
Abstract
Introduction:
The trauma most commonly associated with the military is combat-related trauma. It is increasingly recognised that childhood sexual and physical abuse and military sexual assault may influence or exacerbate posttraumatic stress disorder (PTSD) when military members are exposed to combat.
Aims:
The study aimed to determine whether a history of childhood sexual and physical abuse would increase the likelihood of military sexual assault (MSA) and determine whether a history of sexual abuse (childhood or military) impacted the incidence and severity of post-trauma sequelae compared to veterans without this history.
Method:
A retrospective correlational analysis was performed on baseline data collected from clinical case records of a cohort of 134 Australian veterans with PTSD who had attended an outpatient Military Service Trauma Recovery Day Programme between October 2020 and May 2022.
Results:
Almost half (48.5%) of veterans reported a history of abuse. Prevalence rates of military sexual abuse, child sexual abuse and child physical abuse were 14.9%, 13.4% and 23.1% respectively. The relationship between those who experienced childhood abuse and those who experienced military sexual abuse was not significant. No significant differences were observed between those who experienced any sexual abuse and those who did not on intake scores of psychological symptoms.
Conclusion:
This is the first Australian study to investigate the prevalence of childhood abuse and military sexual abuse and its impact on PTSD and associated psychopathology in a sample of veterans seeking mental health treatment. No additional risks of experiencing military sexual assault were found for those who had survived childhood sexual abuse.
Introduction
Posttraumatic stress disorder (PTSD) is a psychiatric condition characterised by symptom clusters of re-experiencing, hyperarousal, avoidance, and alterations in cognition and mood following exposure to one or more traumatic events (American Psychiatric Association, 2013). Within the Australian Defence Force (ADF) population, the reported lifetime prevalence of PTSD is 12% (Australian Bureau of Statistics, 2022), while a recent report on mental health and wellbeing of transitioned ADF members also found that an estimated 25% met criteria for (PTSD) in their lifetime (Van Hooff et al., 2018). The trauma most commonly associated with the military is combat-related trauma. For the purposes of this paper, combat trauma is defined as exposure to one or more traumas occurring on military operations in war or war-like environments. Examples include being shot at, blown up, handling human remains and witnessing human atrocities, with the trauma meeting the Diagnostic and Statistical Manual of Mental Disorders-5 (DSM-5) definition of a ‘Criterion A’ trauma (American Psychiatric Association, 2013).
Childhood sexual abuse (CSA) and military sexual assault (MSA) can exacerbate the expression of PTSD when military personnel are placed in a combat situation (Calhoun et al., 2002; Cobb Scott et al., 2014; Gross et al., 2018; Zinzow et al., 2007). Childhood sexual abuse is associated with a range of adverse psychosocial, physical, and mental health outcomes (Hailes et al., 2019). In addition, experiencing sexual abuse at any age substantially increases the lifetime risk of any psychiatric diagnosis, and more than doubles the chance of a lifetime diagnosis of PTSD (Assink et al., 2019; Chen et al., 2010; Hailes et al., 2019). Furthermore, a prior history of sexual abuse can increase the risk of adult sexual assault (Phoenix Australia, 2020).
Military sexual assault is defined as any unwanted or forced non-consensual sexual activity or threats, including hazing, occurring in the military setting (Uniformed Services University, 2006). Examples include touching another person inappropriately, forcing a person to commit a sexual act, attempted rape and rape (James Cook University, 2024). Reports of ‘sexual misconduct’, including sexual harassment and assault offences, continue to rise in the ADF (Australian Government Department of Defence, 2021), however true prevalence is difficult to ascertain due to under-reporting stemming from a lack of reporting options, the perpetrator’s rank, shame and embarrassment and fears about retaliation (Wolff and Mills, 2016).
Childhood sexual abuse can be defined as any unwanted sexual contact when the victim is a child and the perpetrator is in a position of power (Mathews and Collin-Vézina, 2019). Within US military veterans seeking, treatment rates of CSA have been reported as 6.4% in a predominantly male sample (Wolfe-Clark et al., 2017), and 27% of females and 5% of males in a mixed gender sample (Zinzow et al., 2008). Within these samples, most of those who experienced CSA had further episodes of sexual assault as adults and sexual abuse survivors had a more extensive trauma history and greater psychological impairment than veterans with other types of traumas (Wolfe-Clark et al., 2017; Zinzow et al., 2008), which is consistent with findings from other researches examining the interactions between sexual abuse and mental health symptoms (e.g. Cobb Scott et al., 2014). We are not aware of any research showing rates of CSA in Australian military populations or investigations of its influence on mental health within this population, which is one of the factors that prompted the current study.
