
Abstract
Background:
The transition out of inpatient mental health is a crucial time for adults experiencing concurrent mental illness and homelessness, yet evidence regarding effective support options is mixed. Choices is an intensive 3-month psychosocial outreach and crisis accommodation support programme for adults experiencing mental illness and homelessness, delivered by Baptcare in Tasmania, Australia. This study examined the effect of Choices on adults’ psychosocial functioning, clinical symptomology and psychiatric readmissions in comparison to standard care only.
Method:
Participants were adults aged 18–64 years experiencing mental illness and homelessness, recruited upon discharge from a psychiatric admission. Intervention participants (n = 124) received the Choices programme. Control participants (n = 122) received standard care, clinical assessment and treatment from hospital-based Mental Health Services. Outcomes were psychosocial functioning (primary), clinical symptomology, hospital readmission rate and readmission length of stay. Outcomes were assessed at programme commencement and closure (3 months) and 3 months post-closure (intervention group only). Analysis of covariance was used to analyse differences between groups at closure, while controlling for baseline differences.
Results:
Intervention participants had significantly improved social functioning (encompassing living conditions, social relationships, self-esteem/confidence), overall psychosocial functioning, symptoms of depression and anxiety and shorter hospital readmission length of stay in comparison to the control group. Intervention participants experienced further improvements in social and overall psychosocial functioning 3 months post-closure.
Conclusion:
The Choices programme is effective in enhancing the psychosocial functioning of adults experiencing concurrent mental illness and homelessness. These findings support the ongoing delivery of this combined accommodation and wrap-around psychosocial model of intensive support.
Introduction
Mental illness and homelessness (i.e. encompassing housing insecurity and risk of homelessness) pose significant challenges to health and social care systems worldwide (World Health Organization [WHO], 2018, 2023). Approximately 76% of adults (ranging between 64% and 96%) experiencing homelessness also have mental health concerns (Gutwinski et al., 2021). This prevalence is concerning given the inequities and adverse impacts that people living with these comorbidities experience (Smartt et al., 2019). This includes difficulties in various areas of psychosocial functioning such as economic participation, community engagement, social functioning and independent living (Jones et al., 2020; Roy et al., 2014). In Australia, people with a mental illness are more than twice as likely to experience homelessness than those without mental health concerns (Australian Bureau of Statistics [ABS], 2016). Furthermore, those with a history of homelessness are significantly more likely to experience mental illness compared to those who are not homeless (54% vs 19%, Australian Institute of Health and Welfare [AIHW], 2023). The rates of concurrent mental illness and homelessness continue to exponentially increase, having doubled in the past decade (AIHW, 2022). This is likely attributed to key social determinants of health that are considered risk factors for homelessness and are disproportionately experienced by those with mental illness, including lack of affordable housing (i.e. ‘housing crisis’) increased rental stress, rising costs of living, job insecurity, unemployment, income inequality, increased financial stress, poverty and family violence (AIHW, 2022).
Transition from an inpatient mental health admission is recognised as a crucial time for adults experiencing concurrent mental illness and homelessness, who are often discharged to unstable accommodation or the streets (Laliberte et al., 2019). Without appropriate supports for this population, especially in the first month post-discharge, this period can adversely impact adults’ functioning or exacerbate existing psychosocial difficulties. Psychiatric readmission rates are high for this population group (Currie et al., 2018; Laliberte et al., 2019; Russolillo et al., 2023). Homelessness is consistently associated with increased 30-day readmission rates and length of stay (LOS) among adults with mental illness (Laliberte et al., 2019); they are almost twice as likely to be rehospitalised in 90 days (Russolillo et al., 2023). Individuals experiencing these concurrent concerns often require intensive intervention to navigate this transition.
Community-based Mental Health Services (MHS) are necessary to help support and stabilise adults through this transition. Mental health-supported accommodation integrated with assertive outreach models of support (e.g. Housing First principles) consistently yields positive housing outcomes for individuals experiencing mental illness (Keenan et al., 2021; McPherson et al., 2018; Tinland et al., 2020). More specifically, Critical Time Intervention (CTI) is one model of support designed to assist individuals at risk of homelessness during life course transitions (e.g. following hospitalisation). CTI aims to strengthen integration and connection to community, including services, supports and social networks, to facilitate a smooth transition (Herman et al., 2011). CTI has been shown to consistently reduce homelessness and increase service engagement among those experiencing mental illness post-transition period (Manuel et al., 2022). However, findings related to other psychosocial outcomes (e.g. social functioning and symptom severity) have been mixed (Manuel et al., 2022). The CTI literature provides a strong foundation of evidence to support the implementation of targeted and relatively short intervention to facilitate transitions for adults experiencing concurrent homelessness and mental illness (Herman et al., 2011; Manuel et al., 2022; Ponka et al., 2020).
