
Abstract
Objective:
Australia’s Better Access initiative enables people with mental disorders to be referred for treatment and management through a range of providers. The costs to consumers are offset by Medicare rebates. We examined eligible providers’ and referrers’ views and experiences with Better Access.
Method:
An anonymous online survey was completed by 2386 participants: 572 clinical psychologists, 1140 psychologists, 398 social workers, 104 occupational therapists, 45 general practitioners and 126 psychiatrists. The survey included questions about processes, outcomes, barriers and facilitators associated with Better Access.
Results:
Most survey participants (54–99% depending on professional group) had provided Better Access services in 2021. The majority believed Better Access enables them to deliver care that is appropriate, tailored to consumers’ needs and achieves good outcomes. However, there were concerns that consumers who require more intensive or linked-up care might not receive adequate care through Better Access. Many providers, particularly allied health professionals, did not have the capacity to take on new consumers, leading to long waiting lists and delayed treatment. High out-of-pocket costs (a flow-on effect of inadequate rebates) were seen as discouraging engagement by consumers on low incomes. Good communication between referrers and providers was seen as a key facilitator of Better Access care, but complicated referral and review processes were identified as impeding communication and disrupting continuity of care for consumers.
Conclusion:
Providers and referrers agreed that Better Access achieves good outcomes for consumers. Strategies to address workforce capacity and affordability for consumers, and to streamline referral and review processes are needed.
Introduction
The Better Access to Psychiatrists, Psychologists and General Practitioners through the Medicare Benefits Schedule initiative (Better Access) was introduced in 2006 following evidence that, despite the high prevalence and burden of common mental disorders in the Australian community (Andrews et al., 2001; Australian Bureau of Statistics [ABS], 1998), treatment coverage was low (Hickie et al., 2001). Most mental health care was being provided by general practitioners (GPs), and access to specialist mental health providers and psychological therapies was limited (Andrews et al., 2000; Groom et al., 2003; Parslow and Jorm, 2000).
Better Access established new care pathways for people living in the community experiencing mental disorders. Eligible practitioners (usually a GP) can prepare a GP mental health treatment plan for a consumer and refer them for up to 10 sessions of individual psychological treatment (‘psychological therapy services’ provided by clinical psychologists and ‘focussed psychological strategies’ provided by psychologists, social workers, occupational therapists [OTs] and GPs) per calendar year and/or up to 10 group sessions with an allied health professional. The consumer’s plan should be reviewed by the GP at least once. Psychiatrists can conduct initial consultations with new consumers, prepare a psychiatrist assessment and management plan and refer for treatment under Better Access or other programmes and review care provided under a psychiatrist or GP plan (Australian Government Department of Health and Aged Care [DHAC], 2023a).
Better Access services are implemented as item numbers on the Medicare Benefits Schedule (MBS). Each MBS item has a schedule fee (i.e. the fee the government determines appropriate for the service, although a provider can set their own fee) and a benefit (i.e. the amount Medicare will pay for the service, calculated as a percentage of the schedule fee). A provider can accept the benefit as full payment for the service (‘bulk-billing’) or can charge a fee higher than the benefit paid, in which case the consumer incurs an out-of-pocket cost.
Better Access has been modified over time in response to policy priorities. In 2020, changes were introduced in recognition of the mental health impacts of COVID-19. These included an additional 10 treatment sessions per year, new items for delivering services via telehealth and expansion of the eligible population to include residents in aged care facilities (RACF). The additional 10 sessions and RACF expansion ceased in 2022; however, telehealth options continue (Australian Government Department of Health, 2020, 2022a). In November 2025, arrangements for services provided by GPs were changed. This included retiring dedicated MBS item numbers for review of a mental health treatment plan and mental health consultations (to support the continuing care of patients with a mental disorder) with GPs to use general attendance items instead (Australian Government Department of Health, Disability and Ageing, 2025).
Given that Better Access pathways are complex, it is important to monitor how well these arrangements work in practice. Surveys and stakeholder consultations conducted between 2007 and 2019 show that providers generally consider that Better Access has supported a wider range of people, especially those on low incomes, to access psychological treatment and has enhanced communication between referrers and providers (De Silva et al., 2017; Fletcher et al., 2011). However, barriers to access and quality of care (e.g. lack of allied health professionals in rural areas, long waiting lists to see psychiatrists, high out-of-pocket costs for allied health professionals’ services, insufficient sessions to meet some consumers’ needs) and to communication between professionals (e.g. inadequately documented treatment plans) have been noted (De Silva et al., 2017; Fletcher et al., 2011; Productivity Commission, 2020).
In 2021–2022, we conducted an evaluation of Better Access comprising 10 studies (Pirkis et al., 2022). The current study and eight others are reported in this issue of the Australian and New Zealand Journal of Psychiatry (Arya et al., 2026; Chilver et al., 2026; Currier et al., 2026; Harris et al., 2026; Newton et al., 2026; Pirkis et al., 2026a, 2026b; Tapp et al., 2026). The evaluation was funded by the (then) Australian Government Department of Health and Aged Care (DHAC) with advice provided by two stakeholder groups – the Clinical Advisory Group (CAG) and the Stakeholder Engagement Group (SEG). In the current study, we surveyed eligible providers and referrers to ascertain their views and experiences regarding Better Access. The survey considered service delivery during 2021 when the COVID-19 changes were in place.
Methods
Design and participants
We designed an online survey of providers and referrers from professional groups eligible to deliver services under Better Access (GPs, psychiatrists, clinical psychologists, psychologists, social workers and OTs) who had worked in private practice in 2021. We did not require participants to have billed for services under Better Access in 2021, as we wanted to include the views of both those who regularly made referrals or provided care under Better Access and those who rarely/never did so.
Participants were recruited through provider group organisations (Supplemental Material Table S1), which distributed invitations to their members via direct emails and/or notices in member newsletters and social media. This strategy of distributing invitations via trusted organisations was intended to promote participation. However, it meant we could not calculate a response rate because we did not know how many people saw the invitation. Emails and notices with a URL and/or QR code for participants to access the survey online were circulated from the week beginning 21 February 2022, and the survey remained open until 25 March 2022. Upon launching the survey, a plain language statement and consent check were presented. Consenting participants continued to the survey questions. Survey data were managed by an independent data services subcontractor (Logicly). The survey was completed by 2386 participants, primarily psychologists (47.8%), clinical psychologists (24.0%) and social workers (16.7%) (Table 1).
Characteristics of participants.