Discrepancies in the literature exist regarding the impact of sexual abuse on military-related PTSD, as seen in a recent systematic review by Kerr et al. (2023). The researchers identified one study that reported a synergistic effect with military sexual trauma (MST) interacting with military combat exposure (MCE) to increase PTSD symptomatology and severity. A further four studies found no interaction. While outcomes are conflicting, four of the five studies did report significant independent associations between MST and PTSD, and MCE and PTSD (Kerr et al., 2023).
Trauma-focused therapies, including prolonged exposure therapy, eye movement desensitisation and reprocessing therapy, and cognitive processing therapy, have been shown to be effective interventions for PTSD, including those stemming directly from CSA (Ehring et al., 2014; Hailes et al., 2019; O’Cleirigh et al., 2019) or MST (Christ et al., 2022; Tiet et al., 2015; Walter et al., 2014). However, symptoms may vary between those with a history of sexual abuse and those without, including differences in hyperarousal, avoidance and reactivity or anger, general distress or depression and guilt (Assink et al., 2019; Phoenix Australia, 2020; Wolfe-Clark et al., 2017). It may be an important factor to consider when tailoring interventions to individual clients.
The current study examined the impact of sexual trauma on a population of Australian veterans referred to a group-based Trauma Recovery Programme for treatment of military-related PTSD. The aims were to identify the prevalence of MSA in this population, determine whether veterans with a history of childhood abuse (sexual or physical) would be at greater risk in adulthood to have also experienced MSA (compared to veterans without a history of childhood abuse), and to determine whether a history of sexual abuse (childhood or military) impacted on severity of PTSD, complex PTSD (CPTSD), or other post-trauma sequelae such as anger, and general levels of distress. It was hypothesised that:
Veterans with a history of childhood abuse would be more likely to have also experienced MSA.
Veterans with a history of childhood abuse or MSA would exhibit greater incidence and severity of post-trauma sequelae compared to veterans without this history.
Methods
Design
A retrospective correlational cohort design was employed, utilising baseline data collected from clinical case records of a cohort of 136 Australian veterans who had attended a Military Service Trauma Recovery Day Programme (TRP) as outpatients at Toowong Private Hospital (TPH) between October 2020 and May 2023. All records were included, where there was consent, intake assessment data, a PTSD diagnosis, and complete demographic data.
Excluded data/case records
Two participant records were excluded from the analysis – one due to missing demographic information (trauma history) and one due to missing intake assessment scores. Three participants had missing data on one of the nine intake measures and were excluded from comparative analysis, with no other missing data observed. Final sample size was 134.
Participants
Participants were ex- or currently serving members of the Australian Defence Force (ADF) who had entitlements through the Department of Veterans’ Affairs (DVA) or Department of Defence to access treatment for PTSD. All veterans had been diagnosed with PTSD in the past by their referring doctors, then referred to the TRP for assessment of suitability to attend.
Procedure and data collection
All veterans participated in a 1.5 hour clinical assessment interview with a psychiatrist and an endorsed psychologist from the TRP. The purpose of this assessment was to confirm a diagnosis of PTSD and assess suitability to participate in a group trauma programme. Ethical approval for the study was obtained from the Departments of Defence and Veterans’ Affairs Human Research Ethics Committee (DDVA HREC) (477-22). On admission to the TRP, participants provided written consent for their data to be used for future research studies. Demographic data collected included age, gender, marital status, employment status, service (e.g. Navy, Army, Air Force), types and number of deployments. A dichotomous answer (Yes/No) was obtained as to whether the veteran had suffered childhood abuse (sexual and/or physical) or military sexual abuse (witnessed, experienced and/or perpetrated). The psychologist would explore this further if the answer was in the affirmative. A PTSD diagnosis was then confirmed by the Clinician-Administered PTSD Scale for DSM-5 (CAPS-5). At the start of the programme, all participants completed a battery of mental health self-report questionnaires which assessed symptoms of PTSD, depression, anxiety, anger, alcohol use, and quality of life. A description of each measure follows.