One particular programme informed by CTI is Choices, an intensive short-term (3 months) psychosocial outreach and crisis accommodation programme to support people experiencing mental illness and homelessness following a psychiatric admission in South Tasmania, Australia. The programme is delivered by Baptcare (2023), a not-for-profit community service organisation that provides a range of support, including aged care, disability support, foster care and family support programmes. Baptcare provides state-wide community-based psychosocial support for adults through its Mindset TAS service. Choices aims to support clients’ transition to independent living following psychiatric admission via Baptcare-operated crisis accommodation and assertive outreach wrap-around support. While similar to CTI in its target population, time-limited approach and core aims, Baptcare’s Choices model is unique in its provision of crisis accommodation, assertive outreach approach, lower caseloads and shorter duration. Furthermore, while underpinned by the evidence-based and recovery-oriented principles of Housing First, the Choices programme focuses on time-limited transitional support as opposed to the longer-term/permanent support offered by Housing First with Intensive Case Management or Assertive Community Treatment (Keenan et al., 2021; McPherson et al., 2018).
There is a lack of controlled evaluation of community-based programmes to support adults experiencing mental illness and homelessness following psychiatric admission, with limited Australian evidence. Specifically, Baptcare’s Choices model of support is yet to be evaluated. Therefore, this study aimed to examine the effectiveness of the Choices programme on adults’ psychosocial functioning, clinical symptomology and hospital readmissions in comparison to standard care only. It was hypothesised that the intervention group (Choices clients) would experience significantly greater improvements in their psychosocial functioning by programme closure in comparison to the control group.
Methods
Study design and setting
A non-randomised parallel controlled study design was employed. The study was conducted in Southern Tasmania, Australia, over 3 years from October 2019 to December 2022. Ethics approval was obtained from the Tasmanian Health and Medical Human Research Ethics Committee (18536) and Monash University Human Research Ethics Committee (39250). This study was registered with the Australian New Zealand Clinical Trial Registry (ACTRN12620000673943). Reporting aligned with the CONSORT guidelines (see Supplemental material, Schulz et al., 2010).
Participants
Participant eligibility for this study included adults who were (1) aged 18–64 years living in Tasmania; (2) diagnosed with a mental illness; (3) about to exit an inpatient mental health admission upon programme referral; (4) actively case managed by state-wide MHS, who provided ongoing clinical care and follow-up post-hospitalisation; (5) were voluntarily willing to engage; (6) could manage their own activities of daily living (assessed by nursing staff prior to discharge); and (7) verbally consented to having their assessments shared with the research team. In addition to the above criteria, eligibility for the Choices programme (intervention) included clients who were homeless/at risk of homelessness 1 or identified as requiring intensive psychosocial support to prevent hospital readmission. Participant eligibility for the control group included those who met the above criteria and were engaged with MHS only. Exclusion criteria included (1) engagement in another community-based psychosocial or accommodation support programme or (2) on an involuntary order. As group allocation could not be randomised nor concealed, participants were matched based on key demographic characteristics (e.g. age, gender, relationship status, programme engagement/duration and mental health diagnoses). Participants were recruited between January 2020 and June 2022; the final follow-up was completed in December 2022. All MHS clients who met the above criteria (i.e. voluntarily engaged with MHS only with no community-based supports) and entered the programme during the study timeframe were asked if they consented to having their routinely collected assessments shared with the research team. Only those who consented were included in this study.
Intervention – the Choices programme
The Intervention programme was Choices – a nationally accredited, intensive, short-term (3 months) psychosocial outreach and accommodation programme to support people experiencing mental illness and homelessness in Southern Tasmania, Australia. Choices provided Baptcare-operated crisis accommodation combined with assertive outreach psychosocial support for the first 2 months, followed by an additional month of community support, to facilitate the client’s transition to more stable housing, independent living and community integration. The programme was underpinned by strength-based and recovery-oriented mental health practice as it drew upon the abilities, goals and resources of the client to facilitate improvements in their psychosocial wellbeing.
Clients were referred into the Choices programme upon discharge from an inpatient mental health stay. Referral sources included MHS, mental health inpatient units, the local specialist psychiatric hospital, hospital in the home or residential short-stay units. The suitability of each referral was initially discussed with the Choices senior practitioner to determine if the client met the programme criteria as described above (i.e. experiencing/at risk of homelessness, requiring intensive psychosocial support) and if there was current capacity at the shelter. Once referred, clients had access to crisis accommodation – Baptcare operated one male shelter (Karingal) and one female shelter (Rose Cottage) in Southern Tasmania. This involved housing with three to four other Choices clients, with rotating staff who visit the shelter every day to ensure that their basic needs are being met. Clients were allocated a key practitioner who visited the client regularly, depending on their needs. Practitioners engaged clients in a collaborative goal-setting process to identify and set their own personalised short-term psychosocial goals and assisted clients in achieving such goals. Examples of key goals included achieving safe and stable housing, fulfilling activities of daily living (i.e. self-care, cooking, etc.) or improving social connections with family/peers. Brokerage was also available to fund activities that may help clients achieve their psychosocial goals (i.e. pay first month of rent) or to provide them with basic necessities (e.g. furniture).
Choices practitioners were trained and experienced mental health clinicians with various backgrounds (i.e. social work, community services) and significant community services experience who were well-equipped to support individuals experiencing mental illness. Practitioners managed a small caseload of five clients each, which facilitated the provision of intensive, flexible and tailored support, depending on each client’s unique needs. Practitioners received regular reflective practice, one-on-one and peer group supervision, training and professional development opportunities. Choices practitioners also often worked collaboratively with clients’ hospital-based case manager from MHS, who coordinated their ongoing clinical care post-hospitalisation.