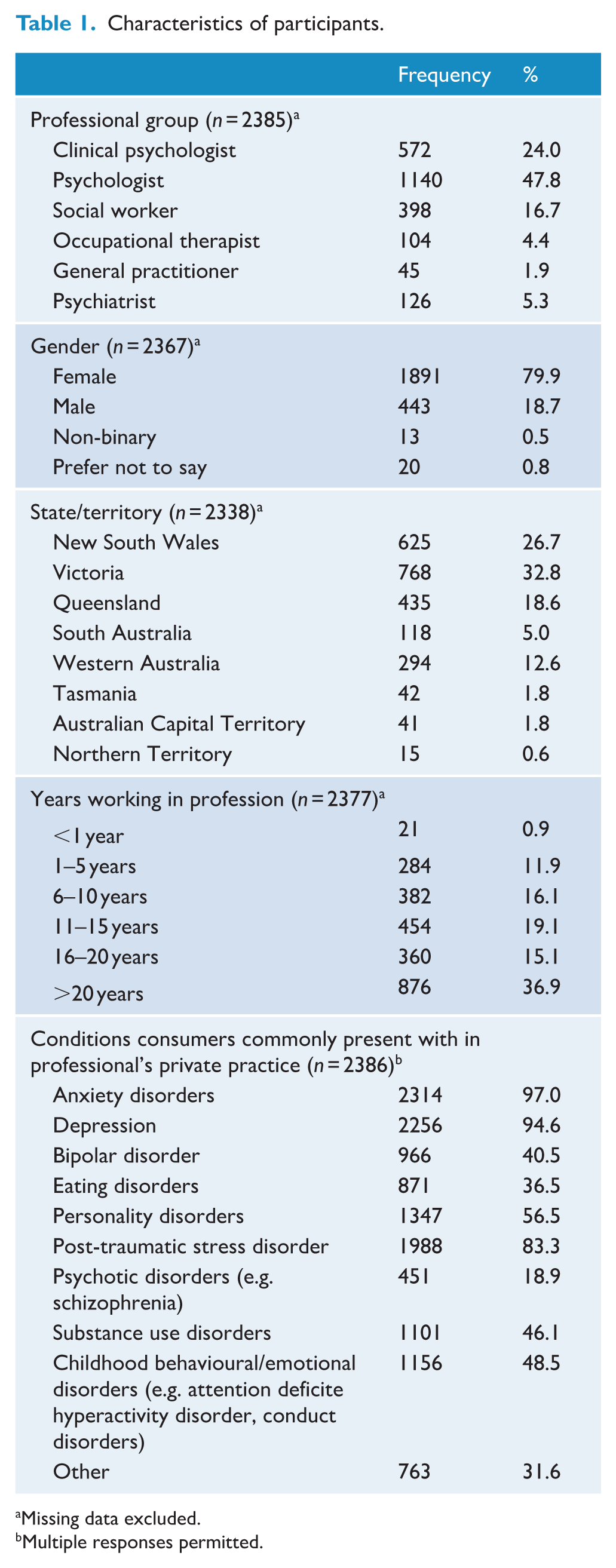
Missing data excluded.
Multiple responses permitted.
Survey
Survey questions were developed by the evaluation team and modified with feedback from DHAC, the CAG and the SEG (see Pirkis et al., 2022 for the final version). First, participants were asked about their demographic, professional and practice characteristics. Second, participants were asked if they had delivered services of each type relevant to their professional group (pop-up boxes showed the MBS items as a memory aid). Third, participants indicated their level of agreement with statements about the processes and outcomes of Better Access on a 5-point Likert-type scale (1 = Strongly disagree; 2 = Disagree; 3 = Neither disagree nor agree; 4 = Agree; 5 = Strongly agree). Fourth, participants selected barriers and facilitators to delivering Better Access services from a list. The different provider and referrer groups were asked different sets of questions about processes/outcomes and barriers/facilitators based on the different types of services they provide under Better Access. Finally, participants indicated their level of agreement with a series of overarching statements about Better Access (same Likert-type scale as above). At various points in the survey, open-ended options allowed participants to provide additional information.
Data analysis
Closed-ended responses were summarised as frequencies and percentages (or medians and inter-quartile ranges [IQR]) using Stata version 17. Open-ended responses were grouped by provider type and were coded using a deductive approach in NVivo version 12.
Ethics approvals
The University of Melbourne Human Research Ethics Committee approved the study (2021-22854-23484-3).
Results
Allied health professionals
Among allied health professionals (n = 2214), most who completed the survey (79–99%, depending on profession) had provided treatment under Better Access in 2021 (see Supplemental Material Table S2). The median number of consumers seen per provider ranged from 20 (OTs) to 60 (clinical psychologists and psychologists). Of the few who had not provided Better Access treatment, most delivered similar services through other programmes/funding mechanisms. Few (4–7%) had provided group treatment sessions. Reasons for not providing group treatment sessions included that groups were hard to arrange, were difficult to run during the COVID-19 pandemic, the rules (i.e. requirements which must be met by the provider to use the MBS item) were difficult to meet (e.g. minimum of six consumers per group), and a lack of appropriate training or physical space (see Supplemental Material Table S3).
In response to survey statements about processes and outcomes, most allied health professionals agreed that Better Access enabled them to provide care that improved consumers’ symptoms, functioning and overall mental health. The majority agreed that Better Access enabled them to offer appropriate and accessible care. However, one quarter to one half disagreed that it enabled them to offer timely and affordable care (Table 2).
Allied health professionals’ views on the processes and outcomes of providing Better Access care.
