
Abstract
A number of population-based studies have found that in the weeks and months after discharge, the rate of suicide several hundred times greater than that of the general population [1–8]. As many as 5% of all suicides by discharged patients occur in the week after discharge from a psychiatric hospital [9], about 20% of suicides by previously admitted patients occur within a year of discharge [9] and the proportion of psychiatric patients who commit suicide in the year after discharge has been variously reported as 1.27% [4], 0.3% [5] and 0.4% [10].
Knowing which factors are associated with suicide in the period after discharge and the strength of those associations could improve clinical management and increase patient safety. By contrast, erroneous beliefs about which patient characteristics are associated with post-discharge suicide could lead to needlessly restrictive treatment for patients who were wrongly labelled as ‘high risk’ and the diversion of health care resources from patients wrongly labelled ‘low risk’.
This study used meta-analytical methods to pool the findings of controlled studies of suicide within a year of discharge from psychiatric hospitals to examine the strength and consistency of individual risk factors, and the utility of high risk categorization.
Methods
Search strategies
We searched for published studies and conference abstracts in the following electronic databases: PsycINFO from January 1967 to August 2010, Embase from January 1980 to August 2010, MEDLINE/PubMed from January 1950 to August 2010, CINAHL from January 1981 to August 2010 (see Figure 1) using the terms ‘suicide’ [All Fields] AND discharge [All Fields] OR hospitalization [All Fields]. The results were checked against the results of searches performed in the course of an earlier study of inpatient suicide [11]. We also examined the lists of references in a recent qualitative review [12] and hand-searched the references lists of the studies located by electronic searches.
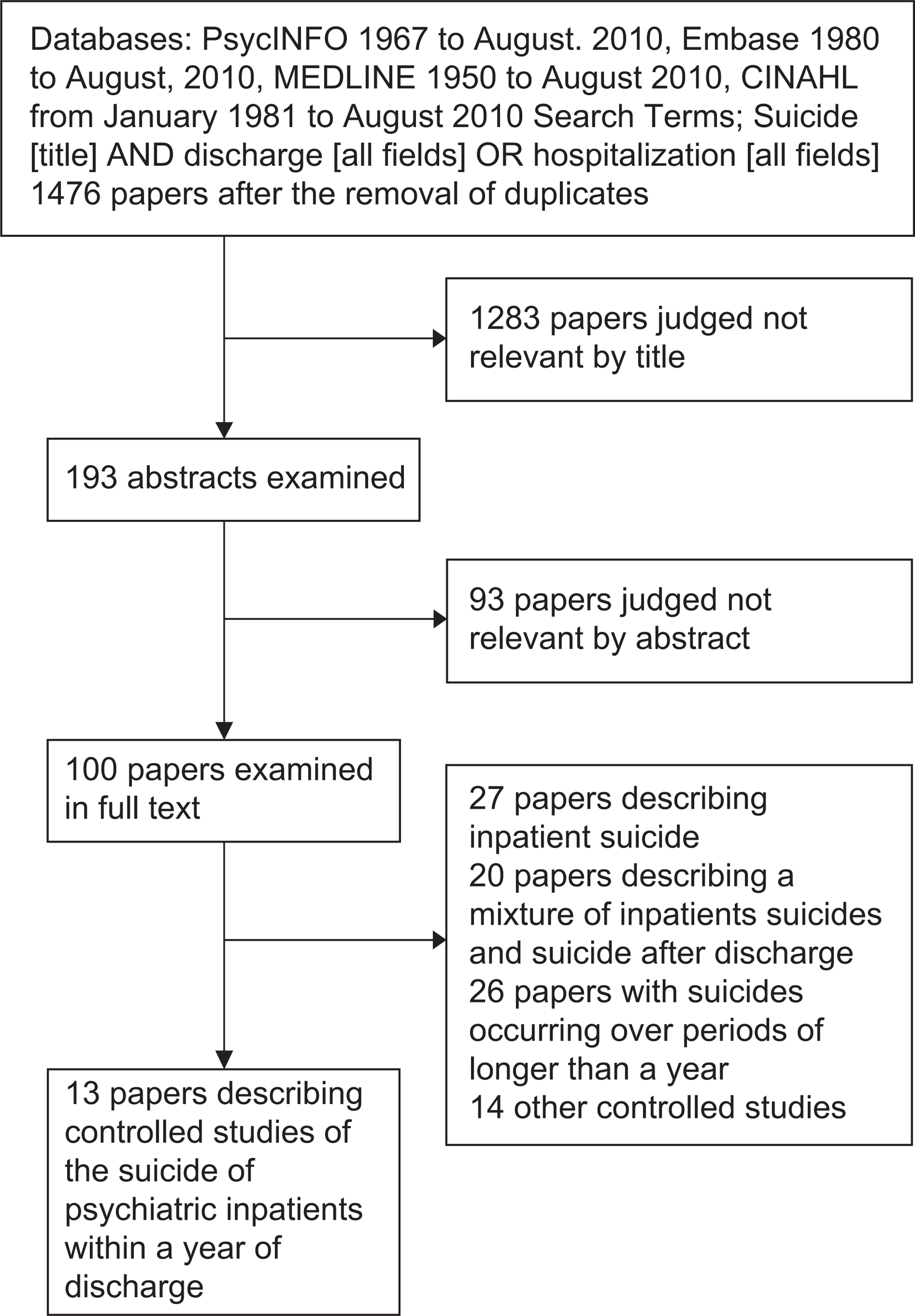
Flow chart of searches.
