
Abstract
Objective:
This paper describes the development of the third edition of the National Health and Medical Research Australian Guidelines for the Prevention and Treatment of Acute Stress Disorder, posttraumatic stress disorder and Complex posttraumatic stress disorder, highlighting key changes in scope, methodology, format and treatment recommendations from the previous 2013 edition of the Guidelines.
Method:
Systematic review of the international research was undertaken, with GRADE methodology used to assess the certainty of the evidence, and evidence to decision frameworks used to generate recommendations. The Guidelines are presented in an online format using MAGICApp.
Results:
Key changes since the publication of the 2013 Guidelines include a new conditional recommendation for Child and Family Traumatic Stress Intervention for children and adolescents with symptoms within the first 3 months of trauma, and a strong recommendation for trauma-focused cognitive behaviour therapy for the child alone or with a caregiver, for those with diagnosed posttraumatic stress disorder. For adults with posttraumatic stress disorder, strong recommendations are made for specific types of trauma-focused cognitive behaviour therapy and conditional recommendations are made for five additional psychological interventions. Where medication is indicated for adults with posttraumatic stress disorder, venlafaxine is now conditionally recommended alongside sertraline, paroxetine or fluoxetine.
Conclusion:
These Guidelines, based on systematic review of the international literature, are intended to guide decision making for practitioners, service planners, funders and those seeking treatment for trauma related mental health concerns. For an Australian Guideline, a critical limitation is the absence of research on the treatment of Australian Aboriginal and Torres Strait Islander peoples. The new online format of the Australian posttraumatic stress disorder Guidelines means that they can be updated as sufficient new evidence becomes available.
Keywords
Introduction
The National Health and Medical Research Council (NHMRC) approved Australian Guidelines for the Prevention and Treatment of Acute Stress Disorder, Posttraumatic Stress Disorder (PTSD) and Complex PTSD (the Australian PTSD Guidelines) have recently been released. This is the third edition of the Australian PTSD Guidelines, with previous releases in 2007 and 2013, and the first to include consideration of the new ICD-11 diagnosis of Complex PTSD. With respect to format, the most important change in the 2020 Australian PTSD Guideline is that it has been developed as a ‘living guideline’. The recommendations, and the research evidence underpinning the recommendations, are presented in the online platform for guidelines, MAGICApp. This online format enables individual recommendations to be updated when there is sufficient new evidence to do so, particularly in areas where there is limited research and new studies significantly influence the strength of the body of evidence. This ensures that guideline recommendations remain current and valid, and a source of timely and trustworthy advice to clinicians, patients and other service decision-makers. The online format also improves the efficiency of guideline development, as effort is not wasted in undertaking formal systematic reviews on topics for which there is insufficient additional evidence to change guideline recommendations.
Internationally, there are several recently released PTSD Treatment Guidelines – two from professional associations, the American Psychiatric Association (APA, 2017) and the International Society for Traumatic Stress Studies (ISTSS, 2018), and two from national organisations, the UK National Institute for Health and Care Excellence (NICE, 2018) and the US Departments of Veterans Affairs and Defence (VA/DoD, 2017). In this context, the need for a separate Australian PTSD Treatment Guidleline may be queried. Although all Guidelines are based on the same published literature, different recommendations can arise due to methodological decisions and the interpretation of the evidence (Hamblen et al., 2019). Further, the formulation of recommendations needs to take into consideration factors relevant to specific healthcare contexts such as available resources and patient preferences and values (Guyatt et al., 2008).
This paper will describe the development of the third edition of the Australian PTSD Guidelines, highlighting key changes in methodology and treatment recommendations.
Background
A degree of psychological distress is common in the early aftermath of exposure to one or more traumatic events and can be considered a part of the normal stress response. However, when an individual’s distress is severe, persists and/or interferes with important areas of psychosocial functioning, assessment for a posttraumatic mental health disorder is indicated. Acute stress disorder (ASD) and PTSD are the focus of the Australian PTSD Guidelines, and are both included in the Trauma-and Stressor-Related Disorders category in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5; APA, 2013). In addition to ASD or PTSD – both of which require exposure toa traumatic event as part of the diagnostic criteria (Criterion A) – mood, substance use and anxiety disorders are also commonly diagnosed following exposure to a traumatic event (Bryant et al., 2010) and should be considered in assessment and diagnosis. The diagnosis of ASD requires at least nine symptoms from a broad list of dissociative, re-experiencing, avoidance and arousal symptoms, and can be diagnosed between 2 days and 1 month following exposure to the traumatic event(s). While having an ASD diagnosis is moderately predictive of PTSD, the majority of individuals who eventually develop PTSD have not previously met full criteria for ASD (Bryant, 2011). As defined by DSM-5, the diagnosis of PTSD requires one of five symptoms of re-experiencing, one of two symptoms of avoidance, two of seven symptoms of negative alterations in cognition and mood, and two of six symptoms of hyperarousal. There are two specifiers for PTSD: a dissociative subtype if the individual reports experiences of depersonalization or derealisation, and delayed expression in cases when full diagnostic criteria are not met until at least 6 months after the trauma (APA, 2013).
A subset of individuals with PTSD, more commonly those who have experienced events of an interpersonal, prolonged and repeated nature (e.g. childhood sexual abuse, imprisonment, torture), present with a constellation of characteristic features that can include: impaired emotional control; self-destructive and impulsive behaviour; impaired relationships with others; hostility; social withdrawal; feeling constantly threatened; dissociation; somatic complaints; feelings of ineffectiveness, shame, despair or hopelessness; feeling permanently damaged; and a loss of prior beliefs and assumptions about safety and the trustworthiness of others (van der Kolk et al., 2005). In DSM-IV, this constellation of symptoms fell within the category of Disorders of Extreme Stress Not Otherwise Specified (DESNOS; van der Kolk et al., 2005), while in DSM-5, many of the symptoms are now included in the broader symptom profile of PTSD, as reflected in the negative alterations in cognition and mood symptoms cluster and the dissociative subtype. In the International Classification of Diseases (ICD-11; World Health Organization (WHO), 2018), a new diagnosis of Complex PTSD [CPTSD] was recognised, that requires symptoms of three types of disturbances of self-organisation (DSO) – emotional dysregulation, interpersonal difficulties and negative self-concept – in addition to the core symptoms of PTSD. Given this formal recognition of CPTSD as a mental disorder in ICD-11, it was included in the scope of the systematic review for these Australian PTSD Guidelines (Brewin et al., 2017).
Within Australia, 75% of the population have experienced one or more potentially traumatic events in their lifetime (Mills et al., 2011), and the 12-month prevalence of PTSD is 4.4% (McEvoy et al., 2011). This means that over 1 million Australians experience PTSD in any 12-month period, making PTSD Australia’s second most prevalent mental health condition (McEvoy et al., 2011). Unfortunately, the uptake of evidence-based treatment for PTSD is low (Spence et al., 2011). This, combined with a proliferation of alternative non-evidence based interventions (Metcalf et al., 2016), highlights the importance of the Australian PTSD Guidelines in providing a much-needed evidence-based treatment framework for practitioners, consumers, service planners and funders.
Importantly, in line with the Institute of Medicine (now called the National Academy of Medicine) standards for clinical practice guidelines (Institute of Medicine, 2011), the Australian PTSD Guidelines are not intended to mandate treatment for people with PTSD but rather guide treatment decisions. The Guideline recommendations should be interpreted and implemented in the context of good clinical judgement and in discussion with people using the health care services.
Aim
The aim of this project was to update the Australian PTSD Guidelines using current best practice approaches and, incorporating consideration of the new diagnosis of CPTSD.
Method
Establishing the guideline development group
Since the Institute of Medicine’s standards for guideline development were published in 2011 (Institute of Medicine, 2011), there has been more awareness of the need for patient and public involvement in guideline development, with the NHMRC’s current Guidelines for Guidelines (NHMRC, 2019) recommending the involvement of end-users and consumers. Accordingly, membership of the Guideline Development Group for the updated Australian PTSD Guidelines was expanded beyond academic subject matter experts to include a broader range of people with lived experience of trauma, and end users (general practice, psychology and social work practitioners) with experience working with particular trauma populations including Aboriginal and Torres Strait Islander peoples, refugees and asylum seekers and survivors of sexual assault and disasters. Each member was invited to participate in the guideline development meetings including a 2-day workshop, and provide input from their unique perspectives at every stage of the development of the guideline. The input of members with lived experience was particularly sought for the ‘preferences and values’ component of the basis for the recommendations where they contributed based on their own experience of treatment-seeking. The members of the Guideline Development Group are listed in Table 1.
Membership of the guideline development group.