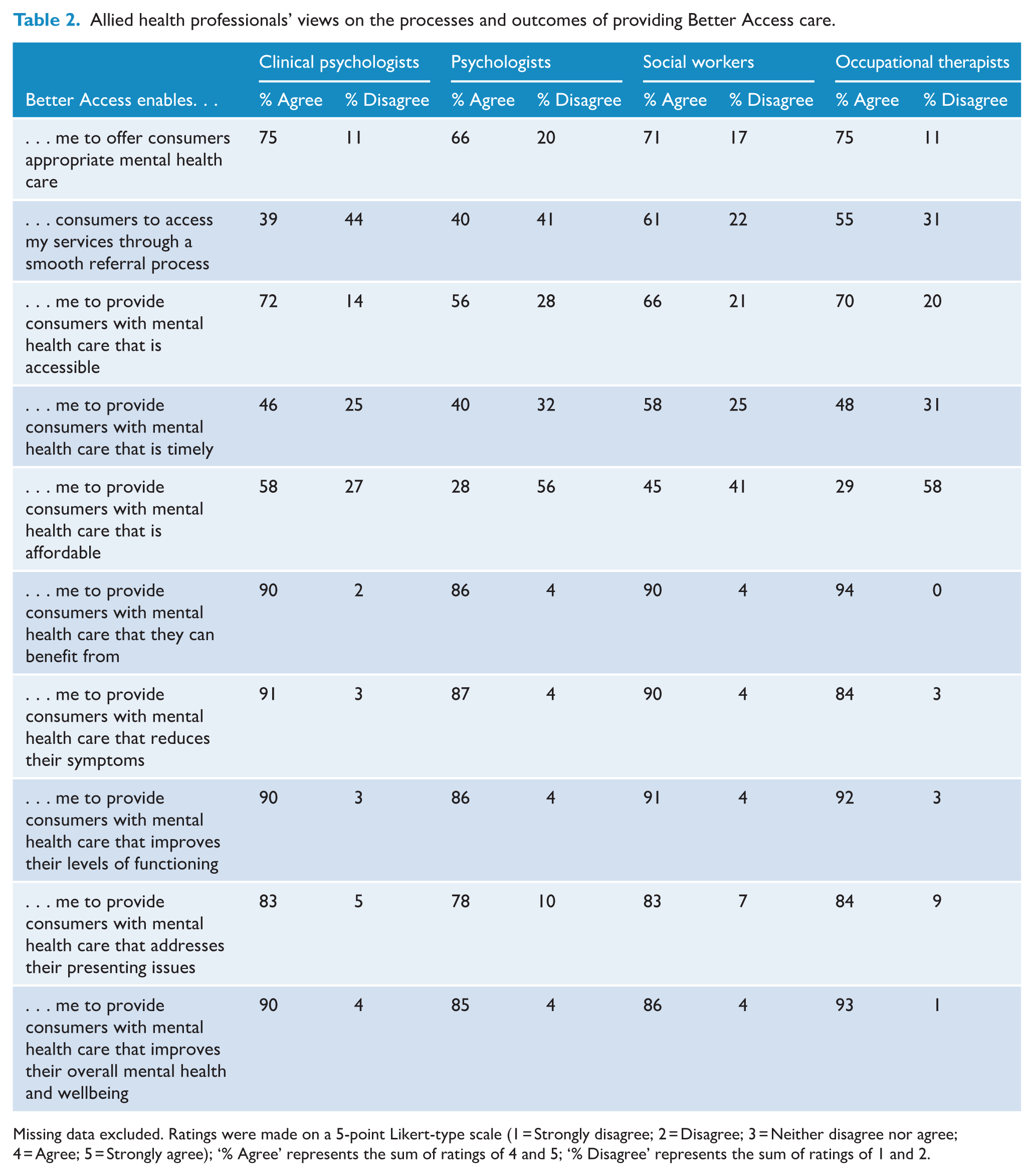
Missing data excluded. Ratings were made on a 5-point Likert-type scale (1 = Strongly disagree; 2 = Disagree; 3 = Neither disagree nor agree; 4 = Agree; 5 = Strongly agree); ‘% Agree’ represents the sum of ratings of 4 and 5; ‘% Disagree’ represents the sum of ratings of 1 and 2.
In their open-ended responses, some allied health professionals elaborated on affordability issues, saying they charged significant co-payments because the Medicare rebates were too low, resulting in prohibitive costs for some consumers. On timeliness, some indicated that they and their colleagues were at capacity, leading to long wait lists. Some recommended that eligibility be extended to other providers (e.g. provisional psychologists, accredited counsellors) to help meet demand. Others noted the importance of credentialing and support for an expanded workforce.
Key barriers to Better Access identified by allied health professionals were: GP referral and review processes were not always smooth, inadequate Medicare rebates, the fee-for-service model not rewarding good practice, and confusing Better Access rules (Table 3). Criticisms voiced in the open-ended comments about referrals included that GPs acted as ‘gatekeepers’ and that consumers should be able to self-refer, and mental health treatment plans were often incomplete or of poor quality. Some noted that wait times for GPs could be lengthy, particularly in regional areas. Some social workers and OTs said many GPs were unaware they provided Better Access treatment, so were unlikely to refer to them. Regarding the review process, some noted that it was administratively burdensome, generated little useful feedback, interrupted, delayed, or even curtailed consumers’ treatment and created an additional cost barrier for consumers. Some equated the referral and review process to a mistrust of their professionalism and said they should be permitted to determine the need for, type and duration of treatment.
Allied health professionals’ perceived barriers and facilitators to the provision of Better Access care.
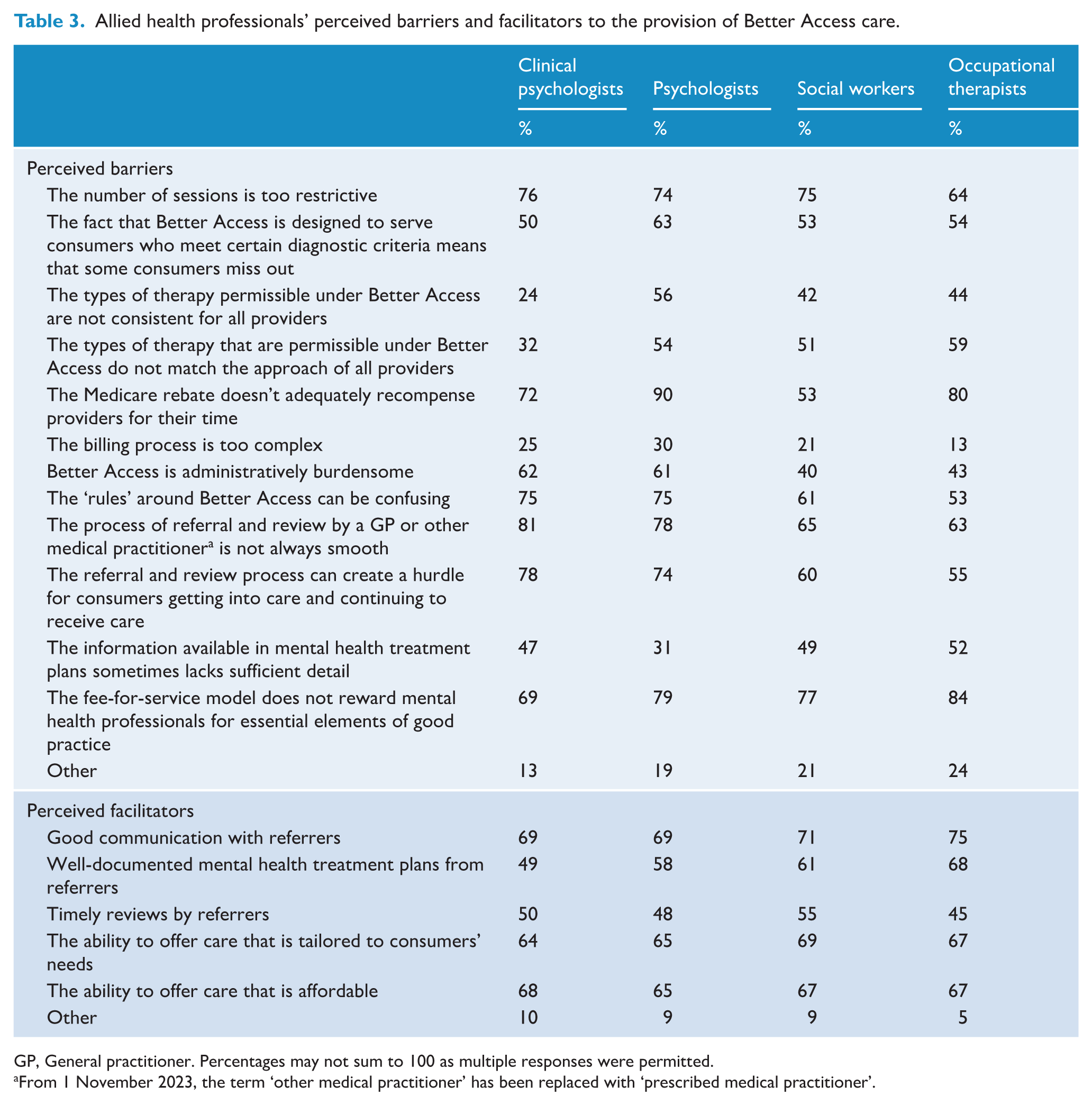
GP, General practitioner. Percentages may not sum to 100 as multiple responses were permitted.
