
Abstract
Objective:
Understanding of nonsuicidal self-injury relies almost exclusively on adolescent and emerging adult samples. We investigated the prevalence of lifetime and past-year nonsuicidal self-injury among New Zealanders aged 16–75 years and above, before evaluating if established associations between nonsuicidal self-injury, and demographic and psychological characteristics generalise to adults.
Method:
New Zealand adults (n = 4906; median age 55–59 years; 55.5% female) completed a cross-sectional survey assessing lifetime and past-year nonsuicidal self-injury, psychological distress, self-esteem, emotion dysregulation, and social desirability susceptibility.
Results:
Nonsuicidal self-injury was common among adults; 25.6% participants reported ever self-injuring and 10.7% had done so at least once in the past year. Women and younger participants were more likely to report lifetime self-injury. Although younger participants were also more likely to report past-year self-injury than older participants, this age effect was attenuated for men (b = −0.09) compared to women (b = −0.18). Self-esteem (odds ratios 0.74, 0.74), psychological distress (odds ratios 1.09, 1.16), emotion dysregulation (odds ratios 2.05, 1.88), and desire to manage others’ impressions of oneself (odds ratios 0.88, 0.85) were uniquely associated with both lifetime and past-year nonsuicidal self-injury, respectively, and these effects were not moderated by age.
Conclusion:
Although self-injury was most common among emerging adults, adults of all ages reported self-injuring. Individuals with a greater desire to manage how others perceive them appeared to underreport their nonsuicidal self-injury. While men were less likely than women to self-injure, they may also be more likely to continue self-injuring over adulthood, suggesting that the developmental factors which drive self-injury cessation among adults differ for men and women.
Plain Language Summary
Current understanding of the nature, risk and protective factors, and correlates of nonsuicidal self-injury (NSSI) is based almost exclusively on adolescent and emerging adult samples. Therefore, while we assume that people of any age may hurt themselves, we have little empirical evidence concerning prevalence or predictors of self-injury among adults, and particularly those aged above 40 years. To address this gap, we used a large, nationwide, online survey to estimate the prevalence of lifetime and past-year NSSI, and the nature and magnitude of correlations with a range of common self-injury-related predictors. The Mental Health State of the Nation survey was promoted by a national New Zealand media organisation and solicited responses from 4906 participants (median age 55–59 years; 55.5% female). Participants completed questionnaires assessing lifetime and past-year self-injury, distress, self-esteem, emotion dysregulation, and social desirability bias. Self-injury was common among participants; 25.6% reported ever self-injuring (10.7% at least once in the past year). Women and younger participants were more likely to report self-injury; almost two-thirds of participants aged below 25 years reported lifetime self-injury compared to 1 in 10 participants aged 65 years and older, and this age effect was reduced for men (b = −0.09) compared to women (b = −0.18). Self-esteem, psychological distress, and emotion dysregulation were all uniquely associated with both lifetime and past-year self-injury, as was reported tendency to manage others’ impressions of oneself, suggesting individuals with a greater desire to manage how others perceive them appeared to under-report their self-injury. Although men were less likely than women to self-injure, they may also be more likely to continue self-injuring over adulthood, suggesting that the developmental factors which drive self-injury cessation among adults may differ for men and women.
Introduction
Nonsuicidal self-injury (NSSI), where an individual deliberately and directly causes harm to their body (e.g. by cutting, scratching, or burning the skin) without suicidal intent, represents a significant mental health concern. NSSI is concurrently associated with elevated psychological distress (e.g. Nock et al., 2006; Whitlock et al., 2006) and longitudinally predicts subsequently poorer wellbeing (Gandhi et al., 2017; Robinson et al., 2019), onset of psychiatric illness (Wilkinson et al., 2018), and increased risk of suicidal thoughts and behaviours (Mars et al., 2019; Ribeiro et al., 2016). NSSI onset typically peaks in early adolescence (Plener et al., 2015), with a second, smaller peak in emerging adulthood (Kiekens et al., 2019). Meta-analyses estimate that 13.4–22.9% of adolescents and emerging adults have engaged in NSSI (Gillies et al., 2018; Muehlenkamp et al., 2012; Swannell et al., 2014), and that young women are more likely to self-injure than young men (Bresin and Schoenleber, 2015; Swannell et al., 2014). Despite the robust literature investigating NSSI among adolescents and emerging adults, considerably less is known about NSSI among adults (for reviews, see Van Hove et al., 2023; Whitlock and Selekman, 2014).
The limited community-based empirical evidence suggests that NSSI is not limited to adolescence and emerging adulthood. Meta-analysis of nine community samples estimated that 5.5% of adults aged ⩾ 25 years report lifetime NSSI (Swannell et al., 2014). However, data from adults seeking psychological treatment suggest considerable variability in NSSI across adulthood. Among patients discharged from New Jersey hospitals with a primary diagnosis of intentional self-harm (a broader category of self-inflicted harm that can include suicidal intent), 50.4% were 15–34, 37.9% were 35–54, and 11.8% were aged above 55 years (Miller et al., 2013). Clinicians at Norwegian adult psychiatric outpatient clinics reported a similar pattern of decreasing prevalence by age; 8.1% of all patients had self-injured in the past 4 weeks, ranging from 11.6% of patients aged 18–23, 6.4% among those 40–49, and 2.9% among those aged ⩾ 70 years (Ose et al., 2021). However, these samples are likely not representative of all adults who self-injure; the majority of youth who self-injure never seek psychological treatment (Hasking et al., 2015; Robinson et al., 2021; Whitlock et al., 2006). Initial evidence drawn from a random digit-dialled sample of US adults aged above 18 years identified similar variability across adulthood (Klonsky, 2011). Specifically, lifetime NSSI was negatively associated with age (rpb = −0.25) such that 18.9% of adults ⩽ 30 years reported NSSI compared to only 4.8% of those aged above 30 years (Klonsky, 2011).
Estimating the prevalence of NSSI among adults is further complicated by widespread NSSI stigma (e.g. Staniland et al., 2020, 2022). Given this stigma, NSSI self-reports are likely influenced by social desirability bias, where people tend to underreport socially undesirable attitudes and behaviours and over-report socially desirable attitudes and behaviours (Paulhus, 1984). Indeed, individuals differ in the extent to which they purposely present themselves in a manner to fit a social situation (i.e. impression management) and are motivated to maintain a positive self-concept (i.e. self-deceptive enhancement; Paulhus, 1984). Greater perceived mental health stigma has been associated with non-response to suicide-related survey items (Kyron et al., 2020), suggesting that individual differences in impression management (or self-deceptive enhancement) may influence reporting of self-injurious behaviours more generally. Preliminary research suggests 12.5–23.7% of adolescents and young adults who report engaging in NSSI behaviours do not consider themselves to have self-injured (Aspeqvist et al., 2024; Robinson and Wilson, 2020), providing tentative evidence that self-deceptive enhancement may also influence NSSI reporting. Self-injury stigma – and thus, social desirability bias – may also disproportionally impact older adults (Van Orden and Conwell, 2016). Although research has demonstrated negative associations between impression management and self-deceptive enhancement with self-reports of other stigmatised health behaviours (i.e. probable underreporting; King, 2022; Latkin et al., 2017; Perinelli and Gremigni, 2016), associations with NSSI remain unexplored.
