
Abstract
Living with a chronic health condition in the home can have a debilitating effect on the psychosocial and psychoaffective wellbeing of the entire family. This is particularly the case for healthy school aged siblings. This research investigated the perceptions and experiences of at-school support for well-siblings to evaluate its effectiveness in mitigating and minimising the at-home illness-related stress effect. Seven siblings (both primary and secondary age) whose brothers had received treatment for a chronic illness (e.g. cancer) were interviewed, as were their mothers, six schoolteachers, and two principals. Responses were analysed thematically, and the findings revealed that the chronic illness of a sibling bears strongly on how well-siblings feel about themselves: their very identity is challenged; and they lose their sense of belonging, worth, and self. Findings identified that inconsistencies in at-school support are linked with a lack of an overarching mandate for support, emphasising the need for urgent remediation in policy development and process reform.
Introduction
Well-siblings of children with chronic health problems like cancer face myriad challenges that impact directly and indirectly on their lives. For over five decades, treating teams, academics, and sibling advocates have stressed the need for governments to recognise that well-siblings are at-risk of long-term negative outcomes as evidenced in numerous papers, publications, and submissions to government by Strohm (2017) and supported by the Royal Australian and New Zealand College of Psychiatrists (2011). A child’s chronic illness often overtakes all other priorities, resulting in a shift in parental attention toward the sick child. With increased attention on the ill-child, it is understandable that well-siblings can become forgotten (Kuo et al., 2017). The separation due to frequent and sometimes extended hospitalisations puts a strain on family relationships, and well-siblings can often be left on their own. Looking through the lens of Bronfenbrenner’s theory of human development (Bronfenbrenner & Evans, 2000), school sits beside a child’s family. It is, according to Niesel and Griebel (2005), a social support system to which all children have access and has very strong microsystemic influences. Herein lies its value.
Each school is a reflection of what an education system can influence. Its structural and functional constructs and its proximity to both the family and the well-sibling phenomenon make it an ideal context within which positive longer-term outcomes for at-risk young people can be addressed. Given the importance of school for well-siblings, this study aimed to understand the potential for at-school supports to buffer, mitigate, and minimise at-home stresses. For the purpose of this study, coping is defined as the process of engaging with or disengaging from stressors to master, tolerate, or reduce the negative effects of stress. Coping is an adaptive process; it is learned and practised, and evolves with age, exposure, and success (Hudson, 2016).
Family responsibilities
Well-siblings face challenges that are characteristically different from those faced by parents. Routines are often interrupted and they miss ordinary everyday experiences. They can often be by a hospital bedside or in waiting rooms instead of being in school or out with friends. Healthy siblings may share care of a brother or sister and face a relationship based more on caregiving than companionship (Taylor et al., 2008), which may result in social unavailability according to Le and Fitzpatrick (2018). This in turn, according to Kuo et al. (2017), impinges on friendships, adding to fear, anxiety, anger, isolation, shame, and guilt. They go on to add that the increased attention on the ill-child precipitates an environment of jealousy and envy (Kuo et al., 2017) and lower psychosocial and physical functioning (Kaleda et al., 2022). Hanvey et al. (2022) report siblings feeling invisible, having difficulties because they internalise roles and life conditions, with feelings of guilt and self-blame. The Department of Education and Communities of New South Wales (DEC NSW) had a resource paper Being a carer, being a student, being a kid 1 that seems to be no longer available but recognises that, as a consequence of increased stresses associated with these roles, if a sibling is a carer (primary or vicarious), as most are, they are at risk.
School implications
Well-siblings report being isolated at school with peers being unsupportive (Vanderwerp, 2011), a lack of social interactions outside of school and lost friendships. This loss of friendships is blamed largely on the well-siblings’ reduced social availability (Le & Fitzpatrick, 2018; Meriska et al., 2018). Psychological distress and unmet needs among the adolescent and young adult (secondary school student) populations result from decreased social connections (Sambuco et al., 2012). Siblings with unmet social and emotional needs experience a host of emotional problems (Long et al., 2018) ranging from low self-esteem to increased withdrawal, isolation, lack of involvement, lack of understanding, clinical levels of distress, and internalised behaviour problems (Hanvey et al., 2022; Kuo et al., 2017). This may manifest as increasing disinterest in school activities, poorer school functioning (Verté et al., 2006), diminished academic competence, social acceptance, and global self-worth (Sambuco et al., 2012). The negative impacts of the well-sibling experience can be long-lasting and difficult to overcome (Porteous et al., 2018). Well-siblings have been described as the invisible patient (Franklin et al., 2018) and the sibling experience as the ‘Well-Sibling Syndrome’ (Brown, 2007; Wolfson, 2007).
The need for support
Negative impacts, however, are not necessarily inevitable (Alderfer & Hodges, 2010) as some siblings do react positively (Knecht et al., 2015) especially when given the right support (Kaleda et al., 2022). Support is a predictor of better mental health outcomes helping to minimise and mitigate the effects of stress and promote coping. Without support, well-siblings continue to be at risk.
Social support is described as the support available through connectedness to people: individuals, groups, or a community and as the network of people who are available in times of need, to provide physical, emotional, and financial help (Ozbay et al., 2007). This is both a valuable mediator and moderator, intervening to break the stress cycle, buffer the stress effect, and decrease its intensity. This affords the opportunity to learn and practice appropriate responses, thereby promoting resilience (Alderfer & Hodges, 2010; Gerhardt et al., 2015).
