuating ongoing colonialism, power imbalances, and genocide in their practice. Occupational therapists may review Beagan (2015) for examples of critically reflexive questions to apply to practice. Occupational therapists need to work towards becoming comfortable with feeling uncomfortable as they continue to challenge themselves through using critical reflexivity (White & Beagan, 2020).
Theories, models, and assessment measures in the occupational therapy profession predominantly reflect the cultural assumptions of the profession's Western, white, and middle-class founders (Hammell, 2011). The insistence on using standardized assessments and quantitative outcomes measures further upholds the neoliberal underpinnings of the profession via categorization and a focus on comparing social “norms” within the profession (Hammell, 2021). As such, the application of these tools with Indigenous clients may be inappropriate as they can be othering, impose cultural assumptions, and reinforce power imbalances (Gerlach & Smith, 2015; MacLachlan et al., 2019; Restall et al., 2016). In place of standardized assessment tools and culturally inappropriate theories, many respondents identified a wide variety of strategies emphasizing flexibility in practice, which has been suggested as a culturally safer approach (e.g., White & Beagan, 2020). However, not all respondents endorsed cultural safety strategies. Some respondents endorsed using stereotype-laden assessment measures (e.g., the previous version 7.1 of the Montreal Cognitive Assessment for First Nations) or a one-size-fits-all approach to practice. Therefore, occupational therapists must critically examine the cultural underpinnings of practice tools to determine their appropriateness for use with Indigenous clients, challenge their routine implementation, and instead favour flexible approaches informed by cultural safety principles. Occupational therapists need to work towards reconciling Indigenous ways of knowing with Western practice, and collaborate with Indigenous Peoples to develop theories and models to positively impact health outcomes (CAOT, 2018b; Phenix & Valavaara, 2016).
Building Collaborative Relationship-Focused Practices
Respondents highlighted the importance of relationship building across multiple themes, both in working with individuals and in collaboration with communities to affect system-level change. This emphasis on relationships is echoed in the TRC and occupational therapy literature. TRC Call to Action #22 specifically calls upon healthcare professionals to recognize the value of Indigenous healing practices and use them in the treatment of Indigenous patients in collaboration with Indigenous healers and Elders (TRC, 2015). Occupational therapy literature highlights that service delivery models should center on building mutually respectful relationships with Indigenous clients that emphasize the value of the client's knowledge and experiences (Brown et al., 2019; Gerlach et al., 2014; Gerlach et al., 2018; Viengkone, 2019; White & Beagan, 2020). Boivin and MacLachlan (2019) further this point, stating informed consent cannot exist without trust in the practitioner–client relationship, as it is an essential component of practice with Indigenous Peoples. Many Indigenous Peoples experience stigma, hostile treatment, discrimination, disrespect, culturally inappropriate care, and a lack of understanding in healthcare environments (Fijal & Beagan, 2019), which can lead to the avoidance of mainstream health care. Health professionals may continue to unknowingly or intentionally ignore cultural contexts, thus perpetuating a colonial relationship with Indigenous Peoples and negatively affecting their health and well-being (Smylie & Firestone, 2016). Furthermore, due to these experiences, Indigenous Peoples may not feel safe or respected when they do choose to access healthcare services (Fijal & Beagan, 2019). As such, occupational therapists must take the time to establish a trusting relationship with Indigenous clients, emphasizing the role of the client as an expert.
Indeed, the emphasis on relationship-focused practice is a central tenet of the newest model of occupational therapy practice proposed by Egan and Restall (2022). There has been a fundamental shift in the clinical approach towards collaborative relationship-focused practice from client-centered occupational therapy (Egan & Restall, 2022; Hunter & Pride, 2021). Critiques of client-centered practice have highlighted that it emphasizes an overly individualistic approach while inadequately considering the practitioner–client power dynamic and the systems of oppression influencing a client's occupational choices (Egan & Restall, 2022). Interestingly, some responses in the survey showed signs of “colour-blindness”—an ideology minimizing the role of systemic racism by claiming to not “see” racial differences—through the assertion that always practicing in a client-centered way and treating all clients equally was sufficient for working with Indigenous clients. By focusing on a one-size-fits-all client-centered approach, an occupational therapist may not recognize the relational context of occupational therapy practice. Furthermore, a practitioner may fail to recognize, and subsequently address, their knowledge gaps related to building trusting relationships with Indigenous clients.