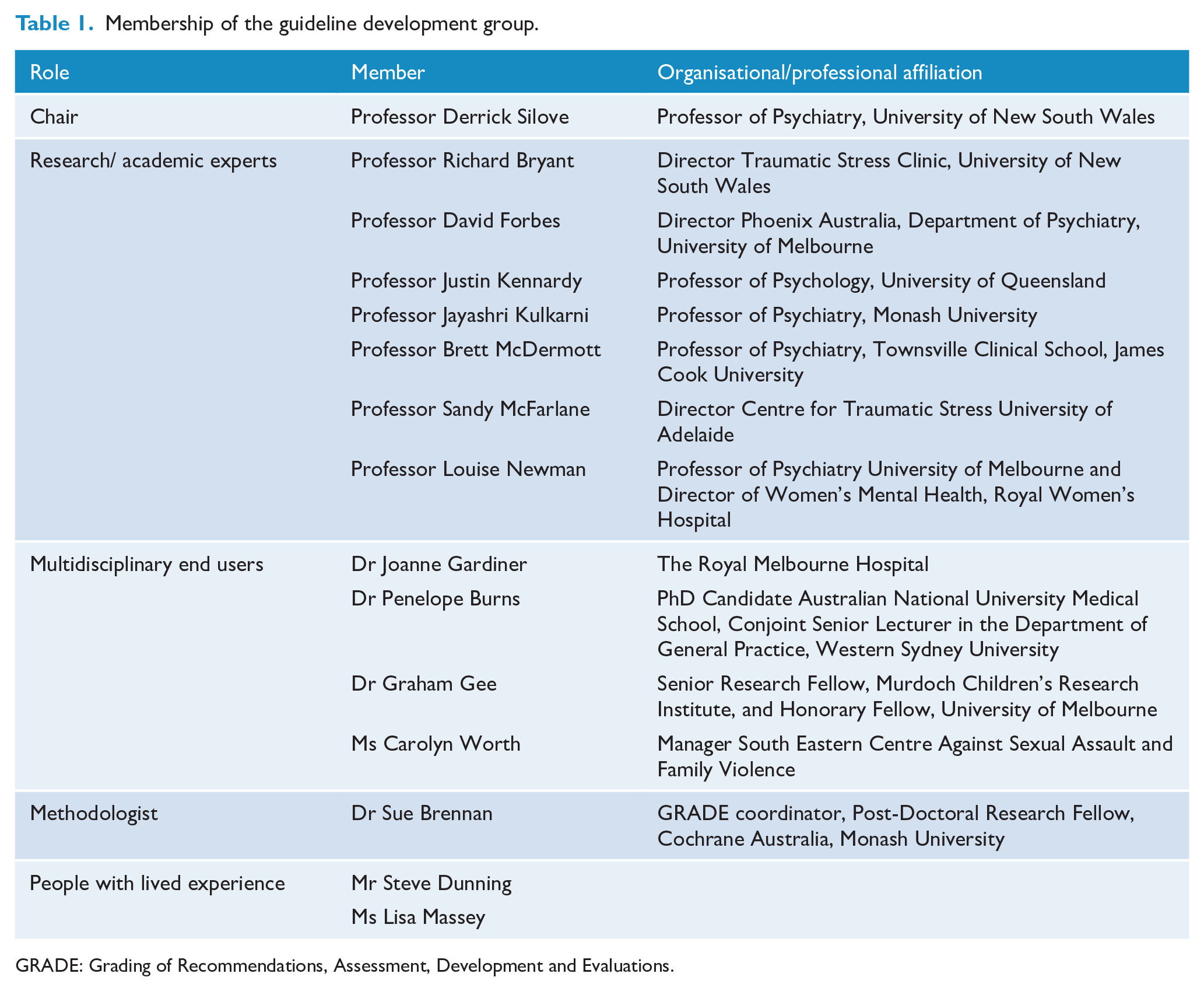
GRADE: Grading of Recommendations, Assessment, Development and Evaluations.
Determining the clinical questions and approach to the systematic review
At the time of commencement of the Guidelines development process, the ISTSS had just completed a systematic review of the literature to inform the development of the ISTSS PTSD Treatment Guidelines. Phoenix Australia was granted permission to use the ISTSS systematic review as the foundation for the Australian PTSD Guidelines. The ISTSS clinical questions and outcomes (PTSD symptom severity and diagnosis) were adopted for the Australian PTSD Guidelines. The Guideline Development Group identified two additional questions to review for the Australian PTSD Guidelines: the first on pre-incident preparedness interventions, and the second on treatment for CPTSD.
Evidence was reviewed separately for adults, and for children and adolescents for each of the following: pre-incident preparedness; intervention within the first 3 months of a traumatic event; treatment for those with clinically relevant post-traumatic stress symptoms. Psychosocial, pharmacological and non-psychosocial and non-pharmacological interventions were considered.
The clinical questions and study eligibility criteria (specifying population, interventions, comparators and outcomes: PICOs) are presented in Tables 2 and 3 respectively.
Clinical questions.
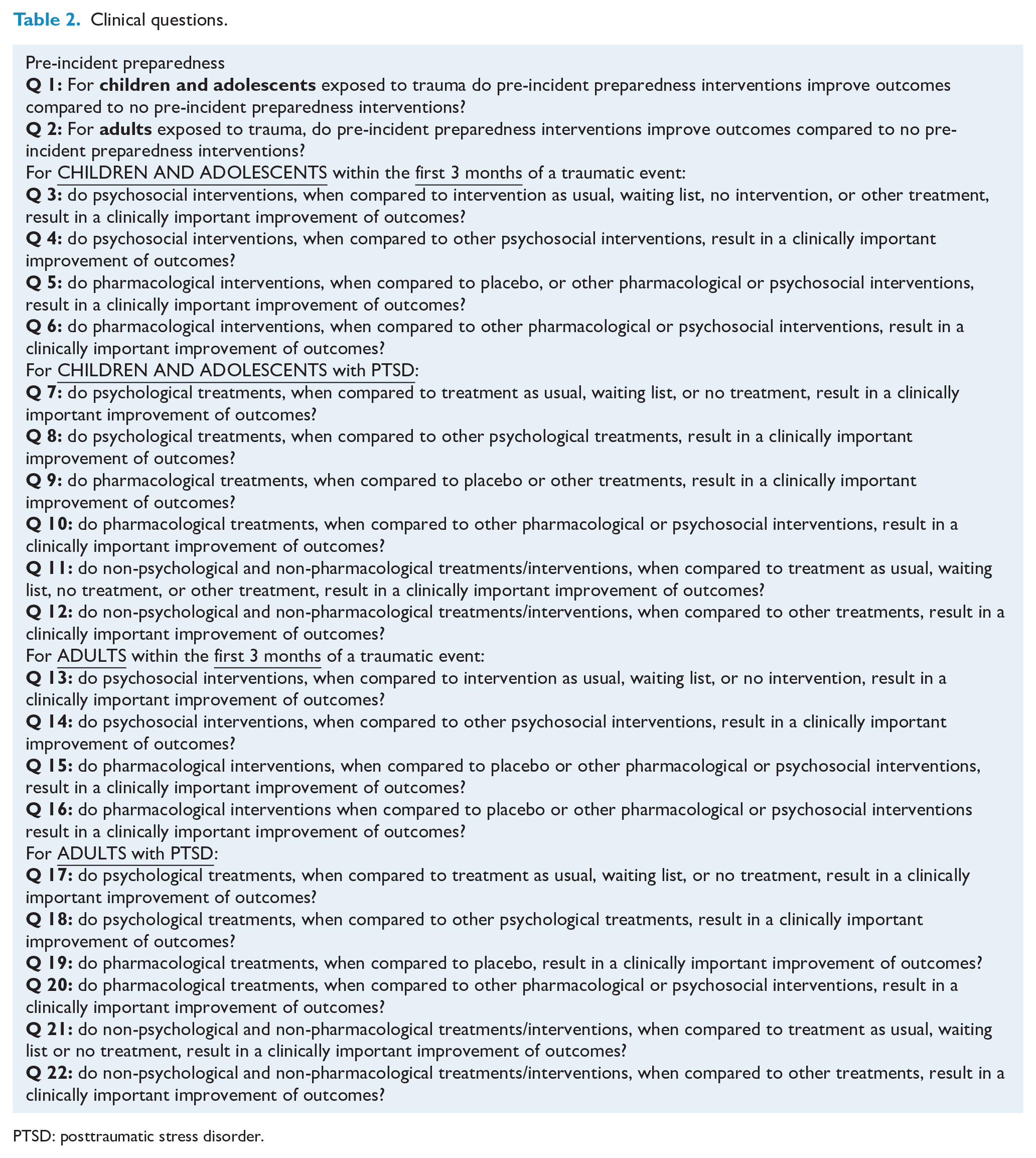
PTSD: posttraumatic stress disorder.
PICO eligibility criteria.
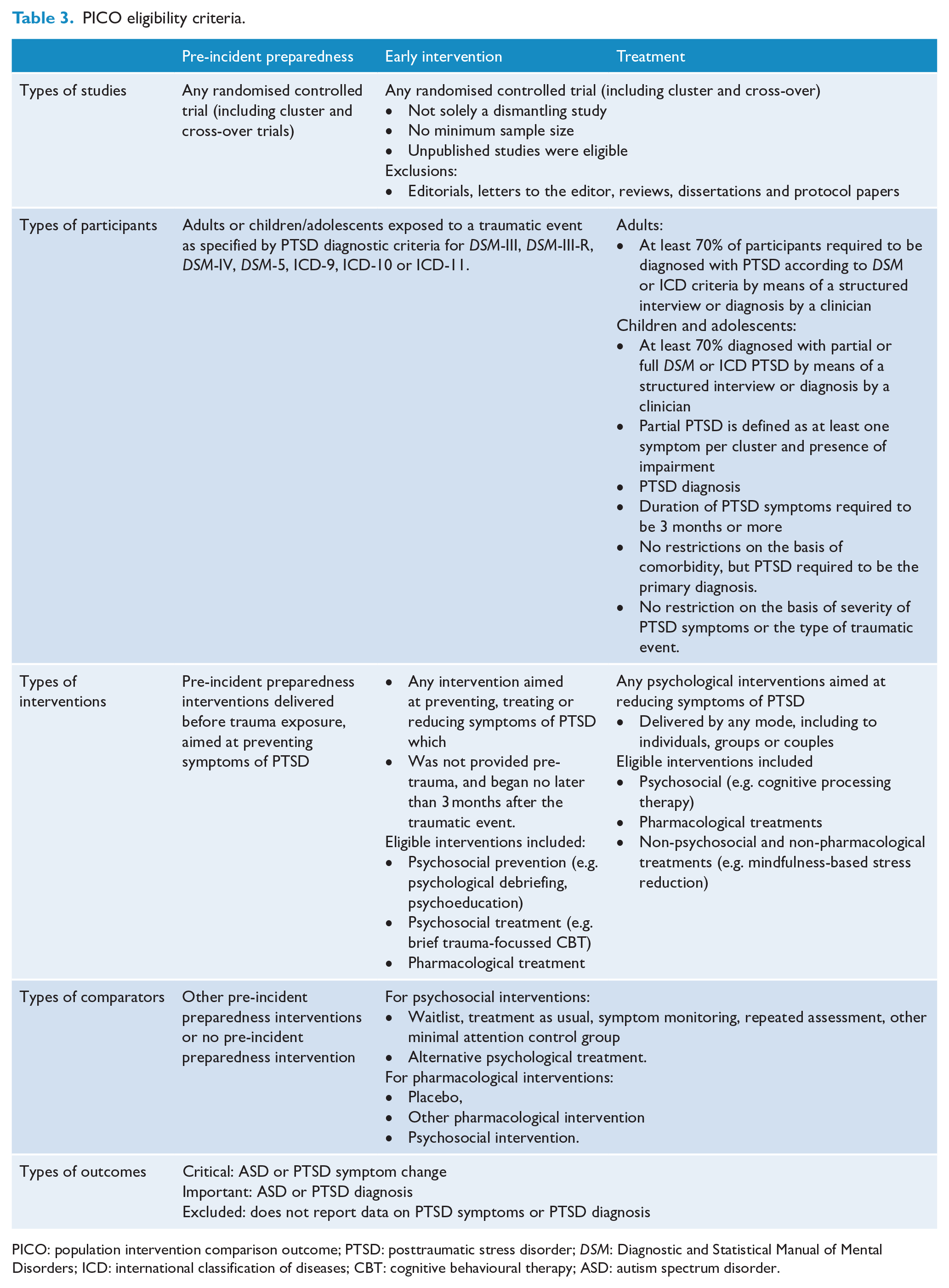
PICO: population intervention comparison outcome; PTSD: posttraumatic stress disorder; DSM: Diagnostic and Statistical Manual of Mental Disorders; ICD: international classification of diseases; CBT: cognitive behavioural therapy; ASD: autism spectrum disorder.