From 1 November 2023, the term ‘other medical practitioner’ has been replaced with ‘prescribed medical practitioner’.
Allied health professionals commented that Medicare rebates were too low to sustain a viable private practice, particularly given the administrative load (e.g. writing reports and letters). As a result, some saw fewer Better Access consumers, charged significant co-payments, or opted out of Better Access provision altogether, further reducing the pool of available providers. Psychologists, social workers and OTs indicated they had to charge higher co-payments than clinical psychologists (whose services attract higher rebates), which they viewed as having impacted demand for their services and influenced GPs’ referral decisions. Demand for clinical psychologists was perceived as outstripping supply, resulting in longer wait lists.
With respect to Better Access rules, some commented that the types of therapy currently permitted were too restrictive compared to the evidence base for effective treatments. Family and couples therapy was noted as a particular gap. Some recommended expanding services for young people (e.g. children in need of early intervention due to trauma; educational/developmental assessments) and improving quality of care by facilitating case conferencing. Some considered the number of treatment sessions permitted too restrictive and an impediment to offering the most appropriate care for consumers with some diagnoses (e.g. personality disorders) and with severe problems and complex needs.
Frequently endorsed facilitators of Better Access care were good communication with referrers and the ability to offer affordable care tailored to consumers’ needs (Table 3). Some commented that the very existence of Better Access had improved access to psychological care for many people. Telehealth was considered an important addition, particularly for those in rural/regional areas. The additional 10 sessions were considered a facilitator of appropriate care for some individuals’ circumstances.
General practitioners
GPs (n = 45) were asked about their views on referring consumers to allied health professionals for Better Access care. Almost all GPs (96%) in our sample had completed mental health skills training and had prepared or reviewed mental health treatment plans in 2021; these GPs had prepared plans for a median of 50 consumers (IQR 20-100) (see Supplemental Material Table S4). GPs referred most consumers with a plan to an allied health professional for treatment, usually to a psychologist (93%) or clinical psychologist (91%). The most common bases for referral decisions were matching the provider’s expertise with consumer needs (83%) and choosing providers they knew (74%).
In response to the statements about referral processes and outcomes, most GPs agreed that Better Access enabled them to refer consumers for appropriate, potentially beneficial mental health care, which improved their symptoms and levels of functioning (Table 4). Around half agreed that the referral process is straightforward, although one-third disagreed. Many disagreed that Better Access fostered good two-way communication between GPs and mental health professionals, that referral pathways are smooth and resulted in accessible and timely care.
General practitioners’ views on processes and outcomes of referring to allied health professionals and providing Better Access care.
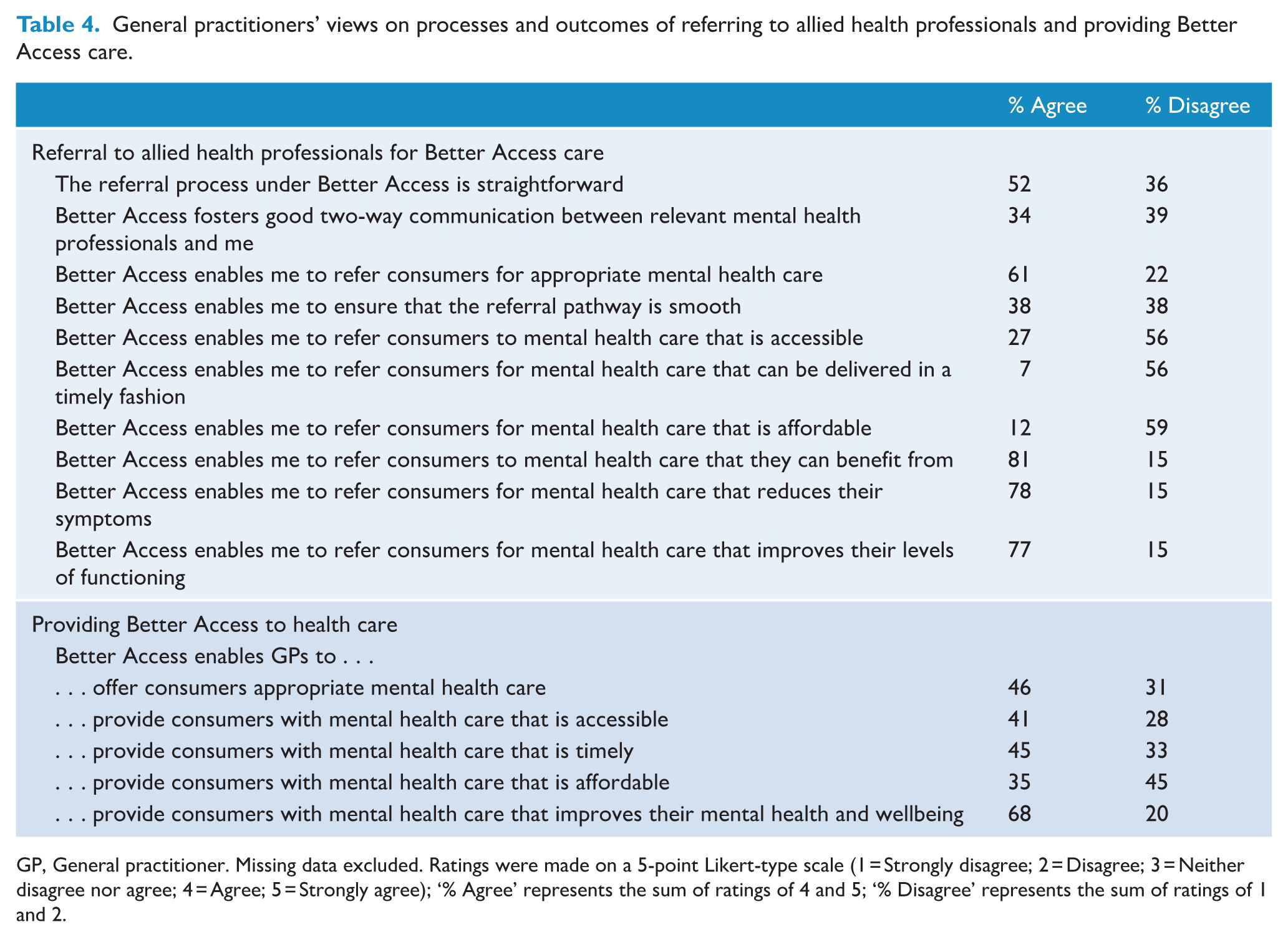