Inclusion and exclusion criteria
Studies were included if they: (i) reported the characteristics of a sample of patients who committed suicide within one year after discharge from a psychiatric inpatient setting; (ii) reported the characteristics of a control group of patients discharged from the same settings who did not commit suicide within the same period; and (iii) employed case control, nested case control or cohort control designs.
Studies were excluded if they included: (i) patients who attempted suicide; (ii) suicides of inpatients or patients on leave from hospital; (iii) a mix of patients who committing suicide during and after psychiatric hospitalization; (iv) suicides occurring more than a year after discharge; (v) suicides after discharge from hospitals other than psychiatric hospitals.
Study quality
We considered the following measures of study quality; the size of the study, measured by the number of suicide cases, the possibility of missed cases due to the examination of discharges from a single or small number of hospitals in a limited geographic region, whether unique patient identity numbers such as social security numbers were used to identify cases, and whether the clinical data had been collected prospectively or by examination of the medical records. Where medical records were examined, we considered whether the researchers were blinded to the suicide outcome and whether inter-rater reliability was examined. We included studies that used information collected prospectively from hospital databases, studies reporting data obtained by a file audit after the suicide and studies relying on the written accounts of treating clinicians after the suicide. In each study, the patient characteristics referred to the patients’ condition at the time of the hospitalization.
Data extraction
The data was independently extracted by M.L. and S.S. Twelve discrepancies were found among 576 data points. A further independent check of the data was performed by E.C., who identified three further discrepancies. All were resolved by a further examination of the studies.
Meta-analysis of effect size, between study heterogeneity and publication bias
Factors were included in the meta-analysis if they were reported in two or more included studies. Comprehensive Meta-Analysis software (version 2.2, Biostat) was used to calculate a pooled estimate of the associations with suicide within a year of discharge [13]. The effect sizes were reported as odds ratios because almost all the data were categorical. Effect sizes were classified as weak (odds ratio (OR) between 1.5 and 2.5), moderate (OR between 2.5 and 4), strong (OR between 4 and 10) or very strong (OR greater than 10) [14]. Assuming 25 independent tests, a factor with a p value of 0.002 or less would be unlikely to be due to a Type-I error.
Heterogeneity was assessed using a Q-value and I-square for each factor. We chose a random effects model for the meta-analysis because of the heterogeneity of study design and because they were conducted in a range of hospitals, in different countries and during different decades.
We assessed publication bias using a fail-safe N test applied to all the meta-analytic results with a p ≤ 0.05. This test estimates the number of hypothetical missing studies with an effect size of zero needed to return to p ≥ 0.05. Because of the small number of studies we were unable to perform a statistical assessment of the possibility of publication bias using a method such as the ‘trim and fill’ procedure [15].
High risk analysis
Some studies used the presence of multiple risk factors to retrospectively classify patients as being at high or low risk. The sensitivity and specificity of high risk categorizations and the odds ratio of suicide in high and low risk groups was estimated by meta-analysis. No study prospectively examined suicide among patients already categorized as high or low risk.
Results
Included studies
The electronic searches, examination of the references in the recent qualitative review and hand searches of reference lists yielded 13 studies that met the inclusion criteria (Figure 1) [1,4,6,7,10,16–23]. We did not locate an earlier meta-analysis or any relevant non-English language papers. One study examined suicides within two months of discharge [16], four studies examined suicides within three months of discharge [17,18,22,23] and one study included suicides within six months of discharge [6]. The remaining seven studies examined suicides within a year of discharge. Differences in the study populations, periods of follow up and reported risk factors meant that the degree of overlap of subjects between studies conducted in overlapping regions in overlapping periods was minimal.
