
Abstract
Background:
Rates of suicide following discharge from psychiatric hospitals are extraordinarily high in the first week post-discharge and then decline steeply over time. The aim of this meta-analysis is to evaluate the strength of risk factors for suicide after psychiatric discharge and to investigate the association between the strength of risk factors and duration of study follow-up.
Methods:
A PROSPERO-registered meta-analysis of observational studies was performed in accordance with PRISMA guidelines. Post-discharge suicide risk factors reported five or more times were synthesised using a random-effects model. Mixed-effects meta-regression was used to examine whether the strength of suicide risk factors could be explained by duration of study follow-up.
Results:
Searches located 83 primary studies. From this, 63 risk estimates were meta-analysed. The strongest risk factors were previous self-harm (odds ratio = 2.75, 95% confidence interval = [2.37, 3.19]), suicidal ideation (odds ratio = 2.15, 95% confidence interval = [1.73, 2.68]), depressive symptoms (odds ratio = 1.84, 95% confidence interval = [1.48, 2.30]), and high-risk categorisation (odds ratio = 7.65, 95% confidence interval = [5.48, 10.67]). Significantly protective factors included age ⩽30, age ⩾65, post-traumatic stress disorder, and dementia. The effect sizes for the strongest post-discharge suicide risk factors did not decline over longer periods of follow-up.
Conclusion:
The effect sizes of post-discharge suicide risk factors were generally modest, suggesting that clinical risk factors may have limited value in distinguishing between high-risk and low-risk groups. The highly elevated rates of suicide immediately after discharge and their subsequent decline remain unexplained.
Among the many established and putative suicide risk factors, previous psychiatric care, particularly psychiatric hospitalisation, is emerging as one of the most significant statistical risk factors for later suicide. In a meta-analysis of 50 years of longitudinal research on risk factors for suicidal thoughts and behaviours, Franklin and associates (Franklin et al., 2017) found that a history of prior psychiatric hospitalisation was the strongest risk factor for suicide. This was also the finding of a Danish population study examining hierarchical levels of psychiatric treatment (Hjorthøj et al., 2014) and is consistent with very high rates of post-discharge suicide demonstrated in two meta-analyses that respectively examined suicide rates after longer and shorter periods of follow-up (Chung et al., 2017, 2019). When the results of these two meta-analyses of suicide rates after discharge are combined, a picture emerges of very high suicide mortality rates in the first week of follow-up = 2950 suicides per 100,000 person years (24 studies, 95% confidence interval [CI] = [1740, 5000]), that subsequently decline over time by a factor of 10, as shown by rates at periods of follow-up of up to 1 month = 2060 (29 studies, CI = [1300, 3280]), 3 months of follow-up = 1132 (18 studies, CI = [874, 1467]), 3 to 12 months of follow-up = 654 (43 studies, CI = [533, 802]), 1 and 5 years of follow-up = 494 (44 studies, CI = [354, 688]), 5 and 10 years of follow-up = 366 (44 studies, CI = [283, 472]), and over 10 years = 277 (34 studies, CI = [218, 352]).
Potential explanations for the very high initial post-discharge suicide rates and their subsequent decline over time are under-researched, and no consistent pattern of temporal changes in the strength of post-discharge suicide risk factors have emerged. In 1993, Goldacre and associates examined a limited set of risk factors over 1 month and 1 year of follow-up after discharge from a group of English psychiatric hospitals. No clear explanation for the decline in suicide rates over longer periods of follow-up was found. Goldacre hypothesised that discharge itself was a suicide risk factor, possibly because of a loss of hospital care, reduced supervision, and psychiatric relapse due to renewed exposure to problems in the home environment (Goldacre et al., 1993). Two further studies examining the strength of post-discharge suicide risk factors found no significant temporal changes (Iliachenko et al., 2020; Kessler et al., 2020). When suicide risk factors have been found to change in strength over time after psychiatric discharge, the results have not been replicated. In 2009, Hunt and associates found that male sex, a history or self-harm, a history of violence, self-initiated discharge, and failure of follow-up were more strongly associated with earlier rather than later suicide (Hunt et al., 2009). In 2021, Britton and associates found that that young age was a stronger risk factor for suicide over a longer period of follow-up and that suicidal ideation became a weaker risk factor over time (Britton et al., 2021). More recently, Aaltonen and associates found that the risk factors of more severe depression and poor global functioning declined in strength over longer periods of follow-up, while involuntary treatment, living alone, and substance use, increased in strength over time (Aaltonen et al., 2024).
To date, there is one meta-analysis of suicide risk factors after psychiatric hospital discharge (Large et al., 2011). In this 2011 study, the strongest associations with post-discharge suicide were a prior history of self-harm or a suicide attempt (odds ratio [OR] = 3.15), depressive symptoms (OR = 2.70), suicidal ideation (OR = 2.47), and a high-risk categorisation (OR = 3.94) as derived from sample of 13 primary studies reporting suicides in the first year post-discharge (Large et al., 2011). In this meta-analysis, numerous widely accepted suicide risk factors in the general community, including older age, single marital status, living alone, unemployment, substance use and physical illness, were not significantly associated with suicide during the post-discharge period. Disconcertingly, patients who had more post-discharge psychiatric care were significantly more likely to suicide than those who received less care. The meta-analysis did not examine changes in the strength of suicide risk factors according to duration of study follow-up.
Aims and hypothesis
The first aim was to use meta-analysis to re-examine the strength of associations between suicide risk factors and suicide over all periods of follow-up, serving as an update and extension of the 2011 meta-analysis (Large et al., 2011). The second aim was to determine whether between-study heterogeneity in the strength of suicide risk factors (effect size) could be explained by the mean duration of primary study follow-up.
We hypothesised that the effect size of the stronger risk factors for post-discharge suicide, as determined by this meta-analysis, would decline over longer periods of time, and/or that the effect size of protective factors would increase over time, thus explaining the decline in post-discharge suicide rates.
Methods
The meta-analysis was performed according to the Meta-analysis of Observation Studies in Epidemiology (MOOSE) (Stroup et al., 2000) and Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) (Moher et al., 2009) guidelines (see Supplemental Material 1., PRISMA checklist). The meta-analysis was registered with PROSPERO: registration CRD42023449429. The study was an extension and update of the 2011 meta-analysis (Large et al., 2011) and a protocol was not published.