GP, General practitioner. Missing data excluded. Ratings were made on a 5-point Likert-type scale (1 = Strongly disagree; 2 = Disagree; 3 = Neither disagree nor agree; 4 = Agree; 5 = Strongly agree); ‘% Agree’ represents the sum of ratings of 4 and 5; ‘% Disagree’ represents the sum of ratings of 1 and 2.
In open-ended responses, many GPs said the referral process was cumbersome, differed from other specialist referrals and imposed time and cost burdens on consumers. Some questioned the appropriateness of the GP's ‘gatekeeper’ function, given the maturity of Better Access and the professionalism of treating providers. Some said reviews were not always necessary, occurred too early in the course of care, or treating provider reports were sub-optimal (e.g. late, poor quality or non-existent). By contrast, others stated that reviews supported high-quality consumer care (e.g. by fostering good communication between providers). Regarding accessibility and timeliness of care, some noted that finding appropriate and available allied health professionals to refer to was increasingly difficult.
Regarding their experiences in providing Better Access care themselves, three-quarters of GPs (74%) had used the mental health consultation items, for a median of 50 consumers (IQR 20–100). The most common reason for not using these items was having provided mental health care under non-Better Access MBS items (67%). One quarter (23%) had used the focused psychological strategies items with a median of 35 consumers (IQR 3–70). The most common reasons for not using these items were having instead used the mental health consultations items (46%) or non-Better Access MBS items (41%).
In response to the statements about providing care, most GPs agreed that Better Access enabled them to provide care that yielded improvements in consumer mental health (Table 4). Just under half agreed that it enabled them to offer appropriate, accessible and timely care. A similar percentage disagreed that Better Access enabled the provision of affordable care. In open-ended responses, some noted that a substantial amount of mental health care was delivered informally (e.g. supporting consumers waiting to see an allied health professional, providing services in areas with few allied health professionals). Others remarked that GP-focused psychological strategies items are counted towards the consumer’s session quota; this introduces a model where care is provided per a quota, rather than according to what is needed to foster holistic and comprehensive care.
Barriers to Better Access endorsed by GPs included long wait lists to see allied health professionals, lack of available allied health professionals, inadequate Medicare rebates and confusing rules (Table 5). GPs’ comments about affordability and timeliness echoed those of allied health professionals. They noted that long wait times (because providers are at capacity or unavailable) resulted in some consumers dropping out of the process of seeking care. Inadequate Medicare rebates impacted the viability of private practice for allied health professionals, resulting in low bulk-billing rates and high co-payments for consumers. GPs also noted confusion around Better Access rules relating to consumer eligibility, billing, and session numbers, and difficulty obtaining information about rule changes.
General practitioners’ perceived barriers and facilitators to the provision of Better Access care.
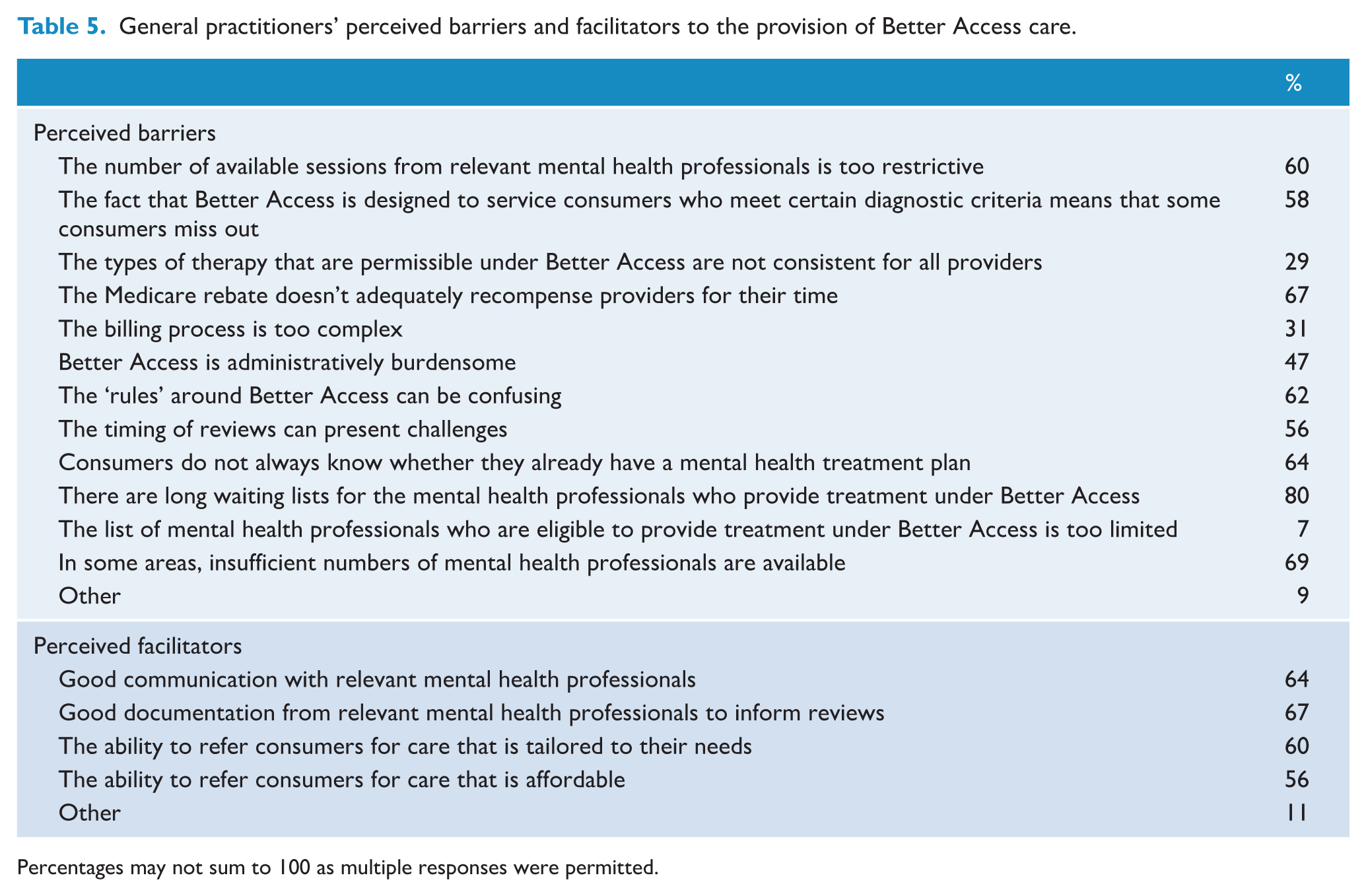
Percentages may not sum to 100 as multiple responses were permitted.