Search methods
The ISTSS systematic review drew upon recent high quality systematic reviews undertaken by the Cochrane Collaboration, the UK NICE and the World Health Organization (WHO). Randomised controlled trials (RCTs) from these reviews were used as the initial set of studies and re-evaluated by the ISTSS review team. Searches were conducted by the ISTSS team to update the identified systematic reviews, in addition to asking experts in the field to identify missing studies. Full details of the methodology for the ISTSS systematic review have been published separately (Bisson et al., 2019).
Literature published up to October 2018 was included in the ISTSS systematic reviews. For the Australian PTSD Guidelines, an update of the systematic review was undertaken with literature published between November 2018 and June 2019. A small number of additional studies were identified and appraised (Nidich et al., 2018; Sloan et al., 2018), and the findings integrated into the meta-analyses and GRADE (Grading of Recommendations, Assessment, Development and Evaluations; Guyatt et al., 2008) assessment of the body of evidence. In addition, a new search was conducted for the pre-incident preparedness question for literature published between 2008 and June 2019. Both searches were conducted in the CENTRAL (Cochrane), Medline, EMBASE, PSYCInfo and PILOTS (now PTSDpubs) databases.
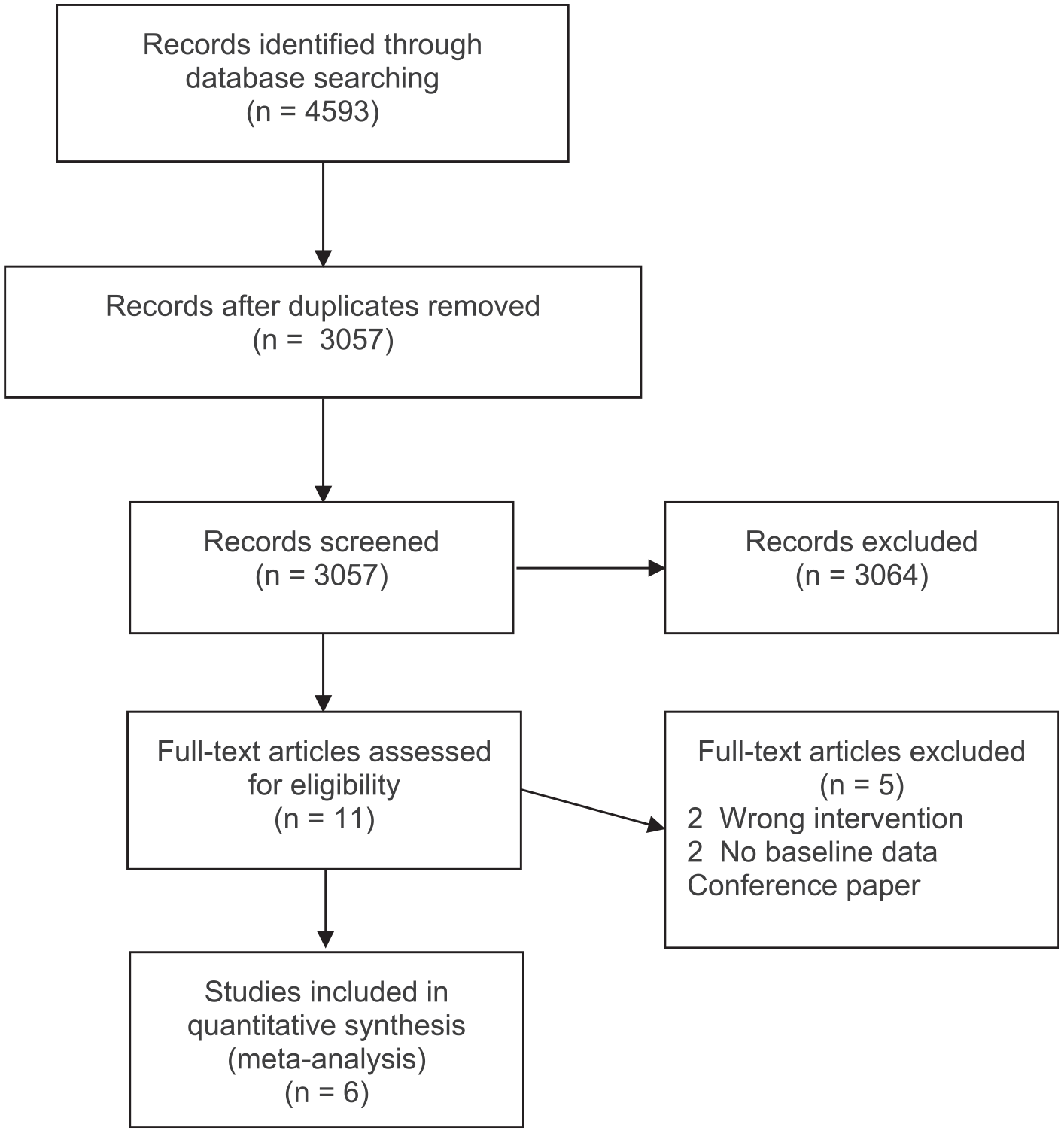
The ISTSS systematic reviews, and the updates to these reviews, used the same search strategy. To ensure that all relevant RCTs were captured the broad search terms used for the update of the ISTSS systematic review were ‘PTSD’, ‘posttrauma*’, ‘post-trauma*’, ‘post trauma*’, ‘combat disorder*’, ‘stress disorder*’. The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) flowchart for the update of the ISTSS systematic review is presented in Figure 1.
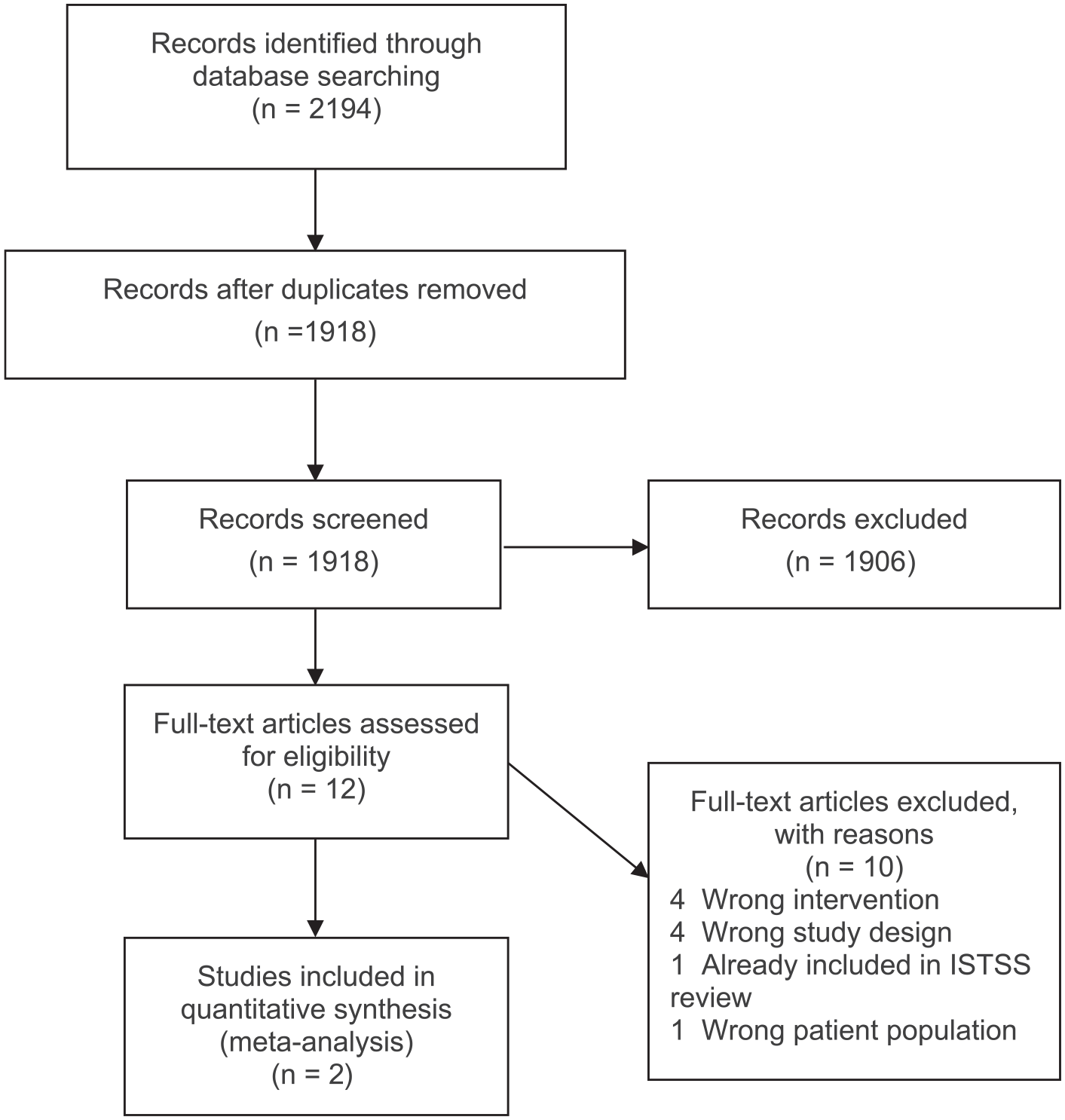
PRISMA for the ISTSS systematic review update.