Measures
Clinician-Administered PTSD Scale for DSM-5 (CAPS-5)
The CAPS-5 is a 30-item structured interview that can be used to make a current (past month) diagnosis of PTSD. In addition to assessing the 20 DSM-5 (Diagnostic and Statistical Manual of Mental Disorders-5) PTSD symptoms, questions target the onset and duration of symptoms, subjective distress, impact of symptoms on social and occupational functioning, overall response validity, overall PTSD severity, and specifications for the dissociative subtype (Weathers et al., 2018).
PTSD Checklist for DSM-5 (PCL-5)
The PCL-5 is a 20-item self-report measure that assesses the 20 DSM-5 symptoms of PTSD. It is used to screen individuals for PTSD, to identify people with probable PTSD and to monitor symptom change during and after treatment. Although the CAPS-5 is the gold standard for diagnosing PTSD, the PCL-5 can provide a provisional diagnosis (with additional clinician assessment information). A total symptom severity score (range from 0 to 80) can be obtained, as well as DSM-5 symptom cluster severity scores (Bovin et al., 2016).
Dimensions of Anger Reaction (DAR)
The DAR is a 5-item self-report measure of anger reactions (Novaco, 1975). Each item is rated to indicate the frequency to which each statement describes the respondent’s feelings or behaviour. Scores range from 5 to 25, with higher scores indicating stronger anger symptoms. It is a reliable and sensitive measure of anger, with an internal consistency of 0.90 (Forbes et al., 2004).
The Kessler Psychological Distress Scale (K10)
The K10 is a simple self-report measure of psychological distress, comprising 10 questions about emotional states, each with a five-level response scale (Kessler et al., 2003). Total scores range from 10 to 50, with higher scores indicating greater distress. It has been shown to be a moderately reliable instrument to detect mental health conditions in the population (Kessler et al., 2002), and demonstrates high factorial validity and internal consistency. For the ADF, an optimal epidemiological cut-off point of ⩾ 25 indicates probable 30-day anxiety or affective disorder (Searle et al., 2015).
International Trauma Questionnaire (ITQ)
Following the procedure adopted by Howard et al. (2021), CPTSD was assessed using the Disturbance in Self-Organisation (DSO) subscale from the International Trauma Questionnaire (Cloitre et al., 2018). This subscale has 6 items: 2 items assessing affective dysregulation, 2 items assessing negative self-concept, and 2 items assessing disturbances in relationships and social isolation. Higher scores indicate an increase in symptoms associated with complex PTSD in people diagnosed with PTSD using ICD-11 criteria. Scores range from 0 to 24. Studies indicate it has good structural validity and adequate internal consistency (Murphy et al., 2020; Shevlin et al., 2018).
Statistical analysis
A number of analytic processes were employed to analyse the data. First, univariate tests of association: X 2 analyses for categorical variables were employed to explore: the association between participant demographics and abuse history; and the relationship between childhood abuse and military sexual assault in the sample. Next, continuous variables such as age and service length were explored using Wilcoxon-Mann–Whitney U tests. Similarly, the Mann–Whitney U tests (adjusted for multiple comparisons using the Bonferroni method) were used to measure the severity of PTSD measures between groups, due to non-normal distribution. RStudio (RStudio Team, 2022) version 12.0 software was used to perform all analyses. A p value of < 0.05 was considered statistically significant.
Results
The participants in this study were predominantly male (93%, 124M, 10 F, N = 134), married/defacto (67%) and in the Army (75%) with a mean age of 44.3 ± 10.9 years. Of the 134 participants, 85% indicated they had experienced combat trauma (n = 114) and 48.5% indicated they had a history of abuse (childhood or military). Of the 65 individuals that reported experiencing abuse, 50.8% experienced at least one form of sexual trauma (childhood or military, n = 33), 47.8% reported a history of childhood physical abuse (n = 31) and 35.4% reported ‘other’ trauma (perpetrating or witnessing MSA, n = 23). See Table 1 for a summary of reported abuse types. Some participants (n = 20) were included in one or more abuse groups, but only participants belonging to one category were included in between groups’ analysis. Frequency of combat trauma was not significantly different across groups (p = 1).
Prevalence of abuse types.