There was strong agreement among GPs that good communication with allied health professionals, good documentation from these professionals to inform reviews, and the ability to refer consumers for tailored care were facilitators of care (Table 5).
Psychiatrists
In our sample of psychiatrists (n = 126), over half (54%) had provided services under Better Access in 2021 for a median of 25 consumers (IQR 5–50) (see Supplemental Material Table S5). Of those who had not provided services under Better Access, most said it was because they had provided equivalent services using non-Better Access MBS items (72%). Others cited high compliance burden, lack of relevance to their practice focus, not taking on new consumers in 2021, and being unaware of Better Access or how to use it. Some said they had not prepared a psychiatrist assessment and management plan because it could be hard to ascertain whether the MBS item had been claimed in the past 12 months (leading to the claim being rejected); others were concerned that the item does not allow for follow-up sessions with the psychiatrist. Of the psychiatrists who prepared a plan or conducted an initial consultation, most had referred consumers on to an allied health professional, usually a psychologist (72%).
In response to the statements about processes and outcomes, almost half of psychiatrists agreed that Better Access helped them ensure consumers get care that addressed their presenting issues (Table 6). The majority disagreed that Better Access enabled timely care and almost half disagreed that it enabled affordable and accessible care.
Psychiatrists’ views on processes and outcomes of seeing consumers under Better Access.
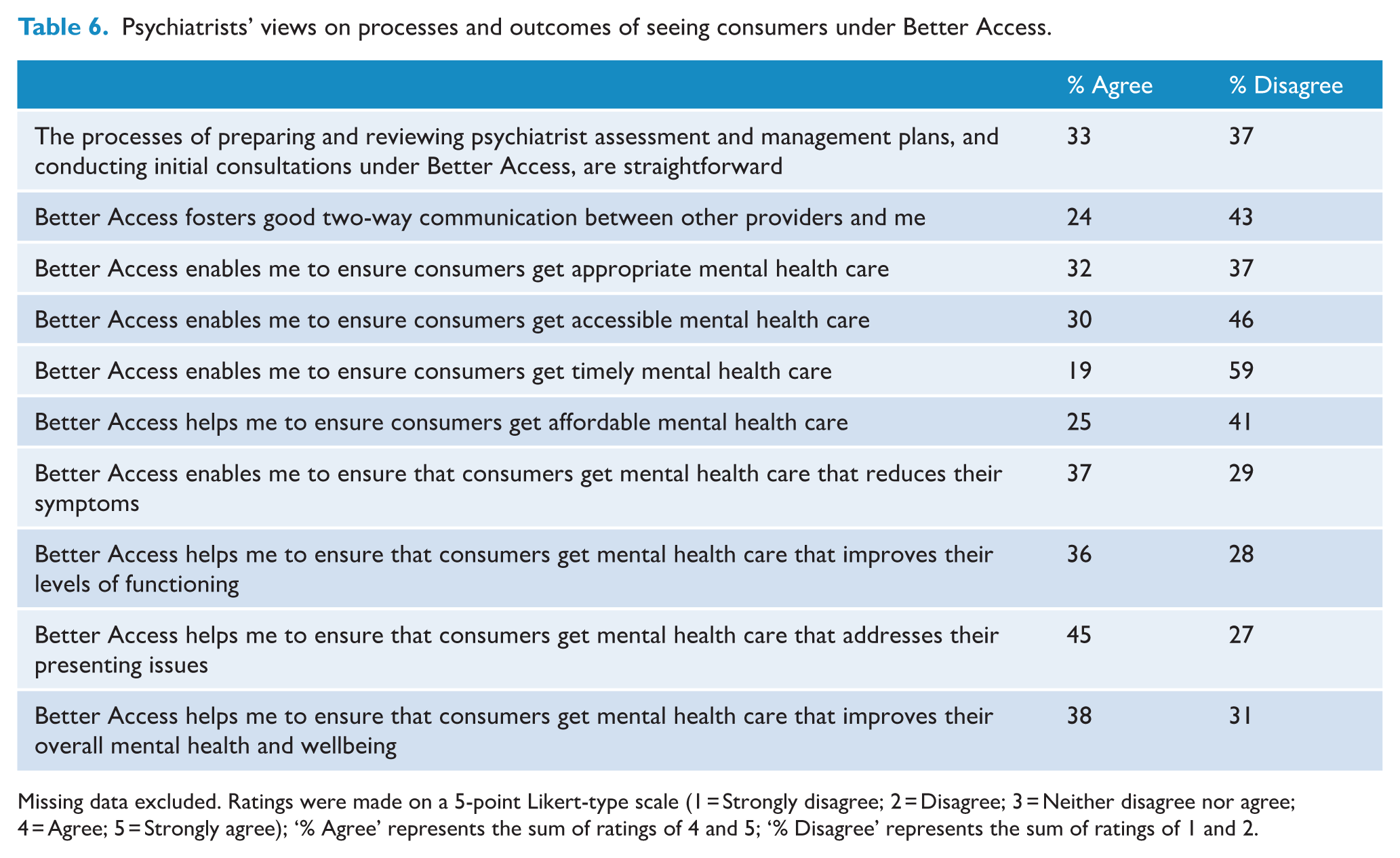
Missing data excluded. Ratings were made on a 5-point Likert-type scale (1 = Strongly disagree; 2 = Disagree; 3 = Neither disagree nor agree; 4 = Agree; 5 = Strongly agree); ‘% Agree’ represents the sum of ratings of 4 and 5; ‘% Disagree’ represents the sum of ratings of 1 and 2.