The pre-incident preparedness systematic review used the search terms: PTSD or ‘post-traumatic stress disorder’ or ‘posttraumatic stress disorder’ or ‘post traumatic stress disorder’ AND preparedness or pre-incident or inoculation or prevent* or resilien* or protect* or pre-trauma or pretrauma or plan* AND intervention or training or programme or trial. The PRISMA flowchart for the pre-incident preparedness systematic review is presented in Figure 2.
PRISMA for the Pre-incident Preparedness systematic review.
Assessing the evidence
While the ISTSS systematic review was used to identify the relevant papers for consideration in addressing the research questions, an independent assessment of the certainty of the evidence was undertaken for the Australian PTSD Guidelines using the Grading of Recommendations, Assessment, Development and Evaluations (GRADE; Guyatt et al., 2008) approach. GRADE is considered best practice (Draft Guidelines for Guidelines Handbook www.nhmrc.gov.au/guidelinesforguidelines, due for completion 2021), providing a structured method for assessing risk of bias, directness (fit with specified PICO), precision (based on sample size and confidence intervals), consistency and publication bias. The use of GRADE in the development of the revised Guidelines, represents a shift from the methodology used in the 2013 Australian PTSD Guidelines based on previous guidance from NHMRC (2000) in which recommendations were graded from A through D based on volume, consistency, clinical impact, generalisability and applicability.
For this third edition of the Guidelines, the quality of individual studies was assessed using the Cochrane Collaboration’s risk of bias tool (Higgins et al., 2011) and GRADE was then used to assess the certainty of evidence for each systematic review comparison (e.g. EMDR vs waitlist).. The overall body of evidence for each intervention (e.g. Trauma-Focused Cognitive Behavioural Therapy [TF-CBT] for adults with PTSD) including all of the comparisons was then assessed using GRADE, to rate the evidence as high quality (i.e. further research is very unlikely to change confidence in the estimate of effect), moderate quality (i.e. further research is likely to have an important impact on confidence in the estimate effect and may change the estimate), low quality (i.e. further research is very likely to have an important impact on confidence in the estimate of effect and is likely to change the estimate) or very low quality (i.e. we are very uncertain about the estimate) to give an overall GRADE certainty of evidence rating for each intervention reviewed.
Formulating recommendations
The formulation of recommendations arising from the assessment of the evidence was also undertaken by the Guideline Development Group, independently of the ISTSS Guideline development process. Compared to the 2013 Australian PTSD Guidelines, a more systematic approach to formulating recommendations was adopted, with the use of the GRADE evidence to decision (EtD) framework (Neumann et al., 2016). The GRADE evidence-to-decision framework provides a systematic and transparent approach to making well-informed healthcare choices. Twelve judgement criteria were considered for each recommendation. In making a recommendation the Guideline Development Group balanced the following factors: benefits and harms, certainty in evidence, values, acceptability, feasibility, equity and costs. These considerations are captured in the ‘key info’ tab accompanying each recommendation. This ensured that the Guideline Development Group’s application of GRADE was transparent and a consistent approach was applied in the development of all recommendations. While the Guideline Development Group followed the GRADE methodology, the decision-making is ultimately a matter a judgement for the group. Under the GRADE system, recommendations are limited to four types – strong or conditional, for or against an intervention. A fifth category, recommendations for further research, was also used when the Guideline Development Group considered that the preliminary evidence for the intervention was promising and warranted further research. A summary of the process used to develop Guideline recommendations is presented in Figure 3.
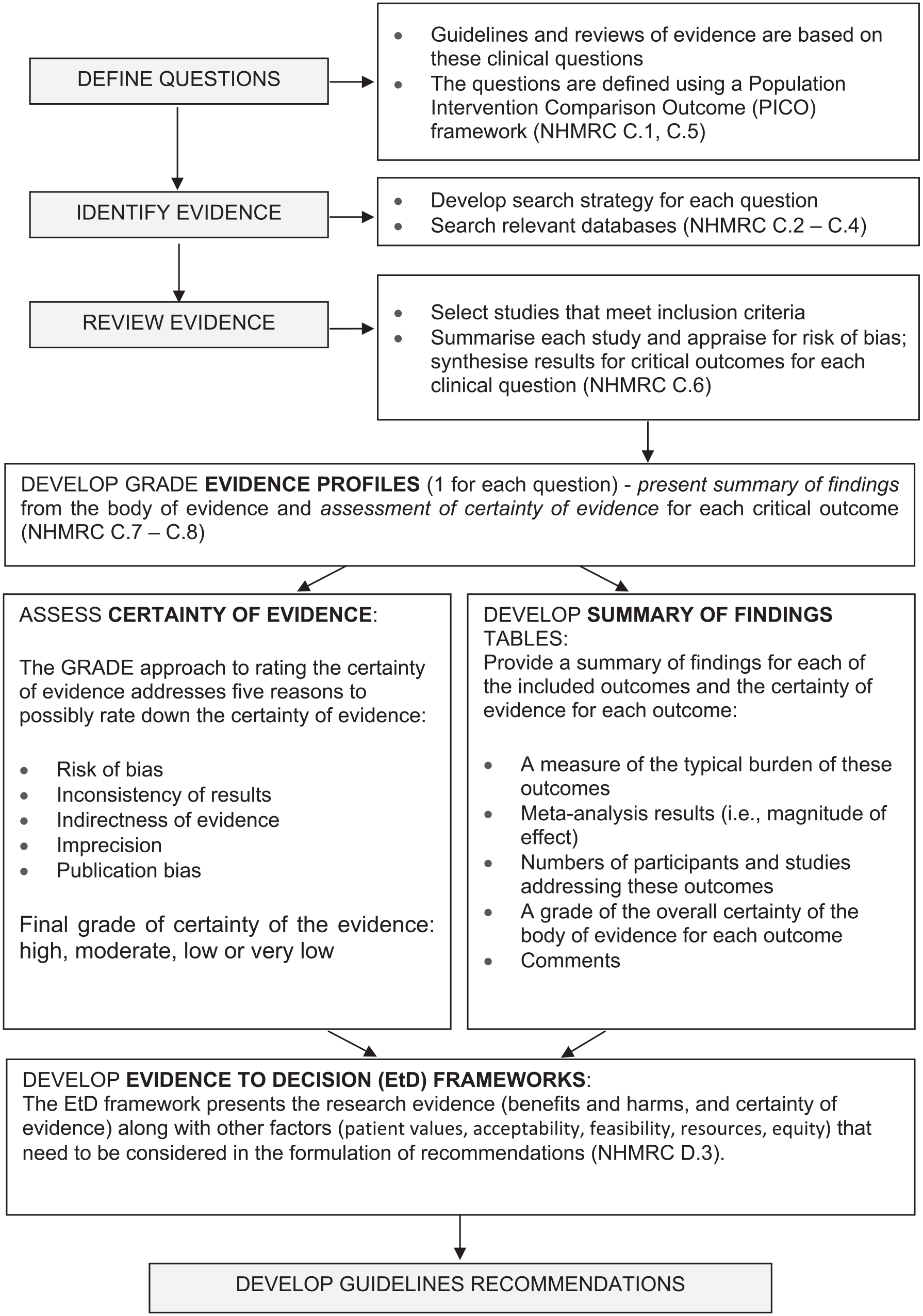
Evidence review methodology.
Results
Evidence reviews and recommendations
The following section begins with the results of research on the two additional questions included in the Australian PTSD Guidelines: Complex PTSD and pre-incident preparedness interventions. It then sets out the key treatment recommendations and summarises the research evidence underpinning the remaining questions, highlighting recommendations that are new in the current edition of the Guidelines. Unfortunately, there is no direct comparison between the old and new systems of grading recommendations but to assist the reader in making comparisons, Table 4 provides a description of recommendations in each system.
Definition of NHMRC and GRADE grades of recommendation.