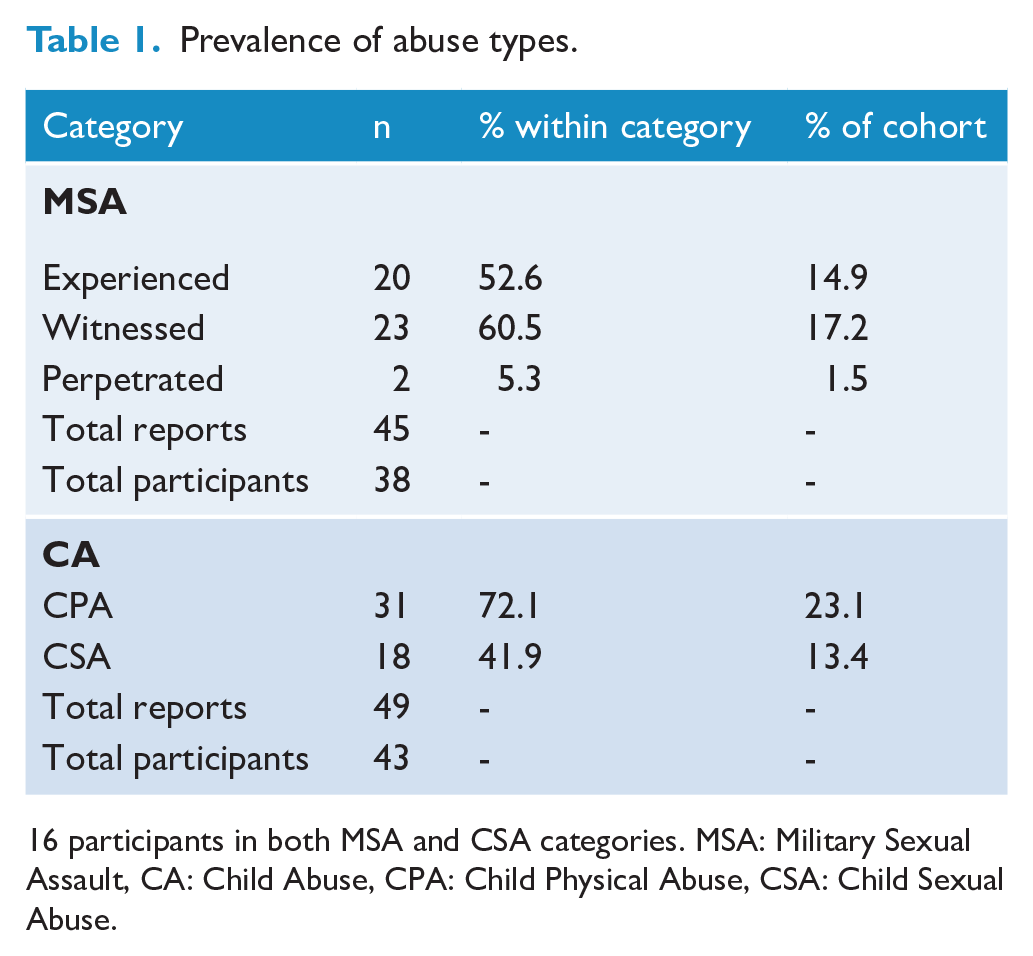
16 participants in both MSA and CSA categories. MSA: Military Sexual Assault, CA: Child Abuse, CPA: Child Physical Abuse, CSA: Child Sexual Abuse.
No significant differences in demographic variables were observed between participants with a history of abuse and those who did not experience any forms of abuse, with all comparisons returning a p value > 0.05 (Table 2).
Demographic variables by abuse category.