Control –MHS
Participants in the control group received standard care only – clinical case management from MHS (hospital-based). Control group participants received support via their MHS Case Manager for an average of 3 months post-psychiatric admission. MHS is operated through the Tasmanian Department of Health and provided individuals with ongoing clinical assessment, treatment, education and support to manage their mental illness and promote clinical improvements. MHS focused solely on addressing the clinical symptoms of the mental illness. MHS case managers were embedded within a team of clinical psychologists, psychiatrists, mental health nurses and other specialist medical staff to provide clinical support. MHS case managers had a caseload of approximately 25 clients and provided ongoing assessment, psychoeducation, symptom management, administered medication and monitored medication adherence. Participants’ frequency of contact with MHS was approximately fortnightly, comprising of in-person visits to the local outpatient clinic or telephone support. Outreach was not part of standard care.
Outcome measures
Demographic information was collected at baseline, upon clients’ referral into the programme. Demographic characteristics included age, gender, country of birth, relationship status, the highest level of education achieved and any mental health diagnoses given by MHS. Participants were assigned a unique code, so all data provided to the research team were de-identified.
The Behavioural and Symptom Identification Scale and the Health of the Nations Outcomes Scale were completed at baseline (upon entry into the programme) and closure (approximately 3 months later) to assess psychosocial functioning (primary outcome) and clinical mental health symptomology (secondary outcome). Intervention participants also completed both measures at 3 months post-closure (follow-up). Ethics approval to collect follow-up data for the control group (i.e. MHS service-users) was not obtained for this study. Data were collected by the allocated Choices practitioner (intervention group) or MHS case manager (control group) in collaboration with the client. MHS use these two measures routinely to inform case planning; so they were embedded into standard practice within the Choices programme. Practitioners received training in administering the two questionnaires to ensure inter-rater reliability. A manual was provided to practitioners that included definitions for each item on the measures to minimise variability associated with individual interpretation.
The Behavioural and Symptom Identification Scale (BASIS-32) is a 32-item questionnaire used to assess psychosocial functioning. It specifically measures the extent of difficulty that an individual experiences in their psychosocial functioning across five domains: (1) relation to self and others; (2) daily living and role functioning; (3) depression/anxiety; (4) impulsive/addictive behaviour and (5) psychosis. Each item was scored on a 5-point Likert-type scale from 0 (no difficulty) to 4 (extreme difficulty). Participants received an average score for each of the five domains, as well as an overall total average score. Higher scores indicated greater impairment/difficulty in psychosocial functioning. The BASIS-32 has high concurrent validity and internal reliability (a = 0.75–0.91, Cameron et al., 2007) and has previously been used with participants experiencing comorbid homelessness and mental illness (e.g. Dunt et al., 2016; Smelson et al., 2018).
The Health of the Nations Outcomes Scale (HoNOS) is a 12-item questionnaire used to assess the severity of clinical mental health problems across four domains: (1) behaviour (i.e. aggression, overactivity, problem drinking, drug taking, self-injury); (2) impairment (i.e. cognitive concerns, physical illness or disability); (3) symptomology (i.e. symptoms of anxiety/depression/psychosis) and (4) social functioning (i.e. social relationships, daily activities, living conditions, employment). Items were rated on a 5-point Likert-type scale from 0 (no problem) to 4 (severe problem). Participants received a total score for each domain and an overall clinical score. Higher scores indicated greater severity of clinical mental health symptomology. The HoNOS is well-regarded as a valid tool with moderate internal consistency (a = 0.59–0.76, Pirkis et al., 2005) and has been extensively used with populations experiencing homelessness (e.g. Casavola et al., 2023; Dunt et al., 2016).
Finally, de-identified hospital data for both groups were provided to the research team by the Tasmanian Health Service. Data included date of hospital admission; reason for admission; LOS and date of discharge. These data were used to assess the number of psychiatric-related hospital readmissions and LOS within 3 months of programme closure for each participant.
Data analyses
All quantitative analyses were performed using IBM SPSS Statistics Version 28. All raw data were entered into SPSS, and a conservative intention-to-treat (ITT) analysis was used to assess outcomes. Chi-square tests were used to calculate differences between groups on categorical baseline characteristics and hospital readmission rates. Independent t-tests were used to calculate differences between groups for baseline age and length of readmission stay. Paired sample t-tests were conducted to compare intervention participants’ mean differences on each outcome measure from closure to 3-month follow-up. Univariate analysis of covariance (ANCOVA) was used to examine differences in post-intervention (closure) scores on the outcomes measures between the intervention and control groups, while controlling for the baseline scores. The baseline time 1 scores therefore served as covariates for the dependent time 2 variables. ANCOVA was chosen to control for non-randomisation pre-test differences in scores (e.g. varying severity of scores and demographic characteristics). The original significance level of the pre-post change in outcome measures was set at p < 0.05. A Bonferroni correction was applied, where multiple comparisons were tested in ANCOVA to account for type 1 error (Larzelere and Mulaik, 1977). Sample calculations were conducted using G*Power, with a total of 194 participants required to detect statistically significant differences in outcome measures between groups with 80% power.