Regarding addressing consumers’ presenting issues, some psychiatrists commented that they typically saw consumers with severe and complex problems and allied health professionals might not be able to provide the appropriate type or intensity of care. Others were more positive, noting that Better Access promoted holistic care by making the services of psychiatrists and allied health professionals available in tandem. Psychiatrists also noted, similar to allied health professionals and GPs, that low rebates resulted in higher co-payments that discouraged consumers from engaging in care. Regarding accessibility, like GPs, some psychiatrists commented on the lack of available psychologists to refer.
On Better Access processes, some psychiatrists commented that mental health treatment plans from GPs could be poor and that standard referral processes would be an adequate, less costly alternative. Better Access reporting requirements were viewed as excessive. Recommended changes included: adding MBS items for delivering parent-only sessions for children and for case conferencing; increasing the session quota for selected problems or conditions (e.g. trauma, personality disorders) and expanding the range of eligible providers (e.g. mental health nurses).
All providers and referrers
Across all participants, the majority agreed that Better Access had improved outcomes for consumers. A majority disagreed that Better Access administrative processes were straightforward and that the rules made sense (Table 7).
All participants’ views on Better Access.
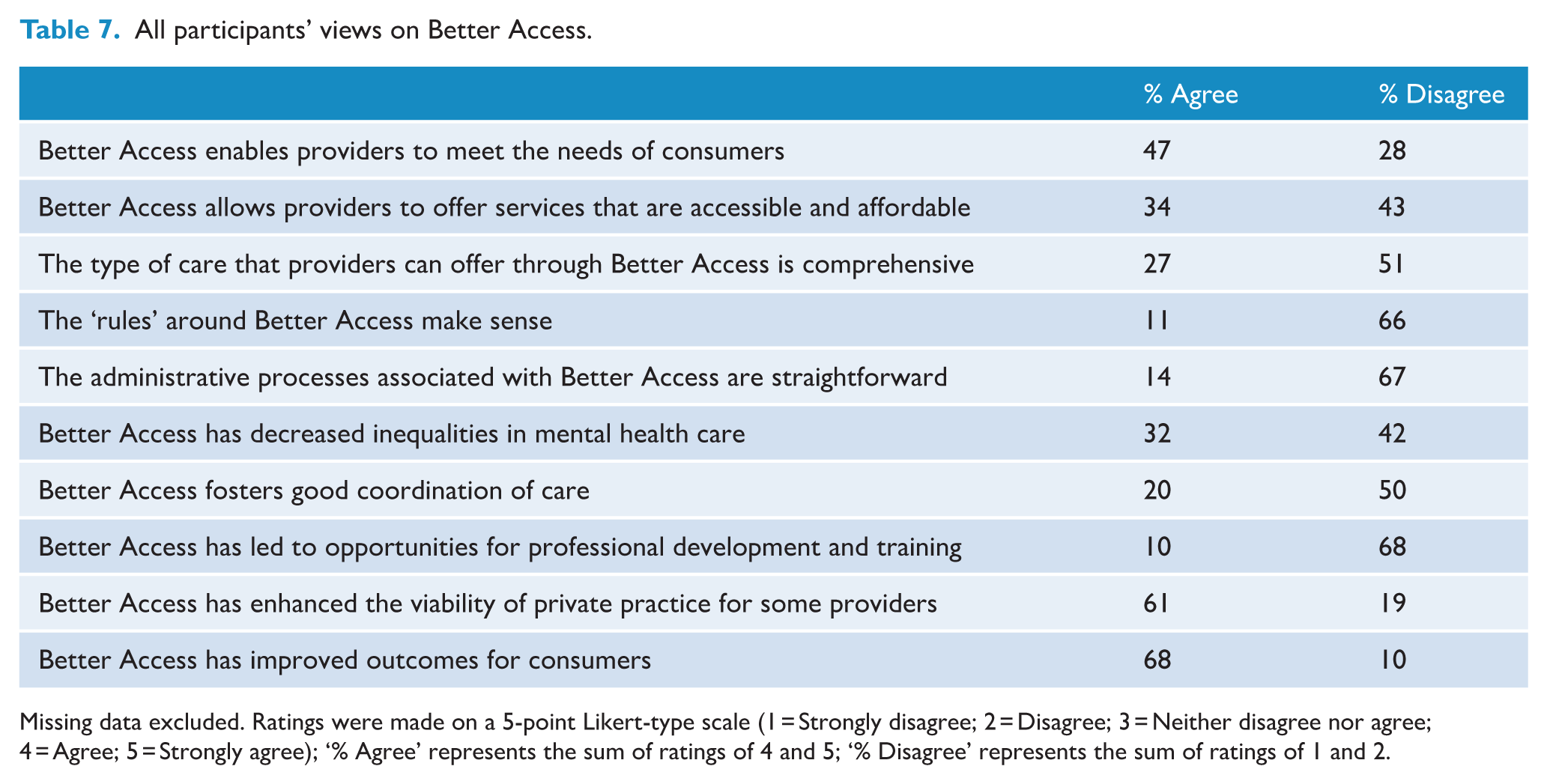
Missing data excluded. Ratings were made on a 5-point Likert-type scale (1 = Strongly disagree; 2 = Disagree; 3 = Neither disagree nor agree; 4 = Agree; 5 = Strongly agree); ‘% Agree’ represents the sum of ratings of 4 and 5; ‘% Disagree’ represents the sum of ratings of 1 and 2.