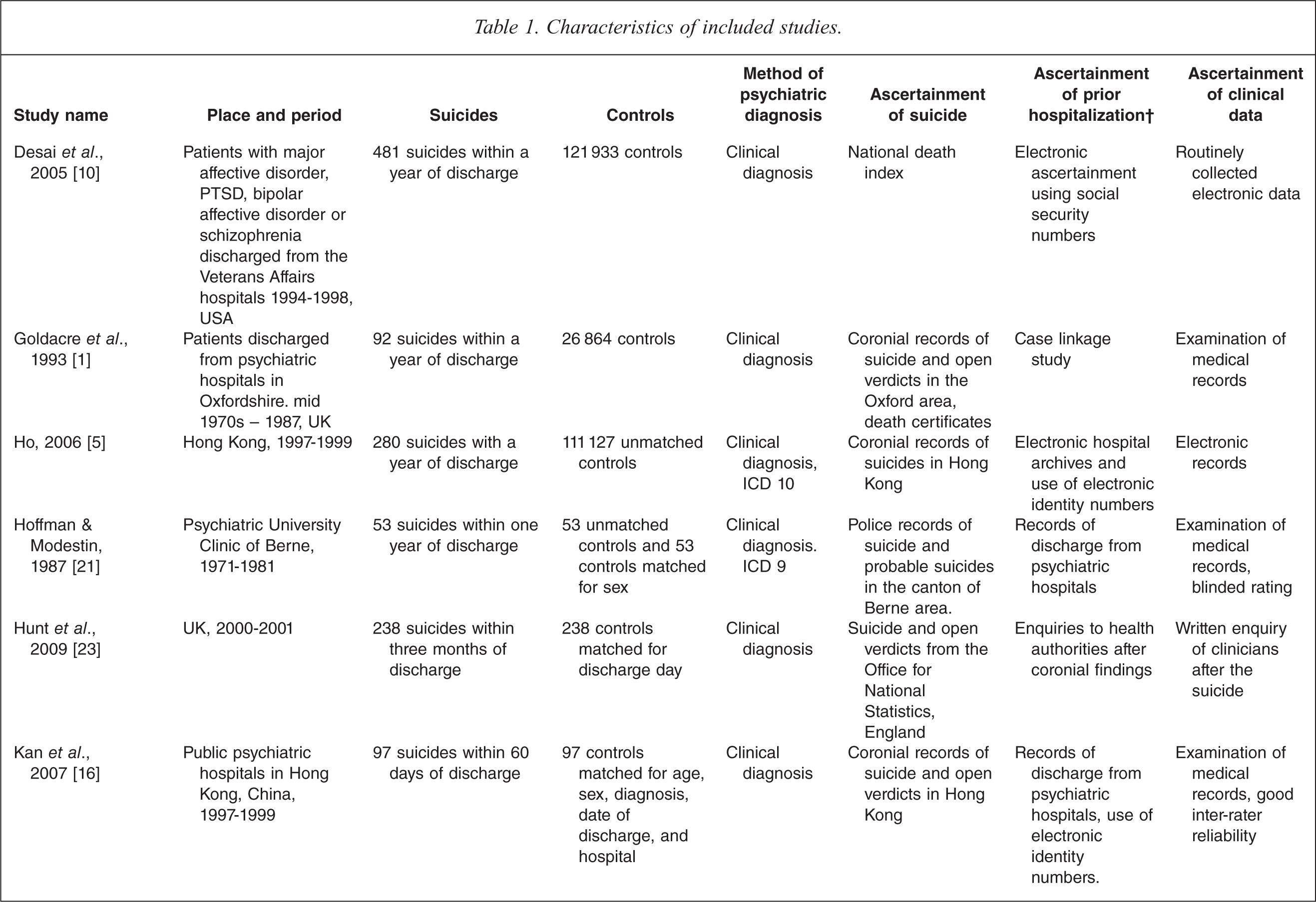
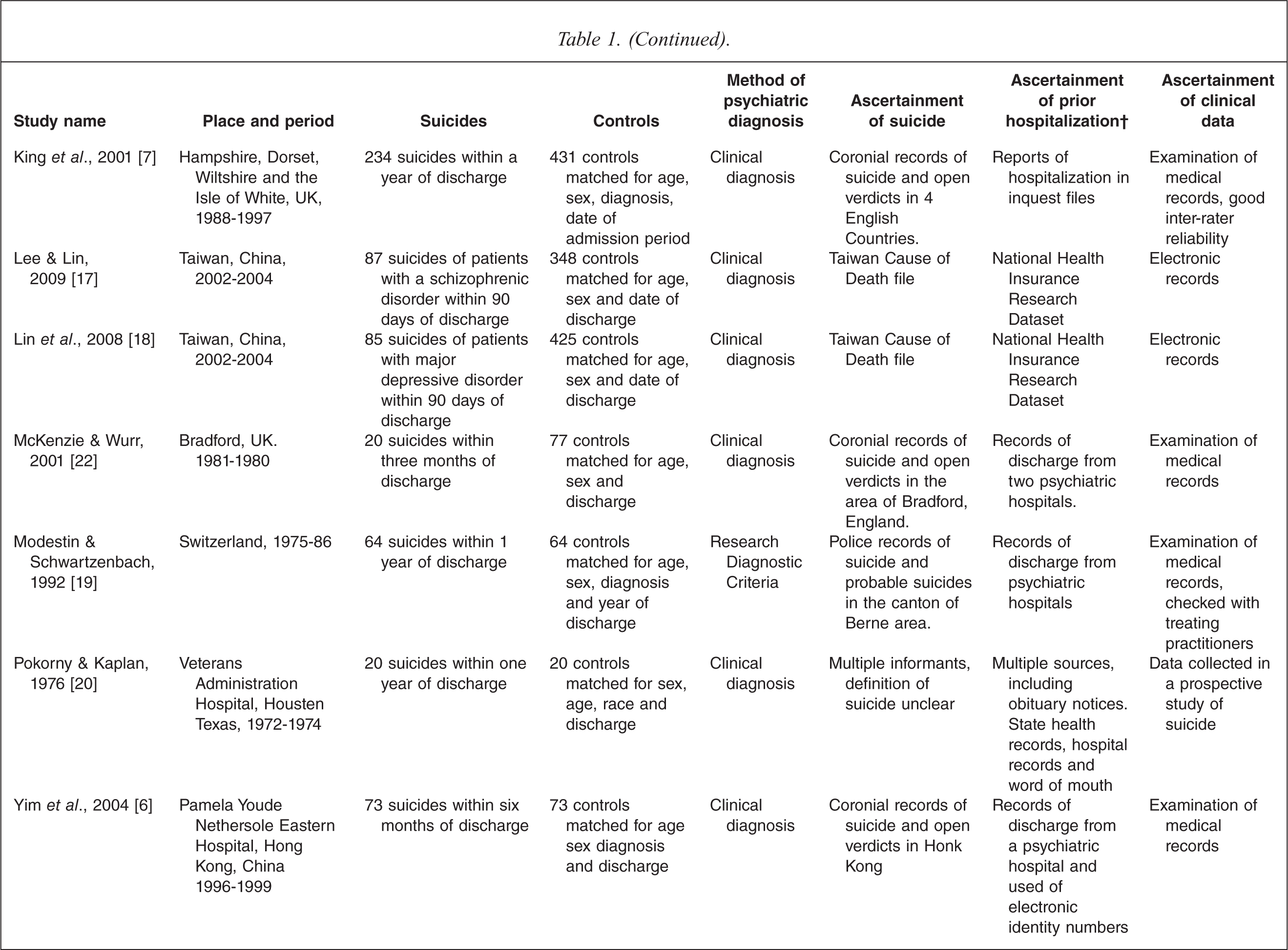
We included all of the available studies because there were so few studies and because every study had several indicators of a high quality study (Table 1). The studies reported a total of 1544 suicides with a mean of 127 (standard deviation (SD) 131) suicides per study. Only two of the studies had sample sizes of fewer than 50 suicides.
Characteristics of included studies.
Meta-analysis of the associations with post-discharge suicide
A prior history of self-harm or a suicide attempt (OR = 3.15) and depressive symptoms irrespective of an affective diagnosis (OR = 2.70) were moderately strongly associated with post-discharge suicide (Table 2, Figure 2). Factors weakly associated with post-discharge suicide (OR 1.5–2.5) were male sex, recent social difficulties, a diagnosis of major depressive disorder, the presence of suicidal ideas and an unplanned discharge (Table 2, Supporting Data Table 1).