Search strategy
A.T. and M.L. independently searched MedLINE, PsycINFO and Embase for relevant articles published in the English language from inception until 11 April 2024 (see Figure 2. Flow chart of search strategy) using the search terms “suicid*.ti. and ((discharge* or hospital* or admit* or admis* or in-patient or inpatient).ab. or (discharge* or hospital* or admit* or admis* or in-patient or inpatient).ti.) and ((psych* or mental or affective or schizophreni* or bipolar or depress*).ab. or (psych* or mental or affective or schizophreni* or bipolar or depress*).ti.)”. A.T. and M.L. independently performed searches and pared down by titles and then abstracts. Papers chosen for full-text examination after examination of abstracts by either author were considered for inclusion and exclusion.
Inclusion and exclusion criteria
Cohort and case-control studies were included if they reported on the clinical characteristics of groups of patients who died by suicide or survived after discharge from a psychiatric inpatient unit.
Studies were excluded if they (1) did not describe the characteristics of non-suicide patients (i.e. had no control or comparator group), (2) included patients discharged from non-psychiatric settings, (3) included suicides among currently admitted patients, (4) included patients who were not admitted or discharged, (5) used controls who died from causes other than suicide, or (6) reported on populations of patients who were unrepresentative of psychiatric inpatients (for example, from forensic hospitals). The inclusion and exclusion criteria were applied by A.T and M.L independently and then by consensus. Where two or more studies reported on overlapping samples, the study with the largest sample size was included.
Data extraction
A.T. and M.L. independently extracted counts (suicide & risk factor, total suicide, non-suicide & risk factor, total non-suicide) and other unadjusted effect size data when counts were not available. The mean and standard deviation of continuous risk variables (such as age, duration of hospitalisation and clinical rating scales) were similarly extracted. Discrepant data points were examined by H.P. and A.B. and resolved by consensus with A.T. and M.L.
A.T. and M.L. standardised terminology of risk factors by consensus. Similar terms in the primary research were aggregated (for example, depressive symptoms, depressed mood and depressed). The continuous variable of age and the categories of older age (defined as >65 years) and younger age (defined as <30 years) were examined.
The pooled effect size for each post-discharge suicide risk factor (defined here to include both risk and protective factors) was expressed as an odds ratio (OR) in line with common reporting practices of primary literature and similar meta-analyses (Grover et al., 2023; Large et al., 2017). The moderator variable of mean study duration of follow-up was extracted and where study follow-up was not reported directly, it was estimated by the interval between the mid-point of data collection and the end-point of follow-up. A.T., H.P. and A.B. reconciled any disputed data points through further examination of studies.
Strength of reporting scale
The strength of reporting of the included primary studies was assessed using a 0 to 6 point scale derived from the Newcastle-Ottawa scale for assessing the quality of non-randomised studies in meta-analysis (Wells et al., 2021). One point was awarded if the study included a (1) sample of patients that were unselected by diagnosis, (2) employed a cohort study design, (3) included a recognised diagnostic system, (4) identified suicides by using coronial records or other external mortality data (as opposed to hospital records), (5) employed a register of discharges, and (6) ascertained research data on suicide risk factors at the time of discharge rather than by retrospective examination of patient notes. The impact of the strength of reporting on the strength of suicide risk factors was examined by comparing groups of studies categorised as having stronger or less strong reporting based on the strength of reporting score dichotomised using the median score.
Statistical analysis
The pooled strength of the effect size of suicide risk factors were estimated by meta-analysis when a risk factor was reported five or more times. This threshold of five was consistent with other large-scale studies of suicide risk factors among psychiatric inpatients (Large et al., 2017) and was chosen to increase the accuracy of the pooled estimates, reduce the impact of possible publication bias, and allow more meaningful assessments of between-study heterogeneity and tests of publication bias. Some studies reported data points at various follow-up periods and subgroups according to gender; in these studies, the pooled mean OR of the data points or subgroups was used as the unit of analysis. Count data and where possible, other effect size data, were converted to OR using Comprehensive Meta-Analysis Version 2 (CMA V2) (Borenstein et al., 2022). Effect sizes that are not able to be converted to OR (for instance, hazard ratios) were recorded, but ultimately were too few for a separate meta-analysis. Pooled OR and 95% confidence intervals were calculated using a random-effects model. A random-effects model was selected a priori due to the variation in study design, hospital settings, clinical populations, countries and year of study. The strength of the pooled effect size was classified as weak if the OR was between 1.0 and 2.0, moderate if the OR was between 2.0 and 3.0 and strong if the OR was above 3.0, in line with the qualitative descriptors of Rosenthal (Rosenthal, 1996). Between-study heterogeneity in effect size was assessed by examination of funnel plots and with Q-value and I2 statistics. Publication bias was assessed using examination of the funnel plot and Egger’s regression. The extent of possible publication bias was assessed using the Tweedie and Duval trim and fill method. The sensitivity and specificity were separately calculated for high-risk categorisation using a random-effects model.
Random-effects (method of moments) meta-regression was used to examine the explanatory value of the moderator variable of the duration of follow-up on the observed heterogeneity in effect sizes reported in 10 or more data points. The threshold of 10 was chosen for consistency with previous research and to ensure the reliability of the results (Grover et al., 2023). Multiple data-points and subgroups within the same study (according to the length of follow-up and gender) were regarded as independent for the purpose of the meta-regressions.
Sensitivity analyses were performed according to the study method (cohort vs control), the diagnostic mix of the patient population (unselected, mood disorders, schizophrenia spectrum disorders), and dichotomised strength of reporting scores, when more than five data points were available in each group. Between-group differences were examined using a mixed-effects model. A sensitivity analysis of the meta-regressions was performed using naturally transformed (ln) follow-up duration.
CMA V2 was used for meta-analyses and meta-regressions (Borenstein et al., 2022).