Results
Participant characteristics
Figure 1 shows the CONSORT flow diagram of participation across both groups. A total of 246 adults participated in the study (n = 124 for intervention group and n = 122 for control group completed both baseline and closure assessments). Seventy-seven intervention participants (62%) completed the 3-month follow-up assessment. The remaining 47 intervention participants (38%) were lost to follow-up, as they did not provide consent/declined to participate in the 3-month follow-up component (n = 27, 57%) or were uncontactable at the 3-month follow-up time-point after three attempts (n = 20, 43%).
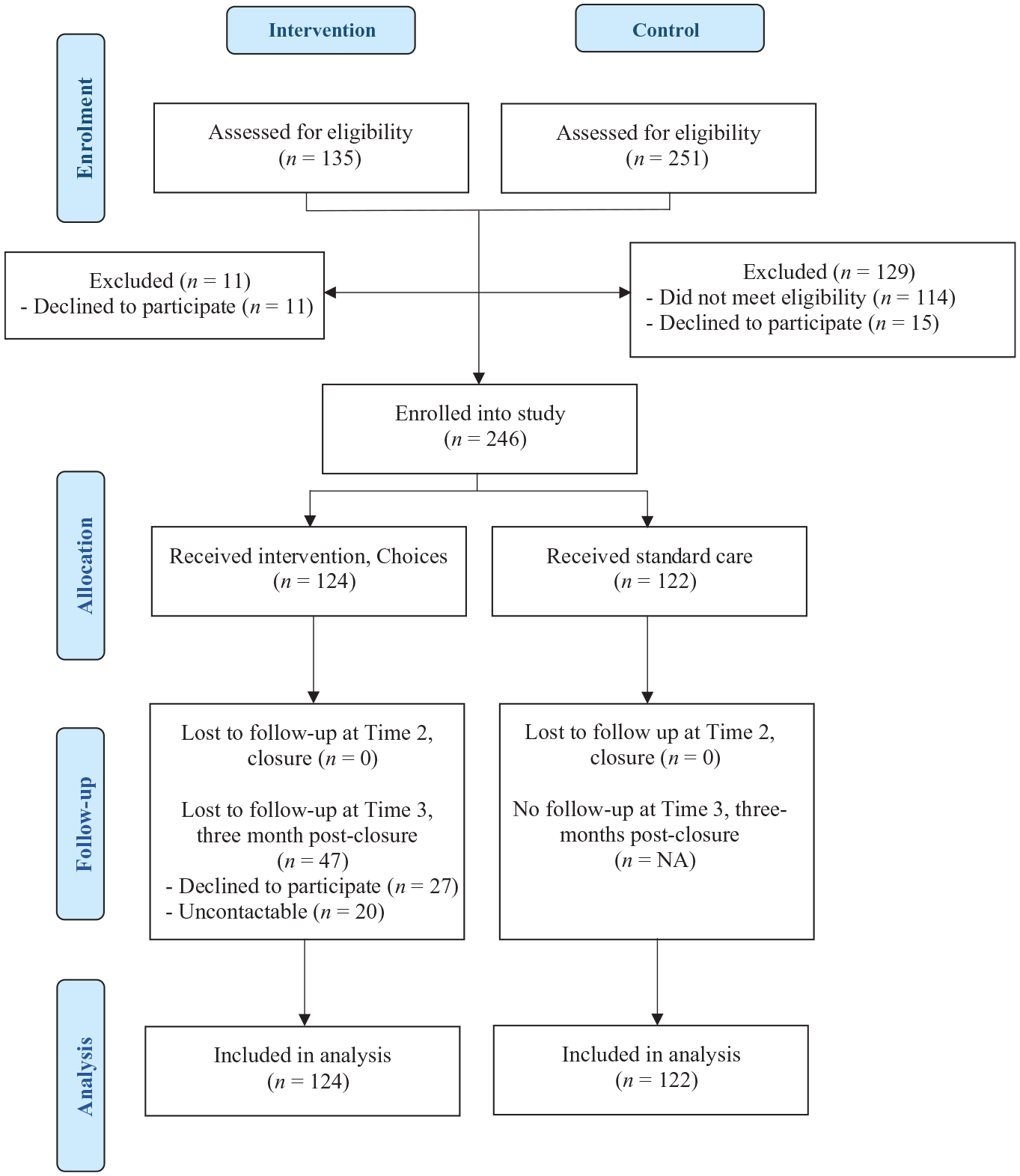
CONSORT flow diagram of participation.
Overall, there were no statistically significant differences in participant demographic characteristics between groups. On average, participants were 40 years of age, identified as male, were single, born in Australia, and most commonly experiencing depressive and/or anxiety disorder, followed by schizophrenia.
Intervention fidelity
Participants engaged in Choices for three and a half months on average (M = 3.63; SD = 1.9, n = 124). While in accommodation, clients were visited by their practitioner every day for 1.5 hours on average, ranging from 0.5 to 2 hours visits (M = 1.48; SD = 0.51). Once clients had transitioned out of the shelter, client received approximately two visits per week from their key practitioner for 1.5 hours on average, at their new place of residence or in the community (i.e. café, park, transport to and from appointments, walk). Practitioners completed an average of four background (non-client) hours per week per client (M = 4.22; SD = 1.36), which included outreach travel time, administration or referral/service navigation.