Looking beyond prevalence, little is known of the psychological characteristics of community-based adults who self-injure. Mirroring findings from adolescents and emerging adult samples (e.g. Nock et al., 2006; Robinson et al., 2021; Whitlock et al., 2006), age above 40-year-old Australians with past-year NSSI reported greater psychological distress, more lifetime suicide attempts, and were more likely to have a psychiatric diagnosis compared to those without lifetime NSSI (Martin and Swannell, 2016). Although psychological distress, emotion dysregulation, and self-esteem are robustly associated with NSSI among adolescents and emerging adults (for reviews, see Bentley et al., 2015; Forrester et al., 2017; Wolff et al., 2019), these relationships remain largely untested among middle-aged and older adults. Initial evidence suggests that the nature of these relationship may differ across adulthood. Among adults presenting with self-harm to emergency departments, middle-aged adults (45–64 years) were more likely to report physical illness as a stressor, have a history of depression and be diagnosed with depression compared to older-aged adults (>65 years; Tan and Cheung, 2019). Given that psychological distress, emotion regulation, and self-esteem processes change across the lifespan (e.g. Caspi et al., 2020; Orth et al., 2010; Orth and Robins, 2014; Silvers, 2022; Zimmermann and Iwanski, 2014), investigation across adulthood is warranted.
Therefore, we aimed to understand the prevalence and nature of lifetime and past-year NSSI among community adults, considering individual differences in demographic and psychological characteristics. Based on the findings from adolescent and emerging adult samples, we predicted both lifetime and past-year NSSI to be more commonly reported by women and younger participants and be associated with greater psychological distress and emotion dysregulation, and less self-esteem. We also explored the association between NSSI and social desirability (both impression management and self-deceptive enhancement). Preregistered predictions and analysis plans are available at: https://osf.io/j8ud4.
Method
Participants
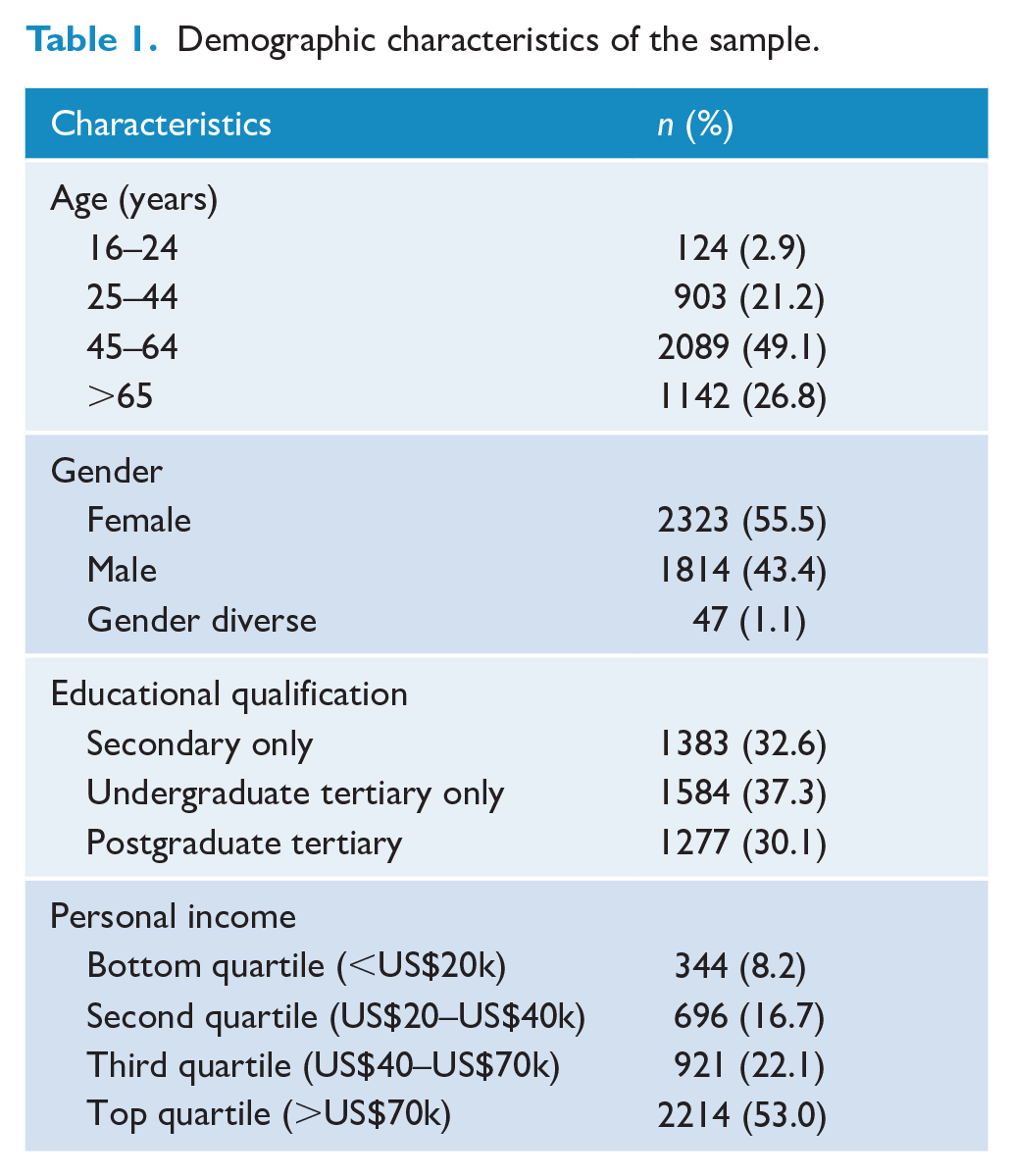
Nationwide news outlet The Sunday Star Times and Stuff advertised the survey over a 3-week period in September–October 2023 as a ‘survey canvassing Kiwis’ mental wellbeing and attitudes towards various social and scientific issues’ timed to coincide with a General Election and Rugby World Cup. The current study comprises participants (n = 4906) who completed items assessing NSSI (74.2% of those who accessed the survey). Table 1 summarises sample demographic characteristics. The median age band was 55–59 years, with 2.9% aged 16–24, 21.2% aged 25–44, 49.1% aged 45–65, and 26.8% aged > 65 years. There was a higher proportion of female (55.5%) than male (43.4%) and gender-diverse (1.1%) participants. Most participants identified as Pākehā/New Zealand European (84.2%), with 2.8% identifying as Māori, 0.6% as Pacific people, 0.8% as Asian, and 11.6% identifying as a non-listed ethnicity. Compared to Aotearoa New Zealand population estimates (Statistics New Zealand, 2018), participants were slightly more educated (median highest qualification was bachelor’s degree or trade certificate) and tended to report slightly higher personal income (median annual income bracket was US$70,001–US$80,000 NZD). Participants provided informed consent and received information about mental health supports available to them.