According to Pulimeno et al. (2020), schools are important settings for support and play a fundamental role in developing preventive resilient attitudes and behaviours, which enhance coping mechanisms (Niesel & Griebel, 2005). A child’s sense of self-worth and self-concept, ability to manage stress in a healthy manner, and psychosocial and cognitive domains are developed through in-school programs (Prince-Embury et al., 2016). Teachers facilitate, encourage, and nurture peer relationships and friendships which in turn foster social development (Pavri & Monda-Amaya, 2001). Educational interventions have demonstrated an ability to decrease overall anxiety and can be critical in promoting positive long-term outcomes (McKenzie Smith, Pinto Pereira, Chan, Rose, & Shafran, 2018). What siblings require is positive experiences at school, which according to the NSW DEC (2015, 2012) encourage and foster resilience through clear rules and structures and high expectations and constructive feedback. School is, according to Bronfenbrenner (1979), the ‘second line’ of social support – second to the immediate family. Families depend on school to help children. It is a place to forget the stresses of home; a place where children can be like their peers; a sanctuary and a place to make friends (Lamb & Holley-Boen, 2016).
The routine and normalcy of school and schoolwork are a great buffer, as is the company of friends, peers, and teachers (Lamb & Holley-Boen, 2016). Since other forms of support such as extended family, friends, sports clubs, and religious organisations among others are not integral to all families, children, or cultures, school is most likely to be the one constant for well-siblings. Consequently, at-school support can be a remedy (Pulimeno et al., 2020) for and replace lost normalcy.
Education policy
The Alice Springs (Mparntwe) Education Declaration (the Declaration) (Education Council, 2019), having built on past declarations signed in Hobart, Adelaide, and Melbourne, is a national commitment to the values and goals of education. Every State and Territory that is a signatory to this declaration is held accountable to deliver on this commitment. While there is no state-based specific policy that mandates and directs support for well-siblings, The wellbeing framework (DEC NSW, 2015), the ‘Every Student, Every School’ initiative derived from the Learning and support framework (DEC, 2012), and the previously mentioned resource Being a carer, being a student, being a kid have social support principles embedded in them and are designed to be inclusive of and accommodate support for every child.
This study positioned the education system (school) as the vehicle of best fit for ensuring sibling support, given that school is the one place where a comprehensive service is provided so that every child would be assured individual support.
Bronfenbrenner’s theory focuses on a child’s ecological context and the complex relationships within and around it. It explains the significance of the interplay between context, relationships (processes), and the family on a child’s development. His Ecological model of human development (1979–2005) serves as the base platform on which well-sibling development can be explained and understood. Bronfenbrenner’s theory supports the idea that a child’s identity is embedded within the person-context and is critical in influencing perceptions of situational stresses, support, and effectiveness of support. It enables an explanation of the negative outcomes on well-sibling development and underscores the value of social support as the mediator and moderator which influence positive long-term outcomes. Bronfenbrenner’s theory upholds the rationale that school, as a second-order entity, is a powerful vector to reclaim a child’s disrupted human development. Bronfenbrenner’s theory is pivotal in exploring and understanding the well-sibling experience and supports the methods of data analysis.
Method
Rationale
The well-sibling experience is a social phenomenon. It requires a social research perspective to establish truths and realities in relation to lived experiences, the reasons for these experiences, and how they could be different (Blaikie & Priest, 2019). The reality of the well-sibling phenomenon can only be understood through the interpretations of those who live it (Blaikie & Priest, 2019). Well-siblings’ realities are a complex construct of their individual perceptions that are deeply attached to and associated with their brother’s or sister’s illness and all the resulting reciprocal relational complexities.
Understanding the reality of the well-sibling phenomenon within its context is imperative to determine the effectiveness of educational support. This was reviewed in light of the research question: ‘To what extent do practices (policies, procedures and programs) of the NSW Department of Education (DoE) provide support for siblings of children with a chronic health condition, as perceived by them (well-siblings) and their parents?’
The case study
Demographics of the Sample of Well-Siblings.