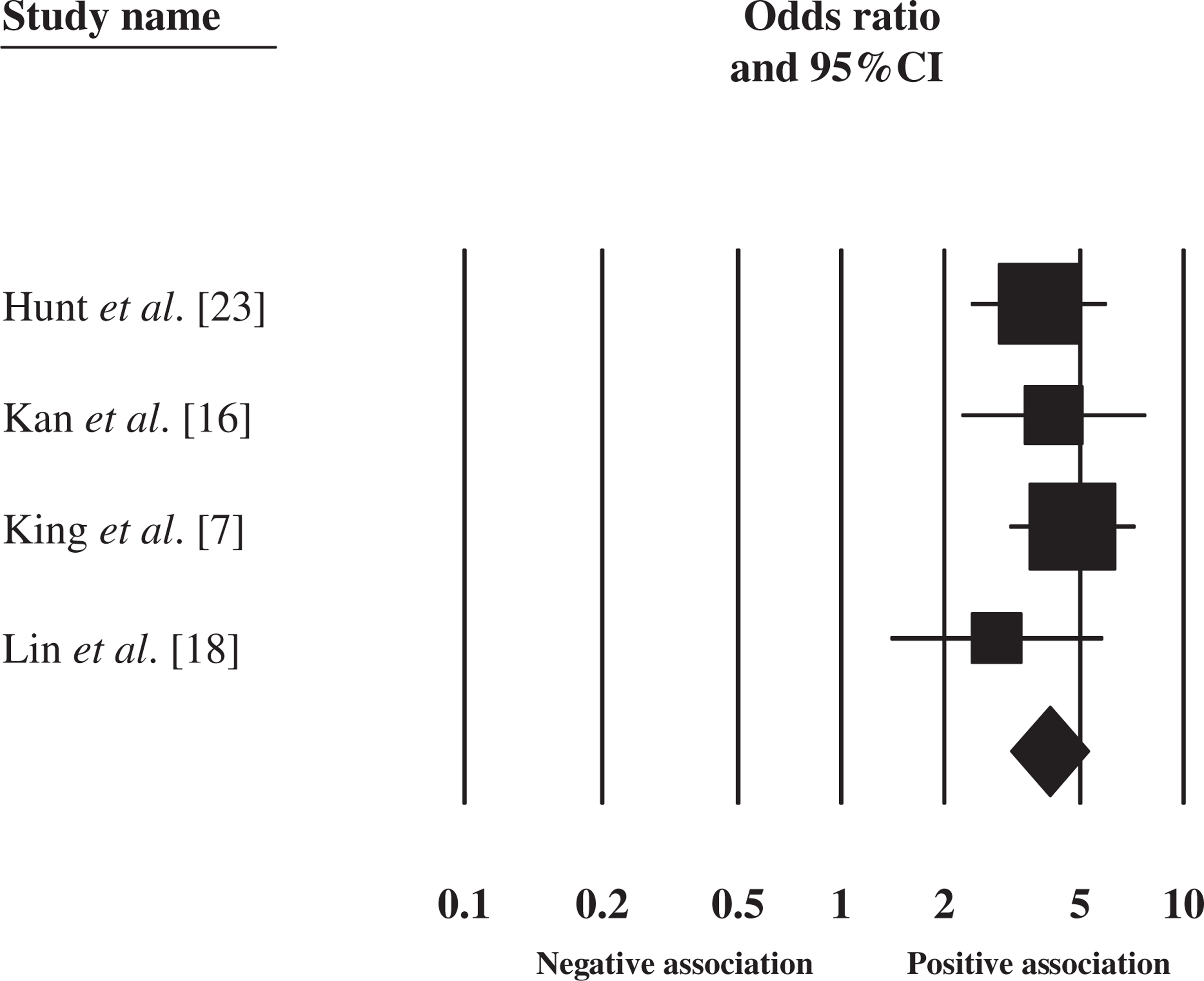
The association between retrospectively classified high risk status and suicide after discharge. Squares and whiskers represent study sizes and the 95% confidence intervals and diamond represents the pooled result and 95% confidence intervals.
Meta-analysis of the associations between demographic, historical, clinical and treatment variables and suicide within a year of discharge from a psychiatric hospital.