Results
Search results
The electronic searches identified a total of 83 studies that met the inclusion criteria (see Figure 1. Flow chart of searches: 1: Supplemental Material 2. Table of Included Studies: Aaltonen et al., 2019, 2024; Agerbo et al., 2001; Allgulander et al., 1992; Appleby et al., 1999; Axelsson and Lagerkvist-Briggs, 1992; Beck et al., 1985, 1989; Berglund et al., 1987; Bickley et al., 2013; Bjorkenstam et al., 2014; Black et al., 1985a, 1985b; Bradvik and Berglund, 1993; Britton et al., 2017, 2021; Carlborg et al., 2009, 2010; Che et al., 2023; Chiu et al., 2023; Choi et al., 2019, 2020; Clapham et al., 2019; De Hert et al., 2001; Deisenhammer et al., 2019; Dennehy et al., 1996; Desai et al., 2005; Enns et al., 2022; Farberow and MacKinnon, 1974; Fazel et al., 2006; Flood and Seager, 1968; Fowler et al., 1979; Fredriksen et al., 2022; Geddes and Juszczak, 1995; Geddes et al., 1997; Goldacre et al., 1993; Goldstein et al., 1991; Guimaraes et al., 2022; Høyer et al., 2004; Haglund et al., 2019; Heu et al., 2018; Ho, 2003, 2006; Hoffmann and Modestin, 1987; Hogan and Awad, 1983; Hong et al., 2024; Hunt et al., 2009; Iliachenko et al., 2020; Isometsa et al., 2014; Jiang et al., 2021; Kan et al., 2007; Kaster et al., 2022; Kessler et al., 2014, 2020; King, 2001; Kuo et al., 2005, 2010; Lee and Lin, 2009; Lin et al., 2008; Luxton et al., 2013; McKenzie and Wurr, 2001; Madsen et al., 2020; Modestin and Schwarzenbach, 1992; Motto and Bostrom, 1990; Motto et al., 1985; Nielsen et al., 2023; Nordström et al., 1995; Olfson et al., 2016; Park et al., 2013; Pirkola et al., 2005; Plans et al., 2019; Pokorny, 1983; Pokorny and Kaplan, 1976; Prestmo et al., 2023; Reutfors et al., 2009; Riblet et al., 2018; Sani et al., 2011; Shaffer et al., 1974; Stephens et al., 1999; Tsai et al., 2002; Tseng et al., 2020; Yim et al., 2004).
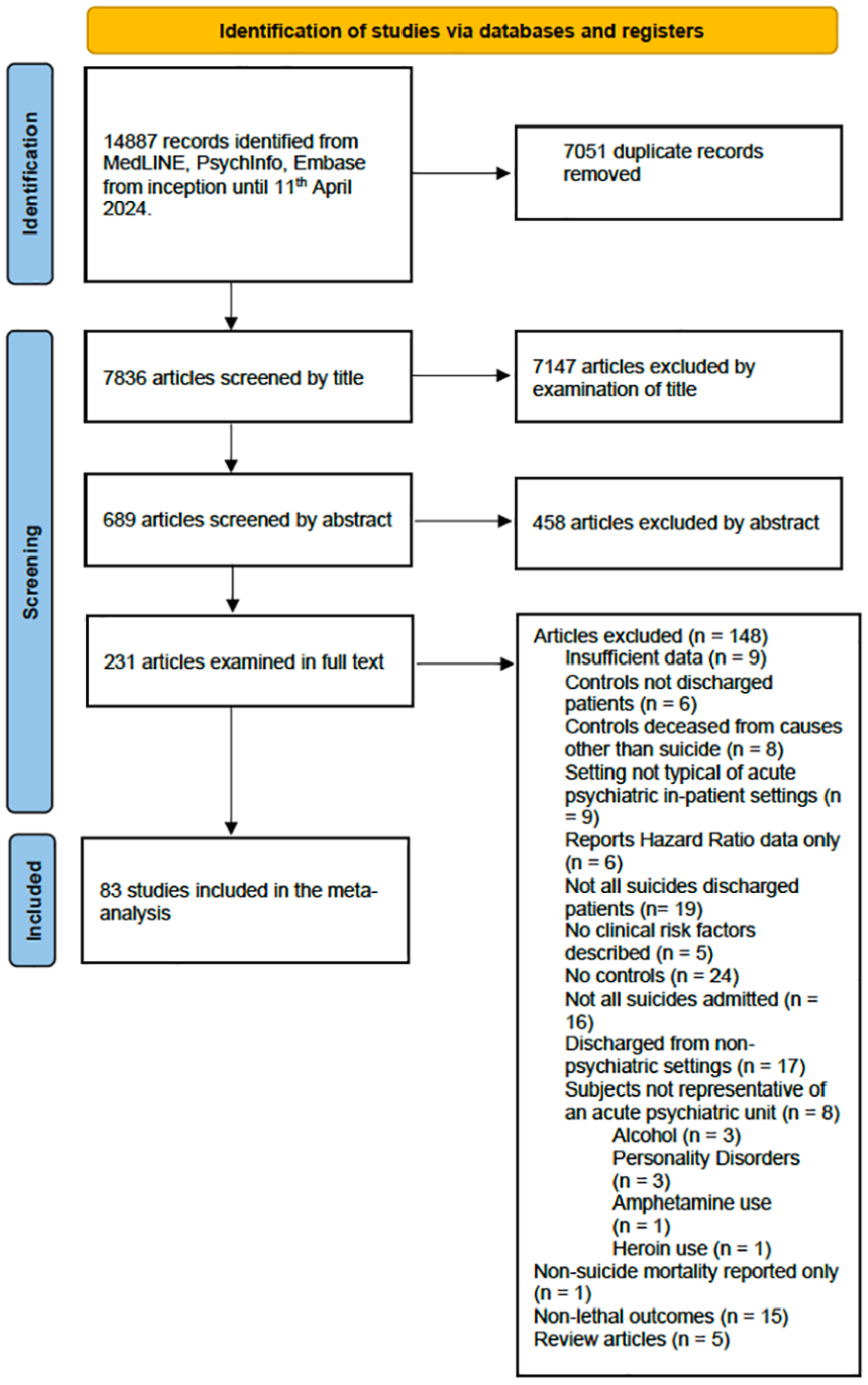
Flow chart of searches.