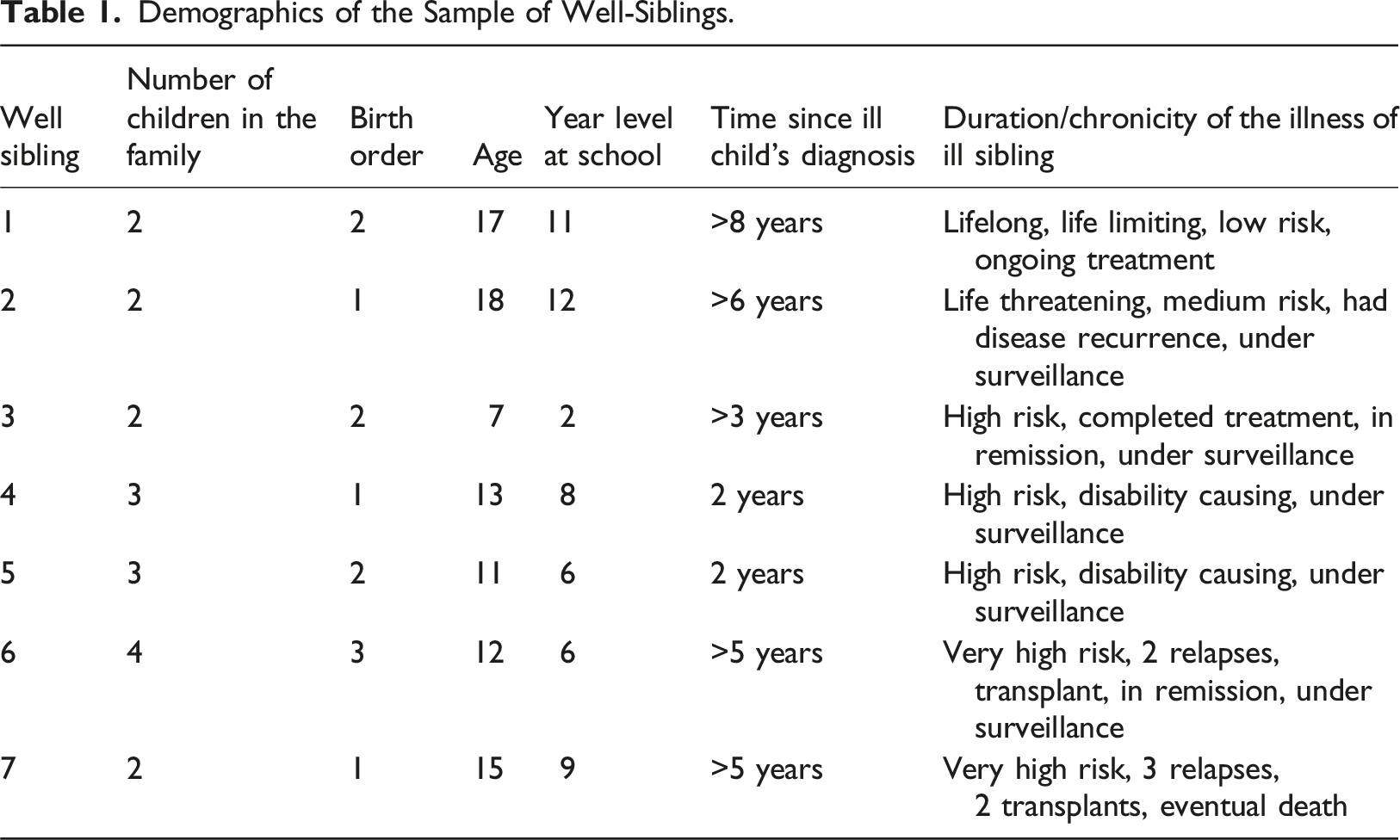
Participants – The case study units
Well-siblings’ lived realities are complex. These realities are subjective, so this multi-case study collected data through structured and semi-structured interviews based on specific Sydney Children’s Hospital Network (SCHN) ethics-approved interview schedules for siblings, parents, and teachers. The interviews were a set of phrased conversation starters to allow for natural conversational questioning and served as a scaffold to foster memory recall and keep the interview focused on targeted data collection. It encouraged conversation, offering participants opportunities to dwell on experiences, memories, and emotions affording flexibility and a chance for siblings, parents, and teachers to share their experiences openly.
A series of interviews with six parents and seven well-siblings (aged 7–18 years) were conducted at the Children’s Hospital Education Research Institute. Interviews with the eight school staff (one child had transitioned from primary to secondary school) occurred on school premises during school hours. Each interview lasted between 30 and 45 minutes and was tape recorded with permission.
Ethics applications were submitted to The University of Notre Dame Australia (Ref No: 012099S), the NSW Department of Education (SERAP, 2013233), and the Sydney Children’s Hospital Network (HREC Ref: LNR/16/SCHN9), and clearances and approvals obtained.
Data collection
Each well-sibling participant was asked to describe their sibling’s (all brothers, coincidentally) illness to create a backdrop against which all their experiences could be explained, explored, and justified. They were asked to share memories of events, people, feelings, and things that helped them and/or hurt them. They were asked about situations that empowered them and those that challenged them. There were questions that prompted them to connect emotionally with what they had lived with and through. Their memories of everyday at-school activities were explored by unpacking their experiences of support. They were asked to talk about how they felt about being at home, helping out, and taking on some of the caring responsibilities for their sick sibling. The well-siblings were encouraged to talk about how they felt at the time of their sibling’s diagnosis and compare that with how they felt about themselves at the time of the interviews. They were asked about their teachers and their friends, and if they had been included in the support planning process at school. They were asked to score the support they received at school on a scale of one to five, with one being not good and five being exceptional. Parents were asked similar questions to add to, corroborate, and describe the illness-related stresses at home, what they experienced as support from their child’s or children’s school/s, and what they thought their well-child had received as at-school support. Teachers and/or principals were asked questions to develop a deeper understanding about the support the well-sibling received at the school: what their school had done to prioritise needs; as well as the part/role/voice of the well-sibling in the planning-of-support process, teacher accountability, funding, staffing, and policies. They were asked to discuss their role in the well-sibling wellbeing and how they assessed their school’s response to the well-sibling.