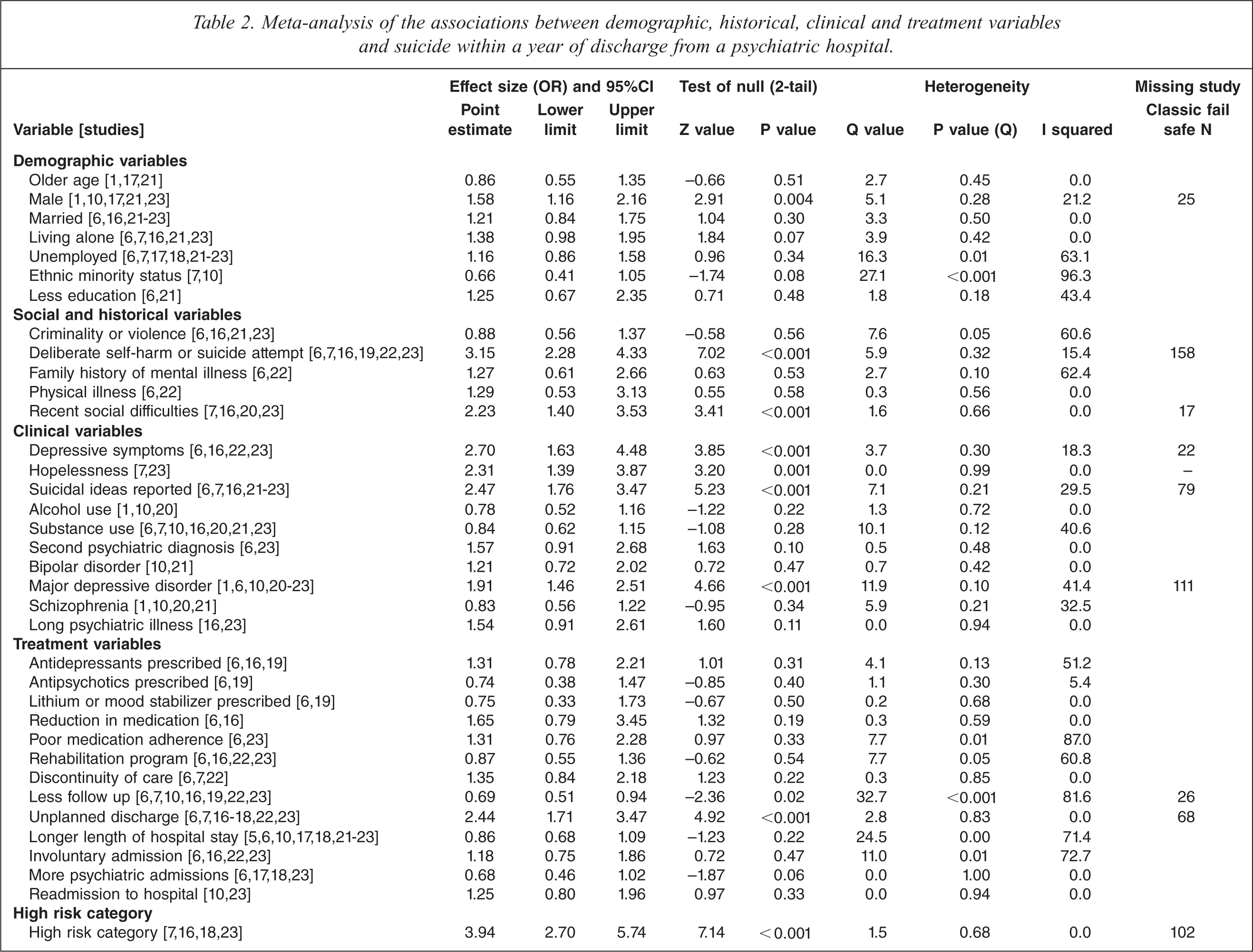
Demographic factors not associated with suicide in the year after discharge included the patient's age, marital status, living alone, employment status, ethnicity and level of education. Factors in the patient's history that were not associated with suicide after discharge were a prior history of criminal conduct or violence, a family history of mental illness and co-existing physical illness. Clinical variables not associated with later suicide were alcohol abuse, use of other substances, a dual diagnosis of a substance abuse disorder and mental illness, a diagnosis of bipolar disorder or schizophrenia, or a long duration of illness. Treatment factors not associated with later suicide were treatment with antidepressant, antipsychotic and mood stabilizing medications, a reduction in the dose of medication after discharge, and poor adherence to medication. Patients who had interrupted care (such as a change in consultant), or who had been re-admitted to hospital, or who had had more prior admissions or who had spent longer in hospital at their last admission were not at a significantly increased risk of suicide in the year after discharge.
Patients who received less psychiatric follow up because they were either discharged from care or had less frequent outpatient appointments were less likely to commit suicide in the year after discharge (OR = 0.69).
A fail-safe N test found that a large number of unpublished studies with an effect size of zero would be required to return p ≥ 0.05 (Table 2).
High risk categorization
In four studies high risk categories were defined by the authors on the basis of some patients having two or more factors that were significantly associated with suicide in the year after discharge. Each of the four studies defined patients as high risk using a different combination of factors and no factor appeared in all four models. Deliberate self-harm and the presence of suicidal ideas were included in three of four high risk models. The patients who were retrospectively classified in the original studies as being at high risk because of the presence of multiple risk factors were more likely to commit suicide than low risk patients (OR = 3.94) (Figure 2). The combined sensitivity of those categorizations was 0.40 (95%CI = 0.29–0.051) and the specificity was 0.87 (95%CI = 0.79–0.92).