The primary studies included 54 cohort studies and 29 case-control or nested case-control studies. 82 studies were conducted in high-income countries: 10 from the UK, 25 from the United States and Canada, 32 from mainland Europe and 15 from high-income Asian countries. One paper was from a South American upper middle-income country. There were no papers from low-or middle-income settings as defined by the World Bank LAMI classification system (Metreau et al., 2024). The mean year of publication was 2006, and the median was 2009.
The included studies reported on a total of 9,452,741 discharged patients, of whom 39,190 (0.41%) died by suicide. There was a mean of 119,655 subjects/study (SD = 378,479), a mean of 496.1 suicides/study (SD = 990.1 suicides/study), and a median 1846 subjects/study and 91 suicides/study.
15 studies or study data points reported follow-up periods of 1 month or less, 14 study data points reported follow-up periods between 1 and 3 months, 19 study data points reported follow-up periods between 3 months and a year, 18 study data points reported follow-up periods between a year and 3 years, and 28 study data points reported follow-up periods greater than 3 years.
The mean of the strength of the reporting scale was 4 (SD = 1.7) and the median was also 4 (interquartile range = 3.5) (see Supplemental Material 3. Strength of Reporting Scores).
The 83 studies reported 1698 effect sizes after the exclusion of a small number of study-specific variables (such as the place and year of suicide). Of the 1698 effect sizes, 255 were excluded: 209 were reported four or fewer times (reported in 1 study = 134, 2 studies = 29, 3 studies = 32, 4 studies = 14) and 46 were residual categories of uncertain meaning. By virtue of being reported in five or more data points, 1443 effect sizes were included in a meta-analysis of 63 risk factors (62 individual risk factors and high-risk categorisation). All variables, including those reported in four or fewer data points, can be found in Supplemental Material 4. Data Used in the Meta-analysis.
The overall pooled effect size for all risk factors was OR = 1.22 (95% CI = [1.19, 1.25]) with a Z value = 14.31 and p = < 0.05. The overall heterogeneity was very high Q = 21673 [df = 1697] and I2 = 92). The Funnel Plot (Figure 2) appeared symmetrical while an Egger’s regression intercept was statistically significant. Correction with Duval and Tweedie’s trim and fill revealed slight publication bias towards studies that reported a lower OR. The Tweedie and Duval method estimated a corrected OR of 1.29 (95% CI = [1.25, 1.33]) by trimming 74 of the 1698 risk factors. The duration of study follow-up was not significantly associated with between-study heterogeneity in effect sizes.
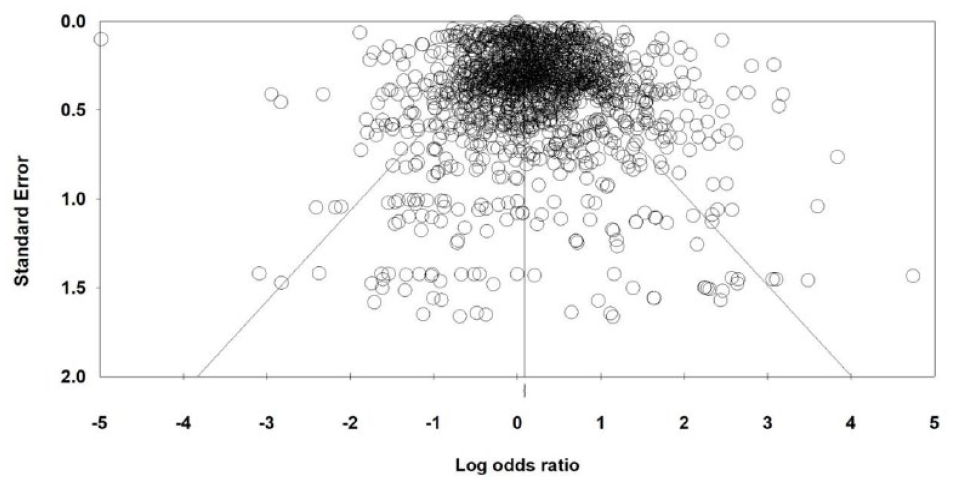
Funnel of 1698 effect sizes of risk factors for post-discharge suicide.
Meta-analysis of post-discharge suicide risk factors