Demographic characteristics of the sample.
Measures
Demographic information
Participants reported their age using response bands and their gender using an open text box. Gender descriptions were classified into ‘male’, ‘female’, and ‘gender-diverse’ according to previous guidelines (Fraser et al., 2020).
NSSI
All participants reported their lifetime and past-year engagement in five common NSSI behaviours: cutting; punching/banging; scratching; preventing wound healing; and sticking sharp objects under the skin; and ‘done something else that caused direct harm to your skin or body’. Items were drawn from the Deliberate Self-Harm Inventory (Lundh et al., 2007) and were selected as the most commonly endorsed NSSI behaviours in previous Aotearoa New Zealand samples (e.g. Garisch and Wilson, 2015; Robinson et al., 2021). Participants were introduced to the items with: Research shows that perhaps as many as 60% of New Zealanders have deliberately hurt themselves, without any intention to die. However, most of this research comes from adolescents and young adults and we have no idea how many adults have thought about this.
Individual items were prefaced with ‘Have you ever deliberately (but without wanting to die). . .’ before listing the behaviour. Participants responded using the options ‘No’ or ‘Yes, I have done this at least once’. Participants who reported engaging in one or more NSSI behaviours were classified as having lifetime NSSI (vs no lifetime NSSI) and were invited to complete additional NSSI items. Participants who indicated they had engaged in at least one form of NSSI in the past were then asked ‘Have you done any of these things in the past year?’ before listing the same five behaviours. Participants responded using the options ‘No’, ‘Yes, on less than five days’ and ‘Yes, on more than five days’. Participants who reported engaging in one or more NSSI behaviours in the past year were classified as having past-year NSSI (vs no past-year NSSI).
Psychological distress
Psychological distress was assessed using the 12-item General Health Questionnaire (Goldberg & Williams, 1998). Participants responded to items including ‘Have you recently lost much sleep over worry?’ and ‘Have you recently been feeling unhappy and depressed?’ on a four-point Likert-type scale ranging from 1 – More so than usual to 4 – Much less than usual. Consistent with previous research (Goldberg & Williams, 2000), responses of 1 and 2 were recoded as 0, and responses of 3 and 4 as 1, before calculating an aggregate score (possible range: 0–12) where higher scores indicate greater psychological distress. A score of 4 or more on the GHQ is taken as indicative of clinically significant distress; 20.2% met this threshold, comparable or slightly lower than previous uses reported in New Zealand (e.g. 23.4%, Bushnell et al., 2001; 31%, Davis et al., 2008).
Emotion dysregulation
Emotion dysregulation was assessed using the 18-item Difficulties in Emotion Regulation Scale – Short Form (α = 0.89; Kaufman et al., 2016). Participants responded to items such as ‘When I’m upset, I acknowledge my emotions’ and ‘I am confused about how I feel’ on a five-point Likert-type scale ranging from 1 – Almost never to 5 – Almost always. Responses were averaged to create an overall emotion dysregulation score.
Self-esteem
Self-esteem was assessed using two items from the Rosenberg (1965) Self-Esteem scale. Participants responded to the items ‘I take a positive view of myself’ and ‘All in all, I am inclined to think that I am a failure’ (reverse-coded) on a seven-point Likert-type scale ranging from 1 – Strongly Disagree to 7 – Strongly Agree which were averaged to create an overall self-esteem score (r = 0.64).
Social desirability
Social desirability was assessed using a short version (Hart et al., 2015) of Paulhus’ (1984) Balanced Inventory of Desirable Responding, capturing Self-Deceptive Enhancement (the non-conscious tendency to unrealistically view oneself positively: three items, α = 0.46) and Impression Management (the tendency to present oneself positively to others: three items, α = 0.56). Participants responded to three items assessing each factor (Hart et al., 2015), such as ‘I am very confident of my judgements’ (Self-Deceptive Enhancement) and ‘I sometimes tell lies if I have to’ (Impression Management) on a seven-point Likert-type scale ranging from 1 – Strongly Disagree to 7 – Strongly Agree. Responses within each subscale were averaged to create overall self-deceptive enhancement and impression management scores.
Missing data
We compared the characteristics of those who completed the NSSI questions with those who did not, where we had data to allow the comparison. Completers did not differ from non-completers for psychological distress and impression management (ps = 0.40 and 0.10), but reported greater emotion dysregulation (M = 2.25, SD = 0.54 vs M = 2.13, SD = 0.45; p < 0.001), poorer self-esteem (M = 5.03, SD = 1.56 vs M = 5.32, SD = 1.36; p < 0.001), and lower scores for self-deceptive enhancement (M = 3.92, SD = 1.01 vs M = 4.09, SD = 1.05; p < 0.01). Slightly more men (1797 vs 1767.5) and slightly fewer women (2291 vs 2320.5) completed the NSSI measures than expected by chance, χ2 (1, N = 4457) = 10.50, p < 0.001. Non-completers were slightly more likely to be aged 45–65 years, and 65 years and older, χ2 (3, N = 4640) = 22.05, p < 0.001. Incomplete cases where participants had not reported their lifetime NSSI engagement were removed. Next, missing data for variables (excluding age and gender) were imputed using expectation maximisation with 50 iterations, as missing values analysis revealed that data were missing completely at random, χ2(26,880) = 26,976.97, p = 0.337. As demographic characteristics were assessed at the end of the survey battery, age was missing for n = 648 (13.2%), and gender was missing for n = 722 (14.7%). Age and gender were not imputed. Gender-diverse participants (n = 47) were excluded from analyses involving gender to guard against spurious findings. NSSI was common among gender-diverse participants (median age band 35–39 years); 72.3% reported lifetime NSSI and 53.2% reported past-year NSSI.
Analysis plan
Statistical analyses were conducted using SPSS (Version 29.0.0.0) with statistical significance set at p < 0.05, and p < 0.10 considered a statistical trend for predicted effects only. Data visualisations were created in R (Version 4.4.1). Pearson’s correlations, Spearman’s rho and chi-square tests were used to investigate associations between NSSI and demographic/psychological characteristics. Hierarchical binary logistic regression models tested unique associations between lifetime and past-year NSSI status with demographic (age, gender; entered at Step 1) and psychological (psychological distress, emotion dysregulation, self-esteem, impression management and self-deceptive enhancement; entered at Step 2) characteristics. Hierarchical binary logistic regression models also tested whether demographic characteristics moderate the relationship between psychological characteristics and NSSI. Demographic (age, gender) and psychological (psychological distress, emotion dysregulation, self-esteem, impression management and self-deceptive enhancement) characteristics were entered at Step 1. Interactions between demographic and psychological characteristics were entered at Step 2. Significant interactions were probed using simple slopes analysis (Aiken et al., 1991; PROCESS Version 4.3).