Discussion
It is widely assumed that clinicians should use the presence of known risk factors to direct more intensive treatment to patients believed to be most at risk of suicide after discharge from hospital. However, since there are relatively few controlled studies examining risk factors for suicide after discharge, it is likely that clinicians make these suicide risk categorizations using risk factors for suicide in the wider community. These include male sex [24], single marital status [25], unemployment and economic hardship [26], substance abuse [27], physical illness [28] and psychiatric illness [29,30]. We found that only two of these community risk factors (male sex and depressive illness) were also risk factors among those recently discharged from psychiatric hospitals. However, when compared with other discharged patients, those who commit suicide within a year of discharge were not significantly more likely to be single, unemployed, to have serious physical illness, schizophrenia, bipolar disorder or substance abuse. In fact, the factors associated with increased risk of suicide among discharged patients were similar to the risk factors identified by a recent systematic review and meta-analysis for suicide in hospital or on approved or unapproved leave [11]. It appears that the risk factors associated with suicide in admitted psychiatric patients or recently discharged patients might differ significantly from the risk factors for suicide in the community.
We found two significant differences between the risk factors for patients within a year of discharge and those for current inpatients. First, inpatients with schizophrenia were at increased risk of suicide as inpatients, whereas the risk of suicide of patients with this diagnosis was not increased in the year after discharge. Second, being categorized as high risk according to the identified risk factors was strongly associated with suicide in hospital (OR = 10.9) [11] but was less strongly associated with suicide after discharge (OR = 3.94).
Utility and validity of high risk categorization for suicide after discharge
The positive predictive value (PPV) of a risk categorization instrument is an important measure of its utility. The PPV is the proportion of high risk patients that go on to commit suicide within a year of discharge. It is calculated using the formula:

Using the values for sensitivity (proportion of suicides which are correctly categorized = 40%) and specificity (the proportion of non-suicides which are correctly categorized = 87%) derived by meta-analysis of high risk models for suicide after discharge and an estimate of 1% for the incidence of suicide within a year of discharge, we calculated that only 3% of patients categorized as high risk will commit suicide in the year after discharge.
A second indicator of the utility of a risk categorization instrument is sensitivity. Sensitivity is the proportion of eventual suicides within a year of discharge categorized as at high risk. The sensitivity of 40% calculated by meta-analysis means that 60% of the patients who commit suicide after discharge would have been categorized as low risk.
Hence, using figures derived by meta-analysis from available retrospective models of suicide within a year of discharge it can be calculated that 97% of patients categorized as being at high risk will not go on to commit suicide and 60% of patients who commit suicide will have been categorized as low risk.
It should be noted that the retrospective nature of studies from which the high risk models were derived suggests that those models would not perform as well in prospective study and would not achieve the same figures for sensitivity or specificity. In three of the studies included in this meta-analysis researchers had retrospectively determined a method of high risk categorization using the results of comprehensive multivariate modelling of identified risk factors [7,16,23]. A fourth study found that depressed patients who discharged themselves against advice were at greatest risk [18]. All four studies used a combination of individual risk factors to define a sample of patients who could have been categorized as high risk at the point of discharge. A history of deliberate self-harm and the presence of suicidal ideas were included in three high risk models; living alone, discharge against advice, recent social difficulties and depressive disorder were included in two high risk models; and male sex, involuntary admission and ethnic minority status were each included as risk factors in one high risk model. These differences in the definition of ‘high risk’ between the studies highlights a problem faced in attempts to develop valid instruments to estimate the risk of suicide after discharge.
Most studies of the suicide of psychiatric patients examine a wide range of factors, (often in excess of 100 factors), associated with a relatively small number of suicides (frequently less than 100) [11]. In a study examining 100 factors, five factors can be expected to be associated with suicide at p ≤0.05 level by chance alone. The inclusion of these chance findings in a high risk model artificially inflates their predictive values in a process that has been referred to as ‘capitalization on chance associations in the original construction sample’ [31, pp 810]. This then results in ‘shrinkage’ of predictive power of the model in future samples [31]. This shrinkage in predictive power is particularly likely to occur in studies of suicide risk because of the large number of variables that are examined (increasing the likelihood of chance findings in individual studies), and the wide variation in study populations and circumstances. Hence, the predictive power of high risk models of suicide within a year of discharge that might be found in a future prospective study is likely to be considerably lower than the findings suggested by our meta-analysis of the existing retrospectively constructed models.
Discharge planning and follow up
Patients who are so unwell as to require an admission to a psychiatric hospital will almost invariably warrant a discharge plan and follow up arrangements, regardless of their perceived risk of suicide. The finding that unplanned discharge is associated with an increased risk of suicide could suggest that making sure that as many patients as possible had a discharge plan might save some lives. However, it should be acknowledged that it is not always possible to make a planned discharge, and some of those who discharge themselves might have other characteristics that place them at risk of suicide.