The strength of post-discharge suicide risk factors that were reported five or more times are shown in Table 1.
Meta-analysis of risk factors for suicide after psychiatric discharge.
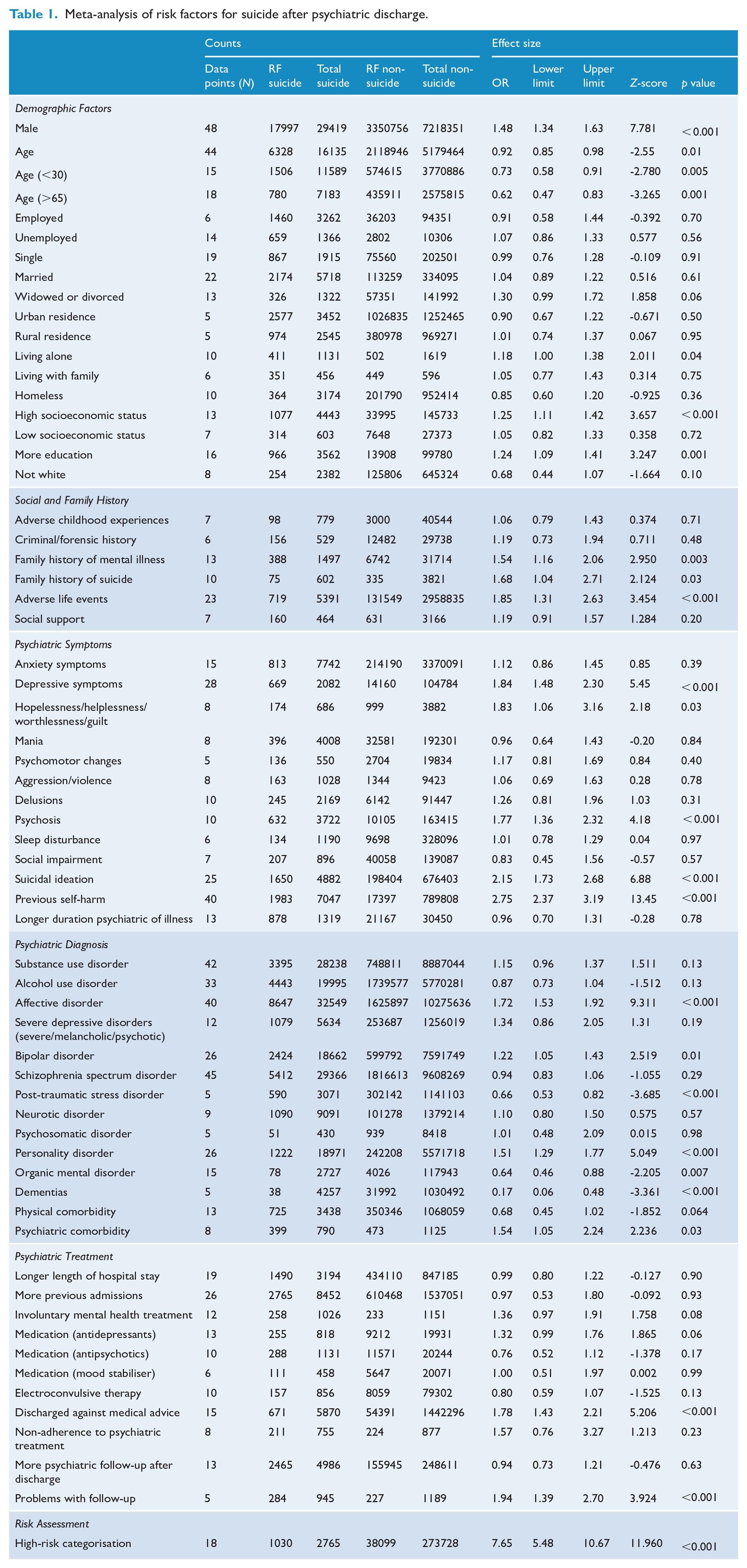
Most of the identified risk factors were only weakly associated with post-discharge suicide. There were 15 suicide risk factors with an OR > 1.5: high-risk categorisation, previous self-harm, suicidal ideation, depressive symptoms, problems with follow-up, adverse life event, hopelessness/helplessness/worthlessness/guilt, discharged against medical advice, psychosis, affective disorder, family history of suicide, non-adherence to psychiatric treatment, family history of mental illness and psychiatric comorbidity (see Figure 3. Forrest plot of the top 15 effect sizes of risk factors for post-discharge suicide).
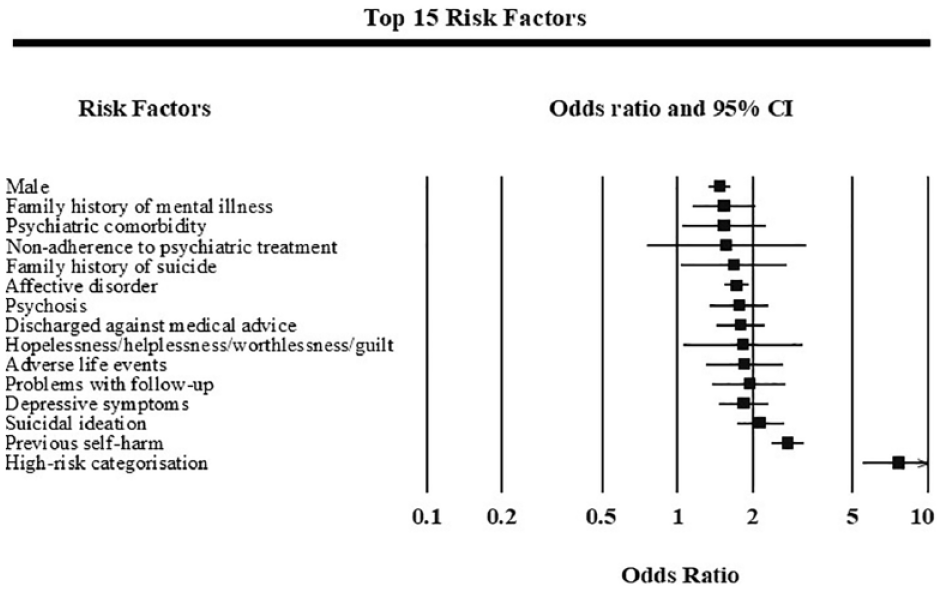
Forrest plot of the top 15 effect sizes of risk factors for post-discharge suicide.
Demographic factors
The demographic risk factors that were significantly associated with post-discharge suicide included male sex (OR = 1.48, 95% confidence interval [CI] = [1.34, 1.63]), living alone (OR = 1.18, 95% CI = [1.00, 1.38]), high socioeconomic status (OR = 1.25, 95% CI = [1.11, 1.42]), and more education (OR = 1.24, 95% CI = [1.09, 1.41]). Both older age (OR = 0.62, 95% CI = [0.47, 0.83]), and younger age (OR = 0.73, 95% CI = [0.58, 0.91]) were protective. Demographic factors not associated with post-discharge suicide included employment status, marital status (single, married or widowed/divorced), urban residence, rural residence, living with family, homelessness, low-socioeconomic status, and ‘non-white’ (noting that the primary research did not clarify whether this referred to race or skin colour).
Social and family history
Having a family history of mental illness (OR = 1.54, 95% CI = [1.16, 2.06]), family history of suicide (OR = 1.68, 95% CI = [1.04, 2.71]), or adverse life events (OR = 1.85, 95% CI = [1.31, 2.63]), were weakly associated with post-discharge suicide. Adverse childhood experience, criminal history, and more social support, were not associated with post-discharge suicide.
Psychiatric signs and symptoms
Previous self-harm (OR = 2.75, 95% CI = [2.37, 3.19]), and suicidal ideation (OR = 2.15, 95% CI = [1.73, 2.68]) were moderately associated with post-discharge suicide. Depressive symptoms (OR = 1.84, 95% CI = [1.48, 2.30]), the specific depressive symptoms of hopelessness/helplessness/worthlessness/guilt (OR = 1.83, 95% CI = [1.06, 3.16]), and psychosis (OR = 1.77, 95% CI = [1.36, 2.32]) showed weak associations. Psychiatric symptoms not associated with post-discharge suicide were anxiety symptoms, mania, psychomotor changes (including agitation and retardation), aggression/violence, delusions, sleep disturbance, social impairment, and longer duration of illness.