BASIS
Baseline and closure mean (SD) scores for participants on the BASIS, and the post-test univariate ANCOVA analysis, are presented in Table 1. There was a significant baseline difference between groups on the depression/anxiety scale, which was accounted for by the ANCOVA analysis. There was a significant post-intervention difference between groups on the BASIS overall with a small effect size (F[1, 245] = 9.307, p = 0.003,
Intervention effect: pre- and post-test mean (SD) scores and post-test univariate ANCOVA.
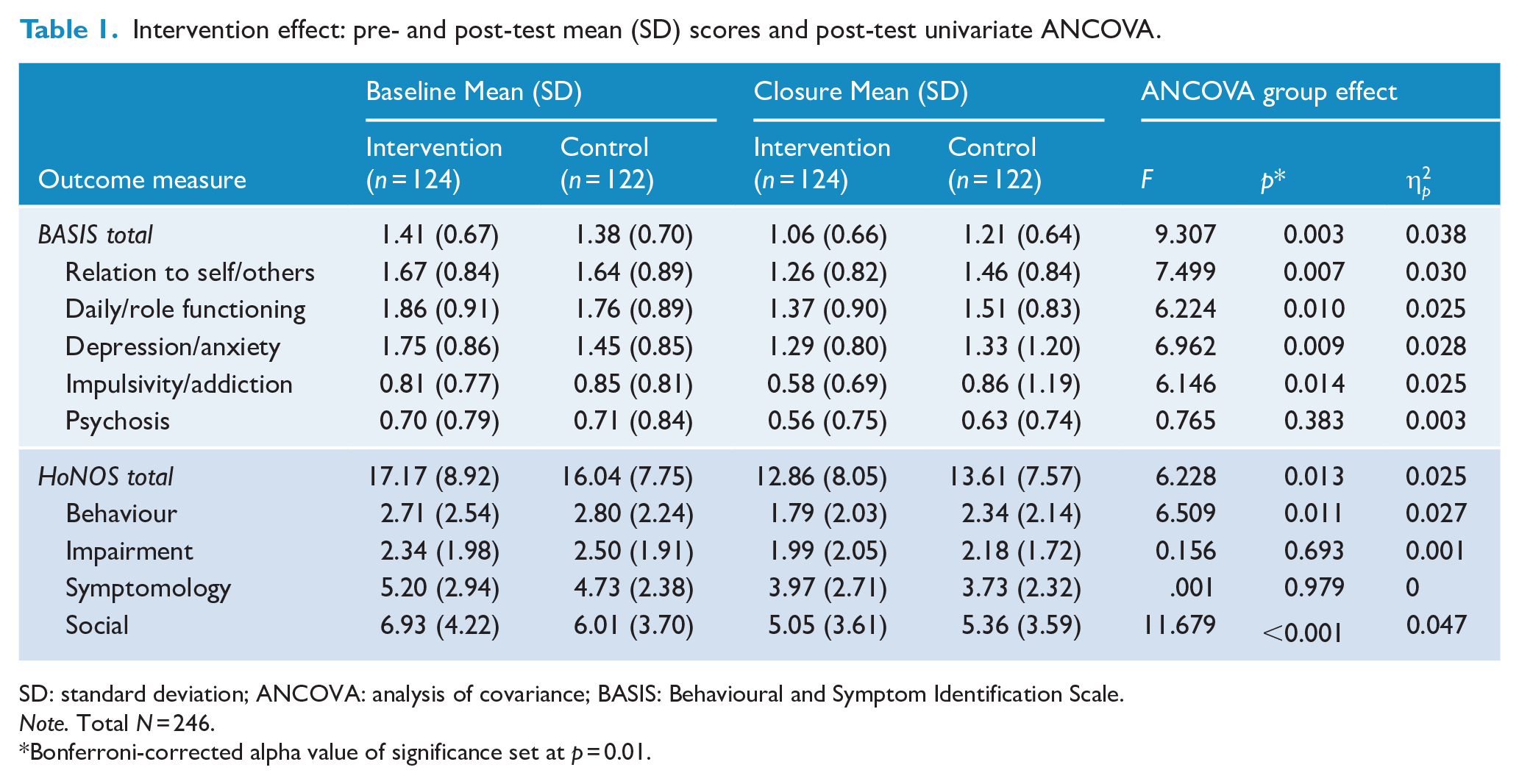
SD: standard deviation; ANCOVA: analysis of covariance; BASIS: Behavioural and Symptom Identification Scale.
Note. Total N = 246.
Bonferroni-corrected alpha value of significance set at p = 0.01.
Table 2 shows the paired t-test comparisons between closure and 3-month follow-up for intervention participants. At follow-up, intervention participants had a larger improvement in their relationships with self and others (T[1, 76] = 2.846, p < 0.006, d = 0.37), and on their psychosocial functioning overall, as indicated by the BASIS total score with medium effect size (T[1, 76] = 3.540, p < 0.001, d = 0.47).
