
Abstract
Suicide rates vary significantly between countries [1]. Notwithstanding methodological issues that may explain some of these differences, this variation presents opportunities for conducting ecological studies of suicide. Recent examples include studies focusing on countries' religion [2], socio-economic conditions [2], [3], legislation on car exhaust emissions [4] and policies on restricting the availability of paracetamol [5]. Many of these ecological studies have primarily made comparisons between relatively affluent countries, despite the fact that suicide has been recognized as a major public health problem in low and middle-income countries.
One area that is ripe for ecological study is the association between national suicide rates and countries' mental health policies, programs and legislation, yet no study has been conducted that considers data from many countries. It would be anticipated that cohesive, national mental health strategies would be associated with comparatively low suicide rates, given that mental health problems significantly increase the risk of suicide [6–8]. The current paper uses an ecological study design to test the hypothesis that the presence of national mental health policies, programs and legislation would be associated with lower national suicide rates.
Method
We combined international data on countries' suicide rates with international data on countries' mental health policies, programs and legislation, and countries' income levels, in order to investigate the relationship between suicide rates and mental health resources at a country level, controlling for level of affluence.
Data and data sources
Dependent variables
We extracted data on countries' suicide rates from the World Health Organization (WHO) Mortality database, which comprises deaths registered in national vital registration systems of reporting countries, with underlying cause of death as coded by the relevant national authority [9]. The database was most recently updated in 2003 and contains number of deaths by country, year, sex, age group and cause of death (coded according to the International Classification of Diseases [ICD]) beginning in 1950. Population estimates by age/sex grouping were available for each country, enabling rates to be calculated. Deaths classified as suicides according to the ICD were converted into crude rates and then standardized to the WHO World standard population[10]. The median number of years for which suicide rates were available per country was 21 and the range was 1–50.
Independent variables
We extracted data on countries' mental health policies, programs and legislation from the Mental health atlas, produced by the WHO in 2001 [11–13]. Using a questionnaire methodology, the Mental health atlas compiled information on mental health resources from key mental health personnel in the Ministries of Health of member states, associate member states and areas. Five specific data items were of interest in the current study, presence or absence at a national level of: (i) a mental health policy; (ii) a mental health program; (iii) mental health legislation; (iv) a substance use policy; and (v) a therapeutic drugs policy. These were selected on the grounds that they were high-level, global indicators of mental health investments by the countries demonstrating a certain level of priority given to this area. Definitions of each are provided in Table 1. All five indicators were associated with a year of implementation, which was important in determining their impact on suicide rates. For the policy and program variables, the year referred to the year of initial formulation of the policy or program; for the legislation variable, the year referred to the year of initiation of the latest law in the field of mental health.
Independent variable definitions
We derived data on countries' income levels from the World Bank Country classification[14]. Countries were classified into one of four income groups, based on their gross national income (GNI) from the latest available information: (i) high income; (ii) upper middle income; (iii) lower middle income; or (iv) low income.
Data analysis
We combined data from the above sources into a consolidated dataset. The WHO collected data from 191 member countries for the Mental health atlas. Of these, 91 were excluded because their suicide rates could not be ascertained reliably. The remaining 100 were available for analysis (see Table 2). We included all of these countries in the analysis; those that had introduced policies, programs and/or legislation enabled a beforeand-after comparison of suicide rates, and those that had not done so provided a picture of the trend in rates in the absence of such interventions.
Countries available for study
As a first step, we undertook simple descriptive analyses to provide a picture of the suicide rates and mental health policies, programs and legislation across countries. The mean suicide rate, standardized to the world standard population, across all years for each country was calculated, with a weighting factor incorporated to account for different countries contributing different numbers of observations. The proportion of countries with and without each mental health initiative was determined, as was the median year of adoption of each initiative.
To test our hypothesis, we then used a random effects generalized least squares (GLS) regression analysis to estimate the strength of association between the policy, program and legislation indicators and suicide rates, after controlling for the other indicators and for the income level of the country. We also controlled for time, in order to make sure that any observed effects were not a function of a secular trend of rising suicide rates in many countries. Country–year was the unit of analysis, and we used a one-year lag to cater for the estimated delay in any effect of the initiative. We considered an approach that used greater lags, but rejected it on the grounds that it would have eliminated too many countries from the analysis. We used a logarithm transform of suicide rate as an outcome variable, to stabilize the variance of residuals, and presented the final results as adjusted percentage changes in suicide rates.
The analysis strategy is summarized in a simplified form (Fig. 1) for a single hypothetical country, Country X, where a given policy was introduced in 1991. The suicide rate for Country X was calculated for each individual year when there was no policy, and for each individual year when the policy was in place. The year of introduction of the policy, 1991, was treated as a year of no policy, to allow for delays in anticipated effects. Suicide rates in years of no policy were then compared with suicide rates in years when the policy was present.