Psychiatric diagnosis
Affective disorders (OR = 1.72, 95% CI = [1.53, 1.92]), bipolar disorders (OR = 1.22, 95% CI = [1.05, 1.43]), personality disorders (OR = 1.51, 95% CI = [1.29, 1.77]), psychiatric comorbidities (OR = 1.54, 95% CI = [1.05, 2.24]) were weakly associated with post-discharge suicide. Psychiatric diagnoses that were not associated with post-discharge suicide included substance use disorder, alcohol use disorder, schizophrenia spectrum disorder, ‘neurotic disorder’, and physical comorbidity. Post-traumatic stress disorder (OR = 0.66, 95% CI = [0.53, 0.82]), organic mental disorders (OR = 0.64, 95% CI = [0.46, 0.88]), and dementias (OR = 0.17, 95% CI = [0.06, 0.48]) were protective against post-discharge suicide.
Psychiatric treatment factors
Psychiatric treatment factors that demonstrated weak associations included discharge against medical advice (OR = 1.78, 95% CI = [1.43, 2.21]), and problems with follow-up (OR = 1.94, 95% CI = [1.39, 2.70]). Psychiatric treatment factors not associated with post-discharge suicide include longer length of hospital stay (OR = 0.99, 95% CI = [0.80, 1.22]), more previous admissions, involuntary mental health treatment, antidepressants, antipsychotics, mood stabilisers, electroconvulsive disorders, non-adherence to psychiatric treatment, and more psychiatric follow-up after discharge (OR = 0.94, 95% CI = [0.73, 1.21]).
High-risk categorisation
16 studies reported 18 high-risk categorisation methods. A variety of methods were used in the primary studies to distinguish between high- and low-risk patients. Three studies utilised clinical judgement, five utilised the number of co-occurring risk factors, four used statistical analysis (logistic regression) and four utilised machine learning. The most frequently included suicide risk factors were previous self-harm and depressive symptoms. High-risk categorisation was strongly associated with post-discharge suicide (OR = 7.65, 95% CI = [5.48, 10.67]). The meta-analytic sensitivity of high-risk categorisation was 45% (CI = [36%, 55%]) and specificity was 92% (CI = [88%, 95%]).
Heterogeneity
8 risk factors had low between-study heterogeneity (I2 < 25%), 10 had moderate heterogeneity (25% ⩽ I2 < 50%), 19 had high heterogeneity (50% ⩽ I2 < 75%), and 26 had very high heterogeneity (I2 ⩾ 75%) (see Supplemental Material 5. Assessment of Heterogeneity and Publication Bias.).
Statistical evidence of publication bias
Evidence of publication bias was found among eight out of the 63 suicide risk factors (see Supplemental Material 5. Assessment of Heterogeneity and Publication Bias). Egger’s test was significant for younger age (intercept = −3.33, p = 0.01), married (intercept = −1.23, p = 0.03), homelessness (intercept = 2.07, p = 0.02), more education (intercept = −1.17, p = 0.03), depressive symptoms (intercept = −2.30, p = 0.01), suicidal ideation (intercept = 1.73, p = 0.01), longer hospital stay (intercept = 2.46, p = 0.01) and discharge against medical advice (intercept = 1.65, p = 0.01). More education and discharge against medical advice were the only risk factors that had a corrected OR that differed by ⩾5% from the uncorrected value, as estimated using Duval and Tweedie’s trim and fill method.
Strength of reporting
The strength of reporting had minimal impact on the effect size of suicide risk factors. The only statistically significant finding was that the OR for male sex was 19% higher in the group of studies with stronger reporting when compared with the group of studies with less strong reporting (Supplemental Material 6. Sensitivity analysis according to dichotomised strength of reporting score).
Meta-regression
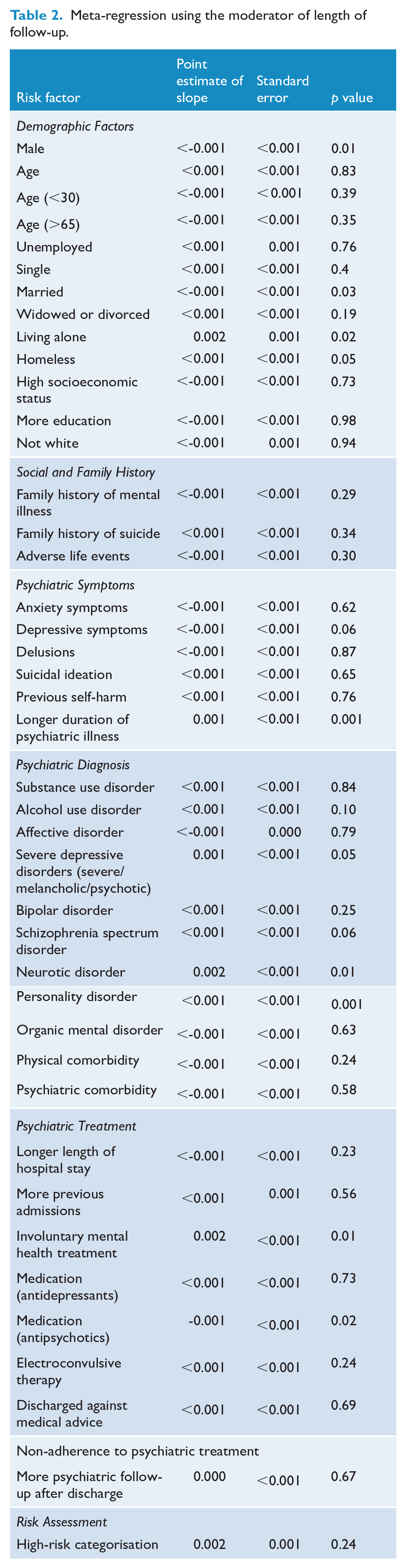
A longer mean duration of follow-up was associated with a lower OR (lower suicide risk) in the meta-regression of the variables of being married and antipsychotic medication (see Table 2. Meta-regression using the moderator of length of follow-up). A longer duration of follow-up was associated with a higher OR (increased suicide risk) in the meta-regression of the variables of male, living alone, longer duration of illness, neurotic disorders, personality disorders and involuntary mental health treatment. None of the risk factors that were most strongly associated with suicide (including high-risk categorisation, previous self-harm, suicidal ideation, depressive symptoms and adverse life events) had effect sizes that were significantly lower in studies with longer follow-up. No significantly protective factor was reported in a sufficient number of primary studies for the meta-regression analysis. An analysis using natural logarithm transformed length of stay data yielded similar results to untransformed length of stay data.