Discussion
We found that eligible providers and referrers consider Better Access to be meeting consumers’ needs. In all professional groups, at least 70% agreed that Better Access enables delivery of care that improves consumers’ mental health and is appropriate for and tailored to consumer needs. The telehealth items and temporary additional 10 treatment sessions were viewed as enabling appropriate care for more consumers. Some improvements to address service provision gaps were suggested including relationship/couples therapy, developmental assessments and other services for young people, and new MBS items to encourage more collaborative care. This is consistent with Productivity Commission (2020) recommendations to: maintain access to telehealth, make additional sessions permanently available for people with complex needs and add MBS items to facilitate collaborative care. Since the completion of our study, selected telehealth/phone services have been made permanent, while the additional sessions ceased in December 2022 (Department of Health, 2022a, 2022b). New items have been introduced which allow allied health professionals and GPs to provide up to two sessions to family/carers to support the treatment and recovery of a consumer (March 2023), and enable providers to coordinate/participate in case conferences (July 2023) (DHAC, 2023b, 2023c). The impacts of these changes on the quality of care and consumer outcomes should be monitored.
In our survey, all professional groups expressed concerns about wait times due to increased demand for services and allied health professionals reducing or opting out of providing Better Access services. Participants recommended expanding the array of eligible providers, supported by training and supervision, to help meet demand. Wait times to access services are a known issue for mental health services more broadly (ABS, 2021; headspace, 2019) and are likely related to documented increases in mental ill-health (Enticott et al., 2022). Workforce capacity issues have been identified system-wide, with moderate under-provision identified across nearly all mental health provider categories (DHAC, 2022b). The Australian Government’s 2023-24 budget included a commitment of $91.3 million over 5 years to increase workforce capacity through additional post-graduate placements, internships and supervisor training sessions (Commonwealth of Australia, 2023).
High out-of-pocket costs were attributed to inadequate Medicare rebates and seen as impacting negatively on consumer engagement, particularly among those with low incomes. Affordability issues have arisen in part due to a freeze on indexation of Medicare fees between 2013 and 2019 and the rising cost of living (Australian Medical Association, 2022; Duckett et al., 2022) and affect many Medicare-funded services (Angeles et al., 2023). Proposed strategies to reduce out-of-pocket costs include bulk-billing incentives in some areas, loadings on specific items, and higher rebates for consumers who spend above a threshold amount (MBS Review Taskforce, 2020). Broader reforms, such as those recommended in recent inquiries (e.g. Productivity Commission, 2020), are likely required to address consumer engagement with treatment and the availability of alternative interventions and models of care.
Our findings highlight issues with Better Access referral processes. Participants indicated that the treatment planning and referral pathways are key facilitators of Better Access care, but may not always work optimally. The quality of mental health treatment plans was a common concern; additional educational material may be needed. Allowing consumers to self-refer and implementing less cumbersome methods of referral and review were recommended. Some referrers were unaware they could refer to social workers and OTs; local service directories listing allied health professionals providing Better Access services may be one way to address this, but would need to be kept up-to-date.
Our findings shed light on why some Better Access items are not well utilised. For example, although group treatment sessions are more cost-effective and less expensive for consumers (Productivity Commission, 2020), few allied health professionals had delivered them. Since our survey was conducted, group treatment session requirements have been modified (DHAC, 2022a); these changes address some barriers voiced by our survey participants (e.g. lowering the minimum number of consumers) but not others (e.g. training needs). Our study corroborates previous findings that many GPs do not use the focused psychological strategies items (GP Mental Health Standards Collaboration, 2021; Royal Australian College of General Practitioners, 2022), partly because only a limited number of these sessions are available to consumers. The MBS Review Taskforce (2020) recommended allowing consumers to receive up to 10 sessions from GPs regardless of the number received from allied health professionals.
Strengths and limitations
This is the largest study of provider and referrer views of Better Access. Participants were recruited systematically, using methods designed to increase participation, but it was not possible to determine response rates because we do not know how many saw the invitations. We cannot determine how representative our participants were of providers in their respective professions, partly due to the lack of published information about the characteristics of Better Access service providers. However, the larger proportion of females in our sample is consistent with workforce data showing that the vast majority of allied health professionals (who made up the majority of our participants) are female (Australian Institute of Health and Welfare, 2023).
The number of participants from each profession broadly reflects the distribution of Better Access services delivered across each profession (Tapp et al., 2026), although we had relatively fewer GP participants. Lower participation rates in research among GPs are not uncommon, with lack of time being the most common reason (McKinn et al., 2015; Parkinson et al., 2015). Our GP sample may be more likely to use Better Access items than average; three-fourths had used the mental health consultation items (whereas GPs more often use general attendance items), and almost a quarter had provided focused psychological strategies (vs 3.5% of GPs registered to do so) (GP Mental Health Standards Collaboration, 2021). Therefore, our results might generalise best to GPs with an interest in mental health. The retirement of the mental health consultation and review items from 1 November 2025 is intended to reduce administrative complexity but could impact the ability to track GP mental health activity (Australian Government Department of Health, Disability and Ageing, 2025).
Conclusion
Most providers and referrers were positive about the outcomes that Better Access achieves for consumers. However, there were concerns that insufficient workforce capacity to meet demand, particularly among allied health professionals, had resulted in delayed access to treatment for some consumers. High out-of-pocket costs were also a significant concern, potentially discouraging less well-off consumers from entering or continuing care. Good communication between referrers and providers was seen as critical to the success of Better Access.
Supplemental Material
sj-docx-1-anp-10.1177_00048674251406056 – Supplemental material for Australia’s Better Access initiative: A survey of provider and referrer views
Supplemental material, sj-docx-1-anp-10.1177_00048674251406056 for Australia’s Better Access initiative: A survey of provider and referrer views by Caley Tapp, Meredith Harris, Dianne Currier, Lisa Brophy, Cathrine Mihalopoulos and Jane Pirkis in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
This study was funded by the Australian Government Department of Health, Disability and Ageing, as part of the broader evaluation of Better Access. We would like to thank the two groups that were constituted to advise on the evaluation, the Clinical Advisory Group and the Stakeholder Engagement Group. We would like to acknowledge the Australian Association of Psychologists Inc., the Australian Association of Social Workers, the Australian Clinical Psychology Association, the Australian College of Rural and Remote Medicine, the Australian Psychological Society, the Institute of Clinical Psychologists, Occupational Therapy Australia, the Royal Australian and New Zealand College of Psychiatrists and the Royal Australian College of General Practitioners for assisting us with recruiting participants. We would also like to thank all of the providers and referrers who completed the survey.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The Better Access Evaluation was funded by the Australian Government Department of Health, Disability and Ageing.
Data availability statement
The datasets generated and analysed for the current study are not available.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.