
Abstract
Objective:
The Better Access initiative enables clinical psychologists, psychologists, social workers and occupational therapists to offer sessions of psychological treatment to people with common mental disorders. Better Access services are listed on the Medicare Benefits Schedule which means that consumers only pay a percentage of the cost. This study sought the views of users and non-users of Better Access about the programme’s accessibility, appropriateness and outcomes.
Methods:
We conducted semi-structured interviews with participants recruited via two national lived experience networks: Beyond Blue’s BlueVoices and Lived Experience Australia.
Results:
We interviewed 23 people who had used Better Access in 2021 and 14 who had not. Participants suggested that, in general, Better Access operates smoothly, allows people to access high-quality care, and yields positive outcomes (e.g. improved functioning, reduced symptoms). However, they indicated that although Better Access makes care more affordable, out-of-pocket costs can still be prohibitive. They also queried whether the number of sessions available through the programme is sufficient.
Conclusion:
Better Access has many strengths, but it meets the needs of some better than others. Future reforms to Better Access should address accessibility and affordability.
Keywords
Introduction
In 2021–2022, we were commissioned by the then Department of Health to conduct an evaluation of the Better Access to Psychiatrists, Psychologists and General Practitioners through the Medicare Benefits Schedule (MBS) initiative (Better Access). Better Access was introduced in 2006 to provide free/low-cost, evidence-based psychological treatment to people with common, mild-to-moderate mental disorders (Australian Government Department of Health, 2021). Under Better Access, general practitioners (GPs) or prescribed medical practitioners (PMPs) prepare a mental health treatment plan (MHTP) and refer consumers with a diagnosed mental disorder to clinical psychologists for ‘psychological therapy services’ or to psychologists, social workers or occupational therapists (OTs) for ‘focussed psychological strategies’. The referring GP/PMP subsequently reviews the MHTP. Under the MBS, these services are associated with various item numbers and attract a rebate which is paid to consumers as a percentage of the schedule fee. Providers can charge above the schedule fee, and consumers cover the difference between the rebate and what the provider charges.
Better Access has evolved over time and continues to do so. Currently, consumers can access up to 10 individual sessions for psychological therapy services or focussed psychological strategies, with a review after the first six (Australian Government Department of Health and Aged Care, 2022). During the COVID-19 pandemic, when we conducted our evaluation, the individual-session number was temporarily increased to 20 and sessions were made available through additional modalities (telehealth/phone, as opposed to face-to-face only). The session cap reverted to the original 10 as planned at the end of 2022 (Australian Government Department of Health, 2022b), but the telehealth/phone options were retained (Australian Government Department of Health, 2022a). More recently, additional changes have been made to the arrangements relating to GPs/PMPs. The preparation of MHTPs, referral for treatment and reviews of MHTPs have been linked to GPs/PMPs in consumers’ MyMedicare practices or to their usual medical practitioners (Australian Government Department of Health Disability and Ageing, 2025). MHTP review item numbers have been removed from the MBS, and GPs/PMPs can now use general attendance item numbers instead (Australian Government Department of Health Disability and Ageing, 2025).
Our evaluation followed a previous one we had conducted in 2009–2011 (Pirkis et al., 2011). One component of the earlier evaluation involved surveys/interviews with 936 people who had used Better Access (Ftanou et al., 2014). Most were positive about the programme, with many noting that it gave them unprecedented access to beneficial mental health care. Some, however, said that affordability was a barrier.
In the current evaluation, we felt that it was imperative to once again hear from people with lived experience of mental disorders who had used Better Access. This time, we also endeavoured to seek the views of people with lived experience who had not used Better Access. We conducted the qualitative study reported here with the aim of eliciting the views of a range of participants in an in-depth way (Pope et al., 2000). This study complemented the others in the evaluation that are also reported in this issue of the Australian and New Zealand Journal of Psychiatry (Arya et al., 2026; Chilver et al., 2026; Currier et al., 2026; Harris et al., 2026; Pirkis et al., 2026a, 2026b; Tapp et al., 2026b; Tapp et al., 2026a) are described in this issue of the Australian and New Zealand Journal of Psychiatry. Like the other studies, this study was informed by a Clinical Advisory Group (CAG), comprising individual mental health professionals who deliver Better Access services, and a Stakeholder Engagement Group (SEG), comprising representatives from the mental health sector, including people with lived experience of mental disorders.