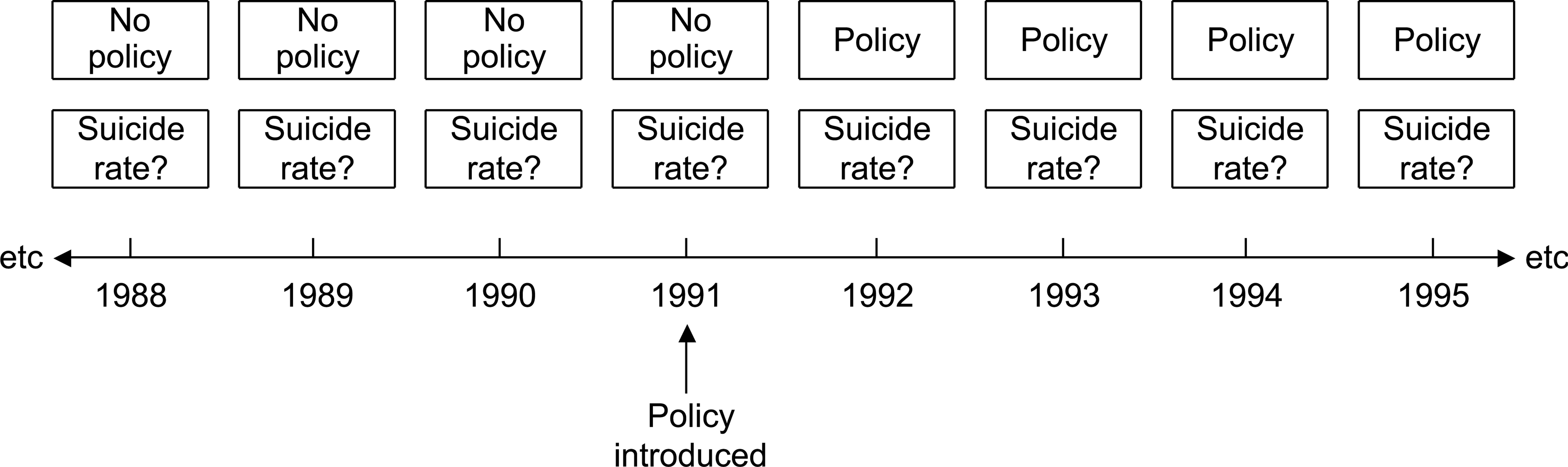
Analysis strategy for hypothetical Country X
Data were analysed using Stata (V. 7) and SPSS (V. 11).
Results
There was considerable variability between countries' average standardized suicide rates between 1950 and 2001. For male suicides, the lowest mean rate was 0.2 per 100 000 per year (in Papua New Guinea) and the highest mean rate was 60.2 per 100 000 per year (in Lithuania). For female suicides, the lowest mean rate was 0.1 per 100 000 per year (in Jordan) and the highest mean rate was 16.8 per 100 000 per year (in China).
Countries also varied in their national mental health activities. As Table 3 shows, two thirds of all countries had a national mental health policy in place. Around two thirds had implemented a national mental health program, and about three quarters had enacted mental health legislation. Approximately four-fifths had a national substance abuse policy and a similar proportion had a national therapeutic drugs policy. Typically, these initiatives had been implemented relatively recently.
Countries' status with regard to national mental health policies, programs and legislation
Mental health policies, programs and legislation as predictors of suicide rates
Table 4 shows the findings of the regression analysis (significant findings are in bold). A country's adoption of a substance use policy in a given year was associated with a decrease in male, female and total suicide rates in the following year and the years beyond that. By contrast, the introduction of a mental health policy and mental health legislation was associated with an increase in male and total suicide rates, and the introduction of a therapeutic drugs policy was associated with an increase in total suicide rates.
Adjusted percentage change in suicide rates
There was also a significant effect of year, with male, female and total suicide rates increasing over time. Income group was also significant, with lower middle income group status being associated with the lowest suicide rates, relative to high income group status.
Discussion
Contrary to expectations, this study found that the adoption of mental health policies, mental health legislation and therapeutic drugs policies were associated with an increase in the countries' suicide rates, even when income status and time were taken into account. This association was particularly evident for male suicides. The only intuitive finding was that the adoption of a substance abuse policy was associated with a decrease in suicide rates.
If these results are taken at face value, the picture is bleak. Mental health problems are known to significantly heighten suicide risk [6–8] and since most national mental health initiatives would include among their overarching goals a reduction in suicide rates, it is of concern to find that national mental health initiatives are associated with an increase in suicide rates. If this were the case, there would clearly be a need to rethink the direction of national mental health initiatives worldwide and to examine more closely the commonalities among those that were associated with particular patterns of suicide rates.