Results
Table 2 reports the prevalence of lifetime and past-year NSSI, separated by age and gender. Overall, 25.6% of participants reported lifetime NSSI, with 10.7% reported engaging in NSSI in the past year. As predicted, NSSI varied by age such that younger participants were significantly more likely (z = −8.47, p < 0.001) than older participants to report both lifetime (rs = −0.35, p < 0.001) and past-year NSSI (rs = −0.22, p < 0.001). Exploratory analyses of lifetime and past-year engagement in specific behaviours identified similar patterns of decreasing engagement by age (all χ2s (3) > 65.40, ps < 0.001), suggesting that participants of all ages engaged in similar NSSI behaviours. As predicted, NSSI also varied by gender such that women were more likely than men to report both lifetime, χ2 (1) = 38.75, p < 0.001, Cramer’s V = 0.10, and past-year NSSI, χ2 (1) = 18.34, p < 0.001, Cramer’s V = 0.07. Exploratory analyses revealed women were more likely than men to report engaging in all NSSI behaviours, all χ2s (1) > 5.66, ps < 0.017, except for punching or banging the body which showed similar prevalence rates across men and women. Both lifetime and past-year NSSI were associated with poorer self-esteem and greater psychological distress, emotion dysregulation, impression management and self-deceptive enhancement (see Figure 1 for intervariable correlations).
Percentage of sample reporting lifetime and past-year NSSI behaviours, separated by gender and age.
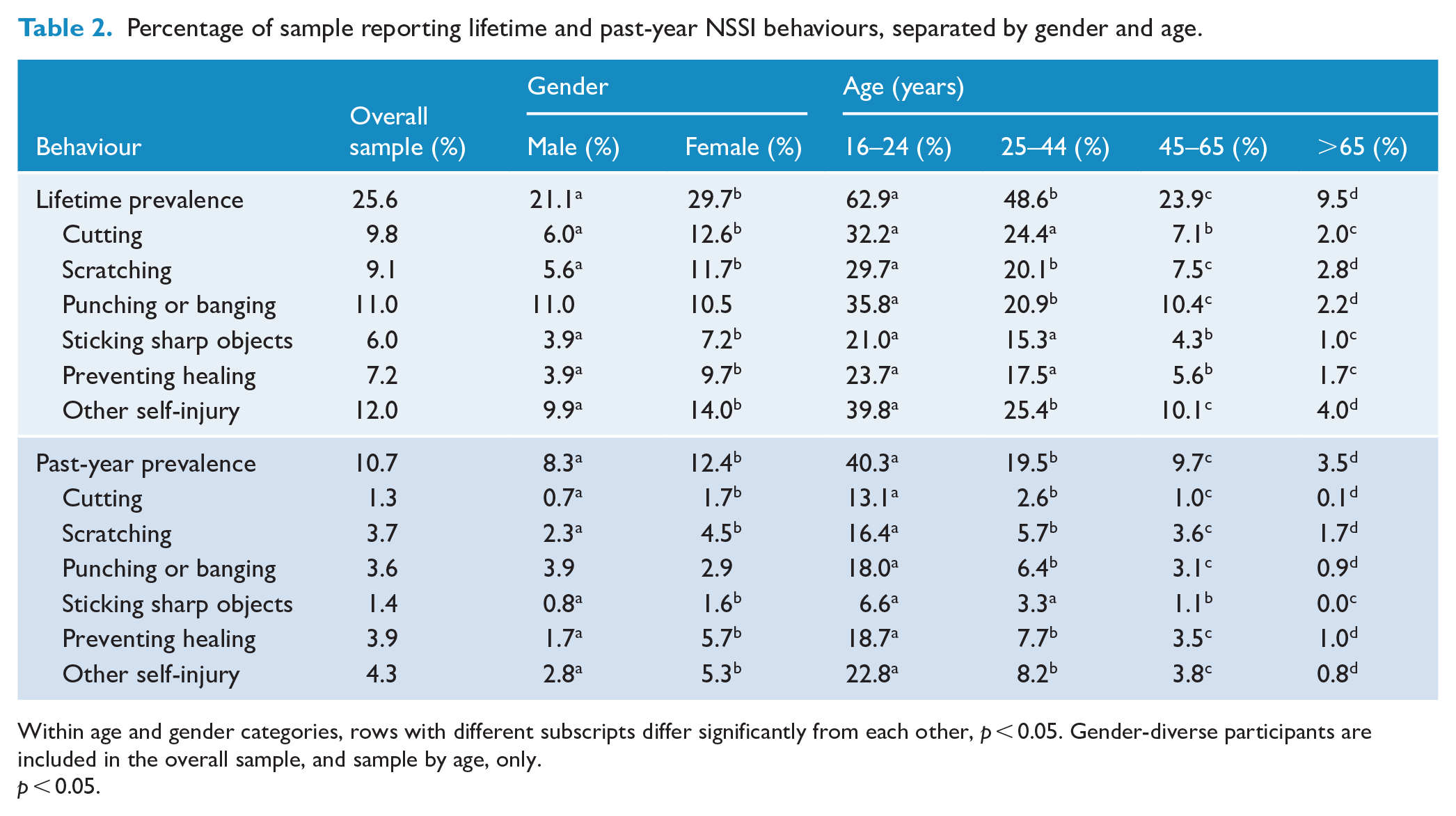
Within age and gender categories, rows with different subscripts differ significantly from each other, p < 0.05. Gender-diverse participants are included in the overall sample, and sample by age, only.
p < 0.05.