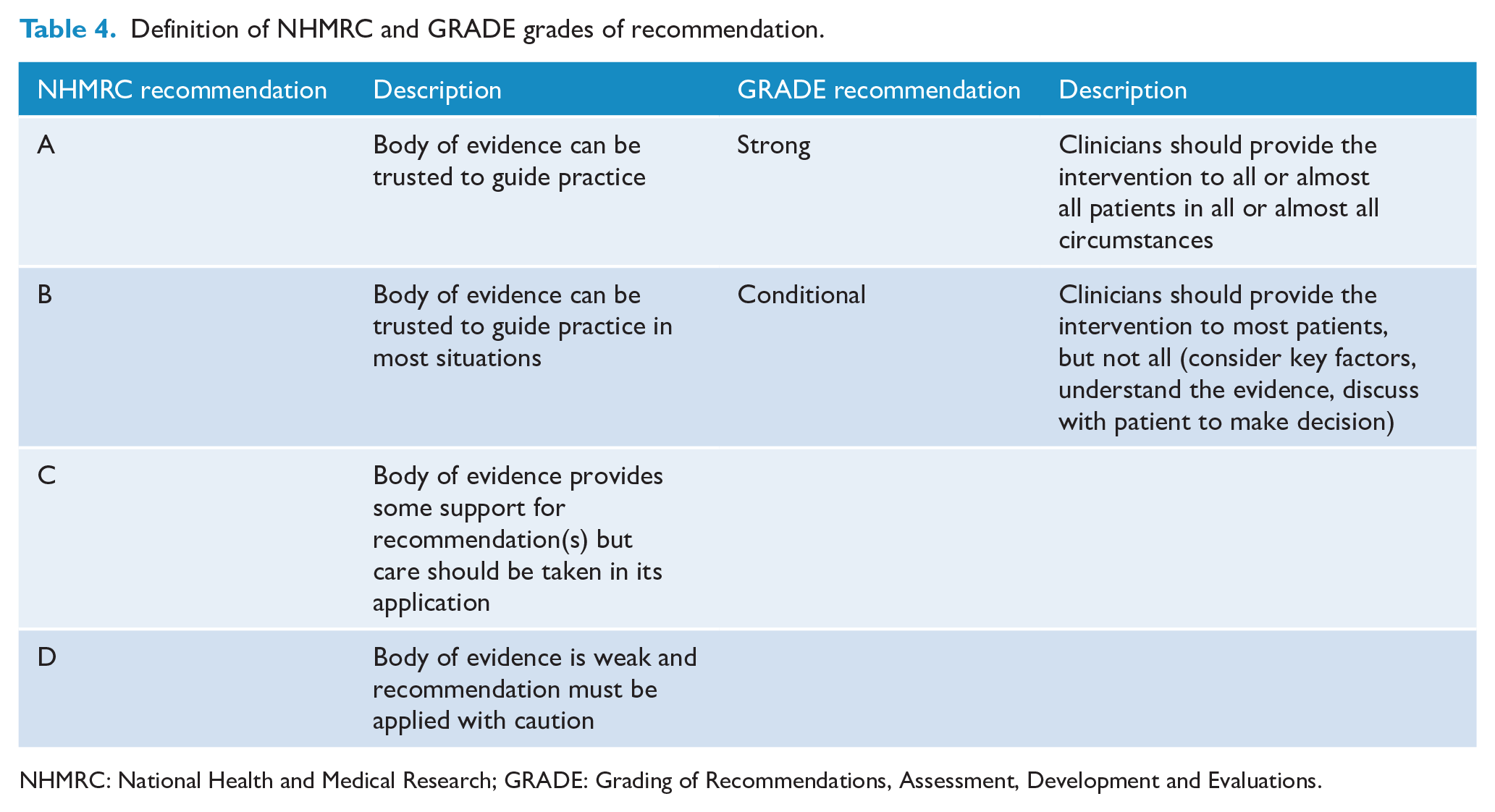
NHMRC: National Health and Medical Research; GRADE: Grading of Recommendations, Assessment, Development and Evaluations.
In the interests of space, the full list of studies that informed the recommendations is not included. Full details of the systematic reviews including citations for included studies can be found at www.phoenixaustralia.org/australian-guidelines-for-ptsd/ and by clicking through to the MAGICApp online platform at https://app.magicapp.org/#/guideline/Edr04L . Unless otherwise stated, there were no harms reported in the studies.
Complex PTSD
Based on an initial scoping of the literature, the Guideline Development Group determined that there was insufficient research available to warrant a systematic review of the evidence for treatments for CPTSD. Instead, a narrative review was undertaken, addressing conceptual, diagnostic, assessment and management issues and outlining treatment outcome research in progress. This review is available at www.phoenixaustralia.org/wp-content/uploads/2020/07/Chapter-7.-CPTSD.pdf. Capitalising on the advantage of the ‘living guideline’, once the ‘in progress’ clinical trials on CPTSD are completed, the data and subsequent recommendations on CPTSD will be included in an updated Guideline. Complex PTSD has been retained in the title of this third edition as a placeholder for when more evidence becomes available.
Pre-incident preparedness
There was sufficient research in the area of pre-incident preparedness to undertake a systematic review, but insufficient evidence for any particular pre-incident preparedness intervention to form recommendations. However, research recommendations were made for three emerging interventions for adults. Two of these involve computerised tasks designed to train individuals to selectively attend to stimuli–attention bias modification training and attention control training. The third involves the use of biofeedback to increase the individual’s control of their heart rate.
Remaining questions
The section begins with recommendations for children and adolescents, then moves on to recommendations for adults. Unless otherwise stated, all interventions are intended for individual rather than group delivery. For both populations, recommendations are divided into interventions within the first 3 months after exposure to a potentially traumatic event (universal and indicated interventions) and interventions for those with PTSD (psychological, pharmacological and non-psychological/non-pharmacological). A summary of the key changes in recommendations between the 2013 Australian PTSD Guidelines and the current Australian PTSD Guidelines is presented in Table 5.
Key changes in guideline recommendations since 2013.
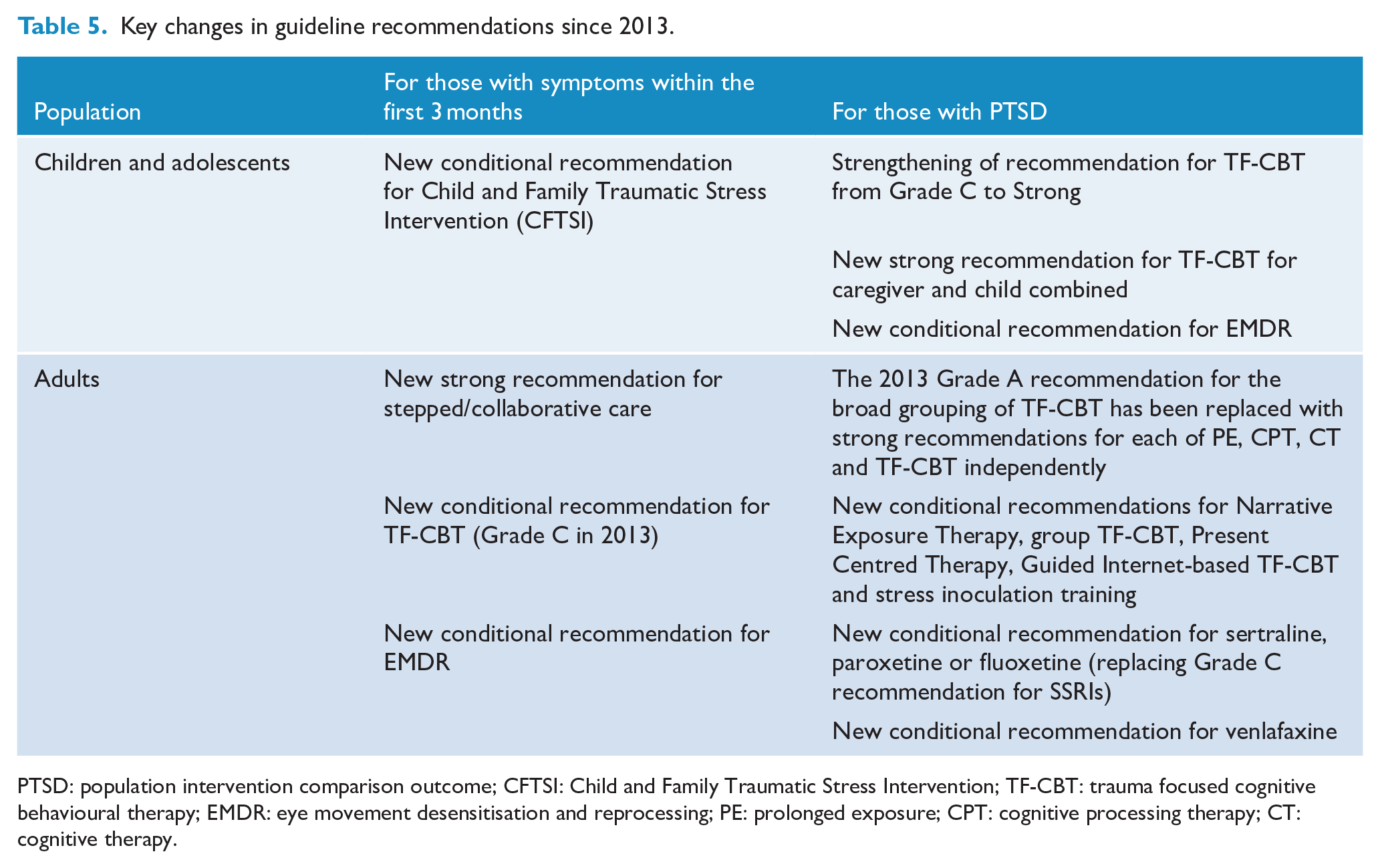
PTSD: population intervention comparison outcome; CFTSI: Child and Family Traumatic Stress Intervention; TF-CBT: trauma focused cognitive behavioural therapy; EMDR: eye movement desensitisation and reprocessing; PE: prolonged exposure; CPT: cognitive processing therapy; CT: cognitive therapy.
Recommendations for children and adolescents
Interventions within the first 3 months of trauma
Universal interventions (for all children and adolescents exposed to trauma)
Similar to the 2013 Australian PTSD Guidelines, the current Guidelines make a conditional recommendation against individual psychological debriefing for all children and adolescents exposed to trauma. Instead it is suggested that children and adolescents be provided with information, emotional support and practical assistance, consistent with psychological first aid. This is based on evidence from two randomised controlled trials (RCTs). The overall certainty of the evidence is moderate due to serious imprecision (a low number of participants).
Indicated interventions (where symptoms of PTSD are present within the first 3 months)
For children with symptoms of PTSD within the first 3 months, a new conditional recommendation is made for Child and Family Traumatic Stress Intervention (CFTSI), in preference to supportive counselling. CFTSI is a four-session caregiver plus child model that focusses on two PTSD risk factors of poor social or familial support and poor coping skills. It aims to ameliorate these risks by (1) increasing communication between the affected child and their caregivers about feelings, symptoms and behaviours with the goal of increasing the caregivers’ support of the child, and (2) teaching specific behavioural skills to both the caregiver and child to assist in coping with symptoms. The evidence is based on a single RCT. Certainty of the evidence is low due to serious risk of bias and serious imprecision. Despite the low certainty of evidence, the Guideline Development Group members drew on their clinical expertise and judged the intervention as unlikely to pose a risk and likely to provide some clinical benefit for children and adolescents with symptoms of PTSD.