Interviews were conducted by a qualified and experienced K-12 teacher who was also familiar with processes and procedures around engaging with children within the hospital. Interviews were pre-booked and coincided with hospital appointments of the ill child. Each interview was adapted to suit the age of the well child (well-sibling) and ranged between 25 and 45 minutes. These were audio recorded with permission. All parents accompanied their well child (well-sibling). After the well-sibling indicated that they were comfortable, parents left and the interview was conducted with just the interviewer and the well-sibling. Introductory conversations with the parent and well-sibling were informal and focussed purely on providing a sense of comfort. Each data collection session was transcribed and each participant was subsequently offered a chance to check their transcripts.
Data analysis
Once data for each case were collected, analysis occurred with a focus to ensure preserving participant voice. A grounded approach to data analysis was employed (see Charmaz, 2000). Each transcript was read numerous times to promote familiarity with the case. This was followed by a three-way grounded thematic analysis. Transcripts were analysed line by line and grouped into distinct ideas with allocated codes and regrouped into themes. The final result was written as a narrative from which final themes and sub-themes were derived (Huberman & Miles, 2002). These themes and sub-themes were then subjected to a cross-case comparison. This afforded a categorisation focused on form and content and explained the themes in terms of temporality, sociality, and place (Clandinin & Connelly, 2000). Second and third iterations were completed by experienced academics in the field and the final structure was reviewed by an in-house academic at the hospital to ensure content validity.
The data were analysed and interpreted through the lens of Bronfenbrenner’s theory of human development (2005) to understand the impact of family and environment on children’s development.
Findings
Overview of Themes and Sub-themes.
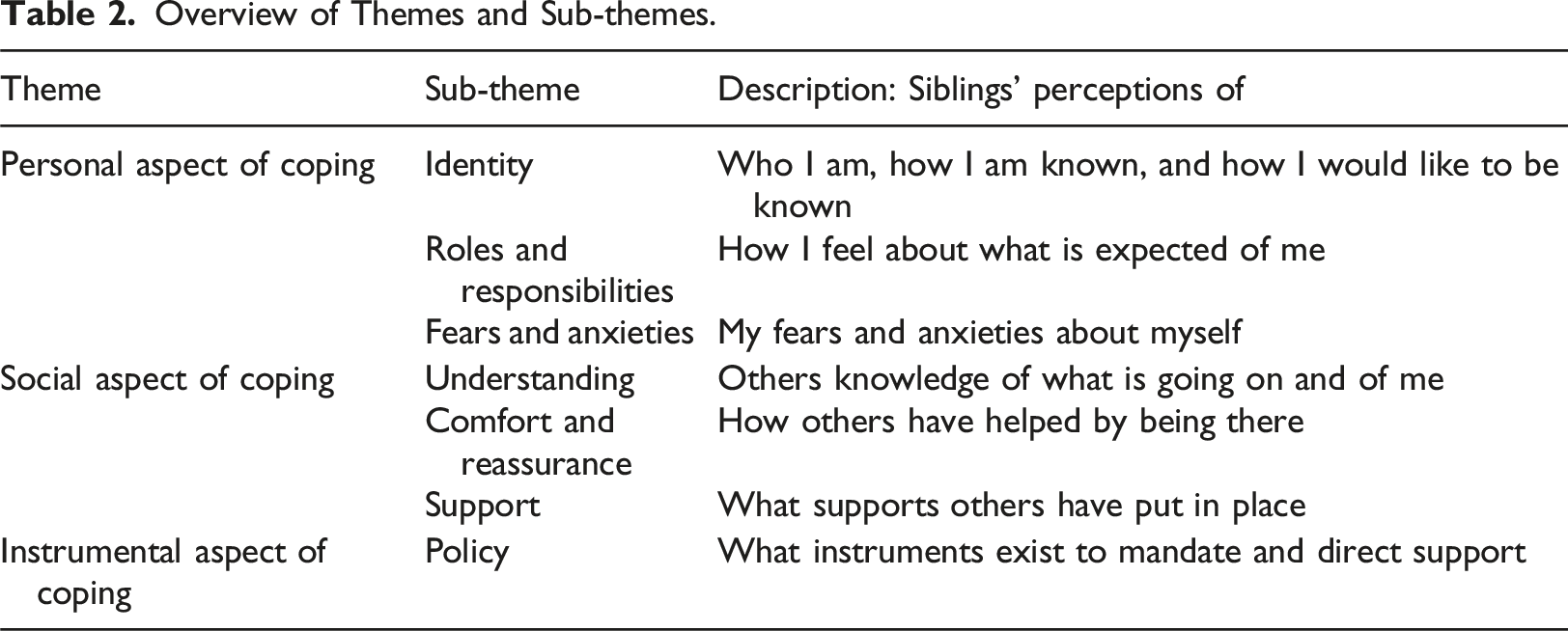
Theme 1: Personal aspect of coping
This theme focussed on the well-sibling’s sense of self from their perspective, corroborated by perceptions of the parent and the school’s support staff. Within this theme three sub-themes emerged: identity; roles, responsibilities, and expectations; and fears and anxieties.