Training, Education, and Learning
The findings suggest that occupational therapists have knowledge gaps related to Indigenous health, and that many seek training to address these gaps. This process relies on an occupational therapist's self-appraisal of their abilities to work with Indigenous clients in a culturally safer manner. However, self-appraisal of one's abilities may be biased. For example, most respondents (72%) indicated that they were confident with their ability to build a trusting relationship with an Indigenous client despite most (61%) having taken less than 10 hours of training and only a minority (9%) being aware of the traditional healing practices in their region. This high level of confidence despite notable knowledge gaps suggests that some respondents may be biased in their self-appraisal. Indeed, clinicians practicing with cultural humility and critical reflexivity may express low confidence due to the constant interrogation inherent in this approach (Beagan, 2015). As such, occupational therapists would benefit from guidance on how to effectively self-appraise and address their knowledge gaps.
Respondents identified that guidance from national and provincial occupational therapy bodies provides direction to address their knowledge gaps. The new "Competencies for Occupational Therapists in Canada" (ACOTRO, ACOTUP, & CAOT, 2021) includes the “Culture, Equity, and Justice” domain containing essential competencies for practice, which are relevant for working with Indigenous clients. However, the performance indicators for this domain lack clarity for implementation. For example, performance indicator C1.3 states to: “Challenge biases and social structures that privilege or marginalize people and communities” (ACOTRO, ACOTUP, & CAOT, 2021, p. 13). While this highlights what to do, it's vague on how an occupational therapist may learn to implement these approaches. While the checklist approach of cultural competency is inappropriate (Beagan, 2015; Grenier, 2020), occupational therapists would benefit from direction for how to address their knowledge gaps.
TRC Call to Action #23 calls “upon all levels of government to: [. . .] provide cultural competency training for all health-care professionals” (2015, p. 164). Anti-oppressive, anti-racist, and decolonizing educational strategies have been offered as effective training approaches to promote culturally safer care (Egan & Restall, 2022). Furthermore, this training should be developed by and specific to the unique traditions and practices of local Indigenous communities (Valavaara et al., 2022). Training is currently available in the occupational therapy profession through a patchwork of various initiatives. Some health districts (e.g., British Columbia and Manitoba) have mandated cultural safety training for healthcare professionals working with Indigenous Peoples (Robinson-Settee et al., 2021). Occupational therapy programs at Canadian universities have undertaken initiatives to address the TRC and implement cultural safety curriculum; however, only four programs have published about their curriculum changes in response to the TRC (Bauer et al., 2022). Most respondents who participated in training did so through their workplace. However, as mandatory training is inconsistent, occupational therapists may not recognize the value nor prioritize this training. This leads to a broader question that our team gleaned from the research: Who will ultimately take responsibility for coordinating these initiatives and providing this training to all occupational therapists to ensure culturally safer care for Indigenous Peoples in Canada?