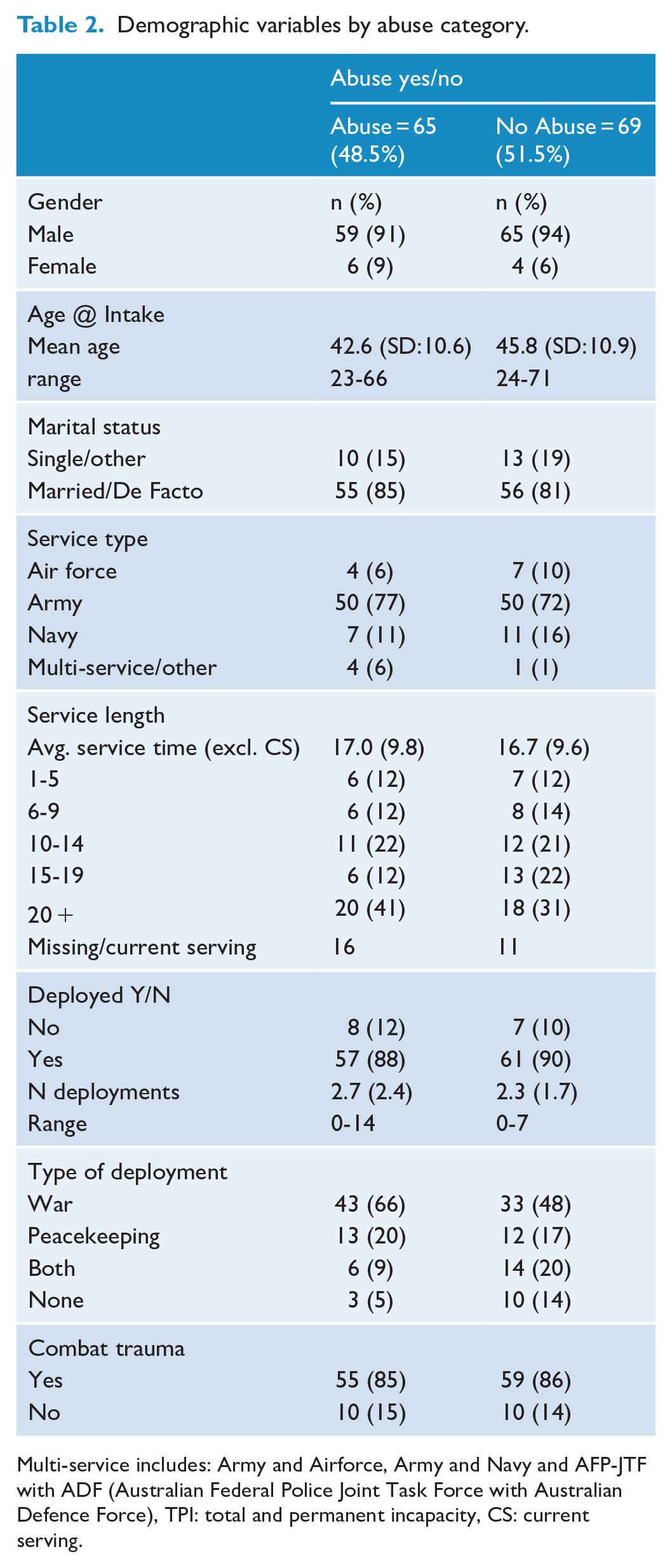
Multi-service includes: Army and Airforce, Army and Navy and AFP-JTF with ADF (Australian Federal Police Joint Task Force with Australian Defence Force), TPI: total and permanent incapacity, CS: current serving.
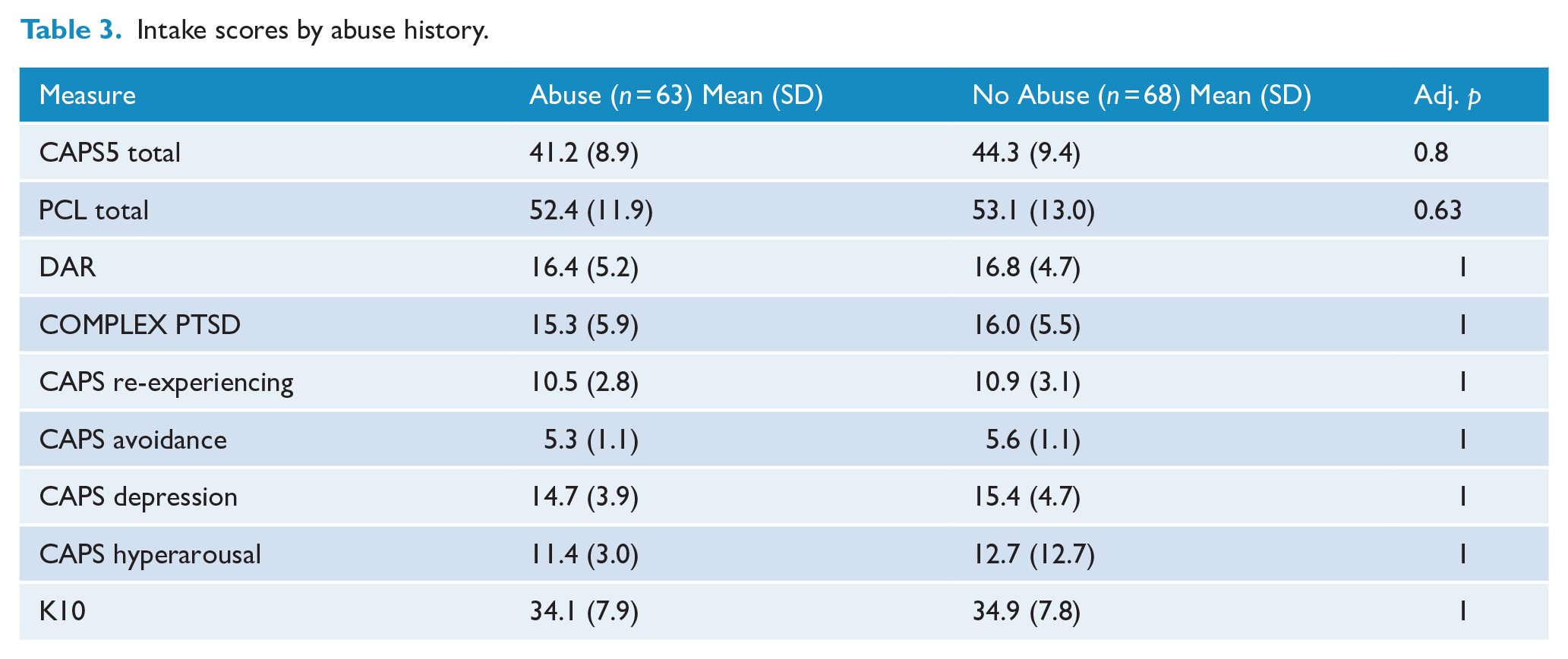
The relationship between those who experienced childhood abuse and those who experienced military sexual assault (MSAExp) was also not significant on a X 2 test of association, X 2 (1, N = 93) = 007, p = 0.932. However, a significant association was observed between childhood sexual abuse and military sexual abuse when including all levels of MSA (Experienced, Witnessed and Perpetrated), X 2 (1, N = 33) = 6.1, p = 0.014. After adjusting for multiple comparisons, no significant differences were observed between those who experienced abuse (Childhood Abuse or MSA) and those who reported no history of abuse on the intake scores of interest; CAPS5 total, PCL, DAR, Complex PTSD, K10 and the four domains of CAPS (Re-experiencing, Avoidance, Depression and Hyperarousal), with all comparisons indicating a p value greater than 0.05 (Table 3).
Intake scores by abuse history.
In addition, no significant differences between intake scores were observed between abuse groups (MSA, CSA, CPA and Other) with all comparisons also indicating a value greater than p < 0.05 (Table 4).