Identity
It was evident that the illness of a sibling bears strongly on the identity of the well-sibling and is both a determinant and an indicator of coping. There was a consistent “yearning to be myself” and “to be known for who I am” with the adolescents Ava and Beverley and Dylan and “to be taken seriously”, with Ava, Beverley, Dylan, and Evie (names changed for the study). An “unrelenting conflict between who I am and want to be versus how I am known and want to be known” exacerbated frustrations and anger over becoming known as “the sister of the cancer kid” for Ava, Beverley and, “the cancer boy’s brother” and “the bald one’s brothers” for Dylan and Darren. They reported confusion over simultaneously becoming the outsider, being “in the shadows”, watching from outside, feeling like “I just wasn’t important” and becoming “a nobody” and then Ava, Beverley, and Evie confiding that they took pride in being his protector and defender. Siblings regretted all the missed opportunities and felt that their lives would never be normal. They reported feeling guilty over being the well one or “just wanting to be me”, “wanting all of this to be over”, waiting to get back to normal, and becoming “emotionally distanced and selfish”, especially as older sisters. Feelings of pride (for being the protector) mixed in with guilt and regret caused self-doubt. The well-sibling experience was described as one that “diminishes self” and “reduces me to nothing” according to Ava and Beverley. Well-siblings reported that they felt they had lost their identity to not only the ill brother but also to the illness as well.
Roles, responsibilities, and expectations
This sub-theme impacted greatly on a sense of self: self-worth, self-concept, and self-esteem, and was fundamental to the development and growth of well-siblings’ identity and coping. The demands of frequently shifting roles and additional responsibilities within the home caused significant physical and psychological disruption to their lives, and siblings reported feeling as if they had to pick up the pieces. Self-imposed expectations mixed in with that of parents and school were deemed stressful, challenging, and burdensome. Well-siblings felt as if they were expected to keep going like nothing was the matter, to maintain normalcy and “perform academically”. Parents corroborated this, reporting, “she saw herself as needing to keep going as if nothing was happening in our lives”, “pushing himself”, “punishing herself for being well”, because “she believed she had no right to have life”, “she wanted to be his voice and my helper all the time”, and “he was unhappy that he wasn’t doing enough to help out”. The routine of school was the best distraction according to all the parents and teachers; special programs at school “like Bob the Builder” (a school program named after a children’s television show) and “hands-on stuff” (the schools description of other activities they used like gardening and keeping pets), the pursuit of personal interests, and the experience of successes in the face of challenge were appreciated as “helping to ease the stress” and boost self-worth and confidence, thus enabling coping. Being of assistance (in the home), acknowledgement and appreciation of efforts and assistance, was a big boost to their sense of self-worth and self-esteem, especially for Evie and Darren. Well-siblings reported needing to be part of the illness by helping out as it helped overcome feelings of guilt and regret and returned some self-worth: “it helped me feel good about myself”. Siblings’ identities and self-concept fluctuated continually between relevance and being of worth, to irrelevance and being unimportant and in the way, from being the outsider to the unofficial carer and this added to the confusion but also gave back a renewed sense of purpose.
Fears and anxiety
Well-siblings reported that they were often home alone, or with grandparents or neighbours or friends and that this could happen without much warning or explanation. They were terrified, with no one to explain things to help calm their fears for their ill brother, their missing parents (who had taken their brother to hospital), and for themselves. The physical separation from “no longer available parents who were completely preoccupied with my brother” and not being included in discussions and decisions “because who asks a kid, right?” exacerbated the isolation and fear. The worsening worry and the ongoing and remnant stresses became overwhelming, “I felt paralysed”, “I dreamt that I was drowning”, “I just couldn’t think”, and “I just wanted to scream all the time”. This resulted in a complete inward withdrawal and “retreating into myself” for some, and for Dylan it was a case of acting out and lashing out and even running away. Parents became distressed as they reported contemplating professional help and themselves experiencing terrible guilt and fear that the well-sibling would become the next patient with mental health issues. Parents wished they had invited them (well-siblings) into discussions or sat down and chatted with them. What stood out was that the well-siblings and their parents believed that parental non-disclosure gave well-siblings false hope about their ill brothers.
The key learning that this theme highlighted was that acknowledging, recognising, and respecting the sibling is the first step in supporting the well-sibling in how he or she feels about ‘self’.
Theme 2: Social aspect of coping
This theme is focussed on the sibling’s perception of self in relation to others and the value that these relationships hold in terms of mitigating stress and promoting coping. It comprises three sub-themes: understanding, comfort and reassurance, and support.