Interventions for children and adolescents with clinically relevant symptoms of PTSD
Psychological interventions
Additional research since 2013 has led to the current Australian PTSD Guidelines making a strong recommendation for TF-CBT for children and adolescents with symptoms of PTSD, upgraded from the Level C recommendation in 2013. The evidence was based on 27 RCTs and certainty of the evidence is moderate.
The Guidelines also make a new strong recommendation for TF-CBT for caregiver and child. This intervention includes caregivers on the basis that, when possible, parents or caregivers should be included throughout treatment to support the child or adolescent’s practice and mastery of skills and to enhance positive parenting and parental support. Evidence was based on 13 RCTs and overall certainty of the evidence is moderate.
A new conditional recommendation is made for eye movement desensitisation and reprocessing (EMDR) where TF-CBT is unavailable or unacceptable. EMDR was previously not recommended for children and adolescents. Although evidence from four RCTs suggests a moderate, clinically unimportant benefit of EMDR for PTSD symptom severity post-treatment relative to waitlist or usual care, this was considered alongside evidence from two RCTs suggesting EMDR to be more beneficial than TF-CBT for children for reducing PTSD symptom severity and evidence from one RCT suggesting no clinically important difference between EMDR and TF-CBT for caregiver and child on PTSD symptom severity. Overall certainty of the evidence is low.
Pharmacological interventions
As was the case in 2013, there was insufficient evidence to recommend pharmacological interventions for children and adolescents with PTSD. The supporting chapters provide some guidance for practitioners in this context, suggesting they follow depression guidelines, which currently favour fluoxetine as the antidepressant of first choice for people aged 12–18 years (Malhi et al., 2015).
A summary of recommended treatments for children and adolescents is presented in Figure 4.
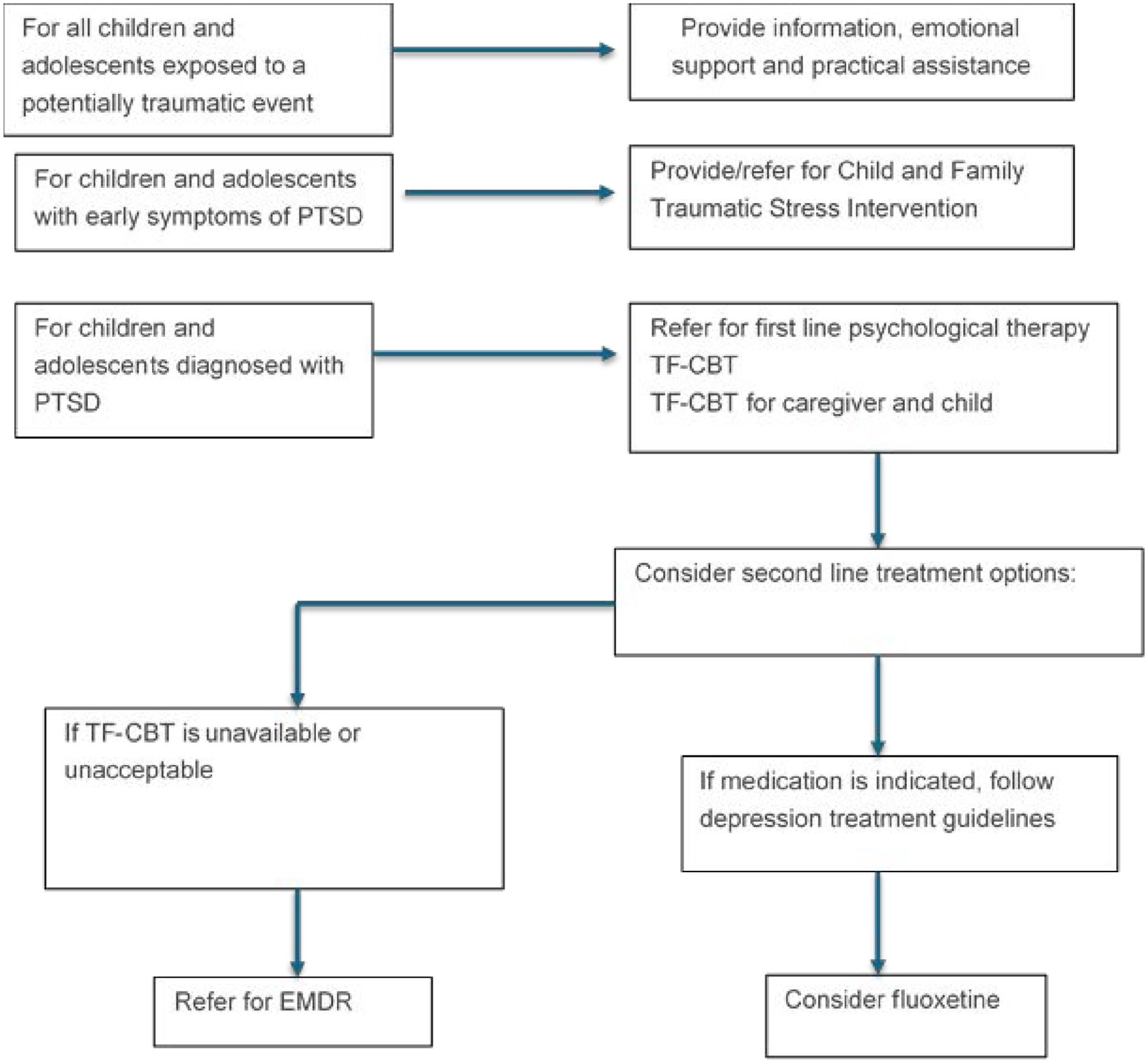
Summary of guideline recommendations for children and adolescents exposed to trauma.
Recommendations for adults
Interventions within the first 3 months of exposure to a traumatic event
Universal interventions (for all adults exposed to a traumatic event)
In line with the previous version of the Guidelines, and with the recommendation for children and adolescents, the current Australian PTSD Guidelines make conditional recommendations against both group and individual psychological debriefing within the first 3 months of exposure to a traumatic event. Instead, it is suggested that adults exposed to traumatic events be provided with information, emotional support, and practical assistance, consistent with psychological first aid. For group psychological debriefing, evidence from three RCTs suggests that the intervention has no effect on PTSD symptom severity, with the certainty of the evidence moderate due to serious risk of bias. For individual debriefing, evidence from three RCTs suggests that individual debriefing may slightly increase PTSD diagnosis while evidence from 5 RCTs suggests that individual debriefing has no effect on PTSD symptom severity. The overall certainty of the evidence is low.
Indicated interventions for those with PTSD symptoms
Psychological interventions
A new strong recommendation is made for a stepped/collaborative care model, in which individuals receive evidence-based care commensurate with the severity and complexity of their need. This approach involves ongoing monitoring of symptoms, in order to guide treatment decisions. Interventions can be stepped up from low intensity and easily delivered interventions such as psychoeducation and problem solving, to more complex interventions such as activity scheduling, as indicated. Interventions are generally CBT-based, but sometimes based on other psychological approaches (e.g. motivational interviewing) and may include components of case management and pharmacological intervention. Although evidence from four RCTs suggested a small clinically unimportant benefit on symptom severity and a clinically important benefit of a stepped/collaborative care model on PTSD diagnosis, with moderate overall certainty of the evidence, the Guideline Development Group made this recommendation in recognition that stepped care is considered best practice and is highly valued by patients.
The Guidelines make a conditional recommendation for TF-CBT (including prolonged exposure, cognitive processing therapy, and cognitive therapy) within the first 3 months following trauma, in preference to no intervention. Evidence from 16 RCTs suggests a clinically important benefit of TF-CBT on PTSD symptom severity and diagnosis, relative to wait list / treatment as usual, supportive counselling, and relaxation. Overall certainty of evidence for TF-CBT is low.
A new conditional recommendation is also made for brief EMDR in preference to no intervention within the first 3 months after trauma. Evidence from five small RCTs suggests large clinically important benefit of 1–3 sessions of brief EMDR on PTSD symptom severity relative to waitlist in adults who have experienced a community critical incident e.g. workplace violence, earthquake, factory explosion, missile attack, intense rocket attacks. Evidence from one RCT suggests a large, clinically important benefit of brief EMDR on PTSD symptom severity and diagnosis relative to critical incident stress debriefing (CISD) in adults who had experienced workplace violence. Overall certainty of evidence for brief EMDR is moderate.
Pharmacological interventions
Considerable research has been undertaken into the utility of early pharmacological intervention for the prevention of PTSD in adults. The systematic review identified RCTs of hydrocortisone, docosahexaenoic acid, escitalopram, oxytocin, propranolol and gabapentin. To date there is insufficient evidence to recommend the use of any of these pharmacological agents, however there is emerging evidence for hydrocortisone, a synthetic form of cortisol, and a recommendation is made for further research into the use of hydrocortisone in the prevention of PTSD.
Interventions for adults with PTSD
Psychological interventions
In the 2013 Australian PTSD Guidelines, Grade A recommendations were made for TF-CBT and EMDR. Reflecting the advances in research, for the current update of the Guidelines there was sufficient evidence to make separate strong recommendations for individual approaches of TF-CBT, specifically, prolonged exposure (PE), cognitive processing therapy (CPT), TF cognitive therapy (CT) as well as the original TF-CBT intervention, comprising a hybrid of PE and cognitive restructuring. EMDR remained a strong recommendation. A brief description of each of these interventions is provided in Table 6.
Sub-types of trauma focused cognitive behavioural therapy (TF-CBT).