Intake score by abuse type.
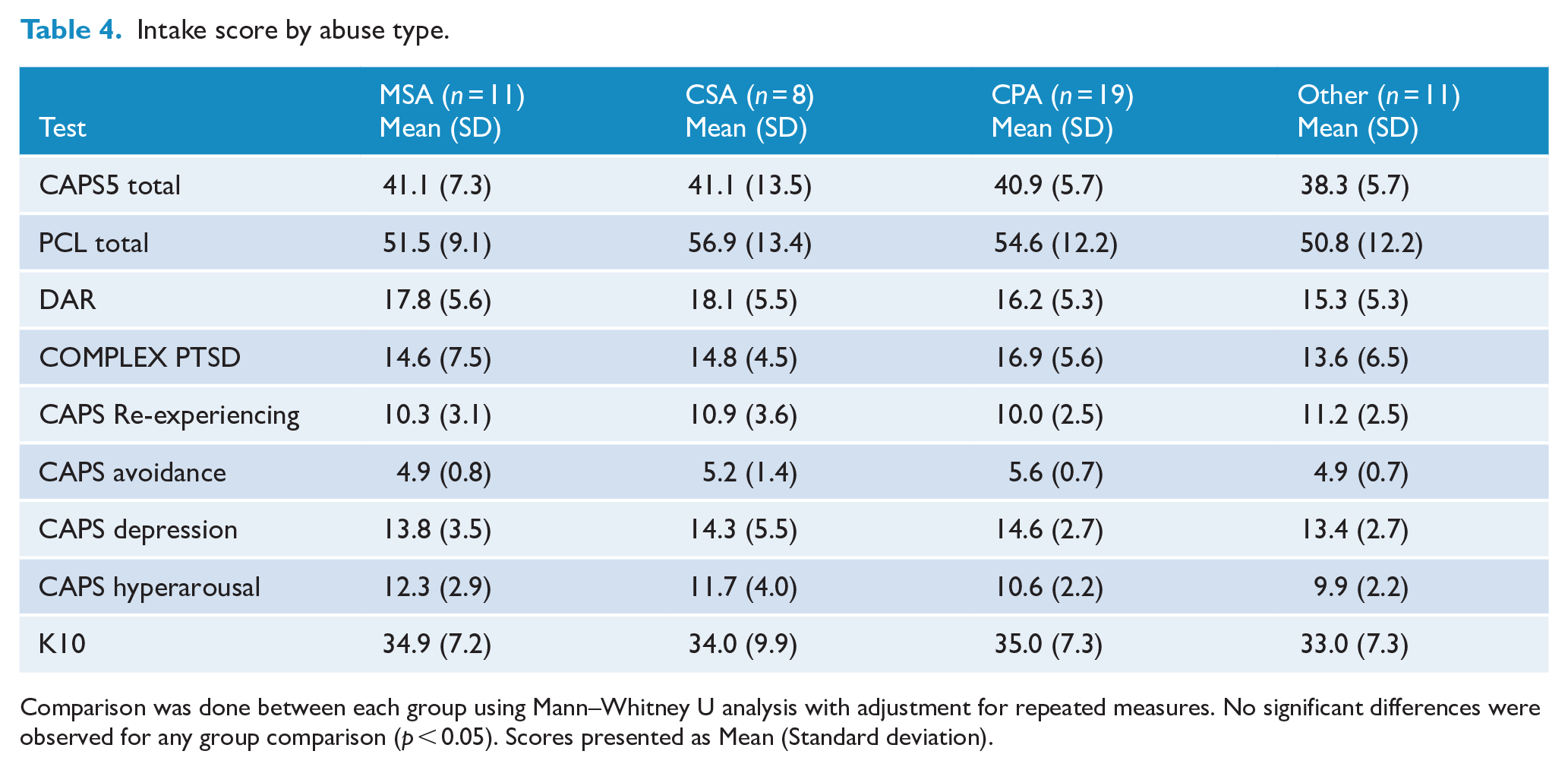
Comparison was done between each group using Mann–Whitney U analysis with adjustment for repeated measures. No significant differences were observed for any group comparison (p < 0.05). Scores presented as Mean (Standard deviation).
Discussion
The current paper is the first study to investigate the association between childhood abuse, military sexual abuse, and mental health symptoms within the Australian military population. In our sample of 134 veterans seeking psychiatric treatment, we found 48.5% reported a history of any form of sexual or physical abuse, which is a similar rate to reports from US military samples seeking treatment (Cobb Scott et al., 2014). Childhood sexual abuse was reported by 13.4% of the sample, childhood physical abuse was reported by 23.1% of the sample, and exposure to sexual abuse, assault, or hazing while working in the Australian Defence Force (either by experiencing the abuse, witnessing, or perpetrating the abuse) was reported by 28.4% of the sample. These findings generally align with the results of a recent national commission which reported 39% of women and 26% of men experienced sexual harassment (admittedly a much broader term than the more narrow concept of exposure to sexual abuse, assault, or hazing) at work in the past 5 years (Australian Human Rights Commission, 2020), as well as reported rates of childhood sexual abuse reported in Australia (e.g. 37.3% of females and 18.8% of males, Mathews et al., 2023).
In regard to the research questions of whether veterans who had a history of CSA were more likely than veterans without a history of CSA to experience MSA, our study found no significant differences. While there is potentially more opportunity for sexual assault to occur in military contexts due to living in close quarters, isolated from potential supports, and the military social and hierarchical structures (Stander and Thomsen, 2016), the current study found there was no additional conferred risk for those with a history of CSA. This result may indicate greater personal qualities such resilience and strength in CSA survivors, thus being less vulnerable to sexual violence within the military (Whitelock et al., 2013). There is potential that the assertiveness and self-defence skills learnt in military training is advantageous and protective in bolstering skills to defend oneself from unwanted sexual advances. It is also possible that people with a history of CSA may be more likely to be drawn to the military to find structure and security, a sense of family who protects them versus those that didn’t in their own childhood, and to learn controlled aggression to prevent sexual abuse happening to them again.