The only positive finding – that the adoption of substance abuse policies was associated with a reduction in suicide rates – is worth considering here. It mirrors the findings of within-country studies of changes in alcohol policy [15], [16]. If substance abuse policies achieve reductions in suicide rates where other mental health initiatives fail to do so, there may be some lessons to be learnt. Substance abuse heightens risk for suicide, particularly when it occurs comorbidly with other mental health problems [6]. The influence of substance abuse as a risk factor has been shown to vary with disorder type, age and sex. For example, illicit drug abuse heightens the risk of suicide for young men, licit drug addiction enhances the risk for young women and alcoholism increases the risk for older men [17], [18]. It is often regarded as a distal or long-term risk factor, but can also be considered to heighten suicide risk proximally or in the short term (e.g. if drugs or alcohol are involved in the suicide act itself) [19]. Substance abuse policies that explicitly address chronic and acute use for a range of drugs and a range of demographic groups, may be particularly successful in reducing suicide. Substance abuse policies and programs are typically funded and implemented separately from mental health policies and programs, but from the point of view of suicide prevention, there may be an argument for a closer alignment of the two.
It would be naïve to accept the above interpretation without question. Even if it is true that the adoption of mental health initiatives (other than substance abuse policies) is directly associated with an increase in suicide rates, there may be acceptable reasons for this. For example, it may demonstrate that policies and legislation have been introduced in areas of increasing need, where suicide rates were on the rise. Alternatively, it may indicate a case-finding effect, whereby a greater awareness of mental health issues generated by the given initiative led to a heightened tendency to label deaths as suicides.
The study's limitations must also be taken into account. First, there are issues with the data on suicide rates. It is widely acknowledged that population-based data on suicide should be treated with a degree of caution. Whether a death is recorded as a suicide may depend on a range of factors, including how suicide is defined, variation in coroners' practices and differences in the extent to which family and friends may try to conceal the cause of death due to the stigma associated with suicide. These factors may vary differentially from country to country, as well as over time [20], [21].
Second, although the Mental health atlas represents a major feat in terms of profiling the mental health resources of countries around the world, the data on mental health policies, programs and legislation also have potential flaws that may have introduced systematic biases. Some of these flaws may have led to overreporting. For example, if a country had an overall health policy that had a section on mental health (irrespective of its relative standing), it was recorded as having a mental health policy. This may have been further compounded by the social desirability of responding affirmatively to having a policy in place. Other flaws may have led to under-reporting. For example, a country that had comprehensive state-based policies but no federal policy, was recorded as having no mental health policy.
Third, the adoption of mental health policies or legislation does not necessarily equate with the implementation of the initiative. Even if policies were well-considered and well-drafted, they would need to be consistently implemented throughout a nation over a reasonable period of time to have a chance of affecting suicide rates. Our study design permitted an observation of the existence of suicide policies over time, but it was not possible to ascertain from the Mental health atlas the extent to which ‘on the ground’ implementation occurred. Fourth, there were issues created once the data on suicide rates and mental health initiatives were combined. Because the majority of countries had implemented given initiatives relatively recently, there were often very few observations after the adoption of the initiative. This was exacerbated by the decision to introduce a year-long lag into all analyses, to allow for the given initiative to be implemented. There is little information on the length of time necessary for an impact on suicide rates to be observed. Repeat analyses in the future would clearly be desirable.
Finally, there is the question of the extent to which mental health policies and legislation might be expected to impact on suicide. As we have already noted, we consider the relationship is a reasonable one to posit, given that mental health problems significantly heighten suicide risk. However, a specific suicide prevention policy or program, which some countries have [22], could be expected to be more closely related to reductions in suicide rates. Equally, other factors such as religion, unemployment levels and wars might be expected to have an influence. Lack of readily available data at a country level meant that examining the relative impact of suicide prevention policies and programs and other potential candidate factors was beyond the scope of the study.
There is a clear need for further work in this area. The WHO's Mental health atlas is a valuable resource, representing a major step forward in information on the mental health resources available in countries around the world, but at present it is a fairly blunt instrument. It provides a picture of the presence or absence of a range of mental health initiatives, but it does not describe the nature or direction of these initiatives. This additional detail would be desirable in teasing out whether the approaches of different countries are having an impact on their suicide rates. Close attention should also be paid to the relationship between general mental health initiatives and suicide-specific initiatives. These refinements, combined with improved data quality and ongoing analysis, have the potential to further knowledge regarding successful country-level approaches to suicide prevention.