Methods
Participant recruitment and profile
A call for expressions of interest (EOIs) to participate was circulated via two national lived experience networks: Beyond Blue’s BlueVoices and Lived Experience Australia. Individuals needed to be aged ⩾18 and have a lived experience of a mental disorder to be eligible. They were asked for some socio-demographic details and information about their mental health, and whether, in the past year, they had received treatment services from a psychologist, social worker or OT that were paid for, at least partially, by Medicare. Because 97% of MBS mental health services delivered by allied health professionals are provided through Better Access (Australian Institute of Health and Welfare, 2023), this gave us confidence in deeming potential participants to be past-year ‘Better Access users’ or ‘Better Access non-users’.
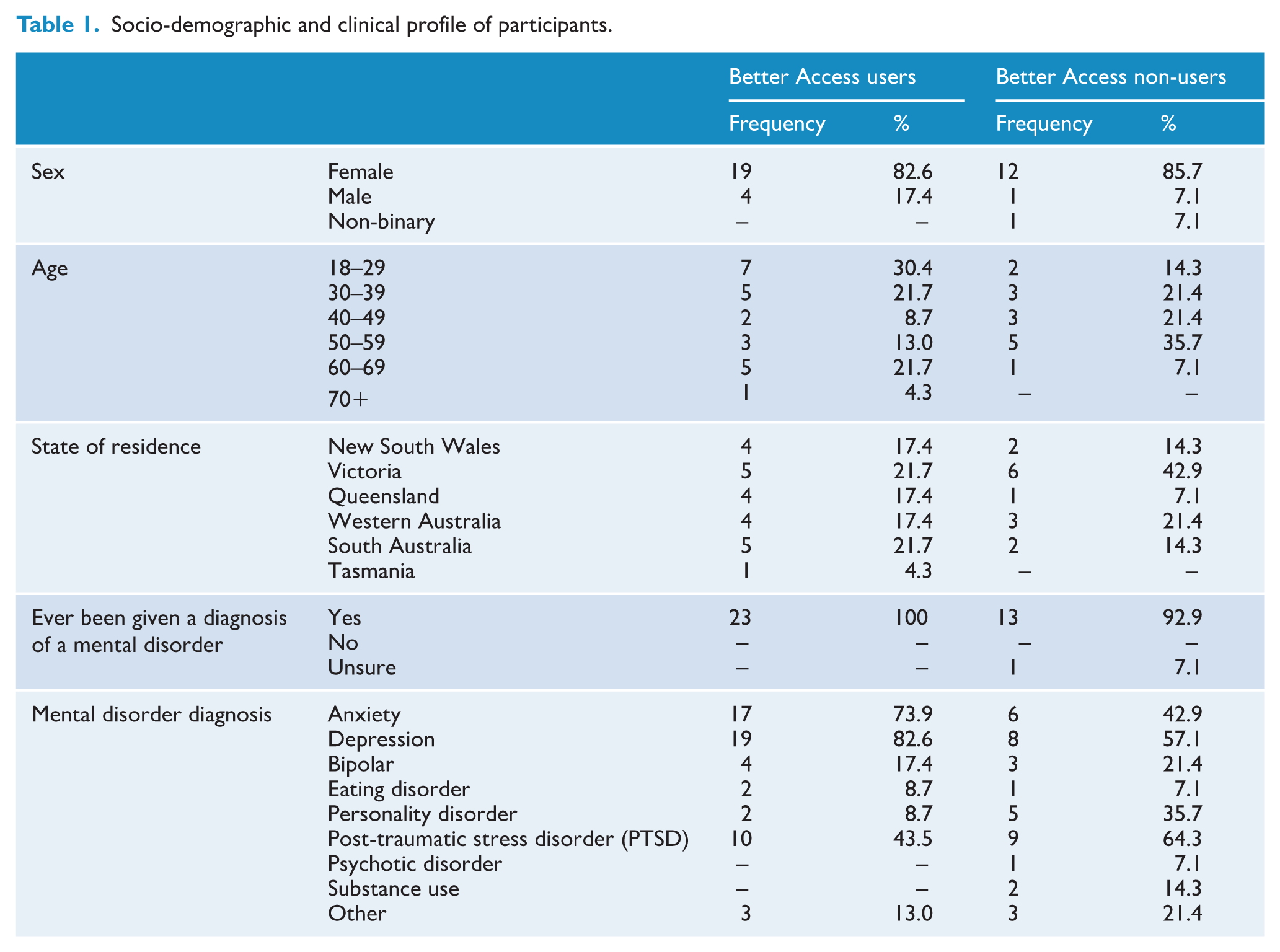
Fifty-six individuals submitted EOIs. Interviews could not be arranged with 17, and 2 were ineligible (1 carer and 1 advocate). We conducted 37 interviews, 23 with Better Access users and 14 with Better Access non-users (Table 1). Most users and non-users were female (83% and 86%, respectively). Better Access users were mostly aged 18–29 (30%), whereas non-users were mostly aged 50–59 (36%). Most Better Access users were from South Australia (22%) and Victoria (22%). The majority of non-users were from Victoria (43%). All of the Better Access users and all-but-one of the Better Access non-users had been given a mental health diagnosis at some point. Among Better Access users, the commonest diagnoses were depression (83%), anxiety (74%), and post-traumatic stress disorder (PTSD; 44%). Among non-users, the same diagnoses topped the response list, although they were ordered differently: PTSD (64%), depression (57.1%) and anxiety (43%).