Study Limitations
It is important to recognize the limitations of this project. There was a low response rate given the overall number of practicing occupational therapists in Canada, and disproportionate response levels between provinces and territories (see Table 1). As a result, this study may represent a sampling bias of those who have already begun to engage in critical reflexivity and have already recognized the need to change occupational therapy practice when working with Indigenous clients and communities. Specifically, there was a high response rate from clinicians in British Columbia, which may skew the survey results due to their leadership as the first province to create an action plan to implement the United Nations Declaration of Rights for Indigenous Peoples (BC Gov News, 2022). Additionally, many surveys were incomplete (n = 64), which could be due to time-constraints of practicing clinicians, the lengthiness of the survey, and potentially discomforting survey questions. Furthermore, the researchers utilized a model of cultural responsiveness (Muñoz, 2007), which is an older model focusing on cultural competence and does not reflect the contemporary approaches of cultural humility and critical reflexivity, nor does it acknowledge the impact of systemic colonialism influencing health. While the survey questions were informed through completion of a Delphi process (Jacek et al., 2022) and pilot testing, the researchers acknowledge that some of the questions may be interpreted in diverse ways. Additionally, survey research represents a positivist perspective and does not engage or incorporate Indigenous ways of knowing or other decolonizing methodologies. Nonetheless, the findings support a nuanced description of the knowledge gaps of occupational therapists in Canada and will add to the current body of literature in Indigenous health.
Conclusion
This research sought to understand the present knowledge of occupational therapists in Indigenous health to identify steps to address knowledge gaps, provide recommendations, and to inform responses to the TRC from the profession. In pursuing this aim, the research team completed a literature review, sought consensus from Indigenous health stakeholders within Canada in the occupational therapy profession (Jacek et al., 2022), and developed and implemented a national survey of occupational therapists. Six core themes were identified to foreground knowledge gaps impacting occupational therapists in Canada and their relationships when working with Indigenous Peoples. The research findings offer insight into the role of the profession in the process of reconciliation and in moving towards cultural humility in collaboration with Indigenous Peoples. It is imperative that occupational therapists recognize and address their knowledge gaps when working with Indigenous Peoples; otherwise, they remain complicit in upholding oppressive systems and practices that perpetuate colonialism.
Key Messages
Knowledge about the ongoing effects of colonization on occupational opportunities for Indigenous Peoples is essential for culturally safer practice.
It is critical that occupational therapists identify and redress their personal knowledge gaps in relation to Indigenous health to appropriately respond to the Truth and Reconciliation Commission.
Supplemental Material
sj-docx-1-cjo-10.1177_00084174231197622 - Supplemental material for Knowledge Gaps Regarding Indigenous Health in Occupational Therapy: A National Survey
Supplemental material, sj-docx-1-cjo-10.1177_00084174231197622 for Knowledge Gaps Regarding Indigenous Health in Occupational Therapy: A National Survey by Claire C. Jacek, Kassandra M. Fritz, Monique E. Lizon and Tara L. Packham in Canadian Journal of Occupational Therapy
Supplemental Material
sj-docx-2-cjo-10.1177_00084174231197622 - Supplemental material for Knowledge Gaps Regarding Indigenous Health in Occupational Therapy: A National Survey
Supplemental material, sj-docx-2-cjo-10.1177_00084174231197622 for Knowledge Gaps Regarding Indigenous Health in Occupational Therapy: A National Survey by Claire C. Jacek, Kassandra M. Fritz, Monique E. Lizon and Tara L. Packham in Canadian Journal of Occupational Therapy
Footnotes
Acknowledgements
The authors thank Matthew Ellies Reg. OT (BC) and Jasper Moedt Reg. OT (BC) for their contribution as members of the research team throughout the systematic literature search, theme identification, and Delphi process. Matthew Ellies Reg. OT (BC) further supported survey development and distribution. Additionally, the authors thank Jinhui Ma, Assistant Professor, Department of Health Research Methods, Evidence, and Impact (HEI), McMaster University for her assistance with statistical and data analysis support. The authors want to acknowledge the active and continuous collaboration and contributions of the Occupational Therapy and Indigenous Health Network throughout the Delphi process.
. The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canadian Occupational Therapy Foundation (2020 McMaster Legacy Grant).
Authors' Note
At the time of the study, C. Jacek and K. Fritz were student occupational therapists at McMaster University in the School of Rehabilitation Science.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.