Intervention follow-up effect: paired t-test comparisons for intervention group at 3-month-follow-up.
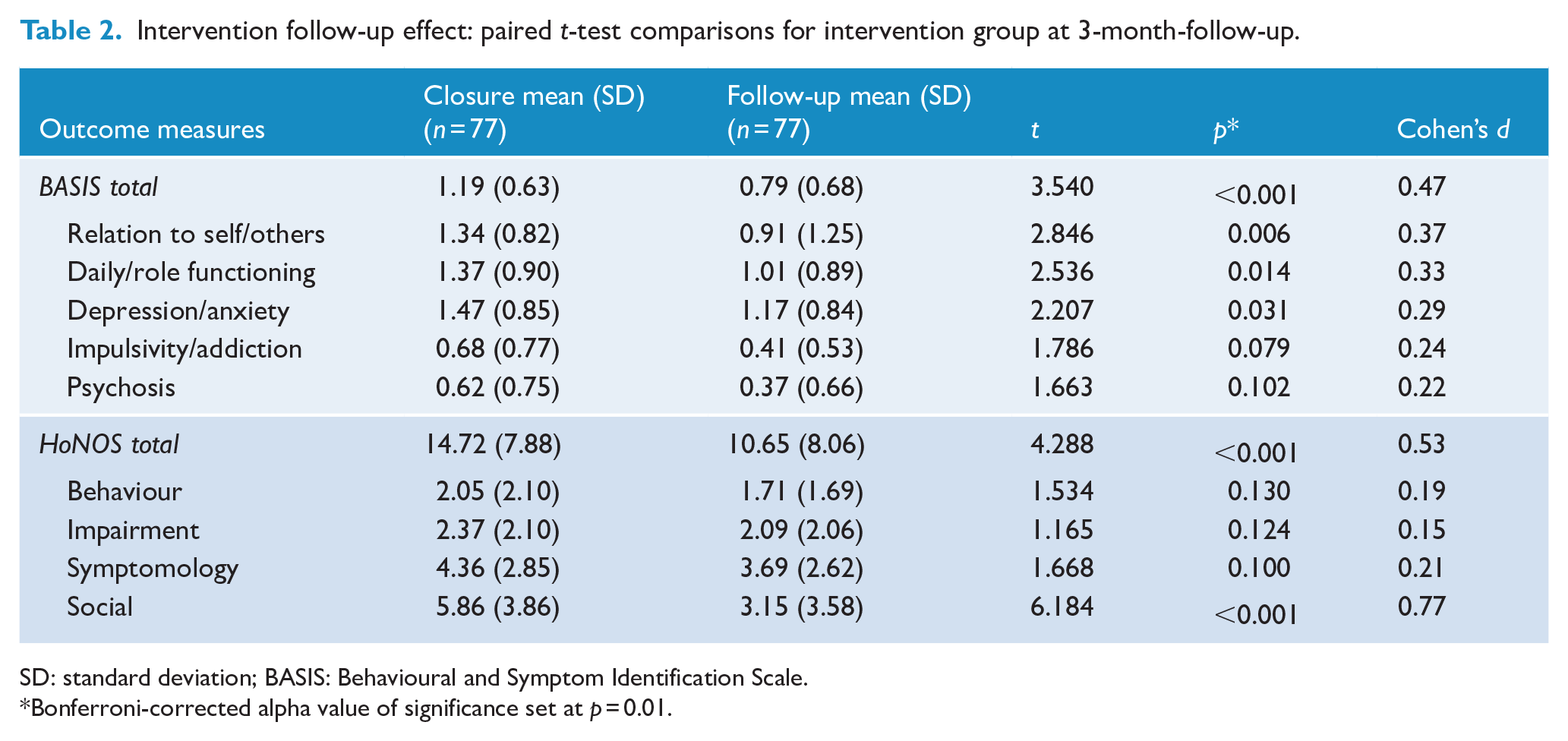
SD: standard deviation; BASIS: Behavioural and Symptom Identification Scale.
Bonferroni-corrected alpha value of significance set at p = 0.01.
HoNOS
Table 1 shows the baseline and closure mean (SD) scores for participants on the HoNOS and the post-test univariate ANCOVA analysis. There were no significant baseline differences between groups. There was a significant post-intervention difference between groups on the Social Functioning domain of the HoNOS, with a small effect size (F[1, 245] = 11.68, p < 0.001,
At 3-month follow-up (see Table 2), intervention participants had a significant improvement on the social domain, with a large effect size (T[1, 76] = 6.184, p < 0.001, d = 0.77). There was also a significant difference on the total HoNOS score, indicating a significant decrease in the severity of their overall clinical symptomology between closure and 3-month follow-up (T[1, 76] = 4.288, p < 0.001, d = 0.053).
Psychiatric readmissions
Table 3 presents the rate of psychiatric readmissions 3 months after programme closure across both groups. There were no significant differences in the number of readmissions between groups, with 12% of the total sample experiencing one readmission and 5% having more than one readmission. Among those who did experience a readmission, intervention participants had a significantly shorter LOS (M = 18 days) than the control group (M = 46 days).
Psychiatric readmission outcomes between groups 3 months post-closure.