Meta-regression using the moderator of length of follow-up.
Sensitivity analyses
Grouping by diagnosis impacted risk factor strength (that is, produced a significant p-value) for male, the continuous variable of age, younger age and older age categories (see Supplemental Material 7. Sensitivity analysis according to study diagnostic group). Study design (cohort vs case-control) impacted on the strength of the risk factors of male, age, and widowed/divorced (Supplemental Material 8. Sensitivity analysis according to cohort or control design).
Discussion
This meta-analysis synthesises data from 83 primary studies of risk factors for suicide after psychiatric discharge. The meta-analysis produced 62 estimates of the strength of easily assessed suicide risk factors, as well as an estimate of the potential strength of risk categorisation. A high-risk categorisation, based on the presence of two or more suicide risk factors, was strongly associated with post-discharge suicide. However, the limited sensitivity of the high-risk categorisation suggested that fewer than half of all future suicides can be identified by combining risk factors. Disappointingly, the strength of individual suicide risk factors was generally weak, with only two risk factors having an OR over 2 (suicidal ideation and previous self-harm) and none having an OR over 3. Contrary to our hypothesis, between-study heterogeneity among the strongest risk factors for post-discharge suicide (including high-risk categorisation) was not explained by a declining strength of association with suicide over longer periods of follow-up. There was insufficient data to examine whether any factor accrued stronger protection against post-discharge suicide over time.
The strengths of this study include the number of included primary studies, the large number of total subjects and the comprehensive set of meta-analytic estimates of common suicide risk factors. The study has several limitations. First, the absence of studies from low- and middle-income settings means that our findings cannot be generalised outside of discharges occurring in high-income countries. Second, most of the variables we reported had a high degree of between-study heterogeneity that was not explained by the moderator variable of the length of follow-up, reporting strength, study design, or diagnostic mix. This suggests that there might be contextual factors affecting the strength of suicide risk factors that we did not capture in the meta-analysis. Third, the meta-analysis focused on associations between clinical risk factors and suicide, and potential interactions between risk factors were not examined excepting the indirect analysis in the analysis of high-risk categorisation. Given that suicide is widely believed to be the result of complex interactions of underlying factors, the merits of examination with individual subject-level data, rather than meta-analysis, could be considered. Fourth, this meta-analysis (and the meta-analyses of rates of post-discharge suicide (Chung et al., 2017, 2019) relied on estimates of cumulative mortality at various durations of follow-up. It is likely that cumulative mortality is less sensitive to change over time than mortality rates at specific intervals, and it is therefore possible that a meta-analysis based on OR calculated at specific intervals might be more sensitive to changes over time. Fifth, some important risk factors, such as specific personality disorders, were reported fewer than five times and were therefore not included in this meta-analysis. No protective factor was reported by enough primary studies to examine changes in their protective strength over time. Finally, the associations that we demonstrated cannot be assumed to be causal because of the cross-sectional way in which the risk factors were ascertained in both cohort and controlled primary studies.
This study builds on the earlier meta-analysis of risk factors for post-discharge suicide (Large et al., 2011) and was able to examine a greater number of suicide risk factors because of new primary literature published in the intervening years and the decision to include studies reporting suicides over more than 1-year post-discharge. Similar to the earlier study (Large et al., 2011), high-risk categorisation, previous self-harm, suicidal ideation and depressive symptoms were the strongest risk factors for post-discharge suicide. Previous self-harm and depressive symptoms were also the most commonly reported risk factors used in high-risk categorisation in a meta-analysis of inpatient suicides (Large et al., 2017) suggesting the salience of these risk factors among psychiatrically admitted patients. Both this and the earlier meta-analyses of post-discharge suicide found that male sex, depressive disorder/affective disorder, symptoms of hopelessness/helplessness/worthlessness/guilt, recent social difficulties/adverse life event and unplanned discharge/discharge against medical advice were significantly associated with post-discharge suicide (Large et al., 2011). The current meta-analysis identified a range of significant post-discharge suicide risk factors that did not reach significance in the 2011 meta-analysis. This suggests that the earlier meta-analysis had type II errors due to the smaller sample size of primary studies. These factors included the protective factor of older age, and the risk factors of living alone, more education, family history of mental illness, psychiatric comorbidity, and bipolar disorder.
A notable finding of the Large and associates 2011 meta-analysis was that less psychiatric follow-up (among seven studies) was a protective factor against suicide (Large et al., 2011). Reassuringly, this earlier finding seems to have been a Type I error. In the current meta-analysis, more psychiatric follow-up was not a risk factor for suicide. However, ‘problems with follow-up’ was associated with post-discharge suicide suggesting that the nature of the follow-up is more important than its duration.
Risk factors identified in this meta-analysis but not examined previously by Large et al. include personality disorders and problems with follow-up (Large et al., 2011). Protective factors identified in this meta-analysis but not previously examined include younger age, dementias, and PTSD (Large et al., 2011).
The finding that PTSD was protective against post-discharge suicide was surprising because PTSD appears to be a risk factor for suicide in the general community (Fox et al., 2021.). However, our result only suggests that a primary diagnosis of PTSD is significantly less associated with suicide than other psychiatric diagnoses in populations of people who were so unwell as to require psychiatric admission. People admitted to a psychiatric hospital exhibit not only mental illness but often pose a risk to themself or others, and the admission may reflect a failure of community care. The nature of the psychiatrically discharged patients studied in this meta-analysis might also explain why several factors that are usually considered to be risk factors for suicide in the community were not significantly significant in this study. These include being widowed/divorced, low-socioeconomic status, and substance use disorder.