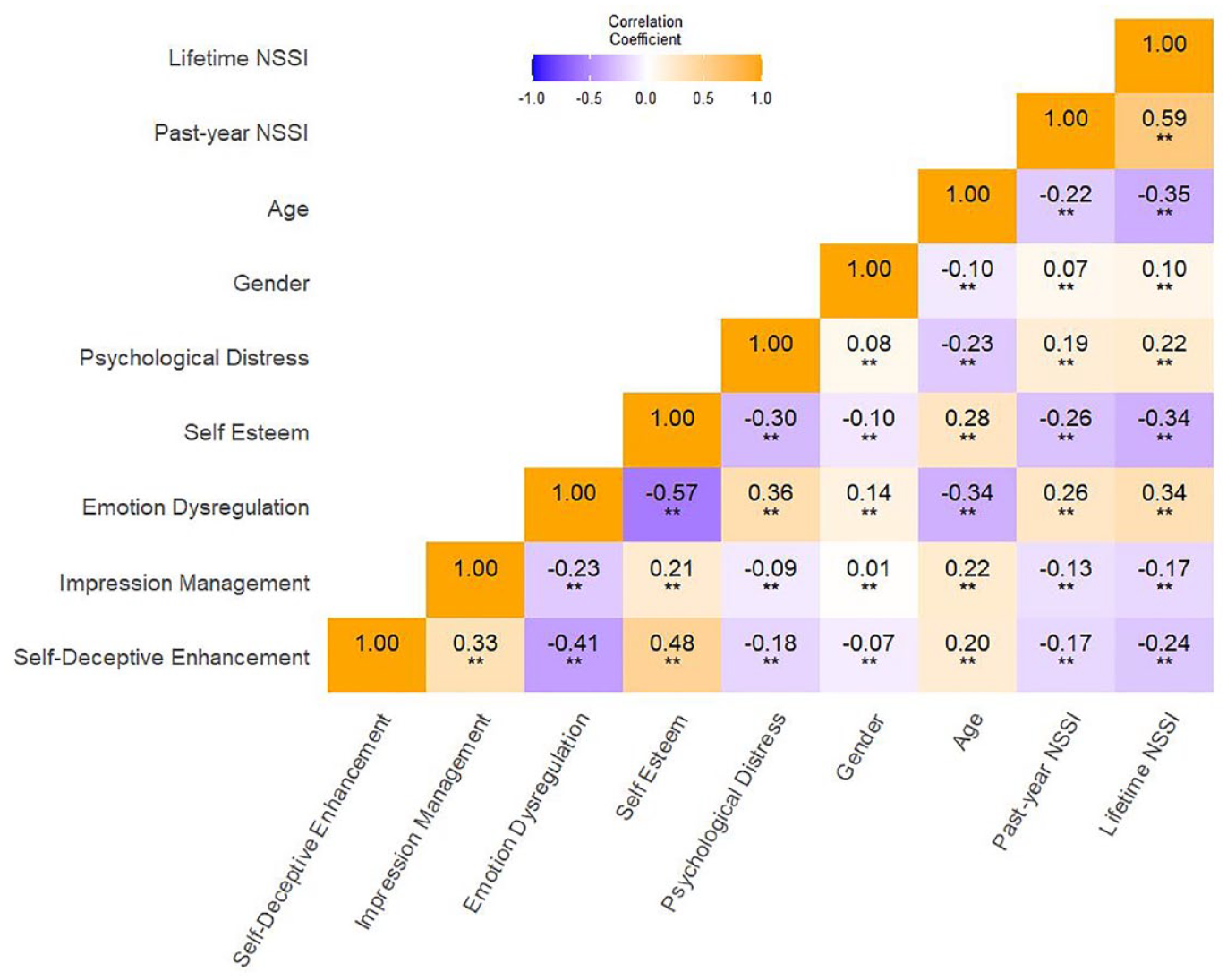
Zero-order correlations between demographic and psychological characteristics and lifetime and past-year NSSI status.
Given the associations among demographic and psychological characteristics, we next tested which (if any) factors were uniquely associated with NSSI. We conducted two hierarchical logistic regression models predicting lifetime NSSI and past-year NSSI (see Table 3). As predicted, younger participants and those reporting lower self-esteem, greater psychological distress and greater emotion dysregulation (most strongly) had greater odds of reporting both lifetime and past-year NSSI. When accounting for psychological characteristics, female gender identity predicted lifetime, but not past-year NSSI. Exploratory analysis considering individual differences in social desirability indicated that impression management, but not self-deceptive enhancement, was related to the lower odds of reporting both lifetime and past-year NSSI.
Demographic and psychological characteristics as predictors of lifetime and past-year NSSI status.
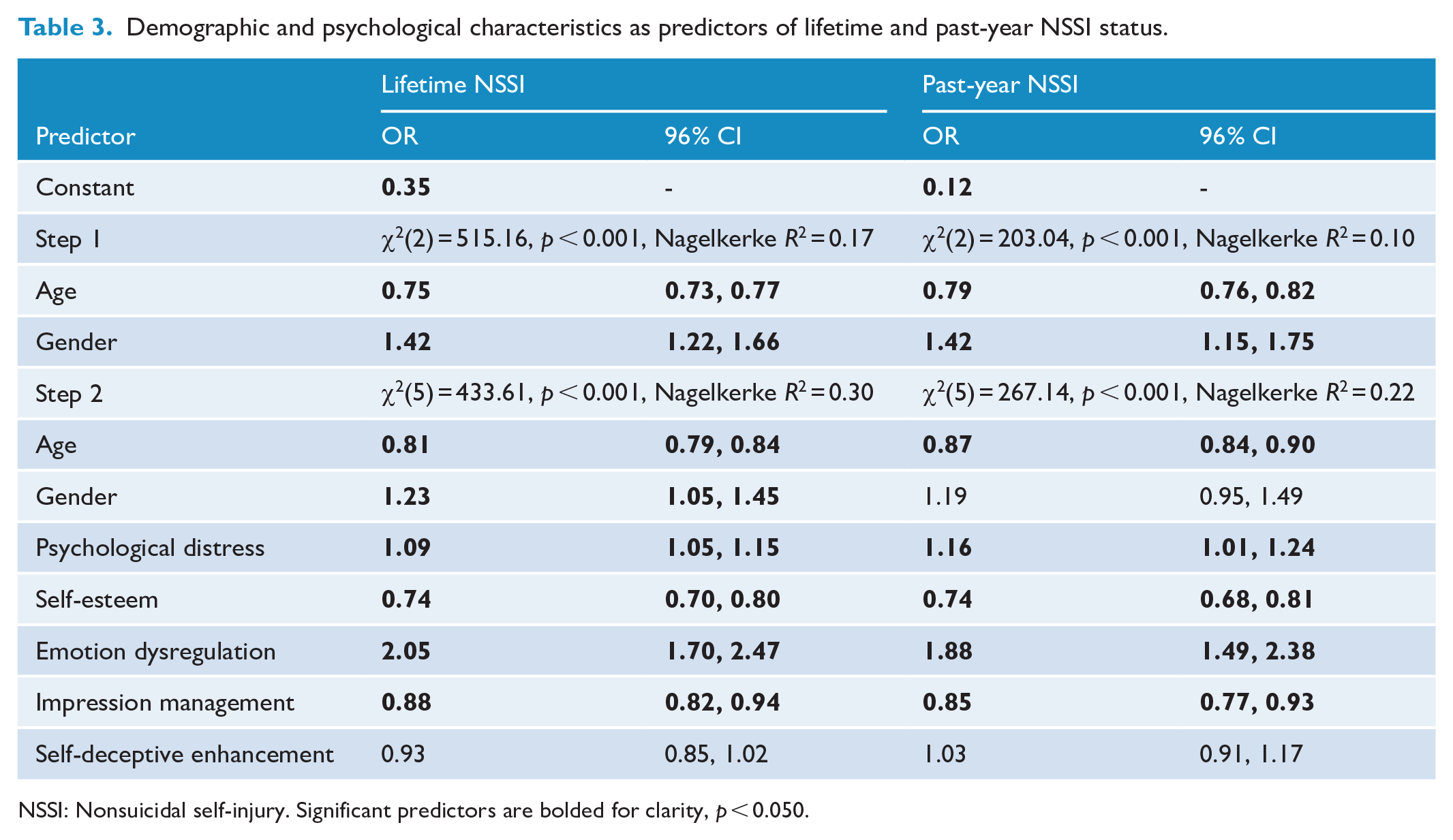
NSSI: Nonsuicidal self-injury. Significant predictors are bolded for clarity, p < 0.050.