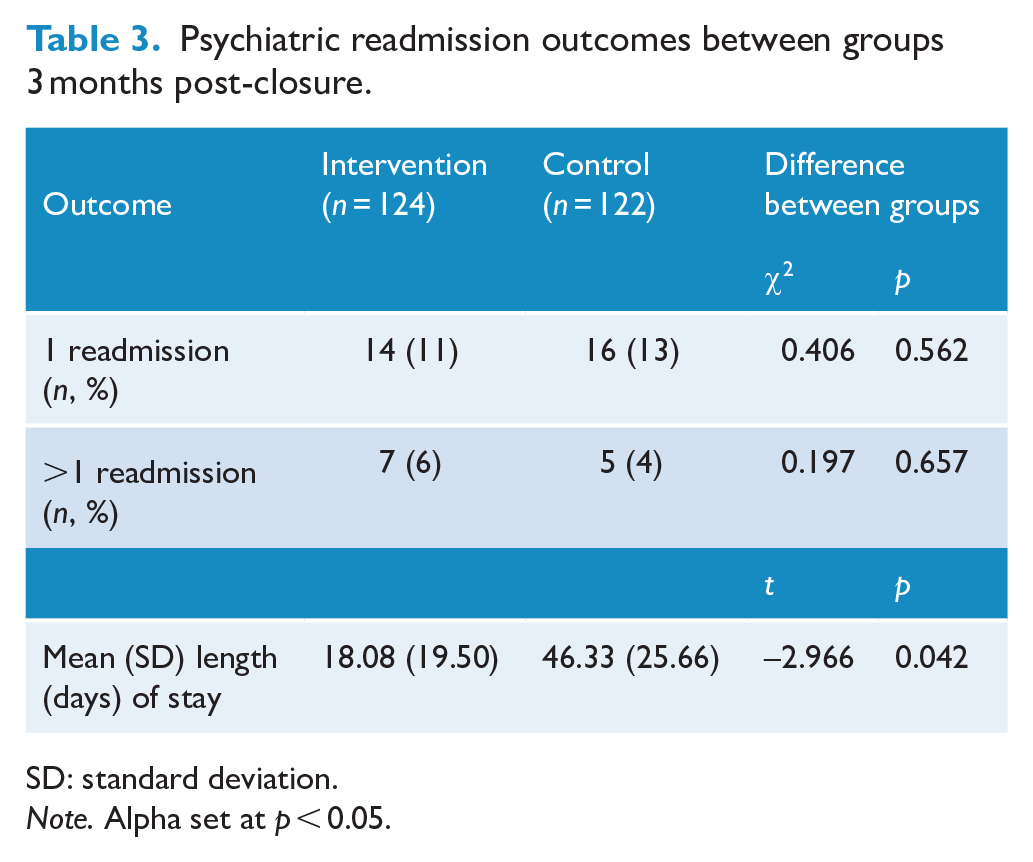
SD: standard deviation.
Note. Alpha set at p < 0.05.
Discussion
To the authors’ knowledge, this is the first study examining the effectiveness of crisis accommodation and psychosocial outreach support for individuals following an inpatient mental health admission in Tasmania, Australia. This is a crucial point of transition for individuals experiencing mental illness and homelessness, yet there remains a lack of evidence regarding effective support options for this population. Therefore, this controlled study aimed to examine the effectiveness of Baptcare’s Choices programme on adults’ psychosocial functioning, clinical symptomology and hospital readmissions in comparison to standard clinical care. The hypothesis that the intervention group (Choices) would experience significantly greater improvements in their psychosocial functioning in comparison to the control group was supported.
By programme closure, Choices participants had better social functioning, which encompassed improved living conditions, engagement in employment/activities, social relationships, self-esteem, self-confidence and daily functioning (i.e. engaging in activities of daily living and managing household responsibilities). The current findings contrast previous research that has shown inconsistent/insufficient evidence to demonstrate improvements in social functioning and community integration among mental health crisis accommodation services (McPherson et al., 2018; O’Donnell et al., 2022). Uniquely, the current evaluation clearly demonstrates that the Choices programme can yield such outcomes above and beyond that of standard clinical care. This may likely be due to two unique programme components: small caseloads and assertive outreach. In comparison to the MHS high caseload of 25:1, the Choices caseload of 5:1 promoted adaptability and flexibility, enabling a more tailored and personalised approach to care that was responsive to each client’s unique needs. The small caseloads also facilitated assertive outreach, in which practitioners deliver place-based support with an emphasis on persistent and intensive engagement (Ponka et al., 2020). Assertive outreach also contributed to strengthening client–practitioner relationships, tailoring support and maintaining engagement (Jiménez et al., 2022). These programme components underpin the recovery-oriented approach of the Choices programme in providing safe and secure housing, ensuring that clients’ basic needs are met, focusing on the transition to more stable housing and community integration and supporting clients to achieve their short-term psychosocial goals.