Socio-demographic and clinical profile of participants.
Interview procedures and content
Interviews were semi-structured. The questions were developed iteratively, with CAG and SEG input. Interviews were conducted by D.N. or M.W. in January–March 2022, took place via Zoom or phone, and averaged 40 minutes (range: 22–59 minutes). Participants were asked about the accessibility and appropriateness of Better Access, outcomes of treatment they received through Better Access or alternative pathways, and their views on potential improvements to Better Access. Interview schedules are available as Electronic Supplementary Material (ESM1 and ESM2).
Data management and analysis
Interviews were recorded and transcribed. D.N. and M.W. conducted the analysis in NVivo 12, initially using a deductive approach to develop a broad coding framework organised around the interview questions and then using an inductive approach to refine the framework to organise the full range of responses thematically. They initially coded two interviews independently and then refined the framework to address any disagreements.
Percentages of participants whose responses related to any given theme are not presented because the interviews’ semi-structured nature meant that although the same questions were initially used, the interviewers ‘drilled down’ further on some issues with some participants so participants were not all asked precisely the same questions (Monrouxe and Rees, 2020).
Ethics approval
The University of Melbourne Human Research Ethics Committee (2022-22921-26065-4) granted approval. All participants verbally consented.
Results
Better Access use/non-use
All Better Access users said they had seen a psychologist in the past year; none reported seeing a social worker or an OT. Non-users most commonly indicated that they had not used Better Access in the past year because they were seeking support through other services/providers or funding schemes, but many had used Better Access in earlier years.
The referral process
The majority of Better Access users were positive about the referral process. Most reported that they had made an appointment with their GP specifically to request a MHTP, and most – though not all – of those who read their plan reported that it accurately represented the way they were feeling.
So I don’t remember the exact detail but I know relative to the state I was in at the time I think it matched up . . . (Better Access user)
Most Better Access users reported that the referral process was smooth. Many did not have a specific mental health professional in mind when they received a MHTP and were referred to a psychologist selected by the GP. For some this was a good match.
I just went with the recommended psychologist. [T]hankfully for me that psychologist was a great fit for me and it’s still the psychologist that I see to this day, so I think I was very lucky. (Better Access user)
For other Better Access users, finding the right provider took time and consumed some of their available sessions. Better Access non-users also noted that finding someone who was the right ‘fit’ was a barrier to their using Better Access.
I found one [psychologist] and then I had to go through a couple to find who I was happy with. (Better Access user) . . . I didn’t feel like the hassle . . . was worth it. . . . it’s the whole process, like if I just had to go to the GP and get a plan it would be okay, but it’s the then finding somebody, the GP can never suggest anybody particularly . . . (Better Access non-user)
The review process
Many Better Access users questioned the requirement to see the GP for a review after six sessions.
Yeah, and I don’t fully understand the reasoning between having six, getting a new care plan, getting an extra four . . . (Better Access user)
Some noted that the review process was a missed opportunity for communication between the GP and the psychologist.