Finally, we explored whether the relationship between psychological characteristics and NSSI varied according to age or gender. We conducted two hierarchical logistic regression models predicting lifetime and past-year NSSI status (see Table 4). Gender significantly moderated the relationship between age and past-year NSSI status. Age was negatively associated with past-year NSSI, but this relationship was stronger for women (b = −0.18, [95% CI: −0.23, −0.13], z = −6.78, p < 0.001) than men (b = −0.09, [95% CI: −0.15, −0.02], z = −2.73, p = 0.006; Figure 2). Neither age or gender moderated the relationships between psychological characteristics and either lifetime or past-year NSSI status. Note that the inclusion of personal income and education did not improve the prediction of lifetime, Δχ2 (2) = 1.83, p = 0.37, or past-year NSSI, Δχ2 (2) = 0.89, p = 0.64, or see changes in magnitude of relationships between other predictors and NSSI.
Interactions between demographic and psychological characteristics in predicting lifetime and past-year NSSI status.
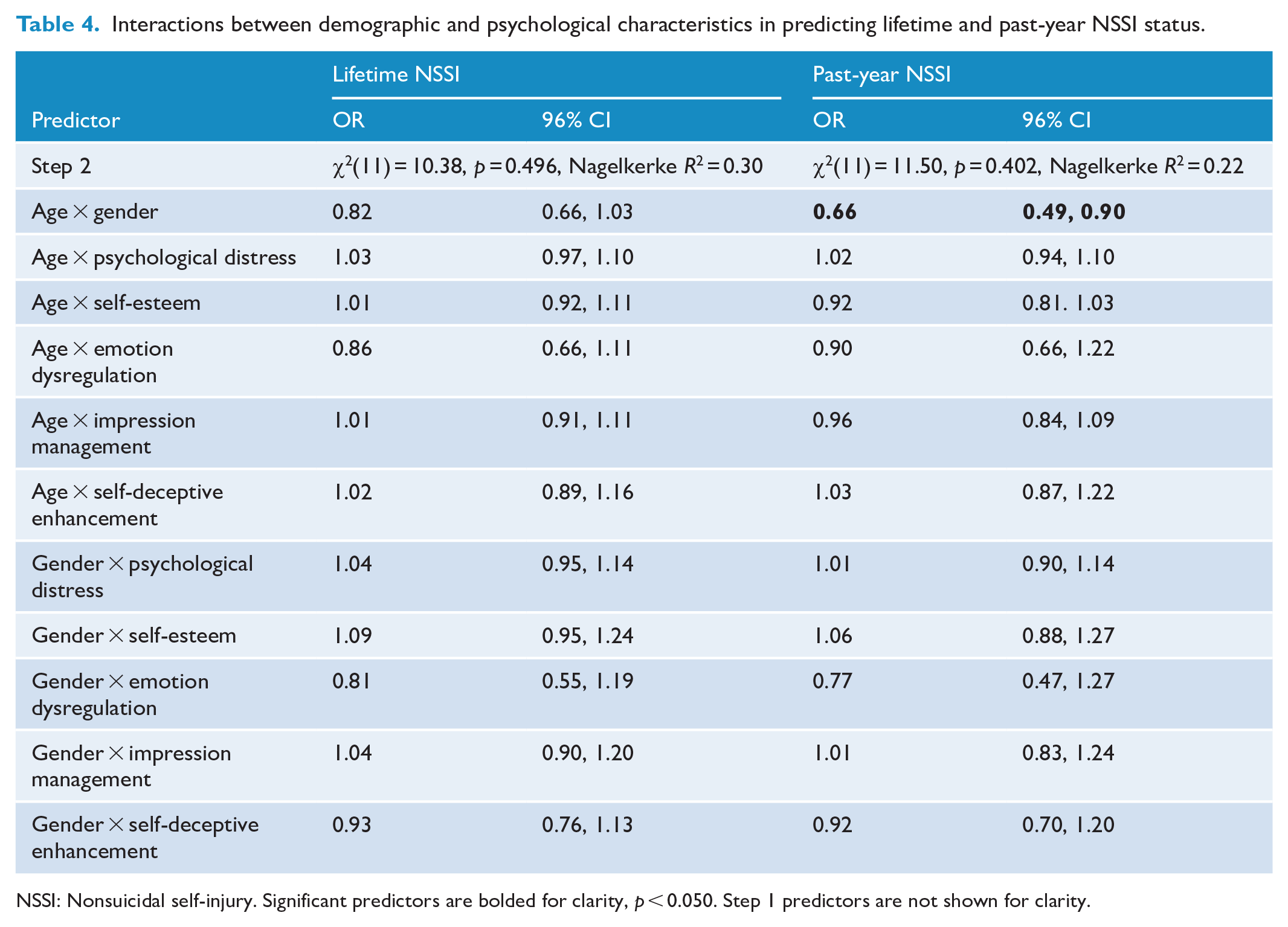
NSSI: Nonsuicidal self-injury. Significant predictors are bolded for clarity, p < 0.050. Step 1 predictors are not shown for clarity.