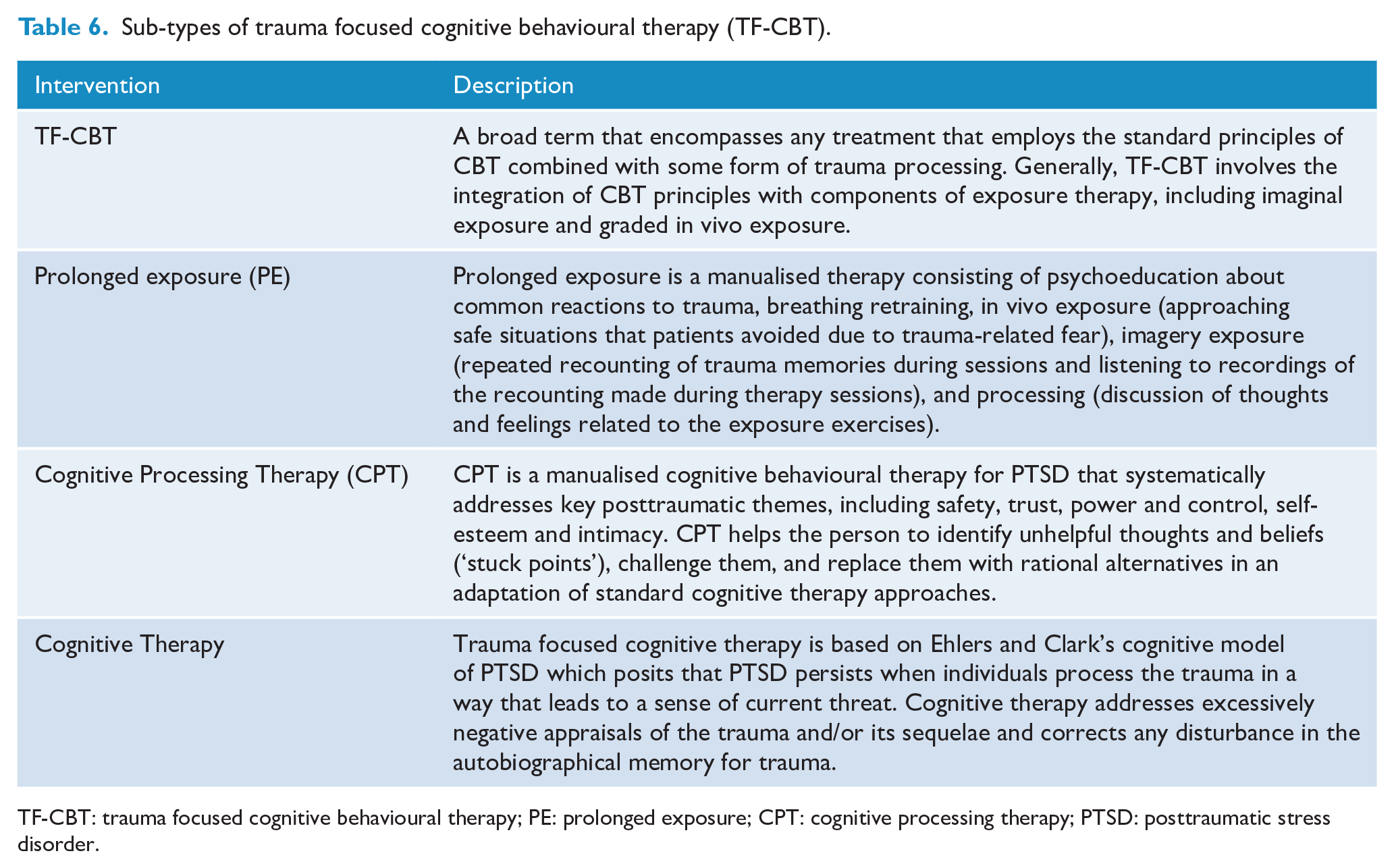
TF-CBT: trauma focused cognitive behavioural therapy; PE: prolonged exposure; CPT: cognitive processing therapy; PTSD: posttraumatic stress disorder.
A strong recommendation is made for prolonged exposure (PE). Evidence from 12 RCTs suggests a large clinically important benefit from PE on PTSD symptom severity. The overall certainty of evidence for PE is moderate.
The evidence supporting a strong recommendation for cognitive processing therapy (CPT) is based on four RCTs that showed a large clinically important benefit of CPT for PTSD symptom severity relative to waitlist or usual treatment (including CBT, psychoeducation, supportive counselling, non-trauma focused symptom management). These studies involved the original CPT protocol including a written trauma narrative.Evidence from a single RCT suggests no clinically important difference in benefit between CPT and prolonged exposure while evidence from another RCT suggests CPT is more beneficial than Dialogical Exposure Therapy for PTSD symptom severity. The overall certainty of evidence for CPT is moderate.
A strong recommendation is also made for trauma-focused cognitive therapy (CT) with evidence from four RCTs suggesting a large clinically important benefit of CT for PTSD symptom severity relative to waitlist. The overall certainty of the evidence is low.
The Guidelines make a strong recommendation for EMDR with evidence from 11 RCTs suggesting a large clinically important benefit of EMDR on PTSD symptom severity relative to wait list or usual treatment and small to moderate, clinically important benefits from 15 RCTs relative to TF-CBT, supportive counselling and relaxation training. The overall certainty of evidence for EMDR is moderate.
The Guidelines make a strong recommendation for TF-CBT, which broadly encompasses the common elements of effective treatments including exposure to trauma related memories, tackling avoidance and addressing trauma related cognitions (Olff et al., 2020). Evidence from seven RCTs suggests clinically important benefit of TF-CBT on PTSD symptom severity relative to waitlist or usual care (including supportive counselling and relaxation training) with overall moderate certainty of evidence.
In addition to these strong recommendations, the Australian PTSD Guidelines make a series of new conditional recommendations for interventions that could be considered when one of the trauma-focused cognitive behavioural therapies or EMDR are unavailable or unacceptable to the individual.
A conditional recommendation is made for guided Internet-based TF-CBT, an online programme in which the intervention is guided by a therapist. This is based on evidence from three RCTs suggesting large clinically important benefit relative to waitlist or attention control and a single RCT suggesting a small clinically important benefit of guided Internet-based TF-CBT relative to Internet-based supportive counselling. Overall certainty of evidence for guided Internet-based TF-CBT is low.
A conditional recommendation is made for present-centred therapy (PCT). PCT includes psychoeducation about the impact of PTSD symptoms, the development of effective strategies to deal with day-to-day challenges and homework to practice newly developed skills. Evidence from three RCTs suggests moderate clinically important benefit of PCT on PTSD symptom severity relative to waitlist and no difference between PCT and non-trauma-focused CBT. Evidence from five RCTs suggests TF-CBT is more beneficial than PCT on PTSD symptom severity, and evidence from a single RCT in veterans found moderate clinically important benefit of virtual reality therapy relative to PCT. The overall certainty of evidence for PCT is moderate.
A conditional recommendation is made for stress inoculation training (SIT). The SIT used in the studies that were assessed is an anxiety management programme for use with rape victims. Evidence from two RCTs suggests large clinically important benefit of SIT on PTSD symptom severity relative to waitlist or supportive counselling, while overall certainty of evidence is low.
The Guidelines make a conditional recommendation for group TF-CBT where individual TF-CBT or EMDR are unavailable or unacceptable. Evidence from six RCTs suggests a large clinically important benefit from group TF-CBT on PTSD symptom severity relative to waitlist or usual care or applied muscle relaxation. Evidence from three RCTs found no clinically important difference between group TF-CBT and group CPT. Evidence from a single RCT found individual TF-CBT had a small clinically important benefit above that of Group TF-CBT. Overall certainty of evidence for group TF-CBT is low.
The Guidelines also make a conditional recommendation for narrative exposure therapy (NET) in cases where trauma is linked to genocide, civil conflict, torture, political detention, or displacement. NET allows people with PTSD to describe and develop a coherent, chronological, autobiographical narrative of their life that includes their traumatic experiences (a testimony). Evidence from seven RCTs suggests clinically important benefit of NET for PTSD symptom severity in adults who have experienced genocide, civil conflict, torture, political detention, displacement or natural disaster. Overall certainty of the evidence for NET is low.
Pharmacological interventions
There has been little additional research into the pharmacological treatment of PTSD since the last edition of the Australian PTSD Guidelines in reference to pharmacotherapy and as a result little has changed in treatment recommendations. Psychological interventions are recommended as first line in the treatment of PTSD but there are a number of circumstances when pharmacological interventions should be considered. These include where the person is unwilling or not in a position to engage in or access recommended psychological therapy, has a comorbid condition or associated symptoms (e.g. clinically significant depression and high levels of dissociation), is not sufficiently stable to commence recommended psychological therapy (as a result, for example, of significant ongoing life stress such as domestic violence), has not gained significant benefit from recommended psychological therapy or there is a significant wait time before psychological treatment is available. In these circumstances, the Australian PTSD Guidelines make a conditional recommendation for selective serotonin reuptake inhibitor (SSRIs), specifically, sertraline, paroxetine, or fluoxetine. There is evidence from 18 RCTs suggesting a small, statistically significant but clinically unimportant benefit from SSRIs for PTSD symptom severity relative to placebo, with this evidence drawn from RCTs on sertraline (n = 5), paroxetine (n = 4) and fluoxetine (n = 9). In making this recommendation, the Guideline Development Group took into consideration the low certainty evidence for SSRIs but also drew upon their expert opinion that SSRIs play an important role in the treatment of PTSD for some adults.
Similarly, the Australian PTSD Guidelines make a conditional recommendation for the serotonin noradrenaline reuptake inhibitor (SNRI) venlafaxine in the same circumstances. Evidence from two RCTs suggest a small, statistically significant but clinically unimportant effect of Venlafaxine on PTSD symptom severity relative to placebo, and one RCT suggests no difference between venlafaxine and sertraline. Overall certainty of the evidence for venlafaxine is moderate. The Guideline Development Group took this into consideration but again drew upon their expert opinion in making this recommendation, that venlafaxine is important in the treatment of PTSD for some adults.