I don’t think they communicated. He filled out the form, sent the form to her and she just told me that she’d received the form. That’s basically it . . . (Better Access user)
Format of sessions
Most Better Access users received both face-to-face and telehealth/phone sessions. Face-to-face sessions were preferred by the majority. Being face-to-face meant that the consumer and the psychologist could pick up on non-verbal cues, develop rapport and establish mutual trust, and engage confidentially without interruptions.
Yeah I definitely prefer face-to-face. [I]t feels safer somehow . . . I find often with telehealth you know because I live with other people it can be difficult to . . . to carve out time that’s private and that won’t be overheard, and when it’s in person I know that there’s like this little cocoon that we’re in for that time, and . . . I won’t be interrupted and I won’t be overheard . . . whatever we discuss is just between us . . . (Better Access user)
Telehealth (and to a lesser extent phone) sessions were seen by many Better Access users as acceptable when face-to-face sessions were not possible. Some non-users also commented that telehealth made Better Access more appealing.
I think I’d always prefer face-to-face but it is very convenient to be able to see her via Zoom because it saves travel time . . . when I saw her in Sydney it was 1½ hours door-to-door . . . (Better Access user) . . . Sometimes it’s better to do it online because if I’m having an anxiety attack about leaving the house you know so there’s some really good things . . . (Better Access user) I am really happy that I don’t have to trudge along because I’ve just been to so many appointments over the last 17 years . . . so I [would be] happy just to do it by telehealth. (Better Access non-user)
By contrast, several participants commented that telehealth (and phone) sessions could be ‘impersonal’ and subject to technological issues.
Oh I didn’t like it. It just seems very impersonal . . . (Better Access user) . . . I think I worry about being dysregulated and having . . . a Zoom issue and then all of a sudden like she’s cut out . . . (Better Access user)
Session numbers
Most Better Access users – particularly those with complex mental health issues – believed that the number of sessions was too few.
So yeah, I guess like with me I feel complex with my mental health history, but I feel like it’s too few even if you don’t have a complex mental health issues. (Better Access user)
Many Better Access users appreciated the additional 10 sessions, although several noted that even these were insufficient.
It’s a great thing that it exists, because without it I wouldn’t have been able to access the amount of care that I have been. And even then . . . even with the 20 sessions it’s not enough. (Better Access user)
Several Better Access non-users referred to limits on session numbers, noting that these influenced their views of the programme.
I just don’t think there was enough sessions. After six it was like just barely getting to know them . . . and then it was over (laughter) so I had to either find another way of paying for it or just wait till the next year. (Better Access non-user)
Almost universally, Better Access users and non-users recommended increasing the session numbers.
. . . you could have more sessions in a year . . . because 10 sessions is really very few unless . . . you have some sort of mild anxiety disorder . . . but for anybody with serious mental health concerns . . . it’s probably not helpful. (Better Access non-user)
Affordability
Both users and non-users of Better Access commented on its affordability. The fact that sessions were available at reduced or no cost was seen as a major advantage by many users.
Definitely the subsidised sessions like the fact that I save $130 or something . . . and get a rebate . . . So . . . that’s probably one of the main things. (Better Access user) . . . I’d be lost without [Better Access] to be honest . . . I can’t afford to be paying the sessions out-of-pocket because I’m on Centrelink . . . (Better Access user)
However, both users and non-users indicated that the programme’s affordability could be improved further, noting that high out-of-pocket costs were a barrier.
And the subsidy isn’t enough. Like the fact that people have to pay $100 out-of-pocket is just . . . not viable because if you look at people with mental health conditions they’re most likely unemployed or have problems with their housing so then how are people supposed to pay $100 for a session. (Better Access user) . . . a lot of practitioners charge above and beyond what the amounts are so you’re probably still going to be out-of-pocket. (Better Access non-user)
Manner and approach of providers
Many Better Access users valued their psychologist’s manner and approach. Experiencing good rapport and feeling safe, comfortable, and accepted were important factors that encouraged participants to continue with treatment.
. . .just feeling like relaxed and comfortable and feeling like I could open up and feeling like I wasn’t going to be judged . . . (Better Access user)
The psychologist’s skills and standards were also seen as important.