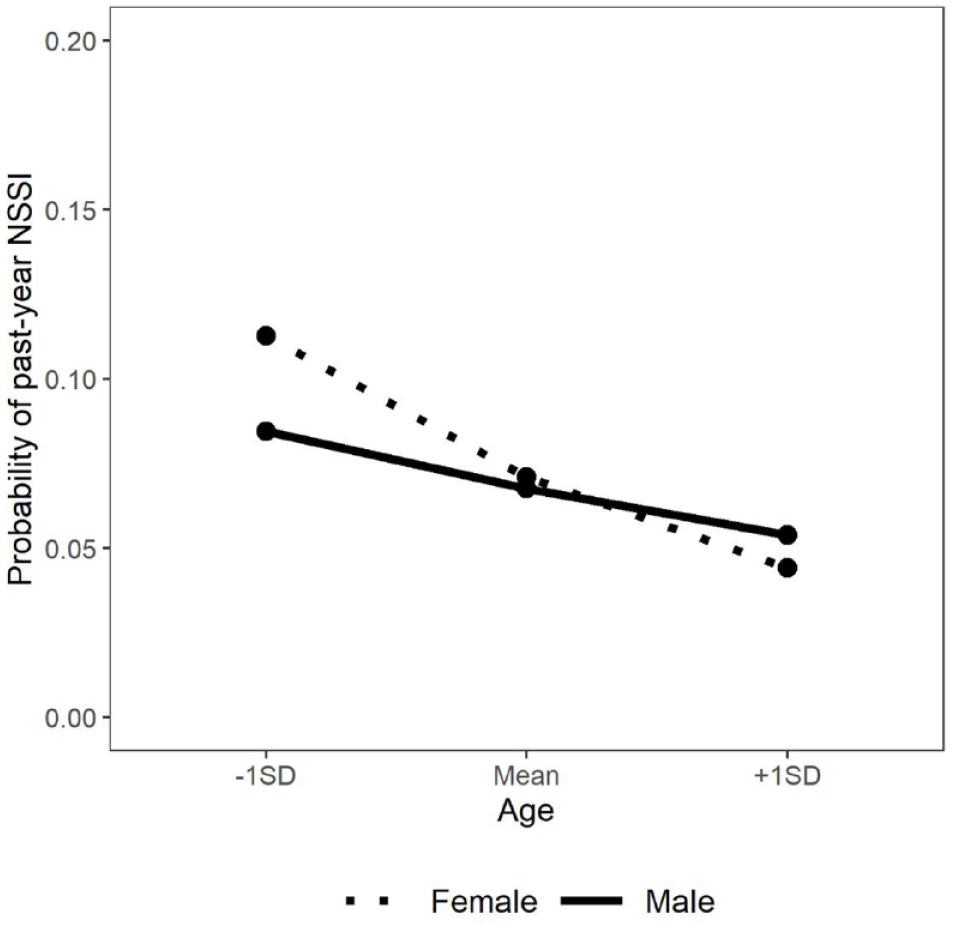
Association between age and probability of reporting past-year NSSI, moderated by gender.
Discussion
Growing evidence suggests that NSSI is not limited to adolescence and emerging adulthood (e.g. Klonsky, 2011; Swannell et al., 2014). However, fundamental understandings of who self-injures and the psychological context of NSSI currently draw almost exclusively on insights derived from adolescent and emerging adult samples, relying on untested assumptions that NSSI presents in the same manner across the lifespan. Drawing from a sample of 4906 New Zealand adults aged 16 years and above, we found that 25.6% of participants reported having ever engaging in NSSI and 10.7% had done so in the past year.
Age and gender were associated with lifetime NSSI, even when accounting for psychological characteristics. Older participants were less likely to report lifetime NSSI than their younger peers. For instance, 9.5% of adults aged above 65 years reported lifetime NSSI compared to 48.6% of adults aged 25–44 years. Given that lifetime prevalence of NSSI can ostensibly never logically decrease over the course of an individual’s life, this finding is consistent with meta-analytic evidence that the prevalence of adolescent NSSI has increased in recent years (Gillies et al., 2018). Although some individuals may forget or come to reinterpret their self-injury overtime (e.g. Mars et al., 2016), these potential memory effects are unlikely to completely account for the effect of age on lifetime NSSI. Consistent with previous meta-analysis drawn primarily from North American and European adolescent and young adult samples (Bresin and Schoenleber, 2015; Moloney et al., 2024), women were more likely to report lifetime NSSI than men. Notably, there were gender differences in engagement across all NSSI behaviours assessed except for self-injury by punching or banging the body (Bresin and Schoenleber, 2015; Victor et al., 2018).
While there are few studies that have included community samples of adults, our estimates of adult NSSI appear high. For example, Swannell et al.’s (2014) meta-analytic review of prevalence of NSSI identified a pooled estimate of 5.5% lifetime NSSI prevalence among ‘adults’ (defined as those aged 25 years and above), whereas 25.8% of our sample aged 25 years and above reported lifetime NSSI. One possibility is that NSSI may be more common in Aotearoa than elsewhere. However, NSSI is also assessed in a variety of ways, and commonly using either a single question (e.g. Briere and Gil, 1998) or a screening question leading to more detailed follow-up (e.g. Klonsky, 2011; Martin and Swannell, 2016) which we know underestimates NSSI prevalence compared to behavioural checklists as used in this research (Robinson and Wilson, 2020).
Demographic factors were also associated with past-year NSSI. Exploratory analysis revealed that although younger men and women were more likely to have self-injured in the past year than their older peers, this age effect was attenuated for men compared to women. Therefore, while men in Western countries are less likely than women to report ever self-injuring (Bresin and Schoenleber, 2015; Moloney et al., 2024), they may also be more likely to continue self-injuring throughout adulthood. In a similar manner, preliminary research tracking NSSI engagement across time finds that young men are more likely to report persistent NSSI than young women (Kiekens et al., 2017; Whitlock et al., 2015; although see Halpin and Duffy, 2020). Taken together, initial evidence suggests that the developmental factors that drive NSSI cessation across adolescence and adulthood may differ for men and women. Thus, interventions aimed at reducing NSSI among adults may need to be tailored differently for men and women, and for different age groups.
Findings revealed that the psychological context of adults who self-injure mirrored the well-established patterns found among adolescents and emerging adults (e.g. Bentley et al., 2015; Forrester et al., 2017; Wolff et al., 2019). Specifically, adults who reported lifetime and past-year NSSI also reported poorer self-esteem, greater psychological distress, and greater emotion dysregulation. Notably, demographic and psychological characteristics appear to explain slightly more variability in lifetime NSSI than in past-year NSSI. Neither age or gender influenced these associations, suggesting that the relationships between NSSI status and self-esteem, psychological distress and emotion dysregulation present in a similar manner across adulthood. Given that emotion dysregulation in particular is thought to drive engagement in NSSI (e.g. Chapman et al., 2006; Hasking et al., 2016; Nock, 2009), our results provide initial support that the therapeutic interventions scaffolding emotion regulation that successfully reduce NSSI among adolescents and emerging adults (Kothgassner et al., 2020, 2021) may show promise for middle-aged and older adults who self-injure.
Individual differences in susceptibility to social desirability influences (and particularly impression management) were also associated with NSSI. Accounting for demographic and psychological characteristics, adult who reported a greater desire to present themselves in a manner that fits the social situation were less likely to report self-injury. In contrast, we found no evidence that adults who were more motivated to maintain a positive self-concept were any more or less likely to report self-injuring, while also accounting for impression management. At the same time, we found that older people reported a greater tendency towards socially desirable responding (Figure 1) and other studies have indicated that age and gender may interact to predict socially desirable responding. Our findings add to the nascent literature quantifying the impact of stigma on assessment of self-injurious thoughts and behaviours. For example, Australian emergency personnel who preferred not to answer survey items assessing suicidal thoughts and behaviours reported greater mental health self-stigma and perceived higher mental health stigma in their workplace than their peers (Kyron et al., 2020). In contrast, we found that interpersonal perceptions, but not self-perceptions, influenced self-reports of NSSI, suggesting that the influence of self-perceptions on self-reports may be specific to suicidal thought and behaviours assessment.