Understanding
Understanding is thought to be the key operative on which both support and coping are dependent. It is foundational, helping to define, determine, and describe the relationship between the well-child and significant others. Siblings were able to delineate between their own needs to understand the situation and their parental and sibling absence, the need for others to understand their (well-sibling) situational needs (which are related but different to the ill-child’s), and the need for understanding to be afforded them, in terms of flexibility and patience and tolerance and support. “You’d be lucky if you got everyone at school to understand and be understanding” was a frustrated comment that seemed to represent the experience of most of the adolescents. The younger siblings were less perceptive and other than two mothers, parental experiences of understanding at the school level resonated with a similar hopelessness. “If one gets it, you can bet the rest don’t” was the experience of three mums and two went on to elaborate that while the year advisor, one teacher did (understand), “the rest were horrible”. When it came to understanding, families’ perceptions ranged from “He (the ill child) was treated like a burden” to the ill child got all the attention, but no one bothered about the well-sibling. Well-siblings shared that even family (uncles, aunts, and cousins) didn’t understand and said all the wrong things. Ava, Beverley, Dylan, Evie, and Frankie shared that they (the well-sibling) were expected to not make a fuss as they were “the lucky one”. “So much for understanding!” were Ava’s words to describe what was the resounding experience. Only two parents had positive responses to their well child’s needs at school and that was because “the principal was personally involved”. The two principals couldn’t stress enough, how much “understanding, and in turn support, is dependent on information being shared” and why some (siblings) have a better experience of support than others. Parents guiltily confessed that had they not been so preoccupied they would have explained things to the school. Adolescent siblings added that understanding depended on the person and his or her personality and that is why some (teachers) understood and were understanding and others “were awful”. Well-sibling experiences ranged from uplifting and positive to demeaning and stressful: from the kindness and generosity of the principal and teacher and coach to being accused of lying or being told to appreciate their wellness and “suck it up”. All well-siblings and almost all parents reported that if they had someone who understood or if someone had asked “how I was doing, I might’ve opened up”. Unfortunately, while some felt that no one at school understood what the well-siblings were going through, others’ experiences were that no one at school cared.
In summary, participants felt that “understanding doesn’t just happen”, and “it depends on genuine interest”, information, and knowledge. If teachers and peers have “no idea” about what is going on, how the situation of stress in the home is affecting the well-sibling and what can be done to make things easier, then “understanding in terms of support is an unrealisable dream”.
A lack of understanding was the single most significant factor in escalating the fear and worry, anger and resentment, and confusion reported by participants. Well-siblings also reported that parental absence or unavailability contributed to their negative feelings.
Comfort and reassurance
Comfort and reassurance are a measure of the effectiveness of understanding. Siblings reported that having someone to go to at school, other kids with similar experiences to share with, someone who understood what he/she was going through, someone who was interested in the well-sibling, “having a school mum”, the music teacher and the soccer coach who went out of their way to make me feel looked after, and having people around, especially those who understood, especially when mum and dad were gone, were all comforting and signs that there was “real understanding”. Parents confessed that they’d wished that someone from school had taken their place and cared for their well child. For all well-siblings who attended the same school as the ill child, “seeing him (the ill-sibling) return to school, doing normal stuff and knowing that he was well” was a source of relief and comfort. One older sibling described her comfort and reassurance in having her family back home after her brother’s recovery because “I had lost both my parents to my brother and then all three of them to the hospital”. The isolation she had felt during her family’s absence was evident in her recollections of having “no one except an empty house to look after for months”. A key function of social support is the comfort and reassurance it affords well-siblings who are alone, feel unimportant and isolated, are afraid, and at times angry and confused. It has great value and importance in enhancing coping and building resilience. Maintaining normalcy, having someone to go to, and the wellness of the ill-sibling are sources of comfort and reassurance.
Support
Support at school is the key to fostering coping and foundational in buffering everyday stress. Siblings were unanimous in stating, “when schools (staff) understand they offer understanding, that is the kind of support we need”. Experiences of support ranged from an inexcusable 1 out of 5 – and even that was just the fact that school itself was a good distraction to 5 out of 5, for “great support”. One sibling reported being given detention for coming late to school after “I was up all night caring for my brother”, another was made to explain why her parent hadn’t given her a note to explain unfinished work and the teacher wouldn’t believe her situation, despite the principal knowing what was going on. Another said that the primary school was so much better at support because everyone treated all the kids like family, but high school was different, “it felt like no one cared”. For one case unit, the well-sibling, parent, and principal appeared to agree that measures taken by the school including allocating learning support time and an in-school program for social and emotional support had proven beneficial, with the well-sibling saying that school “made me feel special” and her mother expressing gratitude that the school “took care of everyday stuff”. The two principals that were part of the study believed very strongly that purposive student placement into a familiar teacher’s class was extremely valuable, as was setting up a friendship group. Speaking of helpful office staff, siblings and mums agreed that “having someone to take the place of mum at school was priceless”. On the human front (as opposed to instrumental support), support was found in people’s presence, their words, and their actions. The inconsistencies in support that siblings reported receiving within their own school (from teacher to teacher) and between schools, that is, primary and secondary school, are a cause for concern because they can add to the already elevated stress experienced by the well-sibling instead of mitigating and minimising it. Parents and schoolteachers agreed that for support to be effective it must be based on a whole-school approach, which takes planning and “training, staffing, and funding”, added the two principals. Siblings who attended the same school as the ill-child found more support “despite their (own) invisibility” due to the “visibility of his illness” as it forced a response even from those who otherwise “didn’t bother”. The schools that did support well were organised and prepared according to parents while others “did things on the fly” and so it was a case of “hit and miss”. All parents wished their children had received the right support to help to ease the stress that surrounds illness in the home, instead of “exacerbating confusion, loneliness, and isolation”.
Theme 3: Instrumental aspect of coping
This theme focused on the non-human or process aspect of coping. It is systemic or process-based in nature and instrumental in guiding thinking and action. It mutually orders and is ordered by both the personal and social aspects of coping, directs planning, and justifies funding and staffing to guarantee understanding and support. It has only one sub-theme: policy.