I’ve always felt that she was using best practice . . . she knows her stuff. The assessments she gives me are . . . reputable standardised assessments. (Better Access user)
Benefits of using Better Access
All Better Access users reported improvements in their wellbeing since seeing their psychologist. They felt more hopeful and empowered and had a better understanding and acceptance of themselves. Some noted that seeing their psychologist had helped them to return to work, improved their social skills and confidence, improved their sleep or reduced their experience of chronic pain. Others indicated that their psychologist had equipped them with self-management tools which had reduced their symptoms.
Each time I finish a session with her I walk out feeling more hopeful and . . . empowered and more like I’ve got someone who can help me fight this or I’ll manage this and like I do walk out of the sessions feeling a little bit more motivated . . . (Better Access user) . . . she explained to me what was going on in a way that made sense to me, and really helped improve . . . my mental health, like resilience and understanding of things, and it became very helpful to be able to . . . go through things and process things . . . (Better Access user)
Most Better Access users attributed their improvements to the aspects of the psychologist’s manner and approach.
. . . his empathy, his care, I know that he respects me as a person, that he’s very affirming of me in terms of my intelligence. (Better Access user) I think exercises. Whenever I would have something that I was really stressing about just a simple exercise to say ‘’Okay, well when you feel this way, fill out this form’. It would sort of say like ‘What’s the situation? What are your emotions? What are you doing? Are you mindreading? Are you saying should a lot? And how can you better approach this? . . . Like how can you look outside the box? I found that to be really helpful’. (Better Access user)
Use of other services
Both users and non-users discussed the other services they used. These included GPs, psychiatrists, counsellors, hospital psychiatric services, emergency departments and crisis lines, and psychologists, social workers and OTs funded through other channels. For users, these services were often seen as complementary to Better Access. For non-users, they were generally viewed as alternatives.
I saw [the counsellor] maybe once a fortnight . . . and for the most part we . . . chatted about stuff, not as deeply I guess as I would with the psychologist, . . . more just talking about everyday things, and that was good because [I] don’t really have other people to do that with . . . (Better Access user) . . . I am actually with the NDIS [National Disability Insurance Scheme] now and they’ve been looking after the psychologist fees. (Better Access non-user)
Community awareness of Better Access
All but two participants (both non-users) were familiar with Better Access. Some felt that they might be the exception though, and that many people could be struggling but not know that the programme exists. They mentioned the need to raise awareness about Better Access, noting that this would reduce stigma and promote help-seeking.
‘I would love it to be normalised, like we were talking about the posters in GPs’ offices and stuff . . . It’d be great if she could hand me some written information about it, and in that written information are testimonials from people . . . that could say, you know, ‘I’m so glad I started this Better Access programme because . . . Because that would help normalise it a little bit . . . (Better Access non-user)
Discussion
Participants in the current study who had seen a psychologist through Better Access in 2021 were generally positive about the programme. Most of these users indicated that the referral process was straightforward, although some were dubious about the need for the review process. This is consistent with the findings from a recent qualitative study of MHTPs by Banfield et al. (2019), in which participants indicated that reviews seemed judgemental and did not necessarily lead to high-quality care. It is not clear whether the recent changes to Better Access regarding GPs/PMPs might have any bearing on these views.
Most users in our study tended to prefer face-to-face sessions but saw significant benefits in telehealth. All reported positive changes to their health and wellbeing since seeing the psychologist (e.g. improved mood, increased feelings of hope and empowerment). The psychologist’s manner and approach was perceived as the main reason for these improvements. Feeling safe and heard was particularly important, as was the psychologist’s willingness to provide unbiased, compassionate feedback. The provision of self-management techniques was also valued. These positive responses from Better Access users are consistent with those in our previous evaluation (Ftanou et al., 2014).
Those who had not used Better Access in 2021 were also generally positive about the programme. Many had used it in the past and their recent non-use tended to be due to accessing other services rather than any negativity towards the programme. Like Better Access users, many non-users suggested that the programme should be better promoted.