Strengths and limitations
This research has two key strengths. First, we assessed NSSI using a behavioural-checklist that is less vulnerable to underreporting than a single-item or two-step screening process (i.e. Klonsky, 2011; Martin and Swannell, 2016), especially among men (Aspeqvist et al., 2024; Robinson and Wilson, 2020). Second, participants were recruited from the community via popular nationwide news outlets to participate in a survey about wellbeing, and sporting and political attitudes, comprising participants aged 16–75 years and above from all regions of Aotearoa New Zealand. Thus, although not sampled at random (i.e. Klonsky, 2011; Martin and Swannell, 2016), the current sample is more representative of the general adult population than samples recruited from treatment-seeking populations (Miller et al., 2013; Ose et al., 2021). Given that the sample reported slightly lower levels of distress (based on the GHQ-12) than other studies conducted in New Zealand (Bushnell et al., 2001; Davis et al., 2008), we have some confidence that the high rates of NSSI do not solely reflect a particularly distressed portion of the population. However, confirmation based on a representative sample of New Zealanders is a valuable next step.
Findings should also be considered in light of four key limitations. First, we assessed lifetime and past-year NSSI using a reduced set of items from the Deliberate Self-Harm Inventory (Lundh et al., 2007). Although we selected the five most commonly endorsed behaviours in Aotearoa New Zealand (e.g. Garisch and Wilson, 2015; Robinson et al., 2021), 91.8% of the lifetime NSSI sample reported using a method of self-injuring via a non-listed behaviour and for 24.6%, ‘something else’ was the only form of self-injury they endorsed. As a result, we cannot be certain whether adults may show differential engagement in the forms of NSSI not assessed here. In addition, NSSI (deliberate, self-directed damage of body tissue without suicidal intent) may be considered a subset of the broader family of deliberate self-harm. Assessment of NSSI (e.g. using the DSHI; Lundh et al., 2007) typically excludes behaviours that do not cause direct tissue damage (e.g. engaging in an emotionally abusive relationship), may cause indirect tissue damage (e.g. overdosing, dietary restriction) or where intent is either suicidal or ambiguous (Hooley et al., 2020). This pragmatic approach does, however, mean the likely exclusion of some behaviours that, for some people, may serve the same functions as more traditional NSSI behaviours (e.g. involve no suicidal intent, but are absent direct tissue damage). For example, Fox et al. (2016) reported that 55% of participants reporting NSSI also reported nonsuicidal overdosing (three-quarters used over the counter or prescribed medications). As a result, NSSI research, including our own, likely underestimates the prevalence of NSSI.
Second, NSSI was operationalised as lifetime and past-year status, preventing nuanced exploration of NSSI frequency, severity, functions and age of onset – characteristics that predict ongoing NSSI (Kiekens et al., 2017; Whitlock et al., 2015) and increased risk of suicidal thoughts and behaviours (Kiekens et al., 2018; Robinson et al., 2021). Third, data are cross-sectional. Longitudinal designs are needed to provide insight into how these relationships develop over time. Finally, we present here the analysis with no adjustments made for sociodemographic characteristics, such as socioeconomic status. Comparison with relevant census and OECD data indicates our sample is older, includes more women, is more educated and more highly paid than average. In our analyses, we focus particularly on age and gender, given their theoretical relevance for NSSI as there has generally been no evidence of differences in NSSI by income or education.
Although largely unrepresented in the empirical NSSI literature (e.g. investigation of NSSI form and function; Kuehn et al., 2022; Swannell et al., 2014), a meaningful proportion of middle-aged and older adults report engaging in NSSI in the past year. Despite the explicitly nonsuicidal nature of the behaviour, older adults who engage in NSSI may also be at elevated risk of hospitalisation and death than their peers (Choi et al., 2016). In addition, NSSI is a risk factor for subsequently poorer psychological health and wellbeing (Ribeiro et al., 2016; Robinson et al., 2019; Wilkinson et al., 2018). Mental health professionals working with adults of all ages should therefore routinely screen for both lifetime and current NSSI. Given that NSSI is related to other forms of self-harm (e.g. suicidal, indirect), screening for more generally for self-injurious behaviours is also warranted (e.g. Self-Injurious Thoughts and Behaviours Interview; Nock et al., 2007). Mental health professionals should be aware of widespread stigma regarding NSSI (e.g. Burke et al., 2019; Van Orden and Conwell, 2016) and take care to approach this topic systematically and respectfully, using appropriate language (Hasking and Boyes, 2018). Due to the limited research and training on self-harm, including NSSI, in adult age groups, clinicians may lack knowledge (e.g. Wand et al., 2018). Brief educational interventions may be necessary (e.g. Wand et al., 2021).
Conclusion
Our research indicates that self-injury is not something that only young people do, though self-reported rates of self-injury are lower among older adults than their younger peers. In addition, self-reported NSSI decreases as people endorse a greater tendency to engage in socially desirable responding, supporting the argument that NSSI may be seen as stigmatised (Staniland et al., 2020). However, adolescents and emerging adults have relatively higher rates of suicidal self-injury in common with older adults (Barak et al., 2020), suggesting that by developing our understanding of the nature and predictors of adult self-injurious behaviour in general, we may increase our ability to identify or prevent more serious outcomes. Given the nascent understanding of adult self-injury, future research should establish the factors uniquely or particularly associated with adult NSSI (e.g. caregiver strain, financial worries, loneliness), and the factors that generalise to self-injury across the lifespan (e.g. emotion dysregulation, psychological distress). In particular, the exploration of the lived experiences of middle-aged and older adults who self-injure is needed to develop a nuanced understanding of NSSI in this population.
Footnotes
Acknowledgements
The authors thank those who participated in this study, and Tracy Watkins and the staff at Stuff.co.nz. In addition, they thank Maggie Shippam for the assistance with data visualisation.
Author Contributions
The study was conceived and designed by K.R., L.V.H. and M.S.W. Data were obtained and curated by T.B. and M.S.W. Statistical analyses were conducted by K.R., I.G. and M.S.W. The original draft of the manuscript was written by K.R. and I.G., and was critically revised for intellectual content by K.R., I.G., T.B., L.V.H, and M.S.W.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a Victoria University of Wellington, Faculty of Science Strategic Research Grant to M.S.W. The funder was not involved in the design of the study; the collection, analysis or interpretation of data; or writing the manuscript and did not impose any restrictions regarding the publication of the manuscript.
Ethical Approval and Informed Consent
This research received ethical approval (HEC#31199) from the Victoria University of Wellington, Human Ethics Committee under delegated authority of the New Zealand Health and Disability Ethics Committee. All participants actively indicated their informed consent prior to participation in the survey by reading study information and selecting an ‘I consent’ checkbox.