There is emerging evidence for two additional pharmacological agents in the treatment of PTSD – ketamine, an antagonist of the glutamate N-methyl-D-aspartate (NMDA) receptor and quetiapine, an atypical antipsychotic that is used for individuals with significant agitation. Both have shown moderate clinically important benefit relative to placebo in single RCTs. They are not currently recommended for use in clinical practice but have been recommended for further research. A summary of recommended treatments for adults is presented in Figure 5.
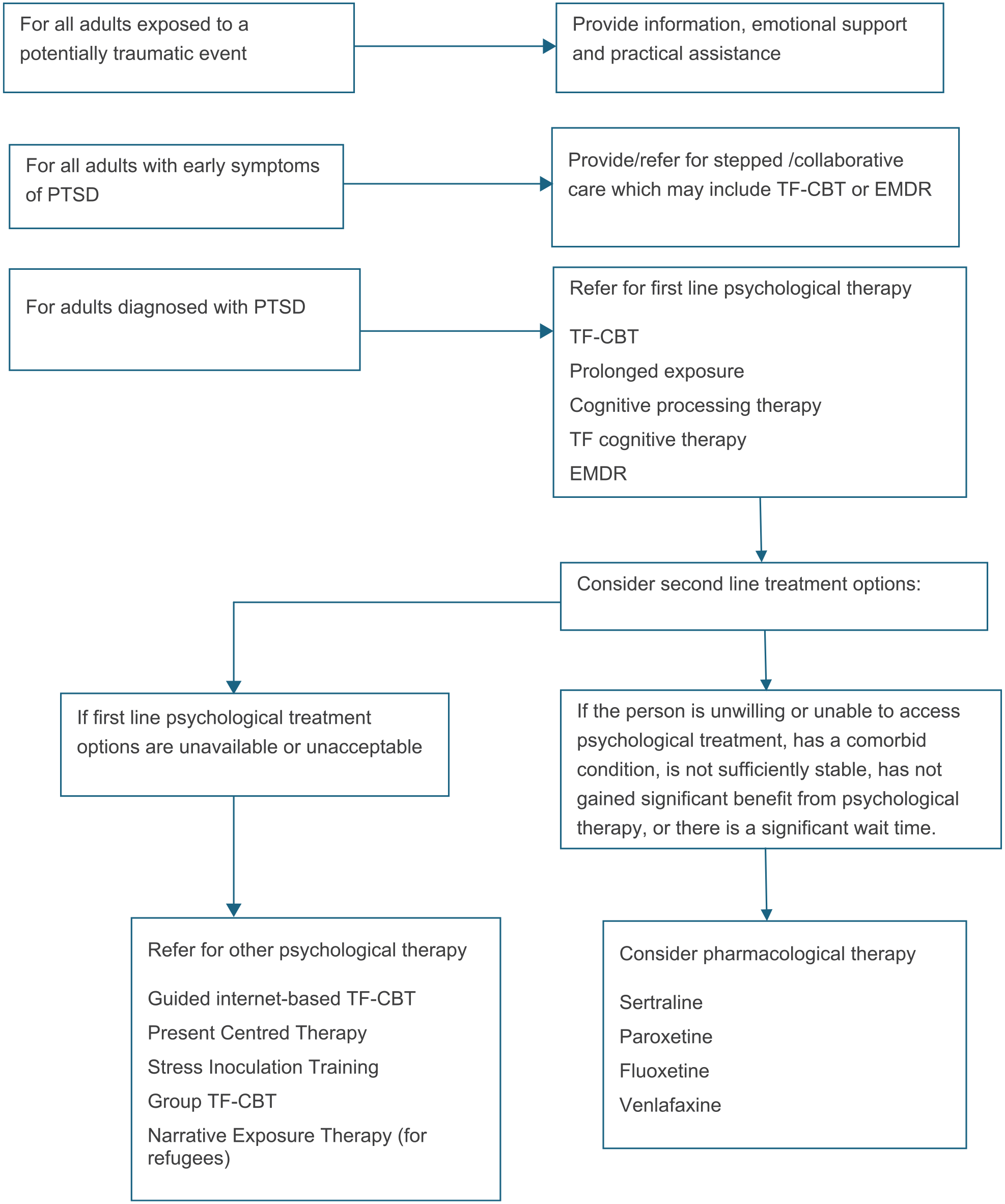
Summary of guideline recommendations for adults exposed to trauma.
Further advice for practitioners
The Australian PTSD Guidelines include substantial supporting chapters, which are also available through the Phoenix Australia website www.phoenixaustralia.org/australian-guidelines-for-ptsd/. These provide background information on trauma and PTSD as well as advice to health practitioners about issues to consider in applying the Australian PTSD Guidelines to particular groups or types of trauma. The groups include Aboriginal and Torres Strait Islander peoples, refugees and asylum seekers, military and ex-military personnel, emergency services personnel, and older people, and the types of traumatic events include motor vehicle accidents, crime, sexual assault, intimate partner violence, disasters and terrorism. These sections have been written in collaboration with subject matter experts.
Discussion
The Australian PTSD Guidelines are based on a systematic review of the latest international research. We hope they will be a valuable resource to guide decision making for practitioners, service planners, funders and those seeking treatment for trauma related mental health concerns. The new Australian PTSD Guidelines represent a significant advance in several ways. First, they were developed by a broad group of stakeholders comprising clinical and research experts, alongside a range of end users including practitioners and people with lived experience of PTSD. Second, they were developed using the new GRADE methodology, ensuring current best practice approaches to evaluating the quality and certainty of the research and ensuring transparency in the process of deriving recommendations from the research with the use of evidence to decision frameworks. Third, they have been developed as a living guideline, to allow revisions to be made in a timely manner as new evidence becomes available. This ensures that the Guideline recommendations are always current and represent the best available guidance. Fourth, with the introduction of the new diagnosis in ICD-11, the scope of the Guidelines was expanded to include consideration of CPTSD. As the results of research that is currently underway are published, specific treatment recommendations for people with CPTSD will be considered.
Limitations
As the ISTSS systematic review was used for the guidelines, the limitations of this review need to be acknowledged. First, outcomes were limited to PTSD symptom severity rather than broader mental health and functional outcomes or quality of life. We acknowledge the importance of considering a broad range of outcomes in assessing the benefit of treatment in a clinical setting. Second, the review did not assess levels of evidence lower than RCTs. As a result, emerging treatments that are showing promise in pilot studies or case studies have not been captured. Third, we acknowledge that despite a rigorous and comprehensive search strategy, it is possible that one or more studies that met the inclusion criteria could have been missed. Finally, any errors in the ISTSS systematic review would have carried through into the current Guidelines.
Although the guideline recommendations are based on the international published research which includes a broad range of people from high- and low-income countries as well as culturally and linguistically diverse backgrounds, it is important to acknowledge that the Guideline Development Group did not undertake sub-group analyses to consider the impacts of treatment on people who have experienced different types of trauma. Further, it needs to be acknowledged that some populations are underrepresented in the published research. For example, there is a dearth of research focused on members of the lesbian, gay, bisexual, trans/transgender, intersex, queer and asexual (LGBTIQA +) community, despite evidence of greater risk of exposure to interpersonal trauma in this group (Roberts et al., 2010). Of particular note in the Australian context, none of the studies in the systematic review has a specific focus on the treatment of trauma in Australian Aboriginal or Torres Strait Islander peoples, and few Australian studies include asylum seekers and refugee groups. This represents a significant gap in the evidence base for an Australian guideline for the treatment of PTSD. We suggest that for many of these population groups, histories of human rights violation and severe trauma, experiences of marginalisation and discrimination and the potential loss or fragmentation of psychosocial and cultural resources can shape the meaning(s) and presentation of distress, understandings and expectations of treatment and the trajectories of recovery from PTSD and other trauma related difficulties. There is an urgent and compelling need for research to address this gap in our understandings of cultural shaped models of trauma and recovery, and what constitutes best evidence based practice for these populations.
Although the recommendations contained in the Guidelines reflect what is currently considered best practice, the limitations of recommended treatments should be acknowledged. Not everyone responds optimally to first line treatments for PTSD, and more research is required to adequately address the issues of relapse and treatment resistance in PTSD. Future Guidelines should address the management of chronic PTSD with physical and mental comorbidities, and the developing area of personalised medicine.
Next steps
The next critical stage for the Australian PTSD Guidelines is implementation. In a field replete with alternative unproven treatment approaches, the gap between guideline-recommended evidence-based practice and routine clinical care still remains significant (Spence et al., 2011). Effective implementation of evidence-based guidelines is therefore of critical importance. It should be acknowledged that effective implementation is a major challenge that requires a multi-faceted approach targeting service systems, individual practitioners and people with lived experience. In addition to publications in the peer-reviewed literature and presentations in professional forums, a range of companion documents that contain plain language descriptions of the guideline recommendations for lay audiences are available from the Phoenix Australia website.
We are undertaking ongoing surveillance of the published literature to guide future decisions about which recommendations are due to be refreshed. This will be a systematic process guided by the volume of new research relative to the volume and certainty of existing evidence. In some areas, such as pre-incident preparedness and the treatment of CPTSD, the dearth of current research means that new recommendations may be warranted on the basis of a small number of high quality trials. This is in contrast to other areas, such as the current strong recommendations for psychological treatments for PTSD in adults, that to change, would require a large volume of new high quality research.
Footnotes
Acknowledgements
Author NoteGraham Gee is now affiliated to School of Psychological Sciences, University of Melbourne, Parkville, VIC, Australia.We gratefully acknowledge the important contribution of our lived experience representatives on the Guideline Development Group, Mr Steve Dunning and Ms Lisa Massey. We also gratefully acknowledge the collaboration with the team from Cardiff University School of Medicine who undertook the ISTSS systematic review, Professor Jonathon Bisson, Dr Neil Roberts and Dr Catrin Lewis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the Commonwealth Department of Health [Deed number 60002795].