The overall strength of risk factors in the current meta-analysis was generally lower than we had expected, with only two of 62 individual suicide risk factors having an OR > 2. These modest effect size were generally lower than those reported in a recent meta-analysis of risk factors for suicide in the community (Favril et al., 2022), but were similar to those reported in a large-scale meta-analyses of prospective studies unselected by discharge status (Franklin et al., 2017; Ribeiro et al., 2016). The similarity of our findings to that of Franklin and associates is not surprising because most studies included in our meta-analysis were also prospective and none relied on psychological autopsy methods. However, it may also be that suicide risk factors generally have less predictive strength among populations of admitted people – almost all of whom are likely to have a mental disorder.
The strongest risk factors for post-discharge suicide (high-risk categorisation, depressive symptoms and previous self-harm) did not decline with increasing periods of follow-up and the findings of the meta-regression did not provide a good explanation for the declining rates of suicide over longer periods of follow-up described by Chung (Chung et al., 2017, 2019). This is consistent with primary studies that have reported modest and inconsistent differences in the strength of a variety of suicide risk factors across different post-discharge periods (Aaltonen et al., 2024; Britton et al., 2021; Goldacre et al., 1993; Hunt et al., 2009; Iliachenko et al., 2020; Kessler et al., 2020).
This meta-analysis suggests that widely accepted risk factors for suicide in the community have limited application in populations of discharged psychiatric patients. Given what is known about the high suicide rate in the immediate post-discharge period, the modest statistical association between risk factors and suicide, and the low sensitivity of high-risk categorisation, clinicians lack the tools to make meaningful distinctions between subgroups of discharged patients according to suicide risk. This suggests that all discharged patients must be regarded as being at some risk of suicide, and efforts should be made to ensure comprehensive follow-up for every patient. Emphasis should be placed on the quality of follow-up, given that the risk variable coded as ‘problems with follow-up’ was associated with suicide, while the duration of the follow-up was not.
In 1993, Goldacre and associates hypothesised that discharge itself was a suicide risk factor (Goldacre et al., 1993). It is disappointing that the same inference might be drawn more than 30 years later. Furthermore, potentially important aspects of the patient’s experience of discharge, such as the loss of the support of the hospital, stigma, loss of social role associated with hospitalisation, and the potential for the renewed exposure to problems in the home environment have rarely been studied. The result is that the very high rate of suicide in the immediate post-discharge period remains unexplained and further research is required, particularly into approaches to prevent post-discharge suicide.
The modest strength of the risk factors for suicide, and low sensitivity of high-risk models, also point to the need for more research using advanced methods. Future primary research using machine learning and artificial intelligence might capture patterns of risk that predict suicide with greater statistical power, and shed light on the complex and hereto unpredictable causes of suicide in this setting.
Supplemental Material
sj-docx-1-anp-10.1177_00048674251348372 – Supplemental material for Meta-analysis of risk factors for suicide after psychiatric discharge and meta-regression of the duration of follow-up
Supplemental material, sj-docx-1-anp-10.1177_00048674251348372 for Meta-analysis of risk factors for suicide after psychiatric discharge and meta-regression of the duration of follow-up by Allyson Tai, Hannah Pincham, Ashna Basu and Matthew Large in Australian & New Zealand Journal of Psychiatry
Supplemental Material
sj-docx-2-anp-10.1177_00048674251348372 – Supplemental material for Meta-analysis of risk factors for suicide after psychiatric discharge and meta-regression of the duration of follow-up
Supplemental material, sj-docx-2-anp-10.1177_00048674251348372 for Meta-analysis of risk factors for suicide after psychiatric discharge and meta-regression of the duration of follow-up by Allyson Tai, Hannah Pincham, Ashna Basu and Matthew Large in Australian & New Zealand Journal of Psychiatry
Supplemental Material
sj-docx-3-anp-10.1177_00048674251348372 – Supplemental material for Meta-analysis of risk factors for suicide after psychiatric discharge and meta-regression of the duration of follow-up
Supplemental material, sj-docx-3-anp-10.1177_00048674251348372 for Meta-analysis of risk factors for suicide after psychiatric discharge and meta-regression of the duration of follow-up by Allyson Tai, Hannah Pincham, Ashna Basu and Matthew Large in Australian & New Zealand Journal of Psychiatry
Supplemental Material
sj-docx-4-anp-10.1177_00048674251348372 – Supplemental material for Meta-analysis of risk factors for suicide after psychiatric discharge and meta-regression of the duration of follow-up
Supplemental material, sj-docx-4-anp-10.1177_00048674251348372 for Meta-analysis of risk factors for suicide after psychiatric discharge and meta-regression of the duration of follow-up by Allyson Tai, Hannah Pincham, Ashna Basu and Matthew Large in Australian & New Zealand Journal of Psychiatry
Supplemental Material
sj-docx-5-anp-10.1177_00048674251348372 – Supplemental material for Meta-analysis of risk factors for suicide after psychiatric discharge and meta-regression of the duration of follow-up
Supplemental material, sj-docx-5-anp-10.1177_00048674251348372 for Meta-analysis of risk factors for suicide after psychiatric discharge and meta-regression of the duration of follow-up by Allyson Tai, Hannah Pincham, Ashna Basu and Matthew Large in Australian & New Zealand Journal of Psychiatry
Supplemental Material
sj-xlsx-6-anp-10.1177_00048674251348372 – Supplemental material for Meta-analysis of risk factors for suicide after psychiatric discharge and meta-regression of the duration of follow-up
Supplemental material, sj-xlsx-6-anp-10.1177_00048674251348372 for Meta-analysis of risk factors for suicide after psychiatric discharge and meta-regression of the duration of follow-up by Allyson Tai, Hannah Pincham, Ashna Basu and Matthew Large in Australian & New Zealand Journal of Psychiatry
Footnotes
Statement of Contribution
A.T. was responsible for the initial draft. The literature searches, identification of papers, and data extraction were conducted independently by A.T. and M.L. A.T., H.P., and A.B. performed the data reconciliation. A.T. and M.L. independently conducted the analysis of results and interpretation. This project was conceived by M.L.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: M.L. has provided evidence in legal matters following post-discharge suicides.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.