Policy
Policy is “in effect the most instrumental aspect of coping”, according to principals and teachers because it mandates and directs action; it ensures consistency, reliability, and effectiveness; and serves to inform and guide planning and support. Principals added that policy also determines funding priorities, staffing, and training so that “kids, who are the direct beneficiaries, do not miss out”. There is no state-based specific policy that mandates and directs support for well-siblings, but teachers and principals referenced what does exist, that is, The Wellbeing Framework (DEC NSW, 2015), the ‘Every Student, Every School’ initiative derived from the Learning and support framework (DEC, 2012), and the Being a carer resource. Both principals involved in this study stressed the urgent need for specific (well-sibling) policy development given improved treatment outcomes and the subsequent expectation for families to manage longer-term illness-related issues at home. One confessed to hoping that the Wellbeing Framework would bring about a change in how support happened at schools but admitted that the lack of specific policy was the real reason siblings were falling through the cracks. Both insisted that “without policy, support could never be anything more than unreliable, dependent on personal empathy, inconsistent and ineffective because while some do (get it) most don’t. They (school staff) need to be mandated, directed to do and to be held accountable”. One principal affirmed that strong policy would ensure information sharing and planning in consultation with the well-sibling and family and would improve the school experience for the well-sibling. Parents and teachers saw a real need for policy “to lock in positive action”. Two teachers who had themselves been the well-sibling (in their younger years) added, “at school, we need to be proactive in our approach and know what is going on for our kids and their families”, and “at present, schools are drawing on related policies and that isn’t good enough. A specific sibling policy is urgently needed”. One mum believed that, if there had been a policy that recognised siblings’ needs, her daughter would not have been overlooked. Both she and the teacher at school agreed that “policies come from legislation and there is nothing in that respect when it comes to well-kids”.
The principal of the primary school that supported the two sibling brothers added that while there was still much to be desired in terms of what support siblings ought to get, schools have very limited resources and increased complexities and needs, and “well-siblings might not even be on our radar. We know that families don’t have the time to come in to inform us but there is no way for us to know. That’s where the gap exists. That’s the problem. Without policy to mandate information sharing, siblings might continue to be invisible, and their needs go unnoticed and unaddressed”.
Discussion
According to Bronfenbrenner, a child’s identity is embedded within the person-context and is critical in influencing perceptions of situational stresses, support, and effectiveness of support.
Siblings of children with a chronic health condition have been frequently described as a population at risk (McKenzie Smith et al., 2018). The content and propositions of Bronfenbrenner’s theory of human development provided a point of deep reflection and served as a powerful heuristic. Social supports at Bronfenbrenner’s micro- and mesosystemic levels are well-documented buffers that enhance coping, build resilience, and effect longer-term positive outcomes. School, by its very nature and design, is well positioned to be an effector of such support. This study aimed to determine the value of educational support to buffer, mitigate, and minimise at-home stresses and positively effect coping. Value justifications of effectiveness of at-school support were based on siblings’ perceptions (corroborated and explained by parents and teachers/principals) of support availability, incidence of support, adequacy of support, and its specific ability to mitigate and moderate at-home stresses.
Compensating the lost microsystem
The case of the well-sibling is often interpreted in terms of typical human development with little consideration of sympathy, empathy, and flexibility to compensate for contextual changes and challenges (Bronfenbrenner, 2005). Well-sibling identity and coping are mutually dependent (Shean, 2015), ordered by the at-home-illness versus at-school-support effect. If the reality of lived experience is considered in its entirety, the detrimental effect on development, sense of self, and identity is unmistakable and cannot be ignored (Kuo et al., 2017). The well-sibling experience is complex and not easily addressed.
The data from well-siblings indicated that with the onset of illness, there is a new order to their lives. Well-siblings, who should have been the core of their own microsystem, were ousted to make room for their ill-sibling. Through a series of role transitions, they oscillate between part-parent, part-carer, and outsider. Bypassing significant milestones of learned, tested, and practiced emotional and psychosocial development, the well-siblings were forced into responsibility well beyond their understanding and/or maturity. Prolonged separation due to treatment, including repeated and extended hospitalisations, left them physically and emotionally distanced at times and burdened with increased stress, resulting in lost confidence accompanied by low self-worth, depleted self-esteem, and self-concept, eventuating in loss of identity and loss of self to the ill-sibling.