A separate issue relates to the finding of a positive association between suicide and the amount of psychiatric follow up. Although it is conceivable that increased psychiatric follow up might actually increase the risk of suicide, a much more plausible reason for this finding is that those patients provided with more follow up had already been identified as being more likely to commit suicide.
Limitations of the study
The study had several limitations. First, all of the studies included in the meta-analysis were naturalistic studies that relied on observations of routine clinical care. It is likely that some patients were identified as being at high risk by the treating clinicians, using similar risk factors to those included in high risk models. For example, some patients classified as high risk in the studies are likely to have been identified as being at high risk prospectively because of their history of deliberate self harm and expressed suicidal ideas. These patients might have received more care and this extra care might have prevented some suicides, leading to an under estimation of the positive predictive value of suicide risk categorization.
Second, there was a relatively small number of published studies that specifically compared the characteristics of patients who suicided within a year with similarly discharged controls. The nature of our inclusion criteria saw the exclusion of some large and well known Australian studies, that examined a mixture of inpatients and outpatients [32] or included suicides after longer periods of follow up [33–35]. Our focus allowed us to address the risk factors for suicides shortly after discharge but might have left the meta-analysis with insufficient power to detect some true associations. Third, the small number of studies meant we were unable to investigate between-study heterogeneity. It is possible that some variables might be strongly associated with suicide in the first month of discharge but weakly associated with suicide between six months and a year post discharge. Some true associations with suicide at certain periods, for example immediately after discharge, may have been concealed by this limitation.
Fourth, the available data does not allow an assessment of the extent of co-variation and the interactions between factors, which could be considered in a meta-analysis of individual subject data, if such data becomes available in the future [36].
The results of this meta-analysis show that it is even harder to usefully categorize patients as at risk for suicide after discharge than it is to categorize them according to their risk of suicide while in hospital. Comparing the results of this study and that of a related meta-analysis [11], the association between gaining a high risk categorization and suicide after discharge was weaker than the association between gaining a high risk categorization and suicide whilst an inpatient. Possible explanations for this discrepancy include the following.
Unpredictable intervening events that alter the risk of suicide which cannot be factored into a suicide assessment might be more likely after discharge than in a hospital setting.
Suicide of psychiatric inpatients has been the subject of a larger number of studies and it is possible that the smaller number of studies of suicide after discharge have not examined all the factors that are associated with these suicides. It is possible, for example, that differences in the quality of inpatient care might be an important factor, particularly if patients who become suicidal after discharge feel uncomfortable about returning to hospital because of an unsatisfactory earlier experience in hospital.
It might be that studies of suicide after discharge are intrinsically more difficult to perform than studies of inpatient suicide, leading to a reduction in the strength of the estimated associations. For example, studies of suicide after discharge face particular problems with case identification. A sound study of suicide after discharge requires that either the suicide mortality of all discharged patients is known or that information about prior hospitalizations is available for each suicide victim. Studies conducted in smaller geographic regions [22], or from a single hospital [21], might not include patients who move. Case identification is likely to be more complete in studies involving multiple hospitals and larger geographic areas, especially if they are able to employ methods such as the co-registration of national health and mortality data sets [16]. However, data collected and recorded prospectively in health data sets can be limited to demographic details and the final diagnosis. In contrast clinical data collected after a suicide is likely to be more complete but less accurate because of hindsight bias [5,17,18]. Hence, studies of suicide after discharge are likely to miss a higher proportion of cases and are likely to have less detailed information than studies of inpatient suicide. This can result in a higher likelihood of error in both the dependent variable (suicide) and independent variables (risk factors) which is likely to result in a reduction in magnitude of effect sizes of otherwise significant associations with suicide after discharge.
Conclusion
The suicide of a recently discharged patient is one of the most serious events faced by a mental health service. In addition to the severe loss and grief of the survivors and the distress felt by clinicians involved in the patient's care, these events are frequently followed by internal and external enquiries and litigation that can be damaging to the morale of clinicians and the treating teams. According to our analysis, no single factor, or combination of factors, is strongly associated with suicide in the year after discharge and while about 3% of patients categorized as being at high risk can be expected to commit suicide in the year after discharge, about 60% of the patients who commit suicide are likely to be categorized as low risk. These results can help to put the problem of post-discharge suicide into perspective, because they demonstrate the severe limitations of attempting to categorize patients by their risk of suicide after discharge from hospital.
Footnotes
Acknowledgment
We thank Peter Arnold for his assistance with the manuscript.