The follow-up findings indicate that Choices clients had further improvements on key psychosocial outcomes 3 months post-programme, particularly in their social functioning and relationships with others (i.e. family, peers, community) and self (i.e. self-esteem, confidence). This highlights that the short-term and intensive wrap-around support provided by Choices can yield longer-term benefits for its clients. All other outcomes remained consistent, which suggests that clients were able to sustain the positive improvements observed at closure. The unique additional month of intensive psychosocial outreach support provided by Choices may enhance clients’ capacity to implement and consolidate newly learned skills, increased knowledge and build resilience and capacity, which are associated with improved quality of life among this population (Mejia-Lancheros et al., 2021). This emphasises the utility of this combined model of support to facilitate adults’ journey from inpatient admission, crisis accommodation, to independent living. Ultimately, these findings are unique as there is a dearth of existing follow-up exploration among this population following psychiatric admission, likely due to high rates of participant attrition among individuals experiencing severe mental illness (Strehlau et al., 2017). Further investigation to reduce follow-up drop-out, compare follow-up outcomes across both groups and extend follow-up duration is required.
Both standard clinical care and psychosocial support yielded significant reductions in participants’ clinical symptom severity. However, there were no significant differences between groups by programme closure in clinical outcomes (i.e. externalising, internalising, physical/cognitive impairment, impulsivity, addiction and psychoses). This aligns with existing mixed evidence of general integrated housing and psychosocial support programmes (Kerman et al., 2020). Nonetheless, intervention participants reported reduced functional impairment associated with the symptoms of depression and anxiety at programme closure in comparison to the control group. This finding demonstrates the additional value of intensive wrap-around psychosocial support by addressing the underlying stressors or functional impact that may often arise from or perpetuate comorbid mental illness and homelessness.
The intervention group had a significantly shorter readmission LOS, which extends current evidence (Baxter et al., 2019; Laliberte et al., 2019). This may be attributable to key components of the intervention, such as supporting clients’ autonomy, independence, community integration, resilience or capacity to cope or may indicate reduced severity and complexity of psychosocial needs, which are factors associated with reduced LOS (Crossley and Sweeney, 2020). Furthermore, the daily cost for a psychiatric admission in Tasmania is $735 (Department of Health, 2023). With Choices clients reporting an LOS of 28 days less than the control group on average, this equates to a saving of $20,580 per Choices client.
Key limitations of this study are acknowledged to highlight potential areas of future research. First, group randomisation or concealment was not feasible due to the eligibility criteria/referral processes of the intervention and the timeliness of support required upon exit from an inpatient mental health stay; it would have also posed ethical challenges if treatment was withheld/delayed. Therefore, matching was implemented to avoid significant differences between groups in demographic characteristics that could have confounded the results, and the ANCOVA analysis enabled more accurate comparisons to be made between groups at closure by controlling for any differences in the severity of scores at baseline. Second, the HoNOS and BASIS are routinely used at MHS (control group) and were embedded into the Choices programme to enable comparisons. As both measures were completed by the practitioner in collaboration with the client, there is potential for positive or negative impression management, which may have biased the results. Furthermore, housing/homelessness was not directly measured, although it is included under the ‘social’ domain of the HoNOS. It is therefore recommended that a more holistic and recovery-oriented psychosocial outcome tool/measure is embedded into standard practice of the Choices programme to capture outcomes of most relevance to the goals of the programme, for example, securing safe and stable housing.
A further limitation is the high rate of attrition at 3-month follow-up. While the inclusion of follow-up is a strength of this evaluation, 40% of the intervention participants either declined to participate in follow-up or were not contactable after three follow-up phone-call attempts (i.e. did not respond). This is common among participants experiencing persistent mental illness and homelessness, potentially due to the transient nature and life circumstances of these participants (Strehlau et al., 2017). The high rate of attrition may have positively skewed the current findings, with participants who were thriving/stable post-intervention more likely to be contactable and consent to participate in the follow-up component. Alternative/flexible attempts at follow-up research are required with this population. Furthermore, not having follow-up data from the comparison group is a significant limitation. Future research would benefit from a longer-term follow-up period of both intervention and control groups to observe longer-term comparisons between groups and examine bidirectional relationships between outcomes (i.e. psychosocial functioning and symptomology).
The current findings advance the Australian evidence base, highlighting the value of crisis accommodation and psychosocial outreach support for adults experiencing mental illness and homelessness following an inpatient psychiatric admission. The Choices programme achieved improvements in clients’ psychosocial functioning above and beyond that of standard clinical care, strengthening the evidence base for this programme. The findings also provide support for its ongoing implementation and potential for scale-up. The exit from an inpatient mental health admission is an important time of intervention, and the Choices model of combined outreach support and accommodation demonstrates its sustainability to support clients’ journey to independent living. As the only psychosocial service of its kind in the state with this level of evidence, it is crucial that Choices is appropriately resourced to continue enhancing the psychosocial wellbeing of individuals experiencing mental illness.
Supplemental Material
sj-doc-1-anp-10.1177_00048674241270996 – Supplemental material for A non-randomised controlled trial of a community-based accommodation and psychosocial support programme for adults experiencing mental illness and homelessness
Supplemental material, sj-doc-1-anp-10.1177_00048674241270996 for A non-randomised controlled trial of a community-based accommodation and psychosocial support programme for adults experiencing mental illness and homelessness by Melissa Savaglio, Ash Vincent, Nicholas Merklin and Helen Skouteris in Australian & New Zealand Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Baptcare.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.