In the case of serious and acute or chronic and prolonged illness of a child, parental loss to the ill-child is unavoidable, accompanied by the loss of the ill-sibling to hospitals and treating teams (Kuo et al., 2017; Strohm, 2017). Compensation for this loss of primary mechanisms (parents and sibling) is best sought in the next accessible context, that is, school
Macrosystemic influences
Buffering situational and contextual stresses, repairing the diminished sense of self, and empowering positive identity require a policy-driven, school-based, planned, and proactive approach that includes sibling voice. Primarily political, policy has the power to determine what is done. It shapes who benefits, for what purpose, and who pays. It goes to the very heart of educational philosophy – the purpose of education (what is it for?), the focus of education (who is it for?), and who decides how it is achieved and how it is afforded (Bell & Stevenson, 2006). Current education policies, while being rightfully focused on academic, social, and emotional outcomes of children, claim to prioritise familial and cultural influences on education but, according to the findings from this research, they fail to recognise the impact of at-home illness-related stresses on life and learning. While shared policies between education and health departments around illness and/or disability support the sick child and/or the child with the disability (McCabe & Shaw, 2008), there is no policy that acknowledges and recognises the dramatic impact on well-siblings. Policies and papers such as Every student, every school (DEC NSW, 2012), the Being a carer resource, and even The Wellbeing Framework (DEC, 2015) were noted by the teachers and principals as coming close but failing to meet specific well-sibling needs. The evidence from this research points to a lack of awareness that stems from a lack of information, a failure to acknowledge and recognise, and the inability to action plans because they are not grounded in knowledge and understanding. When people do not know, the unsympathetic may get away with describing the well-sibling journey as a ‘pity party’ (Strohm, 2017). On assessing the impact of existing policies to effect coping and resilience in well-siblings, it is evident that not only is specific policy urgently needed but policy reform and/or development is, as it was considered the most influencing determinant in the support-coping dynamic, impacting all aspects of social support and coping. If policy development is to be successful, it must consider the educational context or environment, be developed within government, and have investment of and from end-users and society (Bell & Stevenson, 2006). Extending the well-sibling voice to influence policy development process is consonant with the principles of the design thinking process (Mintrom & Luetjens, 2016).
Findings highlight the gravity of these siblings’ experience. All the data pointed to the issue that, if unsupported, at-home illness-related stresses could become compounded over time and lead well-siblings to become the next patient. For most of these well-siblings, the routine and normalcy of school made it a place of respite and repair. In its social construct, this provided the power to buffer and break the stress effect and foster coping. In the absence of specific well-sibling policy, current support appears to be unreliable and inconsistent and may even be more harmful than helpful. It is time to listen to the voice of experience. It’s time to change the invisibility of the well-sibling into an opportunity for change.
Recommendations
The issue with current practice is that, as described by five of the six parents, both principals, and four teachers, it is ‘unreliable and inconsistent’. There would seem to be an urgent need for a higher level of management of the situation. Based on the dialogues with these well-siblings, their parents, and school leaders, the following are recommendations that schools could embrace (in the absence of governmental policy) if they are to effect timely and helpful stress minimisation and mitigation strategies for well-siblings of children with a chronic health condition: • Review school policies to determine their effectiveness to meet the support needs of well-siblings. • Appoint staff who will act as at-school liaisons between education, health, and families and oversee and manage school support. • Organise support planning meetings with stakeholders including families, the well-sibling, and health professionals to discuss the nature and structure of support to be provided. • Utilise community resources, facilities, and expertise through collaborative networks. • Plan, develop, and conduct ongoing professional learning for school staff.
There is also a great need for further research, from a psycho-social perspective. This will not only strengthen and validate this study but also give well-sibling research the impetus it needs to force change.
Limitations of this research
Sensitivities around the illness experience caused hesitation in some participants, delaying data collection and analysis. Emotional memory recall for some participants brought to the fore forgotten distresses that urged a rerouting of the interview process to offer comfort. Another limitation was that the sample comprised all male ill-children and only their mothers/female guardians (coincidentally). The study was limited to public schools in NSW. The cross-section of ill-child illnesses and the length of the time participants had experience with the chronic illness, therefore, comparisons may be compromised. To understand how well-siblings cope and develop over time, after the illness has passed, or years after the death of the ill-child, requires a longitudinal research perspective that wasn’t afforded in this study.
Conclusion
School is a key social system that has access to a child for an extended period, affording ample opportunity to get to know the child (Australian Institute for Teaching and School Leadership, 2011) and his/her context, to effect learning, development, coping, resilience, and positive long-term outcomes. As Bronfenbrenner suggests, school is a fundamental system outside the family (and extended family) that has a positional delivery advantage anchored in a rich collective human resource. Its structural and functional construct and its proximity to both the family and the child, and almost every situation that relates to a child, make it a significant context within which prevention and remediation can be afforded. By virtue of this proximity, and as outlined in the NSW government policy, schools have a responsibility to deliver on support (DEC, NSW, 2015) that is pre-emptive, proactive, reliable, consistent, sustainable, and effective. Being the primary provider to this at-risk population will necessitate substantial efforts to address the complex psychosocial needs.
Well-siblings do not qualify for medical interventions pre-emptively, and practitioners often don’t have access to them. From the conversations with this small group of well-siblings, it is evident that their experience is no simple issue of inconvenience or distraction or displacement and disadvantage; it is a high demand situation that not only disrupts their developmental process but also has the potential to diminish and impact their identity. Among the urgent care needs of the ill-sibling, expectations of family, and prolonged separation and isolation from them and the safety of home, well-siblings may experience severe stress that compounds over time.
Providing targeted support to disadvantaged students in Australia is a fundamental commitment of the Melbourne Declaration on Educational Goals for Young Australians (Ministerial Council on Education, 2008), and the NSW Department of Education honours this commitment as evidenced in the many policies related to student wellbeing and support. At-school support is a fundamental right of every Australian student. Evidence from this research clearly demonstrates that siblings of chronically ill children are disadvantaged in many ways. It was almost unanimous as summarised by one principal, school is not just ‘the place of respite and repair’ it is ‘the only hope’ that this steadily growing at-risk population has. Family and school environments are interconnected, mutually influencing each other. Therefore, educational policies, processes, and practices must consider influences on and of the family in addition to school factors.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.