For both Better Access users and non-users, affordability was extremely important. Consistent with the study by Banfield et al. (2019), many users stressed the benefits of being able to access mental health treatment at low or no cost. However, both users and non-users frequently highlighted that there were still financial barriers, with many noting that out-of-pocket costs were prohibitive. The participants in our previous evaluation made the same observation (Ftanou et al., 2014), and several other studies in the current evaluation support this. For example, 35% of the 2013 participants in a survey of Better Access users considered that the fee they paid was too expensive (Pirkis et al., 2026b), and the 90 key stakeholders who participated in an online consultation forum rated affordability as the highest priority for future programme reforms (Currier et al., 2026). The situation may have worsened as the median per-session co-payment has increased (from $74 in 2021 to $90 in 2022) (Tapp et al., 2026b). Options for addressing affordability issues that have been canvassed elsewhere include: setting (and re-setting) fees in a standardised and more transparent manner; modifying the rules around the Extended Medicare Safety Net (which entitles those who spend a threshold amount on Medicare-subsidised providers in a calendar year to higher rebates for future visits); creating bulk-billing incentives or loadings on specific Better Access items; paying GPs and allied health professionals practice incentive payments (PIPs) or service incentive payments (SIPs) for maximising the quality of mental health care they provide; and considering blended funding models (Australian Government Department of Health, 2022c; Duckett et al., 2022; Medicare Benefits Schedule Review Taskforce, 2020).
Better Access users and non-users also discussed the number of available sessions. There was consensus that the 10 sessions that are available under current arrangements (and even the 20 that were available during the pandemic) were too few, particularly for people with complex needs. Both users and non-users wanted the number to be increased, either for everyone or for those with more complex needs. The participants in the study by Banfield et al. (2019) expressed similar frustrations with session limits, suggesting that these reduce the programme’s reach and effectiveness. By contrast, in our previous evaluation when the standard number of sessions was six (with the option of a further six after a review and a further six in exceptional circumstances), the majority of participants were satisfied with the number of sessions of care they received (Ftanou et al., 2014). The ideal number of sessions is difficult to gauge, and, in a system that is stretched, requires a balance between offering the optimal number to any one individual and making sessions available to the maximum number of people. In other studies in the current evaluation, we showed that, in the main, consumer outcomes improved as a function of session numbers (Harris et al., 2026; Pirkis et al., 2026a, 2026b). However, we also showed that increasing numbers of people with high levels of need were missing out on Better Access care (Chilver et al., 2026; Tapp et al., 2026b). This balance issue is critical, particularly because those with complex needs may not always be able to access other treatment options (Petrie et al., 2021).
Limitations
Our participant numbers were small and their views may not represent those of all users and non-users of Better Access. Only 14 participants had not used Better Access in the past year, and many of these had used the programme previously. Certain groups were over-/under-represented in the sample. All of the Better Access users had seen psychologists; none had seen social workers or OTs. As noted, our intention was to provide an in-depth view of Better Access from a range of participants, rather than to generate data that could be generalised. However, the sample profile may mean that the views of particular groups dominated.
The evaluation timeframes meant that we had to be pragmatic. We conducted one recruitment round, rather than continuing to recruit until saturation was reached, although our interviewers were confident that towards the end of the interviews no new information was being presented. Ideally, we would have returned the transcripts to participants for validation but time did not permit this.
Conclusion
This study sought the views of people with lived experience of mental disorders, the most important Better Access stakeholders. They suggested that, in general, Better Access operates smoothly, allows people to access high-quality care and yields positive outcomes (e.g. improved functioning, reduced symptoms). However, although Better Access makes care more affordable, out-of-pocket costs can still be prohibitive. There are also questions about whether the amount of available care is sufficient. Better Access has many strengths, but it meets the needs of some better than others. Future reforms to Better Access should address accessibility and affordability.
Supplemental Material
sj-docx-1-anp-10.1177_00048674251404766 – Supplemental material for Perspectives on Better Access: In-depth interviews with users and non-users of the initiative
Supplemental material, sj-docx-1-anp-10.1177_00048674251404766 for Perspectives on Better Access: In-depth interviews with users and non-users of the initiative by Danielle Newton, Michelle Williamson, Jane Pirkis, Michelle Banfield, Lisa Brophy, Cathrine Mihalopoulos, Meredith Harris and Dianne Currier in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
This study was funded by the Australian Government Department of Health, Disability and Ageing, as part of the broader evaluation of Better Access. We would like to thank the two groups that were constituted to advise on the evaluation, the Clinical Advisory Group and the Stakeholder Engagement Group. We would like to acknowledge Beyond Blue and Lived Experience Australia for assisting us with recruiting participants for this study. We would also like to thank the participants themselves.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The evaluation of Better Access was funded by the Australian Government Department of Health, Disability and Ageing.
ORCID iDs
Data accessibility statement
The datasets generated and analysed for the current study are not available.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.