No significant differences were found in symptom expression nor symptom severity between veterans who had experienced any form of sexual abuse and those who had not. The current study found that symptom expression and severity did not depend on trauma typology. A recent systematic review found that there was a higher prevalence of complex PTSD as compared to PTSD in ex and currently serving military personnel (Grinsill et al., 2024), and survivors of sexual abuse are often thought to be at higher risk of complex PTSD, a form of PTSD in which there are three additional areas of disturbance in self-organisation including: (1) severe difficulties with affect regulation, (2) persistent negative self-image or concept and (3) persistent difficulties in interpersonal relationships (Cloitre et al., 2013). The current paper suggests that in this sample, survivors were at no higher risk for complex PTSD, nor more severe PTSD, anger or general psychological distress, than those without survivorship.
A finding of interest was that a significant association was found between CSA and MSA only when all levels of MSA were included in the analysis (experienced, witnessed and perpetrated). This finding may be partly explained by the greater statistical power of including the additional 25 participants who witnessed and perpetrated MSA abuse but did not experience MSA. The increased recognition of any form of exposure to MSA and in veterans with a history of CSA might be explained by information processing changes following trauma, with CSA survivors having greater attentional awareness of and memory recall for violations of interpersonal safety (Buckley et al., 2000; Pergamin-Hight et al., 2015), and therefore are able to more easily recognise and recall MSA occurring than those who did not have CSA.
In regards to perpetration of MSA, previous research has established a connection between being a survivor of CSA and becoming a perpetrator. For example, a well-designed Australian study utilised matched cohort controls to determine whether children who had a confirmed and documented history of sexual abuse were more likely to perpetrate sexual offences against others as adults, and they found a significant association (Ogloff et al., 2012). The strongest relationship was for males who were sexually abused after the age of 12 years (Ogloff et al., 2012). Our data collection methods (clinical interview with new patients seeking treatment) were not specifically designed to encourage or normalise reporting of perpetrating MSA, which may have led to under-reporting of perpetrating in our study (i.e. two participants admitted to perpetrating MSA) and limited any analysis of perpetrating.
Limitations
Although the total sample size of n = 134 provided adequate statistical power, when between-groups analyses were performed small sample sizes in some groups limited analysis.
Reporting bias is inherent in research of this nature, and research and clinical experience suggests that veterans may be reluctant to report occurrences of MSA for a range of reasons, including power differences related to military rank, stigmatisation (including potential for being excluded and missing out on promotions), lack of reporting pathways, experiences of seeing other survivors being further victimised, and knowledge of cases where the perpetrator has not been held to account and further promoted (Mengeling et al., 2014). Similarly, in a National Inquiry into sexual harassment in Australian workplaces, only 17% of those who were sexually harassed reported it (Australian Human Rights Commission, 2020).
The veteran cohort included in this research was asked about their history of sexual abuse during their first contact with a psychologist that was also assessing PTSD symptoms and suitability for group CBT treatment, and rapport and trust is likely to have been variable between veterans. Indeed, from the authors’ clinical experience subsequently working with these participants, some veterans who had said ‘no’ to a history of sexual abuse at assessment later disclosed that they had experienced sexual abuse. If veterans were asked about their sexual abuse history after sufficient therapeutic rapport had been established there would no doubt be a higher disclosure rate. In addition, the type of person who has experienced CSA and is able to discuss it when meeting a new psychologist may be different to the type of person who had a similar experience but will only disclose this history over time.
Gender bias influenced the overall prevalence of MSA in our sample. Our participants were predominantly male, and previous research has found higher rates of MSA when higher rates of females are included in the population, or the population is exclusively female (Kerr et al., 2023). This gender bias reflects gender differences in the predominantly male Australian military (e.g. 79.4% as of the 2021 census) (Australian Bureau of Statistics, 2021). Further research in samples with more female veterans would be beneficial.
Conclusion
The current study is the first to investigate childhood sexual assault, military sexual assault, and psychological symptoms in an Australian veteran population seeking mental health treatment. Almost half (48.5%) of the sample reported some history of abuse, and prevalence rates of military sexual abuse, child sexual abuse and child physical abuse were 14.9%, 13.4% and 23.1%, respectively. There were no significant correlations between having a history of childhood abuse (physical or sexual) and subsequent assault in the military, and no significant differences between groups when examining psychological symptoms. Improved awareness of childhood sexual abuse and military sexual assault when working with veterans will better inform future research as well as assist treatment of symptoms.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.